
Abstract
This study examined the influence of adolescent psychiatric disorder on young adult recidivism and compared findings with earlier studies of juvenile recidivism. Logistic regression analysis examined subsequent adulthood recidivism (through age 23 years) by disorder profile, adjusting for prior offense severity and background variables, in 340 Alabama juveniles referred to juvenile justice agencies (probation and detention). Youths with comorbid internalizing and disruptive behavior disorder had a sixfold increased risk for young adult recidivism compared with nondisordered counterparts. Comorbid internalizing disorder likely is a marker for the severity of a youth’s disruptive behavior disorder; similarly, offending that continues into adulthood likely betokens a more serious course of offending behavior. The severity underlying disorder and offending behavior is probably the common link between them. To prevent reoffending into adulthood, the mental health needs of juvenile justice youths’ internalizing and externalizing problems should be addressed.
Mental health problems have been found to be more prevalent in youths in juvenile justice settings than in their peers in the general population (Colins et al., 2010; Vermeiren, Jespers, & Moffitt, 2006; Wasserman, McReynolds, Schwalbe, Keating, & Jones, 2010). The high rate of psychiatric disorder in juvenile justice youths has consequences for more than just clinical management, as psychiatric disorder is found to be linked to recidivism (Colins et al., 2011; Cottle, Lee, & Heilbrun, 2001; McReynolds, Schwalbe, & Wasserman, 2010; Schubert, Mulvey, & Glasheen, 2011; Vermeiren, Schwab-Stone, Ruchkin, De Clippele, & Deboutte, 2002; Wierson & Forehand, 1995). Knowing mental health status may therefore improve identification of youths likely to reoffend.
Although earlier studies reported significant associations between mental health disorder and juvenile recidivism, links between specific disorder profiles and recidivism have been inconsistent (Colins et al., 2011; Colins, Vermeiren, Schuyten, & Broekaert, 2009; Vermeiren et al., 2002; Wierson & Forehand, 1995). For example, a meta-analysis revealed that substance abuse, conduct problems, and anxiety and stress were all associated with juvenile reoffending (Cottle et al., 2001). In one study, youths with substance use disorder were more likely to commit more future substance offenses (Colins et al., 2010), while in another, these youth were less likely to reoffend (Wierson & Forehand, 1995). However, most existing studies (including 12 of 13 considered in the Cottle et al. meta-analysis) of the mental health–recidivism link have relied on unstandardized assessment measures, often derived from chart review of prior unsystematic clinical interview, making comparisons difficult (Niarhos & Routh, 1992), and resulting in a variety of nonspecific associations between mental health disorders and recidivism.
The inconsistencies found in these earlier studies perhaps relate to small sample sizes or frequent reliance on unstandardized assessment of mental health status; in contrast, three studies of recidivism in juvenile justice youth, characterized by large sample sizes and by reliance on standardized mental health assessments, have consistently highlighted the importance of substance use disorder (Hoeve, McReynolds, McMillan, & Wasserman, 2013; McReynolds et al., 2010; Schubert et al., 2011). In one, youths with comorbid substance use and disruptive behavior disorders (also referred to as externalizing disorders, including conduct disorder, oppositional defiant disorder, and attention deficit-hyperactivity disorder [ADHD]) at probation intake were more likely to recidivate than were nondisordered counterparts (McReynolds et al., 2010). Focusing on severity of reoffending, another study revealed that juveniles with substance use disorder, with or without co-occurring other disorders at probation or detention intake, were at greater risk for escalations in subsequent offense seriousness than those without a disorder (Hoeve et al., 2013). Among incarcerated youths who had committed serious offenses, those with a substance use disorder, whether or not they indicated additional psychiatric disorders, were more likely to reoffend in adolescence and early adulthood compared with nondisordered youth, even when controlling for risk factors such as peer influence and antisocial history (Schubert et al., 2011). Evidence shows that compared with other juveniles, those with substance use disorder commit more reoffenses, as well as more severe reoffenses, over time.
These earlier studies concentrated primarily on reoffending during adolescence (i.e., juvenile recidivism). Studies that concentrate on recidivism into the young adult years are scarce. Given that offending that continues in young adulthood may reflect more serious persistent offending (Loeber & Farrington, 2012; Loeber, Hoeve, Slot, & Van der Laan, 2012), focusing on young adult recidivism is important. One of the three recidivism studies mentioned above (Schubert et al., 2011) collected juvenile as well as adult arrest data (14-23 years), but these data were then aggregated into a single measure of recidivism. In a community study (Copeland, Miller-Johnson, Keeler, Angold, & Costello, 2007) of the influence of psychiatric disorder (9-13 years) on subsequent arrests, those with co-occurring internalizing (i.e., affective and anxiety disorders) and disruptive behavior disorders were more likely to be arrested (aggregating first-time and repeat offenders) during young adulthood (16-21 years) compared with those with noncomorbid disorders or no disorder.
Differences in findings between the above community study and the three studies of juvenile justice youths (Hoeve et al., 2013; McReynolds et al., 2010; Schubert et al., 2011) could reflect study design features. First, the community study followed a sample of relatively young children in the general population (9-13 years at baseline), whereas participants in the three juvenile justice studies were adolescents (12-18 years at baseline), and were already in contact with the juvenile justice system. Second, the community study investigated general offending, including first-time offending and reoffending, while the three studies of juvenile justice youths focused exclusively on reoffending. Finally, the community study predicted data from adult criminal court records; in North Carolina, all arrests at ages 16 and older are under the authority of the adult criminal justice system. The three juvenile justice studies, however, focused on juvenile justice records (in one study combined with adult criminal records) at follow-up. These three reports, then, covered a broader age range from age 12 to 18 at follow-up in two studies (Hoeve et al., 2013; McReynolds et al., 2010) and from age 14 to 23 in the third (Schubert et al., 2011) compared with the community-based investigation.
These differences in sample characteristics cloud interpretation of differences in outcomes. They offer some evidence, however, to suggest that the disorder profiles of youths who reoffend in young adulthood may differ from those who reoffend during adolescence. Alternatively, these findings may underscore the importance of substance use disorder for youths already in contact with the justice system, and co-occurring internalizing and externalizing disorder for community youths.
Aside from these few studies of recidivism, earlier research has shown that young persons with comorbid externalizing and internalizing problems often demonstrate greater impairment. For example, in a longitudinal study of community children followed until Grade 5, those with recurrent symptoms in externalizing and internalizing domains had higher levels of social, academic, physical, and global functional impairment compared either with those without symptoms or with those with noncomorbid symptoms (Essex et al., 2009). Likewise, among adolescents, those with comorbid mood and disruptive behavior disorder were more likely to have poorer academic and global functioning than those with mood disorder only (Lewinsohn, Rohde, & Seeley, 1995).
An extensive review of child and adolescent comorbidity (Angold, Costello, & Erkanli, 1999) found that those with conduct disorder were especially likely to develop a comorbid internalizing disorder: Across studies, the risk of anxiety disorder was elevated threefold among those with conduct disorder compared with those without conduct disorder. In a large, multisite epidemiologic study (Robins & Price, 1991), community youths with more conduct problems were at increased risk for a greater number of externalizing disorders, which in turn increased risk for co-occurring internalizing disorders. Similarly, in the Pittsburgh Youth Study, versatility of antisocial behavior (i.e., escalation in overt, covert, and authority conflict pathways) was associated with depression, anxiety, or withdrawal, or with a combination of these problems (Loeber, Russo, Stouthamer-Loeber, & Lahey, 1994). Thus, severity and versatility of antisocial behavior seem to co-occur with internalizing problems (Angold et al., 1999; Zoccolillo, 1992). This literature suggests, then, that comorbid internalizing and disruptive behavior disorder, in particular, is related to greater impairment and may therefore elevate the risk of recidivism in young adulthood.
In sum, because of its association with recidivism, knowing mental health status may improve identification of youths likely to reoffend. Identifying which youths are at risk for recidivism is important for intervention and prevention purposes. Earlier studies showed that substance abuse disorder might be linked with juvenile offending and that co-occurring internalizing and externalizing disorder might be linked to young adults’ recidivism, but interpretations are difficult as studies’ age ranges overlap.
To examine the contributions of different profiles of mental health concerns, the present study considers rearrests in young adulthood as predicted by profiles of adolescent psychiatric disorders in a subsample of those examined in an earlier study on juvenile recidivism (Hoeve et al., 2013). Comparability across sample and methods allows for clearer comparisons of mental health risks for juvenile, as opposed to young adult, recidivism. The present study examines associations between disorder profile and reoffending that occurs between 18 and 23 years of age and considers the degree to which substance use, internalizing, and disruptive behavior disorders, alone and in co-occurring patterns, predict reoffending.
Method
Participants
The sample and procedures have been previously reported in an article on the contribution of mental health profile to juvenile recidivism (Hoeve et al., 2013). Alabama youths in Dallas, Jefferson, Mobile, and Montgomery counties participated in a collaboration with the Center for the Promotion of Mental Health in Juvenile Justice (CPMHJJ) between 2002 and 2006. Following either a systematic universal or randomized (by day of the week) sampling protocol, depending on county, 1,167 youths referred to juvenile justice agencies (874 at probation intake and 293 in detention) reported on mental health status (at baseline). In counties with a lower volume of juvenile justice intakes, all youth were asked to complete the mental health assessment. In counties with larger volume of youth, universal sampling was not feasible, and thus all youth on a randomly selected day of the week were asked to complete the mental health assessment. Of the 1,167 youths, 723 could be matched with either their juvenile justice or adult criminal court records, so that for these 723 youths, data were also available on full offense history, through December 13, 2007 (follow-up, see below). As reported earlier (Hoeve et al., 2013), differences between youths whose assessment data could be matched with justice records and those whose data could not be matched occurred no more frequently than at chance levels, considering a range of demographic, mental health, and offense characteristics, so that the impact of selective attrition was likely limited. Of the 723 youths, 340 were 18 years or older at follow-up and therefore data on adult reoffending were available for this subset, who comprised our final sample.
Procedures
At baseline, youths completed an audio computer-assisted diagnostic self-interview (ACASI) after intake into either their county’s probation or detention system. These assessment data were then sent by local staff to CPMHJJ. The Alabama Administrative Office of the Courts (AAOC), 14 months after the close of data collection, attempted to match individual youths’ assessment data to their cumulative adult criminal court records, relying on agency case number, date of birth, gender, race, county, and admit date at baseline. For each matched youth, AAOC provided the date and type of all offenses, beginning with the first court contact through December 13, 2007. Next, AAOC returned the offense data set to CPMHJJ, where data were matched to baseline assessment data and again de-identified.
Measures
Demographic Characteristics
Background information (date of birth, assessment date, gender, race, and justice setting type) was recorded by local staff at baseline.
Psychiatric Disorder
Youths self-assessed mental health status on the Voice Diagnostic Interview Schedule for Children (V-DISC), which is based on the DISC-IV. The DISC-IV is the most extensively tested child and adolescent diagnostic interview (Schaffer et al., 1996). It is highly structured, and has been evaluated in clinical and community samples. DISC-IV test–retest reliability is as good as, or better than, previous versions (Schaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000).
The V-DISC’s ACASI structure relies on a computer, with questions posed via headphones. No significant differences have been found in reliability of diagnoses between self-administered and interviewer-administered versions (Wasserman, McReynolds, Lucas, Fisher, & Santos, 2002). One-month reliability of most diagnoses (κ) ranged between 0.50 and 0.70 (Lucas, 2003). The V-DISC measures 20 DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed.) disorders in four clusters based on past-month symptoms according to the DSM-IV: substance use (SUD), disruptive behavior (DBD), anxiety (ANX), and affective (AFF) disorder. The V-DISC has been widely used in juvenile justice settings (e.g., McReynolds, Wasserman, Fisher, & Lucas, 2007; Wasserman et al., 2004; Wasserman et al., 2010; Wasserman & McReynolds, 2011).
To make analyses simpler and more efficient, we focused on clusters of disorders, including internalizing (either anxiety or affective: for example, Hughes & Gullone, 2008; Kovacs & Devlin, 1998) and disruptive behavior disorder (e.g., Frick et al., 1994). To examine the unique contributions of various disorder profiles to offending, we first created noncomorbid measures to denote youths who had mental health concerns only in one or another domain: internalizing (anxiety or affective: INT alone), DBD alone, or SUD alone. In addition to the noncomorbid measures, indications denoting mental health concerns in multiple domains (comorbidity) were created: internalizing and disruptive behavior disorder (INT + DBD), substance use and internalizing disorder (SUD + INT), substance use and disruptive behavior disorder (SUD + DBD), and substance use, internalizing, and disruptive behavior (SUD + INT + DBD).
Offense Characteristics
Complaint data (date and charge) were used as an indication of actual offending. Two types of offense data were available. Prior offenses included charges before the baseline mental health assessment (including the current offense); these were all considered juvenile justice cases. Subsequent offenses included adult criminal court charges from age 18 through December 13, 2007. Given that our focus is on adult reoffending, we did not include offenses (nine cases) committed before age 18 whose responsibility was transferred to adult criminal court. We also present descriptive information separately on youths’ current offense, although analyses aggregated current offenses into prior offenses (see below). For each youth, we calculated the number of months after the baseline mental health assessment, for which offense records could be reviewed from age 18 years, through December 13, 2007 (the “censor date”). The average total length of follow-up was 35 months, of which 14 were juvenile months (before age 18) and 21 were adult months (age 18 and older).
Because no determination could be made of their seriousness, charges that referenced administrative actions (e.g., miscellaneous filing or dispositional hearing) were not examined.
Our previous report (Hoeve et al., 2013) predicted juvenile offense severity. Because predictive models for severity, frequency, and “any” recidivism outcomes were similar and because the rate of adult offending was lower than that in adolescence (23% adult recidivism compared with 35% juvenile recidivism in our earlier report), here our focus was on any adult recidivism, defined dichotomously as whether there was any subsequent offense between age 18 years and the censor date. As before, our models adjusted for prior offense severity, referring to the most serious offense prior to baseline. Analyses also considered offense severity and frequency constructs for descriptive purposes.
Offense seriousness for each offense was coded based on the severity ranking system developed by the National Center of Juvenile Justice (Butts, 1997; National Juvenile Court Data Archive, 2007). Each offense was coded (between 1 and 77), with smaller numbers reflecting increased severity. As an example, the most serious charges (e.g., capital murder) received a code of “1,” and the least serious charges (e.g., violation of the seatbelt law) received a code of “77.” Participants who did not recidivate received a code of “78.”
Offense frequency was coded as follows. We calculated the number of days on which offenses occurred prior to baseline and the number of days of subsequent, postbaseline offenses (offense days). AAOC records sometimes noted multiple offenses on the same date, but which were part of the same event. This could happen if a youth was charged with trespassing and a residential burglary for the same event, or if he or she drove a stolen car through two counties. To simplify the tallying of offenses, then, for the frequency constructs, we aggregated all offenses charged on a single date. The 340 participants were charged with juvenile offenses committed on 945 dates before baseline, and with adult offenses committed on 183 dates after baseline.
Data Analysis
Via multivariate logistic regression analysis, using the statistical package SPSS (IBM Corporation, 2011), models predicted presence or absence of young adult recidivism from disorder profile. Because our sample includes youths at different juvenile justice processing points (system intake and detention), and because those who penetrate the system further likely differ systematically from those who do not in demographic and justice characteristics, analyses adjusted for justice setting (detention vs. system intake) and prior offense severity in our multivariate models. The first model considered only demographic and offense features, including prior offense severity, number of months post-baseline of available offense data, baseline age (in years), gender, race, and justice setting type (detention vs. probation). The second model examined further contributions of noncomorbid disorder profiles: INT alone, DBD alone, and SUD alone, and excluding youth who endorsed multiple disorder clusters. The final model considered the added contribution of cross-cluster comorbidity, comparing comorbid youths (INT + DBD, SUD + INT, SUD + DBD, and SUD + INT + DBD) with those with no disorder. For all analyses, nondisordered youths were the reference group for psychiatric disorder profile, female was the reference group for gender, probation was the reference group for justice setting, and White was the reference group for African American. We found no evidence for significant multicollinearity in multivariate models; the variance inflation factors (VIFs) were between values 1.0 and 4.4.
Results
Table 1 presents sample characteristics. Baseline age ranged between 12 and 18 years. The average youth was 16 years old at baseline; most were African American (63%). Most were from Jefferson County (n = 144), almost a third from Mobile (n = 102), and smaller proportions from Dallas (n = 56) and Montgomery (n = 38).
Sample Characteristics and Disorder Profiles.

Note. INT = internalizing disorder; DBD = disruptive behavior disorder; SUD = substance use disorder.
M, SD.
The reference category is the nondisordered group.
p = .5. **p < .05. ***p < .01. ****p < .001.
Paralleling findings for the larger sample (Hoeve et al., 2013), baseline offenses for those who were age 18 years or older at follow-up were most commonly possession of marijuana in the second degree (10.6%, Severity Rank 49), assault in the third degree (8.5%, Severity Rank 24), and disorderly conduct (7.9%, Severity Rank 57). About a quarter (23%) committed a further adult offense after baseline. Concerning all juvenile offenses (until age 18), youths were most often charged with a person-related offense (e.g., assault), followed by a property, substance, and weapon offense (see Table 2), whereas, as young adults (age 18 and after), they were most often charged with property and substance offenses. About a third could not be classified into either of these offense categories (e.g., traffic offenses).
Proportion of Offenses per Offense Type.
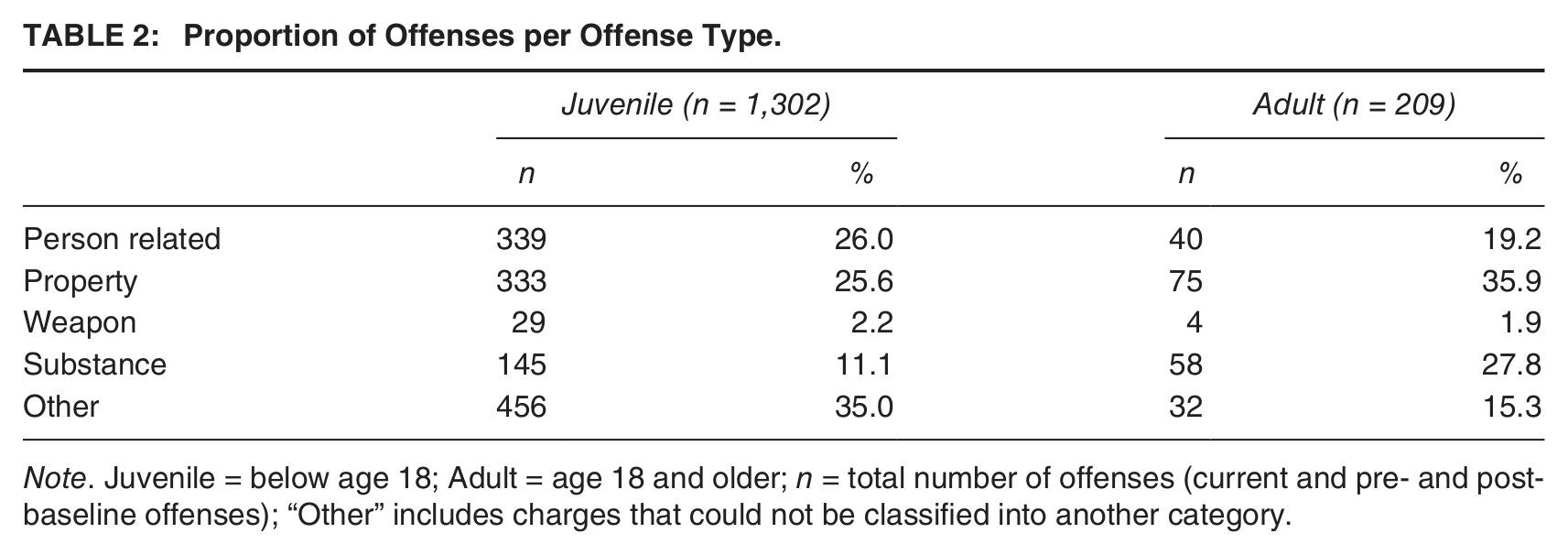
Note. Juvenile = below age 18; Adult = age 18 and older; n = total number of offenses (current and pre- and postbaseline offenses); “Other” includes charges that could not be classified into another category.
Approximately half the subsample who were adult at follow-up reported one or another baseline psychiatric disorder. More than 15% reported disorders in two or more clusters. Internalizing disorders were most frequently identified (about a quarter met criteria for any INT), followed by any DBD and any SUD. Expectably, cross-cluster comorbidity was considerably less common, so that each comorbid group included fewer than 10% of participants. These findings are relatively similar to those from the full sample, except that those who were adults at follow-up were more likely to report SUD (e.g., 21% vs. 16% any SUD) and less likely to report INT (e.g., 26% vs. 30% any INT) than in the full sample.
Table 3 presents results of analyses predicting any adult reoffending. The first model, considering demographic and offense characteristics only, significantly predicted adult recidivism, χ2(6) = 90.4, p < .001; Nagelkerke R2 = .35. Youths who had committed more severe offenses prior to baseline were more likely to reoffend in adulthood (odds ratio [OR] = 0.97). Expectably, youths whose adult records were reviewed for longer periods post-baseline were more likely to commit additional offenses than those whose records were reviewed for shorter periods (OR = 1.05). Males were twice as likely as females (OR = 2.05) to commit subsequent adult offenses.
Predicting Adult Recidivism From Juvenile Disorder Profiles.
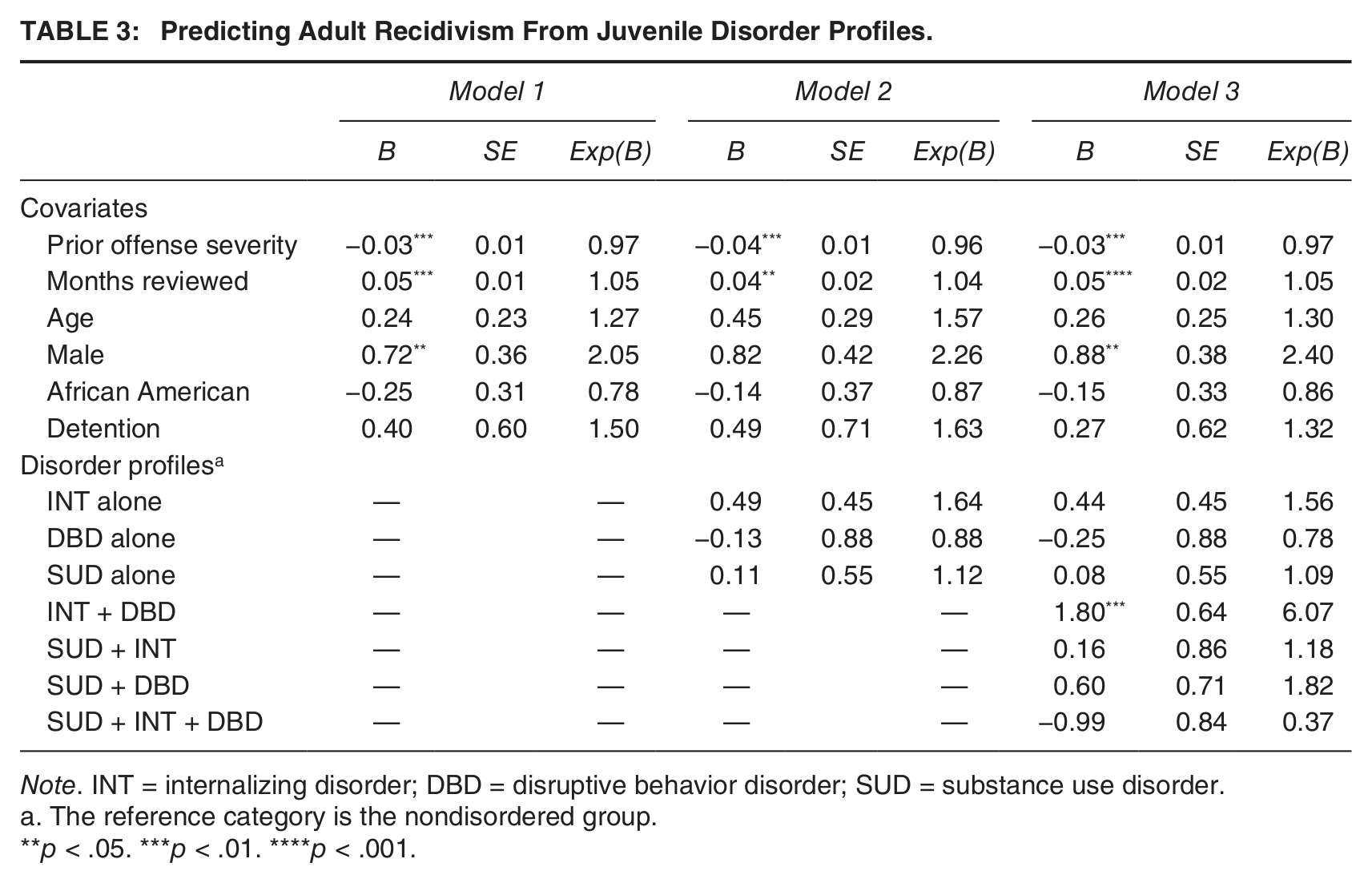
Note. INT = internalizing disorder; DBD = disruptive behavior disorder; SUD = substance use disorder.
The reference category is the nondisordered group.
p < .05. ***p < .01. ****p < .001.
Considering noncomorbid disorder profiles, the second model significantly predicted adult reoffending, χ2(9) = 60.0, p < .001; Nagelkerke R2 = .33, with contributions of demographic and offense characteristics essentially unchanged, and explaining a slightly smaller proportion of the variance compared with Model 1. Noncomorbid disorder profiles were not contributory. In the third model, comorbid profiles made additional contributions to young adult recidivism, χ2(13) = 101.8, p < .001; Nagelkerke R2 = .39, with a small improvement in explained variance. Compared with nondisordered youth, those reporting DBD and INT at baseline were 6 times as likely to reoffend as young adults (OR = 6.07).
To examine the degree to which they were influencing results, we reran models for the subsample without the seven youths who had been transferred to adult criminal court for crimes committed as juveniles after baseline, none of whom recidivated as adults. Results were relatively similar, except that associations for comorbid INT and DBD were now slightly stronger (OR = 6.78). Given the seriousness of their juvenile offenses (serious assault, burglary, murder, rape, and robbery), these seven youths were most likely incarcerated during the months for which young adult offenses could be reviewed. Results then were essentially unchanged whether these seven were classified as “nonrecidivists” or whether they were removed from analyses.
Discussion
We examined the degree to which adolescent mental health disorder profiles predicted subsequent arrests in young adulthood; analyses adjusted for baseline offense severity and demographics. To our knowledge, this study is the first to show that disorder profile in juvenile justice youths contributes to recidivism in young adulthood. A particular strength of this investigation is its longitudinal design; the data incorporated full offending histories, allowing us to adjust for prior offense severity and to predict reoffending up to age 23. Furthermore, examining the same sample used in our earlier study of juvenile reoffending increases comparability across findings.
Youths with baseline comorbid internalizing and disruptive behavior disorders had a sixfold increased risk for young adult recidivism compared with nondisordered adolescents. The combined effect of internalizing and disruptive behavior disorder on adult reoffending is substantial, given that longitudinal associations would be expected to weaken over time as the time interval between measurements grows longer (Loeber, Hoeve, Farrington, Slot, & Van der Laan, 2012). Moreover, because we adjusted for prior offense severity, the effect of psychiatric disorder is not an artifact of prior offending behavior.
Threats to Validity
Earlier studies on youths in juvenile justice settings, including our own (Hoeve et al., 2013), found that substance use disorder, with or without co-occurring disorders, was the strongest mental health predictor of future juvenile offending. Youths with substance use disorder (regardless of additional disorders) were more likely to be rearrested during adolescence and to commit even more severe reoffenses. In contrast to the present results, for offenses up through 18 years, comorbid conditions of internalizing and disruptive behavior disorder were not predictive.
The mental health features that relate most clearly to recidivism at different ages may differ from those identified from earlier studies of juveniles, either because of differences in methodology across studies, or because mental health conditions have differential associations with adverse outcomes at various subsequent developmental time points. Because the present report considers youths from the same sample considered earlier, it is unlikely that findings reflect differences in sample characteristics, procedures, or instruments.
Differences in the events that are considered “criminal” for juveniles and adults may explain differences in results. Because alcohol consumption is illegal only for juveniles, a baseline substance use disorder might be related to adult behaviors that are no longer illegal. However, we found that substance offenses were actually much more frequent in adults (28% of reoffenses among adults were substance offenses) than in juveniles (11% were substance offenses; see Table 2), so that a decrease in the illegality of substance use in adulthood cannot explain the lack of association between adolescent substance use disorder and young adult recidivism.
Comorbid Internalizing and Disruptive Behavior Disorder and Its Consequences
If methodological concerns do not explain these results, we need to look more closely at the differential risk associated with comorbid internalizing and disruptive behavior disorder across adolescent and young adult development. Our findings regarding the risk attributable to comorbid internalizing and disruptive behavior disorder are in accordance with those from another longitudinal study (Copeland et al., 2007). This earlier study of a community sample of children, relying on standardized psychiatric assessment, found that those with co-occurring internalizing and disruptive behavior disorder were more likely than those without a disorder, or those with a diagnosis in a single cluster, to commit offenses in young adulthood. The link between this disorder pattern and adult reoffending also appears in an investigation of adult offenders: Among those meeting criteria for antisocial personality disorder (a disorder that requires a diagnosis of conduct disorder by adolescence) on a structured psychiatric interview (Diagnostic Interview Schedule; Robins, Heizer, Croughan, & Ratcliff, 1981), about one third also reported co-occurring anxiety disorder with an age of onset of about 16 years (Hodgins, De Brito, Chhabra, & Coté, 2010).
In the present study, conduct disorder was the most prevalent disruptive behavior disorder among those with co-occurring internalizing and disruptive behavior disorder (i.e., more than 50% in this profile group met criteria for conduct disorder). Reflecting its severe level of impairment, conduct disorder has been referred to as a “disorder of multiple dysfunction” (Lambert, Wahler, Andrade, & Bickman, 2001; Zoccolillo, 1992). In the Fort Bragg Study (Lambert et al., 2001), children with conduct disorder commonly showed additional impairments at baseline, including the presence of two or more additional disorders. In that cohort, those with conduct disorder had higher levels of internalizing problems, their treatment lasted significantly longer than it did for those without conduct disorder, and their disorder followed a more chronic course, marked by greater relapse within 3 years after baseline. Other research also has shown that internalizing problems often co-occur in conduct disordered youths (Angold et al., 1999; Loeber et al., 1994; Zoccolillo, 1992). While we lacked information on age of onset that would allow determination of which disorder type appeared first, there is evidence to suggest that conduct disorder increases risk for subsequent anxiety and depression (Angold et al., 1999; Zoccolillo, 1992).
Co-occurring conduct disorder and internalizing disorder may be expected to be linked to recidivism because conduct disorder is related to internalizing disorders (Angold et al., 1999) and increases the risk of future offending (Murray & Farrington, 2010). Several possibilities might explain why youths with comorbid internalizing and disruptive behavior disorder are more likely to reoffend in adulthood. First, it may be that this disorder profile is a marker for severity of antisocial behavior (Angold et al., 1999). Comorbid conditions such as disruptive behavior and depression may interact and consequently produce worsening course of behavior (Loeber & Keenan, 1994). Our finding that those with comorbid internalizing and disruptive behavior disorder had a sixfold risk for recidivism, whereas those with either disruptive behavior or internalizing disorder alone were equally likely to recidivate, compared with nondisordered youths, is in line with the idea that these disorders may operate interactively.
Second, shared risks or mediating factors may explain the relationship between these comorbid conditions and future offending. While we lacked information that would have allowed us to investigate shared family factors, there is evidence to suggest that family conflict is a risk factor for offending behavior and comorbid internalizing and externalizing disorders (Chung, Hawkins, Gilchrist, Hill, & Nagin, 2002; Drabick, Gadow, & Loney, 2008). For example, in a clinical sample, boys with co-occurring symptoms of anxiety and oppositional defiant disorder had higher levels of family conflict compared with those with either condition alone or with other conditions (Drabick et al., 2008). In another sample of children from low-income families, comparing escalators and desisters, family conflict significantly predicted escalation in offending from age 18 (Chung et al., 2002). Alternatively, findings from the Fort Bragg Study (Lambert et al., 2001) suggested that the pervasive impairment of conduct disordered children may diminish their social skills and worsen their relationships over time with family, teachers, and peers, perhaps precipitating family conflict. Loosening of bonds to positive influences in these domains is a critical feature in criminological models of the development of antisocial behavior (e.g., Hirschi, 1969; Sampson & Laub, 2005).
Young Adult Recidivism
While juveniles with comorbid internalizing and disruptive behavior disorder may have recidivated in adolescence, results show that they did so at a rate not higher than nondisordered youths (Hoeve et al., 2013). Juvenile offending is more common, even among unimpaired youths with relatively stable backgrounds (Frick, 2012; Moffitt, 1993), than offending in young adulthood. Most adolescent offenders desist over time (Farrington, 2003). Recidivism that extends into young adulthood, therefore, is likely a characteristic of a more clearly defined, and perhaps more clearly impaired, subgroup (Loeber, Farrington, Howel, & Hoeve, 2012; Loeber, Hoeve, Farrington, et al., 2012).
Young adulthood is a period of profound change in which many important life events take place, including completion of education that will be the basis for lifetime occupation and income, resolving important life choices and exploring possible life directions (Arnett, 2000). Both unemployment and single marital status increase the risk of young adult reoffending in those who begin offending during adolescence (Loeber & Farrington, 2012; Loeber, Hoeve, Slot, et al., 2012). Comorbid internalizing and disruptive behavior disorder may derail attainment of important life milestones, and deviating from that expectable young adult trajectory in turn may increase risk for adult offending.
Limitations
There are a number of limitations in the current report. First, we used arrest data as a proxy for reoffending. The various methods used to measure offending behavior have advantages and disadvantages. In particular, official offense data are often thought to underestimate minor offenses (Babinski, Hartsough, & Lambert, 2001). Second, we lacked information on length of incapacitation for those who were incarcerated for adult crimes. Analyses controlled for age and the length of follow-up (months reviewed), and we reran our analysis without the seven youths who had been transferred to adult court and were most likely to be incapacitated during follow-up. Earlier, we examined models without youths who experienced placement in secure care after baseline. Only 7% of the total sample had been incarcerated during follow-up (n = 46; Hoeve et al., 2013). Results, though attenuated by reduced power, were essentially unchanged (available on request). Nevertheless, incarceration might have further limited opportunity for offending during follow-up, so that incarcerated and nonincarcerated youths would have varied in their opportunity to reoffend.
Finally, the sample size was too small to investigate effects of less frequent conditions such as anxiety disorder alone. Few youths reported an anxiety disorder without any comorbid disorder, so that we collapsed anxiety and mood disorder into a single construct. We also lacked power to examine the degree to which the impact of psychiatric disorder on reoffending may be moderated by gender. Girls in community as well as juvenile justice settings are significantly more likely to meet criteria for internalizing problems than are boys (Rosenfield, Phillips, & White, 2006; Wasserman et al., 2010); at juvenile probation intake, we found that girls were more likely to report internalizing, oppositional defiant, and comorbid disorders (Wasserman et al., 2010). Moreover, affective disorder predicted recidivism when it appeared along with disruptive behavior or substance use disorder (McReynolds et al., 2010). Females with comorbid affective and substance use disorder were more likely to reoffend within a year than were males with the same disorder profile or nondisordered males (McReynolds et al., 2010). Accordingly, findings may not be generalizable to those with minor offenses, and they may be less generalizable for females than for males. Further research, with larger samples, should investigate the extent to which psychiatric disorder relates to future offense severity in both genders.
Clinical Implications and Future Research
Unlike most youths who “grow out” of offending by young adulthood, those with comorbid internalizing and disruptive behavior disorder show a more persistent course with offending that continues at least into young adulthood. Most likely, this reflects the increased impairment in those with this pattern of comorbid disorders. Prior studies have shown that identifying youths with substance use disorder and referring them to specialized evidence-based interventions decrease their risk for an escalating pattern of future juvenile offenses. The present study suggests that identifying and treating those with comorbid internalizing and disruptive behavior disorder are likely to decrease risk for future adult offenses. Taken together, findings suggest that mental health screening can not only contribute to the identification of treatment needs but also identify those most likely to engage in a future escalating course of offending.
Interventions are very different for youths with different types of disorder profiles, and therefore, it is important that justice agencies effectively match youths to programs that can address their mental and behavioral health needs. Youths with conduct disorder and co-occurring internalizing disorder may need more intensive treatment programs than do those with other disorder profiles (Lambert et al., 2001). Unfortunately, presently, no evidence-based interventions have been developed that directly target this comorbid profile (Cunningham & Ollendick, 2010; Wolff & Ollendick, 2006). Wolff and Ollendick (2006) suggested that treatments targeting conduct disorder may be the most promising approach, because those with co-occurring conduct disorder and depression more closely resemble those with conduct problems alone than those with depression alone. Future research should examine the effectiveness of this approach, as our results underscore that effective interventions aimed at comorbid internalizing and disruptive behavior disorder might prevent a persistent offending pattern into adulthood, and likely impacts future public safety.
Footnotes
Authors’ Note:
This work was supported by the Carmel Hill Fund and by a Marie Curie grant of the European Union awarded to Machteld Hoeve (FP7-PEOPLE-2010-IOF, Project 274337).
![]() ), a research and policy center offering guidance to juvenile justice agencies on protocols for efficient identification and service referral for those with mental health service needs. She has been conducting research on developmental psychopathology for 35 years. She has authored more than 100 articles for academic and practitioner audiences.
), a research and policy center offering guidance to juvenile justice agencies on protocols for efficient identification and service referral for those with mental health service needs. She has been conducting research on developmental psychopathology for 35 years. She has authored more than 100 articles for academic and practitioner audiences.