
Abstract
Researchers have linked parental incarceration to a host of short-term, negative consequences for children and adolescents. However, it is unclear whether offspring experience some of these consequences, particularly depressive symptoms, as adults, especially racial/ethnic minorities who disproportionately experience parental incarceration. The present study uses data from Add Health to investigate whether parental incarceration during childhood or adolescence predicts depressive symptoms between ages 24 and 34 and whether race/ethnicity moderates this relationship. Results indicate that parental incarceration is associated with long-term consequences for some offspring, but not others. Specifically, respondents whose parent was first incarcerated before birth or age 1 appear to be at risk for adult depressive symptoms. Furthermore, the moderation analysis reveals similarities in the effects of parental incarceration across racial/ethnic groups. Findings from this study suggest that parental incarceration might be associated with long-term mental health consequences only for certain subgroups.
Keywords
Mass incarceration in the United States has produced a host of negative direct and indirect consequences for offenders while concurrently creating another problematic phenomenon: mass parental incarceration. Between years 1991 and 2007, the number of children with an incarcerated parent nearly doubled (Glaze & Maruschak, 2010). An estimated 1.7 million minor children currently have at least one parent in prison, translating to 2.3% of the minor U.S. resident population (Glaze & Maruschak, 2010). It is important to highlight that this estimate of 2.3% does not include the proportion of minors or adults who have ever experienced parental incarceration. Such estimates are hard to come by due to data limitations. Two decades ago, scholars estimated that 10 million minor children had experienced parental incarceration at some point in their lives (Reed & Reed, 1997). This estimate has likely swelled since then, especially if researchers consider the number of minor and adult offspring with histories of parental incarceration.
Although 2.3% of U.S. children currently have an incarcerated parent, this estimate masks the uneven prevalence of parental incarceration across racial/ethnic groups. Just as Blacks and Hispanics are overrepresented in jails and prisons, their offspring disproportionately experience parental incarceration. Youth of color constitute 66% of children with incarcerated parents (Black children: 45%, Hispanic children: 21%, White children: 28%; Glaze & Maruschak, 2010). This is particularly disconcerting for Black youth who make up only 14% of the U.S. minor population (U.S. Census Bureau, 2013). Moreover, Black children are 7.5 times more likely than White children to have a parent in prison (6.7% of Black youth vs. 0.9% of White youth), and Hispanic children are more than 2.5 times more likely than White children to have a parent in prison (2.4% of Hispanic youth vs. 0.9% of White youth; Glaze & Maruschak, 2010). Because youth of color, particularly Black children, have a higher cumulative risk of parental incarceration than White children, parental incarceration contributes to racial inequality among Americans (Wakefield & Wildeman, 2013).
Given the ubiquity and growth of parental incarceration, researchers have devoted much scholarly attention to the effects of this phenomenon on children. In some instances, losing a criminally involved parent—especially an abusive parent—may support the well-being of children (Wakefield & Wildeman, 2011). Nevertheless, evidence from qualitative and quantitative studies overwhelmingly links parental incarceration to a host of negative consequences such as poor school performance, adjustment difficulties, substance use, delinquency, truancy, home instability, and externalizing and internalizing problems (Arditti, 2012; Arditti, Lambert-Shute, & Joest, 2003; Cho, 2009; Foster, 2012; Foster & Hagan, 2013; Hagan & Foster, 2012a, 2012b; Morris, 1965; Murray & Farrington, 2005, 2008a, 2008b; Murray, Farrington, & Sekol, 2012; Phillips, Erkanli, Keeler, Costello, & Angold, 2006; Roettger & Swisher, 2011; Swan, 1981; Swisher & Roettger, 2012). Researchers have examined most of these adverse outcomes as short-term consequences among children and adolescents, leaving more to be learned about the long-term consequences of parental incarceration when offspring become adults. Studies that focus on long-term consequences tend to examine criminal justice-related outcomes, often documenting that adult offspring with histories of parental incarceration are at greater risk of criminal justice contact than adults without such history (see Huebner & Gustafson, 2007). Even fewer studies examine the long-term effects of parental incarceration on the mental health of offspring. Mental health problems are associated with a broad range of social and economic problems for individuals, their families, and society (Kessler et al., 1997). Investigating whether parental imprisonment might compromise the psychological well-being of offspring and confer long-term harm to millions of Americans is a necessary endeavor.
The aim of the current study is to fill this research gap by investigating whether experiencing parental incarceration in childhood or adolescence is associated with depressive symptoms during adulthood and whether this relationship varies by offspring’s race/ethnicity. Compared with Whites, people of color, especially Blacks, have greater exposure to parental incarceration and its potential consequences, are more likely to have multiple incarcerated relatives, and face a greater risk of mental health and behavioral problems after parental incarceration when accounting for preexisting disadvantage (Wakefield & Wildeman, 2011). Therefore, the effects of parental incarceration might be worse for Blacks and Hispanics. The current study uses data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) to answer two research questions:
Given the scope of incarcerating large numbers of parents, especially parents of color, these research inquiries have important criminal justice policy implications as they address whether the collateral damage of incarceration extends beyond offenders by harming the mental health of their offspring in the long term, especially in a way that produces racial/ethnic disparities in mental well-being.
Theoretical Framework
Consistent with previous studies of parental incarceration (Murray & Farrington, 2008b; Wildeman, 2010), the current study uses general strain theory (Agnew, 1992) to guide this research and to understand the relationship between parental incarceration and depressive symptoms. Although it is commonly applied to studies of offending (e.g., violence, drug use, delinquency), strain theory can be used to understand how a stressful event, such as parental incarceration, can directly lead to depressive symptoms or produce hardships that lead to depressive symptoms among offspring. Three forms of strain can result from parental incarceration: psychological (e.g., depression), structural, and social strains (Arditti, 2012; Bowlby, 1969; Bretherton, 1992; Murray & Farrington, 2005, 2008b; Poehlmann, 2003).
Strain theory links parental incarceration with psychological problems, such as depressive symptoms, because parental incarceration is often conceptualized as a form of parental loss for children (Murray & Farrington, 2008b; Wildeman, 2010). Some children experience emotions such as guilt, shame, denial, anger, or sadness when losing a parent to incarceration (Braman, 2004; Carlson & Cervera, 1992; Condry, 2007; Swan, 1981). Murray et al. (2012) compare parental incarceration with parental divorce, in that it can happen suddenly and unexpectedly, involve loss of contact with a parent, and result in reductions in family income. In some cases, the arrest of a parent can happen in the child’s presence. Kampfner (1995) found that witnessing the arrest of a household member predicted post-traumatic stress among maltreated children. Qualitative research by Braman (2004) and Comfort (2009) also showed that exposing children to their parent’s arrest and correctional facilities can be emotionally troubling. Moreover, when a parent is incarcerated, caretakers sometimes shield children from the truth about their incarcerated parent’s absence by fabricating stories or avoiding the discussion altogether (Condry, 2007; Morris, 1965; Swan, 1981). This contributes to the confusion and worry children experience (Carlson & Cervera, 1992), and some eventually discover the truth through stigmatizing means (Braman, 2004; Condry, 2007; Morris, 1965; Swan, 1981).
In addition to psychological distress from losing a parent to incarceration, children may experience changes in their structural conditions. Living arrangements and family structure may shift, especially if the child lived in the same household as the incarcerated parent. This disruption might be more problematic for those with histories of maternal incarceration. Imprisoned mothers (77%) are 3 times more likely than imprisoned fathers (26%) to be primary caregivers of their minor children and are more likely to have lived with their children before incarceration (Glaze & Maruschak, 2010). When fathers are imprisoned, children are more likely to live with their other parent (88%). But when mothers are imprisoned, children have a greater chance of living in someone else’s household, such as with grandparents (45%) or other relatives (23%; Glaze & Maruschak, 2010). In either case, parental incarceration may expose children to the risk of living in single-parent households. In addition, caretakers of offspring can be stressed, depressed, economically strained, and even resentful, making it difficult for them to give children the supervision, emotional attention, and care they need (Morris, 1965). Such impaired parenting can create additional emotional or economic problems for children. In some cases, children are removed from their families altogether and placed in foster care. Children of imprisoned mothers (11%) are 5.5 times more likely to live in foster care than children of imprisoned fathers (2%; Glaze & Maruschak, 2010). In fact, increases in female incarceration rates appear to account for 30% of the increase in foster care caseloads between 1985 and 2000 (Sylvester & Swann, 2006).
Changes in family structure and living arrangements can also result in children having to change schools and neighborhoods, being subject to different disciplinary practices, and living on diminished economic resources. Sometimes, the family must assume additional financial responsibilities in the incarcerated parent’s absence because of debts that he or she left behind or from assuming a new role as the primary bread winner (Morris, 1965). Furthermore, children and families can experience financial strain while attempting to maintain a relationship with the incarcerated parent. Phone calls, traveling to and from the institution for visits, and providing financial support to the incarcerated parent can be expensive and taxing on the families’ income (Arditti et al., 2003; Comfort, 2009). These structural conditions can affect the psychological well-being of children.
Children who experience parental incarceration sometimes have to navigate social stigma. Children and families of the incarcerated are at risk of feeling shamed and experiencing isolation, hostility, and rejection by neighbors, teachers, peers, employers, and other family members (Braman, 2004; Condry, 2007). This stigma might explain why some families keep the incarceration a secret, thus pushing children into silence and withdrawal. Another consequence of social stigma is severing ties with support networks and diminishing the social capital needed for children and families to thrive. These social strains can alter children’s mental well-being.
Together, these psychological, structural, and social strains are related to depressive symptoms for offspring. However, parental incarceration might not affect everyone the same. The effects of parental incarceration can vary by important factors, such as which parent is incarcerated, child’s gender, and child’s age (Besemer, van der Geest, Murray, Bijleveld, & Farrington, 2011; Murray, Janson, & Farrington, 2007). There is also reason to believe that the effects of parental incarceration might be worse for children of color than White children. As strain theory acknowledges, people of color disproportionately experience strains unrelated to parental incarceration (Agnew, 1992, 2006), such as structural disadvantage (Krivo, Peterson, Rizzo, & Reynolds, 1998; Sampson & Wilson, 1995; Wilson, 1987), family disruption (Blackman, Clayton, Glenn, Malone-Colon, & Roberts, 2005; Broman, 1993; Sampson, 1987), and racial discrimination (Fischer & Shaw, 1999; Keith, Lincoln, Taylor, & Jackson, 2009; R. M. Sellers, Caldwell, Schmeelk-Cone, & Zimmerman, 2003; S. L. Sellers, Bonham, Neighbors, & Amell, 2009; Williams, Neighbors, & Jackson, 2008). These strains place people of color at greater risk of mental health problems, and experiencing parental incarceration can exacerbate the effects of these preexisting strains as previous studies have highlighted (Murray & Farrington, 2008a; Wakefield & Wildeman, 2011). Furthermore, Black and Hispanic children face a substantially greater cumulative risk of having an incarcerated parent and other incarcerated relatives than White children (Glaze & Maruschak, 2010; Wakefield & Wildeman, 2011, 2013). This greater cumulative exposure to parental and family incarceration places Blacks and Hispanics at higher risk of experiencing the aforementioned psychological, structural, and social strains of parental incarceration. Thus, it is plausible for parental incarceration to be more consequential on the mental well-being of offspring of color by exacerbating preexisting strains they disproportionately experience and by increasing their exposure to the strains of parental incarceration. The current analysis considers this possibility by testing whether race/ethnicity moderates the relationship between parental incarceration and depressive symptoms.
Prior Research
Findings from extant qualitative and quantitative research show that parental incarceration is associated with long-term deleterious consequences for children. This body of research is dominated by studies that examine the effects of parental incarceration on offspring’s antisocial behavior (Giordano, 2010; Murray & Farrington, 2005), criminal offending (Besemer et al., 2011; Roettger & Swisher, 2011), and criminal justice contact (Bijleveld & Wijkman, 2009; Huebner & Gustafson, 2007; van de Rakt, Murray, & Nieuwbeerta, 2012). Because only a minority of children of incarcerated parents becomes involved in the criminal justice system, and so few female offspring will engage in offending (Wakefield & Wildeman, 2013), criminologists must expand their research agendas by exploring a broader range of consequences of parental incarceration. As such, scholars have recently devoted more attention to the effects of parental incarceration on the psychological well-being of children, as documented in qualitative research by Braman (2004) and Comfort (2009). In quantitative research, scholars examined mental health problems—or internalizing problems—that include concepts such as anxiety, depression, neuroticism, and poor self-concept or self-esteem (Murray et al., 2012), many finding a significant, positive association between parental incarceration and mental health problems/internalizing problems. Most of these studies assess the short-term consequences of parental incarceration on the mental health of children and adolescents.
One example is a study by Wakefield and Wildeman (2011) that uses data from the Project on Human Development in Chicago Neighborhoods (PHDCN) and Fragile Families and Child Wellbeing (FFCW) Study. This study found that children of incarcerated parents experienced heightened internalizing problems such as depression, anxiety, and somatic disorders, and 50% of the children in the PHDCN sample who experienced paternal incarceration had internalizing problem scores high enough to need professional intervention. Considering racial disparities, these researchers estimated Black–White differences in internalizing problems when taking levels of incarceration during 1978 and 1990 into account. They found that Black–White differences in internalizing problems would have been 25% to 45% less without parental incarceration (Wakefield & Wildeman, 2011). Even more, they found that Black children are not only more likely than their White counterparts to have one incarcerated relative, but they are also more likely to have multiple incarcerated relatives (Wakefield & Wildeman, 2011). Wakefield and Wildeman (2011) underscore that children of incarcerated fathers were more disadvantaged than their similarly situated peers without an incarcerated father, even before their father’s confinement; however, they are able to show that parental incarceration has effects over and above childhood disadvantage. Thus, parental incarceration appears to compound disadvantage for already disadvantaged children (Murray & Farrington, 2008a; Wakefield & Wildeman, 2011).
Wilbur et al. (2007) assessed whether disadvantaged children of incarcerated fathers were more likely to exhibit depressive symptoms than similarly situated disadvantaged children without incarcerated fathers. The researchers found a significant positive relationship between paternal incarceration and depressive symptoms among children aged 6 to 11 years (Wilbur et al., 2007). Swisher and Roettger (2012) examined the association between a father’s incarceration and depressive symptoms among Black, White, and Hispanic adolescents in the Add Health data at Waves 1, 2, and 3. They found that having a father incarcerated at Wave 1 (during childhood) was significantly associated with higher depressive symptoms scores at that time, but experiencing paternal incarceration at Waves 2 and 3 was not significantly associated with depressive symptoms at those times (Swisher & Roettger, 2012). With depressive symptoms still as the outcome, Swisher and Roettger also examined interactions between father’s incarceration at various time points and race and ethnicity. None of the interactions was statistically significant, indicating that the relationship between paternal incarceration and depressive symptoms during childhood was similar across racial and ethnic groups.
Geller, Cooper, Garfinkel, Schwartz-Soicher, and Mincy (2012) assessed whether children of incarcerated fathers in the Fragile Families Study exhibited significantly more internalizing problems (Anxious/Depressive and Withdrawn subscales) at age 5 than children whose fathers were never incarcerated. Although their findings suggested a robust effect of paternal incarceration on childhood aggression, a series of cross-sectional, longitudinal, and fixed-effects regression models found no significant relationship between paternal incarceration and internalizing problems at age 5 (Geller et al., 2012). This finding contradicts other studies that find a positive, significant association between paternal incarceration and mental health/internalizing problems. Perhaps the age of the sample is the culprit; Geller and colleagues used a sample of 5-year-old children, whereas previous studies analyzed child and adolescent samples that ranged in age. Similarly, Kinner, Alati, Najman, and Williams (2007) found a non-significant relationship between paternal incarceration and internalizing problems among 14-year-old youth in an Australian birth cohort when controlling for socioeconomic status, mother’s mental health and substance use, parenting style, and family adjustment (Kinner et al., 2007).
The aforementioned studies examined the effects of parental incarceration on mental health outcomes among minor children or adolescents below age 18 years. Very few studies have examined the long-term consequences of parental incarceration when children become adults. Two exceptions are Murray and Farrington (2008b) and Lee, Fang, and Luo (2013) who examined mental health outcomes during adulthood. In their study, Murray and Farrington (2008b) used prospective longitudinal data from the Cambridge Study on Delinquent Development to assess whether parental imprisonment between birth and age 10 predicted internalizing problems for males from age 14 to 48. Compared with boys who did not experience parental separation or who experienced separation from a parent for reasons other than incarceration (e.g., death, hospitalization, parent divorce), boys who experienced parental incarceration had increased internalizing problems during adulthood, controlling for childhood risk factors and parental criminality (Murray & Farrington, 2008b). Their findings attest to the potential long-term consequences of parental incarceration. However, like many studies, this work only examines boys’ outcomes and excludes females. Furthermore, the male sample is all White, respondents were born prior to the prison boom—between the 1950s and 1960s—in the United Kingdom, and the subsample size for boys of incarcerated parents was small: n = 40. The characteristics of their sample might yield results that are not generalizable to offspring in the United States, making a reanalysis of the relationship worthwhile with use of a contemporary dataset that represents the U.S. population.
Lee et al. (2013) examined the relationship between maternal and paternal incarceration and various health outcomes, including being diagnosed with depression, anxiety, post-traumatic stress disorder (PTSD), and attention deficit hyperactivity disorder (ADHD), among young adults aged between 24 and 34 years in the Add Health data. Paternal incarceration was significantly associated with depression, anxiety, and PTSD, and maternal incarceration was significantly associated with depression, both models controlling for potential confounders (Lee et al., 2013). The authors measured mental health problems by using items that asked whether respondents were diagnosed by professionals rather than relying on the self-reported measures of mental health in Add Health. However, not all depressed persons seek or receive professional treatment. Relying on official diagnoses may underrepresent the extent of mental health problems, especially among disadvantaged populations and racial/ethnic groups of color who might be the least likely to seek psychological treatment. In addition, the parental incarceration sample in Lee et al.’s study includes respondents who first experienced parental incarceration before and during the measurement of the outcomes. Without the establishment of proper temporal ordering, it is difficult to decipher the actual effects of parental incarceration in their study. Thus, in light of the limitations of these two studies, the current study examines the relationship between parental incarceration and adult depressive symptoms and extends these works by considering the possible moderating role of race/ethnicity.
Method
Data
Data come from the in-home portion of the National Longitudinal Study of Adolescent to Adult Health (Add Health), a longitudinal study of a nationally representative sample of adolescents in the United States who were in grades 7 to 12 and were age 11 to 21 years when the study began during the 1994-1995 school year (Harris et al., 2009). The study design included a sample of 80 high schools and 52 middle schools with an unequal probability of selection, ensuring representativeness with regard to region of country, urbanicity, school size, school type, and ethnicity. The sample has been followed through adolescence and early adulthood (with ongoing data collection). More than 20,000 students participated in the first wave of data between Years 1994 and 1995. 1 Approximately 15,700 (76%) of these students also completed the Wave 4 survey between Years 2007 and 2008 when they were 24 to 34 years old. The current study uses data from Wave 1, which includes background characteristics, and Wave 4, which contains items needed to measure adult depressive symptoms and retrospective reports of parental incarceration.
Sample
Of the 15,701 respondents who participated in Waves 1 and 4, some have missing data on the variables of interest, and some do not have the survey weights needed to adjust for sample selection and participation. 2 Furthermore, respondents were removed from the analysis if they first experienced parental incarceration after age 17, a period after adolescence that also overlaps with the timing of the adult depressive symptoms outcome. This is done to establish temporal ordering and avoid confounding the analysis. Together, these restrictions result in a final sample size of n = 10,858.
Table 1 shows the demographic characteristics of the sample. The average respondent was 16 years old at Wave 1 and 28 years old at Wave 4. With regard to gender, 53% of the respondents were female, and 47% were male. In addition, respondents self-identified as one of four mutually exclusive racial/ethnic groups: non-Hispanic White (57%), non-Hispanic Black (20%), Hispanic (16%), and non-Hispanic Other (8%). 3 Non-Hispanic Whites were the reference group in this study.
Descriptive Statistics for Variables for Total Sample and by No PI History Versus PI History
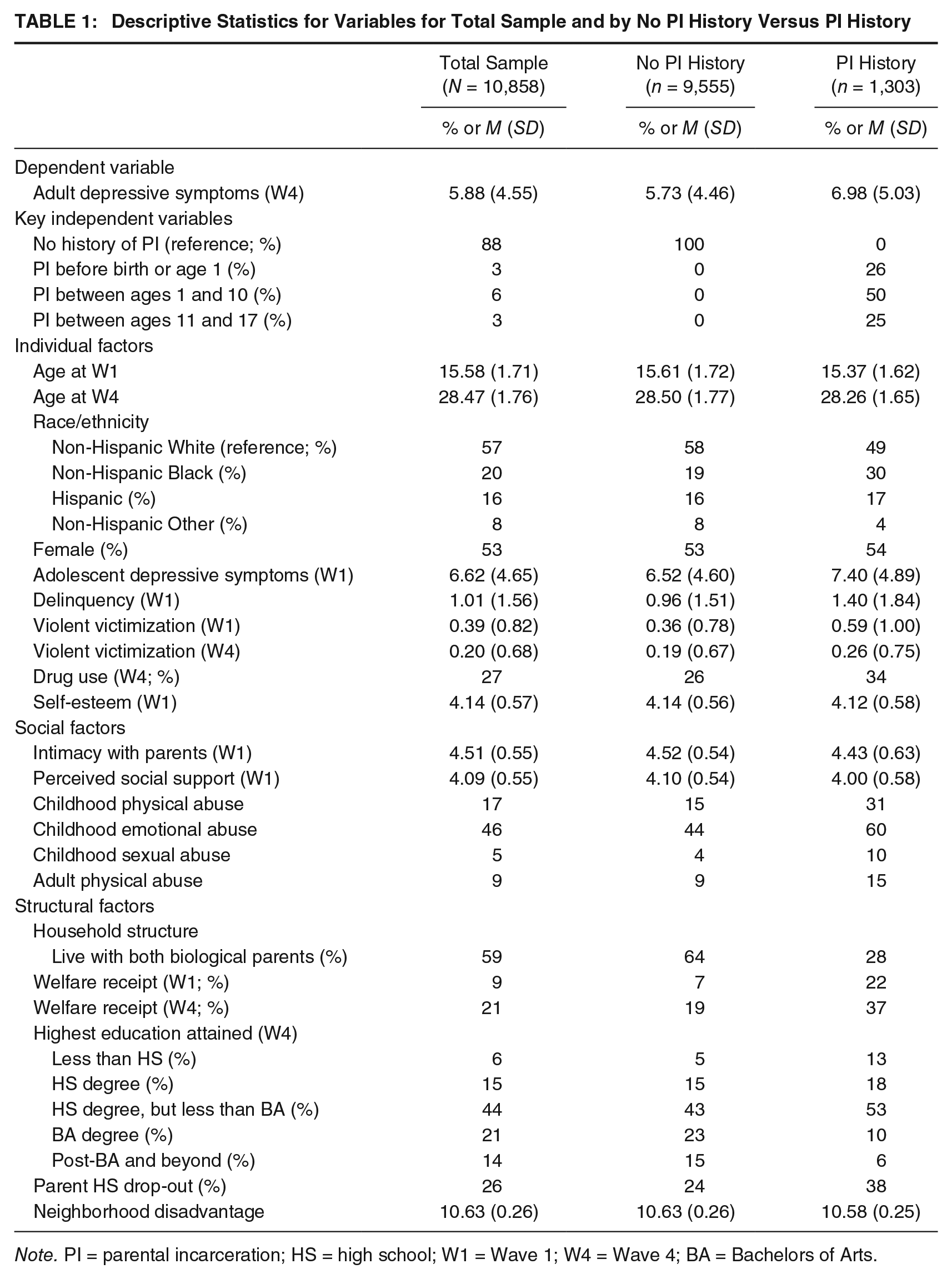
Note. PI = parental incarceration; HS = high school; W1 = Wave 1; W4 = Wave 4; BA = Bachelors of Arts.
Measures
Dependent Variable
Adult depressive symptoms, measured at Wave 4, serve as the dependent variable and gauge the psychological well-being of respondents when they are young adults between ages 24 and 34 years. The depressive symptoms measure comprises items from the Center for Epidemiologic Studies Depression (CES-D) scale that is embedded in Add Health, which is found to be internally consistent and valid (Radloff, 1977). This measure includes 10 items that assessed how often respondents felt particular emotions during the past week, including the following: (1) bothered by things, (2) had the blues, (3) felt as good as others (reverse coded), (4) had trouble concentrating, (5) felt depressed, (6) felt too tired to do things, (7) felt happy (reverse coded), (8) enjoyed life (reverse coded), (9) felt sad, and (10) felt disliked by others. Response choices for each item ranged from never or rarely (coded 0) to most of the time or all of the time (coded 3). The 10 items were summed to compute a continuous measure of depressive symptoms, which produced scores ranging from 0 to 29 and an average score of 5.88 (SD = 4.55). The distribution of scores was slightly positively skewed and kurtotic. Therefore, the original metric of depressive symptoms was log-transformed before including it in the multivariate models. Cronbach’s alpha for the Depressive Symptoms scale was .84.
Independent Variables
Parental Incarceration Measures
Parental incarceration is the key independent variable. Items used to compute the parental incarceration measure come from the Wave 4 questionnaire where respondents retrospectively report histories of parental incarceration. For each parent, the questionnaire first asks, “Has your biological mother/father ever spent time in jail or prison?” Respondents either answered yes (1) or no (0). These two items were used to construct a parental incarceration measure in which “1” is recorded for respondents who reported that their mother, father, or both parents have ever been incarcerated. A “0” is recorded for respondents who reported no parental incarceration. There is 7% of missing data on the parental incarceration measure stemming from refusals and don’t know responses. 4 The prevalence of parental incarceration in the final sample is 12%, with 88% having no history of parental incarceration. 5
If respondents answered yes to the initial maternal/paternal incarceration questions, they were then asked, “How old were you when your biological mother/father went to jail or prison (the first time)?” Respondents answered this item by reporting a discrete age between 0 and 34 years or stating not yet born if their parent was incarcerated before their birth. To address issues of temporal ordering and to consider the timing of parental incarceration, this item was used to create four mutually exclusive comparison groups: (a) parental incarceration first occurred before the respondent’s birth or below age 1 (3%), (b) parental incarceration first occurred between ages 1 and 10 (6%), (c) parental incarceration first occurred between ages 11 and 17 (3%), and (d) a reference category of respondents whose parents were never incarcerated (88%). For respondents whose mother and father were incarcerated (1% of sample), the earliest age of the two was used to assign them to a group. For example, if a respondent was 6 years old when their mother was first incarcerated and 15 years old when their father was first incarcerated, 6 was used as the age of their first parental incarceration experience. Moreover, respondents who first experienced parental incarceration after age 17 were excluded (298 cases); this was done to maintain the proper ordering of events and to focus on parental incarceration during childhood and adolescence only. Roettger and Swisher (2011) used a similar comparison group strategy in their Add Health study of paternal incarceration and delinquency to help establish temporal ordering.
Individual, Social, and Structural Measures
The current study incorporates a host of individual, social, and structural measures at Waves 1 and 4 that the literature and strain theory link to the relationship between parental incarceration and depressive symptoms. Individual variables include age, race and ethnicity, gender, adolescent depressive symptoms, delinquency, violent victimization, drug use, and self-esteem. A measure of depressive symptoms in adolescence is included to control for the propensity for adult depressive symptoms. Adolescent depressive symptoms are measured at Wave 1 and coded identically to the adult depressive symptoms outcome. The mean score is 6.62 (SD = 4.65) on a scale ranging from 0 to 30. Delinquency is measured at Wave 1, and the mean score is 1.01 (SD = 1.56) on a scale ranging from 0 to 10. The mean adolescent violent victimization score at Wave 1 is 0.39 (SD = 0.82), and the mean adult violent victimization score at Wave 4 is 0.20 (SD = 0.68), both on a scale ranging from 0 to 4. Research often reports illicit drug use and mental health problems as co-occurring disorders (Grant et al., 2004), so the current study considers history of drug use. At Wave 4, respondents report whether they have ever used cocaine, crystal meth, or other illicit drugs excluding marijuana 6 (yes = 1, no = 0). These three items are used to compute a binary drug use measure where “1” denotes history of using any of these drugs and “0” denotes never using any of these drugs. Twenty-seven percent of the sample reports a history of drug use. Self-esteem at Wave 1 7 is included as a control measure because of its association with depressive symptoms (McPhie & Rawana, 2012). On a scale ranging from 1 (low self-esteem) to 5 (high self-esteem), the mean self-esteem score for the sample is 4.14 (SD = 0.57).
Strain theory suggests that having a parent incarcerated can elicit social strains and sever relationships with important figures. As such, this study considers the following social variables to gauge how connected offspring feel to important figures and to control for factors related to depressive symptoms: parental intimacy, perceived social support, history of childhood abuse, and adult physical abuse. The mean parental intimacy score for the sample is 4.51 (SD = 0.55) on a scale ranging from 1 (low parental intimacy) to 5 (high parental intimacy), 8 and the mean perceived social support score is 4.09 (SD = 0.55) on a scale ranging from 1 (low perceived social support) to 5 (high perceived social support). Three measures of childhood abuse by a parent or caregiver are included because of their association with mental health problems and as a partial proxy for parent’s antisocial behavior and child’s living environment. At Wave 4, respondents retrospectively report whether a parent or adult caregiver did the following to them when they were below age 18: (a) hit them with a fist, kicked them, or threw them down on the floor, into a wall, or down stairs (childhood physical abuse); (b) said things that really hurt their feelings or made them feel unwanted or unloved (childhood emotional abuse); and (c) touched them in a sexual way, forced them to touch him or her in a sexual way, or forced them to have sexual relations (childhood sexual abuse). Seventeen percent of the sample reported a history of childhood physical abuse, 46% reported a history of childhood emotional abuse, and 5% reported a history of childhood sexual abuse. A measure of adult physical abuse is also included. The Wave 4 questionnaire asked whether respondents had been slapped, hit, choked, or kicked within the past 12 months (yes = 1, no = 0). 9 Nine percent of the sample reported physical abuse as an adult.
According to strain theory, parental incarceration can shift children’s structural conditions and create hardships that increase their likelihood of depressive symptoms. The current study controls for many structural measures related to parental incarceration or depressive symptoms, including household structure, welfare receipt, educational attainment, parents’ education, and neighborhood-concentrated disadvantage. Household structure is a binary measure of whether respondents lived with both biological parents (coded 1) or not (coded 0). Fifty-nine percent of the sample reported living with both biological parents during Wave 1. Binary measures of welfare receipt at both waves are included. At Wave 1, 9% of the sample received welfare sometime during adolescence, and at Wave 4, 21% received welfare sometime during adulthood. Respondents’ educational attainment is an ordinal measure, where 1 = less than high school (6%), 2 = high school degree (15%), 3 = high school degree but less than bachelor’s degree (44%), 4 = bachelor’s degree (21%), and 5 = post-baccalaureate and beyond (14%). Parents’ education is a binary measure that indicates whether either or both of the respondents’ parents dropped out of high school (yes = 1, no = 0). Nearly 26% of the sample had one or both parents drop out of high school. Neighborhood concentrated disadvantage is an index measure at Wave 1 stemming from the 1990 census data at the tract level. It is a scale combining the proportion of welfare receipt, poverty levels, female-headed households, and unemployment in a respondent’s census tract. Higher scores represent higher neighborhood disadvantage. Scores range from 9.70 to 11.80 in the sample with a mean of 10.63 (SD = 0.26).
Analytic Strategy
Ordinary-least-squares (OLS) regression models 10 are used to examine the relationship between parental incarceration and adult depressive symptoms. Diagnostic tests were first performed to analyze outliers, influential data points, collinearity, linearity, homoskedasticity, and model specification. The data meet the assumptions of normality, linearity, and homoskedasticity; collinearity is not a concern in these data, and the models are properly specified. 11 Table 2 presents findings from the multivariate analyses, which occurred in steps. First, to demonstrate a relationship between parental incarceration and adult depressive symptoms, Model 1 regresses adult depressive symptoms on the parental incarceration subgroups, without controls. Then, Model 2 reexamines this relationship while controlling for the before-mentioned individual, social, and structural control measures. Finally, Model 3 assesses whether race/ethnicity moderates the parental incarceration–adult depressive symptoms relationship by introducing a series of interaction terms. Because the study hypothesizes that parental incarceration increases the likelihood of adult depressive symptoms, this unidirectional hypothesis warrants one-tailed tests of significance, which are presented. Regression coefficients, standard errors, and significance levels are presented in Table 2.
Survey-Adjusted OLS Regression Models for Predictors of Adult Depressive Symptoms (N = 10,858)
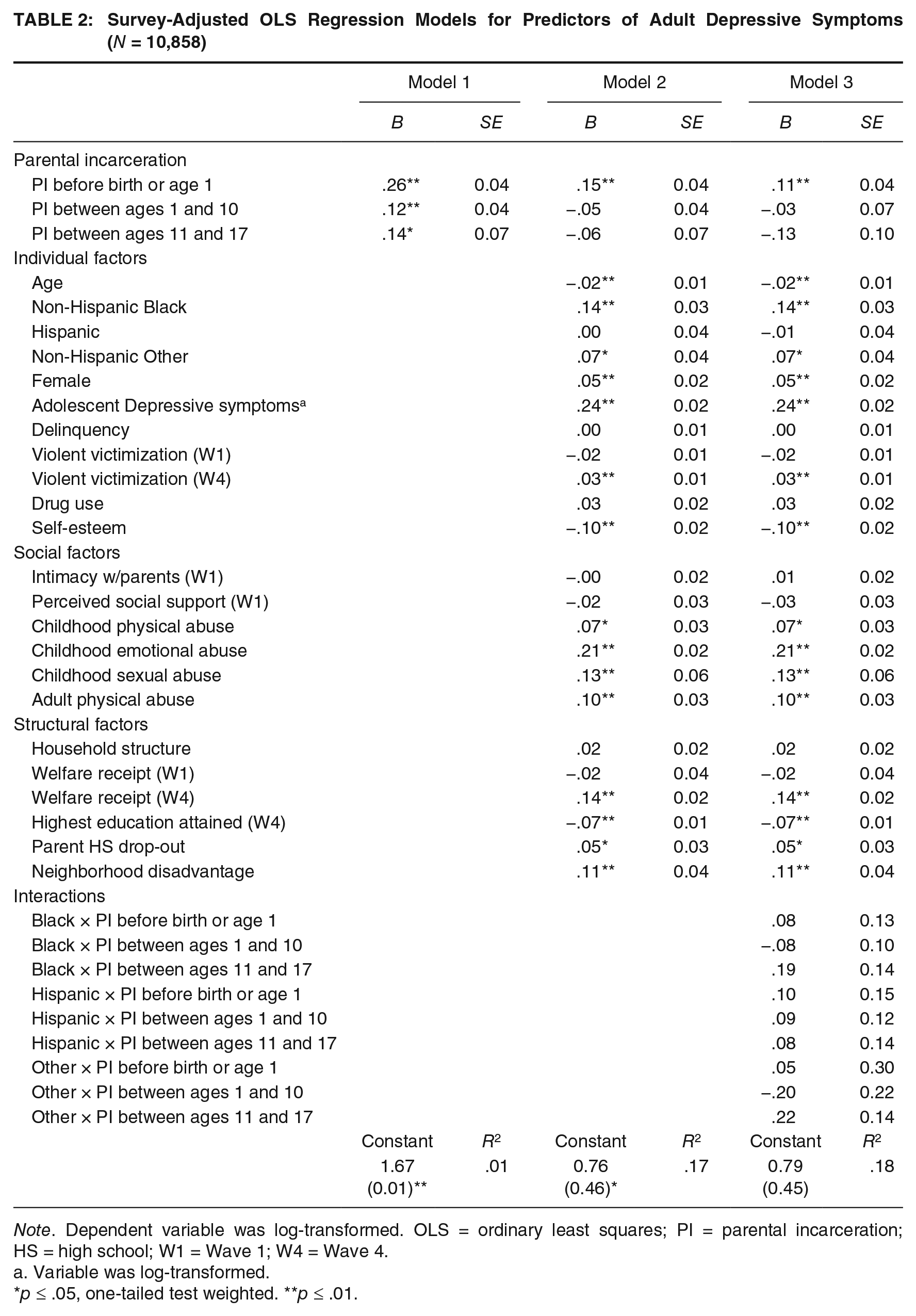
Note. Dependent variable was log-transformed. OLS = ordinary least squares; PI = parental incarceration; HS = high school; W1 = Wave 1; W4 = Wave 4.
Variable was log-transformed.
p ≤ .05, one-tailed test weighted. **p ≤ .01.
Results
Models 1 and 2 assess the first research question of whether parental incarceration during childhood or adolescence predicts depressive symptoms in adulthood. The baseline association presented in Model 1 indicates that parental incarceration is significantly associated with later depressive symptoms. Respondents who first experienced parental incarceration before birth or age 1 scored 26% higher on the depressive symptoms scale (b = .26, p < .001) than respondents who never experienced parental incarceration. Similarly, compared with respondents without parental incarceration histories, experiencing parental incarceration for the first time between ages 1 and 10 is associated with a 12% increase in adult depressive symptoms scores (b = .12, p < .001) while experiencing parental incarceration for the first time between ages 11 and 17 is associated with a 14% increase in adult depressive symptoms scores (b = .14, p = .02). 12 Controlling for the individual, social, and structural confounders in Model 2 reduces the magnitude of these relationships. Nevertheless, the coefficient for respondents in the before birth or age 1 subgroup remains significant, showing that they reported 15% higher depressive symptoms scores (b = .15, p < .001) than respondents with no parental incarceration histories. These findings are consistent with the hypothesis that predicts an association between parental incarceration and mental health problems in adulthood.
Model 3 introduces interaction terms between race/ethnicity and parental incarceration to test whether race/ethnicity moderates the relationship between parental incarceration and adult depressive symptoms. None of the interaction terms is significant, indicating that the effect of parental incarceration on the risk for adult depressive symptoms is similar across racial/ethnic groups. These results refute the hypothesis that the effect of parental incarceration might be more consequential for groups of color.
The magnitude, direction, and significance levels of the control measures were identical across Models 2 and 3. First turning to the individual factors, age is negatively associated with the outcome, showing that a 1-year increase in age lowers the depressive symptoms scores by 2% (b = −.02, p = .01). Black respondents (b = .14, p < .001) and other race respondents (b = .07, p = .02) report depressive symptoms scores 14% and 7% higher, respectively, than Whites. Females report depressive symptoms scores 5% higher (b = .05, p = .01) than their counterparts. The strongest predictor of adult depressive symptoms is adolescent depressive symptoms. For a 1% increase in adolescent depressive symptoms scores, the score for adult depressive symptoms increases by 24% (b = .24, p < .001). Moreover, a 1-unit increase in violent victimization at Wave 4 corresponds to a 3% increase in adult depressive symptoms (b = .03, p = .01). A 1-unit increase in self-esteem corresponds to a 10% decrease in adult depressive symptoms (b = −.10, p < .001).
Several social factors are significantly associated with adult depressive symptoms, specifically factors related to trauma. Respondents who reported that their parents or caregivers abused them emotionally (b = .21, p < .001), physically (b = .07, p = .02), or sexually (b = .13, p = .01) in childhood have higher adult depressive symptoms scores than respondents without such history. Similarly, experiencing physical abuse in adulthood increases depressive symptoms scores by 10% (b = .10, p < .001). In addition, several measures of structural disadvantage are significantly associated with adult depressive symptoms. Receiving welfare at Wave 4 is associated with a 14% increase in depressive symptoms (b = .14, p < .001). A 1-unit increase in educational attainment reduces depressive symptoms scores by 7% (b = −.07, p < .001). Having at least one parent drop out of high school increases depressive symptoms scores by 5% (b = .05, p = .04), and a 1-unit increase in neighborhood disadvantage increases depressive symptoms scores by 11% (b = .11, p < .001).
Discussion and Implications
The current study sought to investigate the potential long-term effects of parental incarceration by examining whether parental incarceration in childhood or adolescence predicted depressive symptoms in adulthood and whether this relationship varied by racial/ethnic group. The analysis finds mixed support for the hypotheses. It appears that respondents who first experienced parental incarceration during childhood or adolescence, especially before birth or age 1, are at risk for exhibiting depressive symptoms in adulthood, indicating that parental incarceration might confer long-term consequences on the mental health of this subgroup in particular.
Although respondents in the before birth or age 1 subgroup were not yet born or were too young to recall the parental incarceration event, it is important to remember that these respondents first experienced parental incarceration during this time. At least 48% of these respondents experienced parental incarceration sometime after this period as well. 13 Because the onset of their parental incarceration experience was very early, they had more time than the other subgroups to accumulate multiple parental incarceration events and incur more strains such as home displacement, parent’s unemployment, and instability from having a parent incarcerated, released, and reincarcerated (Wakefield & Wildeman, 2011). It is possible that their cumulative parental incarceration experiences contribute to their risk for adult depressive symptoms.
While the results show some support for the first hypothesis, they refute the second hypothesis which predicts racial/ethnic differences in the effects of parental incarceration. The risk for developing adult depressive symptoms is similar among White, Black, Hispanic, and other race offspring with parental incarceration histories. This result is consistent with findings from Swisher and Roettger’s (2012) study, which found that the relationship between parental incarceration and current depressive symptoms was similar across racial/ethnic groups.
Implications
Findings from the current study have implications for future research, theory, and policy. To start, findings are partially consistent with those from prior studies that suggest that the consequences of parental incarceration on mental health might be long term for offspring as they emerge into adulthood (Lee et al., 2013; Murray & Farrington, 2008b). However, the current study differs from these studies by showing that parental incarceration does not affect everyone the same, at least when examining depressive symptoms, and that the effects of parental incarceration might be long term only for certain segments of the population, particularly those who first experienced it early in life. Findings from the current study suggest the need to move away from examining “average effects” and begin examining the potential conditional effects of parental incarceration, as some studies have done (Besemer et al., 2011; Foster & Hagan, 2009; Swisher & Roettger, 2012).
In addition, while the parental incarceration literature overwhelmingly focuses on the consequences of parental incarceration for minor children, researchers should expand their scholarly focus on the long-term consequences of parental incarceration when children become adults. Adult offspring might be at risk for the adverse consequences of parental incarceration as well. This also means including adult offspring in our data collection efforts. For example, the Bureau of Justice Statistics, the primary source for national statistics related to parental incarceration, only gathers data on children below the age of 18, leaving more to be learned about the prevalence and nature of parental incarceration at the national level (Glaze & Maruschak, 2010). Criminologists must also expand their research agendas by studying the broader effects of parental incarceration beyond crime-related outcomes to better understand the ramifications of incarceration.
Strain theory posits that once a parent is incarcerated, children begin experiencing negative emotions, structural and economic changes, and strained relationships. This explanation suits proximate, short-term consequences of parental incarceration better than long-term ones. The mechanisms that contribute to the long-term effects of parental incarceration in adulthood are unclear. In the context of this study, it is unlikely that levels of depressive symptoms are static and children constantly exhibit them through adulthood. This is because depressive symptoms tend to be episodic and triggered by stressful events rather than enduring (Hammen, 2003; Kessler & Wang, 2009). It is more likely that early parental incarceration experiences influence adult depressive symptoms via intervening social and structural strains that accumulate over time, similar to Sampson and Laub’s (1997) concept of cumulative disadvantage, and increase the risk of adverse outcomes. Future studies ought to elucidate the intervening mechanisms of the longitudinal relationship between parental incarceration and adult outcomes.
In light of this study’s findings and findings in the parental incarceration literature, the potential long-term damage of parental incarceration indicates the need to adopt policies and practices that reduce harm on offspring. Criminal justice policymakers should carefully evaluate whether the benefits of incarceration outweigh the numerous short-term and long-term social costs when deciding to incarcerate. Of course, some children might benefit from parental incarceration if the parent is violent, but most incarcerated parents are non-violent offenders (Glaze & Maruschak, 2010). It might be better to rely on community corrections and rehabilitative treatment as alternatives to incarcerating non-violent offenders and reserve confinement for the most serious offenders. In addition to criminal justice reform, parental incarceration scholars recommend social reform that includes greater public investment in quality education, social welfare, drug treatment, and work-training programs for disadvantaged populations (Wakefield & Wildeman, 2013). Current intervention efforts should also focus on providing psychological, economic, and social resources to help offspring and families cope with parental incarceration. Furthermore, mental health scholars advocate for national health insurance policies that provide universal health insurance coverage and include the treatment of mental health disorders (Kessler et al., 1997). The association between parental incarceration and mental health problems, in this study and in previous studies, supports the need for such policy, so individuals can have widespread access to treatment for depression.
Conclusion
All in all, this study adds to the literature by considering how parental incarceration might compromise the psychological well-being of millions of Americans in the long term. Depressive symptoms are a public health concern as they can invade various domains of life such as health, work environments, educational attainment, romantic relationships, and parenting/child rearing (Hammen, 2003; Kessler & Wang, 2009; Kessler et al., 2006), and depressive symptoms can be related to offending (Burt, Simons, & Gibbons, 2012). Thus, the policy to incarcerate massive numbers of parents appears to exacerbate social problems, especially for already disadvantaged populations (Arditti et al., 2003; Wakefield & Wildeman, 2013). These consequences can reverberate through families and create long-term problems, even after depressive symptoms subside. In light of abounding empirical evidence linking incarceration to adverse consequences for offenders, their children, and communities, policymakers are compelled to implement effective policy changes to reduce the harm of parental incarceration on society.
Like all studies, the current work contains research limitations that should be considered. Items in the Add Health data could be subject to report or recall bias, especially when reporting retrospective accounts of parental incarceration. Some respondents might have purposely or unintentionally provided inaccurate information. Furthermore, measures of parent’s antisocial behavior and mental health status are absent from Add Health and the current analysis. However, the current study includes three measures of childhood abuse by a parent or caregiver, parent’s educational attainment, and parent’s welfare receipt that likely capture at least part of these underlying factors. In addition to these data limitations, it is important to note that associations between parental incarceration history and adult depressive symptoms might not be uniquely attributed to parental incarceration. Many individual, social, and structural factors were significantly associated with the outcome, indicating that these factors contribute to adult depressive symptoms as well. I therefore carefully refer to these findings as mere associations and do not make causal claims.
Footnotes
Acknowledgements
Special acknowledgment is due to Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from Grant P01-HD31921 for this analysis. In addition, the author extends much gratitude to Drs. Beth Huebner, Janet Lauritsen, Richard Rosenfeld, Robert Bursik, Elaine Doherty, Michael Campbell, and Matt Vogel for their helpful comments on previous drafts and to Dr. Matt Vogel for help with accessing the restricted data used in this study. None of these individuals is responsible for the content of this research.
). No direct support was received from Grant P01-HD31921 for this analysis. In addition, the author extends much gratitude to Drs. Beth Huebner, Janet Lauritsen, Richard Rosenfeld, Robert Bursik, Elaine Doherty, Michael Campbell, and Matt Vogel for their helpful comments on previous drafts and to Dr. Matt Vogel for help with accessing the restricted data used in this study. None of these individuals is responsible for the content of this research.
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by Grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations.