
Abstract
Although studies have consistently demonstrated mentally ill offenders to be disproportionately involved in misconduct within correctional facilities, research is limited on the potential exacerbating effects of co-occurring disorders (CODs) on inmate behavior. With the vast number of offenders who have comorbid psychiatric and substance use disorders, it is essential that we understand whether the clinically interactive nature of CODs may present increased security and management challenges for correctional administrators. Using data from the Pennsylvania Department of Corrections (PADOC), we compared the institutional misconduct experiences of female inmates with CODs to those for inmates with singular disorders or no disorders. The findings of our study support prior research showing mental illness as a risk factor for prison misconduct. The results further suggest that the presence of both a substance use disorder and a mental illness exacerbates the risk of negative behaviors beyond the singular disorder of mental illness.
High rates of mental illness, substance use, and co-occurring disorders (CODs) are typically observed among female inmates. These conditions may hinder their ability to adjust to the stressors of the prison environment, creating security and behavioral management challenges for correctional administrators (K. N. Wright, 2000). Using data from the Pennsylvania Department of Corrections (PADOC), this study examined misconduct among female state inmates with no disorders, single disorders (i.e., mental illness or substance use disorders), and co-occurring mental health and substance use disorders.
Disorder Prevalence Rates by Gender
Women involved in the criminal justice system have higher prevalence rates of mental illness, drug use disorders, and CODs compared with their male counterparts (Bloom, Owen, Covington, & Raeder, 2003; Hills, 2004; James & Glaze, 2006; Mumola & Karberg, 2006). An estimated 73% of female state inmates are reported to have a mental health disorder and 60.2% are considered to be drug abusing or dependent (compared with 55% and 53% of males respectively; James & Glaze, 2006; Mumola & Karberg, 2006). More than half (54%) of women incarcerated in the United States meet the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 2000) criteria for comorbid psychiatric and substance use disorders compared with 41% of male inmates (James & Glaze, 2006).
The true prevalence rates of mental illness and CODs among female inmates are likely even higher than estimates suggest. Mental health and COD diagnoses in prison are generally limited to serious mental health disorders (i.e., psychosis, mania, and major depression), potentially omitting many of the more common psychiatric diagnoses for women (e.g., anxiety disorders, post-traumatic stress disorders, and borderline personality disorders; Bloom et al., 2003; National Institute of Mental Health, n.d.). Accurate assessment of CODs is further hindered by the absence of valid dual disorder screening instruments (Sacks & Melnick, 2007) leaving many CODs undetected and underreported (McMillan et al., 2008; Peters, Bartoi, & Sherman, 2008; Peters, LeVassuer, & Chandler, 2004).
Co-Occurring Psychiatric and Substance Use Disorders
Because of the complex and interactive nature of multiple disorders occurring simultaneously, it is important to distinguish CODs from singular disorders. The simultaneous occurrence of multiple diagnoses affects the course and prognosis of the individual disorders, often exacerbating their symptomatic nature and worsening treatment outcomes (National Institute on Drug Abuse [NIDA], 2008). CODs occur when individual disorders can be independently distinguished from one another and are not merely a myriad of symptoms stemming from a single disorder (Center for Substance Abuse Treatment, 2005). The multifaceted nature of CODs and the complexity of their assessment and treatment, particularly in correctional settings, are generally associated with poorer clinical prognosis than singular disorders of mental illness or substance use disorders (Dennison, 2005; Peters et al., 2008; Peters et al., 2004). Additional clinical implications include poor medication compliance, lower treatment completion rates, and shorter periods of remission following treatment (Lehman, Myers, & Corty, 2000; Peters et al., 2008). Furthermore, individuals with CODs are prone to greater suicidal behavior, more frequent hospitalizations, and experience difficulty with social functioning (Peters et al., 2008).
Inmates with CODs have also been shown to exhibit more aggressive and violent behaviors compared with inmates with singular disorders (National GAINS Center for People with Co-Occurring Disorders in the Justice System, n.d). The MacArthur Violence Risk Assessment Study found significantly higher rates of violent offenses among individuals diagnosed with either a comorbid major mental health and substance use disorder (31.1%) or comorbid other form of mental health and substance use disorder (43%) compared with those with a major mental health disorder only (17.9%; Steadman et al., 1998). CODs often result in protracted periods of institutionalization and an inability of the inmate to function in either community or correctional settings (National GAINS Center for People with Co-Occurring Disorders in the Justice System, n.d.).
COD inmates generally exhibit a poorer clinical response to treatment (Peters et al., 2008). The heterogeneity of symptoms associated with CODs makes this segment of the inmate population more difficult to treat, particularly among inmates with more severe and longstanding mental illness (Lehman et al., 2000; Peters et al., 2008; Peters et al., 2004). The symptoms frequently exhibited by COD inmates such as erratic behaviors, hallucinations and delusions, poor impulse control, and predatory behaviors toward others, are often associated with negative attitudes toward treatment and difficulty with treatment management (Peters et al., 2004).
Disorders and Prison Misconduct
Inmates with mental illness or CODs may also find the rigid structure and stressors of the correctional environment difficult to manage. Indeed, national survey findings report prison inmates diagnosed with a mental illness are more likely to be charged with a rule violation than other inmates (58% vs. 43%, respectively) and twice as likely to be injured in a fight (20% vs. 10%, respectively; James & Glaze, 2006). Mentally ill inmates are also more likely to have been charged with a current or past violent offense compared with non-mentally ill inmates (61% vs. 56%, respectively; James & Glaze, 2006). Research on institutional misconduct has further demonstrated an increased risk of rule-violating behaviors by mentally ill and COD inmates (see Adams, 1983, 1986; Hildebrand, DeRutter, & Nijman, 2004; Houser, Belenko, & Brennan, 2012; O’Keefe & Schnell, 2007; Steiner & Wooldredge, 2009; E. M. Wright, Salisbury, & Van Voorhis, 2007). Adams (1986) suggests that institutional infractions by the mentally ill are often symptomatic reflections of their psychiatric condition (e.g., refusing to come out of their cells, setting fire to their cells, self-injurious behavior, lack of hygiene, and destroying state property).
Using a nationally representative sample of female inmates over two waves (1991 and 1997), Steiner and Wooldredge (2009) found that female inmates with mental illness were significantly more likely to engage in both violent and non-violent prison infractions. E. M. Wright et al. (2007) sampled 272 incarcerated women to determine if gender-responsive needs (e.g., needs that are qualitatively different for women than men such as issues of self-concept and parenting) were related to misconduct at 6 and 12 months post-intake, controlling also for gender-neutral factors including mental health histories. Their results showed that prior mental health problems were predictive of serious rule violations during both the 6- and 12-month periods.
Although there is mounting empirical support for the association between psychiatric disorders and institutional misconduct, limited research examines whether the clinically interactive nature of comorbid disorders aggravates rule-violating behaviors beyond that of singular disorders (see Houser et al., 2012). The exacerbated symptom complex commonly associated with CODs may further impede the ability of the inmate to effectively adapt to the structure of a correctional environment. Using data from the 2004 Survey of Inmates in State Correctional Facilities, Houser et al. (2012) found that female inmates with a major mental health disorder or COD were significantly more likely than those with no disorders to engage in both minor and serious misconduct. The effect, however, was stronger among inmates with CODs than those with a single diagnosis of mental illness.
Factors Associated with Prison Misconduct
With state and federal correctional populations nearing two million in the United States (West, Sabol & Greenman, 2010), maintaining order in facilities has become a significant challenge. Preserving safety and order is further complicated by the vast number of mentally ill and COD offenders. Although misconduct rates are skewed among a small group of offenders, identifying the risk factors of misconduct has important safety, management, economic, and re-entry implications (Goetting & Howsen, 1986). Recognizing risk factors for disruptive behavior can be an effective tool for correctional administrators in helping to maintain control and management of the inmate population (Craddock, 1996). Much of the empirical and theoretical research on inmate misconduct has been conducted on male samples (see Adams, 1983, 1986; Toch & Adams, 1986; K. N. Wright, 1991; Zamble & Porporino, 1988). Only recently there is an increased interest in gender-specific correlates of misconduct (Acevedo & Bakken, 2003; Houser et al., 2012; Steiner & Wooldredge, 2009; Thompson & Loper, 2005; E. M. Wright et al., 2007).
The most robust socio-demographic factor associated with misconduct is age. Findings have consistently demonstrated that as an inmate ages, they are less likely to engage in institutional misconduct (Goetting & Howsen, 1986; Jiang & Winfree, 2006; Steiner & Wooldredge, 2009; Toch & Adams, 1986; Welsh, McGrain, Salamatin, & Zajac, 2007; Wooldredge, Griffin, & Pratt, 2001; Zamble & Porporino, 1988). Race has yielded mix results with some studies finding African Americans to be disproportionately charged with misconduct (see Goetting & Howsen, 1986; Jiang & Winfree, 2006; McCorkle, 1995; Steiner & Wooldredge, 2009; Wooldredge et al., 2001). Gover, Perez, and Jennings (2008) suggest that race may intersect with gender. Their findings showed that non-White females had significantly greater numbers of infractions than White females. The effect of race, however, was non-significant among male offenders. Seriousness of misconduct may also be correlated with race. Steiner and Wooldredge (2009) found that African American women were more likely to be involved in violent misconduct compared with White females; whereas there were no differences in race for non-violent misconduct.
Additional socio-demographic factors including education and marital status may also be important indicators of inmate misconduct. According to Hirschi (1969), prior achievements and commitments to a conventional lifestyle are reflective of an individual’s conformity. Essentially, these individuals have a stake in conforming to a more traditional lifestyle that may transcend incarceration. Compared with single or divorced inmates, individuals married at the time of incarceration have generally been found to be less disruptive (Acevedo & Bakken, 2003; Houser et al., 2012; Myers & Levy, 1978). Steiner and Wooldredge (2009) found that female inmates who were both married and cohabitating at the time of incarceration were less likely to be engaged in violent misconduct but equally likely to be charged with a non-violent infraction. Thus, marital status may be associated with the seriousness and violence of the behavior.
Higher levels of educational attainment may also reflect greater conformity to a traditional lifestyle. It may provide an individual with the ability to more critically evaluate the consequences of their behavior (Harer & Langan, 2001), resulting in the avoidance of certain types of misconduct. In fact, several studies have reported that offenders with higher levels of education are less likely to engage in misconduct (Gover et al., 2008; Harer & Langan, 2001).
Prior involvement in the criminal justice system has generally been found to be associated with increased odds of inmate misconduct. Several studies have found that prior incarcerations (Goetting & Howsen, 1986; Gover et al., 2008; Harer & Langan, 2001; Jiang & Winfree, 2006; Steiner & Wooldredge, 2009) and prior arrests (Goetting & Howsen, 1986; Houser et al., 2012; Steiner & Wooldredge, 2009; Wooldredge, 1991) were significantly related to an increased rate of infractions. Myers and Levy (1978) found that age at the time of first police or court contact and the number of juvenile encounters with the criminal justice system were positively associated with misconduct.
Current Study
This study sought to examine the impact of single disorders (i.e., mental illness only or substance use disorders only) and comorbid psychiatric and substance use disorders on institutional misconduct while controlling for other factors associated with misconduct. We considered institutional misconduct among four mutually exclusive and exhaustive groups of female inmates: (a) those with no disorders, (b) those with mental health disorders only, (c) those with substance use disorders only, and (d) those with co-occurring substance use and mental health disorders. The present study examined two primary hypotheses. First, inmates with mental health disorders only or CODs will have higher odds of misconduct compared with inmates with substance abuse/dependence only or no disorders, net of controls. Second, inmates with CODs will be more likely to engage in misconduct compared with inmates with singular disorders (e.g., mental illness or substance abuse/dependence only), net of controls.
Method
Sample and Procedure
Data for the current study were drawn with the cooperation of the PADOC. All data used for this study were routinely collected and maintained electronically by the PADOC. Applications were made and subsequent approvals were obtained from Temple University’s Institutional Review Board and the PADOC’s Board of Review. All data were de-identified by the PADOC; inmate numbers and names were removed to ensure confidentiality.
Data were provided for all female state prison inmates incarcerated in the State of Pennsylvania between January 1, 2007 and July 30, 2009 (n = 2,279) who were either currently serving or had served time at one of two women’s correctional facilities maintained by the PADOC (State Correctional Institution [SCI] Cambridge Springs, and SCI Muncy), or the co-educational boot camp, Quehanna Boot Camp. Because the intake diagnostic and classification process takes approximately 4 to 6 weeks, this study excluded all inmates who were incarcerated for a period of less than 4 months, which would have been too short a time for them to receive their permanent placement. This criterion reduced the sample size to 2,164 cases.
Two other major criteria for inclusion in the sample were evidence of substance dependence and/or a mental health disorder. Electronic data indicating the presence or absence of a mental health disorder was available from the PADOC for all 2,164 cases in the sample. The Texas Christian University (TCU) Drug Screen II (described below) was the major indicator of substance abuse/dependence used by the PADOC. However, 398 cases were missing scores on this instrument and were removed from the sample, reducing the sample to its final size of 1,766 cases. Imputing missing data for the TCU Drug Screen II was not appropriate because this information was one of the two major criteria required for inclusion in the sample.
Dependent Variable
Similar to previous research on inmate misconduct, data for this study were obtained from official disciplinary records maintained in the PADOC’s electronic database. Misconduct is defined as “a written report completed in response to a violation of a formal rule or regulation by an inmate in the custody of the Department” (PADOC, 2006, p. 10). Misconduct reports are written by either the charging staff member or contracted employee with direct knowledge of the violation. Each infraction receives a formal written misconduct report (DC-141; PADOC, 2008).
Independent Variable
Subjects were classified into four diagnostic categories: (0) no disorders (no mental health disorders or substance abuse/dependence), (1) CODs (any mental health disorder and substance abuse/dependence), (2) mental health disorders but no substance abuse/dependence, and (3) substance abuse/dependence but no mental health disorder. Criteria for meeting the diagnostic classification of a mental health disorder by the PADOC are determined by a battery of psychometric tests designed to evaluate intelligence, achievement, personality, and emotional stability. In addition, members of the prison psychology staff administer the Personality Assessment Inventory (PAI; Morey, 2003), conduct interviews, and assess prior mental health histories (PADOC, 2004).
Classifications of mental health disorders range from any mental health disorder to serious disorders in which the inmate “has a substantial disorder of thought or mood which significantly impairs judgment, behavior, capacity to recognize reality, or cope with the ordinary demands of life” (PADOC, 2003, p. 1). Should the psychiatric staff diagnose an inmate with a mental health disorder meeting the DSM-IV diagnostic criteria, the inmate is placed on the Department’s Mental Health and Mental Retardation (MH/MR) Roster.
Substance abuse and dependence are assessed using the TCU Drug Screen II. The TCU Drug Screen II is used widely in criminal justice agencies nationally, and it has been extensively validated with inmate populations (Broome, Knight, Joe, & Simpson, 1996; Knight, Simpson, & Morey, 2002; Zajac, 2007). The TCU Drug Screen II is a standardized, 15-item screening instrument developed to identify individuals with a history of heavy drug/alcohol use or dependence in the past 12 months (in the case of inmates, the 12 months prior to their incarceration). Scores range from 0 to 9 with a score of 3 or greater indicative of substance dependence (Institute of Behavioral Research, Texas Christian University, 2009; Zajac, 2007). The clinical and diagnostic criteria for substance abuse or dependence in the TCU Drug Screen II are representative of those found in the DSM-IV and the National Institute of Mental Health Diagnostic Interview Schedule (NIMH DISC; Zajac, 2007).
Two criteria were used to form the COD group: (a) any inmate meeting the criteria specified above for a mental health disorder (e.g., placement on the MH/MR roster) and (b) clinical evidence of a substance use disorder (TCU Drug Screen II score of 3 or greater). Inmates not listed on the PADOC MH/MR roster and who scored less than 3 on the TCU Drug Screen II comprised the referent group (i.e., inmates with no disorders).
Covariates
Covariates (i.e., control variables) were selected based on empirical research on predictors of institutional misconduct. Age upon the current admission date to the PADOC was measured as a continuous variable with a range of 18 to 79 years. An inmate’s race was measured in four mutually exclusive categories as follows: 0 = White non-Hispanic (reference category), 1 = African American non-Hispanic, 2 = Hispanic, and 3 = Other. The “Other” category was defined by the PADOC and comprised 0.7% of the sample. Due to the small number of Native Americans and Asians in the sample (comprising less than 0.5% of the total sample), these cases were merged into the “Other” category. Grade level was examined as a continuous variable with a range of 4 to 18 (Grades 13 and above represented the number of years of college completed).
The study also examined standardized measures of intelligence as controls. IQ scores should provide a more valid measure of intelligence compared with completed grade level; maximum grade level could be a measure of multiple factors including socio-economic status. IQ tests are administered to inmates during intake classification. IQ scores have a mean of 100 and a standard deviation of 15 with average scores considered between 90 and 109 (Kaufman & Lichtenberger, 2006). IQ scores were coded as a continuous variable with a range between 60 and 153. The mean scores for the current study resembled those reported in the PADOC’s Corrections Education Outcome Study (Smith, 2005).
We also controlled for the reading level of inmates using scores from The Wide Range Achievement Test–Revised (WRAT-R). The WRAT-R is one of the most highly used screening instruments for evaluating learning disabilities (Kareken, Gur, & Saykin, 1995). The reading component of the WRAT-R converts scores to grade-level equivalents. These scores were coded as a continuous variable and ranged from illiterate to first year college. The mean reading level of our sample resembled those reported in the PADOC’s Education Outcome Study (Smith, 2005).
Criminal history was measured using the Criminal History subscale of the Level of Service Inventory–Revised (LSI-R), which is a 54-item actuarial classification instrument designed to assess criminogenic risk and need (Flores, Lowenkamp, Smith, & Latessa, 2006). The LSI-R is a standardized instrument that has been empirically validated on diverse samples of offenders (Andrews & Bonta, 1995). The Criminal History subscale (0-10) assesses the number of prior adult convictions, the number of current offenses, age of first arrest, prior incarcerations, escape history, institutional misconduct history, probation/parole violations, and history of violence.
This study also controlled for the inmate’s primary custodial institution. The primary institution for each inmate was based on the institution where they were incarcerated the greatest amount of time. This had the effect of removing other institutional locations where the inmate may have been temporarily housed for much shorter periods of time for classification, medical, security, or other reasons. The location variable was coded accordingly: 0 = SCI Muncy (reference category), 1 = SCI Cambridge Springs, and 2 = Quehanna Boot Camp. SCI Cambridge Springs is a minimum security facility and typically houses female inmates nearing their release date. SCI Muncy is classified as a close security prison responsible for housing all female inmates incarcerated for capital offenses. Quehanna is a military style motivational boot camp classified as a minimum security facility, housing both men and women (PADOC, n.d.).
Length of incarceration was measured as a continuous variable in months (range = 4-33 months). To compute this variable for inmates who were already discharged, the date of admission was subtracted from the date of discharge and converted to months. Incarceration length for inmates still actively serving their sentence was computed by subtracting their admission date from the date of the data run and converted to months.
Because time in treatment may reduce time at risk for committing misconduct, as well as potentially curb misbehavior, this study controlled for time in treatment. Studies examining the time needed to affect post-treatment outcome suggest that a minimum temporal threshold must be met before clients begin to show favorable outcomes (NIDA, 2007; Taxman, Perdoni, & Harrison, 2007). Because duration in treatment has been found to be an important indicator of post-treatment outcome, retention rates may be an important proxy for therapeutic engagement and compliance with the program. Longitudinal studies suggest that a minimum 3-month threshold is needed before clients begin to show favorable outcomes (see Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997; Sells & Simpson, 1980). Because of the strong empirical support for minimum temporal thresholds, we coded treatment exposure as a categorical variable reflecting 3-month intervals (0 = no time in treatment, 1 = 1-90 days, 2 = 91-180 days, and 3 = 181 days or more). Treatment exposure was calculated by subtracting the date of admission to the treatment program from the date of discharge. Treatment exposure for inmates who were still actively participating in treatment at the time of the data run was created by subtracting the date of admission to the program from the date of the data run. The total time in treatment per inmate was summed and converted to days. Due to restrictions of the Health Insurance Portability and Accountability Act (HIPAA), we were unable to obtain specific treatment program information. Inmates may have participated in additional programs not limited to substance use or mental health programs. In addition, inmates may have participated in more than one program during their incarceration. Therefore, time in treatment included all programs that inmates may have participated in.
Analyses
An initial bivariate analysis of the relationship between disorder type and misconduct was conducted (any misconduct vs. no misconduct). Following the bivariate analysis, we estimated a logistic regression model for the dichotomous measure of institutional misconduct to determine whether differences in the probability of prison misconduct among female inmates with mental illness, CODs, and/or substance use disorders persisted net of statistical controls.
Results
Univariate Analysis
An initial univariate analysis of the final sample revealed some missing data, though no single variable accounted for a large proportion of missing cases. Comparisons of the total eligible sample (maximum n = 1,766) with the final sample using listwise deletion (n = 1,470) were undertaken using one-sample t tests (Table 1). Mean differences were very small, although 4 of 17 mean comparisons were statistically significant. Due to the large sample size and the number of comparisons, some differences were expected (Tabachnick & Fidell, 2006). As a result, some caution in generalizing the results to all female offenders in the state of Pennsylvania is required.
Descriptive Statistics for Total Sample and Final Sample Using Listwise Deletion
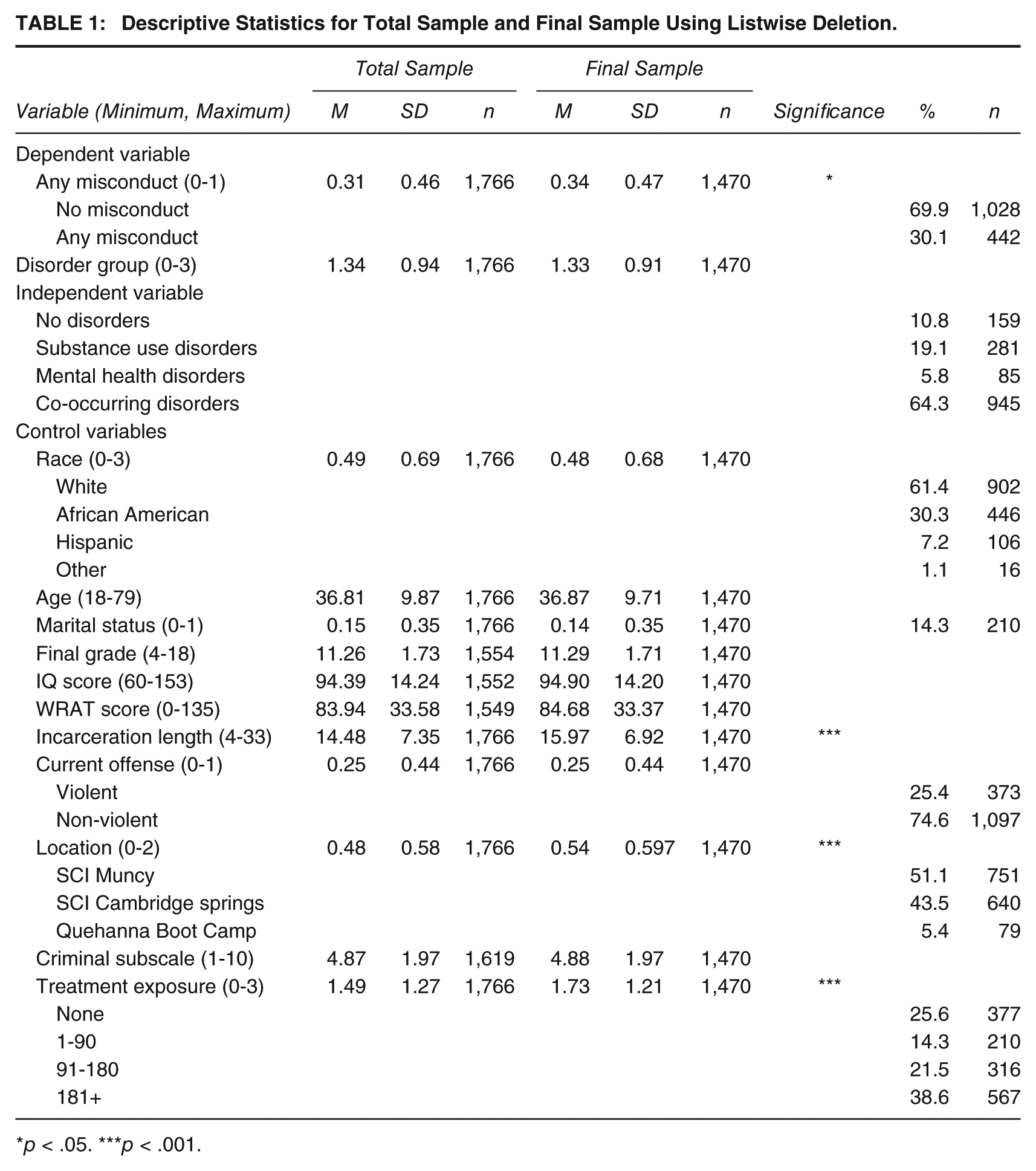
p < .05. ***p < .001.
Table 1 provides the distribution of the dependent and independent variables and covariates, as well as the mean comparisons between the total and final sample. Supporting prior research, the majority of women in our study were not charged with any form of misconduct (69.9%). Examination of disorder classification revealed that greater than half (64.3%) of the women met the criteria for CODs, 19.1% met criteria for a substance use disorder only, 5.8% were diagnosed with a mental illness but exhibited no substance use problem, and 10.8% of the sample did not meet the criteria for either a mental health or substance use disorder. More than half of the women were White non-Hispanic (61.4%) with 30.3% African American non-Hispanic. The average age of the women in the study was 36.8 years old with only 14% married at the time of incarceration.
The mean education level of the women was 11th grade with an average IQ score of 94.9, which would place most of the women in the average intelligence category. WRAT scores showed the average reading level to be eighth grade. At the time the data were collected for this study, 23.5% of the women had been discharged with an average length of incarceration of 15.9 months. Twenty-five percent of the sample had at least one violent offense conviction for which they were currently serving prison time. As expected, most of the women were primarily housed at SCI Muncy and SCI Cambridge (51.1% and 43.5%, respectively) with only 5.4% housed at Quehanna Boot Camp. The average score for the Criminal History subscale of the LSI-R was 4.8 (range = 1-10). Among women who received treatment during the current incarceration, 38.6% received 180 days or more. Approximately 14% of the inmates received between 1 and 90 days of treatment and 21.5% had between 91 and 180 days of treatment. At the time of data collection, 25.6% of the sample reported receiving no treatment.
Bivariate Analysis
Rates of misconduct were highest among female inmates with mental health disorders only (34.1%), followed by inmates with CODs (32.9%), inmates with substance use disorders only (26.7%), and last, inmates with no disorders (17%). We see, therefore, that women with mental health disorders or CODs were approximately twice as likely to be charged with an infraction as women with no disorders. Although inmates with substance use disorders only were more likely to be involved in misconduct than inmates with no disorders, they were not as likely to be charged with misconduct as women with mental health disorders or CODs.
Logistic Regression
Results from the logistic regression analysis (Table 2) showed that differences in the likelihood of having any form of prison misconduct among female inmates with CODs or mental health problems persisted net of statistical controls. Relative to women with no disorders, the odds of any prison misconduct were 2.2 times greater for inmates with mental health problems and 2.4 times higher for inmates with CODs. Although not statistically significant, estimates suggested that the effect appeared stronger among women with CODs than for those with mental illness only (based on the log odds ratio). Relative to those with no disorders, women with substance use disorders only were not significantly more or less likely to engage in prison misconduct.
Logistic Regression of Prison Misconduct on Control and Predictor Variables

Note. The coefficients for the independent variables that exerted a statistically significant effect on the dependent variable are given in boldface. χ2 (19, n = 1,470) = 331.389***; −2 log likelihood = 1466.243; Nagelkerke R2 = 286.
p < .05. ***p < .001.
With regard to the effects of other variables in the analysis, for every additional month an inmate remained incarcerated, their likelihood of being involved in misconduct increased by 11%. Relative to inmates housed at SCI Muncy, women housed at either SCI Cambridge Springs or Quehanna Boot Camp were significantly less likely to be charged with any misconduct (51% and 58%, respectively). Findings further showed that for every year older, an inmate was 5% less likely to be involved in misconduct.
Being married at the time of incarceration was neither found to be significantly related to an inmate’s likelihood of being charged with a prison rule violation nor was their IQ or reading level. Level of educational achievement was, however, significantly related to prison misconduct such that the more education women received, the less likely they were to be charged with misconduct. Race was also significantly related to misconduct, with African American women being 1.9 times more likely to be charged with an infraction compared with White non-Hispanic females.
Findings further revealed that women convicted of a violent offense were neither more nor less likely to be charged with misconduct compared with women convicted of non-violent offenses. Relative to their criminal history, however, the model shows that with each increase in an inmate’s Criminal History subscale score, the odds were 1.2 times greater of being charged with misconduct. Treatment exposure for 1 to 90 days or 91 to 180 days was not found to influence an inmate’s likelihood of being charged with a prison rule violation. However, women who were exposed to a minimum of 181 days were 34% less likely to be involved in a prison infraction.
Discussion
The high prevalence of mental illness and CODs among the female correctional population creates concern among practitioners for maintaining order and safety (Serin, 2005), as well as potentially hindering their ability to provide other organizational services including treatment (O’Keefe & Schnell, 2007). Although there is mounting awareness of the challenges that mentally ill inmates confront in conforming to the structure of the prison setting (see Adams, 1983, 1986; Houser et al., 2012; James & Glaze, 2006; O’Keefe & Schnell, 2007; Steiner & Wooldredge, 2009; E. M. Wright et al., 2007), our understanding of the clinically interactive nature of CODs on inmate behavior is limited (Wexler, 2003).
The current study expanded upon extant literature on the association between mental illness and institutional misconduct by creating clinically distinct disorder groups. Using clinically distinct disorder groups allowed an examination of the independent effects of mental illness, substance dependence, and CODs on inmate misconduct. This study also furthered our understanding of the clinically interactive nature of comorbid psychiatric and substance use disorders on inmate misconduct compared with single disorders.
At the outset of this study, we proposed two hypotheses: Inmates with mental health disorders only or CODs will have higher odds of misconduct compared with inmates with substance use disorders only; and inmates with CODs will be more likely to engage in misconduct compared with inmates with singular diagnoses of mental illness or substance use disorders. The results of the regression model indicated that female inmates with a mental health disorder or a COD were significantly more likely than those with no disorders to be charged with institutional infractions after controlling for other predictors of prison misconduct. Inmates with substance use disorders only were neither more nor less likely to be charged with a prison infraction than those with no disorders. These findings support our first hypothesis and prior research suggesting that inmates with mental illness and CODs are more likely to engage in rule-violating behaviors. Results of the regression model also suggested that the effect appeared stronger among women with CODs than those with a singular diagnosis of mental illness (based on the log odds ratio), though the differences were not statistically significant. Although this difference was in the expected direction, our second hypothesis that the interactive nature of CODs on inmate behavior creates additional challenges for mentally ill inmates was not confirmed.
Additional findings showed that younger inmates and African Americans were more likely to engage in prison misconduct. Lower educational achievement and more extensive criminal histories were also significantly associated with increased rates of rule-violating behaviors. Although educational achievement was positively associated with higher rates of infractions, IQ scores and reading levels were not found to be significant predictors of misconduct. An inmate’s marital status at the time of incarceration was also found to be non-significant in predicting prison misconduct.
Implications of Findings
Our findings suggest that mental health disorders may hamper the ability of female inmates to successfully conform to the rules and policies of correctional institutions. Our findings further suggest that when a substance use disorder interacts with a psychiatric illness, the inmate’s capacity to adhere to prison regulations may be further compromised. This is not surprising because the interactive nature of CODs often worsens the symptomatic character of the individual disorders. Hence the negative behavior exhibited by the mentally ill inmate is augmented by the addition of a substance use disorder. For the mentally ill and COD inmate, typical forms of social control within correctional institutions, including the threat and use of sanctions, may be ineffective or even inhumane as rule abiding behavior may not be within their control.
Findings from this study further reinforce the importance of screening instruments in the correctional setting designed to assess CODs. Proactive measures to accurately assess, treat, and respond to inmates with CODs may serve to reduce prison misconduct, thereby increasing safety and reducing costs within the institutions. With prisons assuming a dual role of incarceration and providing treatment, the need for more integrated treatment programs (integrated treatment designs employ cross trained and certified professionals familiar with dual disorders treating each individual disorder as primary within the same treatment setting) to respond to the needs of COD inmates, and staff trained on the complexities of dual diagnoses is essential. National surveys estimate that only 34% of state prison inmates (both male and female) with a mental health disorder receive mental health treatment after their admission (James & Glaze, 2006). Treatment for the COD inmate is likely no better, and perhaps worse, due to the limited number of integrated treatment programs available in correctional institutions (Peters et al., 2004). Thus, many mentally ill and COD inmates may return to their communities with minimal mental health or integrated COD treatment.
Although this study furthers our understanding of the policy implications of COD within the offender population, some limitations must be addressed. This was a cross-sectional sample of female inmates limited to one geographic location, Pennsylvania. Therefore, caution should be exercised in generalizing these findings to be reflective of all female state prison inmates or all inmates with mental illness, substance use disorders, or CODs. However, there are several benefits to conducting a study in a single state. All inmates included in this research were sentenced under the same state law; they were all assessed using the same procedures, and they were all subject to the same policies of the same state Department of Corrections.
A second limitation concerns the use of the TCU Drug Screen II as the single instrument for screening alcohol and/or drug abuse or dependence. Although this screening instrument distinguishes alcohol and drug usage, the current study only had the final TCU Drug Screen II score and therefore was not able to distinguish between drug use disorders and alcohol use disorders or whether an inmate was considered to have problems with both. In addition, because the TCU Drug Screen II is designed only as a screening instrument, results of the screening should serve to establish the need for further assessment of substance abuse or dependence. Therefore, this study was not able to assess if specific substance use disorders were more problematic than others or interacted differently for inmates with COD. Although the TCU Drug Screen II has been extensively validated with inmate populations (Knight et al., 2002; Zajac, 2007), it is still a self-reported screening instrument. As such, some concerns include inmate recollection that could reduce accuracy and the potential of either under- or over-reporting on the part of the respondent.
Due to restrictions regarding dissemination of confidential personal information under HIPAA, several types of information were not available. For example, we could not access specific medical information for inmates including medication usage, type and dosage, or specific medical diagnoses. For the same reasons, we could not access information on the specific treatment modality that inmates received, although we were able to control for overall treatment exposure (number of days). Different types of treatment programs may vary in their focus, methods, and intensity. In addition, facility and staff-level data were not available, which precluded analyses of the effects of facility-specific variables or staff-specific variables on institutional misconduct.
An additional limitation relates to the validity and reliability of officially gathered misconduct data. Light (1990) provides a detailed description of these issues based on a critical review of the literature. Concerns with official data are often in regard to correctional officer discretion, variations in definitions of events, possible effects of participant characteristics, jurisdictional effects, temporality, and other environmental/contextual influences. However, the best way to further explore such factors in depth would be to conduct additional studies that include detailed qualitative examinations of individual cases and case processing characteristics. Such an examination was beyond the scope and resources of this study.
The current study used the PADOC MH/MR roster as the criteria for a diagnosis of a mental health disorder. However, it was not possible to distinguish whether an inmate was placed on the roster for a mental health diagnosis or mental retardation. Although the current study was not able to differentiate inmate diagnoses, examination of the sample revealed the lowest IQ score to be 60 with 1.7% of the sample having IQ scores below 70, suggesting possible mild mental retardation. In addition, each inmate in the study who was on the MH/MR roster had a corresponding DSM-IV mental health diagnosis. Therefore, even if an inmate in the study was deemed to have mild mental retardation, they were also considered to have a mental health disorder.
Conclusion
The current results support findings of prior research showing mental illness as an important risk factor of prison misconduct. The results further suggest that the addition of a substance use disorder exacerbates the risk of negative behaviors beyond a singular mental health disorder. The clinically interactive nature of CODs may present increased security and management challenges for correctional administrators. These findings reinforce the importance of dual disorder screening instruments designed for use in the correctional setting. Correctional institutions must also move toward the use of integrated treatment modalities to more effectively meet the treatment needs of a growing COD offender population.
Future research is needed to further our understanding of the complexity of CODs on women in the criminal justice system. This includes replicating and expanding our findings on different samples, studying the assessment process for female inmates, and examining the interaction of treatment modalities by disorder type on inmate misconduct. Female offenders often have unique pathways into the criminal justice system, along with higher rates of mental illness, drug use, and CODs compared with males; yet, they remain a vastly understudied population in criminal justice research and the misconduct literature.
Footnotes
Acknowledgements
The authors gratefully acknowledge the valuable contributions of the Research and Evaluation Department of the Pennsylvania Department of Corrections (PADOC) in providing access to their data, as well as their input and advice throughout this project. In particular, Gary Zajac, former Chief of Research and Evaluation for the PADOC; Kristofer Bucklen, Chief of Research and Evaluation for the PADOC; Michael Antonio; and Nicholas Scharff, Chief of Clinical Services for the PADOC. We also extend thanks to our colleagues, Steven Belenko and Matthew Hiller who both provided guidance for this article.
Opinions expressed are those of the authors. The authors alone take full responsibility for errors or omissions that may have been made.
A preliminary version of this article was presented at the Annual Meeting of the American Society of Criminology, Washington, DC, November, 2011.