
Abstract
Sexual assault nurse examiner (SANE) programs can be a vital resource to victims and the legal community. This study examined how police may use SANE services during the investigation phase and how this involvement may affect whether a case is forwarded by police to prosecutors. Police reports (N = 343) of adult sexual assault cases in three midwestern law enforcement agencies were content-analyzed to capture the nature of SANE involvement in the investigation, the specific investigatory steps taken in each case, and the referral outcome. When the victim had a medical forensic exam, police collected more kinds of other evidence to support the case, which was associated with increased likelihood of case referral for prosecution. When SANEs conducted a suspect exam (i.e., a forensic examination of the suspect’s body), police were more likely to collect other kinds of evidence and more likely to interview the suspect, both of which were associated with increased likelihood of case referral.
Keywords
Most sexual assault victims do not report to law enforcement (Bureau of Justice Statistics, 2007), and even when they do contact the police, on average, only 18% of reported sexual assaults are prosecuted (Campbell, 2008; Chen & Ullman, 2010; Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007). To address this problem of underreporting and underprosecution, communities throughout the United States have implemented multidisciplinary response interventions to improve postassault care for victims and increase prosecution rates (Campbell, 2008). One such model is sexual assault nurse examiner (SANE) programs, whereby specially trained nurses (rather than hospital emergency department physicians) provide comprehensive psychological, medical, and forensic services for sexual assault victims (Campbell, Patterson, & Lichty, 2005; Ledray, 1999). 1 Sexual assault forensic nurses offer crisis intervention and emotional support, health care (e.g., sexually transmitted infection [STI] screening and prophylaxis, pregnancy testing, and emergency contraception), injury detection and treatment, and state-of-the-art forensic medical evidence collection (Department of Justice [DOJ], 2004; Ledray, 1999). In addition, SANEs provide case consultation to police and prosecutors and are sometimes asked to testify as expert witnesses should a case go to trial (DOJ, 2004). SANE programs can be a vital resource to both sexual assault victims and the legal community, which has raised interest in whether SANE programs can have a positive impact on prosecution rates in their communities.
Numerous case studies suggest that SANEs are helpful to police and prosecutors (see Campbell, Patterson, & Lichty [2005], for a review), but only a handful of studies have rigorously tested the hypothesis that SANE programs contribute to higher prosecution rates (Campbell, Patterson, & Bybee, in press; Crandall & Helitzer, 2003; Nugent-Borakove et al., 2006). These projects have documented increased prosecution rates after the implementation of SANE programs, but the mechanisms by which these interventions can facilitate system change remains unclear. The underlying questions of how and why SANE programs can affect prosecution outcomes is important to understand, because it is possible communities could implement these interventions in the hope of achieving more convictions, but such effects may not materialize if critical key ingredients are not incorporated. Therefore, the purpose of the current study was to begin exploration into this issue by examining how SANEs affect the earliest stages of the legal process, namely, the law enforcement investigation. Our goal was to understand how police may use SANE services during an investigation and how this involvement may affect whether a case is forwarded by police to prosecutors for further legal action. First, we will review the extant literature on SANE programs and their role in the prosecution of sexual assaults.
Impact of SANE Programs on the Criminal Justice System
A victim’s body is a crime scene, and because of the invasive nature of sexual assault, a medical professional, rather than a crime scene technician, is needed to collect the evidence. Thus, when victims seek professional help after a sexual assault, they are most likely to be directed to the medical system, specifically, hospital emergency departments (EDs; Resnick et al., 2000). There are numerous problems with an ED-based approach to postassault health care and forensic collection (see Campbell, 2008, and Martin, 2005, for reviews). Many ED physicians are reluctant to perform the rape exam (Martin, 2005), and most lack training specifically in forensic evidence collection procedures (Littel, 2001). As a result, many rape kits collected by ED doctors are done incorrectly and/or incompletely (Littel, 2001; Sievers, Murphy, & Miller, 2003). In addition to problems with evidence quality, many victims are retraumatized by the ED exams, which often leave them feeling more depressed, anxious, blamed, and reluctant to seek further help (Campbell, 2008). These negative experiences have the unintended effect of decreasing victims’ willingness to participate in law enforcement investigations and legal prosecution (Campbell & Raja, 2005).
To address these problems and better attend to victims’ forensic-legal issues as well as their psychological and medical needs, SANE programs were created in the 1970s by the nursing profession, in collaboration with rape crisis centers and victim advocacy organizations (DOJ, 2004; Ledray, 1999). They grew in rapid numbers during the 1990s, now numbering more than 500 programs in the United States (International Association of Forensic Nurses [IAFN], 2011). SANE programs are staffed by registered nurses or nurse practitioners who have completed a minimum of 40 hr of classroom training and 40 to 96 hr of clinical training, which includes instruction in evidence collection techniques, use of specialized equipment (e.g., colposcope), injury detection methods (e.g., Toluidine blue dye), pregnancy and STI screening and treatment, chain-of-evidence requirements, expert testimony, and sexual assault trauma response (DOJ, 2004, 2006; Ledray, 1999).
SANEs provide law enforcement personnel and prosecutors with valuable resources, including but not limited to high-quality medical forensic evidence, so it is reasonable to ask whether these interventions have a positive impact on prosecution rates. Several case studies suggest that SANE programs increase arrest and prosecution rates (see Campbell, Patterson, et al., 2005 for a review). However, these evaluations did not include comparison groups or other methodological controls, as is common in case study research (Stake, 1995), so it is difficult to know whether the reported rates were significantly higher and attributable to the efforts of the SANE program.
To date, only two studies have used rigorous, pre- and postintervention quasiexperimental designs to evaluate whether SANE programs can contribute to increased prosecution rates. 2 Crandall and Helitzer (2003) compared prosecution rates in a New Mexico jurisdiction 2 years before to 3 years after the implementation of a SANE program. Their results indicated that significantly more victims treated in the SANE program reported to the police than before the SANE program was launched in this community, and significantly more victims had evidence collection kits taken. Police filed more charges post-SANE as compared to pre-SANE. The conviction rate for charged SANE cases was also significantly higher, resulting in longer average sentences. A study by Campbell et al. (in press) compared case outcomes 5 years before to 7 years after the implementation of a SANE program in a midwestern community. They also found that cases were significantly more likely to progress through the criminal justice system, resulting in more guilty pleas and trial convictions. Drawing on archival and supplemental qualitative data, this study also carefully examined threats to internal validity and concluded that the significant increase could be reasonably attributed to the work of the SANE program.
Effect of SANE Programs on Sexual Assault Prosecution Rates
Why the implementation of a SANE program could contribute to increased prosecution rates has not been studied, but several mediating mechanisms have been suggested in the literature. First, although there has been considerable focus on the value of SANE’s court testimony (Campbell et al., 2007; Canaff, 2009; Ledray & Barry, 1998), their earlier interactions with law enforcement during the investigation may be particularly impactful (Campbell, Patterson, & Fehler-Cabral, 2010). If medical forensic exam findings are communicated to law enforcement clearly and in a timely way, there is opportunity for police to act on that information to strengthen the investigation itself. For example, Stone, Henson, and McLaren’s (2006) survey of law enforcement personnel in 100 randomly selected agencies found that 85% felt that the statements victims make to SANEs are useful in identifying and apprehending suspects, 93% indicated that the use of SANEs increases the likelihood that police will be able to create a successful case for prosecution, and 82% noted that SANEs are accessible to law enforcement after the exam and are willing to explain or interpret their findings. Similarly, in a qualitative study of a midwestern SANE program, detectives noted that the SANE’s medical documentation of injuries, the medical forensic exam findings, and case consultation directly affected their investigative activities, such as directing new leads to pursue, collecting supplemental evidence, and obtaining search warrants for a medical forensic examination of the suspect’s body (termed a “suspect exam”) to look for corroborating evidence (Campbell et al., 2010).
Second, SANE programs’ focus on patient care may have a positive effect on the emotional well-being of victims, which may make it more likely that victims are willing and able to engage in the lengthy process of the investigation and prosecution (Campbell, Greeson, & Patterson, 2011). Several studies have found that sexual assault victims characterize the nature of the care they receive at SANE programs as supportive, caring, and empowering (Campbell, Patterson, Adams, Diegel, & Coats; 2008; DuMont, White, & McGregor, 2009; Ericksen et al., 2002). Taking this issue further, Campbell and colleagues interviewed forensic nurses and their patients and found that high-quality patient care, which emphasized victims’ choice and empowerment, had a supportive indirect effect on victims’ participation in the legal system (Campbell et al., 2011; Patterson & Campbell, 2010). Victims noted that they did not feel pressured by the SANE program to report and pursue prosecution but did feel that the program’s nurses and advocates provided them with useful information to make informed decisions and that resources were available to help them should they decide to pursue prosecution (Fehler-Cabral, Campbell, & Patterson, in press). Other research suggests that SANE programs may directly contribute to increased victim participation with law enforcement. Stone et al. (2006) found that law enforcement personnel perceived higher victim cooperation when SANEs are involved in a case. In addition, key informant interviews in Crandall and Helitzer’s (2003) study suggested that SANEs are instrumental in helping police establish rapport with victims more effectively, thereby increasing quality of witness statements.
Finally, several case studies suggest that the implementation of SANE programs fosters interagency collaboration and cooperation (Hatmaker, Pinholster, & Saye, 2002; Hutson, 2002; Selig, 2000; Smith, Homseth, Macgregor, & Letourneau, 1998). Research with domestic violence coordinating councils has found that positive working relationships are an important mechanism by which these kinds of interventions affect case outcomes (Allen, 2005; Allen et al., 2010). In the context of SANE programs specifically, key informant interviews in Crandall and Helitzer’s (2003) study revealed that before the SANE program was implemented, community services were disjointed and fractionalized, but after, care for victims was centralized and working relationships between medical and legal professionals had improved substantially. How these improved relationships come about is not well understood, but it has been suggested that interagency case review meetings and/or cross-disciplinary training are key mechanisms for changing investigative and prosecution practices (Allen, 2005; Allen et al., 2010; Lonsway, Welch, & Fitzgerald, 2001; Lord & Rassel, 2000).
The Current Study
The current literature on SANE programs highlights several possible mechanisms by which these interventions can contribute to successful legal outcomes, but the relationship between these factors and case outcomes has not been empirically tested. Because several studies have suggested that the law enforcement investigation is a particularly critical juncture in which SANE services may be useful and influential, we decided to focus in depth on this stage as a first step in the pathway to prosecution. The purpose of this study was to examine how SANE services were used by police and detectives in the investigation process and whether SANE involvement in a case predicted law enforcement decisions to forward cases for prosecution. Consistent with other studies on police practices in sexual assault cases (Jordan, 2004; Sherley, 2005), we examined police reports as official, written records that document law enforcement’s investigative activities in a case. We content-analyzed police reports written before and after the implementation of the SANE program to determine whether there have been substantive changes in how sexual assault cases were investigated since the emergence of the SANE program. Furthermore, within the post-SANE era, we explored what specific aspects of SANE case involvement (e.g., victim exams, suspect exams, case consultation, training) affected law enforcement actions (e.g., suspect interviews, witness interviews, collection of additional evidence). Specifically, our aim was to test whether the relationship between SANE involvement in a case and referral of a case to the prosecutors was mediated by law enforcement investigatory efforts. It was hypothesized that SANE involvement would be associated with (a) increased police investigation effort and (b) decreased victim withdrawal, (c) which in turn would be associated with increased case referral to the prosecutors.
Method
Research Setting
The setting for this study was a geographically diverse county in the Midwest with a population of 829,453 that included urban, suburban, and rural areas. In 1997, a multidisciplinary community task force was formed to address the problems of low reporting and conviction rates for sexual assault cases, inadequate forensic evidence collection, and victim-blaming treatment by hospital emergency department personnel. The task force determined that a SANE program was needed in the community, and in September 1999, the program opened with established agreements from all hospitals and law enforcement agencies in the county to transfer sexual assault victims to the program for evidence collection. In the event a survivor needed urgent medical care, the SANE program nurses would be permitted to conduct the exams on-site in every county hospital. The programs’ clientele is predominately female (97%) and White (68%) (25% African American, 1% Latina, and 6% Other), which is consistent with the racial-ethnic composition of this county. This program is consistent with emerging national-level data on SANE program characteristics with respect to size, staffing, number of patients served, services provided, and training and supervision of nurses (Campbell, Townsend, et al., 2005; Logan, Cole, & Capillo, 2007).
Sample
Adult sexual assault police reports were requested under the Freedom of Information Act from the three law enforcement agencies in the focal county that had the highest adult sexual assault case loads. All cases that fit the following eligibility criteria were requested: (a) The reported crime was classified as a criminal sexual conduct offense (the focal state’s term for sexual assault crimes), (b) the victim was at least 18 years old, and (c) the crime occurred between January 1994 and December 2005, which spans the 5 years prior to the implementation of the SANE program (January 1994 to August 1999) to 7 years after SANE (September 1999 to December 2005). Unfortunately, even within the highly organized records units of these departments, police reports from 1994 were completely unavailable, and only 52 were available from 1995 through August 1999 (the pre-SANE era). As a result, our capacity to test for changes in police reports before and after the implementation of the SANE program has limited statistical power (see below), but it was still possible to examine what specific aspects of SANE involvement (in the post-SANE era) affected law enforcement actions.
A total of 393 reports were provided by the three departments, and these records were reviewed by two research assistants to verify whether all cases fit the study criteria. Of the original cases, 41 were excluded: 31 cases were dropped because the survivor was under 18 years old (sampling error), 8 cases because the police report was largely incomplete, and 2 cases because the reported crime was not a sexual assault (sampling error; 92% sampling reliability). The research assistants then conducted a quantitative content analysis on the remaining 352 cases. As will be noted below, 9 additional cases were dropped during the analysis because of missing data.
Procedures
To develop the content analysis coding framework, a random subsample of 20 reports was reviewed by the principal investigator (PI), co-investigators, and research assistants. Each independently developed a list of broad thematic codes that should be captured for each report on the basis of recommended investigative practices for sexual assault cases (e.g., Hazelwood & Burgess, 2008; Savino & Turvey, 2004). The team met to compare ideas, develop a final list, and write operational definitions for each of the broad thematic codes. Ten thematic areas were selected: (a) report characteristics (e.g., days between assault and initial report, length of lead detective’s report), (b) victim characteristics (e.g., age, race-ethnicity), (c) suspect characteristics (e.g., age, race-ethnicity, relationship to victim), (d) assault characteristics (e.g., type of penetration or fondling), (e) medical forensic findings (e.g., DNA, injury documentation), (f) law enforcement interactions with victim and suspect (e.g., interviews conducted, attempted to resolve inconsistencies), (g) other law enforcement investigation actions and effort (e.g., collection of other evidence, interviewing witnesses), (h) consultation with SANE and/or other professionals about the case, (i) victim withdrawal from the investigation process (e.g., whether victim withdrew participation or otherwise decided not to pursue the case), and (j) law enforcement decision to refer case (e.g., no referral or referral to prosecutor).
After these broad thematic codes were established, the PI worked with the research assistants to develop multiple subcodes within each theme to capture specific information (more than 200 variables were created). A detailed codebook was developed that included operational definitions for each subcode, along with examples of what would and would not be considered an appropriate application or exemplar of the code. The 20 cases randomly selected for use in the development of the coding framework were independently coded by two research assistants. Initial interrater reliability was fair, which prompted more team discussion of inconsistencies and revisions to the codebook. These 20 cases, plus 20 new cases, were recoded, which finally yielded acceptable interrater reliability (percentage agreement >90%, kappa >.80; Pett, 1997). Overall, 30% of the total reports were double-coded to monitor interrater agreement, which remained high (percentage agreement >90%, kappa >.80).
In addition to coding the thematic content of the police reports, we recorded the badge number for the officer or detective who wrote the report to verify whether that individual had participated in any of the law enforcement sexual assault trainings conducted by the focal SANE program (cross-checked against the official training attendance rosters). After this information was obtained, the identifying badge number was removed from the database, and only the variables reflecting training participation (yes or no; if yes, the number of times trained) remained.
Measures
The dependent variable in these analyses was whether the police had referred the case to the prosecutor (i.e., referral; 154 cases, 54%). For the independent variables, our indicators of SANE involvement included (a) whether the sexual assault occurred after implementation of the SANE program (300 cases, 85%), (b) whether there had been a forensic examination of the victim (168 cases, 49%), (c) whether SANE conducted a suspect exam (29 cases, 8%), (d) whether law enforcement had consulted with SANE about the case (60 cases, 14%), and (e) whether any member of the police team investigating the case had participated in sexual assault training conducted by the focal SANE program (78 cases, 22%).
For the mediating variables, the indicators of law enforcement effort included (a) whether evidence in addition to the medical forensic exam had been collected (e.g., evidence found at crime scene; 186 cases, 53%), (b) whether one or more suspects had been interviewed (187 cases, 53%), (c) whether witnesses had been interviewed (157 cases, 45%), (d) whether inconsistencies in the victim or witness statements had been resolved (94 cases, 27%), (e) whether the suspect had been offered a polygraph (63 cases, 18%), (f) whether other professionals had been consulted in the course of the investigation (191 cases, 54%), and (g) the number of pages the police report comprised (M = 5.32, SD = 1.66, range = 1 to 8). In addition to these indicators of law enforcement effort, whether the victim had withdrawn from the law enforcement process (126 cases, 36%) was also examined as a mediator. All analyses controlled for whether the rape kit results supported the victim’s account of the assault (present in 26 cases, 7%). It is important to note that it was unusual for the police reports to have documentation regarding the rape kit findings, which is likely why percentage is so low for this variable.
Analyses
Data analysis focused on identifying law enforcement investigatory efforts that were associated with SANE involvement in a case. Of the 352 cases that met the study’s sampling criteria, 9 additional cases were dropped because of missing data on key variables, yielding a final analysis sample size of 343. These 343 cases were investigated by law enforcement teams led by 152 police officers. To account for possible similarities in law enforcement effort across cases handled by the same lead officer, cases (Level 1) were nested within lead officer (Level 2) for analysis; the number of cases handled by each lead officer ranged from 1 to 19 (M = 2.98, SD = 3.37). Each officer was associated with one of three law enforcement agencies, which were incorporated as two dummy-coded variables at Level 2. Cases spanned 11 years: 4 years (1995 through 1998) prior to the implementation of SANE and 7 years (1999 through 2005) following the initiation of the SANE program. Because cases handled near the same time were likely to have been influenced by shared historical circumstances other than the SANE program, the month of each assault was incorporated in the analyses at Level 1. Graphical inspection and preliminary analysis showed no identifiable linear or nonlinear trend over time in rates of referral for prosecution.
To reflect the nesting of individual cases within lead officer, multilevel modeling was used to analyze the effect of SANE involvement on law enforcement effort, victim withdrawal, and referral for prosecution. Multilevel random intercept models allowed for between-officer variability in the frequency of various investigation activities and produced standard errors appropriate for testing the influence of group-level variables, reflecting the lack of independence of their effects on individual cases (Raudenbush & Bryk, 2002). Other than law enforcement agency, covariates were modeled at Level 1 (i.e., as varying across individual cases); this allowed for within-officer comparisons of cases handled by the same lead officer before and after he or she received SANE training. This approach controlled for individual officers’ case-handling styles and optimized precision through within-person comparison.
Because all but one of the variables was dichotomous, most analyses used multilevel logistic regression (i.e., the hierarchical generalized linear model with a logit link function). The remaining effort variable, number of pages in the police report, was relatively normal in distribution and was analyzed using linear multilevel regression. All analyses used restricted maximum likelihood and were conducted using HLM 6 software (Raudenbush, Bryk, Cheong, & Congdon, 2004). To reduce the influence of non-normal distributions, robust standard errors were used to compute confidence intervals; however, results were virtually identical using robust or nonrobust estimation. To assess whether the effect of SANE involvement on referral of a case for prosecution was mediated by law enforcement investigatory efforts, formal tests of the significance of the indirect effects were performed, using the recommended product-of-coefficients method, as adapted for Level 1 mediation in multilevel analysis (MacKinnon, 2008).
Results
Table 1 summarizes the first set of regression equations, which tested whether the five SANE involvement variables predicted the hypothesized mediators—the law enforcement effort variables and victim withdrawal from the case—as well as police referral of the case to the prosecutor. Law enforcement agency, month, and whether the forensic exam evidence supported the victim’s account were also included in these analyses. Whether the case was handled before or after implementation of the SANE program was not significantly related to nearly all law enforcement effort variables; cases handled after SANE implementation had significantly shorter police reports than those handled before SANE. As noted previously, most cases in this study were post-SANE (85% of the sample), and this restricted variability may have played a role in the nonsignificant results. On the other hand, perhaps it is the nature of SANE involvement in a case, rather than the simple before- and after-SANE contrast, that matters with respect to law enforcement effort in a case.
Multilevel Regressions Results: The Effect of Sexual Assault Nurse Examiner (SANE) Involvement on Law Enforcement Effort
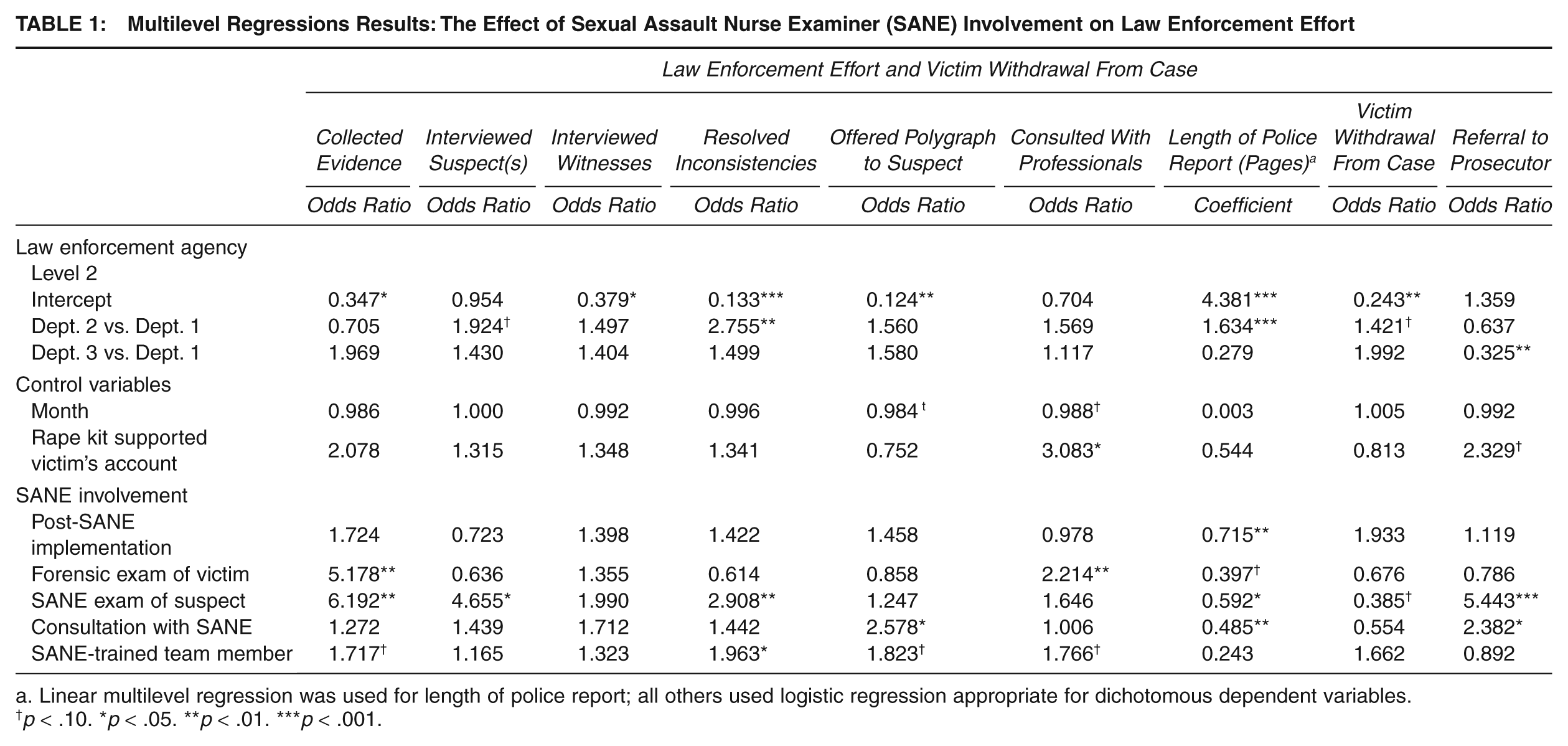
Linear multilevel regression was used for length of police report; all others used logistic regression appropriate for dichotomous dependent variables.
p < .10. *p < .05. **p < .01. ***p < .001.
Indeed, there were several significant associations between specific features of SANE involvement in a case and law enforcement effort (as well as victim withdrawal and police referral outcome). A forensic exam of the victim was associated with consultation with other professionals and with shorter reports. A SANE suspect exam was positively related to law enforcement officers’ collecting additional evidence, interviewing suspects, and resolving inconsistencies; and it was associated with shorter police reports. Cases with a SANE suspect exam were 40% as likely to involve a victim’s withdrawing from the case (i.e., victims were less likely to withdraw if there had been a suspect exam). Cases with a SANE suspect exam were also more than 5 times as likely to be referred to the prosecutor as cases without a suspect exam. Law enforcement consultation with SANE was related to offering a polygraph to the suspect and to shorter police reports as well as to greater likelihood that the case would be referred to the prosecutor. Having a SANE-trained member of the law enforcement team was associated with a greater likelihood of resolving inconsistencies in victim’s and suspect’s accounts and, at p < .10, with collecting additional evidence, consulting with professionals, and offering a polygraph to the suspect.
Table 2 presents the results of the mediational analyses. These regressions tested each of the law enforcement effort variables along with whether the victim withdrew from the case as mediators of the effect of SANE involvement on referral to the prosecutor. With the exception of the length of the police report, all SANE involvement variables that were associated with law enforcement effort at p = .10 or less were included in these analyses (see first section of Table 2). The middle section of Table 2 lists the direct effects of each of the intervening or mediating variables on the dependent variable (referral to prosecutor), controlling for all SANE involvement variables, all law enforcement effort variables, whether the victim withdrew from the case, the law enforcement agency, month, and whether the evidence kit produced evidence supporting the victim’s account. As can be seen, two of the potential mediators did not relate to referral for prosecution: consulted with professionals and resolved inconsistencies. Collected additional evidence, interviewed suspect(s), and victim withdrew all showed significant associations with referral to the prosecutor; consulted with professionals was also associated with referral at p < .10.
Mediation Results: Indirect and Mediated Effects of Sexual Assault Nurse Examiner (SANE) Involvement on Referral Through Law Enforcement Effort and Victim Withdrawal
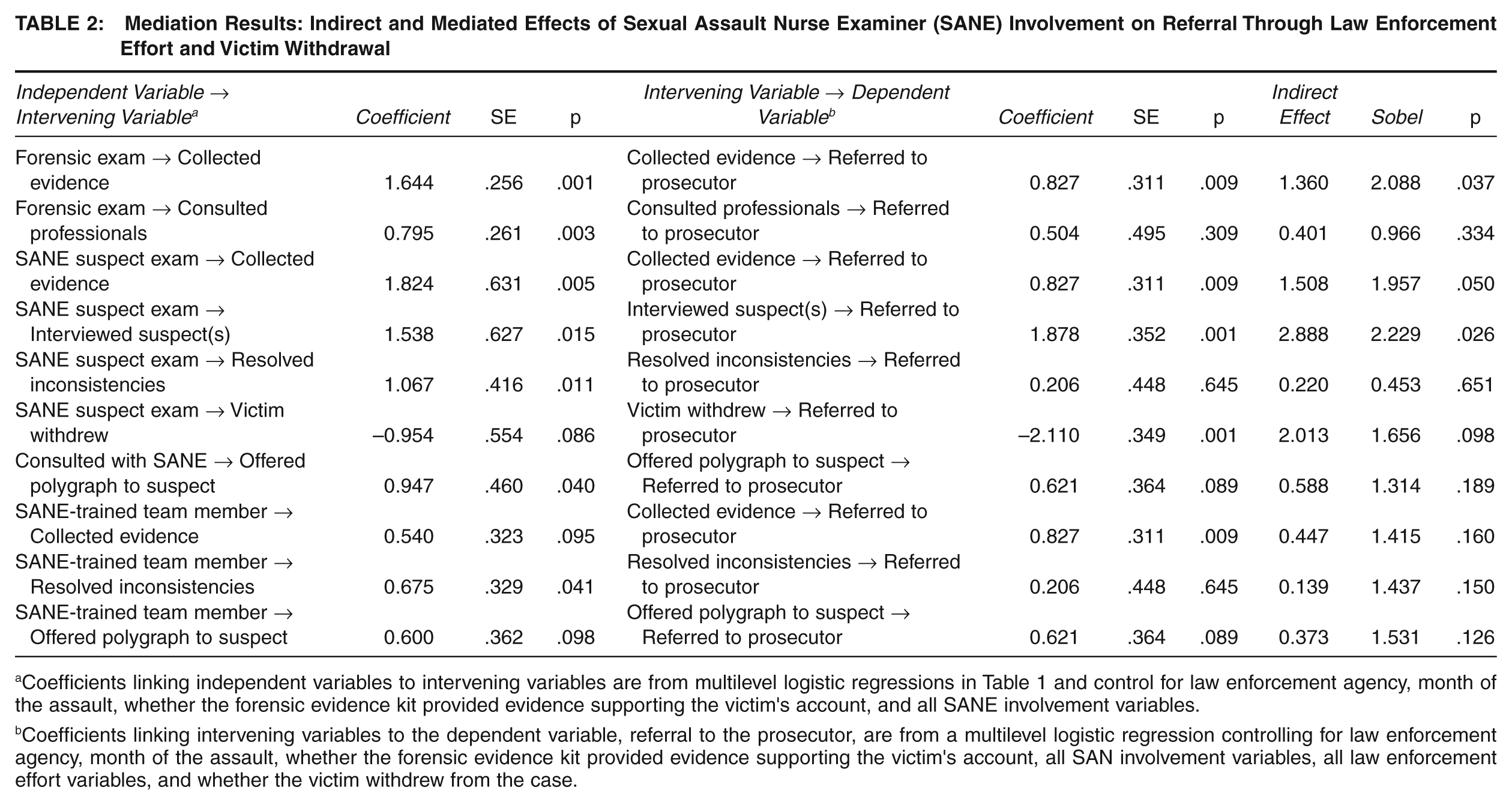
Coefficients linking independent variables to intervening variables are from multilevel logistic regressions in Table 1 and control for law enforcement agency, month of the assault, whether the forensic evidence kit provided evidence supporting the victim’s account, and all SANE involvement variables.
Coefficients linking intervening variables to the dependent variable, referral to the prosecutor, are from a multilevel logistic regression controlling for law enforcement agency, month of the assault, whether the forensic evidence kit provided evidence supporting the victim’s account, all SAN involvement variables, all law enforcement effort variables, and whether the victim withdrew from the case.
The final section of Table 2 presents formal tests of the indirect effect of each SANE involvement variable on referral for prosecution, through each of the law enforcement variables. Three indirect effects were significant at p < .05 (and one trend at p < .10). First, for medical forensic exam through law enforcement–collected evidence, in cases in which the victim had a forensic exam, police collected more kinds of other evidence to support the case, which was associated with increased likelihood of case referral. Second, for SANE suspect exam through law enforcement–collected evidence, in cases where SANE conducted a suspect exam, police collected more kinds of other evidence to support the case, which was associated with increased likelihood of case referral. Third, for SANE suspect exam through law enforcement interview of suspect, in cases where SANE conducted a suspect exam, police were more likely to interview the suspect(s), which was associated with increased likelihood of case referral. Finally, for SANE suspect exam through victim withdrawal (trend), in cases where SANE conducted a suspect exam, victims were somewhat less likely to withdrawal, which had a modest positive effect on case referral.
Because SANE suspect exam showed a significant direct effect on referral for prosecution, its effects, through collected evidence, suspect interview, and victim withdrawal, can be termed mediated effects. The effect of forensic exam through collected evidence is typically not considered a mediated effect because the direct effect of forensic exam on referral for prosecution was not significant (Holmbeck, 1997), although it can be termed an indirect effect. An effort was made to test cross-level interactions to examine the possibility that the effects of SANE involvement or law enforcement effort might differ by law enforcement agency. None of the interactions was significantly different from zero, so these effects were removed from the final models. However, power was not optimal, so the tests for these interactions should not be taken as definitive.
Discussion
Since the 1990s, SANE programs have proliferated throughout the United States in efforts to improve postassault medical care for sexual assault victims and to increase criminal justice system reporting and prosecution. This widespread dissemination has occurred despite minimal data on the effectiveness of these interventions. Only a handful of studies have rigorously evaluated the impact of SANE programs on sexual assault legal case outcomes, and although those findings are promising, there is still much to learn about how and why these nursing programs may have positive crossover effects in the legal system. To that end, this study focused on the law enforcement investigation process to understand (a) how police use SANE program services, (b) whether those services have any demonstrable impact on their investigative practices, and (c) whether SANE services ultimately affect their decision whether to refer a case to prosecutors for further consideration.
Using police reports as the official record of what occurred in the investigation, we explored whether detectives’ practices changed after the implementation of a SANE program in a midwestern community. Unfortunately, we were not able to access an equivalent number of pre-SANE adult sexual assault case reports—which remains an important limitation of this study—but we were able to explore within the post-SANE era how police choose to use the services and expertise offered by the SANE program. Indeed, even after the implementation of the SANE program in this community, not all sexual assault cases had SANE involvement, so we did have sufficient variability to evaluate whether and how SANE services can be useful to police. Using multilevel logistic regression, we found that when victims had medical forensic exams, law enforcement was more likely to reach out to other professionals for consultation regarding the case. Although suspect forensic exams were not typical (8%), they were associated with multiple indices of increased investigative effort, including collecting additional evidence, interviewing suspects, and resolving inconsistencies between the victim’s and suspect’s accounts. Interestingly, victims were significantly less likely to withdraw from the investigation process in cases in which there was a suspect forensic exam. This finding was unexpected and needs further replication, but it is possible that suspect exams may provide supporting evidence for the victim’s account of the assault, which may give victims more hope and confidence that their case will be prosecuted, and hence, they are less likely to withdraw from participation. Other markers of SANE involvement related to law enforcement effort included that police consultation with SANE was associated with suspect polygraphing and having a SANE-trained member of the law enforcement team meant there was a greater likelihood police would attempt to resolve inconsistencies in victim’s and suspect’s accounts.
However, the critical issue is whether SANE involvement affects case referral decisions. Cases cannot be prosecuted if they are not referred by police to prosecutors; cases will not be referred if they have not been found to meet the elements of the crime. Therefore, increasing investigational effort could be a key component of increasing referral rates. We hypothesized that use of SANE services would be associated with increased law enforcement investigational effort, which would predict higher rates of case referral. These mediational analyses are important for understanding the mechanisms by which SANE programs may have positive effects. Overall, our findings revealed that SANE involvement in a case was significantly associated with increased referral rates. Three specific pathways were supported.
First, in cases in which the victim had a medical forensic exam, police collected more kinds of other evidence to support the case, which was associated with increased likelihood of case referral. Medical exam findings may suggest specific investigational leads that police can follow to obtain other evidence. Given the potential utility of medical forensic exams, these findings underscore the importance of ensuring victims’ access to these services. The federal Violence Against Women Reauthorization Act (2005) made significant strides in removing barriers for victims (e.g., victims cannot be billed for exams, victims do not have to file a police report to receive medical care), but in many communities throughout the United States, victims still do not have access to trained medical forensic service providers (IAFN, 2011).
The other two significant pathways highlighted the potential benefits of suspect forensic exams. In the cases in which SANEs conducted a suspect exam, police were also more likely to collect other evidence to support the case and more likely to interview the suspect, both of which were associated with increased likelihood of case referral. In other words, evidence begets more evidence: The additive effect of evidence from the SANEs plus the evidence collected by law enforcement appears to be instrumental in creating a more complete documentation of the crime. Although these findings demonstrate compelling reasons to conduct suspect exams, SANE programs need to evaluate their internal resource capacity before expanding program services to include suspect exams. Critical issues to evaluate include how suspect exams could limit resources available for victim patient care and how and where suspect exams should be conducted to maintain victim safety and confidentiality.
Although these findings have potential to inform policy and practice, it is important to note several limitations of this study that temper the strength of the conclusions that can be drawn from this work. Any study that uses archival records as the primary data source is limited by the quality of the reports themselves. It is certainly possible investigative work was done and not documented, which would mean that these results underrepresent law enforcement effort in sexual assault cases. In spite of this concern, Sherley (2005) noted that analysis of police reports remains one of the best methodologies for understanding the investigative process.
As noted previously, we were not able to obtain a large sample of pre-SANE police reports, because the data systems at the three participating law enforcement agencies did not have such dated reports available. As such, the pre- and post-SANE analyses have limited statistical power. Perhaps not surprisingly, the comparison of pre-SANE and post-SANE reports yielded only one significant finding: Police reports were shorter in the post-SANE era. Our coding of the case files suggests that the post-SANE reports were more focused and actually contained more details and relevant information, perhaps because the implementation of this intervention contributed to increased knowledge and shared expectations regarding critical elements of a sexual assault investigation. Otherwise, we did not find any significant relationships between SANE implementation and investigative practices. However, this pattern of results is actually consistent with the notion that it is not mere implementation of an intervention that matters but rather what services it provides and how it is used by community stakeholders. We did find multiple significant relationships, including indirect and mediated effects, linking specific aspects of SANE involvement to investigation practice and ultimately case referral decisions.
Finally, it is important to keep the scope of this study in context—this was an in-depth examination of police records from three large law enforcement agencies served by one SANE program. Given that there are more than 500 SANE programs in existence, it would be inappropriate to generalize the findings of this one evaluation to the success of SANE programs as an intervention model. Previous research suggests there is substantial variability among SANE interventions with respect to program operation and philosophy (Patterson, Campbell, & Townsend, 2006) as well as organizational relationships with other community stakeholders (Cole & Logan, 2008; Payne, 2007). As such, the ways in which police use SANE services may vary by jurisdiction, and therefore the mechanisms by which these programs contribute to the investigative process could vary tremendously. Our results indicate that SANEs may have positive effects on law enforcement, but these findings need to be replicated in other sites and with different intervention models.
Footnotes
This research was supported by a grant from the National Institute of Justice awarded to the first author (2005-WG-BX-0003). The opinions or points of view expressed in this document are those of the authors and do not reflect the official position of the U.S. Department of Justice.