
Abstract
Posttraumatic stress disorder (PTSD) is a potentially important, yet understudied, mental disorder to consider in models of criminal recidivism. The present study sought to address this gap in the literature with a large-scale secondary analysis of observational data from a sample of justice-involved persons with mental disorders. Administrative data were reviewed for 771 adult jail detainees with mental disorders. Hierarchical logistic regression models showed that PTSD was associated with a greater likelihood of general (arrest for any new charge) and serious (arrest for a new felony charge) recidivism during the year following the index arrest, after controlling for risk conferred by a recent history of arrest, demographic characteristics, and other mental disorders. Furthermore, risk of rearrest for new charges was comparable for PTSD and substance use disorders. Findings show that PTSD increases risk of both general and serious recidivism and suggest it should be considered in interventions to reduce justice-system involvement.
According to the U.S. Department of Justice, approximately 60% of jail inmates have a mental health problem (James & Glaze, 2006). A large-scale study using structured diagnostic interviews reported that 14.5% of male and 31.0% of female jail inmates meet criteria for a serious mental disorder (Steadman, Osher, Robbins, Case, & Samuels, 2009). These data highlight the widely recognized overrepresentation of individuals with mental disorders in jails (Condelli, Dvoskin, & Holanchock, 1994; Dvoskin, Skeem, Novaco, & Douglas, 2012) and the importance of understanding how mental illness confers risk of criminal offending and recidivism (Constantine et al., 2010). Understanding how mental disorders influence risk of recidivism could help guide the development of interventions to reduce involvement of persons with mental illness in the criminal justice system (Scott, McGilloway, Dempster, Browne, & Donnely, 2013).
Persons involved in the criminal justice system and those with mental disorders are at significantly higher risk of trauma exposure and development of Posttraumatic Stress Disorder (PTSD) compared with the general population (Choe, Teplin, & Abram, 2008; Goff, Rose, Rose, & Purves, 2007; Maxfield & Widom, 1996; Mueser et al., 1998; Teplin, McClelland, Abram, & Weiner, 2005). The high rates of trauma exposure among individuals involved in the criminal justice system suggest that PTSD may be an important risk factor for justice-system involvement and criminal recidivism. Indeed, PTSD and victimization experiences have been associated with increased rates of violent behavior and drug use (Chilcoat & Breslau, 1998; MacManus et al., 2012; Sullivan & Elbogen, 2014), including among justice-involved persons with mental illness (Sadeh, Binder, & McNiel, 2014). Trauma exposure is especially common among female offenders, with incarcerated women exhibiting higher rates of PTSD than incarcerated men (Goff et al., 2007). Furthermore, there is growing evidence that a history of trauma exposure is a key risk factor for justice-system involvement and antisocial behavior in women and girls (Javdani, Sadeh, & Verona, 2011). Thus, research has linked PTSD with a history of justice-system involvement and behaviors that increase contact with the criminal justice system (e.g., violence, drug use).
In military populations, cross-sectional research has shown that rates of criminal offending are higher in veterans with a PTSD diagnosis than those without (Elbogen et al., 2012; Wilson & Zigelbaum, 1983). Studies of PTSD in civilian samples where trauma exposure may be less salient to mental health providers also suggest that the disorder covaries with criminal arrests (Collins & Bailey, 1990; Donley et al., 2012; Kubiak, 2004; Peller, Najavits, Nelson, LaBrie, & Shaffer, 2010). For example, a cross-sectional study of 1,140 incarcerated males found that PTSD was positively associated with current or previous incarceration for a violent offense (Collins & Bailey, 1990). Similarly, a sample of 4,113 adults recruited from the general community found that PTSD was correlated with higher rates of self-reported contacts with the criminal justice system (Donley et al., 2012).
Two longitudinal treatment studies specific to individuals with substance-related offenses also found that PTSD increases risk of rearrest. Specifically, a 1-year prospective study of 729 adults charged with driving under the influence (DUI) who were admitted to a 2-week inpatient program found that PTSD increased risk of rearrest for DUI (Peller et al., 2010). PTSD diagnosis also correlated positively with new bookings over a 12-month period in a sample of 183 men who were recruited based on a history of substance-related charges and substance dependence (Proctor, Hoffmann, & Allison, 2012). Our literature review identified no longitudinal studies that examined the relationship of PTSD with criminal recidivism in samples of justice-involved persons characterized by a range of mental disorders.
Theoretical models posit that PTSD increases risk of criminal behavior partly through the use of substances to cope with the psychological and biological sequelae of trauma exposure. Specifically, “self-medication” via substance abuse is theorized to function as a mechanism for attenuating untreated symptoms of PTSD (Chilcoat & Breslau, 1998; Leeies, Pagura, Sareen, & Bolton, 2010), as well as changes in physiological reactivity and other biological systems that regulate the stress response (Norman et al., 2012). In addition, prospective research suggests that a history of alcohol and drug use increases risk of the development of PTSD (Breslau, Troost, Bonhert, & Luo, 2013), and behavioral genetics research suggests that substance use disorders and PTSD share common genetic risk factors (Sartor et al., 2011). Other overlapping features of PTSD and substance use disorders include hypersensitivity to environmental stressors (Sinha, 2008) and high levels of negative emotionality and dysconstraint (Elbogen et al., 2012; Miller, Vogt, Mozley, Kaloupek, & Keane, 2006). These theories are consistent with the high rates of substance use disorders among individuals with PTSD (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Some research suggests that severe mental illness does not predict violence unless substance abuse/dependence is comorbid (Elbogen & Johnson, 2009), although others have reported that mental illness increases risk above and beyond substance use (Arseneault, Moffitt, Caspi, Taylor, & Silva, 2000; Swanson, Borum, Swartz, & Monahan, 1996; Van Dorn, Volavka, & Johnson, 2012; Volavka & Swanson, 2010). The association between PTSD and recidivism risk is not examined in these studies, and whether PTSD contributes uniquely to criminal recidivism above the risk conferred by substance use disorders remains an unresolved and important research question.
Based on the literature reviewed, the present study tested the hypothesis that PTSD increases the risk of rearrest for new criminal charges in the 12 months following arrest in a sample of justice-involved adults with mental disorders. We conducted secondary analysis of observational data to test this hypothesis and examined whether the diagnostic information available to clinicians at the time of the index arrest showed hypothesized relationships with criminal recidivism. We used clinical diagnoses (the diagnostic information gathered by clinicians at the time of booking into jail) rather than research diagnoses (systematic evaluation of PTSD symptoms using a structured interview or self-report questionnaire), because this approach allowed us to evaluate the diagnostic utility of routine evaluation procedures in jail settings. Specifically, we wanted to assess whether the clinical information gathered during triage assessments, which are most pertinent to clinical decision making in jail settings, can be used to assess recidivism risk.
A large body of research has linked risk of criminal recidivism to demographic variables including age and gender (Bonta, Law, & Hanson, 1998), as well as a history of antisocial behavior (e.g., criminal activity), substance use disorders, and antisocial personality patterns, among others (Dvoskin et al., 2012; Monahan et al., 2001). To assess whether PTSD is an important factor to consider in models of risk, we examined how it relates to criminal recidivism above and beyond these risk factors as well as other mental health disorders. We first tested the association of PTSD with criminal recidivism using a measure of general criminal recidivism, which we operationalized as a new arrest for any charge. We also examined its association with more serious forms of recidivism, namely, new felony arrests, to determine whether any findings for general recidivism generalized to more serious felony arrests.
Method
Participants and Procedures
All 8,325 men and women who entered the San Francisco jail system from January 14, 2003 to November 19, 2004 and were diagnosed with a mental disorder were eligible for the study. The study sample included all individuals who met criteria for a diagnosis of PTSD (n = 201), and a comparison group was constructed by randomly selecting 600 individuals from the larger study population. Individuals in the study sample did not differ from the population on any of the covariates or explanatory variables, with the exception of PTSD and female gender. PTSD was purposely oversampled, which likely increased the proportion of women in the study sample compared with the larger study population. However, consistent with the population characteristics, there were fewer women in the study sample than men.
Only participants with complete data were included in analyses (excluded for missing 12-month outcome data: n = 30), resulting in a final sample of 771 justice-involved male (72%) and female (28%) adults (ages 18-84, M = 38.4, SD = 11.3) with mental disorders. Individuals without outcome data did not differ from those included in the study on any of the covariates or explanatory variables. Descriptive characteristics of the sample are presented in Table 1. This project represents secondary analysis of a data set collected in a previous study (McNiel & Binder, 2007), which did not examine the relationship of PTSD with criminal recidivism.
Descriptive Statistics for the Total Sample and by PTSD
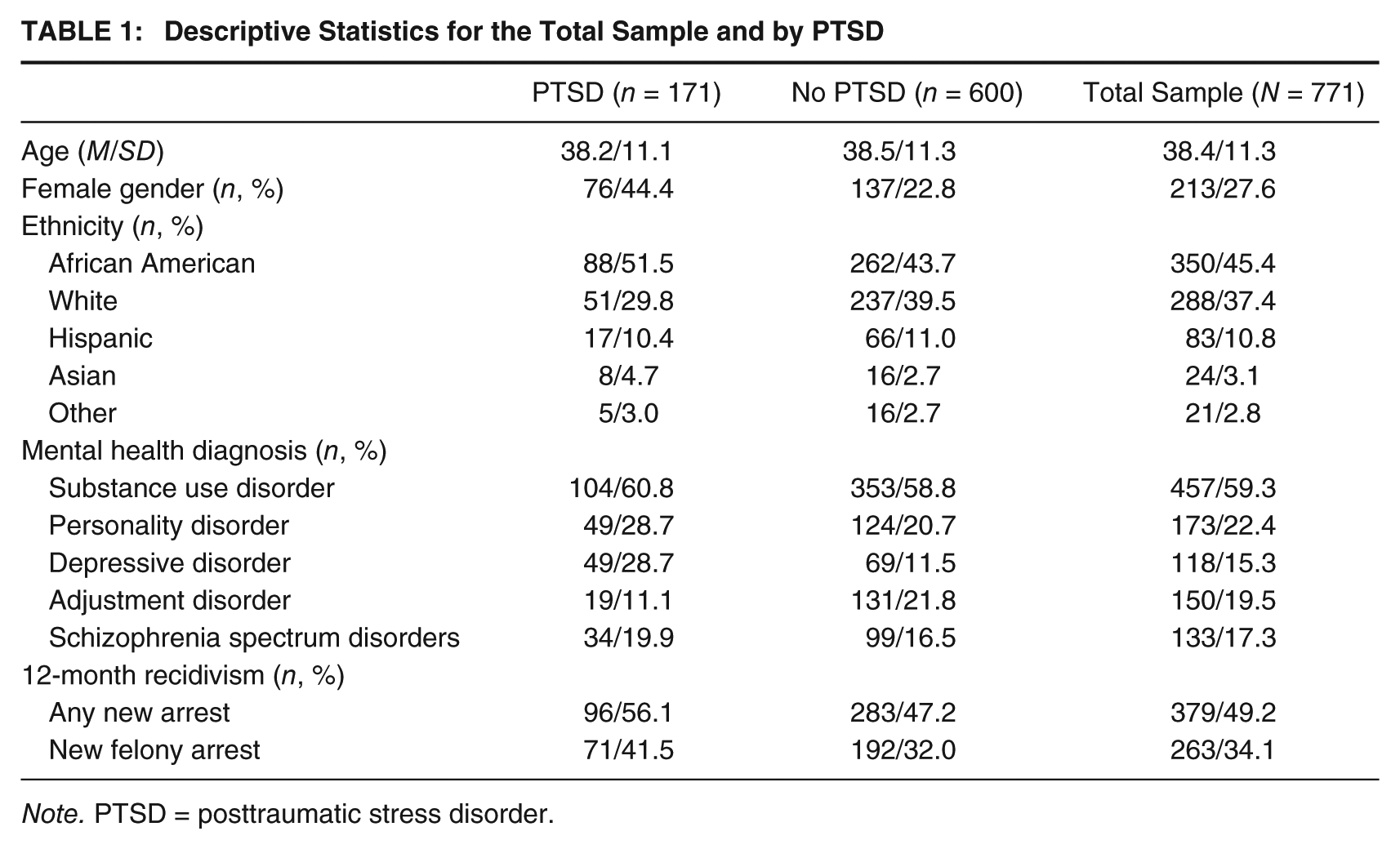
Note. PTSD = posttraumatic stress disorder.
Data were collected by reviewing de-identified administrative databases from the San Francisco county court and jail systems. Study procedures were approved by relevant institutional review boards, who determined that informed consent was not necessary due to the de-identified nature of the data.
Measures
Psychiatric Diagnosis
Each participant’s diagnostic status was determined by a medical screening conducted by jail psychiatric services; the prevalence of psychiatric disorders (allowing for comorbidity) in the sample is presented in Table 1. Participants were first screened by a registered nurse on entering the jail and then underwent a more detailed medical screening 1 to 2 hr later by a second nurse. If the initial screens conducted by nursing staff were positive for a possible mental health problem, participants were referred to mental health staff for further evaluation. The clinical diagnoses were made by a mental health professional using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) criteria. PTSD was diagnosed in 22.2% of the study group, and a diagnosis of PTSD was entered as the main explanatory variable in analyses. Other mental health diagnoses, specifically substance use disorders, personality disorders, depressive disorders, and schizophrenia spectrum disorders were included as covariates in analyses to assess whether PTSD increased risk of recidivism above the risk already accounted for by these variables.
Criminal Recidivism
Criminal recidivism was examined using two outcome variables: general criminal recidivism and serious criminal recidivism. These variables were based on arrests for new charges, and did not include technical violations.
General criminal recidivism was operationalized as rearrest for any new charge during the 12 months after the index arrest. We created a dichotomous general criminal recidivism variable that reflected the presence (coded 1) or absence (coded 0) of an arrest for a new charge in the 12 months following the participant’s first arrest between January 14, 2003, and November 19, 2004 (any new charge present = 49%; any new charge absent = 51%).
To determine whether study findings were also relevant for serious forms of criminal recidivism, we also examined felony charges as defined by the California penal code. Rearrest in the 12 months following the index arrest was established for each participant and used as an outcome measure of felony recidivism. We created a dichotomous felony recidivism variable that reflected the presence (coded 1) or absence (coded 0) of a new charge for a felony offense in the 12 months following the participant’s first arrest between January 14, 2003, and November 19, 2004 (new felony charge present = 34%; new felony charge absent = 66%).
Time at risk in the community varied across the sample. The mean number of days in jail for the sample was 20 (SD = 37.6), approximately 50% of the sample were released on the day of their index offense, and 80% spent less than 1 month in jail. Supplementary analyses indicated that the number of days in jail during the year following the index arrest did not reduce the likelihood of rearrest (days in jail were positively correlated with rearrest for any new offense and a new felony charge, rs = .43 and .47, respectively).
Recent History of Arrest
History of arrest prior to the index arrest was also measured and used as a covariate in analyses. First, we created a measure of general arrest history, which we defined as the presence (coded 1) or absence (coded 0) of an arrest in the 6 months prior to the participant’s index arrest (first arrest between January 14, 2003, and November 19, 2004). We used a dichotomous variable to parallel the criminal recidivism outcome variable. Ninety-two percent of the sample had an arrest in the 6 months prior to the index arrest. This variable was entered as a covariate in analyses to test whether PTSD increased risk of new bookings above the risk captured by arrest history. Second, we created a measure of prior felony charges, which we defined as the presence (coded 1) or absence (coded 0) of a charge for a felony offense in the 6 months prior to the participant’s index arrest (first arrest between January 14, 2003, and November 19, 2004). Sixty-three percent of the sample had an arrest for a felony charge in the 6 months prior to the index arrest. This variable was entered as a covariate in analyses to test whether PTSD increased risk of new felony charges above the risk captured by felony arrest history.
Statistical Analysis
First, we examined the relationship of PTSD with the outcome variables using logistic regression analyses. Next, we constructed hierarchical logistic regression models to test the predictive power of PTSD in a multivariate model by creating separate blocks of predictors that represent categories of risk factors for recidivism. These predictors were grouped conceptually and entered as follows: recent history of arrest in Block 1, demographic information in Block 2, and other mental health diagnoses in Block 3. We then entered PTSD in Block 4 to test whether it explained additional risk in recidivism above these other variables. Finally, in Block 5, we entered the interaction of PTSD and substance use disorders to examine their comorbidity. Chi-square statistics for the full models and each block of the hierarchical regression analyses are presented in Tables 2 and 3 as measures of how well the models fit the data. Cox and Snell r2 values and odds ratios (OR) were calculated to provide measures of effect size and are also included in Tables 2 and 3. A small subset of the final sample (1.9%) was enrolled in a mental health court during the year following the index arrest. Supplemental analyses indicated that inclusion of a variable representing mental health court participation did not moderate the study findings or produce new findings; consequently, this variable was not included in the final model. We tested for and did not find multicollinearity problems, as evidenced by tolerance levels within the acceptable range (tolerance level > .80; Gaur & Gaur, 2006). Predicted probabilities from the hierarchical logistic regression analyses are displayed in Figures 1 and 2 to illustrate the relative probability of rearrest during the year following the index arrest for PTSD and substance use disorders. We included these data, because we were interested in describing the unique probabilities associated with rearrest as a function of PTSD, substance use disorders, and their comorbidity. All analyses were conducted with SPSS Version 20 (SPSS, Chicago, IL).
Hierarchical Logistic Regression Analysis of Posttraumatic Stress Disorder Predicting Any New Arrest in the 12 Months After the Index Offense (N = 771)
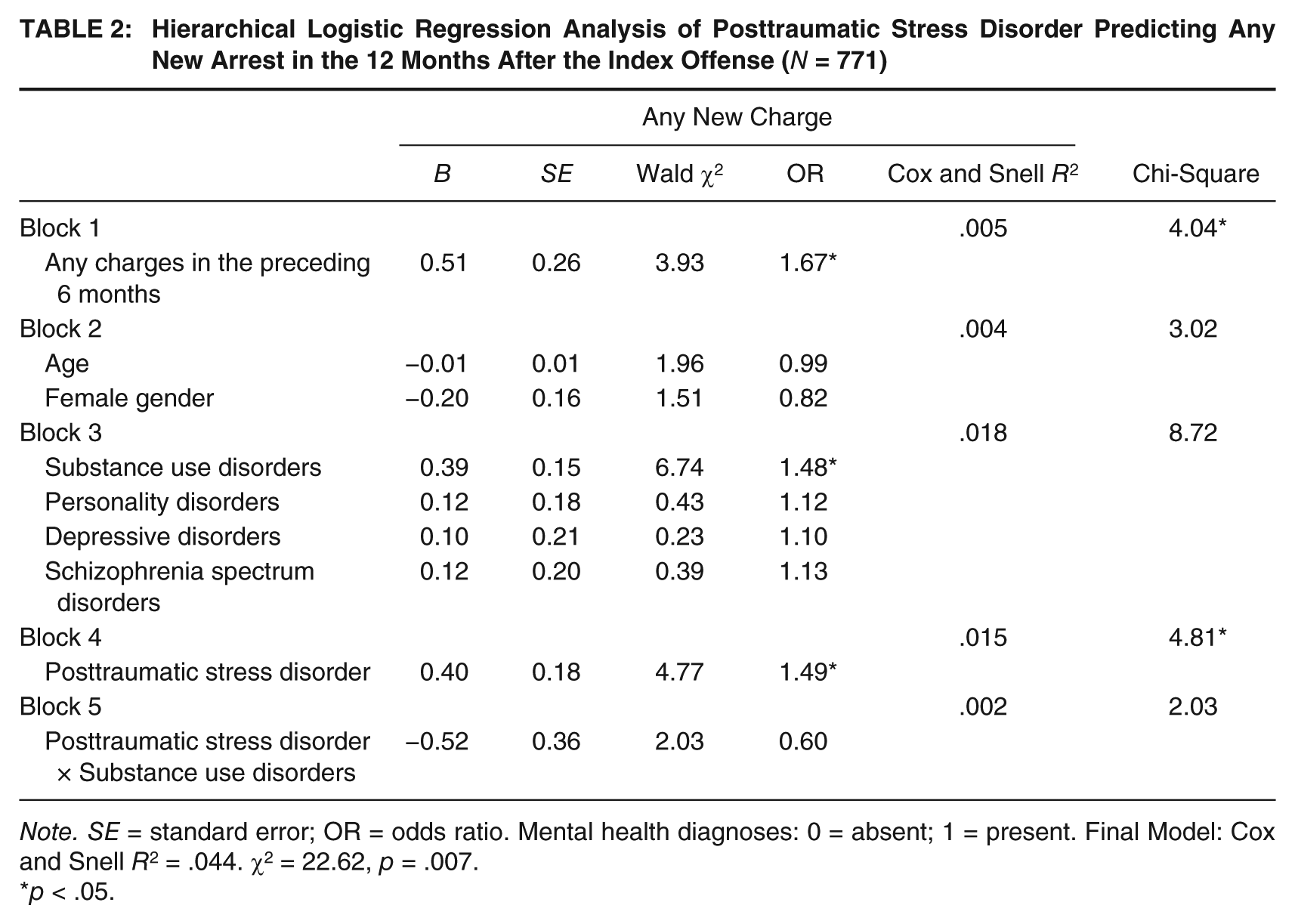
Note. SE = standard error; OR = odds ratio. Mental health diagnoses: 0 = absent; 1 = present. Final Model: Cox and Snell R2 = .044. χ2 = 22.62, p = .007.
p < .05.
Hierarchical Logistic Regression Analysis of Posttraumatic Stress Disorder Predicting Risk of a New Felony Arrest 12 Months After the Index Offense (N = 771)
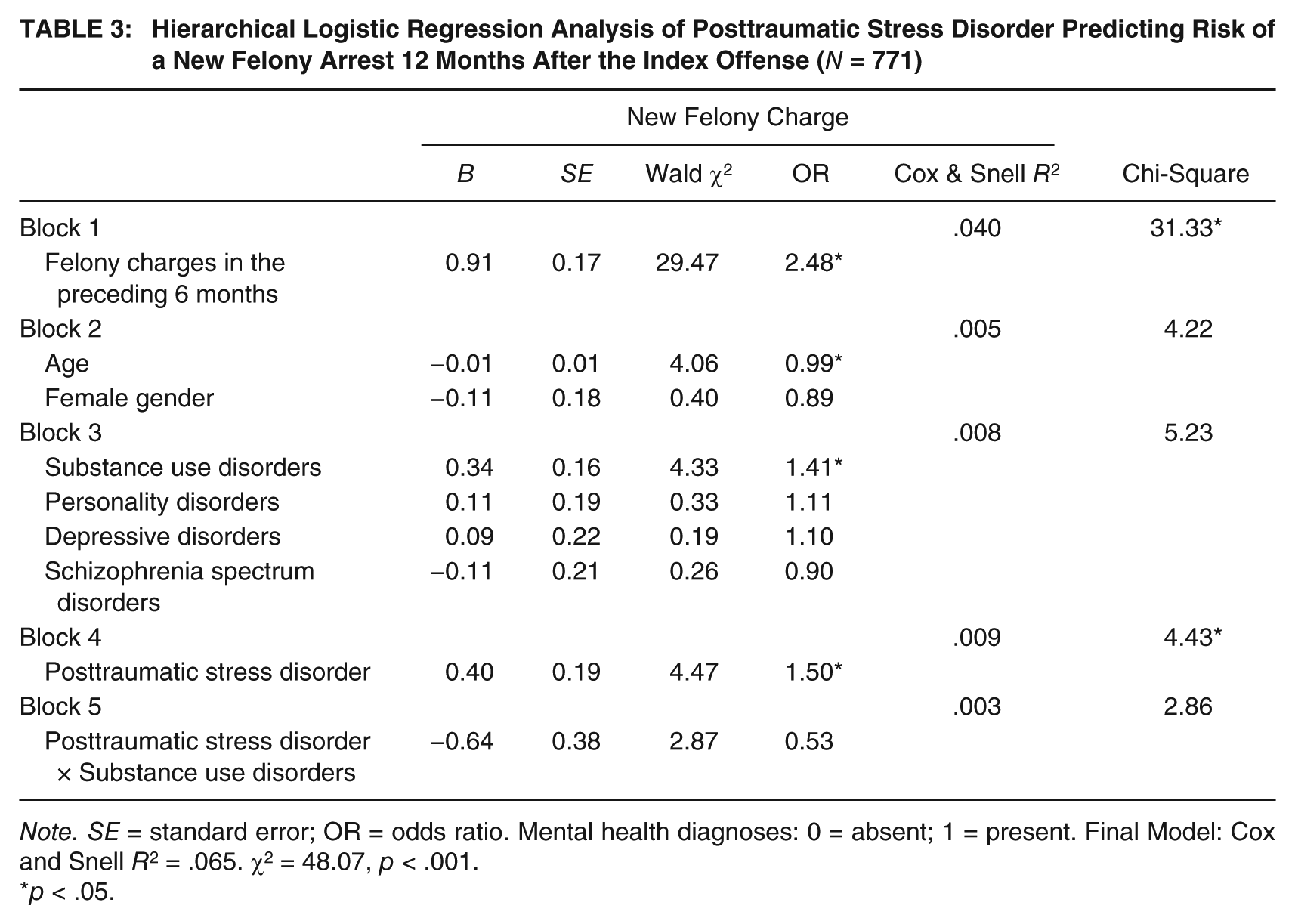
Note. SE = standard error; OR = odds ratio. Mental health diagnoses: 0 = absent; 1 = present. Final Model: Cox and Snell R2 = .065. χ2 = 48.07, p < .001.
p < .05.
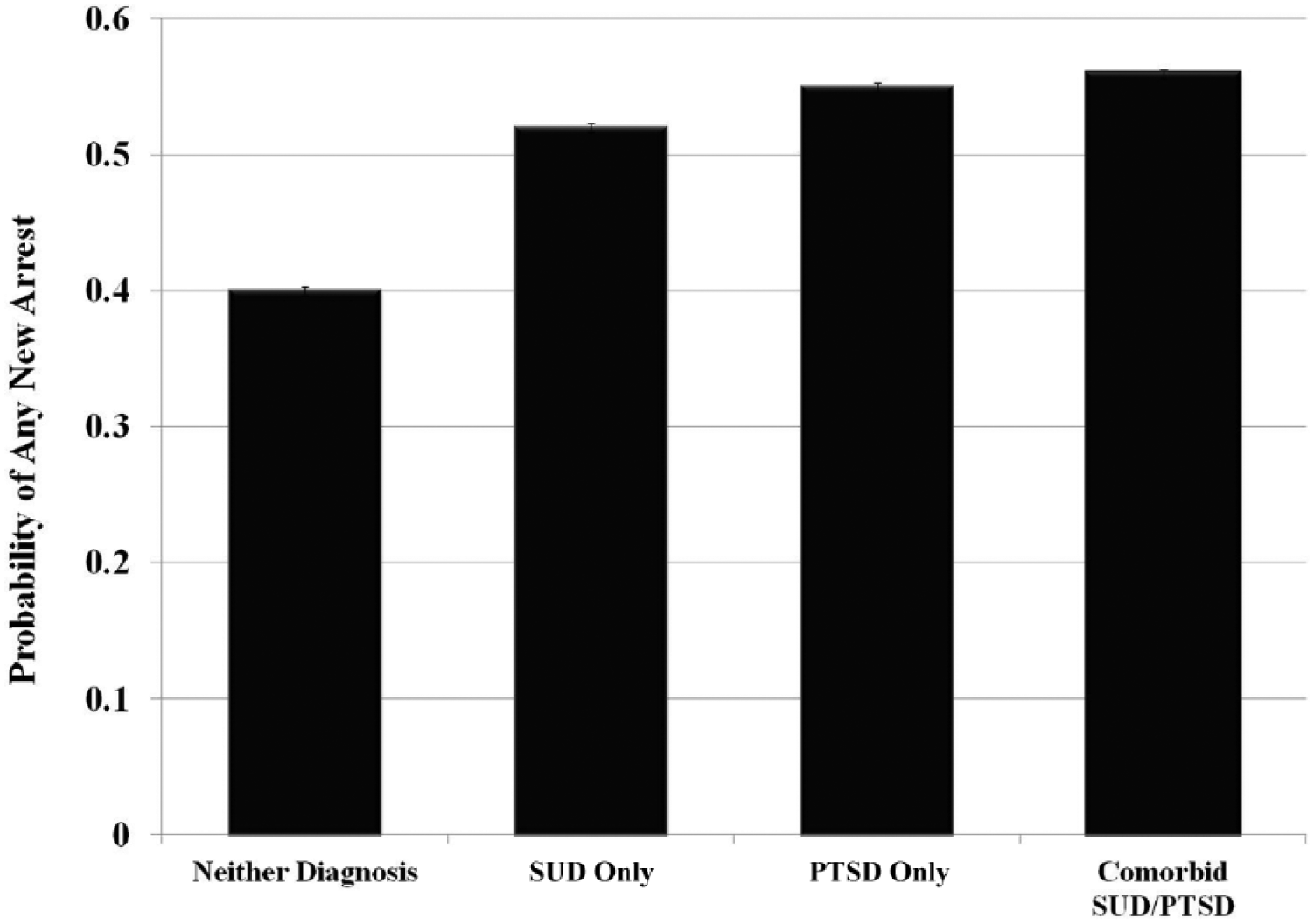
Predicted Probability of Any New Charge During the 12 Months After the Index Arrest by PTSD and SUD Diagnostic Status
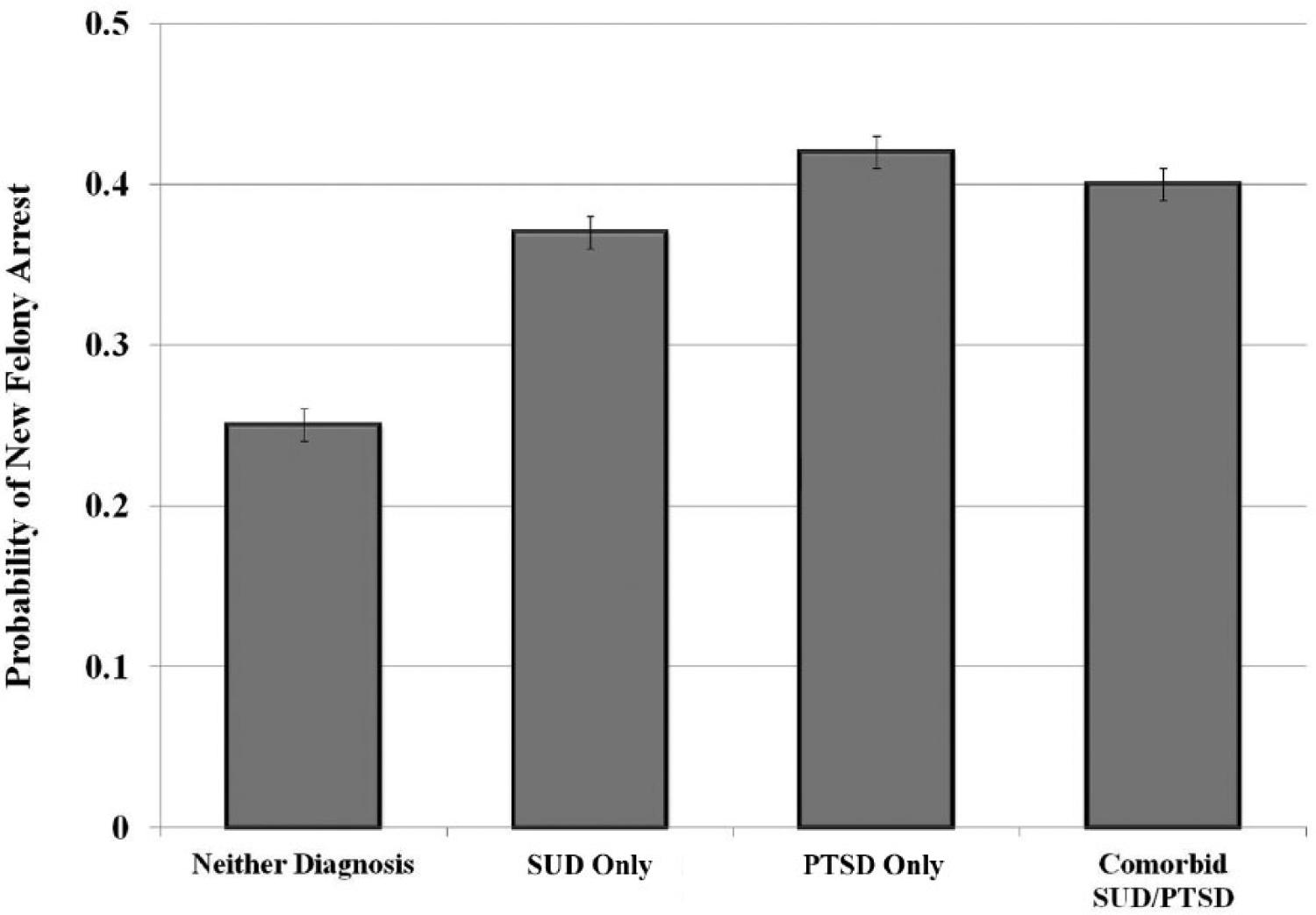
Predicted Probability of a New Felony Charge During the 12 Months After the Index Arrest by PTSD and SUD Diagnostic Status
Results
Our first aim was to assess whether PTSD increased risk of general criminal recidivism. To address this aim, we conducted a logistic regression analysis with PTSD entered as a predictor of any new arrest in the year following the index arrest. As expected, the presence of PTSD increased the likelihood of a new arrest during the year following the index arrest, Wald χ2 = 4.27, p = .039, OR = 1.43, such that the odds of being arrested increased by 1.4 for individuals with PTSD versus those without.
We next performed a hierarchical logistic regression to test the hypothesis that PTSD is associated with an increased likelihood of arrest for any new charge during the 12 months following the index arrest when considered in a model with other risk factors. Results of this analysis are shown separately for each block in Table 2. As would be expected based on previous research, a recent history of arrest significantly predicted rearrest for any new offense, Wald χ2 = 3.93, p = .048, OR = 1.67. When age and gender were entered into the model in Block 2, they were not significant predictors. The addition of other mental health diagnoses in Block 3 revealed that the odds of rearrest increased by about 1.5 times for individuals with a substance use disorder versus those without, Wald χ2 = 6.74, p = .009, OR = 1.48, but the other disorders were not significant predictors. As predicted, a diagnosis of PTSD improved the fit of the model to the data, and the odds of rearrest for a new charge in the 12 months following the index arrest was approximately 1.5 times higher for those with PTSD versus those without, Wald χ2 = 4.77, p = .029, OR = 1.49. With PTSD entered in the model, substance use disorders remained a significant predictor of rearrest, Wald χ2 = 6.64, p = .01, OR = 1.47. The interaction of PTSD and substance use disorders in the final block did not predict general criminal recidivism. The relative probabilities of rearrest by PTSD and substance use disorder are depicted in Figure 1. As illustrated by this figure, the predicted probability of rearrest for participants with PTSD (.55) was similar to that for participants with a substance use disorder (.52) and those with comorbid PTSD and a substance use disorder (.56).
Our second aim was to assess whether the relationship of PTSD with general criminal recidivism generalized to more serious criminal charges, specifically felony charges. We conducted a logistic regression analysis with PTSD entered as the predictor to test this hypothesis. As expected, PTSD was associated with a greater likelihood of a new felony arrest, Wald χ2 = 5.33, p = .021, OR = 1.51. Specifically, the odds of rearrest were 1.5 times higher in participants with PTSD versus those without.
We then conducted a hierarchical logistic regression analysis with the likelihood of arrest for a new felony charge as the outcome variable to measure the predictive power of PTSD in a multivariate model. Findings from this analysis are presented in Table 3. Consistent with the findings for general criminal recidivism, a recent history of a felony arrest increased the risk of rearrest for a new felony charge during the 12 months following the index arrest, Wald χ2 = 29.47, p < .001, OR = 2.48. The addition of demographic characteristics in Block 2 produced a significant negative effect of age, Wald χ2 = 4.06, p = .044, OR = 0.99, but not gender. Paralleling the findings for general recidivism, substance use disorders was the only category of mental disorder to produce a significant effect in Block 3, Wald χ2 = 4.33, p = .037, OR = 1.41, such that the odds of being arrested were 1.4 times higher in those with a substance use disorder versus those without. As hypothesized, PTSD predicted a higher likelihood of arrest for a new felony charge in the year following the index arrest, Wald χ2 = 4.47, p = .035, OR = 1.50 and improved the fit of the multivariate model. The odds of being rearrested were approximately 1.5 times higher for individuals with PTSD versus those without. Examination of the interaction of PTSD and substance use disorders in Block 5 did not emerge as significant. The relative predicted probabilities of rearrest by PTSD and substance use disorder are depicted in Figure 2. As illustrated by this figure, the predicted probability of rearrest for participants with PTSD (.42) was similar to that for participants with a substance use disorder (.37) and those with comorbid PTSD and a substance use disorder (.40).
Taken together, the present results demonstrate that a diagnosis of PTSD was associated with increased risk of recidivism among justice-involved individuals with mental disorders, and the risk of rearrest among individuals with a PTSD diagnosis was comparable with those with a substance use disorder diagnosis.
Discussion
Trauma exposure is increasingly being recognized as an important vulnerability to consider in models of risk of criminal justice system involvement and recidivism. The present study tested the hypothesis that PTSD would be associated with heightened risk of rearrest among justice-involved persons with mental disorders after taking into account other risk factors for recidivism. As hypothesized, hierarchical logistic regression analyses showed that a diagnosis of PTSD at the index arrest was associated with a greater likelihood of arrest for any new criminal charge and a new felony charge over the subsequent 12 months, above the risk conferred by other mental health disorders and common predictors of recidivism. Highlighting the importance of PTSD as a risk factor for recidivism, the probability of rearrest for any new charge and a new felony charge was comparable for individuals with PTSD and those with substance use disorders (Figures 1 and 2). Although preliminary, the study findings provide new evidence that PTSD increases risk of both general and serious forms of criminal recidivism among individuals with mental disorders and that it contributes unique information about recidivism risk that is distinct from other well-established risk factors, including substance use disorders.
Although PTSD has occasionally been used as a basis for criminal defenses (Berger, McNiel, & Binder, 2012), it may be overlooked in service delivery in criminal justice settings, as research suggests it often has been in routine clinical practice (Zimmerman & Mattia, 1999). The potential relevance of PTSD in criminal justice settings is supported by research that consistently shows justice-involved persons experience much higher rates of trauma exposure than the general population, including elevated rates of recent victimization in adulthood (Jennings, Piquero, & Reingle, 2012; Sadeh et al., 2014). Based on these findings, one reason that PTSD may be particularly important for understanding recidivism risk is the high base rate of trauma exposure and related psychological distress in these groups. However, the relatively low base rate of PTSD observed in the present study suggests that it is likely underdiagnosed in jail settings, which typically rely on clinical assessments rather than research-based structured diagnostic assessments.
Previous research also has found that justice-involved adults with mental illness experience high rates of recent victimization (55% in the prior 6 months), and recent victimization relates to increased risk of criminal behavior (Sadeh et al., 2014). Recent trauma exposure among justice-involved persons with mental disorders may create periods of heightened stress and vulnerability that increase recidivism risk by, for instance, triggering the use of maladaptive coping skills to attenuate trauma-related symptoms. Furthermore, evidence is growing that PTSD confers risk of other maladaptive behaviors that increase contact with the justice system, including other-directed violence and illicit substance use (Chilcoat & Breslau, 1998). Overall, the results of the present study, in combination with the research reviewed above, provide compelling evidence that PTSD deserves attention in developing interventions to reduce justice system involvement of persons with mental disorders.
Future research on the mechanisms by which mental disorders are associated with risk of recidivism is important not only for preventing entry to the justice system, but also for reducing the likelihood of reoffending (Dvoskin et al., 2012; Skeem & Monahan, 2011). In particular, identifying causal processes and generating models that examine the interplay of multiple risk factors for criminal offending might help explain inconsistencies in the literature regarding the relative contributions of mental illness versus substance use disorders for recidivism. The finding that PTSD and substance use disorders are frequently comorbid suggests that there are shared etiological and risk mechanisms that cut across both disorders. Potential mechanisms identified in the literature include common genetic risk factors (Sartor et al., 2011); hypersensitivity and chronic exposure to environmental stressors (Sinha, 2008); and high levels of negative affect, impulsivity, and anger (Elbogen et al., 2012; Miller et al., 2006), among others. The present findings provide evidence that substance use disorders cannot fully account for the relationship of PTSD with criminal recidivism, which supports the need for future research to investigate whether certain causal risk factors are specific to PTSD. For instance, the hypervigilance to threat cues and tendency to interpret safe environments as dangerous that are specifically observed in PTSD may increase recidivism risk via an increase in suspiciousness that decreases prosocial attitudes and social affiliation, or increases reactive aggression. Although the interactive effects of PTSD and substance use disorders did not emerge as significant in this study, identifying the etiological mechanisms that contribute to comorbidity among these disorders remains an important area of research. Thus, future research that moves beyond examining the relative importance of a particular diagnosis or behavior (PTSD vs. substance use disorders) to a level of analysis that strives to understand causal mechanisms for criminal recidivism has the potential to provide greater opportunity for clinical intervention and prevention.
From a clinical standpoint, the finding that PTSD predicts reoffending in a multivariate model that included substance use disorders suggests that treating substance use disorders will not be sufficient to eliminate the recidivism risk conferred by PTSD. This finding is consistent with efforts to incorporate more trauma-informed treatment in correctional settings and in interventions aimed at reducing comorbid PTSD and substance use disorders (Wallace, Conner, & Dass-Brailsford, 2011). The call for the development of interventions aimed specifically at addressing trauma history has spurred research on the efficacy of such interventions, and preliminary evidence suggests they are beneficial for reducing symptoms of PTSD, decreasing recidivism, and improving treatment adherence (Messina, Calhoun, & Braithwaite, 2014; Messina, Grella, Cartier, & Torres, 2010). The trauma-informed treatment movement has largely emphasized the need to consider trauma history when treating female offenders, partly due to the higher rates of trauma exposure reported by incarcerated women than men (Messina, Grella, Burdon, & Prendergast, 2007). However, the present study found that PTSD increased risk of recidivism in both men and women, suggesting that attending to trauma exposure and treating PTSD symptoms in men may also be relevant to reducing risk of recidivism. Investigating whether gender differences in responsiveness to trauma-informed treatment affect the risk of criminal recidivism is a promising future direction that remains largely unexplored.
Strengths of the study design include the use of an observational design that took into account temporal relationships between the hypothesized explanatory variable and outcomes of interest, inclusion of a clinically relevant sample of arrestees with mental disorders, and use of objective arrest data to measure recidivism. As with any study, there are also limitations. Diagnoses of PTSD and other disorders were ascertained with the routine evaluation procedures used by clinicians in the jail system; a structured research diagnostic assessment was not used. Consequently, the reliability of prevalence rate estimates of PTSD in the study group is unknown, and those diagnosed with PTSD in this sample may have had particularly severe or acute symptom presentations. Given that the rates of PTSD that are ascertained in adult jail detainees during routine evaluation procedures at intake are largely unknown, we cannot determine whether the rates reported in the present study are comparable with other observational designs. Examining whether the present findings replicate with more systematic assessment of mental health diagnoses is an important next step in this area of research. Also, we did not have information on the recency of the traumatic event or the type of trauma experienced, and potential heterogeneity in these factors may moderate relationships of PTSD with recidivism risk. Examining these relationships would be an interesting avenue for future research. Although number of days in jail did not reduce recidivism risk in this study, time in the community may affect risk of rearrest. As such, assessing the reliability of the current findings using a study design that equates participants on the number of days spent in jail during the follow-up period is a topic for future research. Finally, the number of covariates included in the analyses was limited by the observational design, and future research on this topic would benefit from including a broader range of sociodemographic control variables.
Even in the context of these limitations, the present study advances understanding of risk of criminal recidivism in justice-involved persons with mental disorders by examining an understudied, yet seemingly relevant, mental health diagnosis. It is one of the first studies to examine whether PTSD confers unique risk of reoffending that is not captured by other risk factors and provides promising data that can serve as a foundation for future research.
Footnotes
Acknowledgements
The authors thank Renée L. Binder, MD, and Jennifer Johnson, JD, for their assistance. Views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of Veterans Affairs.
Authors’ Note:
Naomi Sadeh is now at the National Center for Posttraumatic Stress Disorder (PTSD), Veterans Affairs (VA) Boston Healthcare System, Department of Psychiatry, Boston University School of Medicine.
This research was sponsored in part by grants from the University of California, San Francisco Academic Senate Committee on Research, the San Francisco Mayor’s Office on Disability, and the Cathleen Baker Living Trust.