
Abstract
Community corrections professionals may employ shared decision making (SDM) in many ways with those they supervise who have serious mental illness (SMI). This study examined the psychometric properties of the Community Corrections Shared Decision Making Scale (CCSDM), an instrument developed to measure attitudes that support SDM in community corrections settings. Community corrections professionals were surveyed as to their support of collaborative decision making with their supervisees with SMI. Exploratory factor analysis (n = 146) and confirmatory factor analysis (n = 145) were used to explore and validate the scale’s factor structure. Results indicate the CCSDM functions as an internally consistent, two-factor scale useful for measuring attitudes toward SDM with people who have SMI and are under community supervision. Respondents were generally supportive of SDM. Given the benefits of SDM, assessment of these beliefs is essential to inform implementation strategies aimed at establishing SDM policies and practices in community corrections settings.
Shared decision making (SDM) can be defined as a process between providers and consumers of health-related services that involves sharing of information (e.g., treatment options, evidence of treatment efficacy, and associated outcomes along with consumers’ treatment preferences and values), consensus building as to preferred course of treatment, and agreement on treatment implementation (Charles, Gafni, & Whelan, 1997; Makoul & Clayman, 2006).
Employing SDM comports with the endorsement by the Institute of Medicine (IOM) of person-centered care that considers consumer preferences and satisfaction within health services (IOM, 2006). SDM leads to accord on treatment planning and promotes consumer adherence to treatment regimens and attainment of both physical (e.g., Goldring, Taylor, Kemeny, & Anton, 2002) and mental health treatment goals (e.g., Ludman et al., 2003). The benefits of sustained engagement in effective treatments for people with chronic, serious mental illness (SMI) can be substantial and include enhanced health and wellness as well as reduced criminal justice involvement (World Health Organization, 2005, n.d.).
A relatively unexplored area in research on SDM pertains to the subpopulation of individuals with SMI who are under criminal justice supervision in the community (i.e., probation or parole, together, termed community corrections here). Adherence to treatment regimens is particularly important with this group, as nonadherence not only precludes attainment of the benefits that accrue for those with SMI who are adherent and not justice involved but also may result in legal sanctions (including incarceration) that can be imposed as the result of noncompliance with justice system mandates for treatment (Skeem, Emke-Francis, & Louden, 2006). Community corrections can facilitate compliance with treatment mandates via SDM by working with clients to identify mutually agreeable treatment providers and by collaborating with providers and with clients to identify client-centered goals and agreed-upon service planning to attain these goals.
However, support for SDM among community corrections professionals can vary (Matejkowski, Severson, & Manthey, 2015), and the beliefs of these professionals about the appropriateness of using SDM with persons under their supervision who have SMI can negatively affect the implementation of SDM strategies in this context (Lipsky, 2010; Watkins-Hayes, 2009). This makes assessment of these beliefs essential to inform implementation strategies aimed at establishing policies and practices supportive of SDM in community corrections settings. As such, the purpose of this study is to examine the psychometric properties of the Community Corrections Shared Decision Making Scale (CCSDM), a novel instrument newly developed to measure attitudes that support SDM among professionals in community correctional settings serving persons with SMI. Considering that 70% of the persons under correctional supervision are supervised in the community (Kaeble & Glaze, 2016) and that there is increased opportunity to employ SDM in the community, the authors focus on community (vs. institutional) corrections.
Benefits of SDM in Mental Health Treatment
Involving mental health service consumers in the decision-making process can result in better agreement between consumers and providers on treatment-related choices (Hamann et al., 2009). Furthermore, research indicates that treatment engagement is fostered by a process that incorporates SDM, where the identification of specific goals that are meaningful and important to the person occurs (Adams & Drake, 2006; Joosten et al., 2008; Martin, Williams, Haskard, & DiMatteo, 2005; Tibaldi, Salvador-Carulla, Carlos, & Garcia-Gutierrez, 2011). When the interests of the two parties are aligned, a partnership, or therapeutic alliance, between service recipients and clinicians is established, satisfaction with and engagement in treatment is promoted, and progress toward service goals is advanced (Deegan & Drake, 2006; Malm, Ivarsson, Allebeck, & Falloon, 2003; Rapp & Goscha, 2012). “Simply put, mental health services, including prescription of medications, that are explicitly linked to patient-prioritized goals and offered in a way that facilitates opportunities for self-direction and SDM will drive greater service engagement” (Salzer, 2017, p. 753).
Research on the benefits of SDM with mental health service consumers is promising. One recent systematic review found clinician–patient alliance (i.e., agreement on treatment tasks) and collaborative communication between these parties in mental health care to promote treatment adherence (Thompson & McCabe, 2012). Another recent review found clients who were involved in SDM or received their preferred treatment had higher treatment completion and satisfaction with treatment and superior treatment outcomes compared with those clients whose preferences were not integrated into treatment (Lindhiem, Bennett, Trentacosta, & McLear, 2014). Research also indicates that mental health clients can be encouraged to be more actively involved in treatment discussions to promote their preferred course of treatment, and that doing so can ultimately maintain their engagement in treatment. For example, Alegria and colleagues (2008) tested an intervention aimed at empowering a sample of predominately racial/ethnic minority mental health consumers to more actively seek treatment information from providers and to become more involved in decision making. They found that those receiving the intervention had increased levels of “patient activation” (i.e., communicating with health care professionals and obtaining relevant information, asking questions about and discussing treatment options) over that of those who had not received the intervention. Moreover, persons in the treatment group were more than twice as likely as those in the comparison group to attend and to be retained in mental health treatment, with levels of patient activation associated with this engagement. Indeed, a collaborative bond between treatment provider and consumer has long been understood to promote engagement and positive outcomes for individuals in mental health treatment (Krupnick et al., 1996) and is beginning to be seen as important for the same reasons in the treatment of persons who are involved in the justice system (Marshall et al., 2003).
Employing SDM in Community Corrections With Persons Who Have SMI
More than 4.6 million people were under community corrections supervision at yearend 2015 (Kaeble & Glaze, 2016). It is estimated that 15% of these individuals have SMI and that those with SMI are likely (a) to have conditions of supervision that require engagement in mental health treatment and (b) to have difficulties complying with these conditions (Lurigio, 2001; Skeem et al., 2006; Skeem & Louden, 2006; Veysey & Bichler-Robertson, 2002). As such, integrating SDM into supervision and treatment services targeted to justice-involved individuals with mental illness may increase the likelihood of a substantial number of people engaging in mental health and crime reduction programs (Mann, Webster, Schofield, & Marshall, 2004; Netto, Carter, & Bonell, 2014), attaining the benefits of this treatment, and avoiding legal sanctions that can result from treatment nonadherence.
There are myriad ways in which community corrections professionals may employ SDM with those they supervise to promote engagement in mandated mental health treatment and supportive services. However, a similar engagement may need to occur first between the supervisee and his or her probation officer. This form of therapeutic alliance, or in the justice context what some term a “working alliance” (Morash, Kashy, Smith, & Cobbina, 2015; Taxman & Ainsworth, 2009), when perceived as positive by the supervisee, has been shown to be a powerful contributor to the supervisee’s perception of the relationship as a caring, fair, and trustworthy one, and also to improve supervisee outcomes, including criminal behavior that occurs during postrelease supervised periods (Blasko, Friedmann, Rhodes, & Taxman, 2015). This is akin to the concept of procedural justice, particularly the notion that having the opportunity to voice and have one’s opinion heard by authorities improves an individual’s assessment of the quality of decision making and interactions with law enforcement, thereby improving adherence to decisions (Thibaut & Walker, 1975; Tyler, 2003).
A working relationship characterized by trust, caring, and respect is likely to clear the way for the kind of problem-solving collaboration that needs to occur between the probation officer and supervisee for the latter to feel primed to engage in the clinical therapeutic experience. For example, when options exist, an officer, well trained to engage with the person who has significant mental health challenges, can work with him or her to identify preferred service providers. Once service providers are identified, collaborative discussions among the officer, provider, and client can involve person-centered goal planning, which situates the person receiving services as an integral director of care shaped by goals that are personally valued (Rapp & Goscha, 2012; Reuben & Tinetti, 2012; Tondora, Miller, Guy, & Lanteri, 2009). In this context, person-centered goal planning is a process between the officer, the individual, and the clinician in which a mutual exchange of information leads to identification of specific goals that are meaningful and important to the person and that meet public safety needs.
Once identified, the officer, clinician, and person work together to align treatment and support decisions with the person’s goals. Specifically, this translates into collaborative decision making with the person receiving services about what goals are most important, what approaches are to be taken, and selection of ways of monitoring and self-monitoring the outcomes (Reuben & Tinetti, 2012). Within these processes, the role of the officer is to help supervisees continually examine their thinking and behaviors, communicate and advise about the acceptability of their decisions and when their decisions conflict with public safety goals, and implement measures to prevent criminal behavior and recidivism (Lamberti, 2016; Lewis, 2014).
Collaborative community supervision models provide opportunities to employ SDM with supervisees (Lamberti, 2016). Examples of these models include collaborations among community corrections and substance abuse treatment providers (Friedmann et al., 2008) as well as specialty mental health probation that involves “officer coordination of and direct involvement in probationers’ treatment, and reliance on collaborative problem solving approaches” (Skeem, Manchak, & Montoya, 2017, p. E2). Some concerns related to these models (and by extension, with the SDM suggested here) include the sharing of protected health and treatment information, the inappropriate monitoring of conditions of supervision by treatment providers, and the additional skills required of community corrections officers to effectively contribute to shared treatment plans. However, research has shown that these concerns can be effectively managed with appropriate releases of information, training, and structural supports (for thorough descriptions and reviews, see Friedmann, Rhodes, & Taxman, 2009; Lurigio, 2001; Petrila, Fader-Towe, & Hill, 2015; Skeem & Louden, 2006).
Research specifically on the use of SDM with correctional populations who have SMI is limited. The good lives model of offender rehabilitation (Ward & Stewart, 2003) utilizes SDM through its focus on approach goals in treatment rather than on avoidant goals. The reframing of treatment goals from avoidant goals (i.e., the reduction of criminal risk) to approach goals that reflect prosocial outcomes sought by the justice-involved person is expected to result in reduced criminal behavior (Mann et al., 2004; Ward, Mann, & Gannon, 2007). In a randomized trial of this proposition with recipients of outpatient forensic psychiatric services in the Netherlands, Troquete and colleagues (2013) found no differential effect on violent or criminal incidents with the addition of SDM to standard services; though, the authors highlight differential attrition between the experimental and control groups may have contributed to the null findings. However, it is also important to note that the Troquete study did not specifically consider the significance that potential noncompliance with justice system treatment mandates has for contributing to technical violations of conditions of community supervision, recidivism, and reincarceration rates (Langan & Levin, 2002). Until these processes can be disentangled and the impact on these specific processes that engagement with treatment associated with implementation of SDM can be isolated, it is difficult to discount the potential benefits SDM may have for persons with SMI who are under supervision in the community. This is particularly so in light of the evidence supporting its use in the nonoffending population.
Measuring Attitudes Toward SDM Among Community Corrections Professionals
The attitudes and beliefs of frontline professionals play a critical role in the effective implementation of agencies’ policies and practices (Lipsky, 2010; Watkins-Hayes, 2009). Indeed, implementation science employs conceptual frameworks highlighting the role individuals’ beliefs and values related to agency policies and practices have in implementation, with valence of opinions being positively associated with behaviors supportive of implementation (e.g., Atkins et al., 2017; Damschroder et al., 2009; Proctor et al., 2011). In illustration, the 2008 findings by Alegria and colleagues cited above indicating positive effects of SDM on patient activation and treatment engagement were not subsequently replicated in a randomized controlled trial. The authors claim this negative finding was due, in part, to treatment professionals responding adversely to activated patients, increasing tension between patients and providers, and diminishing use of services (Alegría et al., 2014). Specific to implementation of evidence-based practices (EBPs) in criminal justice settings, in a review of the relevant literature, Viglione similarly concludes “research overwhelmingly suggests practitioner attitudes toward EBPs can either facilitate or impede adoption and implementation of EBPs” (Viglione, 2016, p. 3).
Collaborative decision making can be hamstrung in probation and parole services where public safety concerns often result in placing primacy on monitoring individuals’ compliance with imposed community supervision requirements (Young, 2015). These challenges can be compounded when the individual under supervision has an SMI. For example, a large proportion of people with SMI who are living under supervision in the community may be regarded as incapable of responsibly contributing to their own service planning (Matejkowski et al., 2015; Viglione, 2015). However, within the mental health literature, there is a wealth of research indicating that, despite experiencing severe psychiatric symptoms, individuals can and do contribute meaningfully to their own service planning (Drake, Deegan, & Rapp, 2010; Linhorst, Hamilton, Young, & Eckert, 2002). Similarly, criminological expositions suggest offenders are capable of contributing a valued perspective to the development of supervision plans and also highlight the value of offering those who are justice involved an opportunity to do so in collaboration with supervising officers (Taxman, 2013; Tyler, 2010).
As the research summarized above indicates, beliefs community corrections professionals hold in regard to the abilities of those they supervise to contribute to case planning meaningfully and via SDM can either hinder or promote its use. In addition to these beliefs regarding capacity, the research cited above suggests that the value community corrections officials place on developing a working alliance with those they supervise may affect use of SDM. It is, therefore, necessary to assess these beliefs to determine the methods that are likely to have the most success at promoting implementation of SDM.
Method
Participants
The target population was community corrections professionals who work directly with formerly incarcerated individuals who have an SMI. Table 1 shows descriptive statistics of the total sample (n = 291) and of the subsamples used to conduct the exploratory factor analysis (EFA; n = 146) and confirmatory factor analysis (CFA; n = 145). In aggregate, participants worked in regions across the United Sates and averaged 46.7 years of age. More than half were female (59%) and lacked a graduate degree (54%). A majority worked in county agencies (51%) and within urban settings (51%) and most supervised people leaving jail (79%) or prison (61%). To compare the characteristics of the EFA sample and the CFA sample, chi-square tests for categorical variables and an independent samples t test for the age variable were conducted. The results of bivariate statistics show that there were no significant differences between the EFA sample and the CFA sample on any of the study variables (p > .05), indicating that the two samples had similar characteristics.
Sample Characteristics
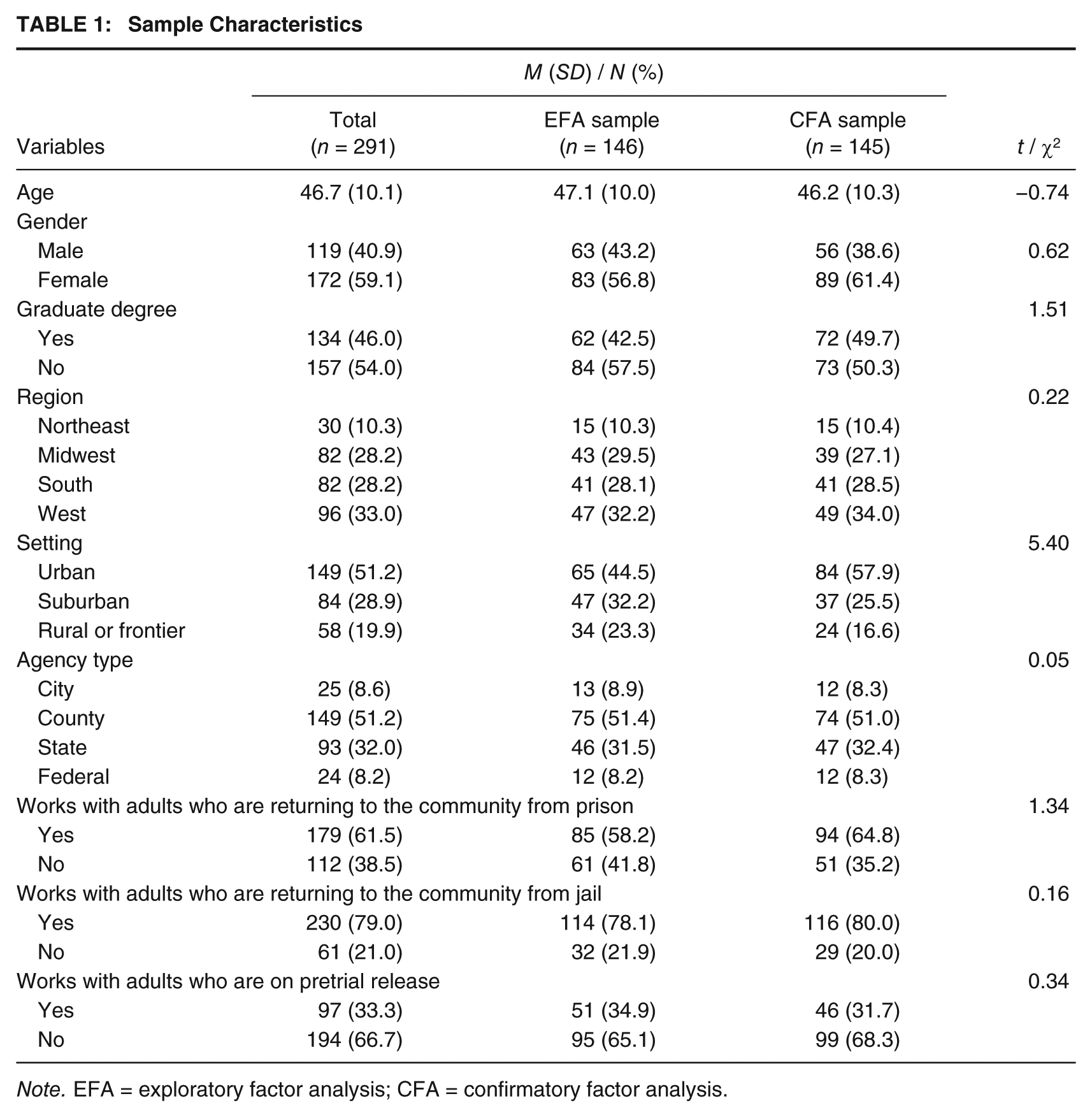
Note. EFA = exploratory factor analysis; CFA = confirmatory factor analysis.
Procedure
Approval for this research was granted by the institutional review board of the university with which the first author is affiliated. Study methods have been described previously (Matejkowski et al., 2015) and are summarized below.
Sampling Method
The American Probation and Parole Association (APPA) provided the sampling frame in the form of a list of its members. The APPA is an international association composed of members (i.e., dues-paying community corrections agencies and corporations or individual persons actively involved in community corrections as well as students, and interested citizens) from the United States, Canada, and other countries actively involved with probation, parole, and community-based corrections (APPA, 2009).
Recruitment of potential research participants began with the APPA sending an initial and two follow-up recruitment email messages to all those in their member database who provided the APPA with email addresses. Of the initial 6,200 email addresses to which APPA reported sending survey invitations, 1,173 were reported as no longer in service. The invitation and reminder messages contained a brief description of the study, a link to an anonymous survey and the notice that the current study was seeking only those community corrections professionals who were (a) currently working specifically with adults who have SMI and who were released from custody under supervision or (b) currently employed as an administrator or supervisor who has the authority to set policy regarding the approaches taken to the management and supervision of adults with SMI who had been released from custody under supervision.
Once participants clicked on the link to the anonymous survey, they were presented with a consent form describing the study. Those interested in participating were asked two questions designed to screen out individuals who did not meet one of the two inclusion criteria listed above (currently working directly with, or functioning as an administrator supervising those directly working with adults released from custody under supervision who have an SMI). Respondents were provided with the following definition of SMI to aid in their responses: An SMI is a mental, behavioral, or emotional disorder (excluding developmental and substance use disorders) that results in serious functional impairment, which substantially interferes with or limits one or more major life activities (see Substance Abuse and Mental Health Services Administration, 2013). A total of 291 individuals reported that they met the inclusion criteria, and were then presented with and completed the survey. As an incentive to their participation, respondents who completed the online survey were transferred to a separate online survey site and given the opportunity to enter their email address for inclusion in a random drawing for a US$100 gift card.
It is possible, as mentioned in prior research using similar survey methodology (e.g., Miller, 2014), that some APPA members forwarded the survey to non-APPA members. Moreover, not all APPA members who were emailed were likely to have been eligible to participate in the survey (e.g., not currently working directly or supervising those directly working with adults released from custody under supervision who have SMI). As such, it is not possible to calculate an accurate response rate to the survey.
The CCSDM
The CCSDM was developed with the aim of assessing attitudes supportive of collaborative decision making between community corrections officers and those they supervise. The CCSDM was developed after reviewing literature on SDM in recovery-oriented health and mental health care, the limited amount of literature of SDM in community corrections (e.g., Légaré et al., 2008; Scholl et al., 2011; Shared Decision Making Programme, 2012; Tatman & Love, 2010; Walters, Clark, Gingerich, & Meltzer, 2007), as well as lierature on how stigma may affect one’s views of the capabilities of persons with mental illness (e.g., Schulze, 2007; Wahl, 1999). Using the tools that were included in this review as a guide, and informed by the authors’ years of experience in mental health and criminal justice system settings, the authors developed 10 items that were subjectively determined to measure SDM in this context (i.e., to have face and content validity). Responses to each item are scored on a 1 to 4, strongly disagree to strongly agree, Likert-type scale.
Initial analysis of survey responses to these 10 items indicated that data associated with three of them displayed low variability, excessive missing values, and/or nominal correlation with other potential CCSDM scale items. These three items with undesirable properties were excluded from subsequent analyses. The remaining seven items, subjected to the analyses described immediately below, reflect the core ideas that offenders have the capacity to contribute a valued perspective to the development of supervision plans and that they are most likely to be offered an opportunity to do so by officers who value the development of a working alliance with those they supervise (Taxman, 2013; Tyler, 2010).
Data Analyses
First, to examine the extent to which the items were internally consistent with the CCSDM, an item analysis was conducted and Cronbach’s alpha was computed. Second, to explore and validate the CCSDM factor structure, EFA and CFA were conducted using Mplus 7.2. In the process of factor analysis, the total sample of 291 respondents was randomly split into two groups: one for the EFA (n = 146) and the other for CFA (n = 145).
Considering the nature of multilevel data (i.e., statistical dependence of data due to “nesting” within shared environments), the possibility of the need to employ multilevel CFA that accounts for this nesting was tested using methods described by Muthén (1994) and with region (Northeast, Midwest, South, West), state, agency setting (urban, suburban, rural, frontier), and agency type (city, county, state, federal) as clustering variables. Due to the anonymous nature of the survey, we were unable to test for nesting by specific agency. Results of this testing indicated that multilevel CFA was not necessary in the current study (i.e., intraclass correlation coefficients were all less than .10; Dedrick & Greenbaum, 2011).
Maximum likelihood with robust standard errors and Geomin, an oblique rotation method, was employed to allow correlation among factors (Fabrigar, Wegener, MacCallum, & Strahan, 1999; Muthén, 2017). To determine the number of factors, the criterion of an eigenvalue greater than one (Kaiser, 1960) was used along with examination of the scree plot (Cattell, 1966). To examine the goodness of model fit, a number of model fit statistics with identified criteria were employed: chi-square statistic (p > .05), comparative fit index (CFI; ≥.90), Tucker–Lewis index (TLI; ≥.90), and standardized root mean square residual (SRMR; ≤.08; Hu & Bentler, 1999; Kenny, Kaniskan, & McCoach, 2015).
Results
Item Characteristics and Internal Consistency
Descriptive and internal consistency statistics of the CCSDM are presented in Table 2. With some variation, results indicated substantial support for SDM. Means of each of the items ranged from 2.96 to 3.84 and the percentage strongly agreeing with an item ranged from 21% (Item 3) to 85% (Item 4). The average of the total scale items was 24.56 with a standard deviation of 2.86. The item-scale correlations were examined using Cronbach’s alpha. The overall coefficient alpha for the CCSDM with seven items was .83 and the values for item-remainder coefficient also indicate the CCSDM had a good reliability and correlations. Cronbach’s alpha coefficients when an item was removed indicate that all items were equally important and necessary for the scale.
Item Characteristics (n = 291)
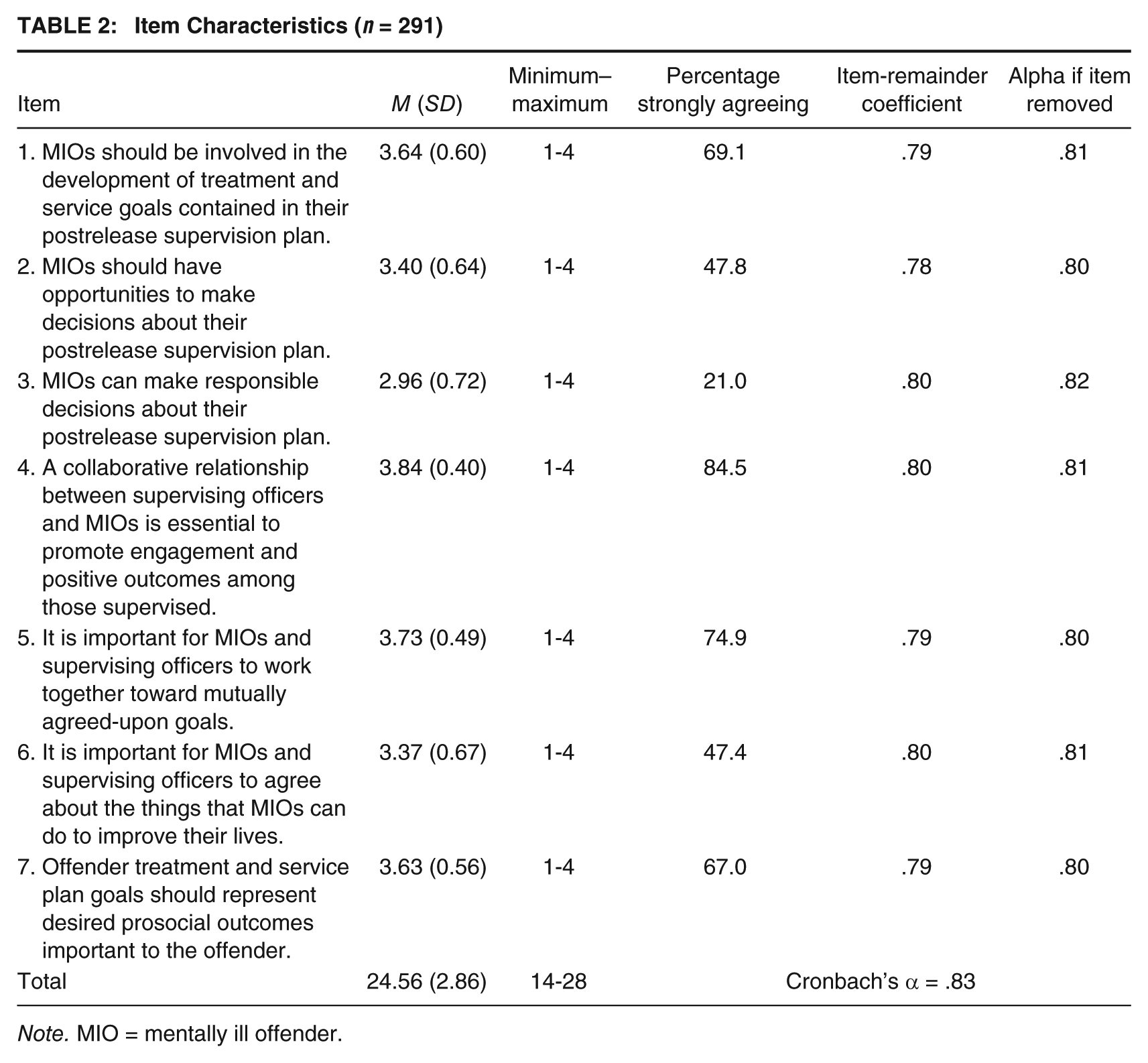
Note. MIO = mentally ill offender.
EFA
Table 3 presents the results of EFA. Based on the criterion of an eigenvalue greater than one (Kaiser, 1960) and the evaluation of a scree plot (not pictured), two factors were identified. In terms of factor loadings, three items had loadings from .490 to .922 with Factor 1, and four items had loadings from .461 to .849 with Factor 2. The first factor had a higher eigenvalue of 3.567 and the second factor had an eigenvalue of 1.057. The two factors that emerged reflect the research indicating that attitudes regarding the capacity of individuals with SMI to contribute to service planning (termed the capacity factor of the CCSDM) as well as the beliefs in the value of developing a working alliance with offenders (termed the alliance factor of the CCSDM) play distinct roles in supporting SDM with supervisees who have SMI.
Results of Exploratory Factor Analysis (n = 146)

As Brown (2006) suggests, the present study used multiple goodness of model fit statistics for more reliable evaluation. Using the criteria stated above, the goodness of EFA model fit statistics indicate that the two-factor structure model fits the data well: χ2 = 10.50 (p = .232), CFI = .991, TLI = .976, and SRMR = .022.
CFA
To validate the two-factor structure from the EFA, a CFA was also conducted. The results of CFA indicate that the two-factor structure was acceptable based on the following goodness of model fit statistics: χ2 = 25.23 (p = .022), CFI = .939, TLI = .902, and SRMR = .053. Although the EFA displayed a slightly more desirable fit profile than the CFA, the results of both the EFA and CFA support a reliable two-factor structure.
Discussion
Results indicate the CCSDM functions as an internally consistent, two-factor scale for measuring attitudes toward SDM with formerly incarcerated persons who have a mental illness and who live under correctional supervision in the community. Given the 4.5 million people on probation or parole (Kaeble & Glaze, 2016), a rate of SMI of approximately 15% (Lurigio, 2001; Skeem et al., 2006; Skeem & Louden, 2006; Veysey & Bichler-Robertson, 2002), and the expanding use of recovery-oriented approaches to assist this population’s involvement in needed supportive services (e.g., Taxman, 2013; Tibaldi et al., 2011), the potential for employing this scale in efforts toward officer recruitment and training and in postincarceration, community supervision research, and practice evaluation is substantial.
Respondents expressed considerable support for employing SDM with supervisees who have an SMI. Yet, the variance in observed scores indicates that effort will be required to increase attitudes that are supportive of SDM for extensive use of this practice to be realized in community corrections settings. Findings from the two factors identified in this study can inform these efforts.
Together, the two factors identified in the EFA, and supported with the CFA, establish important prerequisites for developing and implementing an SDM protocol in community supervision agencies. The capacity factor (i.e., Factor 1 of the CCSDM) reflects officers’ attitudes about the capacity of individuals with SMI to engage in SDM. Extensive evidence exists about the power of stigma to undermine beliefs in the ability of persons with SMI to contribute valued perspectives to their care plans and to exercise responsible decision making (Schulze, 2007; Wahl, 1999). Stigma and its effects are accentuated in work with the formerly incarcerated and SMI population who until recent years were largely regarded as failures found in the revolving door that too often stops only for a term of imprisonment.
An absence of confidence that supervisees with SMI are capable of making meaningful contributions to the development of postrelease supervision plans is likely to preclude the use of SDM among supervising officers. Consequently, engagement of officers in the movement from disbelief-to-faith in successful reintegration planning with persons with SMI should start early in the hiring process, when viable candidates for parole positions are identified. Hiring the right people and providing targeted training about working with supervisees with mental illnesses may be supported by the use of the CCSDM as both a preemployment screening device and a postemployment training tool. Where the probation/parole agency seeks to support a paradigm shift from a practice of imposing demands, toward one of embracing an SDM process, the CCSDM might be used as support for developing new training and supervision protocols. Furthermore, among existing supervising staff, an informed movement toward using SDM might consider use of the CCSDM to gauge staff attitudes about persons with SMI, which in turn reflect staff readiness to embrace the new paradigm. Coaching in the methods of achieving SDM, employment of peer supports for persons with SMI, and frequent opportunities for supervising officers to share successes and challenges may serve to reduce the social distance among those with and without SMI and improve perceptions about what is possible for persons with SMI.
Given the relevance of SDM to working alliance (see introductory literature review), the alliance factor of the CCSDM (i.e., factor 2) can be construed to assess beliefs in the importance of establishing a working alliance that supports SDM among supervisors and supervisees. The origins of those beliefs are certainly found in the culture of the parole and probation agency. Items on this factor stress the importance of a collaborative relationship and reflect attitudes that support achieving goal and task agreement, components posited to support therapeutic alliances (Horvath & Greenberg, 1989). In agencies, these are rooted in management philosophies and the operational guidelines that spring from these philosophies.
If administrators planning to employ SDM in their agency find there is little value of collaborative decision making among officers, the first step is to look inward. The CCSDM may help bring to the fore the unconscious bias at play when considering the following very basic question: Can persons with SMI meaningfully contribute to the making of decisions about how they will live their daily lives? That question can be answered with science, but the discovery of bias starts with self-reflection, assisted and otherwise. Once SDM is even tentatively embraced, there are tools available to assist service consumers to identify goals of their mental health treatment and to use this information as the basis for collaborative discussions with providers (Deegan, 2010; Deegan et al., 2017). These tools can be easily used in community corrections settings to bring supervising officers fully into conversation with supervisees and their treatment providers. In the community corrections context, the therapeutic or working alliance is both sought and furthered by the use of “structuring skills” (Raynor, Ugwudike, & Vanstone, 2014, p. 239; see also Cullen, Jonson, & Mears, 2017), which include the use of motivational interviewing and problem-solving techniques to encourage the supervisee’s continual examination of his thinking and behavior in the movement toward change.
The psychometric evaluation of the CCSDM reported here indicates it may be a useful tool in facilitating the processes discussed above. However, it is important to point out some methodological limitations of the current study prior to considering its use. Although study respondents represented an array of geographic territories, agency, and community settings, as well as the most common community supervision populations (i.e., those on parole and probation), the absence of a probabilistic sampling method (e.g., a random sample) limits comprehensive generalizations of findings to community corrections officers in the United States. As with any initial instrument development, further research is necessary to determine whether the factor structure can be maintained in differing environments.
Another limitation could be the sample size for the current study. Using a Monte Carlo simulation, MacCallum, Widaman, Zhang, and Hong (1999) demonstrated that a level of communality plays a critical role in determination of an adequate sample size for factor analysis. Based on their recommendation, our study sample has a wide communality level with a 7:2 ratio of variables to factors, which indicates our sample size is admissible in factor analysis. To improve statistical power, a larger sample size is recommended in future research. In addition, the anonymous nature of the survey data precluded testing as to whether data were nested by specific agency; however, results of testing clustering more broadly, by region, state, and agency type and setting were negative. Finally, the CCSDM is a measure of attitudes, not behaviors. Although actual SDM behaviors are not measured, attitudes toward these behaviors are important determinants of the degree to which such behaviors are and can be carried out to good end. Relatedly, advancing SDM within this context cannot be accomplished by changing attitudes alone. Research in this area is underdeveloped, necessitating further examination of the personal, interpersonal, and structural facilitators and limiters of SDM as well as continued testing of its potential benefits.
Conclusion
Cullen and colleagues (2017) assert that “[t]he future of effective community supervision does not lie in deterrence-oriented systems devoted to graduated sanctions but in therapeutic-oriented systems devoted to human change” (p. 62). Having an SMI does not mean that the person is incapable of contributing to their reintegration plan in meaningful ways. In using SDM, for many, the identification and articulation of goals for successful life in the community may well mirror the process of persons who do not have an SMI, though for some, it may take a more idiosyncratic and dynamic path. The process itself is shaped by a belief in the power of shared goals and in the collaboration important to reaching them. Stigma about mental illness may influence the process by substituting what is essentially a paternalistic relationship for one of recognizing the capacity of supervisees with SMI to know something about what will help them succeed.
We propose that, with replication of the research presented here, the CCSDM may help move parole and probation supervisors and their supervisees to a new level of shared responsibility for successful community reintegration. Ninety-six percent of persons currently incarcerated will return to a community at release (Hughes & Wilson, 2004). It is fair to estimate that more than 15% of these returnees will have an SMI that will be a contributor to their return to incarceration for violations of an agreement that traditionally has not been a shared one. Introducing the ideas of SDM, embracing the capabilities of persons with SMI, and striving for buy-in of the new paradigm of supervision with them must be supported by science. In its ability to identify bias and so begin to defeat it, the validation of the CCSDM is a significant first step toward altering the course of community supervision for formerly incarcerated persons with mental illness.
Footnotes
This study was developed through support from the University of Kansas New Faculty General Research Fund and the assistance of the American Probation and Parole Association.