
Abstract
This research uses specific diagnoses and symptoms of mental disorder (MDO) to predict whether inmates offend in prison. Social psychological theories of aggression are used to make predictions about what types of MDO affect whether inmates commit violent and nonviolent infractions. The analysis was based on a survey of a nationally representative sample of more than 16,000 inmates from state and federal facilities. The evidence suggests that psychosis and major depression have strong effects on infractions involving aggression, whereas the effects of anxiety disorders are weaker and inconsistent. Psychosis and depression are also associated with nonaggressive offenses, suggesting that they have disinhibitory effects on misconduct generally. Analyses of the effects of symptoms suggest that paranoid thinking is the best predictor of offending, particularly, offending that involves aggression. In general, the evidence suggests that both cognitive and emotional aspects of MDO lead to prison offenses.
Research shows that people with at least some types of mental disorders (MDO) are more likely to engage in violence than those without (for reviews, see Link & Stueve, 1995; Monahan, 1992, 2002; Mulvey, 1994; Silver, 2006). Although the association between MDO and violence is fairly well established, it is still unclear whether it is attributable to the causal effects of mental illness (e.g., Silver, 2006; Skeem, Manchak, & Peterson, 2010) or whether it exists in the absence of substance abuse (Elbogen & Johnson, 2009; Steadman et al., 1998). It is also unclear whether particular types of MDO have effects on particular types of aggressive or criminal behavior.
In this research, we examine whether inmates with MDO are more likely than other inmates to engage in violence and other deviant behavior while incarcerated. We use a retrospective longitudinal design in which we control for prior violence and other potentially confounding factors, such as alcohol and drug use. In addition, we examine the effects of various diagnoses and symptoms to determine which types of mental illness affect which types of misconduct. Analyzing the effects of different types of MDO and symptoms on different behavioral outcomes allows us to address the issue of why mental illness might affect deviant behavior, including violence.
Background
Disruptive behavior by prison inmates is a major concern for prison staff and administrators (Friedman, Melnick, Jiang, & Hamilton, 2008). Prison administrators believe that MDO is the most important factor contributing to disruptive behaviors among inmates—more important than gang membership or the presence of long-term inmates or repeat offenders (Ruddell, Decker, & Egley, 2006). Understanding the effects of specific types of MDO on prison misbehavior is important, not only because of the need to maintain order in the prison environment but also because it can help researchers determine what types of services are most likely to improve inmate adjustment.
Concern about MDO among inmates has grown, probably as a result of two social changes in incarceration patterns. The first is the enormous increase in the number of persons admitted to prison since the 1980s. The second is the deinstitutionalization of mental patients that began in the 1950s and 1960s. These changes have likely contributed to growth in the number and proportion of individuals with MDO in jails and prisons. In 2005, more than half of all prison and jail inmates had a recent history of some type of mental health problem, including 56% of state prisoners, 45% of federal prisoners, and 64% of jail inmates (U.S. Department of Justice, 2006), and recent surveys indicate that between 14% and 25% of people in U.S. prisons and jails suffer from a diagnosable mental illness (for reviews, see Morgan, Fisher, & Wolff, 2010; Skeem et al., 2010).
Prison inmates tend to have the same disorders as the general population, although with greater frequency (Adams & Ferrandino, 2008). According to the American Psychiatric Association, mental illnesses most commonly diagnosed in the inmate population are serious, including major depression, schizophrenia, and bipolar disorder (Adams & Ferrandino, 2008). Many have been diagnosed with co-occurring substance abuse disorders as well (Young, 2003). Inmates are also frequently diagnosed with personality disorders, a category that includes antisocial personality. Despite these figures, Beck and Maruschak (2001) found that only about half of all state prisons provide 24-hr mental health care to their inmate populations.
Prior Research
Several studies have examined the relationship between MDO and violence within the prison setting. In one study, Adams (1983) found that former mental patients serving time in federal prison were more likely to attempt escape and to commit assaults, suggesting a tendency toward both aggressive and nonaggressive infractions. In a subsequent study of male inmates in a maximum security state prison, Adams (1986) found that those who had been treated for mental health problems were more likely to commit a variety of prison rule infractions, including refusing to come out of the cell, setting fire to the cell, committing health and hygiene violations, destroying state property, and intentionally injuring themselves. Toch and Adams (1986) also found that among male inmates serving time in New York State’s prison system, those who had been treated for or diagnosed with MDO were more likely to engage in disruptive behaviors, including violence. These results held with criminal histories controlled. More recently, a study of inmates in a prison-based substance abuse treatment program found that symptoms of thought insertion and thought control (e.g., believing that an outside force put thoughts into one’s mind or made one act in unusual ways) increased risk for violent behavior (Freidman et al., 2008). The study, however, found no effect of psychiatric diagnosis per se. Finally, previous bivariate analyses of the data used in the current study revealed that inmates with MDO were more likely to be charged with physical assaults, verbal assaults, and other rule violations while in prison (U.S. Department of Justice, 2006).
Several other studies, however, report null or mixed results. In a study of Ohio State Prison inmates, for example, Cao, Zhou, and Van Dine (1997) found no relationship between mental health history and prison infractions (see also Porporino & Motiuk, 1995). Also, a study of male inmates drawn from the Bureau of Justice Statistics’ 1986 Survey of Inmates of State Correctional Facilities (McCorkle, 1995) found no relationship between mental health status (including prior and current treatment) and prison infractions. Similarly, Baskin, Sommers, and Steadman (1991) found no relationship between psychotic symptoms and offenses among New York State prison inmates. However, a measure of confused thinking (including “trouble remembering” and “getting confused”) was associated with both violent and property offenses, whereas a measure of depression was associated with property offenses only. These results held with criminal histories and demographic characteristics controlled.
Overall, prior research tends to suggest that MDO is associated with prison rule infractions. However, with the exception of Baskin and colleagues’ (1991) results reported above, little is known about which types and symptoms of MDO are associated with which types of infractions. This is because most prior studies have used nonspecific indicators of mental health treatment to categorize inmates as mentally disordered. In addition, most prior work has used incarceration offense as a proxy for criminal history, thus ignoring the longer span of criminal involvement that may predate incarceration. Finally, with rare exceptions, studies have not considered the effects of drug and alcohol involvement in their analyses of prison misconduct. Alcohol problems are a strong correlate of MDO and a strong predictor of violence and other misconduct (e.g., Swanson, 1993). Our multivariate analysis and quasi-longitudinal design using a large, nationally representative inmate sample (U.S. Department of Justice, 2007) will enable us to build on prior work and better address the question of whether specific types and symptoms of MDO are related to violent and disruptive behaviors in prison, controlling for other known risk factors for crime and violence.
Why does MDO have effects?
A major problem in studying the relationship between MDO and violence is the possibility that the relationship is spurious (Hiday, 2006; Link, Andrews, & Cullen, 1992; Monahan & Steadman, 1983; Silver & Teasdale, 2005). Research shows that mental illness and violence share many of the same risk factors, including gender, age, race-ethnicity, individual and neighborhood socioeconomic status, physical and sexual abuse, stressful life events, impaired social support, and substance abuse (Aneshensel, 1992; Arseneault, Moffitt, Caspi, Taylor, & Silva, 2000; Hiday, 2006; Monahan et al., 2001; Silver, 2000, 2006; Silver & Teasdale, 2005; Swanson, 1993; Swanson, Holzer, Ganju, & Jono, 1990). Although individual studies have taken into account some of these variables, no study has taken into account all or most of them. In addition, there are probably other common causes that are not yet known. Thus, the possibility remains that the association between MDO and violence that has been reported in prior studies is spurious, not causal.
Two large-scale longitudinal studies found no evidence that MDO has an effect on violent behavior when substance abuse was taken into account (Elbogen & Johnson, 2009; Steadman et al., 1998). On the other hand, a retrospective longitudinal analysis that controlled for substance use and prior violence did find evidence that MDO was associated with violent offending (Silver, Felson, & VanEseltine, 2008). None of these studies examined specific types of MDO.
The literature on why MDO might lead to violence is rather limited. The most well-known approach is research that focuses on the effects of what Link and colleagues called “threat-control override” delusions (e.g., Link, Monahan, Stueve, & Cullen, 1999; Swanson, Borum, Swartz, & Monahan, 1996). These delusions include paranoid beliefs and perceptions of thought control by others. In an Israeli sample, Link et al. (1999) found that the relationship between psychosis or bipolar diagnoses and violence was reduced and became statistically insignificant when they controlled for threat-control override delusions. Hallucinations and other psychotic symptoms had no effect. Earlier studies by Link and Stueve (1994) and Swanson et al. (1996) also found that threat-control override symptoms were related to violence even with controls for other psychotic symptoms.
Empirical support for the effects of threat-control override delusions on violence, however, has been mixed (Appelbaum, Robbins, & Monahan, 2000; Stompe, Ortwein-Swoboda, & Schanda, 2004). In addition, there is reason to question whether the measure established by Link and colleagues (1991), which combined paranoid beliefs with perceptions of thought control by others, was the best approach. For example, Teasdale, Silver, and Monahan (2006) found that when they separated the paranoid and thought-control components of this measure, only the paranoid component was predictive of violence, and this result held only for males (but see Link et al., 1999). Moreover, Quanbeck et al. (2007) found that aggressive acts committed by 88 chronically assaultive psychotic patients in a state hospital were most often committed under the influence of paranoid ideation. Thus, more research is needed to better understand the role that paranoid delusions play in the occurrence of violence.
A Social Psychological Approach
We borrow from Link and colleagues’ (1999) work and attempt to place the discussion in a larger theoretical context. Specifically, we rely on the social psychological literature on aggression to formulate hypotheses as to why MDO might be associated with violence and other forms of offending behavior. We draw on this literature to make predictions regarding how different types of MDO, including paranoid delusions, should be associated with violence and other deviant acts.
Social psychological theories emphasize the distinction between causal factors that instigate aggression and causal factors that act as inhibitors (or disinhibitors). Instigators produce the motivation to harm someone, whereas inhibitors constrain people from acting on that motivation. Inhibitors include moral values and perceptions of costs, and their impact depends on the ability of people to engage in self-regulation or self-control (e.g., Baumeister, Heatherton, & Tice, 1994). Self-control, however, plays a role in all deviant behavior, not just behaviors that involve intentional harm doing. Thus, Gottfredson and Hirschi (1990) argue for a general theory of crime based on self-control and reject the idea that individual differences produce violent crime specifically. They claim that the incentives for crime are similar for everyone and that individual differences in criminal behavior reflect differences in inhibitions or controls. As a result, offenders are versatile, that is, they commit a variety of crimes rather than specialize in particular types of crime.
Mental illness could affect aggression because it interferes with an actor’s ability or desire to inhibit or regulate behavior. People with MDO may be less likely to engage in self-regulation or self-control because their focus of attention is on themselves (Baumeister et al., 1994). Those who are severely depressed, for example, may not think about costs or legal rules because they are preoccupied with their own problems. However, if people with MDO lack self-control, they should be more likely to engage in deviance generally, not just deviance involving aggression; they should be versatile offenders, not just violent offenders, following Gottfredson and Hirschi’s (1990) logic.
An alternative argument is that MDO leads specifically to the instigation of aggression or intentional harm doing. Social psychology suggests two explanations for why people with severe mental illness might have a stronger motivation to harm others. The first is Berkowitz’s (1989) theory of reactive aggression, a revision of the frustration-aggression approach originally proposed by Dollard, Doob, Miller, Mowrer, and Sears (1939). Berkowitz distinguishes between reactive and instrumental aggression, that is, harm doing that is a means to an end. According to the theory, negative affect is an innate instigator of reactive aggression. Any type of aversive stimuli leads to negative affect, which then leads to aggression, depending on inhibitory factors. Cognitions still play a role in reactive aggression, however, since negative affect depends on the person’s interpretation of stimuli as aversive and since people tend to inhibit their aggression if they anticipate that it will be too costly. From this perspective, serious depression should be a particularly strong predictor of aggression. Depression is diagnosed, according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 2000), when a person experiences chronic negative affect (e.g., sadness) and associated behaviors. On the other hand, depression should not instigate instrumental aggression or deviant behavior where there is no intent to harm. 1
The second approach to instigation treats all aggression as instrumental and emphasizes cognitive factors, the offender’s definition of the situation, and social interaction between offender and victim (Tedeschi & Felson, 1994). It suggests that people use aggression when they believe the rewards are greater than the costs. People often engage in aggression when they feel they have a grievance or when they believe they are under attack. Their behavior is directed toward the person who has offended them, and their goal is to deter their antagonist, save face, or to promote retributive justice. Sometimes their decision making is careless, and they attack impulsively, without consideration of costs. Other times, they are more calculating, and prepare for aggressive encounters. Either way, they harm their victim to achieve something they value.
Thus, the instrumental approach implies that MDO is an instigator of aggression primarily because of its cognitive effects. Mental illness can lead to aggression and violence if it is associated with delusional (or psychotic) thinking and these delusions are conducive to aggression and violence. It is disordered thinking among people who are mentally ill, rather than negative affect, that motivates them to harm others. Their aggressive response is “rational,” given their definition of the situation (Silver, 2006). The instrumental approach does not rule out the effects of emotions, however. Negative affect can produce careless decision making, but it is a disinhibitor (or facilitator), not an instigator. Thus, depression should play a disinhibiting role if it reduces self-control among people who are mentally ill. In addition, people often feel anger and fear when they believe they are under attack. But their aggression is an instrumental act, not an innate and automatic response to these emotions. Along these lines, Storbeck and Clore (2007) suggest that cognition and emotion may be interdependent systems but that emotion modulates and mediates basic cognitive processes. In addition to the work by Link and colleagues (1999; described above), studies finding a relationship between delusional thinking and violence provide evidence in favor of the instrumental perspective (Junginger, Parks-Levy, & McGuire, 1998; Swanson et al., 1996; Taylor, 1985; Taylor et al., 1998).
From our perspective, then, Link and colleagues’ (1999) studies of the effects of threat-control override delusions on violence fits within the instrumental approach because they emphasize cognitive factors, that is, the definition of the situation. They argue that individuals suffering from psychosis engage in violence when they feel threatened.
Current Study
We examined the relationship between various mental health diagnoses and symptoms and offending in prison. The offenses included violence against staff, verbal aggression against staff, violence against inmates, verbal aggression against inmates, weapon offenses, substance abuse violations, and other nonviolent offenses. All involve deviant behavior by definition, but only some involve intentional harm doing, that is, aggression. The diagnostic categories include psychosis, major depression, and anxiety disorders. The symptoms include hopelessness, paranoia, delusions of thought control, and hallucinations. Hopelessness is a symptom of depression, whereas the others are symptoms of psychosis.
The discussion above implies that if MDO affects self-control or some other inhibitory factor, it should be associated with deviant behavior regardless of whether that behavior involves aggression. Versatility implies individual differences in inhibition rather than instigation. Both the reactive aggression and the instrumental approach recognize the effects of inhibitory factors, so they would not rule out effects of MDO on all types of deviant behavior. However, both imply that MDO should more strongly predict deviant behavior involving aggression, since MDO is related to instigation as well as inhibitory factors.
On the other hand, they would make different predictions about which types of MDO are likely to predict offenses involving aggression. The reactive aggression approach implies that depression should be better than other MDOs at predicting offenses involving aggression since it involves extreme and chronic negative affect. The instrumental approach, on the other hand, implies that paranoia—a symptom of psychosis—should be the best predictor of offenses involving aggression because people who are paranoid think they are defending themselves from attack. The instrumental approach would also predict that paranoid inmates are more likely to commit weapon offenses. Paranoid inmates who respond “rationally” to imagined threats, may acquire weapons to protect themselves in anticipation of violent encounters. Their response is a reasoned one, not just an emotional outburst reflecting an accumulation of negative affect, as proposed by the reactive aggression approach.
Following Link et al. (1999), we also examine whether the effects of a diagnosis of psychosis is reduced when threat-control override symptoms (and other symptoms associated with psychosis) are controlled. Recall that they found evidence that controlling for a scale combining paranoia and thought-control delusions reduced the effect of a combined measure of psychotic and bipolar diagnoses on violent offending. We argue that paranoia, not delusions about being controlled, should be the key symptom, and we have sufficient cases to examine the issue.
A summary of the hypotheses associated with each of the theoretical perspectives described above is presented below:
Hypothesis 1: According to the disinhibition hypothesis, all types of MDO will predict all types of infractions, not just those involving aggression.
Hypothesis 2: According to the reactive aggression approach, depression will be the best predictor of infractions involving aggression and will be less predictive of other infractions.
Hypothesis 3: According to the instrumental approach, (a) psychotic disorders involving paranoid ideation will be the best predictor of infractions involving aggression but will be less predictive of other types of infractions, and (b) the effects of a diagnosis of psychosis should be reduced when paranoia is controlled.
Method
Sample
Our analyses were based on the Survey of Inmates in State and Federal Correctional Facilities, 2004 (U.S. Department of Justice, 2006). The data were obtained from a nationally representative sample of inmates from state and federal facilities. The survey used computer-assisted personal interviews to ask questions about personal characteristics, criminal history, conditions of the current offense, offenses while in prison, drug and alcohol use, and inmate health. The total response rate was 88%, leaving an eligible sample of 18,185 cases. The variables included in the analysis had less than 5% missing data, with the exception of income (17.5%). Those with missing data on income were assigned the mean for the sample. A variable indicating those cases where income was imputed was included in equations but was not statistically significant and so is not shown in the tables. After listwise deletion on all other measures, our analytic sample consisted of 16,285 individuals.
Measures
Our dependent variables were based on questions in which inmates report whether, since admission, they were “written up or found guilty” of violence against staff, verbal aggression against staff, violence against inmates, verbal aggression against inmates, weapon offense, substance abuse violations, or other nonviolent offenses (e.g., possession of stolen property or disobeying orders). Respondents could answer yes or no.
The inmate survey includes measures of MDO involving both diagnoses and symptoms. Major (Axis I) diagnoses were measured by asking inmates whether they had ever been told by a mental health professional, such as a psychiatrist or psychologist, that they had major depression, mania, or a psychotic disorder (such as schizophrenia). Inmates were also asked about less serious psychiatric (Axis II) disorders: posttraumatic stress disorder, anxiety disorder (e.g., panic disorder), and personality disorder.
We did not include mania in our analyses because its relationship with depression (phi = 0.53) weakens the effects of each somewhat. In addition, since mania is a mood disorder that often includes both depression and euphoria, it does not provide a clear test of the effects of negative affect. We also did not examine the effects of personality disorder because it includes antisocial personality disorder. Clinicians sometimes use this diagnosis for people with a history of criminal behavior. To that extent, we have a problem of tautology. In analyses where we included mania and personality disorders (not presented), the results we present were slightly weaker, but the conclusions were the same. Mania had inconsistent effects that were a bit weaker than the effects of depression.
Unfortunately, the inmate survey included only a limited number of questions about symptoms. All of the questions were based on the inmate’s experience during the past year. Our indicator of depressive symptoms is whether they reported that they had “given up hope for life or the future.” Paranoia is indicated if they reported that they “felt spied on or plotted against.” Our measure of thought-control delusions was based on two summed items: whether they thought that other people could either read their minds or control their thoughts. Our measure of hallucinations was also based on two summed items: whether they reported that they could see things or hear voices other people could not. Respondents could indicate yes or no for diagnoses and symptoms questions.
Our control variables included prior violent behavior, years in prison since admission, alcohol and drug use, and demographic factors. The measure of violent history consisted of the most recent offense, that is, the one that resulted in current incarceration, and any violent offenses that resulted in incarceration or probations in the past. Chronic alcohol use was measured from self-reports of drinking during the year prior to the offense and was coded as a series of dummy variables: daily or almost daily, at least once a week, or less than once a week. The reference category included those who did not drink or drank less than monthly.
To measure drug use, respondents were asked about the frequency of use of 14 categories of illicit drugs, including inhalation of legal chemicals and use of regulated drugs without a prescription. If respondents reported ever using a drug, they were asked for the frequency of use of that drug in the month before arrest. The highest reported frequency of all the drug types was taken and coded as three dummy variables: daily or almost daily, at least weekly, or less than weekly. The reference group includes those who did not report any drug use in the month prior to arrest.
Demographic control measures included gender, age, race, education, and income. Gender is a dichotomous variable coded 1 for male and 0 for female. Age at admission was coded in years, calculated using the respondent’s date of admission and date of birth. Race was measured using three dummy variables: African American, Hispanic, and other races (primarily Asian and Native American), with a reference category of non-Hispanic White. Education was the highest grade of school attended and ranged from 0 to 18. Income was personal monthly income during the month prior to entering prison, captured in a scale that ranged from 0 (no income) to 12 ($7,500 or more per month).
Data Analysis
We used multinomial logistic regression to assess the relationship between MDO diagnoses and symptoms and various prison infractions. Multinomial regression is appropriate when the dependent variable consists of two or more nonordered categories and is particularly useful for facilitating comparisons among multiple categories (Long, 1997). The seven dependent variables in this analysis have three distinct categories. The first consists of individuals who committed the infraction of interest (such as violence against inmates), the second is composed of individuals who reported zero prison infractions, and the third includes inmates who had a prison offense but not one that involved the infraction of interest. For the purposes of the present study, we focused on the comparison between Categories 1 and 2, individuals who committed the infraction of interest compared to individuals who did nothing. We do not report or interpret the results from the third category because of its heterogeneity. Isolating this residual category allows us to compare specific infractions, such as violence against inmates, from those who had never been written up or found guilty of a prison infraction.
We began our analysis by examining descriptive statistics and correlations among key constructs. Next we drew on multinomial logistic regression to assess the effects of different MDO diagnoses and symptoms on seven different prison infractions (Hypotheses 1, 2, and 3a). Finally, we examined whether symptoms mediated the effects of diagnoses on infractions (Hypothesis 3b), again relying on multinomial regression.
Results
In Table 1, we present the descriptive statistics. The table shows that the most frequent prison infractions by far were other nonviolent offenses (32%). The most frequent offense involving aggression was violence against another inmate (12%). Physical aggression against staff (2%) and weapon possession (3%) were the least common offenses.
Descriptive Statistics (N = 16,285)
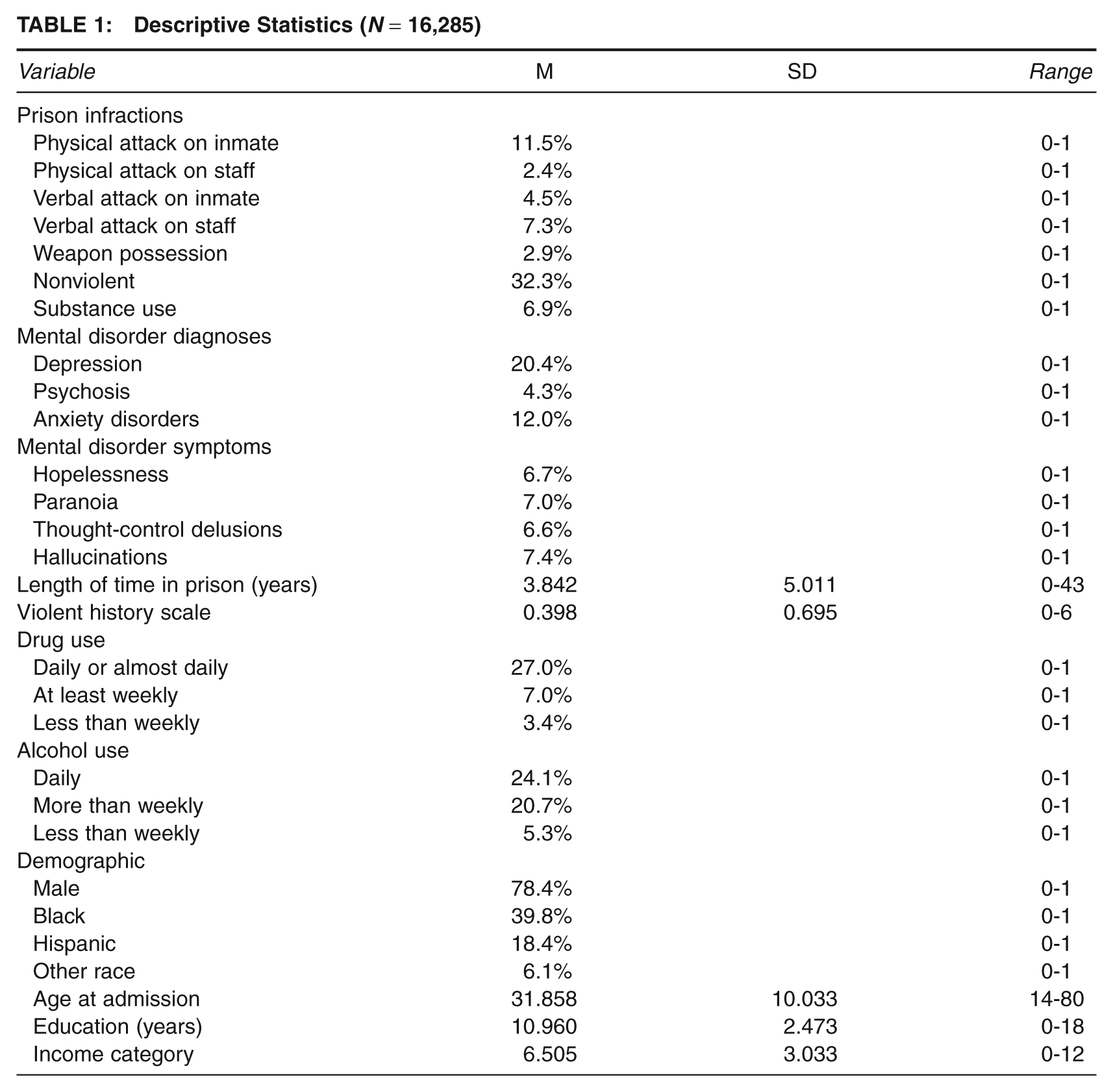
The table also shows relatively high rates of MDO. Major depression was the most frequent diagnosis (20%), and psychosis was the least frequent diagnosis (4%). In terms of symptoms, 7% reported feeling hopeless, 7% felt paranoid, 7% reported at least one thought-control delusion, and 7% reported experiencing at least one hallucination. These rates are much higher than those typically found in general population samples (e.g., Link et al., 1999), making it possible for us to analyze their unique associations with prison infractions.
Before embarking on the multivariate analyses, we examined bivariate correlations between the diagnosis and symptom measures for evidence of convergent validity. The association between having a major depression diagnosis in one’s lifetime and exhibiting the symptom of hopelessness in the past year was phi = 0.19 (p < .001). The associations between having a diagnosis for psychosis and symptoms of paranoia, thought-control delusions, and hallucinations in the past year were phi = 0.20 (p < .001), phi = 0.18 (p < .001), and phi = 0.31 (p < .001), respectively. These associations show that the lifetime diagnosis and past-year symptom measures are related to one another in the expected direction.
In Table 2, we present results from a multinomial logistic regression equation predicting violence against other inmates. The reference category includes inmates who have not had a prison offense. First, we discuss the effects of the control variables. We delay the discussion of the effects of MDO until we present Table 3. The results show that inmates who are male, young, Black, and uneducated are more likely to commit violence against another inmate than their counterparts. The results in this study do not differ by gender. Inmates are more likely to commit violence against another inmate if they have been incarcerated for a longer period, have a history of violent offenses, and were drug users or frequent drinkers before coming to prison. These are all expected patterns and suggest that our measures have predictive validity. We do observe one unexpected finding: Inmates with higher incomes in the month preceding their arrest were more likely to have committed an offense. Note that this income effect was observed for many of our other outcome variables as well (results not shown but available upon request from the authors).
Multinomial Logistic Regression Predicting Violence Against Other Inmates Compared to No Infractions (
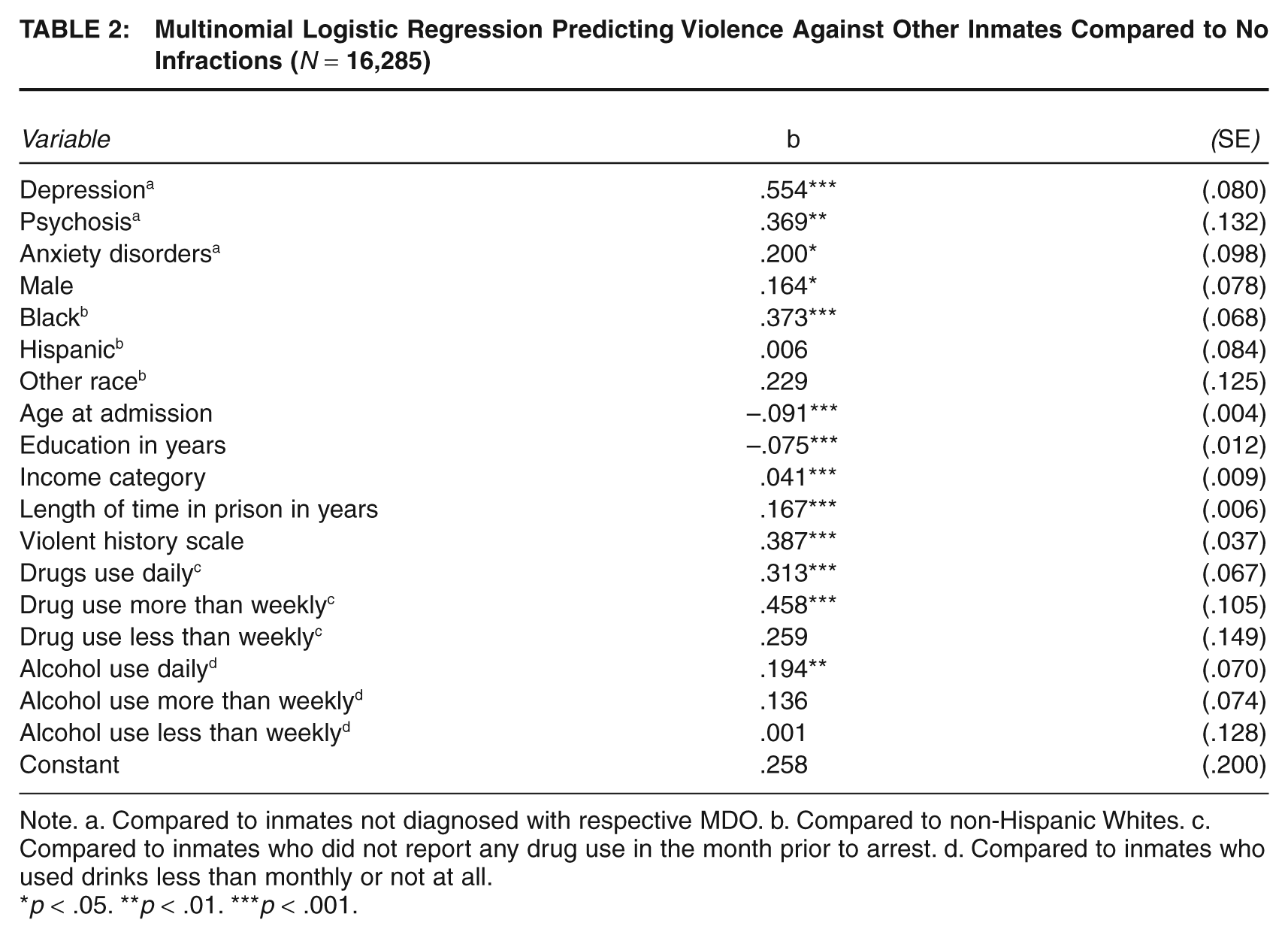
Note. a. Compared to inmates not diagnosed with respective MDO. b. Compared to non-Hispanic Whites. c. Compared to inmates who did not report any drug use in the month prior to arrest. d. Compared to inmates who used drinks less than monthly or not at all.
p < .05. **p < .01. ***p < .001.
Multinomial Logistic Regression Predicting Inmate Misconduct Compared to No Misconduct (
Note. All control variables are included in the analyses but not shown. Standard errors are in parentheses.
p < .05. **p < .01. ***p < .001.
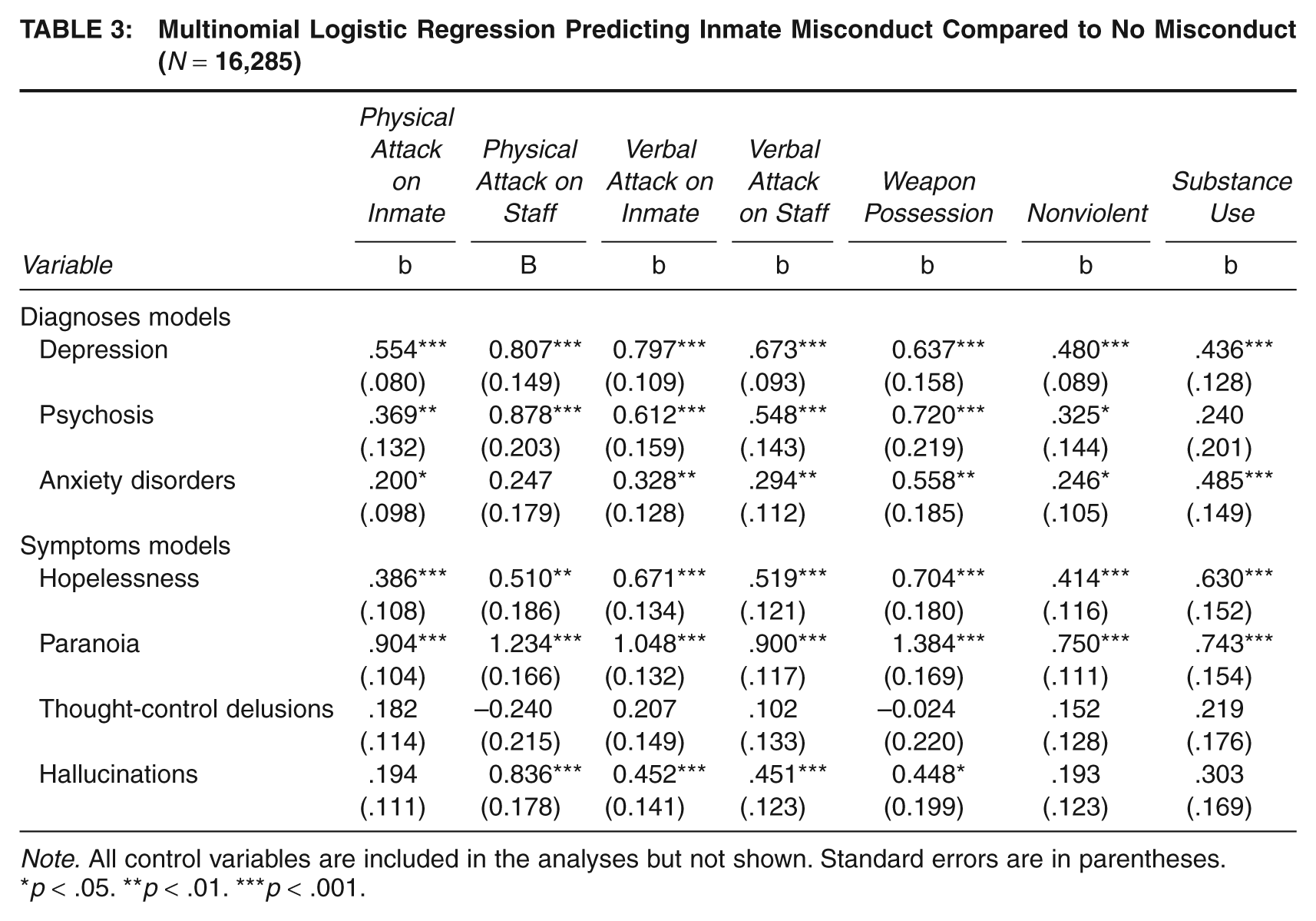
In Table 3, we present the results from multinomial logistic regression equations predicting the seven offenses. The results are based on equations similar to the equation presented in Table 2. Thus, the reference category for each outcome includes inmates who had never committed a prison offense. Because of space limitations and because the effects are substantively uninformative, the results for the residual categories—those inmates who committed a prison offense but not the one being analyzed—are not presented. To facilitate comparison, we include the results for MDO and violence against inmates from Table 2. To preserve space and avoid redundancy, we do not present the effects of the control variables, although they were included in the equations. Their effects were similar to those presented in Table 2. In the lower panel of Table 3, we present the results for equations in which we substitute symptoms for diagnoses.
According to the disinhibition hypothesis (Hypothesis 1), all types of MDO should predict all types of offending. We generally observe support for the hypothesis when we examine the effects of the Axis I diagnoses, major depression and psychosis. Depression is associated with all seven offenses, whereas psychosis is associated with every offense except substance use. 2 The symptom results also provide some support for the disinhibition hypothesis. Those who experience hopelessness, paranoia, and hallucinations are more likely to commit almost every offense. The effects of hallucinations are the weakest, and they predict only violent offenses. None of the offenses is significantly related to delusions of thought control.
The results for the Axis II diagnosis in our analysis, anxiety disorders, provide mixed support for the disinhibition hypothesis. Anxiety disorders are related to all outcomes, although the coefficient for physical violence against staff is not statistically significant. The effects are generally weaker than the effects of depression and psychosis. The effects on weapon violation and substance use, however, are substantial.
Our second hypothesis, based on reactive aggression theory, is that depression is the primary predictor of offenses involving aggression but not the other offenses. We observe some support for this hypothesis in our analyses involving diagnostic categories. For three of the four offenses involving aggression (excluding weapon violations), depression has a larger effect than the other diagnoses. In addition, the coefficients for depression appear to be somewhat stronger for offenses involving aggression than those not involving aggression. Note, however, that all of these differences are slight and may reflect random variation.
When we focus on the measures of symptoms, we do not find support for the reactive aggression hypothesis. Hopelessness, our measure of depression, is never the strongest predictor. In addition, the coefficients for hopelessness are similar in strength for offenses involving aggression and those not involving aggression. This pattern does not support a reactive aggression approach, which predicts that the coefficients for hopelessness should be stronger for offenses involving aggression.
We do see evidence supporting the main hypothesis derived from the instrumental approach (Hypothesis 3a). For every offense, the strongest coefficients are observed for paranoia. They are particularly strong for the offenses involving aggression, with coefficients ranging from 0.90 for violence and verbal aggression against staff to 1.38 for weapon offenses. For example, paranoia increases the odds of an inmate committing a weapon offense 3.99 times (exp[1.36]). The coefficients for hallucinations are small, with one exception, and in every case, they are much weaker than the coefficients for paranoia. The coefficients for delusions of thought control are small and nonsignificant.
Analysis of Psychotic Diagnosis and Related Symptoms
In Table 4, we examine whether controlling for psychotic symptoms affects the relationship between diagnosed psychosis and offending (Hypothesis 3b). We do not examine substance use offenses because it was not significantly related to psychosis in our earlier analysis, and we do not include delusions of thought control because we have already established they have no effects. First, we present the effects of psychosis that were shown in Table 3. Then we show the effect of psychosis when hallucinations and paranoia are included in the equations and the coefficients for paranoia and hallucinations. The results show all of the coefficients for psychotic diagnosis are dramatically reduced in magnitude when the symptoms are introduced into the equations and are rendered nonsignificant for violence against inmates, weapon, and nonviolent offenses. Reductions in the psychosis coefficients range from 51% for violent behavior against other inmates to 40% for verbal aggression against staff. In addition, hallucinations are significant in only two instances (physical and verbal aggression against staff), whereas paranoia remains highly significant for all offenses. Overall, the results suggest that paranoia is the key symptom that explains the effects of psychosis. Analyses not presented indicate that controls for the psychotic symptoms (paranoia or hallucinations) did not alter the effects of depression.
Analyses of Diagnosis and Symptoms: Multinomial Logistic Regression Predicting Inmate Misconduct (
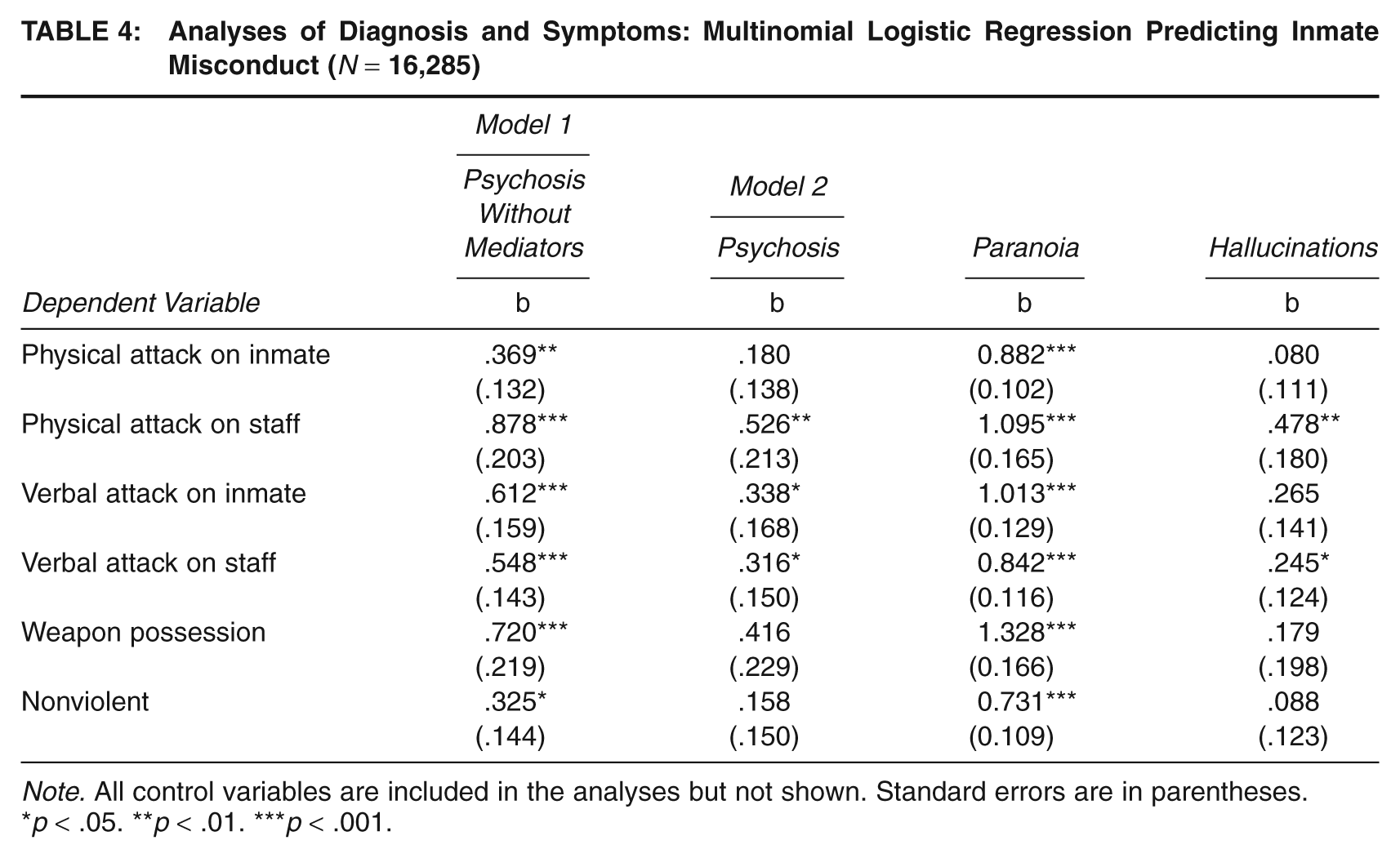
Note. All control variables are included in the analyses but not shown. Standard errors are in parentheses.
p < .05. **p < .01. ***p < .001.
Supplementary Analyses
One possibility is that inmates with MDO are more likely to aggress against other inmates because they have been victimized by those inmates. To address this issue, we examined whether the effects of MDO on a combined indicator of verbal or physical aggression against another inmate were weaker when we controlled for victimization. The results (not presented) showed that this control did reduce some of the effects of diagnoses and symptoms on aggression; however, the effects for depression and psychotic disorder remained significant, as did the effects of paranoia and hopelessness. All supplementary analyses are available from the first author.
We also were able to address the causal ordering issue, at least for diagnoses. Perhaps prison inmates received a diagnosis because of the offenses they committed in prison. To address these concerns, we reanalyzed the data separating those inmates who were diagnosed before admission and those who were diagnosed after admission. The distinction was based on a question in the survey that asked when inmates received their most recent diagnoses. We separated inmates with diagnoses into those who were diagnosed within the past 2 years and those who were diagnosed more than 2 years ago. We restricted the analysis to those inmates who had been incarcerated for 2 years or less so we could be certain the diagnoses occurred prior to admission. If offending leads to diagnosis, then offenses should be more strongly related to postadmission diagnoses. We found no evidence that the timing of diagnosis mattered. The effects of pre- and postadmission diagnoses were similar in strength and not significantly different from each other.
Discussion
We examined three basic questions in the study of MDO: (a) Is there evidence that it has a causal effect on offending? (b) If so, what types of MDO affect offending? and (c) What types of offending does MDO affect? Theoretically, we were interested in which social psychological approach to aggression better explained the pattern of effects. The reactive aggression approach focuses on negative affect and therefore emphasizes the role of depression as an instigator of offending. An instrumental approach focuses on cognition and emphasizes paranoid beliefs as an instigator of aggression. Both approaches are consistent with the idea that MDO might reduce inhibitions and that any type of MDO can lead to versatile offending. They differ in their approach to motivation and therefore in their identification of what aspect of MDO is an instigator and what type of behavior gets instigated.
Our results suggest that major depression and psychosis, and most of the associated symptoms, have strong effects on offending in prison. These effects are observed with controls for prior violence and other potentially confounding factors, such as alcohol and drug use. The fact that these effects were observed for all types of offenses supports the idea that major mental illnesses affect deviant behavior, in part, because they reduce inhibitions. Inmates with major forms of MDO lack either the ability or the willingness to control themselves. We based this argument on Gottfredson and Hirschi’s (1990) argument that versatility of offending indicates that it is not the attractiveness of particular crimes that leads to offending but rather more general inhibitory deficits. Future research should directly measure inhibitions and examine whether they play a mediating role, as we suggest.
The effects of anxiety disorders were weaker and were not consistently observed. It is interesting, however, that that they had substantial effects on weapon violations and substance use. Apparently, inmates who are more anxious and fearful obtain weapons to protect themselves and self-medicate by drinking and using drugs. They are only slightly more likely to engage in verbal aggression and physical violence.
Support for the reactive aggression approach was mixed. Diagnosed depression was generally a better predictor of infractions involving aggression than were other diagnoses, and it appeared to have a somewhat stronger effect on offenses involving aggression than other offenses. On the other hand, the evidence on symptoms was not supportive. The effects of hopelessness were not nearly as strong as the effects of paranoia, and they were just as strong for nonviolent offenses as for infractions involving aggression. In addition, both of our measures of depression were just as strongly related to weapon violations as they were to aggression. Reactive aggression implies a stronger effect on spontaneous acts of aggression than on a variable measuring preparation for aggression or protection.
The evidence was more consistent with an instrumental approach and its emphasis on cognition. Paranoia is the strongest predictor of violent offenses, and it accounts for a substantial portion of the effect of psychosis. When inmates think others are spying on them or plotting against them, they are much more likely to verbally and physically attack staff and other inmates, and they are much more likely to arm themselves. The findings are consistent with the social psychological literature on the hostility bias. When people think that they are being attacked, whether they are or not, they are more likely to engage in aggression. Finally, the finding that paranoia is a particularly strong predictor of weapon offenses is consistent with an instrumental approach. Paranoid inmates do not just strike out at others, as one might expect if they were responding automatically to negative affect; they sometimes plan for violent offenses by obtaining weapons.
Our findings clarify prior research by Link et al. (1999), who did not distinguish paranoid delusions from thought-control delusions. Consistent with results reported by Teasdale and colleagues (2006), our results suggest that the assertion that threat-control override symptoms produce violence should be amended. Thought-control delusions have no effects. It is primarily the person’s definition of the situation as threatening that leads to violence and arming oneself in anticipation of violence.
Although not examined here, it is also possible that types of thinking other than those involving paranoia may be involved in the offending behavior of people with MDO (Mandracchia, Morgan, Garos, & Garland, 2007; Morgan et al., 2010; Sacks, Sacks, McKendrick, Banks, & Stommel, 2004). Simourd and Oliver (2002), for example, found that inmates with MDO exhibited higher scores on a scale measuring criminogenic thinking than other inmates, including negative attitudes toward the justice system, tolerance for law violations, and identification with criminal others. In addition, studies show that the predictors of recidivism among offenders with MDO tend to be similar to those of offenders without MDO (Bonta, Law, & Hanson, 1998). If inmates with MDO hold attitudes conducive to crime, they should have lower inhibitions and should have higher rates of crime generally.
We interpreted the perception that others are spying on and plotting against the inmate as reflecting paranoia. An alternative interpretation is that the perception is not a delusion and that violent inmates actually are more likely to be the target of spying and plotting by staff and by other inmates. However, paranoia correlates just as highly with a diagnosis of psychosis as the other symptoms do, suggesting a strong role of delusion. In addition, one could just as easily argue that violent inmates are less likely to be the target of plots, since other inmates are more likely to fear them.
Limitations
Our measures include only offenses for which the inmates were written up or convicted. We therefore miscode those inmates who committed offenses but avoided sanctions. In addition, we had to rely on self-reports of infractions, since the data set does not include prison records. However, as long as the measurement error is not related to our independent variables, it should not bias our parameter estimates. Random measurement error on the dependent variable can influence the intercept or increase the size of standard errors, but it does not bias parameter estimates (Alwin, 2007). On the other hand, we cannot rule out the possibility that systematic measurement is biasing our effects. For example, one could argue that inmates with MDO, or with particular types of MDO, are more likely to be apprehended or written up than other inmates. On the other hand, the reverse may be true. Engel and Silver (2001) found that police were less likely to arrest suspects they believed had MDO.
It is also possible that our coefficients are biased because of error in our diagnosis measures. For example, some inmates may have MDO but were never diagnosed, whereas others were diagnosed but do not remember it. In addition, the diagnoses that were reported to inmates by prison staff may be inaccurate. Unfortunately, we are unable to examine their validity. Note, however, that we are most interested in the relative effects of different types of MDO on different types of offenses. Only if there was more measurement error in one type of diagnosis than another would it affect the relative strength of each. Even if this were the case, it would not affect the relative strength of effects on different types of offenses.
Finally, we have no way of knowing whether our results can be generalized to criminal behavior in the general population. Perhaps MDO has stronger effects on inmates because they already have a propensity to commit crime. In addition, prison settings are dramatically different from other settings. It may be that the effects of MDO are stronger in prison because of the stress or weaker because of the structure and constraint.
Note, however, that studying the effects of MDO on offenses committed by incarcerated felons also has advantages. First, it allows us to examine serious violence. Research based on the general population focuses on minor acts of violence since they occur much more frequently than serious violence. Second, we have many more cases of serious mental illness than we would if we were studying the general population. We have enough cases to examine the effects of specific diagnoses and symptoms.
Policy Implications
Our results have implications for the management and treatment of inmates with MDO in prison. Specifically, our results suggest that inmates who enter prison with major MDO may have greater difficulties adjusting to the prison environment than inmates without MDO, as evidenced by their greater likelihood of violating prison rules. These findings are especially important since “by all objective measures, correctional facilities in the United States have become the primary mental health institutions in the nation” (Adams & Ferrandino, 2008, p. 913). Our results suggest that treatment services should be aimed at inmates with depression and psychosis, focusing especially on those with paranoid delusions. Alleviating the adjustment problems of these inmates is in the interest of the inmate, since infraction records affect parole decisions. It is also in the interest of staff and other inmates, since it increases their safety.
Conclusion
We have provided evidence that inmates with depression and psychosis are much more likely to engage in verbal and physical aggression against the staff and against other inmates. In addition, they are much more likely to garner weapons. The fact that they are also somewhat more likely to engage in nonaggressive offenses suggests that a lack of inhibition may help explain why people with MDO are more likely to engage in misconduct. We also see evidence that MDO is an instigator of aggression when it involves paranoia, a delusional definition of the situation. When people believe they are being attacked, whether they are or not, they attempt to defend themselves, and sometimes their response involves aggression.