
Abstract
Contemporary social cognitive theories of aggression, such as the general aggression model (GAM), highlight the role of several key knowledge structures in aggressive behavior. There has been limited investigation of these structures in offender populations, however, meaning that their relevance to the rehabilitation of violent offenders cannot be adequately determined. In the present study, the role of three aggression-related knowledge structures—normative beliefs, behavioral scripts, and early maladaptive schema—along with trait anger, were examined with respect to the aggressive behavior of an offender sample. Normative beliefs and scripts were associated with aggression over and above the effect of anger, with these variables accounting for almost a quarter of the variance in participants’ aggression. These findings suggest that the knowledge structures described by the GAM concurrently increase aggression and underscore the need for more routine and systematic targeting of aggression-related cognitions in violent offenders.
Social cognition is the dominant theoretical perspective in the field of aggression, contending that learning, mental representation, and subsequent interpretation are important routes for the development of aggressiveness (Fiske, 2009). Accordingly, social cognitive theories emphasize the importance of various cognitive constructs (e.g., interpersonal knowledge, attitudes) that are proposed to underlie aggressive behavior. In particular, prevailing theories contend that aggression-prone individuals hold more entrenched aggression-related cognitions (Anderson & Bushman, 2002; Crick & Dodge, 1994; Huesmann, 1998). The most comprehensive social cognitive theory of aggression, the general aggression model (GAM; Anderson & Bushman, 2002), refers to these cognitions as “knowledge structures”: strongly interconnected concepts that represent prior knowledge about aggression, its attributes, and relations to other concepts (Huesmann, 1998). Various kinds of knowledge structure are considered to be important, including normative beliefs, aggressive scripts, and hostile world schemas (Anderson & Bushman, 2002; Anderson & Carnagey, 2004; Anderson & Huesmann, 2007). Although contemporary models are grounded in a substantial accumulation of experimental research, there has been relatively little empirical investigation of the content and structure of aggression-related cognitions (Collie, Vess, & Murdoch, 2007).
It is likely that the shortage of research in this area is attributable, in part, to the perceived difficulty in reliably assessing information about the nature of these knowledge structures. To date, most studies have focused on the acquisition and development of knowledge structures in children and adolescents (Huesmann & Guerra, 1997), and studies exploring their importance and operation in adults with established histories of aggression are scarce and fragmented. As a consequence, the cognitive features that are theoretically considered specific and fundamental to aggressive and violent behavior are not exhaustively targeted in violent offender treatment programs (Gilbert & Daffern, 2010). Therefore, although the GAM has much to offer in explicating aggressive behavior, the role of aggression-related knowledge structures requires empirical investigation and validation in violent offender populations.
In the present study, the importance of three main types of aggression-related knowledge structure described by the GAM, that is, normative beliefs supportive of aggression, aggressive scripts, and maladaptive cognitions, were investigated in relation to the aggressive behavior of a sample of offenders. By examining aggression-related beliefs, scripts, and maladaptive cognitions simultaneously, the study was novel in exploring how these structures were interrelated.
The GAM
The GAM (Anderson & Bushman, 2002; Anderson & Carnagey, 2004; Anderson, Gentile, & Buckley, 2007; DeWall & Anderson, 2011) integrates existing theoretical frameworks designed to account for the development and enactment of aggressive behavior. At its broadest level, the GAM contends that factors influencing aggression in the long term, such as personality characteristics, as well as those aspects that operate in the situation to prompt aggressive responses (e.g., provocation) are mediated by the internal states of cognition, affect, and arousal. These internal states provide the means by which aggression proceeds from the various person and situation inputs to a behavioral outcome. The GAM was recently extended to more severe forms of aggression, including intimate partner violence, with the implications for interventions for aggression also considered (DeWall, Anderson, & Bushman, 2011). The GAM has also influenced the development of I3 theory (Slotter & Finkel, 2011), a process-oriented model that seeks to understand the complex interplay between the various risk factors for aggression.
From the perspective of the GAM, more aggressive people are those with an inherent predisposition toward aggression, which is subsequently consolidated by life experiences that prepare them to behave aggressively across different situations. The role of learning is emphasized (Anderson et al., 2007), since it is responsible for the development of aggression-related knowledge structures that contain more extensive and developed normative beliefs, scripts, and affective states relating to aggression. These structures influence a person’s understanding and response to their social world and represent proximal factors that directly influence their likelihood of behaving aggressively. One of the main routes by which aggression-related knowledge structures operate, however, is via the impact of affective states, such as anger. Anger is variously understood to reduce inhibitions against acting aggressively, provide a justification for aggressive retaliation, interfere with higher-level cognitive processes regarding the appropriateness of aggressive acts, activate normative beliefs and scripts, and enable a person to maintain aggressive intentions over time (Anderson & Bushman, 2002). Anger has been frequently identified as an antecedent of aggression and violence in forensic (Cornell, Peterson, & Richards, 1999; Novaco & Taylor, 2004), clinical (McNeil, Eisner, & Binder, 2003; Posternak & Zimmerman, 2002), and nonclinical populations (Tafrate, Kassinove, & Dundin, 2002; Taft et al., 2006) but has yet to be examined in relation to aggression-related normative beliefs and scripts.
Aggressive Scripts
According to the GAM, scripts are a kind of knowledge structure that are used as guides for behavior and social problem solving by providing an indication of the events that are to happen, how a person should respond, and the likely outcome of these behaviors. Scripts are established via observational learning and conditioning, and it is presumed that individuals who regularly retrieve and employ aggressive scripts have developed a large number of scripts of this type in memory, thereby having readily accessible information about how to behave aggressively in varying circumstances (Huesmann, 1998). An example of an aggressive script is “If insulted, respond aggressively,” which could be retrieved and employed for the following situation: Attend bar, approach counter to buy drinks, victim bumps into you, demand apology, victim insults you, punch victim. The selection and retrieval of scripts is influenced by the interpretation of social cues; the activation of associated content, such as normative beliefs; the prevailing affective state or level of arousal; and the extent to which the script is rehearsed. Script rehearsal increases and reinforces the availability of those scripts in memory and strengthens their links with related knowledge structures, thereby having the potential to change expectations and intentions regarding appropriate social behaviors (Huesmann, 1998).
Evidence for the relevance of aggressive scripts to aggressive behavior is scant. Although considerable theoretical attention has been paid to the operation of scripts (e.g., Huesmann, 1998), investigations of their relevance to aggression has largely focused on script acquisition and development in children (e.g., Musher-Eizenman et al., 2004). Overall, there is a lack of evidence to demonstrate that a greater amount of procedural knowledge for aggressive action and retaliation, that is, guidance about when and how to behave aggressively, increases a person’s proneness toward aggression, and there are few measures available to assess the nature and extent of aggressive scripts. One exception is the Schedule of Imagined Violence (SIV), which was used by Grisso, Davis, Vesselinov, Applebaum, and Monahan (2000) to examine scripts in patients hospitalized for psychotic, depressive, substance-use, or personality disorders at three inpatient facilities. They found that one third of patients reported experiencing recent thoughts of violence toward others and that the degree of script rehearsal was predictive of violence after discharge. Two further studies support the predictive validity of the SIV (Kelty, Hall, & Watt, 2011; Nagtegaal, Rassin, & Muris, 2006).
Normative Beliefs
The second kind of aggression-related knowledge structure is normative beliefs supportive of aggression, which comprise beliefs about the acceptability of aggressive behavior. The GAM contends that for habitually aggressive individuals, activated aggressive scripts are filtered through normative beliefs that perceive aggression to be a favorable response. The empirical evidence for the role of normative beliefs in aggressive behavior is well developed. Aggression-supportive beliefs are predictive of physical aggression in offenders (Archer & Haigh, 1997a), violent offending (Kelty et al., 2011; Polaschek, Calvert, & Gannon, 2009), and violent recidivism (Mills, Kroner, & Hemmati, 2004) as well as self-reported violence in nonoffending samples (Archer & Haigh, 1997b). A range of measures have also been developed that purport to measure normative beliefs; these include the Measures of Criminal Attitudes and Associates (Mills, Kroner, & Forth, 2002) and the Criminal Attitudes to Violence Scale (Polaschek, Collie, & Walkey, 2004). People holding normative beliefs supportive of aggression were also recently found to be more likely to engage in the rehearsal of aggressive scripts (Kelty et al., 2011), although further examination of the relationship between these beliefs and other knowledge structures is required to substantiate the theorized process by which these aspects are connected.
Maladaptive Cognitions
Although the GAM focuses greater attention on the knowledge structures that it proposes are directly linked to aggression, it also posits a role for other entrenched cognitions that influence perceptions and expectations of the social world, particularly those that generate uncomfortable cognitive and affective states and that cue aggressive responses (Anderson & Carnagey, 2004). Although important types suggested are hostile world (Anderson et al., 2007) and narcissism-related (Anderson & Carnagey, 2004) cognitive structures, the model has been designed to incorporate any structure that generates internal states conducive to aggression and increases the accessibility of aggressive concepts in memory. It also draws on the work of Dodge and colleagues (e.g., Crick & Dodge, 1994; Dodge, 2006; Dodge & Pettit, 2003), who have proposed an association between aggression and biases toward interpreting other peoples’ actions in a hostile manner (i.e., hostile attributions).
Research into maladaptive cognitions has most often occurred with the schema theory framework developed by Young and colleagues (Young, Klosko, & Weishaar, 2003), which contends that personality dysfunction, in addition to other forms of psychopathology, is initiated by the existence of rigid core beliefs. This cognitive structure, termed early maladaptive schema (EMS), is proposed to develop as a result of adverse experiences in which maladaptive styles of perceiving oneself, others, and interpersonal relationships are reinforced, a pattern that is then elaborated throughout the lifetime. Similar to the GAM’s conceptualization of knowledge structures, the more extensive or developed the EMS, the greater the number of situations in which it is activated and the greater the intensity of its associated emotions (Young et al., 2003).
Although the importance of EMS has been established in relation to personality disorder (Jovev & Jackson, 2004; Nordahl, Holthe, & Haugum, 2005) as well as psychopathology, such as depression (Halvorsen et al., 2009) and substance abuse (Ball & Cecero, 2001), the role of EMS in aggression has received limited investigation. Several EMSs appear to overlap with specific contentions of the GAM, however, and thus might be speculated to increase the likelihood of aggression. Those EMSs resulting in hostile attributions toward others, such as mistrust and abuse and abandonment and instability, map onto the hostile attribution biases that the GAM proposes increase the accessibility of aggressive scripts (Anderson & Bushman, 2002). Insufficient self-control may also be linked to aggression via the tendency toward insufficient appraisal of behavior and difficulty restraining impulses, routes that the GAM also suggest increase the potential for aggression (Anderson & Bushman, 2002). In addition, EMSs have been shown to trigger anger (Ball & Cecero, 2001) and therefore may prompt aggression by activating the various anger-aggression routes outlined by the GAM. Finally, it is possible that aggression may eventuate from an individual’s attempts to escape or avoid distressing memories or emotions experienced during activation of their EMS.
To date, only one study has investigated the association between EMS and aggressiveness. In a nonclinical, predominantly female sample, Tremblay and Dozois (2009) found that 10 EMSs had positive relationships with aggression; those demonstrating the strongest associations were mistrust and abuse, insufficient self-control, and entitlement. Elsewhere, these three EMSs have also yielded a positive relationship with anger (Calvete, Estevez, Lopez de Arroyabe, & Ruiz, 2005). In an offending population, Loper (2003) examined the association between EMS, personality disorder, and psychological and behavioral adjustment in a sample of incarcerated women, finding that EMS suggestive of “impaired limits” (i.e., entitlement, insufficient self-control) predicted higher levels of self-reported threats and assaults while in prison. In terms of psychological distress, impaired-limits EMSs were also predictive of hostility, and disconnection or rejection EMSs (e.g., mistrust and abuse) were associated with hostility, paranoid ideation, and interpersonal sensitivity.
It is of note that these emerging findings appear to parallel the results of violent offender studies that have used alternative methodologies. For example, Polaschek et al. (2009) analyzed the transcripts of offense-process interviews in a sample of violent offenders for relevant “implicit theories.” In addition to a preponderance of beliefs associated with the normalization of violence, Polaschek et al. identified three further implicit theories, specifically, the need to act violently to achieve or maintain status and autonomy (“beat or be beaten”), the sense of moral superiority and entitlement to harm others (“I am the law”), and the inability to regulate one’s own behaviors without assistance (“I get out of control”). The three latter “theories” appear similar to the EMS constructs of mistrust and abuse, entitlement, and insufficient self-control, respectively.
The Present Study
The present study has three aims, specifically, to (a) investigate the GAM’s proposition that aggressive scripts and normative beliefs supportive of aggression are important predictors of aggression by examining the relationship between these phenomena in a sample of offenders, (b) describe the nature and prevalence of EMS in offenders with respect to their histories of aggression, and (c) explore the relationships between aggressive scripts, normative beliefs supportive of aggression, EMS, and trait anger with regard to offenders’ histories of aggression. It was hypothesized that participants with more significant and entrenched aggressive scripts and normative beliefs supportive of aggression (Grisso et al., 2000; Kelty et al., 2011) and trait anger (Cornell et al., 1999) would have more extensive histories of aggressive behavior. With respect to maladaptive cognitions, on the basis of the previous literature (Calvete et al., 2005; Polaschek et al., 2009; Tremblay & Dozois, 2009), it was hypothesized that three particular EMSs would be positively associated with aggression, namely, mistrust and abuse, entitlement, and insufficient self-control. Finally, it was expected that normative beliefs supportive of aggression would interact with script rehearsal on aggression, whereby a stronger relationship between aggressive scripts and histories of aggression would be identified when attitudes to aggression were more positive. Since social desirability biases have been noted to compromise the use of self-report methodology with offenders (Mills & Kroner, 2005) and depressive states can bias the reporting of EMS (Stopa & Waters, 2005), the respective impact of these variables on participants’ responses was assessed.
Method
Participants
Eighty-seven participants between 19 and 64 years old (M = 33.4, SD = 10.7) were recruited from a community forensic mental health service in Melbourne, Australia. All were referred by the criminal courts for psychological or psychiatric presentence evaluation between June 2009 and December 2010. Seventy-eight of the participants were male (90%), and 9 were female (10%). More than half of the sample either had pleaded guilty or had been found guilty of a violent offense (n = 47, 54%), most commonly, assault, recklessly causing injury, or intentionally causing injury, with the remainder having been convicted of nonviolent offenses (n = 40, 46%), such as theft and drug offenses. People who were unable to speak English without the aid of an interpreter, had an intellectual disability, or were unable to complete the assessment because of pervasive psychotic symptomatology were excluded (n = 4).
The majority of the participants were of White Australian (n = 62, 71%) background; the remainder were of “other” or mixed-ethnicity (n = 15, 17%), Asian (n = 7, 8%), or Aboriginal or Torres Strait Islander (n = 3, 3%) origin. Participants were diverse with respect to their education level, with 22% (n = 19) reporting that they had 10 years or less of education, 44% (n = 38) reporting between 11 and 13 years of education, and 31 % (n = 27) having undertaken vocational training or tertiary education. More than half of the sample indicated that they were currently unemployed or on a pension (n = 50, 58%); the rest were employed full-time (n = 19, 22%) or part-time (n = 16, 18%) or were undertaking home duties (n = 1, 1%). According to the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) assessment, 36 participants (41%) met criteria for a current depressive disorder (major depressive disorder, dysthymic disorder, adjustment disorder, or depressive disorder not otherwise specified), and 12 participants (14%) had a lifetime diagnosis of a psychotic disorder.
Measures
Aggression-Related Constructs
History of aggression
Participants’ histories of aggression were assessed using the Life History of Aggression–Aggression Scale (LHA-A; Coccaro, Berman, & Kavoussi, 1997). Using a structured interview format, the LHA-A quantifies the number of overt aggressive acts occurring since early adolescence in relation to five categories (i.e., verbal, indirect, nonspecific fighting, physical assault, temper tantrums) using a standardized scoring algorithm. The number of events in each category is rated on a 6-point response scale ranging from 0 (zero events) to 5 (more events than can be counted); scores are then summed to produce an overall score. Previously reported psychometric properties for the LHA-A suggest strong interrater agreement (intraclass correlation coefficient [ICC] = .94) as well as good test-retest reliability (r = .80) and internal reliability (α = .87), with moderate to strong correlations with other trait-based measures of aggression (Coccaro et al., 1997).
Aggressive script rehearsal
Aggressive behavioral scripts were assessed using the SIV (Grisso et al., 2000). The SIV is a semistructured interview that screens for aggressive scripts through participants’ self-reported responses to eight criteria (presence, recency, frequency, chronicity, similarity or diversity in type of harm, target, change in seriousness of harm, and proximity to target). Since participants’ histories of aggression were of interest (as opposed to the prediction of impending violence), several amendments were made to the SIV. The measure was introduced with the following passage:
So far I have asked you about times when you feel angry, and about how you have reacted in the past when this happens. I now want to ask some questions about your thinking. Most people tend to experience aggressive thoughts from time to time.
Consistent with Nagtegaal et al. (2006), the SIV was also modified so that the initial question (“Do you ever have daydreams or thoughts about physically hurting or injuring other people?”) was removed and replaced with the frequency item, “How often do you have thoughts about hurting or injuring other people?” The 2-month time period specifier was also removed from this item, resulting in eight possible response options including 0 (never), 1 (once every few years), 2 (several times a year), 3 (several times a month), 4 (once a week), 5 (several times a week), 6 (once a day), and 7 (several times a day). The second question was the recency item, “When was the last time you had such a thought?” Participants whose responses to both the frequency and recency items were never were not administered any further items.
Previous research has used two items from the SIV (acknowledged thoughts of hurting others and reported that this had happened in the past 2 months) to examine the predictive value of aggressive script rehearsal for future episodes of violence (Grisso et al., 2000). These items have been used to create a dichotomous split whereby participants have been considered either “SIV positive” (answered both items positively) or “SIV negative” (failed to meet either criterion). In the current study, following advisement from the original author (T. Grisso, personal communication, March 1, 2011), the SIV frequency item (SIV-F) was selected to denote participants’ previous levels of engagement in script rehearsal. The seven SIV-F response options were dichotomized via a median split (median = 2), whereby participants were classified as reporting that their script rehearsal was either “infrequent,” ranging from response categories 0 (never) to 1 (once every few years), or “frequent,” ranging from categories 2 (several times a year) to 7 (several times a day).
Normative beliefs supportive of aggression
Normative beliefs supportive of aggression were assessed using the Attitudes to Violence scale of the Measures of Criminal Attitudes and Associates (Mills & Kroner, 2001), a self-report measure that was developed using multiple samples of incarcerated offenders and that demonstrates good internal consistency (α = .80) and test-retest reliability (ICC = .73; Mills et al., 2002). The Attitudes to Violence scale contains 12 items (e.g., “It’s all right to fight someone if they stole from you” and “Sometimes you have to fight to keep your self-respect”) that the respondent rates as either agree or disagree. The Attitudes to Violence scale shows predictive validity for violent recidivism in offenders (Mills et al., 2004).
Maladaptive Cognitions
EMSs were assessed using the Young Schema Questionnaire–Short Form, Version 3 (YSQ-SF; Young, 2005). The YSQ-SF comprises 90 items and measures the 15 original EMSs described by Young et al. (2003) in addition to three more recently identified EMSs (approval seeking, negativity and pessimism, punitiveness), grouped into five broad domains. Participants rate themselves on a 6-point Likert-type scale from 1 (completely untrue of me) to 6 (describes me perfectly), with higher scores indicating a greater relevance of the EMS to the respondent. In accordance with the recommended scoring procedure and previous research (Jovev & Jackson, 2004; Lee, Taylor, & Dunn, 1999; Reeves & Taylor, 2007), the scores for each schema were summed and then divided by the number of items. This produced a mean score for each schema (range = 1 to 6). The short and long versions of the YSQ demonstrate equivalent, acceptable psychometric properties (Stopa, Thorne, Waters, & Preston, 2001). Although previous versions of the YSQ-SF have been found to assess relatively stable constructs associated with psychological distress (e.g., Riso et al., 2006; Schmidt & Joiner, 2004), its validity in offending populations has yet to be examined.
Trait Anger
The Trait-Anger scale of the State-Trait Anger Expression Inventory–2 (Spielberger, 1999) was used to measure the extent to which individuals held a disposition toward perceiving a wide range of situations as annoying or frustrating and their tendency to respond with anger. The scale contains 10 items rated on a 4-point Likert-type scale ranging from 1 (not at all) to 4 (very much so), where higher scores represent higher levels of trait anger. Good internal consistency for the scale is reported in both non-clinical adults (α = .84 to .86) and psychiatric patients (α = .87) (Spielberger, 1999).
Socially Desirable Responding
Participants’ tendency to engage in socially desirable responding was assessed using the Impression Management (IM) subscale of the Paulhus Deception Scale (PDS; Paulhus, 1999). This 20-item subscale identifies distortions in self-responding associated with the tendency to present an overly inflated self-description. The PDS is appropriate for use in forensic contexts (Lanyon & Carle, 2007) and is sensitive to impression management demands (Paulhus, 1999). The IM scale has excellent internal consistency and correlates highly with other measures of socially desirable responding (e.g., Lie scale of the Eysenck Personality Inventory; Paulhus, 1999).
Axis I Psychopathology
Diagnostic information regarding lifetime psychotic and depressive disorders was obtained using the relevant modules of the SCID-I–Patient Edition (SCID-I/P; First, Spitzer, Gibbon, & Williams, 2007). Acceptable levels of diagnostic reliability for the SCID-I/P have been demonstrated in various populations (Spitzer, Williams, Gibbon, & First, 1992). Where possible, self-reported responses were corroborated using information available from significant others or from file review. The number of current depressive symptoms experienced by each participant was quantified dimensionally; psychotic disorders were classified categorically (i.e., present or absent).
Demographic Information
A semistructured interview was also conducted in which information relating to participants’ marital status, number of children, education level, living arrangements, current employment, and past psychiatric history was obtained.
Procedure
Participants were administered the assessment measures by doctoral trained research assistants. The assessment process was divided into two sessions; the first session formed part of the participant’s presentence evaluation and included the diagnostic assessment (SCID-I/P) as well as the assessment of aggression history (LHA-A), EMS, trait anger, script rehearsal (SIV-F), and socially desirable responding (IM scale). The results of this assessment were conveyed to the psychologist or psychiatrist conducting the presentence evaluation to assist with preparation of this report. The second battery comprised the research-specific measures (demographic information, attitudes to violence) and represented an optional session that participants completed immediately after their presentence evaluation. In addition to the two assessment sessions, the data collection procedures involved a review of the available collateral information.
Ethics Approval
The current study formed part of a larger research project approved by the Victorian Institute of Forensic Mental Health and the Monash University Standing Committee on Ethics in Research Involving Humans.
Statistical Analyses
Data were analyzed using PASW Version 18. Fourteen participants (16%) were missing data on attitudes to violence since they had chosen not to complete the optional research battery or were unable to because of time constraints. Preliminary analyses revealed that these participants displayed no differences in their scores on other measures (i.e., aggression, trait anger, script rehearsal, levels of impression management) and thus did not appear to represent a discernibly different population. Pairwise correlations were initially computed to examine the relationships between the independent and dependent variables. Stepwise regression was then used to identify the EMS predicting aggression to account for the maximum amount of variance in individuals’ histories of aggression while avoiding the problems associated with a large number of predictors. A stepwise backward procedure was specified. This method takes into account suppressor effects, in which predictors yield a significant effect only when another variable is held constant, thus reducing the likelihood of type II errors (Field, 2009). Hierarchical multiple regression was then used to examine the variance in aggression as a function of trait anger, attitudes to violence, aggressive script rehearsal, and EMS. In the first step, impression management and depressive symptoms were entered as control variables. In the second step, trait anger and attitudes to violence were entered, and in the third step, aggressive script rehearsal (frequent vs. infrequent) and the EMS.
Although a priori hypotheses were that attitudes to violence would interact with both anger and scripts with respect to participants’ aggression histories, analysis revealed no significant moderating effects. Consequently, no interactions were included in the final regression model. Further analyses also suggested that attitudes to violence did not mediate the anger-aggression or script-aggression relationships. For all regression analyses, no major violations of the data that required any variable to be transformed were identified. After testing for multicollinearity, significant problems were not detected, as evidenced by all tolerance levels being above .20 (Menard, 1995).
Results
Descriptive Statistics
Descriptive statistics and internal consistency coefficients (Cronbach’s alpha) for participants’ aggression histories and attitudes to violence, levels of anger, and endorsement of the 18 EMSs are presented in Table 1. All main study variables demonstrated good internal consistency, although four EMSs had alpha coefficients below .70 (dependence and incompetence, enmeshment, entitlement, and unrelenting standards). Descriptive statistics for levels of impression management are also found in Table 1. The mean for the sample was in the average range relative to the general population (Paulhus, 1999).
Means, Standard Deviations, Ranges and Alphas for Main Study Variables

Note. N ranged from 73 to 87.
Differences in anger, attitudes to violence, frequency of aggressive script rehearsal, and aggression histories between males and females were examined using independent-samples t tests. No significant differences were obtained, with the exception of aggression, where males (M = 12.13, SD = 7.60) reported more extensive histories than females (M = 6.11, SD = 7.90), t(85) = 2.24, p = .028. Age was negatively correlated with aggression (r = –.25, p = .021), trait anger (r = –.28, p = .009), and attitudes to violence (r = –.34, p = .003), with younger participants demonstrating higher scores on these variables.
Prevalence of Script Rehearsal
Seventy-one percent of the sample (n = 62) acknowledged rehearsal of aggressive scripts; a larger proportion (n = 53, 61%) reported engaging in frequent aggressive script rehearsal (i.e., between several times a year and several times a day) than infrequent rehearsal (n = 34, 39%, i.e., never experienced aggressive thoughts or only once every few years). A chi-square test of the relationship between gender and frequency of script rehearsal revealed no significant differences between males and females, χ2(1) = .12, p = .73. Participants classified as engaging in frequent script rehearsal were younger (M = 31.6, SD = 10.3) than those whose rehearsal was infrequent (M = 36.2, SD = 10.7), t(85) = 2.00, p = .049.
Relationships among Aggressive Scripts and Beliefs, Anger, and Aggression
Bivariate correlations between the aggression-related knowledge structures, anger, aggression, depressive symptoms, and impression management are presented in Table 2. All aggression-related variables covaried in the positive direction. Attitudes to violence and trait anger both correlated strongly with aggression, whereby higher scores on these variables were associated with more frequent past aggression. Attitudes to violence and trait anger were also interrelated. The frequency of script rehearsal was positively correlated with aggression; the strength of this relationship was greater than the strength of the association between scripts and attitudes to violence or trait anger. Impression management was negatively related to all aggression variables.
Bivariate Intercorrelations Among Aggression-Related Variables, Impression Management, Depression, and Early Maladaptive Schema
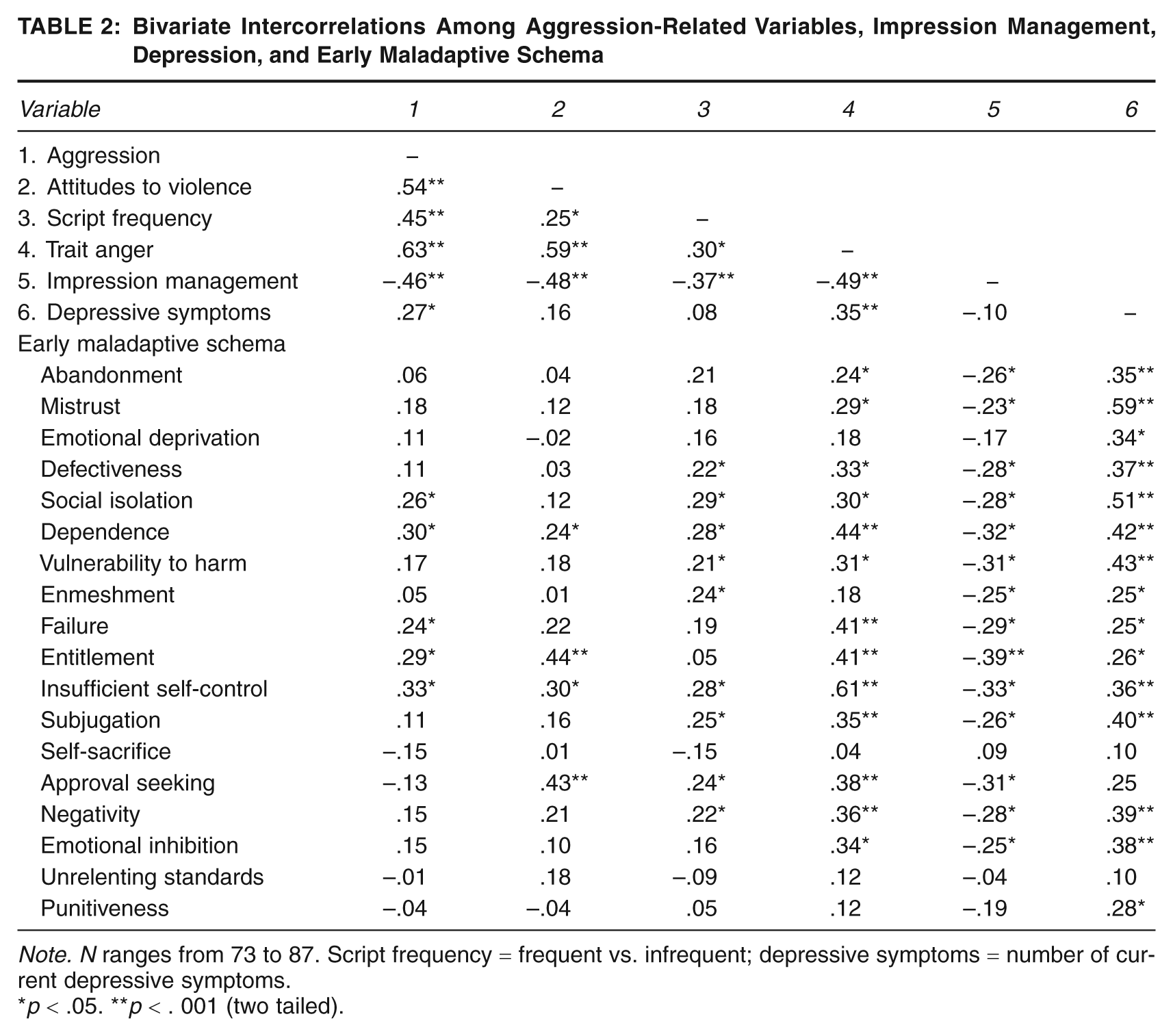
Note. N ranges from 73 to 87. Script frequency = frequent vs. infrequent; depressive symptoms = number of current depressive symptoms.
p < .05. **p < . 001 (two tailed).
Relationships between Ems and Aggression Variables
Bivariate correlations for the relationships between EMS and aggression, attitudes to violence, aggressive scripts, trait anger, and current depressive symptoms are found in Table 2. Five EMSs showed small to moderate positive correlations with aggression (insufficient self-control, dependence, entitlement, social isolation, and failure to achieve). The majority of EMSs were positively related to both trait anger and the frequency of script rehearsal, whereas only four EMSs (dependence, entitlement, insufficient self-control, and approval seeking) correlated positively with attitudes to violence. Furthermore, dependence and insufficient self-control were unique in being the only two EMSs that were related to all of the main study variables, and insufficient self-control demonstrated a particularly strong relationship with trait anger. Overall, the results suggested heterogeneous relationships between each of the EMSs and the aggression-related variables, although all significant relationships were in the positive direction. The number of current depressive symptoms was positively related to 12 of the 18 EMSs (Table 2), most strongly, mistrust and abuse and social isolation.
The next step was to select the EMS for inclusion in the regression analyses. An initial stepwise multiple regression was conducted, the set of EMSs that was included in the regression comprised the five EMSs whose bivariate correlations with aggression were significant at p < .05 (see Table 2) as well as the additional EMS that was hypothesized to be related to aggression (mistrust and abuse). This resulted in a total of six EMSs overall (social isolation, dependence, entitlement, insufficient self-control, failure, mistrust and abuse). The results of this analysis suggested that higher levels of insufficient self-control, β = .35, p = .003, independently predicted higher aggression scores (R2 = .12), F(1, 72) = 9.78, p = .003, when the remaining scales were controlled, with social isolation, dependence, entitlement, failure, and mistrust and abuse not significantly related to aggression. Thus, only the insufficient self-control EMS was selected for inclusion in the final regression model.
Effect of Aggression-Related Knowledge Structures, Insufficient Self-Control Ems, and Anger on Aggression
The unique relationships between each of the variables (i.e., trait anger, attitudes to violence, and frequency of script rehearsal) and aggression, after we controlled for levels of impression management and depressive symptoms, was next examined using hierarchical regression analyses. An initial model included age and gender, neither of which emerged as a significant predictor; these two variables were therefore not included in the final model. As can be seen in Table 3, the variables trait anger (β = .39, p = .005), attitudes to violence (β = .23, p = .049), and frequency of aggressive script rehearsal (β = .29, p = .003) were significant independent predictors of aggression (R2 = .52), F(6, 65) = 11.62, p < .001. Insufficient self-control did not contribute a significant portion of variance beyond the effects of these variables (β = –.16, p = .163).
Hierarchical Regression Analyses of Trait Anger, Attitudes to Violence, Scripts, and Insufficient Self-Control Early Maladaptive Schema (EMS) on Aggression

Note. N = 73.
p < .05. **p < .001.
Discussion
Although aggression-related cognitions are central to contemporary understandings of aggressive behavior, theoretically important constructs have received little investigation in populations with established histories of aggression and violence. It is speculated that these cognitions may be specific to offenders and less readily accessed from nonoffender populations (Collie et al., 2007), underscoring the need to examine their operation in forensic populations. The present study addressed this shortcoming in the literature by examining whether key knowledge structures delineated by the most comprehensive psychological aggression theory, the GAM (e.g., Anderson & Bushman, 2002), assisted in accounting for differences in the aggression histories of a sample of offenders.
Overall support for the GAM’s assumptions regarding the role of aggression-supportive beliefs and scripts was obtained, promoting the view that greater application of this framework within forensic settings will enhance current conceptualizations of aggression and violence. Several findings, including those relating to the role of EMS with respect to aggression and the relationship between aggressive scripts and aggression-supportive beliefs, were, however, not as expected. Given the widespread recognition that greater consideration of aggression theory is likely to advance current approaches to violent offender assessment and treatment (e.g., Howells, 2011; McGuire, 2008), the study highlights the need for further empirical investigation in the area of aggression-related cognitions.
Aggression Proneness as a Function of Aggression-Related Knowledge Structures
The findings regarding aggressive scripts and normative beliefs supportive of aggression supported the GAM’s contention that more aggressive individuals tend to hold several kinds of more elaborate and readily accessible aggression-related cognitions. That these constructs could be accessed and measured separately speaks to the possibility of a more sophisticated characterization of the cognitive features underlying aggressive behavior. The combination of these constructs and trait anger accounted for almost a quarter of the variability in participants’ histories of aggression, suggesting these should be a key focus of violence reduction programs.
The finding that aggressive script rehearsal bore a unique relationship with aggression is consistent with other studies indicating that the rehearsal of scripts containing aggressive content is an important antecedent for aggression (Grisso et al., 2000; Nagtegaal et al., 2006). Scripts denote how a person should interact with their social environment, and the results substantiate the GAM’s proposition that aggressive individuals are more likely to hold scripts that emphasize aggressive problem solving and regularly retrieve and employ aggressive scripts for social behavior (Huesmann, 1998). More routine assessment of aggressive scripts in aggression-prone individuals may therefore have considerable utility for case formulation and treatment planning. It is important to note, however, that the measurement and testing of the role of scripts in the present study was relatively simple as a result of the lack of previous research in this area and a need for a parsimonious measure of violent script rehearsal. This research has shown that scripts can be inferred and assessed via self-report methodology, confirming the need to develop more comprehensive assessment instruments to measure aggressive scripts.
The finding regarding the relationship between normative beliefs supportive of aggression and aggressive behavior was as expected, given the results of previous studies that have investigated violence-supportive beliefs (e.g., Archer & Haigh, 1997a; Polaschek et al., 2004). However, to our knowledge, this is the first time that beliefs about aggression have been examined empirically within a broader framework for understanding individual differences in aggressiveness. Consideration of aggression-supportive beliefs in this manner seems to indicate that when working with aggression-prone individuals, it is important to appraise their beliefs about aggression and violence specifically as opposed to their more generalized antisocial cognitions. The findings also reiterate the importance of assessing and modifying violence-supportive attitudes in those whose violence is problematic.
Aggression Proneness as a Function of Other Maladaptive Cognitions
The results regarding the EMS-aggression relationship were only partly in accord with the propositions of the GAM regarding the role of maladaptive cognitions in aggressive behavior. Although higher scores on entitlement and insufficient self-control EMSs were associated with more extensive past aggression, a similar pattern was obtained for three further EMSs (social isolation, dependence, and failure to achieve). According to Young et al. (2003), these EMSs correspond to deficiencies in setting internal limits and in behaving responsibly toward others (entitlement, insufficient self-control), beliefs that one is different from others (social isolation), and expectations about one’s ability to function independently (failure to achieve, dependence). This profile is somewhat consistent with previous EMS research. The insufficient self-control EMS has been linked to aggression in nonforensic populations (Tremblay & Dozois, 2009), and similarly, the implicit theory “I get out of control” is common among violent offenders (Polaschek et al., 2009). However, both these lines of research have also substantiated the role of cognitive structures representing mistrust of others in relation to aggression and violence, a relationship that the GAM also draws attention to (Anderson et al., 2007; Anderson & Carnagey, 2004). In the present study, however, no relationship between mistrust and abuse EMS and past aggression was identified.
A further notable finding with respect to EMS was that the strength of the individual EMS-aggression relationships was modest, with no single EMS contributing to aggression beyond the influence of the broader aggression-related variables (i.e., aggressive scripts, normative beliefs, trait anger). At the present time, the GAM does not provide clear expectations about the relationship between various kinds of maladaptive cognitions and aggression, although there is an overall assumption that those knowledge structures that make an individual vulnerable to hostile cognitions and negative affect are likely to increase aggressive tendencies through their connection to aggression-related cognitions and anger (Anderson & Bushman, 2002).
However, the present results seem to disavow the notion that any particular style of maladaptive cognition uniformly increases aggression potential across individuals. The importance of individual variation may instead be important; in particular, different maladaptive cognitions may be relevant and related to aggression for different individuals. The finding that there were idiosyncratic relationships between the various EMSs and trait anger, attitudes to violence, and scripts is also consistent with this possibility, particularly in light of the observation that the majority of EMSs were positively related to scripts. It may be that rehearsal of scripts containing aggression can function as a coping response to alleviate the intense and overwhelming cognitions and emotions arising from various activated EMSs. Young et al. (2003) suggest that methods of coping with EMS are typically behavioral in nature, although they may also be cognitive or emotional. Although different responses may be used across time and situation, broad coping patterns tend to be established. For instance, some individuals attempt to avoid activating their EMS by suppressing associated thoughts and emotions, whereas others surrender to the EMS and fully experience the ensuing pain and discomfort, leading to repetition of EMS-driven patterns of behavior. Thus, how people respond to activated EMS may be important in understanding the relevance of EMS to aggression and violence.
Aggression Proneness as a Function of Trait Anger
Consistent with previous research (e.g., Howells, 2004), the results of the present study also suggest a close relationship between trait anger and aggression. The GAM stresses the importance of anger by identifying the multiple routes by which aggression is induced (e.g., reducing inhibitions, maintenance of aggressive intentions over time). The present findings may further suggest that the tendency to experience anger more intensely, with greater frequency and for longer periods of time, is the most important aspect of an individual’s experience, over and above their tendency to retrieve aggressive scripts and to endorse the view that violence is acceptable. Consequently, they corroborate the notion that high levels of anger may be most influential in the maintenance of persistent aggressive behavior.
The Effect of Normative Beliefs on the Script-Aggression Relationship
A novel aim of the study was to explore how scripts, normative beliefs, and trait anger interacted with regard to offenders’ histories of aggression. Although the GAM does not assume that aggression-supportive beliefs must be present for a person to act violently, these beliefs are understood to represent a filter or gateway for aggressive scripts (Anderson & Bushman, 2002). Individuals engaging in habitual aggression are therefore considered more likely to hold favorable attitudes about this behavior. Although in the present study a relationship between scripts and beliefs was identified, the strength of this association was weak. In addition, aggression was better accounted for by the combined presence of trait anger and aggression-related scripts and beliefs than by beliefs alone, perhaps suggesting that the retrieval and enactment of aggressive scripts is not highly contingent on an individual’s beliefs about the acceptability of aggression.
These results may be partly accounted for by the pronounced effect of anger on scripts and normative beliefs. Anger was moderately related to aggressive scripts, a finding that is consistent with the results of Grisso et al. (2000) and that supports the idea that the process of selecting scripts that are in accord with normative beliefs is frequently overridden by the presence of anger. The GAM proposes that anger provides a justification for aggressive retaliation and influences the decision-making process for whether to employ a particular aggressive script. Although the current findings were unable to elaborate on the specific manner in which anger was related to scripts and beliefs, they supported the proposition that people who are prone to anger have aggressive scripts activated and accessible for longer periods of time (Anderson & Bushman, 2002).
Although the findings also suggested that anger was strongly related to normative beliefs about aggression, the nature of the relationship between these constructs remains unclear. It is uncertain, for example, whether people who hold more positive attitudes to violence are prone to using aggression to ameliorate angry affective states. Nonetheless, the present results suggest that people who frequently experience anger tend to hold more positive attitudes to violence and rehearse aggressive scripts more often, with anger therefore representing a key route by which aggression-related cognitions become relevant during an aggressive episode.
Limitations of the Present Study
A limitation of the current study was the method used to quantify participants’ aggression histories, which relied on retrospective reporting of aggressive events. Since participants were asked about their involvement in aggression since early adolescence, the self-reported frequency of their aggression was likely to be affected by participants’ ability to recall these events. The reporting of aggression and its associated cognitions may also have been biased by subsequent beliefs that had developed during the time elapsed between aggressive episodes (O’Leary, Malone, & Tyree, 1994). Although the results suggest that the aggression variables could be reliably quantified, social desirability was also moderately related to all aggression-related constructs. There may, for instance, have been a tendency to use cognitive distortions to justify past aggressive behavior or to deny aggressive episodes because of feelings of shame or guilt. A further contention of the GAM is that these knowledge structures represent relatively stable constructs; this assumption could also not be examined in the present study given its cross-sectional design. These limitations could be addressed via future studies using prospective methods.
There were also limits to the severity of participants’ aggression histories, as the current sample of offenders comprised individuals who were residing in the community prior to sentencing. It therefore did not include offenders who had recently engaged in more serious acts of violence (e.g., homicide). There was also an underrepresentation of females, and the current findings may not necessarily generalize to this population. Finally, to date, the YSQ-SF has not been validated for forensic populations, and it is possible that the construct validity of this instrument was compromised. Given the modest relationships that were identified between EMS and aggression, it may have been that the current sample had difficulty reflecting on their prevailing cognitions or comprehending the more abstract nature and sophisticated wording of the YSQ-SF items. Although the YSQ-SF has been used previously with offenders both clinically (e.g., Baker & Beech, 2004) and for research purposes (e.g., Specht, Chapman, & Cellucci, 2009), additional research is required to confirm the relationship between EMS (using both the YSQ and YSQ-SF) and aggression, anger, normative beliefs supporting aggression, and aggressive scripts.
Implications
As the present study attests to the notion that the GAM emphasizes various cognitions that can be empirically quantified and investigated in offender populations, there are several important research implications. Primarily, to strengthen the link between the theoretical basis of the GAM and applied work with forensic populations, replication of the current study in violent offenders without mental disorder and in female offender populations is required. This research would assist in gaining further insight into the operation of aggressive scripts, normative beliefs, and maladaptive cognitions with respect to aggression and violence, particularly if future studies were to include individuals with histories of more severe acts of violence. To better demonstrate a causal relationship in the interplay between aggression-related knowledge structures, affective arousal, and aggressive outcomes and to test the GAM’s assumption that knowledge structures remain relatively stable throughout the lifetime (Anderson & Carnagey, 2004), prospective studies are also required. Investigation of the aggressive-scripts construct was also limited in the present study, with information about the frequency of rehearsal used to infer the storage, accessibility, and retrieval of aggressive content. Further research in this area, particularly into the development of tools to more comprehensively assess aggressive scripts, will be critical to increase knowledge regarding how scripts exert an influence on aggression. Future research will also need to examine the moderating effect of coping styles on the relationship between EMS and aggression.
In terms of clinical implications, the results of the present study suggest that greater application of the GAM within the forensic field is likely to establish a more sophisticated and theoretically sound understanding of aggression. Since the specified cognitive and affective constructs appear to predispose people to higher levels of aggression, application of this knowledge will enable more extensive assessment and formulation of violence-prone individuals and, potentially, differentiation in aggressive tendencies in violent offenders. It appears that the presence of scripts, normative beliefs, and anger concurrently increase a person’s inclinations toward violence, and therefore these aspects should all be deemed as important treatment targets. Furthermore, the findings suggest that each construct should not be considered discretely; for example, it is to be expected that anger-prone individuals are also more likely to access aggressive scripts and to hold more positive beliefs about aggression. Finally, despite some knowledge structures appearing to be pervasive in their influence (e.g., aggressive scripts), the relationship between maladaptive cognitions and aggression is likely to be more idiosyncratic. It will therefore remain important to consider these aspects during assessment and treatment to determine their relevance to an individual’s aggressive behavior.