
Abstract
The current study examines multiple pathways to antisocial behavior involving neurobiologically based measures and indicators of executive functioning in the interest of informing treatment and intervention services for the deepest end juvenile justice placements. Specifically, using a statewide, multiyear sample of over 11,000 male juvenile offenders completing residential commitment placements, we employ structural equation modeling (SEM) to examine whether parental drug, alcohol, and mental health problems have a direct effect on neurocognitive deficits (as measured by formal Attention-Deficit/Hyperactivity Disorder [ADHD], or formal Conduct Disorder [CD] diagnoses) and temperamental deficits (as measured by effortful control and negative emotionality), which in turn are examined for their direct effects on recidivism. Results show that parental problems were associated with an increased likelihood of formal ADHD diagnosis as well increased negative emotionality among youth. Furthermore, ADHD and temperamental deficits (both effortful control and negative emotionality) were significantly related to continued offending. These findings may be helpful in treatment planning, targeting of intervention, and discussions of primary and secondary prevention efforts.
Keywords
Introduction
Individual-level constructs relating to self-regulation and the cascade of behavioral processes that flow from it hold prominence within major theoretical frameworks that were developed to explain a variety of antisocial and criminal behaviors (Gottfredson & Hirschi, 1990; Moffitt, 1990, 1993; Raine, 1993; Wilson & Herrnstein, 1985). Although there was initial resistance to the power of individual-level constructs relating to self-control, the empirical evidence accumulated so quickly and resoundingly that the discipline recognized it was here to stay. Approximately 20 years later, further attention on individual-level constructs gained momentum with the advent of biosocial research asserting that individual-level constructs are themselves downstream manifestations of higher order neurological processes and neuropsychological constructs, both of which are moderately to profoundly heritable in their etiology (Blair, 2004; Davidson, Putnam, & Larson, 2000; DeLisi, 2014; Dorfman & Buckholtz, 2014; Raine, Lencz, Bihrle, LaCasse, & Colletti, 2000; Séguin, 2004). In this way, biosocial research demonstrated that self-regulation/self-control should also be studied from neuropsychological and neurogenetic perspectives to fully understand its development and subsequent associations with conduct problems as well as criminal justice outcomes. In keeping with this line of research, the current study examines the effects of neurocognitive deficits and temperamental indicators on recidivism of juvenile offenders released from long-term residential placement. Specifically, we assess the extent to which parental drug, alcohol, and mental health problems are related to recidivism by influencing the likelihood that juveniles would display neurocognitive deficits, namely, Attention-Deficit/Hyperactivity Disorder (ADHD) and Conduct Disorder (CD), as well as exhibit two specific types of temperamental deficits, effortful control (EC) and negative emotionality (NE).
Executive Governance, Neuropsychological Deficits, and Crime
Fundamentally, the prefrontal cortex or frontal cortical area is responsible for modulating emotional stimuli that are produced from the limbic system or subcortical area. A large body of research has accrued on these integral emotional centers implicating the limbic system in altered reward processing that is germane to not only the study of pathological criminal behavior, but also addictive disorders, which are characterized by compulsive substance seeking despite negative consequences (DeLisi, Umphress, & Vaughn, 2009; Marsh & Blair, 2008; Volkow, 2003; Volkow, Koob, & McLellan, 2016). Findings from previous research suggest that subareas of the prefrontal cortex, such as the dorsolateral prefrontal cortex, orbitofrontal cortex, medial prefrontal cortex, and anterior cingulate cortex are specifically involved in a variety of functions that are required for behavioral competence. These functions, including decision making, impulse control, emotional control, reward anticipation, information processing, maintenance of goal-directed behavior, working memory, and others are known as executive functions. Those with strong executive functioning (or executive governance) are adept at modulating emotional and behavioral stimuli to comply with social norms. Conversely, those with weak executive functioning are at increased susceptibility for poor emotional and behavioral control that manifests in a variety of ways including imprudent norm violations, aggression, delinquency, and criminal violence (Monahan, Steinberg, & Piquero, 2015). Indeed, in their review of the connection between the frontal lobe and problem behavior, Cummings and Miller (2007) suggested,
The orbitofrontal cortex, particularly the right-hemispheric orbitofrontal regions, mediates the rules of social convention. Patients with orbitofrontal lesions are socially disabled, manifesting interpersonal disinhibition, poor social judgment, impulsive decision making, lack of consideration for the impact of their behavior, absence of an appreciation for the effect of their behavior or comments on others, and lack of empathy for others. (p. 15)
The causal link (or endophenotype) between executive functioning and crime appears to be centered upon neuropsychological deficits. It is these neuropsychological deficits that criminologists have uncovered that are so closely related to one’s propensity for crime through such constructs as self-control. And, importantly, low self-control has been shown in prior work to be relatively stable from adolescence through emerging adulthood (Vaske, Ward, Boisvert, & Wright, 2012). At the same time, related literature on the stability of self-control reflects both continuity and change (or relative and absolute stability; Diamond, 2016; Turner & Piquero, 2002), with components of self-control (impulsivity and sensation seeking) having distinct developmental impacts on offending behavior (Burt, Sweeten, & Simons, 2014). From this perspective, it is understandable as to why Raine (1993) and others (mainly in psychiatry) have long viewed criminal behavior as a clinical disorder.
Neuropsychological deficits are an expressed part of major general theoretical statements on antisocial behavior (e.g., DeLisi & Vaughn, 2014; Glenn & Raine, 2014; Moffitt, 1993) and are explicitly implicated in mainstream criminological theories (Gottfredson & Hirschi, 1990). The evidence that neuropsychological deficits are associated with antisocial behavior is overwhelming. In a meta-analytic review of 43 structural and functional brain imaging studies, Yang and Raine (2009) found that compared with healthy controls, antisocial individuals displayed both structural and functional reductions in the orbitofrontal cortex, anterior cingulate cortex, and dorsolateral prefrontal cortex. These reductions contributed to deficits relating to behavioral control, affective and cognitive flexibility, impulsivity, disinhibition, and aggression, among others. Furthermore, a more recent systematic review and meta-analysis of 29 structural and functional magnetic resonance imaging (MRI) studies on childhood behavioral disorders including Oppositional Defiant Disorder and CD revealed that even with or without Attention-Deficit/Hyperactivity Disorder (ADHD), there were abnormalities in emotional processing and regulation, specifically implicating “hot” areas of executive functioning such as bilateral amygdala and bilateral insula, right striatum, and left medial superior frontal gyrus (Noordermeer, Luman, & Oosterlaan, 2016).
Among social science research, a variety of studies including those using nationally representative data such as the Early Childhood Longitudinal Study, Kindergarten Class of 1998-1999 (Beaver, Wright, & DeLisi, 2007), National Collaborative Perinatal Project (Piquero, 2001; Piquero & White, 2003), National Survey of Children (Ratchford & Beaver, 2009), and National Longitudinal Study of Adolescent to Adult Health (Beaver, DeLisi, Vaughn, & Wright, 2010; Jackson & Beaver, 2013) have shown that neuropsychological deficits contribute to reduced self-control and increased involvement in diverse forms of antisocial behavior. Linkages between neuropsychological deficits and crime are also robust using clinical/offender samples. Drawing on data from juvenile offenders in the California Youth Authority, Cauffman, Steinberg, and Piquero (2005) found significant associations between neuropsychological deficits, low self-control, and serious offender status. Similarly, psychiatric typologies also show the salience of neuropsychological deficits to crime as youth and/or adults with ADHD, CD, and Antisocial Personality Disorder present with significant neuropsychological deficits that contribute to their aggressive and antisocial behavior (Moffitt et al., 2011; Moffitt & Caspi, 2001; Séguin, Arsenault, & Tremblay, 2007; Séguin, Nagin, Assaad, & Tremblay, 2004; Séguin, Pihl, Harden, Tremblay, & Boulerice, 1995; Vaughn, DeLisi, Beaver, & Wright, 2009; White, Moffitt, Earls, Robins, & Silva, 1990). Along these lines, research has indicated that adolescents with ADHD evidence significantly worse performance on neuropsychological measures of executive function, and that among youth with clinically elevated externalizing problem behaviors, executive function deficits are specific to those with ADHD (Clark, Prior, & Kinsella, 2000). Similarly, childhood ADHD has been demonstrated to be associated with neurocognitive deficits, polygenic risk, and residual life impairment, with diagnosed youth evidencing a mean IQ score 10 points below the norm, deficits in reading achievement, executive control, and verbal learning-delayed recall (Moffitt et al., 2015; see also Sjöwall, Roth, Lindqvist, & Thorell, 2013). In addition, the neurodevelopmental disorders of conduct disordered adolescents have been demonstrated through neuroimaging studies to include abnormalities in the paralimbic system regulating motivation and emotion control (Arnsten & Rubia, 2012).
To be sure, the overall impact of these developments is that a focused and empirically supported neurocriminology has emerged (Glenn & Raine, 2014). However, despite the ongoing achievements of this emerging area of work, numerous research gaps are in need of attention. One of these gaps involves the explicit application of neurocriminology to criminal justice populations, adults, and juveniles, to draw closer linkages between the basic scientific work on the epidemiologic and etiologic fronts and the applied sciences of prevention and treatment. One such linkage, examined in the current study, is between parental mental health and substance abuse and juvenile antisocial behavior. Prior longitudinal work on the intergenerational transmission of offending has indicated parental alcohol and drug use have a significant positive relationship with convictions among their offspring (Auty, Farrington, & Coid, 2015). Finding increased parental drug and alcohol use relating to more offspring convictions held for both male and female offspring, especially when the father was involved in such use (Auty et al., 2015). In addition, Moffitt’s (1993) hypothesized life-course persistent offenders are more often reared in adverse home environments, including those with parental mental health problems. Both parental mental health problems and parental substance abuse are included in the Centers for Disease Control and Prevention’s measure of adverse childhood experiences (ACEs), which have demonstrated relationships to a host of health and behavioral problems, including juvenile recidivism (Centers for Disease Control and Prevention, 2016; Felitti et al., 1998; Wolff, Baglivio, & Piquero, 2015).
Based on this review, even the most descriptive of research studies is needed for prevention and intervention efforts directed toward pertinent populations. As discussed, one such population is juvenile offenders. Specific to the study site used in the current study, the statewide average recidivism rate for juveniles completing long-term residential programs in Florida between July 1, 2009 and June 30, 2013 has ranged from 41% to 46% (Florida Department of Juvenile Justice [FDJJ], 2016). Comparably, analysis of a 7-year follow-up from the Pathways to Desistance study found recidivism rates ranging from 75% to 80% (Brame, Mulvey, Schubert, & Piquero, 2016). With between four and five of every 10 juveniles completing placement in Florida being reconvicted within 1 year of release, research regarding the pathways to juvenile reoffending is paramount.
Current Study
The current study examines multiple pathways to recidivism involving neurobiologically based measures and indicators of executive functioning in the interest of informing treatment and intervention services for the deepest end juvenile justice placements (youth committed to long-term juvenile residential facilities). Specifically, a statewide, multiyear sample of male juvenile offenders completing long-term residential commitment placements was employed to examine whether parental drug, alcohol, and mental health problems have an indirect effect on recidivism through neurocognitive deficits, as measured by formal Attention-Deficit/Hyperactivity Disorder (ADHD), or formal CD, as well as temperamental deficits, as measured by effortful control and negative emotionality. Rather unique to the current study is that all measures (neurocognitive deficit and temperamental) were captured within the required statewide risk/need assessment. The following hypotheses are assessed:
Method
Data and Study Procedures
Data for the current study are inclusive of all White, Black, and Hispanic males who were released from an FDJJ residential program from July 1, 2009 to June 30, 2013 (N = 11,557), after successfully completing the program. In Florida, only a judge can commit a youth to a residential program, and commitments are for an indeterminate period of time (based on completion of case/treatment plan), and not an arbitrary or determinate length of stay. Subsequently, only a judge may approve the release of a juvenile placed in a residential program. To provide context regarding FDJJ long-term residential programs, any youth who has not obtained a high school (or equivalent) diploma attends school 25 hr per week, instructed by certified Florida teachers. All youth attend treatment groups and individual counseling sessions (provided by licensed or supervised therapists) based on their individualized needs. Group services predominantly include cognitive behavioral interventions (to address criminal thinking/thinking errors), skills training groups, substance abuse prevention or intervention (based on the youth’s substance use history and/or diagnoses), sex offender services (based primarily on offending history), mental health group services (such as healthy relationships, identifying internal and external triggers, and anger management), and family therapy. All residential programs have a behavior management system that requires level progression, with increased privileges per level.
Official FDJJ archival records from its Juvenile Justice Information System (JJIS) centralized database were used for demographic and placement information. This system also maintains all social, offense, and risk assessment history data for all youth referred (equivalent to an adult arrest). Demographic items were taken from the information system, and the remaining measures were gleaned from the Residential Positive Achievement Change Tool (R-PACT) risk/need assessment information also maintained in the information system. The R-PACT is administered to each youth at intake, every 90 days to assess changes in risk/needs, and at release. The exit (at release) R-PACT is used in the current study to capture the youth’s risk and needs just prior to the 12-month recidivism tracking period. Specific R-PACT items were used (as described below) to construct parental problem history measures, youth psychiatric diagnoses measures, temperament constructs, and other prominent risk factors (to ensure hypotheses are tested with adequate controls).
Measures
Dependent Measure: Recidivism
Recidivism was captured dichotomously as a new law offense (= 1) for which the youth was convicted/adjudicated within 365 days from release from the residential program. Both juvenile and adult official records were included as some youth were 18 years of age or older at release, and some youth turned 18 during the 12-month follow-up. Only new law violations are included; technical/nonlaw violations, such as failed drug screenings or curfew violations are excluded. Importantly, only convictions/adjudications for arrests that occurred in Florida were available and counted.
Problem History of Parents
Youth whose parents have a history of problems/issues, which arguably affect the youth’s upbringing and development, and may contribute to neurological deficits, are captured through two indicators: parental substance use problem history and parent mental health problem history. Parental substance use problem history ranged from no alcohol or drug problem history, either an alcohol or a drug problem history, or both an alcohol and a drug problem history (coded 0-2, respectively). Parental mental health problem history was dichotomous (= 1, else = 0). These items are based on self-reported information by the youth and parent either during the comprehensive psychosocial evaluation (conducted prior to admission by a licensed mental health practitioner, as explained below) or throughout placement during family therapy sessions or treatment team meetings.
Psychiatric Diagnosis: Behavioral Disorders
Prior to youth placement in a Florida juvenile justice residential program, the youth must first receive a comprehensive evaluation conducted by a licensed mental health practitioner (providers throughout the state, contracted by FDJJ). A comprehensive evaluation is the “gathering of information addressing physical health, mental health, substance abuse, academic, educational, or vocational problems of a youth for whom a residential commitment disposition is anticipated” (Florida Administrative Code, 2016, p. 1). The comprehensive evaluation providers conduct psychosocial histories, psychological testing, and include treatment and placement recommendations, and also include mental health diagnoses in their reports for each youth. These formal diagnoses are used to respond to a specific R-PACT item in the mental health domain where the assessor indicates all diagnoses that apply. The current study focuses on CD and Attention-Deficit/Hyperactivity Disorder. These specific diagnoses were selected due to their association with neurological deficits and related externalizing and antisocial behavior symptomology, as discussed earlier (Cauffman et al., 2005; Glenn & Raine, 2014; Mallett, Fukushima, Stoddard-Dare, & Quinn, 2013; Yancey, Venables, Hicks, & Patrick, 2013; Yang & Raine, 2009)
CD
Whether the youth has a formal psychiatric disorder diagnosis of CD was captured dichotomously (= 1, else = 0) through an R-PACT assessment item regarding the youth’s specific psychiatric diagnoses (as indicated by the comprehensive evaluation conducted by a licensed mental health professional, as discussed above).
ADHD
Whether the youth has a formal psychiatric disorder diagnosis of ADHD was captured dichotomously (= 1, else = 0) through an R-PACT assessment item regarding the youth’s specific psychiatric diagnoses (as indicated by the comprehensive evaluation conducted by a licensed mental health professional, as discussed above).
Temperament Constructs
Temperament represents a stable and largely innate tendency of an individual to both experience the environment and to regulate his or her responses to that given environment in a certain way (DeLisi & Vaughn, 2014). Both the self-regulation aspect (effortful control) and the extent to which an individual interacts with his environment in a generally negative way (negative emotionality) were included in the current study. Prior work examining recidivism among Florida juvenile offenders has used similar constructions of effortful control and negative emotionality, with significant results, supporting the face and construct validity of the current work (Baglivio, Wolff, DeLisi, Vaughn, & Piquero, 2016a; Wolff & Baglivio, 2015; Wolff, Baglivio, Piquero, Vaughn, & DeLisi, 2015).
Effortful Control
Five items from the R-PACT risk/need assessment were used to capture effortful control. The selected response to these items, as per the R-PACT protocol, is collaboratively agreed upon by the youth’s treatment team members. The treatment team is a multidisciplinary group composed of the youth’s therapist, case manager, member of the program’s administration (such as a program director), direct care staff, education representative, and medical/nursing staff. Self-report by the youth, as well as actual observation of youth’s behavior in various program settings (e.g., school, individual, and group therapy, on the unit interacting with other youth and staff) are considered.
School conduct
School conduct during residential placement was assessed along a continuum of good behavior/no problems with conduct, problems which were handled by teachers, problems that required an escalating response/additional staff involvement, and removals from the classroom (coded 0-3). Higher values indicate more serious school conduct problems. School conduct problems are operationalized as fighting or threatening students, threatening staff/teachers, overly disruptive behavior, crimes such as theft and vandalism, lying, cheating, and dishonesty.
Techniques for keeping out of fights
The youth’s ability to refrain from physical altercations with others is assessed as lacking the ability, rarely using techniques to keep out of fights, sometimes using such techniques, and often using techniques to avoid physical altercations (coded 0-3). Higher values indicate a greater skill at avoiding altercations.
Resisting peer pressure
The youth’s ability to resist peer pressure was measured on a continuum from 0 to 3, with higher values indicating a greater ability. The item ranged from lacking the ability, rarely using techniques to resist peer pressure, sometimes using such techniques, and often using techniques to resist peer pressure.
Avoiding trouble with others
The youth’s demonstrated use of techniques for avoiding trouble with others ranged from lacking the ability, rarely using techniques to avoid trouble with others, sometimes using such techniques, and often using techniques to avoid trouble with others (coded 0-3). Higher values indicate more ability to avoid trouble with others.
Using self-control
The youth’s demonstrated use of self-control skills to control aggression ranged from lacking the ability, rarely using self-control to control aggression, sometimes using such techniques, and often using self-control to control aggression (coded 0-3). Higher values indicate more self-control to control aggression.
Negative Emotionality
One R-PACT item assessed “cold variants” of NE (depression/anxiety), while three assessed “hot variants” (anger/irritability, frustration tolerance, and hostile interpretation of the actions of others). Similar to effortful control items, responses to NE items are based on collaborative agreement by the youth’s treatment team members through consideration of both youth self-report and extensive behavioral observation.
Depression/anxiety
A history of feelings of depression or anxiety was measured as no history, occasional feelings of depression or anxiety, consistent feelings, or impairment in everyday tasks due to feelings of depression/anxiety (coded 1-4). Higher values indicate a greater extent of depression/anxiety.
Anger/irritability
A youth’s history of feelings of anger/irritability was captured as no history, occasional feelings of anger/irritability, consistent feelings, or history of aggressive reactions to feelings of anger/irritability (coded 0-3). Higher values indicate greater dysfunction related to anger/irritability.
Frustration tolerance
A youth’s tolerance for frustration was captured as never gets upset over small things or has temper tantrums, rarely gets upset, sometimes gets upset, or often gets upset over small things/has temper tantrums (coded 0-3). Higher values indicate a lower level of tolerance to frustration.
Hostile interpretation
Hostile interpretations of the actions and intentions of others in a common nonconfrontational setting was included with higher scores indicating greater levels of hostility attributed to others’ actions and intent. Hostile interpretation ranges from primarily positive, primarily negative, and primarily hostile view of the intentions of others (coded 0-2).
Key Independent Risk Factors
Demographics
Race/ethnicity was captured through dichotomous indicators for Black (= 1) and Hispanic (= 1), with non-Hispanic White serving as the reference group. In addition, the age (continuous) at which the youth was released from the residential placement was included (ranging from 11 to 21 years of age).
Criminal History
Measures of prior official offending were included. Age at first offense was captured as per the R-PACT categories of 12 years and younger, 13 to 14, 15, 16, and 16 years and older (coded 1-5), where higher values indicate the youth was older when first arrested. The extent of prior juvenile detention center placements more than 24 hr was captured as none, 1, 2, or 3 or more (coded 1-4). Prior residential placement history (not including the current placement) was captured as none, 1, or 2 or more (coded 1-3), where higher values indicate a greater extent of prior long-term residential placements. The youth’s prior adjudicated felony offenses were captured as none, 1, 2, or 3 or more (coded 1-4), where higher values indicate more prior adjudications in each instance.
Individual Risk Factors
Measures of individual-level risk factors were included as controls. Specifically, a youth’s substance use history was captured as no past use of alcohol or drugs, past use, or past use and such use caused problems in certain life domains (coded 0-2, where higher values indicate more substance use and associated problems). Problem areas affected by substance use could include disruptions in education, causing family conflict, interfering with keeping prosocial friends, causing health problems, contributing to criminal behavior, or increased tolerance to the substance or withdrawal problems. Antisocial peer associations were addressed dichotomously separating youth with exclusively antisocial peers (= 1) from those with positive/prosocial or mixed peer groups. History of physical abuse captured youth who either self-reported such exposure, or whose child welfare records indicated such abuse (= 1, else = 0). Sexual abuse history was also dichotomous (= 1, else = 0), similarly based on self-report and child welfare records. Finally, incarceration/jail history of a member of the youth’s household was included (= 1, else = 0), based on youth self-report and corroborated with the comprehensive psychosocial evaluation conducted prior to admission. Descriptive statistics for all measures included in the current study are shown in Table 1.
Descriptive Statistics
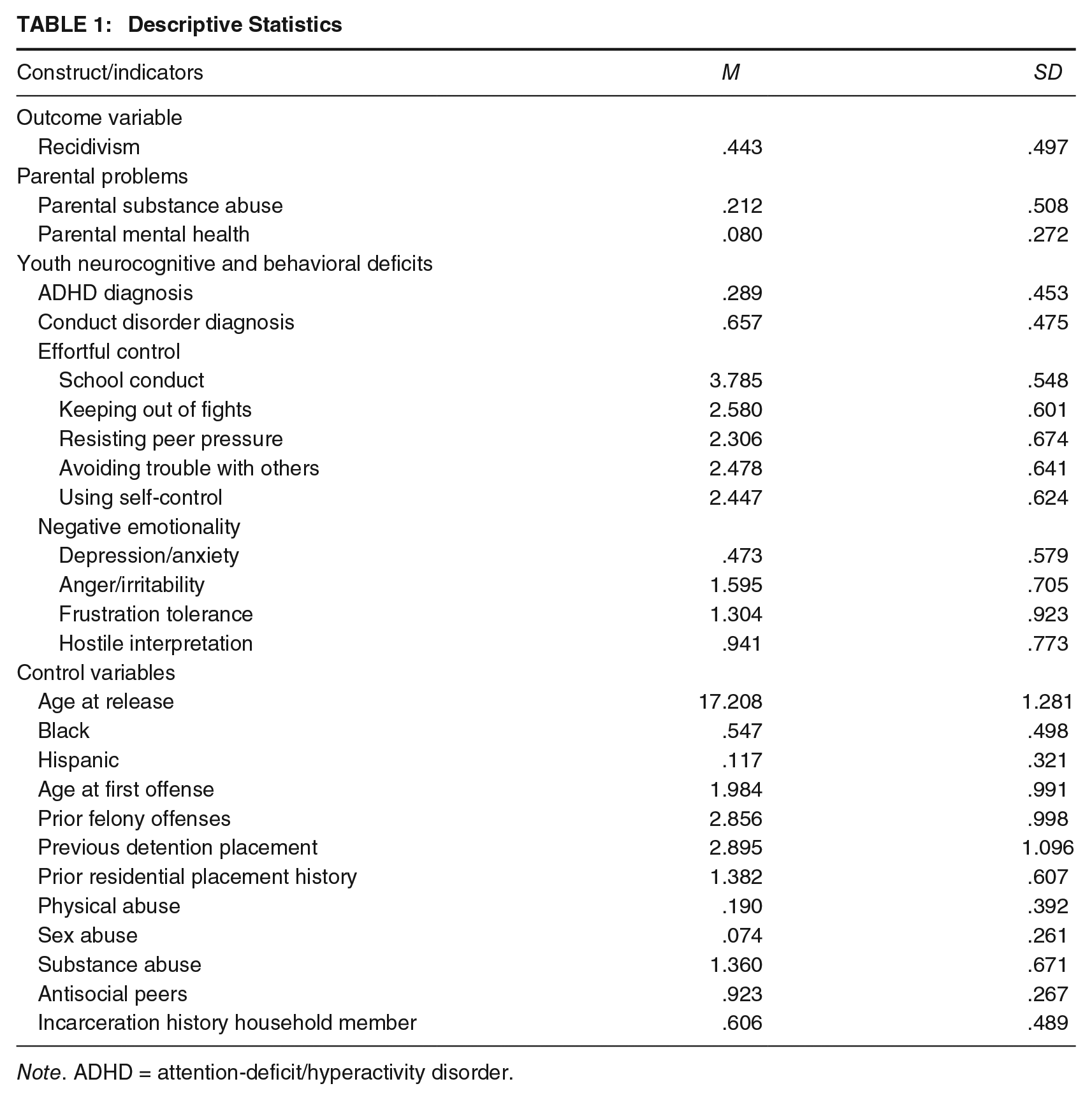
Note. ADHD = attention-deficit/hyperactivity disorder.
Analytic Strategy
As the current study seeks to examine the multiple pathways to recidivism involving neurobiologically based measures, and indicators of executive functioning, structural equation modeling (SEM) represents an appropriate analytic technique. Following Kline (1998), we use a two-step process, first developing a measurement model using confirmatory factor analysis (CFA), followed by a structural model to assess the relationship between variables in the model. The measurement model consisted of factor loadings for the observed variables that index the two latent variables (effortful control and negative emotionality). The structural portion of our model examines how parental problems affect executive functioning and temperament among youth and in turn how these factors are related to reoffending within this deep-end sample of youth placed in long-term residential facilities in the juvenile justice system. This model consisted of the two latent variables and all observed control variables. Fitting was done in MPlus Version 7.3 because of its ability to combine categorical, ordinal, and continuous data (Muthén & Muthén, 1998-2015). For each of these steps, we report a number of fit statistics (i.e., root mean square error of approximation [RMSEA], Tucker–Lewis index [TLI], and comparative fit index [CFI]), evaluating the fit of our final model using criterion developed by Hu and Bentler (1999). To test the hypothesized effects, the current study uses robust weighted least squared mean- and variance-adjusted (WLSMV) estimators with bias-corrected bootstrap confidence intervals (5,000 bootstrap replications). As traditional maximum likelihood (ML) estimators assume multivariate normality, and our outcome variables are dichotomous, ML would not provide accurate estimates and WLSMV represents the most appropriate approach (Brown, 2006). Bootstrap confidence intervals were used to guard against the problems of Type I error associated with the Sobel test. Following recommendations by MacKinnion, Lockwood, Hoffman, West, and Sheets (2002) as well as Preacher and Hayes (2008), a nonparametric resampling procedure that does not impose the assumption of normality of the sampling distribution was used to test the mediation process. These methods have been shown to be superior to the Sobel test in studies that assess indirect effects using large samples (MacKinnion et al., 2002; Preacher & Hayes, 2008).
Results
Measurement Models
Table 2 displays the results of the two preliminary measurement models assessed in the current study. The first measurement model that examined the components of effortful control demonstrated a good fit to the data (RMSEA = .041, CFI = .999, TLI =. 996). All factor loadings for the observed indicators are above Kline’s (1998) threshold of .50 and are all statistically significant (p < .001). The fit statistics, as well as size and significance level of the factor loadings suggest that the five measures are suitable indicators of their hypothesized trait, effortful control. The results for the measurement of negative emotionality are also displayed in Table 2. Again, all four measures load on a single construct, and fit the data adequately (RMSEA = .063, CFI = .891, TLI = .886). 1
Confirmatory Factor Analyses of Key Temperament Constructs
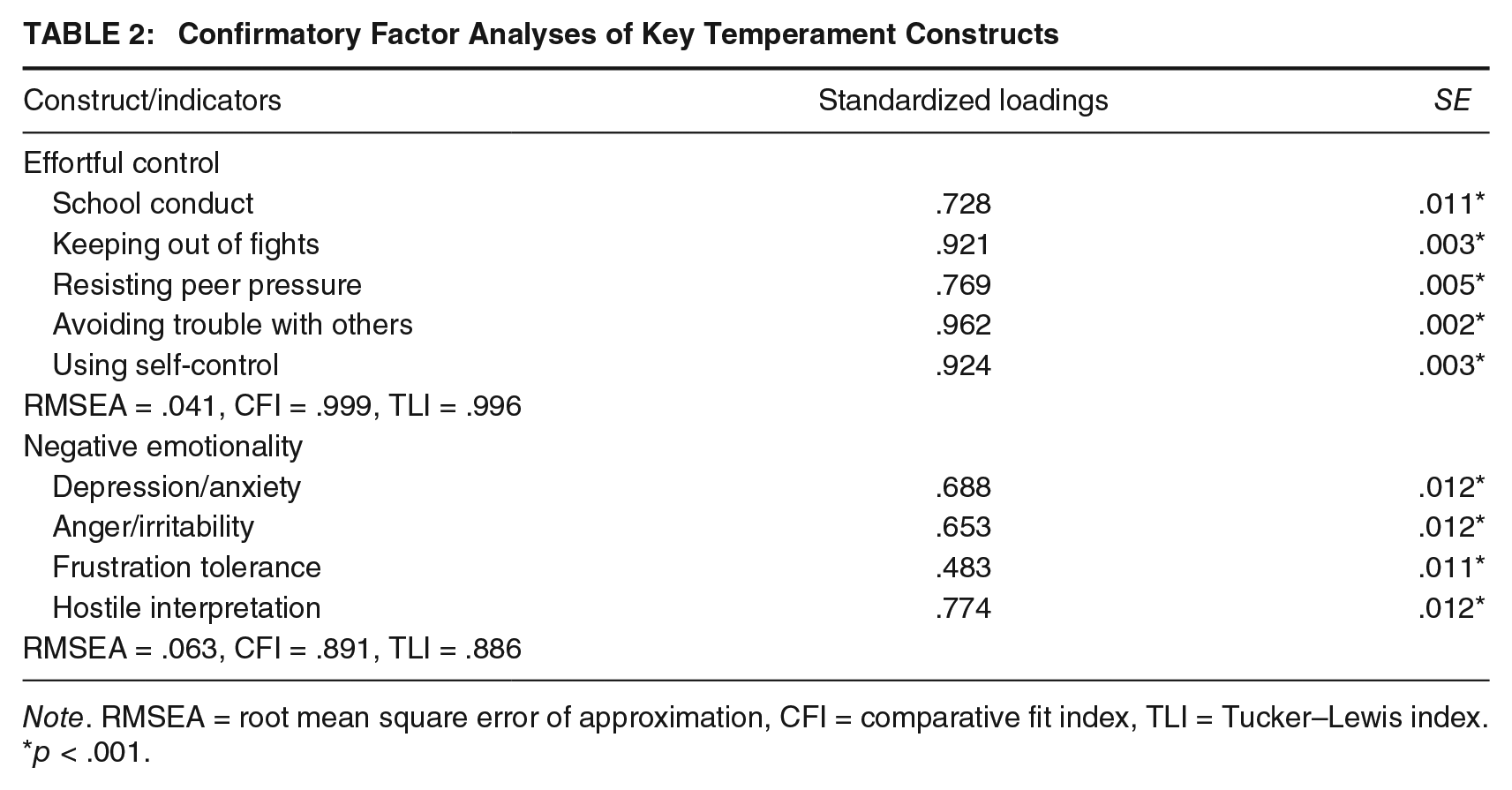
Note. RMSEA = root mean square error of approximation, CFI = comparative fit index, TLI = Tucker–Lewis index.
p < .001.
Structural Model
The results of the full structural model that examines whether parental substance abuse and mental health problems are associated with psychiatric diagnoses (CD and ADHD) and temperamental deficits (effortful control and negative emotionality) among youth in the juvenile justice system and, in turn, whether these youth characteristics are associated with continued delinquent behavior are presented in Tables 3 and 4. The fit statistics suggest that the structural model fits the data very well (RMSEA = .037, CFI = .983, TLI = .978).
Structural Equation Modeling Results Assessing the Impact of Parental Problems on Youth Psychiatric Diagnoses and Temperament Constructs
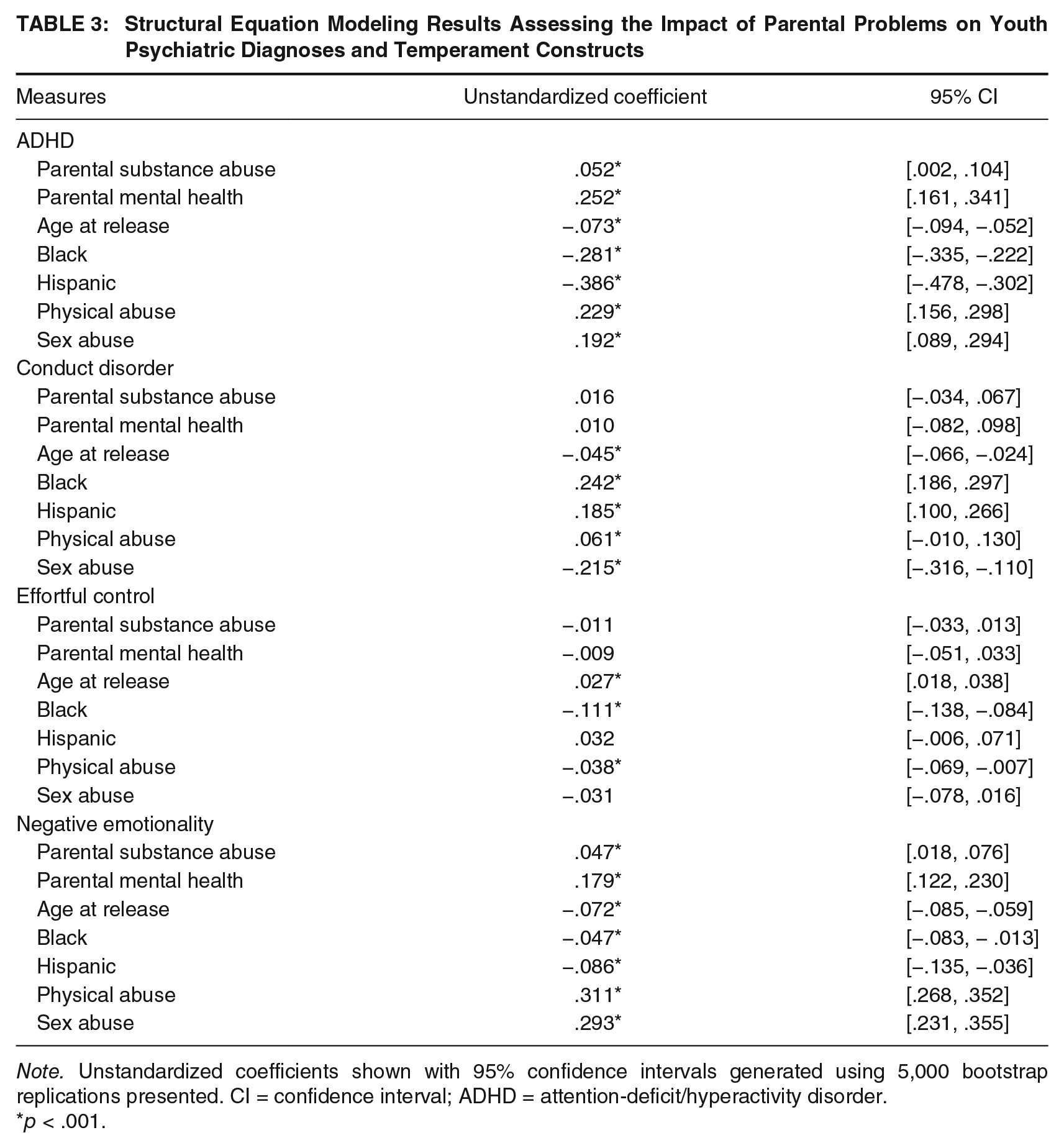
Note. Unstandardized coefficients shown with 95% confidence intervals generated using 5,000 bootstrap replications presented. CI = confidence interval; ADHD = attention-deficit/hyperactivity disorder.
p < .001.
Structural Equation Modeling Results Assessing the Impact of Youth Psychiatric Diagnoses and Temperament Constructs on Juvenile Recidivism
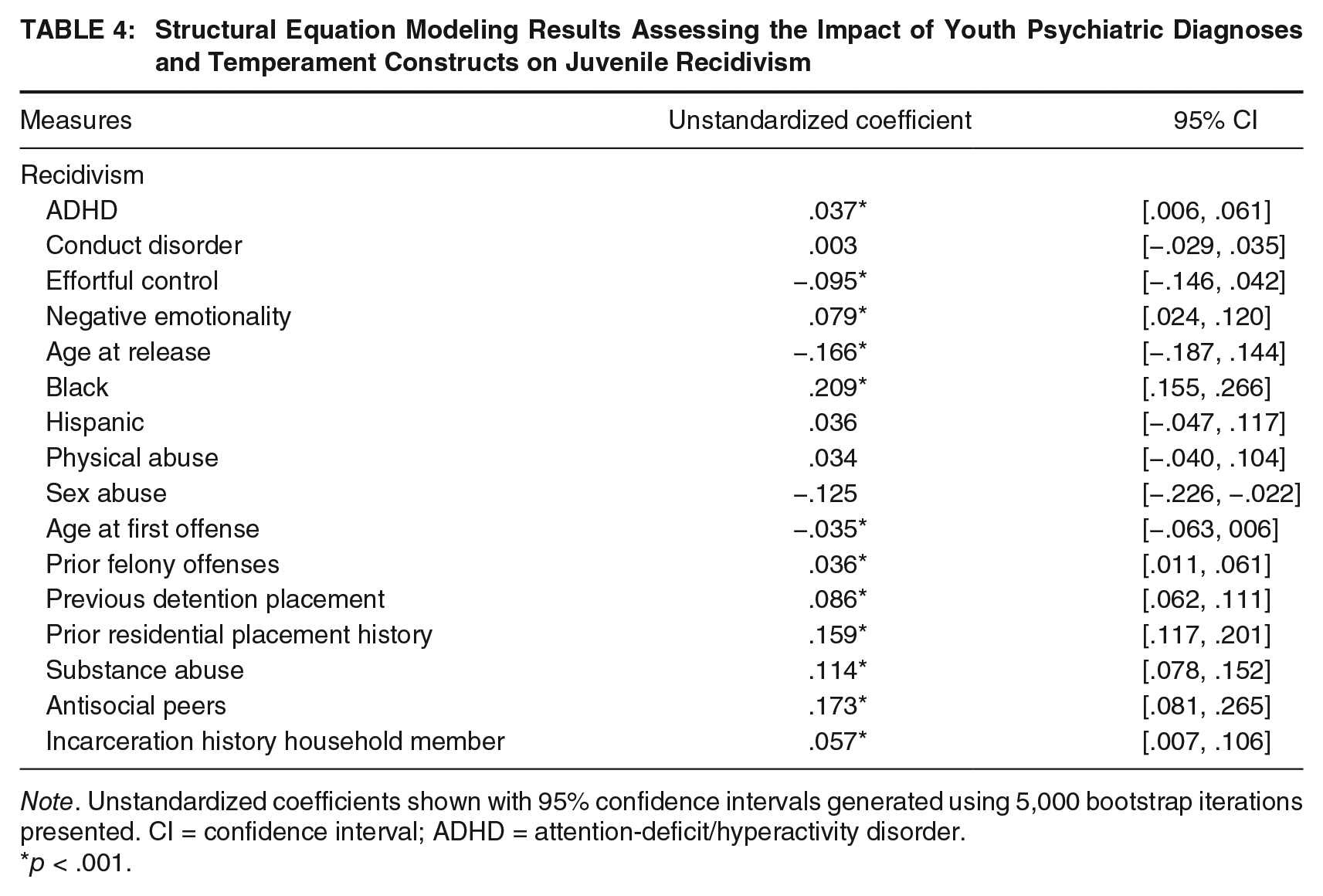
Note. Unstandardized coefficients shown with 95% confidence intervals generated using 5,000 bootstrap iterations presented. CI = confidence interval; ADHD = attention-deficit/hyperactivity disorder.
p < .001.
Table 3 presents the results pertaining to the link between parental problems and youth risk factors (ADHD diagnosis, CD diagnosis, effortful control, and negative emotionality). Both parental substance abuse and mental health issues were significantly related to formal ADHD diagnoses among youth (b = .052 and .252, respectively). Surprisingly, neither of the parental problem measures included in the current study was related to an official CD diagnosis or levels of effortful control among youth. However, both parental substance abuse (b = .047; p < .05) and mental health problems (b = .179; p < .05) were significantly associated with an increase in negative emotionality within this sample of male offenders. Although not of central importance to the current study, of the controls included in this portion of the structural model, both race/ethnicity as well as history of physical and sexual abuse have fairly consistent effects on the measures of youth functioning within this sample of deep-end juvenile offenders. Overall, results suggest that parental problems have the ability to affect important proxies for executive functioning (psychiatric diagnoses and temperament deficits) within youth, which may contribute to continued involvement in the juvenile justice system. The results of this second portion of the structural model are presented in Table 4.
As shown in Table 4, three of the four measures of psychiatric diagnoses and temperament deficits considered were significantly related to juvenile recidivism. Specifically, youth with a formal ADHD diagnosis were more likely to recidivate (b = .037, p < .05), while the likelihood of recidivism was not related to having a CD diagnosis (b = .003, p > .05). In addition, both temperament constructs, effortful control (b = −.095, p < .05) and negative emotionality (b = .079, p < .05), were significantly associated with recidivism in the theoretically anticipated directions. Consistent with prior research, several demographic and individual risk factors included as controls in the structural model were significantly related to juvenile recidivism. Youth who began offending later in adolescence were less likely to recidivate (b = −.166, p < .05), whereas those with a greater number of prior felony offenses, or history of detention and/or residential placement, were more likely to recidivate. The presence of antisocial peers, substance abuse, or history of household incarceration were also significantly related to continued offending among male youth in the state of Florida.
Figure 1 displays the results of the full structural model in a reduced form (control variables and measurement portions omitted). Here, standardized coefficients are displayed. Again, we see that parental functioning has a significant effect on youth constructs which, in turn, affect the likelihood of recidivism. Specifically, parental substance abuse and mental health issues affect the likelihood of ADHD diagnoses and contribute to higher levels of negative emotionality among male youth. Along with levels of effortful control and several other individual risk factors, both ADHD and negative emotionality are significantly related to recidivism among this sample of male offenders. Below, the implications stemming from these findings for policy and prevention are discussed.
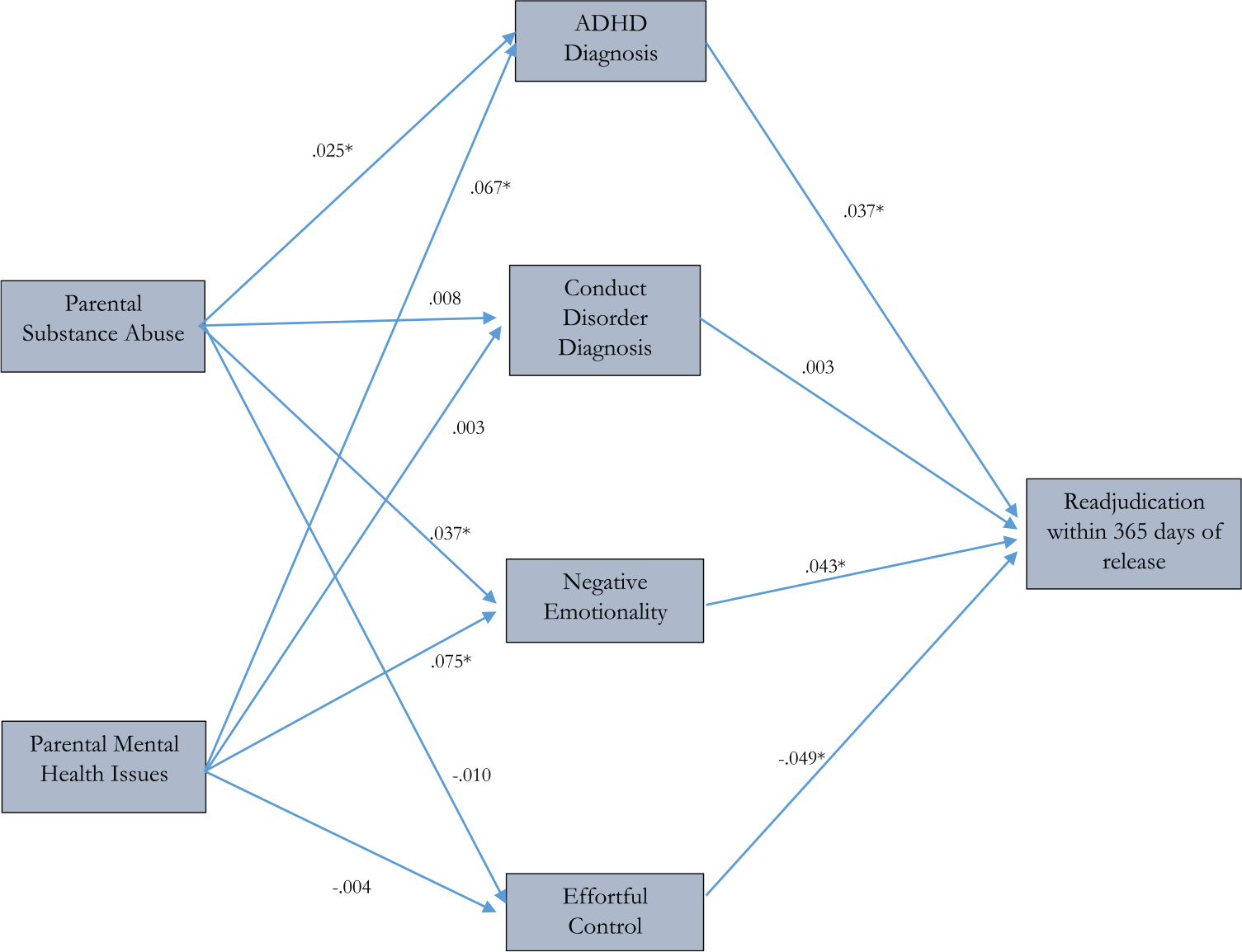
Pathway Analysis of Parental Problems, Youth Deficits and Temperament Issues, and Juvenile Recidivism
Discussion/Conclusion
Psychologists and psychiatrists have long been interested in the neuropsychological correlates of (antisocial) behavior and it was only as recent as the latter part of the 20th century that criminologists started to pay attention to this critical correlate of crime. So much has happened since the works of Wilson and Herrnstein, Raine, Moffitt, and Gottfredson and Hirschi to name a few, such that an entire field of neurocriminology has blossomed and started to flourish over the past 10 years (Glenn & Raine, 2014). The evidence for a neurobiological bases of criminal behavior is strong and growing stronger as researchers continue to study such correlates, as the requisite data become more widely available, and as the mysteries and puzzles associated with the brain and our biology start to get addressed and answered. Yet, because of the recency of this area of scholarship, a great many questions are in need of attention—especially those questions devoted on the populations that are at the forefront of both practice and policy, namely, serious adolescent offenders (Mulvey et al., 2004).
Accordingly, this study used data on a large sample of serious male adolescent offenders who were involved in the Florida juvenile justice system. Specifically, we examined multiple routes to recidivism that were a function of neurobiologically based measures and indicators of executive functioning. Specifically, we assessed the extent to which parental drug, alcohol, and mental health problems were related to recidivism by influencing the likelihood that offspring would evince two specific types of neurocognitive deficits, ADHD and CD, as well as exhibit two specific types of temperamental deficits, effortful control and negative emotionality. In addition, we were keenly interested in the extent to which ADHD, CD, and both effortful control and negative emotionality would be related to recidivism.
Our structural equation model–based analyses, which combined both measurement and structural models and provided good fit to the data, yielded three key conclusions. First, parental substance abuse and mental health issues were significantly related to formal ADHD diagnoses among youth as well as negative emotionality, but not CD diagnoses or effortful control. Second, ADHD, but not CD, was related to official recidivism within 1 year after the males completed treatment. Third, both effortful control and negative emotionality were significantly related to recidivism, the former inversely and the latter positively, as would be expected. Importantly, the findings predicting recidivism held even after controlling for a wide range of relevant risk factors.
These results, while helping to inform the growing knowledge base surrounding neurocriminology, are also especially relevant for informing treatment and intervention services for the deepest end juvenile justice placements, being those youth placed in long-term residential facilities. Of course, we are cognizant of the fact that identification of neurological, neuropsychological, and especially neurobiological correlates may cause some readers concern, but we also believe that there is a socially acceptable way to target such risk factors and develop prevention and intervention programs in a thoughtful manner. In fact, there already exists several different evidence-based strategies for improving self-control among children and adolescents (Piquero, Jennings, & Farrington, 2010; Piquero, Jennings, Farrington, Diamond, & Gonzalez, 2016b). One especially exciting program that has generated increasing attention and has been backed by very high quality scientific work is the Stop Now and Plan (SNAP) intervention, which is a cognitive behavioral self-control and problem-solving technique that helps children and their parents interrupt negative behavior patterns and replace them with more positive options (https://childdevelop.ca/snap/home). Several empirical investigations of SNAP, using both quasi and experimental designs, have shown very positive effects on a wide variety of outcomes including CD, delinquency, and violence (Augimeri, Farrington, Koegl, & Day, 2007; Burke & Loeber, 2014, 2015).
We do need to acknowledge several limitations to the current study. First, only Florida juvenile offenders were included, limiting generalizability to other states. In addition, the current study did not control for the year the juvenile was released or geographic measures. These limitations should be tempered somewhat as Florida is a large, diverse state, with juvenile offenders coming from and returning to all counties across the state. Furthermore, recidivism rates ranged narrowly from 41% to 44% across the years included. Being concerned with parental problems and neurological deficits, geographical and annual recidivism differences may not be critical; nevertheless, results should be interpreted with those limitations in mind. We argue that including geographic indicators may mask the effects of parental problems or neurological deficits on juvenile recidivism to the extent those measures differ across locales. Avenues of future work, however, should explore the nexus of differences in neurological deficits and parental problems across geographical contexts, such as rural and urban areas.
In addition, the current study relied upon youth and parent self-report to capture the parental mental health and parental substance abuse problem history. Although self-report of these items has been used in prior work examining juvenile offenders in Florida (cf. Baglivio, Wolff, DeLisi, Vaughn, & Piquero, 2016b; Wolff, Baglivio, & Piquero, 2015), we acknowledge that psychometrically sound clinical assessments of such issues would be preferable. Related to the measurement of constructs, the current study used a dichotomous recidivism variable. We note future work could use survival models to examine the timing of reoffending, which has additional implications for policy, including aftercare services and postrelease supervision of released offenders. Finally, although our study focused on the important role of parenting for understanding the neurological functioning of children, it is also possible that the parent problem–child neurological deficit association could be influenced by genetic factors (Dick, Viken, Kaprio, Pulkkinen, & Rose, 2005). Although our data do not contain genetic information, future research should attempt to tease out the various influences of the parent–child relationships investigated herein, including familial, social, and genetic factors.
Going forward, there is more to the recidivism-reduction puzzle than focusing on the neurological correlates of behavior. As our work showed, problems in temperament are also, in part, due to parental substance abuse and mental health problems. Working backwards, then, attention should be paid to the parental unit(s) in charge of caring for the offspring and resources and interventions need to be devoted to those persons as well. As before, there are several evidence-based programs that are effective in helping parents to overcome some of their problems, which in turn also help them to better socialize their children (see Piquero, Farrington, Welsh, Tremblay, & Jennings, 2009; Piquero et al., 2016a); Multicomponent treatments integrating family, cognitive behavioral, and behavioral strategies, such as Multisystemic Therapy (MST) and Treatment Foster Care Oregon (TFCO; previously Multidimensional Treatment Foster Care), evidence well-established empirical support in reducing maladaptive behavior among delinquent populations (McCart & Sheidow, 2016). In short, addressing the child and his or her neuropsychological/neurobiological problems is important, but it is also important to bear in mind that those children grow up in a certain familial context that is also important for understanding their overall socialization and ultimately their behavior.
Although the efficacy of multisystemic treatments with family components clearly supports their recommendation, policy and practice recommendations for youth placed in long-term residential commitment programs would be remiss to not mention difficulties surrounding family engagement. Residential youth, often from lower income families, may be placed several hours from home, making family visits (for both visitation and family therapy sessions), requiring money and time, difficult and burdensome. Efforts can be made to reduce financial burdens by providing hotel accommodations, gas cards, and meals to families willing to travel, and by having flexible visitation and family session scheduling. Technological advances, such as secure webcam software applications, can provide for viable alternatives and increase contacts, family sessions, and support for committed youth. As many youth suffer substantial maltreatment and abuse (Baglivio et al., 2014; Baglivio et al., 2015), they may be reluctant to commence family therapy, necessitating skilled therapeutic staff within programs to ascertain whether such therapy is appropriate, and to maintain fidelity to such practices while mediating family conflict. Beyond family therapy is the use of cognitive behavioral therapy (CBT) and cognitive skills programs in juvenile justice residential settings. While meta-analyses have demonstrated the efficacy of CBT and social skills training for offenders, with average recidivism reductions of 26% and 13%, respectively (Lipsey, 2009), recent work has indicated CBT programs may improve brain functioning across multiple neural regions, thus supporting its widespread implementation in juvenile residential settings (Vaske, Galyean, & Cullen, 2011). Indeed, FDJJ has embraced CBT and social skills training programming, as evidenced by its creation of a victim impact social skills training intervention for residential youth, which has been demonstrated to reduce social skills dynamic risk factors in a random control trial employing the same risk assessment used in the current study (Baglivio & Jackowski, 2015). This highlights the importance of not only assessing self-control, social skills, and temperament constructs to target intervention, but also the relevance of reassessment to measure change. Future work should continue to explore the potential of specific interventions to improve brain functioning and effortful control, and to reduce negative emotionality or behavioral reactions to emotionally charged stimuli.
Although it is rare for standardized risk/needs assessments to capture neurocognitive and temperamental indicators, the current study findings suggest the importance of including such measures. Prior work, examining various samples of Florida juvenile delinquents has also found both effortful control and negative emotionality predictive of subsequent offending (Baglivio et al., 2016a; Wolff & Baglivio, 2015; Wolff, Baglivio, Piquero, Vaughn, & DeLisi, 2015). The significance and strength of these measures in the current study, even after the inclusion of more traditional risk factor controls, further highlights their potential to enhance current risk/need assessment protocols. Additional examination is warranted into the extent to which neurobiological and temperamental constructs may improve predictive validity of prominent risk/needs tools, and whether such constructs hold similar value across race/ethnicity and gender subsamples and for subtypes of offending (such as drug, property, and violence). Furthermore, study of whether such measures are dynamic in nature and capable of indicating change across reassessments in response to targeted intervention (at varying dosages) is needed.
We not only are excited about the potential that our work may have for informing both theory and practice but also recognize that the knowledge base needs to grow and extend its research findings to develop the best possible prevention and intervention strategies. As such, there are many important topics to be considered. First, work should be extended to female samples to assess if the pathway(s) to recidivism via the neuropsychological route is the same as it is for boys. As well, future work should expand the type of parental problems focused on in the current study, perhaps to also include nutrition and stress. Recent evidence has in fact pointed to an important linkage between nutrition, self-control, and interpersonal violence, and we encourage further work in this area (see Vaughn, Salas-Wright, Naeger, Huang, & Piquero, 2016). Furthermore, studies should consider whether the links studied in the current article relate to other outcomes, such as violent behavior specifically and even other noncriminal life domains, such as failed relationships, poor health, and so forth. Echoing the recent work of Glenn and Raine (2014), “there is initial proof of concept that neuroscience can become an important influence in society’s approach to the punishment, prediction, and prevention of criminal behaviour” and we hope that such research is a key feature of criminological attention throughout the 21st century (p. 61).
Footnotes
Acknowledgements
The authors wish to thank the anonymous reviewers for suggestions on a previous draft of this article.