
Abstract
This pilot study compared outcomes for 94 women offenders in San Diego County, California, who participated in four drug court programs. Women were randomized to gender-responsive (GR) programs using Helping Women Recover and Beyond Trauma or standard mixed-gender treatment. Data were collected at program entry, during treatment, and approximately 22 months after treatment entry. Bivariate and multivariate analyses were conducted. Results showed that GR participants had better in-treatment performance, more positive perceptions related to their treatment experience, and trends indicating reductions in posttraumatic stress disorder (PTSD) symptomology. Both groups improved in their self-reported psychological well-being and reported reductions in drug use (p < .06) and arrest (a diagnosis of PTSD was the primary predictor of reductions in rearrest, p < .04). Findings show some beneficial effects of adding treatment components oriented toward women’s needs. Significant questions remain, particularly around PTSD and whether it should be targeted to improve substance use outcomes for women.
Keywords
Standard substance abuse treatment programs in the community typically treat both men and women together, without much variance in services with regard to gender (Grella, Polinsky, Hser, & Perry, 1999; Oser, Knudsen, Staton-Tindall, & Leukefeld, 2009). Yet a substantial body of literature has shown that the treatment needs of women are quite different and more complex than those of men (Binswanger et al., 2010; Bloom, 1999; Bloom, Owen, & Covington, 2003, 2004; Greenfield, Back, Lawson, & Brady, 2010; Grella & Joshi, 1999; Messina, Wish, & Nemes, 2000; Tuchman, 2010). Women offenders are significantly more likely than men to have coexisting psychiatric disorders, parental stress, housing issues, and extensive histories of sexual and physical abuse (Kelly et al., 2009; Langan & Pelissier, 2001; Messina et al., 2008; Messina, Burdon, & Prendergast, 2003; Messina, Grella, Burdon, & Prendergast, 2007). Additionally, by the time women come into the criminal justice system, their drug abuse issues and needs are often more severe than those of their male counterparts (e.g., they are using multiple drugs on a daily basis and are more likely to be injecting drugs; Messina et al., 2003; Tuchman, 2010). Although some research suggests that many of these issues are stronger predictors for criminal activity among women than among men (McClellan, Farabee, & Couch, 1997; Van Voorhis, Wright, Salisbury, & Bauman, 2010), other findings suggest that there are very few or no gender differences in the predictors for criminal offending specifically (Makarios, Steiner, & Travis, 2010; Rettinger & Andrews, 2010).
A number of studies have shown that men and women have different pathways to crime and addiction (Pollock, 2002; Wasilow-Mueller & Erickson, 2001), continue to use drugs for different reasons (Covington & Surrey, 1997), enter and remain in treatment for different reasons (Grella & Joshi, 1999), and have a greater unmet need for treatment and therapy (Holloway & Bennett, 2007; Palm, 2007). Women’s patterns of addiction have been described as more socially embedded than men’s and primarily revolve around interpersonal relationships (Bloom et al., 2004). Additionally, economic dependence on a partner increases the risk of intimate partner violence (Engstrom, El-Bassel, Go, & Gilbert, 2008). Women offenders are typically impoverished members of ethnic minorities with inadequate transportation and resources, factors that limit their access to community-based health systems (Staton, Leukefeld, & Webster, 2003). Women also report more shame about their drug use and criminal activity than men, which often creates an additional barrier to their obtaining treatment (Palm, 2007).
The consistent findings regarding the complexity of women’s needs have led many researchers, theorists, and clinicians to propose gender-responsive (GR) treatment for women as a more appropriate and effective way to facilitate their recovery. Bloom et al. (2004) define this as “creating an environment through site selection, staff selection, program development, content, and material that reflects an understanding of the realities of the lives of women and that addresses and responds to their strengths and challenges” (p. 42). However, services specifically for women are minimally available. A national survey of substance abuse treatment facilities surveyed 13,371 facilities. Only 33% of those offered special programs or groups for adult women, 14% offered services for pregnant or postpartum women, 9% offered child care, and 4% offered residential beds for children (Substance Abuse and Mental Health Administration, 2005).
Some evidence indicates that women are less likely to drop out of specialized programs that take into account their specific treatment needs (Greenfield et al., 2007; Grella, 1999, 2008). Duration of treatment has been shown to be consistently associated with successful outcomes (DeLeon, 2000; Simpson, 1981), especially for women (Messina et al., 2000). A large-scale comparison study of 4,117 women in GR residential treatment and mixed-gender (MG) residential treatment found that women were twice as likely to complete the specialized GR programs than the MG programs (Grella, 1999) and that longer retention rates were strongly associated with high levels of posttreatment abstinence (Grella, Joshi, & Hser, 2000). Other studies have noted the importance of social supports and relationships for women offenders (Wisdom, Hoffman, Rechberger, Seim, & Owens, 2009), indicating that facilitating the relational strengths of women can help to keep them in treatment longer.
Outcomes of Women in GR Versus MG Treatment Programs
Prendergast, Messina, Hall, and Warda (2011) assessed the relative effectiveness of gender-specific outpatient treatment programs compared to MG outpatient programs (N = 291) for women who were predominantly referred to treatment via the criminal justice system. 1 Baseline pretreatment interviews and 1-year follow-up interviews were completed (89% follow-up rate). Propensity scores were calculated to control for group differences. Logistic regression and generalized estimating equation analysis were used to examine four outcomes: drug and alcohol use, criminal activity, arrests, and employment. Women in the gender-specific treatment reported significantly less substance use and criminal activity than did the women in MG treatment. But both groups showed improvement with regard to arrest and employment status at follow-up.
Another study examined the long-term outcomes of women who were pregnant or parenting at admission to gender-specific (n = 500) versus MG (a matched sample of 500) substance abuse programs (Hser, Evans, Huang, & Messina, 2011). Administrative records on arrests, incarcerations, mental health services use, and drug treatment participation were collected, covering 3 years preadmission and 8 years postadmission. Women treated in gender-specific programs had lower levels of arrest, mental health services use rates, and drug treatment participation during the 1st year after drug treatment. Gender-specific program participants also had lower incarceration rates during the 3rd year after treatment. The study findings suggest a positive short-term impact of gender-specific versus MG programs with regard to arrest and mental health service use. The long-term gain was shown in the reductions in posttreatment incarceration.
Evidence from Randomized Controlled Studies
The studies reviewed above outline outcomes for women participating in gender-specific programs, but such programs do not necessarily incorporate GR elements of treatment for women. A few controlled studies comparing women in MG versus GR treatment programs are available. Dahlgren and Willander (1989) randomly assigned 200 alcohol-dependent women to GR or MG outpatient programs. At a 2-year follow-up, the GR treatment participants showed significantly greater retention in treatment, greater decreases in alcohol consumption, and improved social adjustment (e.g., employment, improved mother–child relationship) compared to those in the MG programs. However, since the women in the GR treatment program were in treatment longer, it is difficult to determine whether the differences in outcome were attributable to the GR treatment elements or to the longer time in treatment. The second study also randomized alcohol-dependent women to GR or MG outpatient treatment programs. This study found no significant differences in psychological improvement or posttreatment substance use between women in the MG or GR treatment programs (Kaskutas, Zhang, French, & Witbrodt, 2005).
In an exploratory pilot study (Greenfield et al., 2008), women with high severity of psychiatric symptoms made greater reductions in substance use at the end of 12 weeks of group therapy treatment (implementing a 12-session manualized Women’s Recovery Group Model) when they were randomly assigned to GR treatment as opposed to MG treatment. Substance abuse treatment outcomes for women enrolled in the GR group continued to improve across the 6-month posttreatment follow-up compared with those enrolled in the MG group. ESes were medium to large in spite of the very small sample size (7 women were randomized to the MG group vs. 29 to the GR group).
A more comprehensive experimental pilot study compared postrelease outcomes for 115 women who participated in GR treatment while in prison. Women were randomized to a GR program implementing Helping Women Recover and Beyond Trauma or a generic prison-based program. Results indicate that both groups improved in psychological well-being at the 6-month follow-up; however, GR participants had significantly greater reductions in drug use, were more likely to remain in residential aftercare treatment (2.6 months vs. 1.8 months), and were less likely to have been reincarcerated within 12 months after parole (31% vs. 45%, respectively; a 67% reduction in odds for the experimental group; Messina, Grella, Cartier, & Torres, 2010).
Meta-Analysis of Women’s Treatment
Orwin, Francisco, and Bernichon (2001) conducted the first formal quantitative synthesis of the available outcome studies on women’s treatment. The authors used the standardized mean difference, d, to combine effect sizes (ESes) across the studies examined. Four studies were included in the average ES of GR treatment programs versus MG treatment programs. These studies contrasted six outcome domains: alcohol use (ES = .15), drug use (ES = .04), psychiatric symptoms (ES = .30), psychological well-being (ES = .06), attitudes and beliefs (ES = .14), and criminal behavior (ES = .16). One ES exceeded the small threshold: reduced psychiatric problems. However, each of the six mean ESes was positive, indicating better outcomes for the GR participants. Findings should be interpreted with caution, given the limited number of studies available and eligible for the meta-analysis.
Although gender-specific or GR treatment has not been consistently shown to be more effective than MG treatment, some evidence indicates that specialized treatment programs increase retention for women. Moreover, greater effectiveness has been demonstrated by treatment programs that address problems and issues common among substance-abusing women, such as the need for child care, services for women who are pregnant or postpartum, or services for women with histories of trauma and domestic violence. Improved outcomes have also been found for women involved in the criminal justice system. In sum, some studies have shown a positive impact from services that are designed to meet the needs of substance-abusing women. However, rigorous empirical assessment of the effectiveness of GR programs compared to traditional programs or MG programs is limited. It is vitally important to gain insight from empirical evidence to determine the types of services, settings, and approaches that are optimal to enhance outcomes for women offenders.
The current study randomized women participating in four drug court treatment programs to receive a standard MG drug court treatment program model or a GR treatment model. Based on the review of the available literature, the following hypotheses were proposed:
Hypothesis 1: Women in the GR treatment condition will have more positive in-treatment performance than will the women in the MG treatment condition.
Hypothesis 2: Women in the GR treatment condition will be less likely to report posttreatment drug use than will women in the MG treatment condition.
Hypothesis 3: Women in the GR treatment condition will have reduced trauma symptomology and be more likely to have improved psychological functioning, compared with women in the MG treatment condition.
Hypothesis 4: Women in the GR treatment condition will have reduced recidivism, compared with women in the MG treatment condition.
Method
Study Design
The data for this study were collected between 2007 and 2010 as part of an experimental pilot study. There are four drug court programs throughout San Diego County, California, that provide women offenders with approximately 18 months of MG outpatient substance abuse treatment. In each of the four program sites, a new program was created to be the experimental GR treatment program. A total of 150 women entering drug court treatment in San Diego County who agreed to participate in the study were randomly assigned to the GR treatment program or the standard MG program. The GR treatment program enhanced the usual drug court standards of care by becoming a woman-only program, facilitated by women only, and using GR treatment curricula (i.e., Helping Women Recover and Beyond Trauma). The comparison programs continued to deliver regular drug court standards of care.
All study procedures were reviewed and approved by the University of California, Los Angeles (UCLA), General Campus Institutional Review Board. All of the women approached agreed to participate in the study and provided written informed consent prior to being interviewed. Participants were paid $15 for a baseline interview and $10 for a follow-up interview via gift cards. Randomization took place at intake at the respective programs. The drug court program managers were provided with sealed envelopes with a randomly generated assigned program (GR or MG) for admission of new clients.
Drug court program standards in San Diego, California
The drug court model provides early assessment of drug abuse disorders and mandates eligible offenders into community-based treatment. Drug courts combine intensive supervision, mandatory drug testing, escalating sanctions, and treatment to break the cycle of addiction and criminal activity in which many repeat offenders are caught. The treatment components for each of the county’s four drug court programs are contracted to one substance abuse treatment provider, Mental Health Systems. The standards and practices for drug court programs in San Diego County are intended to be a guide for required minimum program components and operational procedures and principles. Drug court treatment programs are required to provide individual and group counseling (with a strong emphasis on vocational or educational counseling and referral), 12-step meetings, recreational and mutual self-help group discussions, and random urine testing throughout the five phases of treatment. The MG drug court programs are typical outpatient programs in which participants spend 2 to 3 hr, 5 days a week, in group counseling, with one-on-one counseling given on an as-needed basis. The contracted drug court treatment provider may also provide additional services beyond the minimum requirements, including relapse prevention, family planning, anger management, HIV-AIDS education, and referrals for psychological, medical, and/or legal services.
Typically, gender issues and trauma histories were not addressed in these MG drug court programs. Additionally, both men and women were employed as treatment staff to facilitate the groups and counsel the women.
GR treatment programs
The GR treatment programs included the components listed above for the MG programs but with a focus on issues specific to women’s recovery in a setting compatible with women’s interactional styles. The GR treatment program was a unique environment in that it was modified to be a gender-specific environment, with only female treatment staff facilitating the groups and counseling the women. The female counseling staff were specially trained for this study by Dr. Stephanie Covington, the developer of the curricula. Dr. Covington provided 2 days (5 to 6 hr each day) of training for the GR treatment program staff. Training was implemented early in the study to ensure that the new procedures and the GR treatment program were fully operational prior to subject recruitment. Additionally, an on-site clinical supervisor and expert in the Covington curricula was hired to provide technical assistance, clinical supervision, and feedback to the GR treatment staff to enhance fidelity to the curricula. In each of the four sites, the GR and MG programs maintained separate counseling staff, separate treatment rooms, and separate programming schedules to minimize any contamination between treatment conditions.
The GR treatment model encompassed two manualized curricula, Helping Women Recover and Beyond Trauma, designed to be relevant to the needs of drug-dependent women under criminal justice supervision. Each provides a facilitator’s guide and a participant’s workbook. Both curricula use cognitive-behavioral approaches, mindfulness meditation, experiential therapies (guided imagery, visualization, art therapy, movement), and psychoeducational, relational, and expressive arts techniques.
Helping Women Recover (Covington, 2008) is a 17-session program organized into four modules:
Self module: Women discover what the “self” is; learn that addiction can be understood as a disorder of the self; learn the sources of self-esteem; consider the effects of sexism, racism, and stigma on a sense of self; and learn that recovery includes the growth of the self.
Relationship module: Women explore their roles in their families of origin, discuss myths and realities about motherhood and their relationships with their mothers, review relationship histories, and consider how they can build healthy support systems.
Sexuality module: Women explore the connections between addiction and sexuality and discuss body image, sexual identity, sexual abuse, and the fear of sex when sober.
Spirituality module: Women are introduced to the concepts of spirituality, prayer, and meditation. Spirituality deals with transformation, connection, meaning, and wholeness.
Beyond Trauma (Covington, 2003) consists of 11 sessions focused on three areas: teaching women what trauma and abuse are, helping them to understand typical reactions to trauma and abuse, and developing coping skills. The foundation of this material is the work of Judith Herman and several other trauma theorists (Covington, 2003). With this curriculum, women begin a process of understanding what has occurred in their past (i.e., sexual or physical abuse or other victimization) that has been traumatizing. They explore how this abuse has affected their lives and learn coping mechanisms while focusing on personal safety. This curriculum uses a strengths-based approach.
Additionally, the GR treatment program provided the participants with Covington’s A Woman’s Way Through the Twelve Steps Workbook (2000) and Women in Recovery: Understanding Addiction (2002). A Woman’s Way Through the Twelve Steps illuminates how women understand the 12 steps of Alcoholics Anonymous and offers stories of how they have traveled through the steps and discovered what works for them. Women in Recovery is an interactive workbook intended for use as an educational journal by women in substance abuse treatment programs. The material is based on the most up-to-date information about the impact of substance-use disorders on women’s health, families, and relationships. It uses the research-based process of Interactive Journaling®.
Fidelity
Fidelity to program curricula and to the creation of a GR and trauma-informed environment was assessed via direct observations and multiple site visits by the evaluation staff. Additional data were collected on each site regarding staff turnover and trained staff on site. Initially, programs were provided with on-site technical assistance by an expert in Helping Women Recover and Beyond Trauma. As facilitators’ expertise and program procedures were assessed, assistance was provided to improve implementation as necessary. However, it was concluded that programs varied in their fidelity to the treatment protocol initially and continually. One site was conducting the GR treatment group with very high fidelity and continued to do so throughout the course of the study. Another site was assessed as having moderate fidelity initially and then high fidelity after on-site assistance and guidance. The two remaining sites were implementing the GR treatment groups with low fidelity but improved to moderate fidelity after assistance was provided.
Data Collection
All participants were interviewed within the first 30 days after entry into the drug court programs (baseline) by UCLA research assistants. Baseline interviews focused on capturing behaviors 30 days and also 4 months prior to the arrest that led to court-mandated drug court treatment. Recruitment began in February 2007 and ended in March 2009, resulting in a total sample of 150 participants (85 GR, 65 MG). Follow-up interviewing was designed to take place 18 months after treatment entry. By the time of the final follow-up interview, 1 participant was found to be deceased and 23 participants remained in treatment. Thus, they were removed from the potential follow-up sample. Out of the 126 remaining participants, 103 were located (82%) and 94 completed the follow-up interview (77% of the GR treatment group and 71% of the MG group). 2 The average time to complete the postbaseline follow-up interview was 22.2 (SD = 6.9) months for the GR treatment group and 20.6 (SD = 5.7) months for the MG group. The drug court treatment programs provided the treatment admission and discharge data and court progress data to UCLA Integrated Substance Abuse Programs.
Eligibility
Women offenders admitted into each of the participating drug court programs during the recruitment period were eligible to participate in the study. Defendants are eligible for drug court if they are at least 18 years old; have had no more than three prior nonviolent, nondrug felony convictions; and do not have a current charge of driving under the influence of alcohol or drugs or a charge of sale or transportation of drugs.
Participant Population
T test was used to compare the GR treatment program and the MG treatment program for characteristics represented by a single continuous variable. For categorical and binary variables, chi-square analysis was used. Participants were predominantly either White (58%) or Hispanic (22%), and 47% had never been married at the time of program admission (36% reported being divorced, separated, or widowed). On average, participants were approximately 36 years old (SD = 8.9) with 12 years (SD = 1.8) of completed education. A majority of the women were either not in the labor force or unemployed (74%) prior to program entry. Fifty-five percent of the women reported histories of depression, and 31% met the criteria for a diagnosis of posttraumatic stress disorder (PTSD) via the Post Traumatic Stress Diagnostic Scale (Foa, 1997). (The essential feature of PTSD is the development of characteristic symptoms following exposure to an extreme traumatic stressor. The person’s response to the event must involve intense fear, helplessness, or horror. The characteristic symptoms resulting from the traumatic event include persistent reexperiencing of the traumatic event, persistent avoidance of stimuli associated with the trauma, and persistent symptoms of increased arousal. The full symptom picture must be present for more than 1 month, and the disturbance must cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.) Methamphetamine was the primary drug problem (71%). There were significant differences in primary drug categories reported between the two groups, as more of the women in the GR treatment group reported cocaine or crack use and much less opiate use compared with the MG group. A majority of the women also reported histories of sexual abuse (55%) and physical abuse (37%) as well as substantial histories of other trauma. No other significant differences were found in background characteristics between the two randomized groups (see Tables 1 and 2).
Sample Characteristics at Treatment Admission, by Program
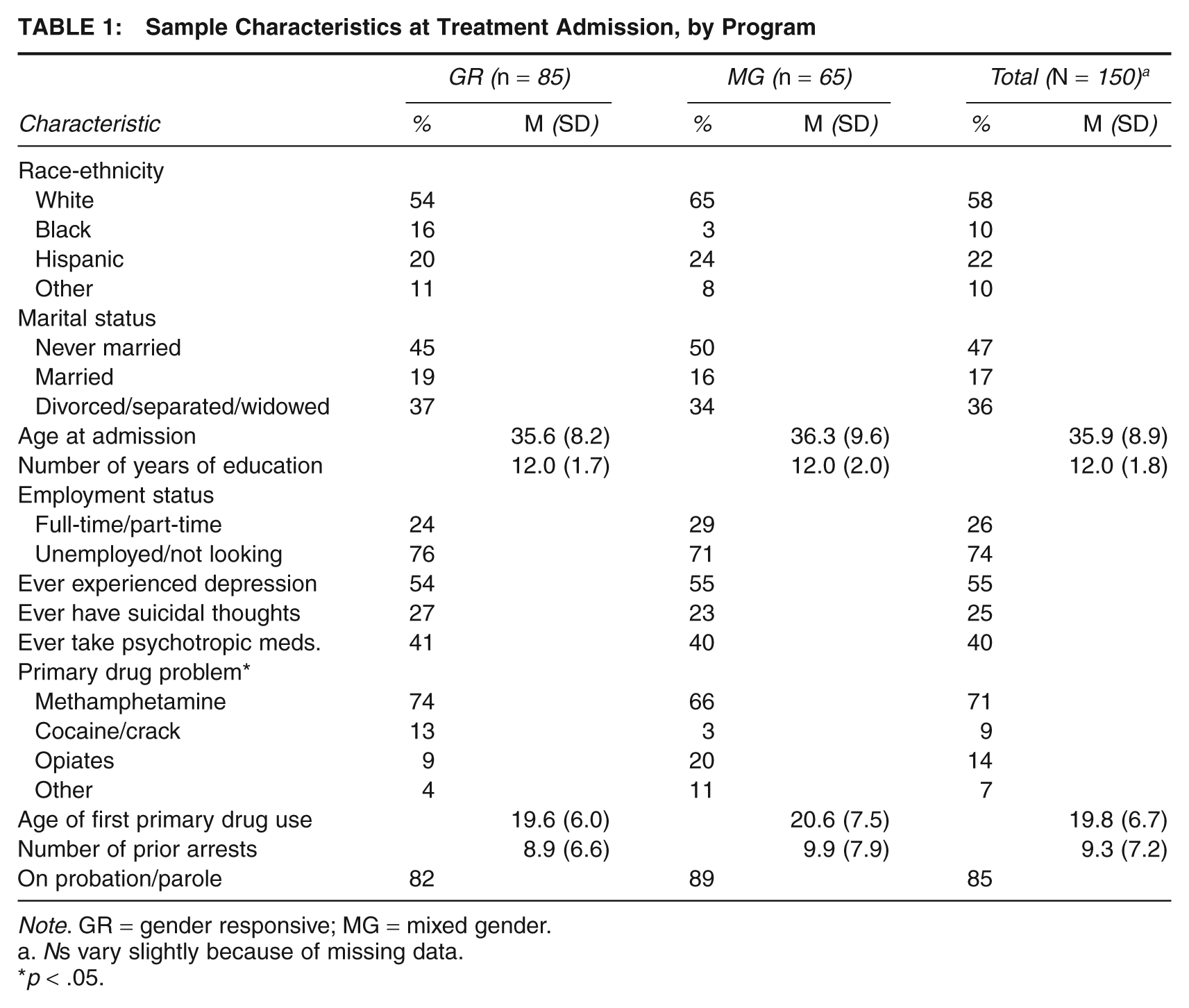
Note. GR = gender responsive; MG = mixed gender.
Ns vary slightly because of missing data.
p < .05.
Prevalence of Traumatic Events and Diagnosis of PTSD (in percentages)
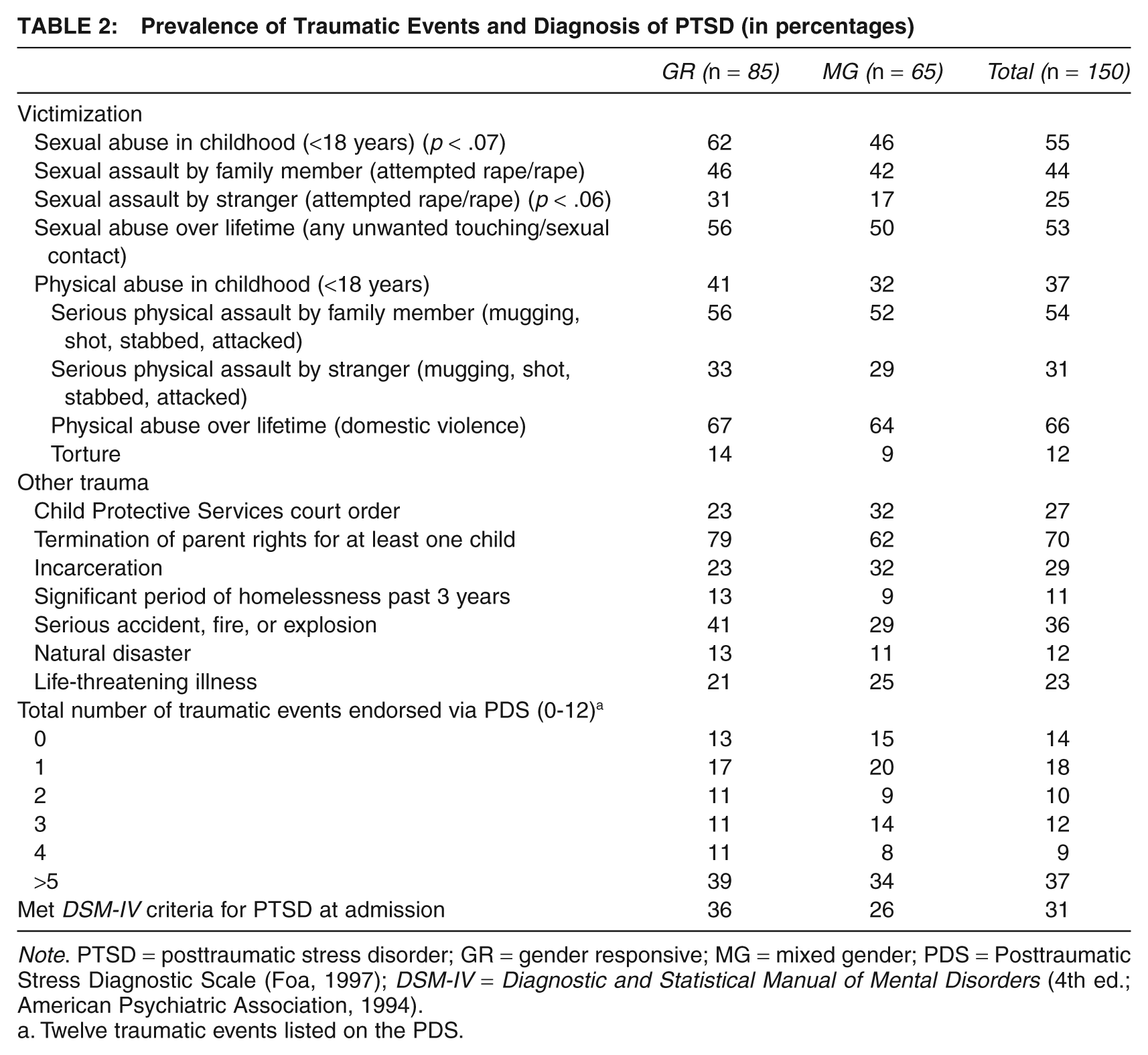
Note. PTSD = posttraumatic stress disorder; GR = gender responsive; MG = mixed gender; PDS = Posttraumatic Stress Diagnostic Scale (Foa, 1997); DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994).
Twelve traumatic events listed on the PDS.
There were no significant differences with regard to motivation and readiness for treatment scores between treatment groups. Scores ranged from 1 to 3, with higher scores indicating more motivation for treatment. Both groups appeared to have a strong desire for help (2.92, SD = 0.21) and acceptance for treatment (2.76, SD = 0.32). However, both groups scored much lower with regard to their problem recognition (1.58, SD = 0.28).
Data Sources and Outcome Measures
Data were collected on specific outcome measures, including treatment retention, drug use, psychological well-being and self-efficacy, and recidivism. The measures used to describe the study participants and to test hypotheses were collected from standardized instruments, such as the Addiction Severity Index–Lite (ASI; McLellan, Alterman, Cacciola, Metzger, & O’Brien, 1992) and the Posttraumatic Stress Diagnostic Scale (PDS; Foa, 1997). 3 The ASI has excellent interrater and test–retest reliability as well as discriminant and concurrent validity (McLellan et al., 1992).
The PDS has shown a .70 test–retest reliability (Foa, Cashman, Jaycox, & Perry, 1997). The PDS follows the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for a diagnosis of PTSD, requiring exposure to a traumatic event (must cause fear of injury and/or helplessness, Items 15 through 20), reexperiencing symptoms (one or more of Items 21 through 25), avoidance symptoms (three or more of Items 26 through 32), arousal symptoms (two or more of Items 33 through 37), symptom duration of 1 month or more (Item 38), and distress or impairment in functioning (one or more of Items 40 through 48).
Drug court treatment intake procedures and surveys, the Motivation and Readiness for Treatment Scale (Knight, Holcom, & Simpson, 1994), the Self Efficacy Scale (Annis & Graham, 1988), and administrative records data from the drug courts and the treatment providers (admission and discharge dates, completion status, sanctions, aftercare participation, criminal justice arrest records) were also used to test hypotheses.
Data Analysis
The primary analyses tested the study hypotheses by comparing participants in the GR treatment group with those in the standard MG group using an intent-to-treat design. Analyses included all participants assigned to each group by keeping each participant in her originally assigned group. This intent-to-treat approach capitalizes on the strengths of the random assignment design of the study, increases generalizability and validity of study results, and avoids possible selection bias (Nich & Carroll, 2002). 4 Additionally, all participants were included in the analyses, regardless of their completion of the treatment program. Although the hypotheses are expressed as one tailed, we recognize that outcomes may occur that were not in the direction expected. Therefore, all hypotheses were tested at the .05 significance level using a two-tailed test. T test was used to compare the GR treatment program and the MG program for outcomes represented by a single continuous variable. For categorical and binary outcome variables, chi-square analysis was used. A generalized estimating equations (GEE) model for repeated measures approach was used to consider changes over time (e.g., change in PTSD or PTSD symptomology and ASI composite score changes from baseline to follow-up). GEE, introduced by Liang and Zeger (1986), is used to analyze repeated-measures data, taking into account the possibility of correlated data. This method can also accommodate a wide variety of distributions, such as normal, binomial, and gamma, and it provides the option of including covariates in the model. The PTSD data reflected a binomial distribution.
Also, multivariate analyses were run to assess reductions in posttreatment arrest. We conducted logistic regression analyses assessing the relationship between treatment group and any arrest within 2 years of baseline while controlling for primary drug problem, race-ethnicity, and PTSD.
Results
Client-level background characteristics for the GR treatment and standard MG treatment groups are shown in Tables 1 and 2. With the exception of primary drug reported, there were no statistically significant differences between the two groups prior to their drug court involvement. Although the baseline comparisons revealed only one significant difference at the conventional p < .05 alpha level (primary drug problem), it was apparent that there were some “practical differences” with regard to race-ethnicity and histories of trauma between the two groups. Results indicated approximately a 10-percentage-point or greater difference among the indicators within these variables. A greater proportion of women from the GR treatment program were Black compared to the MG treatment program women (16% vs. 3%). Both groups reported high percentages of trauma during childhood and adulthood; however, the GR treatment group once again had higher percentages among several categories of traumatic experiences (e.g., childhood sexual abuse, sexual assault by a stranger, termination of parental rights, and serious accident). Cumulatively, the women endorsed family abuse as the most traumatic event experienced (24%, sexual abuse in childhood by a family member; 24%, physical abuse in childhood by a family member). Sixty-seven percent of the women reported that the most traumatic event occurred during childhood or more than 5 years ago, and 68% reported being extremely bothered by the traumatic event within the past 30 days. Thirty-seven percent of the women reported experiencing five or more traumatic events as listed on the PDS (see Table 2). The women in the GR treatment program appeared to meet the previously outlined PTSD criteria at a higher rate than those in the MG group (36% vs. 26%). These practical differences may indicate that women in the GR treatment program were at a substantial disadvantage at program admission than women in the MG program.
In-Treatment Performance
Table 3 displays the results from the in-treatment data collection in support of Hypothesis 1. Approximately 58% of both groups completed the drug court program in approximately 15 to 24 months of outpatient treatment (15% were still in treatment at the time of the program records data collection). Removing those who remained in and/or were transferred out of treatment, the graduation rate was 69% overall. Treatment completion was not included in our main hypotheses because drug court participants are extensively monitored; thus, differences in completion rates between the GR and MG treatment groups were likely to be minimal.
In-Treatment Performance
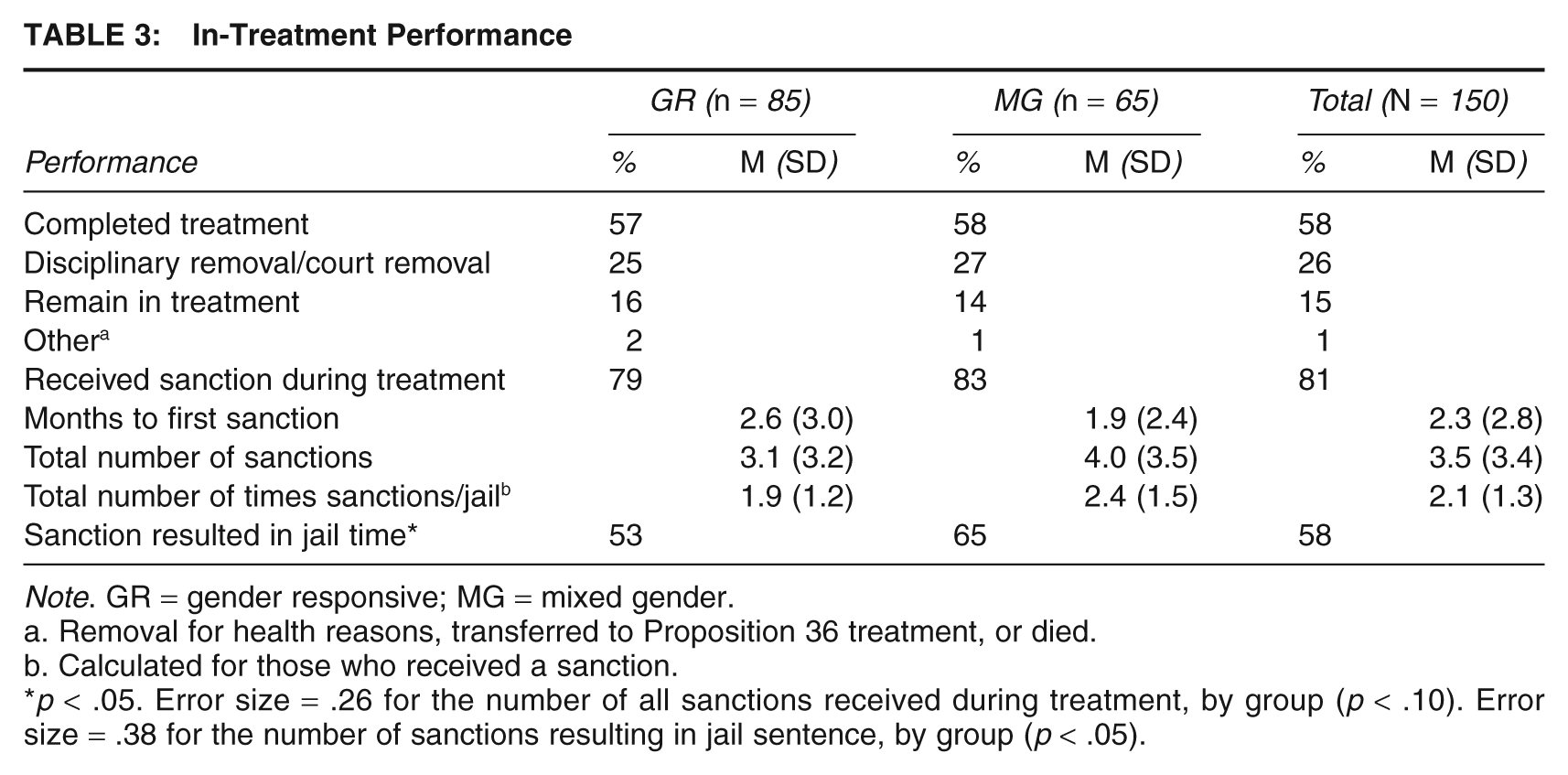
Note. GR = gender responsive; MG = mixed gender.
Removal for health reasons, transferred to Proposition 36 treatment, or died.
Calculated for those who received a sanction.
p < .05. Error size = .26 for the number of all sanctions received during treatment, by group (p < .10). Error size = .38 for the number of sanctions resulting in jail sentence, by group (p < .05).
Graduated sanctions are used within the drug court system as a way to encourage program participation and to enhance program completion. As rules are violated in treatment, participants are given a variety of graduating sanctions in response to their misconduct. Seventy-nine percent of the women in the GR treatment group and 83% of the women in the MG group received a sanction for any reason during the 15 to 24 months of treatment. There were no differences in the number of sanctions received in total during the course of treatment between the groups (GR, M = 3.1, SD = 3.2; MG, M = 4.0, SD = 3.5; p < .10); however, GR treatment participants were less likely than those in the MG group to receive sanctions as treatment progressed. During the first 6 months of treatment, drug court participants received sanctions at equal rates; however, during the second and most intensive phase of treatment, the GR treatment group received significantly fewer disciplinary sanctions (GR, M = 0.65, SD = 1.2; MG, M = 1.2, SD = 1.8; p < .03) compared with those in the MG group.
The most serious sanction is for a client to be remanded to jail for a period of time. The number of times a sanction resulted in detention in jail was also significantly different between the two groups, with GR treatment participants less likely to be remanded to jail (GR, M = 1.9, SD = 1.2; MG, M = 2.4, SD = 1.5; p ≤ .05). Violations of court-mandated attendance or other program rules can further result in early dismissal from the program. Data collected from the respective drug court programs indicate that the women in the GR treatment groups were significantly less likely to be terminated from treatment for unsatisfactory progress during the first 6 months (13% vs. 16%, p < .05). 5 The findings regarding in-treatment performance indicate support for our first hypothesis.
Reductions in Drug Use
ASI composite drug score change from baseline to follow-up was explored with regard to Hypothesis 2. This hypothesis was not supported, but mean change over time between groups approached significance in the hypothesized direction, p < .06. Both the GR and the MG groups had significant and improved drug and alcohol composite scores from baseline to follow-up.
Reductions in Trauma Symptomology and Improved Psychological Functioning
Hypothesis 3 was explored via change in PTSD symptomology and overall psychological functioning over time. Thirty-one percent of the total sample met the PTSD criteria at baseline, as assessed by the PDS following DSM-IV PTSD criteria (American Psychiatric Association, 1994). At follow-up, only 13% of the total sample assessed met the full criteria for current PTSD (36% at baseline reduced to 9% of the GR group; 26% at baseline reduced to 18% of the MG group). As only 8 women met full criteria for PTSD at follow-up, chi-square significance tests may not be generalizable. However, the reduction in a current PTSD diagnosis for the GR group (see Table 4) was twice that of the MG group, and the GEE model of change in diagnosis over time approached significance (p < .07).
Generalized Estimating Equations Model for Posttraumatic Stress Disorder
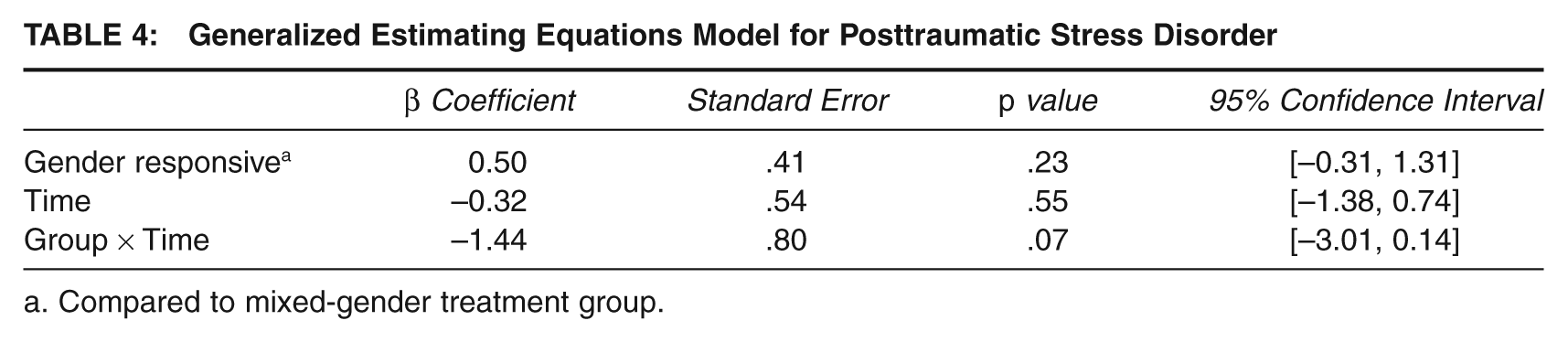
Compared to mixed-gender treatment group.
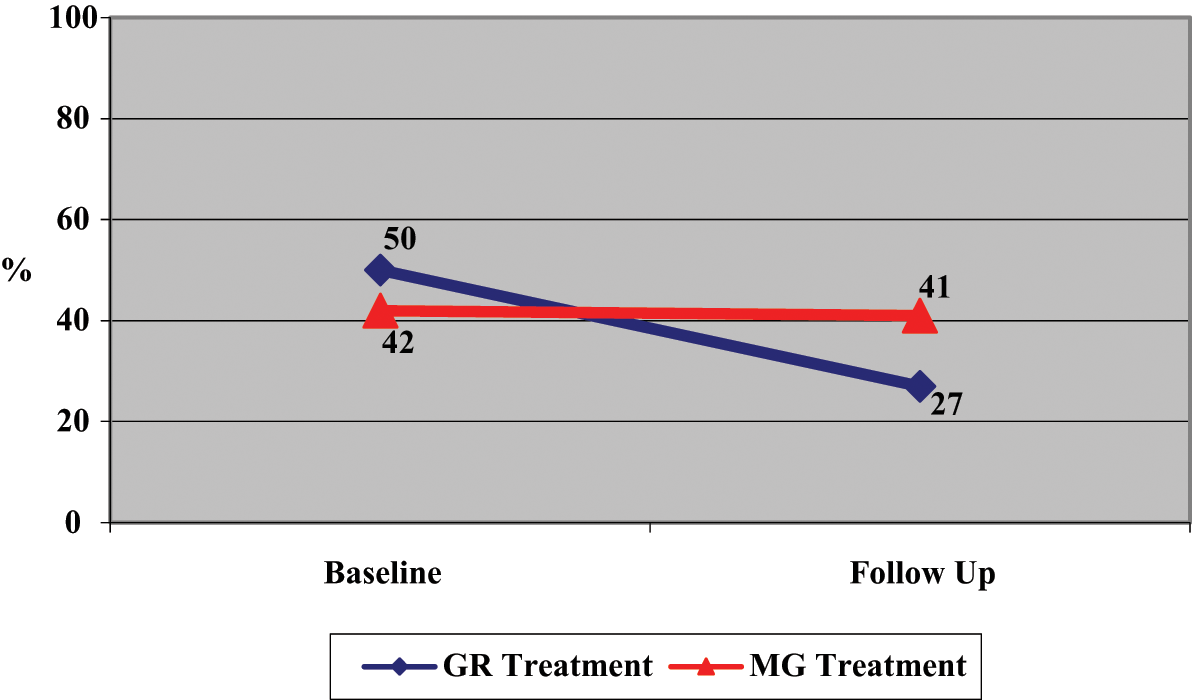
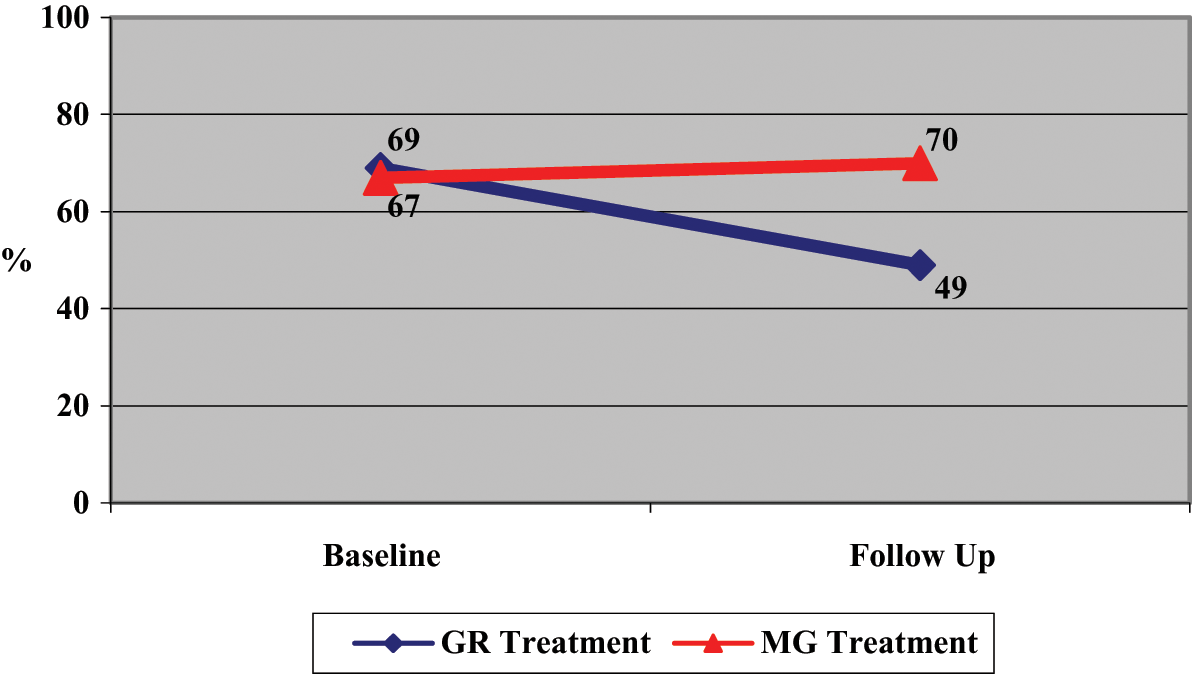
When we explored the change in endorsement of specific symptoms for the total sample (i.e., reexperience, avoidance, arousal, functioning), we found that the GR group consistently reported reduced symptoms for each symptom measured. In contrast, the women in the MG groups reported an increase in reexperiencing their traumatic event from baseline to follow-up and no change in their other symptoms (see Figures 1 through 4). These comparisons approached significance. As there was reduction in sample size for those who met the criteria for a specific symptom, there was also a reduction in power. ESes were calculated to examine the between-group differences at follow-up by symptom (reexperience, ES = .31; avoidance, ES = .31; arousal, ES = .19; functioning, ES = .43). Three of the four symptom ESes between groups resulted in a medium ES. An index of all possible affirming symptom responses was also calculated at baseline and follow-up (not including the number of actual traumatic events). The GR group endorsed on average 35.6 (SD = 15.9) symptom criteria at baseline and 29.3 (SD = 14.8) at follow-up (mean change of 6.3; ES = .40). The MG group endorsed on average 35.0 (SD = 15.0) symptom criteria at baseline and 32.7 (SD = 18.6) at follow-up (mean change of 2.3; ES = .15).

Reduction in Posttraumatic Stress Disorder Reexperience Symptoms by Time Point, by Group
Reduction in Posttraumatic Stress Disorder Avoidance Symptoms by Time Point, by Group

Reduction in Posttraumatic Stress Disorder Arousal Symptoms by Time Point, by Group
Reduction in Posttraumatic Stress Disorder Poor Functioning Symptoms by Time Point, by Group
The ASI psychological composite score and self-efficacy changes over time were further analyzed in exploration of Hypothesis 3. Both groups’ mean composite scores significantly improved from baseline to follow-up with regard to their ASI psychological composite score and self-efficacy score. Thus Hypothesis 3 was partially supported, as the GR group showed significant reductions in PTSD symptomology compared with those in the MG group, but both groups showed improved general psychological functioning over time.
Reductions in Arrest
Department of Justice arrest records were available and analyzed for 138 participants in exploration of Hypothesis 4. There were no differences between the two groups’ postbaseline arrest rates. Thirty-three percent of the total sample were arrested at least once during their posttreatment follow-up time period (i.e., within 2 years after treatment entry). Multivariate analyses controlling for treatment group, race, primary drug problem, and presence of PTSD at baseline was run exploring rearrest. Logistic regression analyses indicated that a diagnosis of PTSD at baseline was the only significant predictor of rearrest, indicating that those who met criteria for PTSD at baseline were less likely to be arrested compared to those who did not met criteria for PTSD (β = .51, N = 108, df = 1, p < .04).
Discussion
The greater severity of women’s drug abuse, past trauma, and physical and mental health problems compared with their male counterparts has led many researchers, clinicians, and theorists to advocate for GR treatment for women as a more effective way to facilitate their recovery. However, there has been a lack of rigorous empirical studies to support these beliefs, particularly experimental studies that apply rigorous controls. For practical and ethical reasons, random assignment of offenders to either a treatment or control group is rare in evaluations of treatment programs. A major strength of our design was the use of random assignment, allowing all drug court participants to receive the minimal standard treatment of care, with some participants receiving enhanced treatment designed specifically for women offenders (i.e., Helping Women Recover and Beyond Trauma). This rigorous design enhances the strength of our findings by eliminating potential confounds attributable to self-selection into groups.
Predominantly, the findings were in the hypothesized direction, with GR model participants showing more success during treatment and at the follow-up compared to the standard MG treatment group of women. Comparisons between the two groups indicated that GR treatment participants had better in-treatment performance, positive trends indicating reductions in PTSD symptomology, and more positive treatment perceptions (reported via focus groups). However, both groups of women improved in their self-reported psychological well-being and self-efficacy across the study time period, and both groups reported reductions in posttreatment drug use (this comparison approached significance, p < .06) and had reductions in posttreatment arrest. Although some of the indicators did not reach statistically significant differences, the percentages, means, and ESes reported were in the expected direction. In addition, the finding that the women in the GR treatment group reported greater exposure to sexual abuse and childhood trauma than those in the MG group suggests that they could have been expected to have more difficulty adjusting to treatment initially (e.g., because of issues of fear and mistrust).
The trends indicating that the GR participants had reductions in their PTSD symptomology is an important area of research, as there is currently great debate over addressing trauma issues during substance abuse treatment. Although many of the staff initially reported having inadequate skills to deal with the severity of the traumatic experiences of the clients, they were dedicated to learning a curriculum that could help them navigate such issues. Staff also had very positive attitudes toward integrating trauma-informed services into their programs and to have training and a facilitator’s guide to aid them. Additionally, the GR participants expressed more satisfaction with their groups and were very engaged in their treatment experience. The GR participants also expressed gratitude for having the chance to safely discuss their histories of trauma and abuse with other women who share in their experiences, which was something that could not be done in the MG group (Calhoun, Messina, Taube, Bond, & Ordille, 2010).
A variety of studies have shown that women who complete drug court treatment are more likely to have reductions in drug use and criminal activity. These are widely accepted findings. Thus it is not surprising to find improvement in some measured outcomes for both treatment groups. However, the consistent literature outlining the extensive trauma histories of women as compared to men and the undeniable link between childhood trauma and adult addictive and criminal behaviors suggest that these issues need to be addressed safely and systematically for women to best meet their treatment needs. The diagnosis of PTSD at baseline was the primary predictor of reductions in posttreatment arrest. This finding could be an indication that women suffering from PTSD symptoms are responsive to, and can improve in, a therapeutic environment. It is possible that GR treatment can result in reduced trauma symptomology and thus create an opportunity for long-term well-being and stability.
Limitations
As this was a pilot study, our design was limited by time, budget, and sample size, but we were able to identify important findings and trends in posttreatment behavior and well-being. These findings lay the groundwork for a larger, more in-depth study in this area. We also found that the drug court programs varied in their fidelity to the treatment protocol. Without strong fidelity to program curricula, it is difficult to determine the full impact of the curricula. Our study included measures to assess staff performance and adherence of the newly integrated curriculum, and modifications were made to increase fidelity during the study. Also, the “usual-care” group was not a “no-treatment” group; thus, measured outcomes between groups were possibly minimized. The findings are strengthened by the rigorous design of the study, and thus, there is a reasonable probability that the differences we detected are relevant in guiding our recommendations to those making decisions regarding women under criminal justice supervision.
Recommendations
There are a number of implementation challenges when integrating GR treatment curricula within an existing program. Our extensive staff interviews resulted in many suggestions and solutions for integrating treatment. There is a need for ongoing staff training and monitoring of their adherence to the protocol. Direct observations from the evaluation team, the clinical director, and Dr. Covington revealed concerns with the fidelity of the implementation, and therefore, additional training and onsite technical assistance was provided. Low fidelity to the curricula in some of the programs may significantly affect any measured outcomes by reducing the potential aggregate strength (i.e., effect) of the intervention.
There is a need for further exploration with larger samples of women to determine whether findings can be replicated or whether trends can be substantiated with greater power. Experimental studies are needed to continue to address the gap in knowledge regarding drug abuse treatment for women offenders in general and by providing specific information on the types of services, settings, and approaches that should be emphasized when treating women. Given the aggregate impact of trauma represented in the lives of women offenders, the field will further benefit from research that takes into account how traumatic exposure influences their outcomes and that identifies effective services that moderate the negative impact of such histories. Future studies would also benefit from a quantitative fidelity measure for the specific curriculum being delivered.
Following from research indicating that the treatment needs of women are different from those of men, researchers and clinicians have argued that treatment programs for women should be designed to take their needs into account. Such programs tend to admit only women, often employ only women, and have a philosophy and activities that are based on a social, peer-based model that is responsive to their needs. Gender-specific programs are designed to address the needs of women and appear to have a positive effect on at least some important outcomes. But future studies are needed of programs that explicitly incorporate GR elements of treatment for women.
Footnotes
Authors’ Note:
This study was funded by the National Institute on Drug Abuse (NIDA Grant No. R01 DA22149-01). The findings and conclusions of this article are those of the authors and do not necessarily represent the official policies of the San Diego County Adult Drug Court Programs. The authors would like to thank Jerry Cartier, Stephanie Taube, Brittany Horth, Stephanie Torres, Claudia Gonzales, and Dave Bennett for their help with study coordination, data collection, data entry, and data building. We would also like to thank Kim Bond, president and CEO for Mental Health Systems; Alison Ordille; Patricia Lazalde; and the program directors and counseling staff for their cooperation with training, implementation, recruitment, randomization, and support of program data collection. We are grateful to the San Diego County Drug Court System judges and staff for their support and assistance on this project. We are also grateful to Stephanie Covington for her many hours of training and program site visits and Penny Philpot for her on-site facilitation with implementation of the curricula and clinical supervision. Finally, we wish to thank the participants who volunteered to be interviewed and to share their life experiences with us.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.