
Abstract
This study theoretically develops a three-stage model in which certain types of health behavior functions (i.e., health-affirming vs. health-detection/treatment) prime individuals to process information with either a defensive or accuracy motivation. Such information-processing motivations, in turn, are expected to influence the contribution and consumption of user-generated health content. The three-stage model was tested with data from an online sample of American adults (N = 767). A well-fitting structural equation model provided evidence for each of the hypothesized paths except for that from health-detection/treatment behavior to accuracy motivation. Individuals’ information search for health-affirming behaviors instigated a defensive motivation. Moreover, while both information-processing motivations influenced user-generated content consumption, only defensive motivation had a significant effect on user-generated content contribution. Finally, there was also one significant cross-stage path in which health-affirming behavior had a direct effect on content contribution, thus, overstepping defensive and accuracy motivations.
Keywords
The construal or cognitive representation of a health behavior can greatly influence how individuals make medical decisions (Hagger & Orbell, 2003). When people cognitively reappraise a health behavior or view a behavior from a different perspective, they alter the decisions they make about treatment and coping options (Hagger & Orbell, 2003). Moreover, individuals’ engagement in certain types of health behaviors (e.g., health-affirming and health-detection) can evoke distinct patterns of thoughts and motivations that can subsequently influence information processing (Rothman, Wlaschin, Bartels, Latimer, & Salovey, 2008). In particular, people engaged in health-affirming behaviors tend to be persuaded by positively framed messages, whereas those engaged in health-detection behaviors tend to be persuaded by negatively framed messages (Bartels, Kelly, & Rothman, 2010; Rothman et al., 2008). Demonstrating the influence of health function on information processing, research has documented the same pattern of effects when a single behavior is presented either as health-affirming or health-detection (Rivers, Salovey, Pizarro, Pizarro, & Schneider, 2005; Rothman, Martino, Bedell, Detweiler, & Salovey, 1999). For example, when a health behavior such as a Pap smear is presented as health detection (e.g., detecting cervical cancer), negatively framed messages are more persuasive (Rivers et al., 2005). In contrast, when that same behavior is presented as health affirming (e.g., preventing cervical cancer), positively framed messages are more persuasive. This highlights that the function or purpose of a health behavior can greatly influence information processing.
Although much of the existing research has centered on how the function of a behavior can differentially prime individuals to prefer positively versus negatively framed messages (Cesario, Corker, & Jelinek, 2013; Rivers et al., 2005; Rothman, Bartels, Wlaschin, & Salovey, 2006), research has not examined how people’s engagement in certain classes of health behaviors can influence their motivation to process information. To address this gap in the literature, we theorize upon the relationship between people’s health functions and two types of motivations—accuracy and defense—which are among the most widely studied motivations for information processing (Hart et al., 2009). The present study, to the best of our knowledge, is the first to investigate whether health behavior function can influence defensive and accuracy motivations for information processing.
In addition to expanding the behavior function literature to these new information-processing motivations, we aim to make two other novel contributions. First, we propose in the current study that seeking treatment for a medical condition can elicit similar construals as health-detection behavior. Inclusion of health-treatment behavior is important given that seeking information on medical and treatment options is a common health behavior. Second, research on the relationship between health behavior function and motivation has been largely limited to how people process various aspects of health messages (e.g., positively vs. negatively framed messages) and has not been extended to the Internet in general and, in particular, to the contribution, as well as consumption, of user-generated health content. This is an important extension given that online health information is an integral part of health management (Fox & Duggan, 2013) with the majority of Internet users relying on user-generated content for their health information needs (Fox, 2009). To permit these three advances, the current study theorizes upon how health behavior functions (i.e., health-affirming vs. health-detection/treatment) induce certain information-processing motivations (i.e., defensive vs. accuracy), which, in turn, influence the contribution, as well as consumption, of user-generated content on the Internet. A three-stage model is conceived and then empirically tested with data from an online sample of American adults.
Health Behavior Function
Behavior function is the notion that individuals’ engagement in certain types of health behaviors (e.g., health-affirming and health-detection) can evoke distinct patterns of thoughts and motivations that can subsequently influence information processing (Rothman et al., 2008). Health-affirming behavior pertains to how a person can maintain one’s health status by preventing the possible onset of an illness. Examples of health-affirming behaviors include sunscreen use and physical exercise. In contrast, a health-detection behavior pertains to how a person seeks information to screen for the presence of a health problem (Rothman et al., 2008). Examples of health-detection behaviors include mammography and colonoscopy. Thus, health-affirming behaviors pertain to preventive health, whereas health-detection behaviors pertain to diagnosis.
Although previous studies have differentiated between health-affirming and health-detection behaviors (Bartels et al., 2010; Cesario et al., 2013), we propose an expansion that merges health-detection with health-treatment. This merger is based on the notion that a person seeking treatment for a medical condition can elicit similar construals as health-detection behavior. Health-treatment behavior pertains to how a person manages or combats an illness. Examples of health-treatment behaviors include chemotherapy and radiation. An individual searching for information for a medical treatment lives with a certain amount of uncertainty and risk given the potential side-effects associated with medical treatment (Hunink et al., 2014) and the possibility that the prescribed treatment may not be effective. Thus, health-treatment behaviors and health-detection behaviors both carry the risk associated with their respective health behaviors. In addition, health-treatment behaviors and health-detection behaviors occur in the presence of an illness or the potential for having an illness that would affect one’s health status (World Health Organization, 2007). Perceived risk and health status are common ways of representing and viewing health (Hagger & Orbell, 2003; Leventhal, Brissette, & Leventhal, 2003). Thus, health treatment would be expected to share common ground with health detection in terms of the characteristics of perceived risk and health status.
In the message framing literature, the preference for messages framed positively versus negatively is based on the assumption that individuals will consistently construe certain behaviors as either a risky or relatively safe course of action (Bartels et al., 2010; Rothman et al., 2008). Specifically, people tend to perceive health-affirming behaviors to be low in risk because the behaviors are associated with preventing the onset of illness by maintaining health status, whereas they generally perceive health-detection behaviors as high in risk because of the uncertainty of diagnosing the presence of an illness (Rothman et al., 2008). With a basis in Prospect Theory (Kahneman & Tversky, 1979), messages that emphasize positive outcomes (i.e., gain framed) should be more persuasive for health-affirming behaviors (e.g., using sunscreen) whereas messages that emphasize negative outcomes (i.e., loss framed) tend to be more persuasive for health-detection behaviors (e.g., mammograms) because of the perceived differences in risk associated with the respective behaviors (Cesario et al., 2013; Rothman et al., 2006).
Despite the theoretical appeal of the premise that people’s engagement in different health behaviors can prime them to construe health in terms of riskiness, relevant empirical findings have been inconsistent (O’Keefe & Jensen, 2006). The main point of divergence in these findings appears to be whether behaviors are seen as health-detection or health-affirming. In studies where participants are told the type of behavior they are engaging in, negatively framed messages are more persuasive for health-detection behavior, whereas positively framed messages are more persuasive for health-affirming behaviors (Rivers et al., 2005; Rothman et al., 1999). This highlights that construals of health vary among individuals and that such construals can be influenced by external sources of information (Hagger & Orbell, 2003; Leventhal et al., 2003), such as characterizing a health behavior as detection or affirming. More importantly though, it supports the premise that engaging in certain health behaviors can prime individuals toward certain motivations (Rothman et al., 2008).
User-Generated Content in Internet Health Search
The current study considers health behavior function processes specific to the contribution and consumption of user-generated content on the Internet. The participatory architecture of Web 2.0 allows Internet users to contribute content readily in the form of videos, text, and images, which can permit better health management, participatory health care, and health promotion (Hesse et al., 2011). The collective intelligence garnered from user-generated content (Hesse et al., 2011) can enhance the credibility of evidence-based health information, making it more accessible for the layperson when making medical decisions (Metzger & Flanagin, 2011). This is of particular significance given that the Internet is rife with unsubstantiated and erroneous health information (Reavley & Form, 2011). Despite the importance of contributing content, fewer than 15% of Internet users contribute health content in general (Thackeray, Crookston, & West, 2013). Thus, although the majority of Internet users already rely on user-generated content for their health information needs (Fox, 2009), only a small minority of users contribute such content (Fox & Duggan, 2013).
In determining the factors that predict the contribution of user-generated content, much of the research differentiates between intrinsic and extrinsic motivations. In Self Determination Theory, different goals drive behavior adoptions (Ryan & Deci, 2000). This includes intrinsic motivation, which pertains to adopting a behavior because of the inherent joy and satisfaction of the action. In contrast, extrinsic motivation pertains to the external rewards gained from the action. For example, intrinsic motivational factors associated with the contribution of user-generated content include the need for social approval (Li, 2011), enjoyment (Nov, Naaman, & Ye, 2010), and reciprocity (Cho, Chen, & Chung, 2010). Pertinent extrinsic motivational factors include self-development and building one’s reputation (Nov et al., 2010). However, a first limitation of this line of research is that some motivations may be conceptualized as being both intrinsic and extrinsic. For example, self-development (i.e., motivation to enhance one’s skills through feedback and learning from others) has been conceptualized as an extrinsic motivation because it can be instrumental in a person’s garnering rewards (e.g., finding a better job) (Nov et al., 2010). However, it has also been conceptualized as an intrinsic motivation in which one’s development can bring about inherent satisfaction (Oreg & Nov, 2008). A second limitation of this line of research is that these motivational factors are not consistent predictors of the contribution of user-generated content (Nov et al., 2010; Xu & Li, 2015). A third limitation of research is that these mixed findings result from studies that are largely based on the assumption that volunteering behavior drives motivation (Cho et al., 2010; Nov et al., 2010). This assumption overlooks the fact that individuals may freely contribute content online because it satisfies their information-processing goals. For this reason, motivational factors for information processing may be more pertinent to the contribution of user-generated content given the interactive informational environment of the Internet.
The current study focuses on two such information-processing motivations—the motivation to defend one’s preexisting attitudes and beliefs (i.e., defensive motivation) and the motivation to make accurate evaluations (i.e., accuracy motivation). Importantly, these information-processing motivations are examined within the context of an Internet health search. Most of the research on user-generated content has focused on participation in online communities rather than on the actual likelihood of contributing content during an Internet search. This is an important distinction because searching for health information online has become a common use of the Internet and an integral part of health management (Fox & Duggan, 2013).
Conceptual Model
We construct a multi-stage conceptual model on content contribution and consumption (see Figure 1). The first stage in the model is behavioral function, which is viewed to be the driver of subsequent information processing and, in turn, online information use. Behavioral function has two dimensions: health-affirming behavior and health-detection/treatment behavior. In the second stage of the model, information-processing motivation takes on two forms: defensive motivation and accuracy motivation. The third stage encompasses content consumption and content contribution.

Conceptual model of content consumption and contribution.
Our model is based on the likelihood of content contribution, as well as content consumption, during an Internet search for health information. At its core, searching for health information online is a goal-driven process (Rice, McCreadie, & Chang, 2002), with individuals contributing more content when given a specific goal than when given a non-specific goal (Ling et al., 2005). Although there is an array of goals for any Internet health information search, we focus on health-affirming behavior and health-detection behavior (Rothman et al., 2008), as well as health-treatment behavior.
Effects of Behavior Function on Information-Processing Motivation
The present study, to the best of our knowledge, is the first to investigate whether health behavior function (e.g., health-affirming and health-detection/treatment) influences defensive and accuracy motivations, which are two of the most widely studied motivations for information processing (Hart et al., 2009). The Heuristic-Systematic Model proposes that defensive and accuracy motivations are but two forms of motivation that influence whether information is processed systematically, heuristically, or in both ways (Cha & Chaiken, 1999). In the multi-motive Heuristic-Systematic Model, although information processing is likely engendered by both motives, information processing is likely influenced primarily by one of the motives (Cha & Chaiken, 1999; Chaiken, Liberman, & Eagly, 1989). For defensive motivation, information processing is driven by a person’s desire to protect attitudes and beliefs that are closely tied to one’s self-concept (Cha & Chaiken, 1999). By finding information that is congruent with their preexisting attitudes and beliefs, people can satisfy their defensive motivation because information congenial to preexisting attitudes and beliefs does not induce the negative arousal state of cognitive dissonance (Cha & Chaiken, 1999; Hart et al., 2009). Moreover, the selection of congenial information allows individuals to defend their preexisting attitudes and beliefs. However, there are situations in which individuals want to find correct information irrespective of its congeniality. Such scenarios relate to accuracy motivation, which is the desire to form unbiased appraisals of available information (Chaiken et al., 1989). With accuracy motivation, as compared with defensive motivation, information processing is more evenhanded, and the selective exposure to and evaluation of negative information occurs more frequently.
A meta-analysis on selective information processing demonstrated that defensive motivation is associated with the selection of congenial information, whereas accuracy motivation is associated with the selection of uncongenial information (Hart et al., 2009). Defensive and accuracy motivations are biased with predispositions toward negative and positive information, respectively (Hart et al., 2009). Said in another way, people’s information processing with defensive motivation is characterized by their avoidance of negative information, whereas their information processing with accuracy motivation is characterized by the approach of negative information. The characterization that defensive motivation entails the avoidance of negative information whereas accuracy motivation entails the approach upon negative information is analogous to research that has documented that people prefer messages that emphasize positive (i.e., gain frame) versus negative outcomes (i.e., loss frame) contingent on whether they are utilizing a health-affirming or health-detection behavior, respectively (Rivers et al., 2005; Rothman et al., 2006). Indeed, gain and loss frames are forms of approach and avoidance, respectively (Levin, Schneider, & Gaeth, 1998). Based in this literature, we propose that health-affirming behaviors will elicit a defensive motivation to process information because of their preference for congenial information. Likewise, health-detection/treatment behaviors will elicit an accuracy motivation to process information because of their preference for uncongenial information.
Health-detection/treatment behaviors are also likely to elicit an accuracy motivation because topics with high outcome-relevant involvement (i.e., importance of the outcome) tend to make people process information in an objective manner (Albarracin, 2002). The importance of such health-detection/treatment behaviors (e.g., mammography and chemotherapy) results from their being directly related to life or death. Additional support for the link between health behavior function and information-processing motivation can be found in Regulatory Focus Theory (Higgins, 1997), which suggests that people with certain mind-sets (i.e., promotion vs. prevention orientations) prefer either accuracy or defensive motivations when processing information (Higgins, 1999). Specifically, individuals with a promotion orientation are geared toward attaining positive outcomes, whereas their counterparts with a prevention orientation, who are concerned with “errors of commission” (i.e., making mistakes), tend to gravitate toward negative outcomes (Higgins, 1997, 1999; Pham & Higgins, 2005). Research specific to online health information search has supported the proposed preferences of promotion and prevention orientations for favorable and unfavorable information (Hong, 2014). Such preferences for favorable and unfavorable information are the hallmark of defensive and accuracy motivations, respectively (Hart et al., 2009). It is also likely that engaging in health-affirming and health-detection/treatment behaviors primes a promotion and prevention orientation, respectively (Rothman et al., 2008). Based on these observations, we articulate the following hypotheses:
Effects of Information-Processing Motivation on Online Information Use
In the next step of our conceptual model (see Figure 1), we contend that in an Internet health information search, while all Internet users consume content, those with a defensive motivation to process information will be most likely to contribute content. Thus, we postulate that defensive motivation, as well as accuracy motivation, will encourage people to consume content. Content contribution pertains to content created or produced by individual Internet users and not by paid professional content providers. Contribution of user-generated content constitutes a variety of online activities, all of which result in visible content for viewing by other Internet users (Preece & Shneiderman, 2009). There are assorted such activities—rating, tagging, and posting—which require progressively more effort on the part of the contributor. For example, rating entails giving a score (e.g., a number of stars for a health care provider), whereas tagging involves labeling content. In contrast, posting entails the submission of written feedback (e.g., written comments on a news article) or uploading a video or image. The current study considers these types of postings as contributions of user-generated content. Often contributors of user-generated content progress through sequential steps from rating to tagging to posting, thus increasing their contribution of user-generated content (Preece & Shneiderman, 2009). Although most contributors of user-generated content begin by consuming content, including reading and seeing Internet content (e.g., reading textual information, viewing a video), most Internet users do not go beyond such content consumption to partake in content contribution (Ortega, Gonzalez-Barahona, & Robles, 2008).
By operationally defining user-generated content in terms of posting, our model predicts that defensive motivation is more likely than accuracy motivation to lead to the contribution of user-generated content. Defensive motivation, which entails individuals’ tendency to defend their own beliefs and attitudes (Cha & Chaiken, 1999; Chaiken et al., 1989), often drives people’s determination of whether they will—or will not—expose themselves to uncongenial content (i.e., selective exposure; Hart et al., 2009). Selective exposure, though, is but one of many defensive strategies utilized during information processing. When information processing is conceptualized as having distinct stages, selective exposure is more likely to occur in the initial two stages—preattention and focal attention (McQueen, Vernon, & Swank, 2013). The preattention stage constitutes a person’s subconscious evaluation of information, whereas the focal attention stage encompasses a person’s conscious evaluation of information. In either of these two stages of information processing, individuals can defend their beliefs and attitudes by either avoiding content entirely or avoiding uncongenial content. People utilize more complicated defensive strategies in the latter two stages—comprehension and elaboration. For example, in the comprehension stage, suppression is a defensive strategy by which individuals deny that a negative implication could affect them. In addition, in the elaboration stage—which is most relevant to the current study—people can use counter-arguing as a defensive strategy. In our model, defensive motivation entails people’s posting messages as a form of counter-arguing by which they can protect their preexisting beliefs and attitudes.
The basis for our relevant hypotheses also comes from research on ego-defensive motivation, which shares conceptual ground with defensive motivation (McQueen et al., 2013). In particular, ego-defensive motivation, which entails protecting one’s own self-image, is associated with a person’s contributing user-generated content (Daugherty, Eastin, & Bright, 2008). Individuals with high ego-defensive motivation can protect their self-image by posting messages or related user-generated content. Thus, posting content is one way to counter-argue or refute an argument, with these actions common among individuals with elevated defensive motivation.
Based on these observations, we articulate the following hypotheses:
Method
The hypotheses were tested with data from an online survey of American adults between April and May 2009. 1 The survey had a total of 992 respondents, 2 with a completion rate of 91.09%. Because of this study’s focus on health information search, respondents who reported never having read or looked for health or medical information online in the last 12 months (n = 225) were dropped from the dataset, resulting in a final sample of 767 respondents, which is used for all analyses in this study. Institutional Review Board approval for this study was acquired at the Tulane University Health Sciences Center.
Measurement
In terms of exogenous variables, analyses were controlled for respondent age (M = 46.22, SD = 14.74, range = 19-66), ethnicity (83.18% White), education level (M = 14.16, SD = 2.22, range = 0-19), household income level (M = 2.56, SD = 1.46, range = 1-7), gender (43.55% male), Internet use frequency (i.e., hours in a typical week, not counting work; M = 17.67, SD = 9.34, range = 0.5-31), and years using the Internet (M = 5.37, SD = 1.43, range = 0.5-6). In addition, pertinence to self of the sought health information (i.e., searching for information for one’s self rather than for someone else) was measured (yes = 66.88%). The final exogenous variable, perceived risk (M = 3.40, SD = 1.21, range = 1-5) was measured with a 5-point scale from strongly disagree to strongly agree that assessed the perceived risk of the health. Given that severity is a dimension of perceived risk (Brewer et al., 2007), the following statement was used: “This health or medical topic was serious in nature.” This perceived risk measure, along with an additional measure on health status, was also used to test the validity of the construal of health-affirming and health-detection/treatment. Health status (M = 3.20, SD = 1.01, range = 1-5) was measured on a 5-point scale from poor (1) to excellent (5).
The other variables were endogenous. Respondents were asked to answer the following questions pertinent to “the most important topic from your searching for health or medical information on the Internet in the past 12 months.” For behavior function (Rothman et al., 2008), respondents were asked whether the health or medical information was primarily related to “prevention” (22.82%), “diagnosis” (46.67%), or “treatment” (30.51%). Prevention is consistent with health-affirming behavior, whereas diagnosis is consistent with health-detection behavior. Given that treatment shares common ground with detection in terms of perceived risk and health status, it was combined with detection to create the measure of health-detection/treatment.
The measurement of content consumption (i.e., reading or viewing) and content contribution (i.e., posting; Preece & Shneiderman, 2009) was specific to “the most important topic from your searching for health or medical information on the Internet in the past 12 months.” The following types of online content were assessed: (1) health websites such as cdc.gov, webmd.com, or mayoclinic.com; (2) online blogs or message boards, including those on health websites or portals; (3) social networking websites such as Facebook, MySpace, or Second Life; (4) video/picture websites such as YouTube or Flickr; (5) online support groups such as Yahoo Groups or Google Groups; and (6) news websites such as CNN.com or NYTIMES.com. The time frame for related consumption or contribution was the last 12 months. Responses were on a 5-point scale from “never” to “very often.” Indexes were created for content consumption (based in content Types 1-6 above [α = .89]) and for content contribution (based in content Types 2-6 above [α = .94]). The mean for content consumption was 1.93 (SD = 0.87, range = 0-5) and for content contribution was 1.43 (SD = 0.83, range = 0-6).
With bases in previous research (Chen, Duckworth, & Chaiken, 1999; Neuwirth, Frederick, & Mayo, 2002), accuracy and defensive motivations were measured with responses on a 5-point scale from strongly disagree to strongly agree. Accuracy motivation (M = 3.40, SD = 0.72, range = 1-5) was assessed with the following four items: (1) It was important to find health or medical information on the Internet that corrected misconceptions that I had, (2) I sought health or medical information on the Internet to see both sides of an issue, (3) Health or medical information on the Internet helped me determine what was true and what was not true, and (4) I found myself trying to decide whether health or medical information on the Internet was accurate (α = .82). Defensive motivation (M = 2.85, SD = 0.82, range = 1-5) had the following four items: (1) When looking for the health or medical information on the Internet, I usually avoided information that contradicted my current viewpoint; (2) I looked for health or medical information on the Internet that supported my current opinions; (3) I found myself preferring health or medical information on the Internet that was consistent with what I already thought; and (4) I primarily looked for health or medical information on the Internet that was in line with my values (α = .70).
Statistical Analysis
Structural equation modeling (SEM) was conducted with Stata 14, using the maximum likelihood method (ML) of estimation with covariance structure analysis. To test the hypotheses, the model had three main stages of endogenous variables: (1) health-affirming versus health-detection/treatment, (2) defensive motivation and accuracy motivation, and (3) content contribution and content consumption. Paths were positioned from the Stage 1 variable to Stage 2 variables and from the Stage 2 variables to Stage 3 variables. In addition, covariance paths were inserted between same-stage endogenous variables (i.e., between defensive motivation and accuracy motivation and between content contribution and content consumption). Modification indices were calculated to determine whether any cross-stage paths should be added to the SEM. In addition, exogenous variables were entered as control variables. Overall model fit was assessed with the comparative fit index (CFI), the root mean square error approximation (RMSEA), and the standardized root mean square residual (SRMR). A CFI value of .95 or higher, an RMSEA value of close to or less than .06, and an SRMR value of close to or less than .08 are indicative of good model fit (Hu & Bentler, 1999). In addition, χ2 statistics are reported.
Results
Given the size of our sample (N = 767), two initial z tests were run to test the validity of our measure of health-affirming versus health-detection/treatment behaviors (Shafer & Zhang, 2012). Health status was significantly better for health-affirming respondents (M = 3.37, SD = 1.00) than health-detection/treatment respondents (M = 3.16, SD = 1.01), z = 2.44, p = .015. Perceived risk was significantly lower for health-affirming respondents (M = 3.12, SD = 1.10) than health-detection/treatment respondents (M = 3.48, SD = 1.23), z = 4.16, p < .001. These results are consistent with our prior conceptualization of health-affirming and health-detection/treatment according to perceived risk and health status.
In SEM, modification indices suggested the addition of a cross-stage path from health-affirming versus health-detection/treatment behavior directly to content contribution. Although different from the parsimonious theoretical model, this path is theoretically justifiable and, thus, was added to the model. The tested SEM had good model fit, CFI = .998; RMSEA = .057; SRMR = .006; χ2(1) = 3.49, p = .062. The Bentler–Raykov squared multiple correlation coefficients were as follows: health-affirming versus health-detection/treatment behavior, 6.77%; defensive motivation, 9.78%; accuracy motivation, 9.46%; content consumption, 26.02%; and content contribution, 27.15%. There were significant covariance paths between defensive motivation and accuracy motivation (ϕ = .48, p < .001) and between content consumption and content contribution (ϕ = .71, p < .001). The direct effects of exogenous variables and endogenous variables are presented in Table 1 and Figure 2, respectively.
Direct Effects of Exogenous Variables on Endogenous Variables in SEM (N = 767).
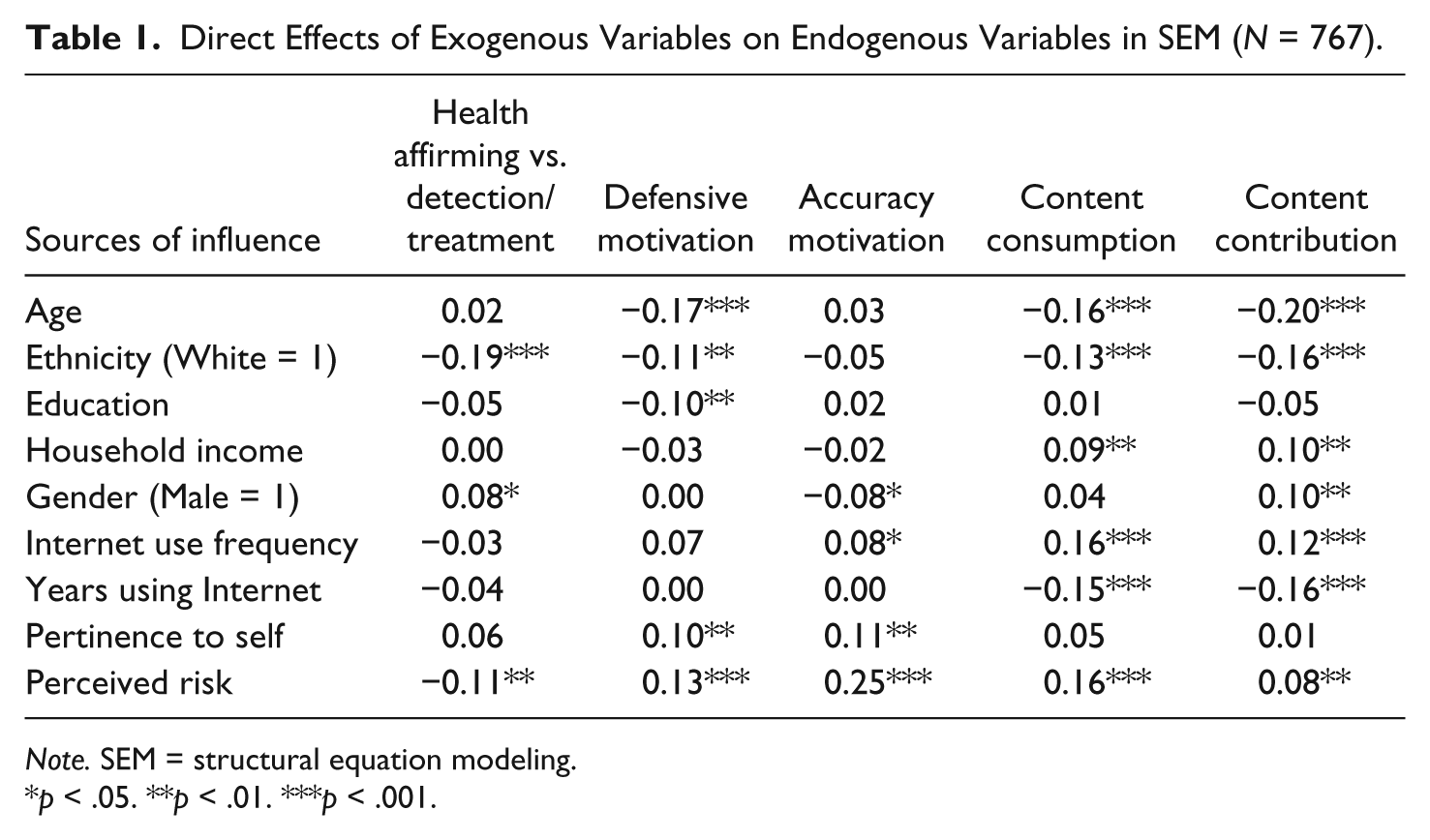
Note. SEM = structural equation modeling.
p < .05. **p < .01. ***p < .001.

SEM predicting content contribution and consumption.
Hypothesis 1a posited that individuals with health-affirming behavior for Internet search have higher defensive motivation for information processing than their counterparts with health-detection/treatment behavior. Support for this hypothesis comes from the significant path from health-affirming behavior to defensive motivation (β = .07).
Hypothesis 1b held that individuals with health-detection/treatment behavior for Internet search have higher accuracy motivation for information processing than their counterparts with health-affirming behavior. The path here was non-significant, leaving Hypothesis 1b unsupported.
Hypothesis 2a predicted that, as compared with accuracy motivation, defensive motivation has more positive effects on content contribution. The path from defensive motivation to content contribution was significant (β = .28), whereas the path from accuracy motivation to content contribution was non-significant. These findings provide general support for Hypothesis 2a. To compare these two effects more closely, we conducted an ad hoc test of coefficient equality. This calculation entailed the standardized coefficients and standard errors for both paths (Clogg, Petkova, & Haritou, 1995; Paternoster, Brame, Mazerolle, & Piquero, 1998), resulting in a z score of 6.45 (p < .001). This result indicates that the standardized effect of defensive motivation was significantly greater—and more positive—than that of accuracy motivation, which provides additional support for Hypothesis 2a.
Hypothesis 2b posited that both defensive and accuracy motivations predict content consumption. This hypothesis is supported by the significant paths from defensive motivation (β = .18) and accuracy motivation (β = .18) to content contribution.
Discussion
A hallmark of behavior function studies is that individuals’ engagement in certain types of health behaviors (e.g., health-affirming and health-detection/treatment) can evoke distinct patterns of thoughts and motivations. The current study, to the best of our knowledge, is the first to extend the literature on behavior function by demonstrating that engaging in certain behaviors can lead to the information-processing motives of defense and accuracy. Connecting behavior function to these information-processing motives is important given that defensive and accuracy motivations are perhaps the two most widely used approaches to analyzing attitude-relevant information (Hart et al., 2009). In particular, this study suggests that research on selective exposure should consider how engaging in behaviors can strengthen defensive motivation. This approach is divergent from the current literature, which focuses primarily on how an individual’s personality or characteristics can strengthen defensive motivation. For example, when a behavior is consistent with enduring values, people are more likely to process information defensively (Hart et al., 2009). Thus, the current study suggests that the very act of searching for health-affirming information can strengthen defensive motivation. Although we tested only health-related behaviors, future research should consider the conceptualization and subsequent empirical testing of behaviors in other domains (e.g., politics).
In addition, by demonstrating that information-processing motives (i.e., the desire to process information defensively) predict whether users contribute content on the Internet, this study offers an alternative theoretical understanding beyond the self-determination approach that has dominated the literature (Nov et al., 2010; Oreg & Nov, 2008). In this manner, much of the preexisting literature focused on people’s innate growth tendencies and needs (e.g., need for social approval, reciprocity) in predicting why they freely contribute content on the Internet (Nov et al., 2010). In contrast, the findings of the current study suggest that people’s information-processing needs and, in particular, their inclination to process information defensively can help explain why they freely give their time to post messages on the Internet. This documented process especially makes sense given that the Internet is an immersive and interactive medium that requires substantial cognitive effort to search for health information.
In terms of the online context, the current findings also suggest that Internet health information seekers, whether using defensive or accuracy motivation, consume user-generated content, which is in line with the increasing demand for such health content (Fox & Duggan, 2013). However, it is only individuals with defensive motivation who contribute health content. This meaningful distinction leads one to question the quality and bias of user-generated online health content given that its creation is driven by a person’s need to preserve one’s own viewpoints. That is, although there is a need for unbiased online health content, the more objective Internet health information seekers are less likely to contribute to user-generated content than their less objective counterparts. Although our study was limited to whether health information seekers posted user-generated content, future research should assess the nature of the posted content to determine whether, indeed, the content appears to be biased according to one’s defensive information-processing motivation. Future research may also consider, to what degree, information-processing motives compete with intrinsic and extrinsic motivations to predict contributing user-generated content. Other related potential areas for future inquiry include examining whether impression motivation can also influence information consumption and contribution given that the Heuristic-Systematic Model is a multi-motive model (Cha & Chaiken, 1999; Chaiken et al., 1989). Moreover, per the Heuristic-Systematic Model, future research may examine whether the consumption and contribution of online content are done systematically, heuristically, or in both ways.
The current study also extends the literature on behavior function by considering that health-treatment is conceptually similar to health-detection. The literature is limited to the distinction between health-affirming and health-detection behaviors. By including a commonly occurring behavior such as seeking information for health-treatment, the current study provides a fuller representation of the types of behaviors that may influence information-processing motivations. We differentiated health-affirming and health-detection/treatment behaviors by perceived risk and health status. In particular, while perceived risk is a multi-dimensional construct that includes perceived likelihood, perceived susceptibility, and perceived severity (Brewer et al., 2007), we only assessed the latter dimension. Future studies should ascertain if other dimensions of perceived risk differ between health behavior functions—and if these dimensions have subsequent impact on motivations for information processing.
It is also important to consider why our three-stage model did not function as expected for health-detection/treatment behavior. Research has documented that thoughts and motivations associated with health-detection/treatment behaviors are analogous to a prevention orientation (Rothman et al., 2008). Although we argued such health-detection/treatment behaviors would encourage accuracy motivation, a major premise of this argument was that a person’s thought of or engagement in detection/treatment behavior would prime a prevention orientation. In our study, however, it appears that the act of searching for health information for a detection/treatment topic was not enough to prime the prevention orientation, nor subsequent accuracy motivation. It could be that only high-risk behaviors prime prevention orientation. For example, actually getting a mammogram may instigate more thoughts and motivations related to the prevention orientation than just thinking about getting a mammogram and searching the Internet for pertinent health information. Although the literature does not specify in this manner the level of behavioral engagement necessary to prime a regulatory orientation, such benchmarks should be explored in future research.
Also of interest is the cross-stage path from health affirming to content contribution, which makes the final model less parsimonious than initially theorized. To be clear, whereas it seems that defensive motivation completely mediates the effect of health behavioral function on content consumption, it only partially mediates the effect of health behavioral function on content contribution. In the latter regard, there is also a direct effect of health behavioral function on content consumption. Thus, while motivation is essential to the development of content consumption, it is not in the case of content contribution. We posit three potential rationales for this pattern of effects. First, it could be that the representation of illness and how people construe health can cause them to cognitively reappraise illness or change the way they view their health condition, which, in turn, can greatly influence the types of coping strategies that a person adopts (Hagger & Orbell, 2003). Second, the partial mediation path could entail how not all media use stems directly from motivation, with, instead, some types of media use being incidental. However, when considered more closely, this rationale seems counter to the current findings. After all, it would seem that content consumption would be more likely to be incidental than content contribution. Third, it could be that other dimensions of motivation could be also functioning here. For example, the Uses and Gratifications literature has identified other motivational dimensions that can explain media use, including surveillance, which entails using the mass media to obtain information (Payne, Severn, & Dozier, 1988). Empirical research has found that a related surveillance motivation played the core role in a multi-stage model, predicting increases in health-related Internet use and health literacy, as well as a decrease in perceived health information overload (Jiang & Beaudoin, 2016). Thus, it could be that all of the effects of behavioral function on content contribution and consumption are mediated by motivation, but our two measures do not encompass all such types of motivation. In this manner, other dimensions of motivation (e.g., surveillance) may mediate the effect of health behavioral function on content consumption—or, when controlling for such other dimensions of motivation, defensive motivation may completely mediate the effect of health behavioral function on content consumption.
In closing, it is important to note five limitations of this study. First, the current study’s reliance on cross-sectional survey data permits testing of association, but not causation. That said, the tested three-stage model (i.e., from behavioral function to information-processing motivation to online information use) is intuitive and theoretically justified. Second, our study focused solely on content posting, including that of videos, text, and images. It is encouraged that future research investigate whether the tested processes vary according to contribution typologies for user-generated content such as rating versus tagging versus posting. Because rating and tagging are more common forms of contributing user-generated content (Preece & Shneiderman, 2009), it is possible that different effects may emerge in a model with these forms of content contribution. Third, while our measures of defensive and accuracy motivations have a basis in the literature, some of the questionnaire items are actually retrospective measures of defensive motivation rather than measures of the underlying motivation. Fourth, given that information seeking is often described as a process with distinct stages that are characterized by different function, it is possible that certain stages are more prone to elicit the contribution of user-generated content while other stages are more fitting for the consumption of user-generated content. Our study did not differentiate between stages of information search. Experimental studies may be particularly effective in ascertaining such a distinction. Fifth, our study centered on whether health information seekers posted user-generated content, not on the actual nature of the user postings. For example, it is unknown whether user postings were congenial to their preexisting attitudes and beliefs as would be expected per defensive information-processing motivation. An additional caveat should be noted. Given perpetual changes in the Internet and new media technologies, it is important that scholars continue research in this area, including retesting the current study’s focal processes with data from different time periods.
Footnotes
Acknowledgements
The authors are grateful for the constructive feedback provided by Dr. Michael Roloff and the two reviewers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.