
Abstract
We examined the predictive validity of individual, service, and neighborhood factors for aggression by 1,491 forensic clients found Not Criminally Responsible on account of Mental Disorder (NCRMD), under the jurisdiction of a Review Board, and thus subject to supervision conditions. Younger patient age and personality disorder diagnosis were associated with both clinically documented aggression and recidivism. Medication adherence was related to clinically documented aggression, but not criminal recidivism. Number of reports from an institution (possibly reflecting assessor or institutional experience with NCRMD assessments) did not predict clinically documented aggression, but more comprehensive risk reports were associated with fewer such clinical incidents. More community mental health resources within a 45-min drive of an individual’s residence were associated with less recidivism, but not less clinically documented aggression. We conclude that extra-individual factors are related to aggression, the neighborhood to which forensic clients return matters, and effects can differ for criminal recidivism versus clinically documented aggression.
Keywords
In Canada, persons who commit crimes, but who either did not know that what they were doing was wrong, or were not able to control themselves as a result of mental disorder, can mount a defense of Not Criminally Responsible on account of Mental Disorder (NCRMD; Criminal Code, 1985). The NCRMD defense is similar in common law origin and rationale as the Not Guilty by Reason of Insanity defense in the United States (R. v. Swain, 1991; Verdun-Jones, 1994; Winko v. British Columbia, 1999). In our earlier research on 1,800 persons found NCRMD in the National Trajectory Project, from which this study is drawn, we found the following characteristics (Crocker et al., 2015a, 2015b): 84% of the sample was male, the average age was 36, 84% of the sample was single, and 84% were not employed. The most common primary diagnosis was a psychotic spectrum disorder such as schizophrenia, followed by substance use disorder (31%), mood disorder (23%), or personality disorder (11%). Two thirds of the persons had been found NCRMD for an offense against a person, the most common being assault (26%).
Once found NCRMD, these individuals come under the jurisdiction of a Review Board, which are tribunals responsible for making decisions about the disposition of persons found NCRMD, ranging from detention in hospital to community release under specified conditions (conditional discharge), or under no further legal restrictions (absolute discharge). Conditions might include curfews, travel restrictions, requirements to abstain from alcohol, and whatever else the Review Board considers necessary to find the right balance between public safety and personal liberty. Decisions about disposition and conditions are made at Review Board hearings that are legally required to occur at least annually, except under exceptional circumstances. In a 3-year follow-up of the 1,800 men and women in the National Trajectory Project sample, Charette et al. (2015) found that recidivism was relatively low at 17% for any kind of new offense, with a lower rate of recidivism while individuals were under the supervision of a Review Board (detained at a hospital or living in the community under specified conditions). Consistent with the research summarized by Bonta, Blais, and Wilson (2014), Charette et al. (2015) found that prior criminal history, substance use disorder diagnosis, and personality disorder diagnosis were all positively associated with the likelihood of committing a new offense. Contrary to popular belief, but consistent with other research, the severity of the offense(s) resulting in the NCRMD verdict was inversely related to recidivism, such that those who committed more serious index offenses were less likely to reoffend (Bonta et al., 2014; Harris, Rice, Quinsey, & Cormier, 2015).
Consistent with the idea that supervision in the community can be beneficial, Salem, Crocker, Charette, Seto, and Coté (2015) found that rehospitalization or recidivism rates were lower when individuals were discharged into supportive housing, as opposed to living on their own or with family or friends, even after controlling for individual factors such as age, gender, and psychiatric and criminal history. Those who were placed in independent housing were 1.4 times as likely as patients in supportive housing to be readmitted to hospital and 2.5 times as likely to reoffend in some way.
Individual Risk Factors
Many risk factors for recidivism identified for individuals with mental disorders in conflict with the law are shared with offending individuals who do not have such disorders, for example, age, gender, criminal history, and antisocial personality (Bonta et al., 2014). There are also some unique factors such as psychiatric diagnosis that can predict future violence among persons with mental disorders (e.g., Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Strub, Douglas, & Nicholls, 2014). Drawing from this research, there has been substantial progress in the prediction of reoffending by persons with mental disorders, including the validation of risk assessment tools such as the Historical Clinical Risk Management-20 (HCR-20) and Violence Risk Appraisal Guide (Douglas et al., 2014; Fazel, Singh, Doll, & Grann, 2012). These risk assessment tools are increasingly used and are recommended in forensic psychology and psychiatry practice guidelines (American Psychological Association, 2013; Fazel et al., 2012; Glancy et al., 2015). The work has mostly focused on individual-level variables, partly because studies have relied on clinical files that typically emphasize patient characteristics. There is emerging evidence, however, that considers the influence of extra-individual factors such as social context and neighborhood, in line with Bronfenbrenner’s (1977) ecological framework.
Theoretical Lens
The Bronfenbrenner (1977) framework suggests individuals are influenced by, and act upon, the environment within concentric systems, beginning with those they have direct contact with, such as family or friends, to larger social groups, and then to the social contexts of neighborhood and then society. This perspective has been supported by research demonstrating the importance of neighborhood (e.g., Silver, Mulvey, & Monahan, 1999), housing (e.g., Salem et al., 2015), and other environmental factors (Heilbrun, 2009) on outcomes for individuals with mental disorders who leave institutions to return to the community. There is also a growing literature on environmental criminology that describes how places can affect crime (Melnychuk, Verdun-Jones, & Brink, 2009; Vaughan, Hewitt, Andresen, & Brantingham, 2015; White & Weisburd, 2017). For example, Melnychuk et al. (2009) followed forensic clients who had left hospital, and found that those who moved to neighborhoods characterized by lower income, higher unemployment, poor educational achievement, and concentrated rental properties were more likely to return to inpatient care.
It may be harder to assess extra-individual factors in clinical settings, and such factors may be more likely to change over time, or might change more quickly, as contrasted to the more stable or static prediction provided by individual history. Moreover, there may be more opportunity for external influence and control over extra-individual risk factors. As such, there is a need for research on extra-individual factors. Hiday (1995) argued for the importance of social context, such that both individual (e.g., antisocial personality) and extra-individual (e.g., social disorganization) factors are involved.
Social Context
Studies have shown that variables beyond the person, including peers, social supports, and residential neighborhoods, are also relevant to the likelihood of successful community transitions among individuals who have been in custody (Silver, 2000; Stahler, Mennis, Belenko, Welsh, & Hiller, 2013; Swanson et al., 2002; Wang, Hay, Todak, & Bales, 2014). Stahler et al. (2013) demonstrated that moving back to a neighborhood with high levels of recidivism by other ex-prisoners was related to recidivism in a sample of more than 5,000 offenders released from a Pennsylvania state prison, consistent with a social contagion effect. In contrast, neighborhood variables reflecting social resources—for example, the percentage of the population who received public income assistance, percentage of high school graduates, percentage who were renting—were unrelated to recidivism. Wang et al. (2014) also found evidence for a social contagion effect regarding the impact of recidivism in adjacent counties as well as evidence that social context factors such as residential mobility, racial inequality, and racial heterogeneity predicted recidivism. Swanson et al. (2002) reported that witnessing violence had an effect on the violent behavior of adults with psychotic or mood disorders who were seen in inpatient or outpatient services; other predictors included the individual factors of violent victimization history and substance use. Together, these results suggest that models of recidivism that include both individual and extra-individual factors have added value. Furthermore, distinguishing between factors that are static or cannot change over time from those that are dynamic and that—at least in principle—change as a result of time or intervention might also enhance predictive validity.
Dynamic Individual and Extra-Individual Risk
More attention has been paid to static risk factors than dynamic risk factors, with one-time assessment or data collection and then follow-up over time to look at associations with outcomes such as rehospitalization or recidivism rates. Thus, we know more about static individual factors that cannot change—such as psychiatric diagnosis or criminal history—than dynamic risk factors that can change over time and need to be repeatedly assessed in the prediction of rehospitalization or recidivism (Douglas & Skeem, 2005). However, there are an increasing number of studies that show the relevance of dynamic individual factors. For example, Quinsey, Coleman, Jones, and Altrows (1997) found that antisocial attitudes, dysphoric mood, psychiatric symptoms, and noncompliance with rules distinguished forensic clients who eloped or reoffended from those who did not. Reflecting the potential value of dynamic risk assessment for targeting treatment and supervision, a number of forensic risk tools focus more on dynamic risk factors, including the Short-Term Assessment of Risk and Treatability (START; Webster, Martin, Brink, Nicholls, & Desmarais, 2009) and Structured Assessment of Protective Factors for Violence Risk (SAPROF; de Vries Robbé, de Vogel, & de Spa, 2011). Desmarais, Nicholls, Wilson, and Brink (2012) demonstrated the incremental value of dynamic variables over static variables in a forensic psychiatric sample. McDermott, Edens, Quanbeck, Busse, and Scott (2008) also found that the clinical and risk management items on the HCR-20, which can change over time, were helpful in predicting institutional aggression in a forensic sample.
Less is known about dynamic extra-individual factors. For example, individuals may move multiple times once they return to the community, and changes in neighborhood characteristics may have an important impact on their outcomes (Steiner, Makarios, & Travis, 2015). In other words, social context can matter, and so can changes in social context.
Present Study
We examined the contributions of individual, service, and neighborhood factors to the prediction of criminal recidivism and clinically documented aggression among persons found NCRMD. Replicating previous work reviewed by Bonta et al. (2014), we expected individual static (or highly stable) factors such as age, criminal history, and personality disorder would be related to both criminal recidivism and clinically documented aggression that could have resulted in criminal charges (Charette et al., 2015; Harris et al., 2015). Extending this work, we further predicted that dynamic individual factors—substance use, medication nonadherence, and active psychiatric symptoms (see Skeem & Mulvey, 2002; Skeem et al., 2006)—would also be associated with these outcomes. Last, given our interest in social context, we examined extra-individual service and neighborhood factors: We predicted that hospitals with more experience with persons found NCRMD (as indicated by number of reports completed) or that produced more detailed evaluation reports (as indicated by number of risk items mentioned) would be associated with better outcomes. We also predicted that moving into supportive housing and moving into a residence with greater proximity to community mental health resources would be associated with better outcomes, consistent with Melnychuk et al. (2009) and Salem et al. (2015).
Method
Sample
We followed 1,491 individuals found NCRMD between May 1, 2000, and April 30, 2005, until 2008. As mentioned, these data were drawn from the National Trajectory Project (NTP), a file-based study of a cohort of 1,800 individuals found NCRMD in the provinces of Quebec, Ontario, and British Columbia (Charette et al., 2015; Crocker et al., 2015a, 2015b; see http://ntp-ptn.org for additional studies and other resources). From the initial NTP sample, 309 individuals (17%) were excluded from this study because they received an absolute discharge at the first hearing, and thus had no dynamic information available.
The sample selection is described in more detail in Crocker et al. (2015b). Owing to time and budgetary constraints, time frames varied slightly across provinces. Quebec had a much higher number of NCR verdicts than Ontario or British Columbia, even after controlling for number of court decisions. Quebec cases were, therefore, randomly sampled to generate a geographically representative sample across justice administration regions, whereas all eligible NCRMD cases in Ontario and Quebec were included. As the population was sampled differently across different regions, the analyses were weighted accordingly. This research was approved by our institutional research ethics boards.
Study Variables
Data were coded from Review Board files, which contained information about sociodemographic characteristics (e.g., age at verdict, gender, marital status), clinical history (e.g., age at first psychiatric hospitalization, psychiatric diagnoses at time of verdict), criminal history, the index NCRMD verdict, the initial and subsequent dispositions under the Review Board, and information from each Review Board hearing regarding treatment participation and behavior since the last hearing.
As noted, many of these variables are commonly examined in predictive studies involving forensic or correctional samples (e.g., age, gender, criminal history), including our previous research examining the trajectories and outcomes of persons found NCRMD. We included this set of established individual risk factors to set a “baseline” to examine the contributions of potential hospital-level and neighborhood-level predictors. Where the individual resided from hearing to hearing was also available, but only for those still under the jurisdiction of the Review Board (i.e., before absolute discharge). As commonly observed in retrospective studies of this kind, file data quality and quantity varied both within and across provinces, and over time as well.
Figure 1 describes the timeline of data collection and how data were analyzed. There were 5,600 observation periods (M = 3.8, SD = 2.5 per individual), with an average follow-up time of 963.2 days (SD = 797.0, Mdn = 783, range = 1-3,041 days). This follow-up time is shorter than in the original National Trajectory Project follow-up reported by Charette et al. (2015) because we only examined outcomes while individuals were under the jurisdiction of a Review Board; we were particularly interested in dynamic factors in this study, and these data were only available until someone received an absolute discharge.

Temporal Structure of the Analysis
Extensive training and coding checks resulted in very good interrater reliability. For example, interrater reliability for the coding of the presence or absence of HCR-20 items (based on 1,835 reports associated with 573 individuals found NCR) was .78, which according to the thresholds proposed by Cicchetti et al. (2006), demonstrates excellent agreement.
Variables used in this study are described next, along with descriptive information. We chose variables based on whether they fit our conceptualization of static versus dynamic, and individual versus service or neighborhood factors.
Static Individual Characteristics
Table 1 summarizes our study variables, including participant characteristics. Participants were, on average, 36 years old at the time of the NCRMD finding (SD = 12.5), and mostly male (84.5%). Over the study period, the majority was diagnosed with a psychotic spectrum disorder (67.9%) and about half were diagnosed with a substance use disorder (51.5%) or personality disorder (45.4%). These psychiatric diagnoses were not mutually exclusive.
Description of the Study Sample

Note. NCRMD = Not Criminally Responsible on account of Mental Disorder; HCR-20 = Historical Clinical Risk Management-20.
The sample had a median of one conviction prior to their index NCRMD verdict. Index offenses were categorized using the Uniform Crime Reporting. The severity of index offenses descriptions of the offenses were coded using the Uniform Crime Reporting manual, with severity scored using the Crime Severity Index, which is based on average sentence lengths (Canadian Centre for Justice Statistics Policing Services Program, 2008). These sociodemographic, clinical history, and criminal history variables formed our static individual factors.
Dynamic Individual Factors
We examined problems in the last year for this domain. Drawn from 5600 annual clinical reports submitted to the Review Board, we considered psychoactive substance use, medication nonadherence, and presence of active psychotic symptoms as potential dynamic risk factors (coded as present or not). These behaviors were present in 23.4%, 22.1%, and 45.7% of the observation periods, respectively.
Dynamic Extra-Individual Factors
Residential status
Across the 5,600 observation periods, the plurality of patients were in the hospital (42.5%); others lived alone (21.9%), in supportive housing (e.g., group home; 19.7%), or with a partner (4.1%), family member (9.7%), or a friend (2.0%). These residential statuses are mutually exclusive; if the patient was observed in more than one residential status during one period, the least restrictive was selected because it represented more opportunity to reoffend.
Service
Patients were supervised by 206 different hospitals or mental health services, with more than half of these services in Quebec (Quebec [QC]: n = 112; Ontario [ON]: n = 78; British Columbia [BC]: n = 16). These were the services with which patients were registered upon entering the Review Board system, where both assessment and treatment services were typically received. We considered the average number of HCR-20 risk items (Webster, Douglas, Eaves, & Hart, 1997) mentioned in clinical reports as an indicator of the comprehensiveness of the evaluation, where the mention of more of the 20 items (whether present or absent) suggested the report was more thorough. Our logic was that future readers of the report would not know if the absence of any mention of a risk item meant it was considered but deemed irrelevant for the individual being assessed, or was not considered at all. We chose the HCR-20 for this purpose because it is the mostly widely used risk assessment measure in forensic mental health practice and it has been extensively validated in Canada and elsewhere (Fazel et al., 2012; Otto & Douglas, 2011; Singh et al., 2014). Our interest was in whether the item was mentioned as present or absent, not whether it was accurately described or whether the individual had more risk items present. On average, across the 206 services, 8.5 (SD = 2.2) out of 20 HCR-20 items were mentioned.
Some hospitals might be more effective because they have more experience with persons found NCRMD and the Review Board system, or more suitable staff and/or facilities (e.g., security level, rehabilitation programming). The number of Review Board reports by each hospital was calculated for the entire study period; the 206 hospitals completed between 1 and 767 Review Board reports, with a median of 4.
Neighborhood
As suggested by Hewko, Smoyer-Tomic, and Hodgson (2002), we focused on number of community mental health services within an arbitrarily prespecified driving distance. We coded this factor using the postal code of the patient’s residence and online lists of mental health resources maintained by provincial ministries of health (BC: http://www.healthlinkbc.ca; ON: http://www.connexontario.ca; QC: http://www.msss.gouv.qc.ca). The actual path of travel was favored over Cartesian distance because it is a truer estimate of travel time, which is especially important when comparing regions with different population densities; for example, the distance that can be traveled in 10 min is much different in a busy city with its usual traffic compared with a small town or a rural area (Apparicio, Abdelmajid, Riva, & Shearmur, 2008).
Our participants resided in a total of 531 different neighborhoods (by postal code). We examined resources within a 15-, 30-, 45-, and 60-min drive from their residences: There were between 0 and 248 mental health resources within 15 min (M = 62.5, SD = 67.5), 0 and 322 within 30 min (M = 114.9, SD = 102.9), 0 and 345 within 45 min (M = 150.4, SD = 116.8), and 0 and 359 within 60 min (M = 182.9, SD = 128.8). Figure 2 shows the geographic distribution, by postal code, of residences and community mental health resources. Addresses were aggregated at the postal code level, using population-weighted centroids based on 2001 Canadian census dissemination blocks, which identify the central point of an area based on where most of the population lives. Using postal codes avoided any potential identification of participants by residential address, yet was specific enough to calculate travel distances.

Geographic Distributions of Mental Health Resources and Participants’ Residential Addresses (as Postal Code)
Study Outcomes
We coded data on the following outcomes: (a) any new criminal conviction or NCRMD verdict; (b) any new criminal conviction or NCRMD verdict for an offense against a person, which included threats or assaults against a person; and (c) clinical reports of aggression (e.g., the individual threatened or assaulted another client or a staff member). Information about new convictions or NCRMD verdicts was obtained from national criminal records and review board files. Information about clinical reports of aggression was obtained from hospital reports submitted to the review boards in anticipation of annual hearings. Many of these clinically documented incidents (69%) were not reported to police and, therefore, did not result in new criminal charges or convictions, even though they could affect the victim, workplace safety, the therapeutic milieu, and the public (e.g., some aggression might be directed at family members or others in the community). For this reason, the developers of the Violence Risk Appraisal Guide included both criminal charges as well as institutional reports of violence that could have resulted in criminal charges in their analyses of violence outcomes (Harris et al., 2015). In the present study, individuals could have been convicted more than once and could have multiple incidents of clinically documented aggression.
About 14% of our sample was convicted of a new offense at least once during the follow-up period. A total of 269 convictions were reported; the majority (61%, 164 convictions) were against persons, ranging from uttering threats (n = 46, 17%) to homicide (n = 3, 1%). A total of 837 incidents against others were clinically documented, involving 29% (n = 437) of the sample; as noted, only 31% of these incidents resulted in criminal convictions.
Data Analysis
As we only had information for the independent dynamic variables from each Review Board hearing, we considered time as a discrete variable while under the purview of the Review Board (i.e., while the individual was detained in hospital or conditionally discharged). We used a discrete time event history analysis, which can be interpreted as a logistic regression at the hearing level, with random effects on the intercept at the individual level and on the slope of time at the individual level (Steele, 2008). Observation periods were nested in individuals, individuals were nested in hospitals, and hospitals were nested in neighborhoods. A general linear model with crossed random effects was appropriate for this complex data structure. This technique accounts for right censoring (individuals were not observed for the same amount of time), nonindependence of some observations (individuals, services, and neighborhoods were observed more than once), and nonhierarchical dependencies (e.g., individuals could be treated at more than one hospital during the observation period). Three variables (age, severity of index offense, number of prior convictions) were log transformed because they were highly skewed; their coefficients should be interpreted accordingly. All variables were standardized using z scoring to facilitate the comparison between coefficients (β). Significance of the random effects was estimated by comparing model fits with null models without each specific random effect. The regression models were run with R 3.3.2 and the nlme4 package; geographic analyses were run with ArcMap 10.2.2 (Bates, Maechler, Bolker, & Walker, 2015; Environmental Systems Research Institute, 2013; R Core Team, 2015).
Results
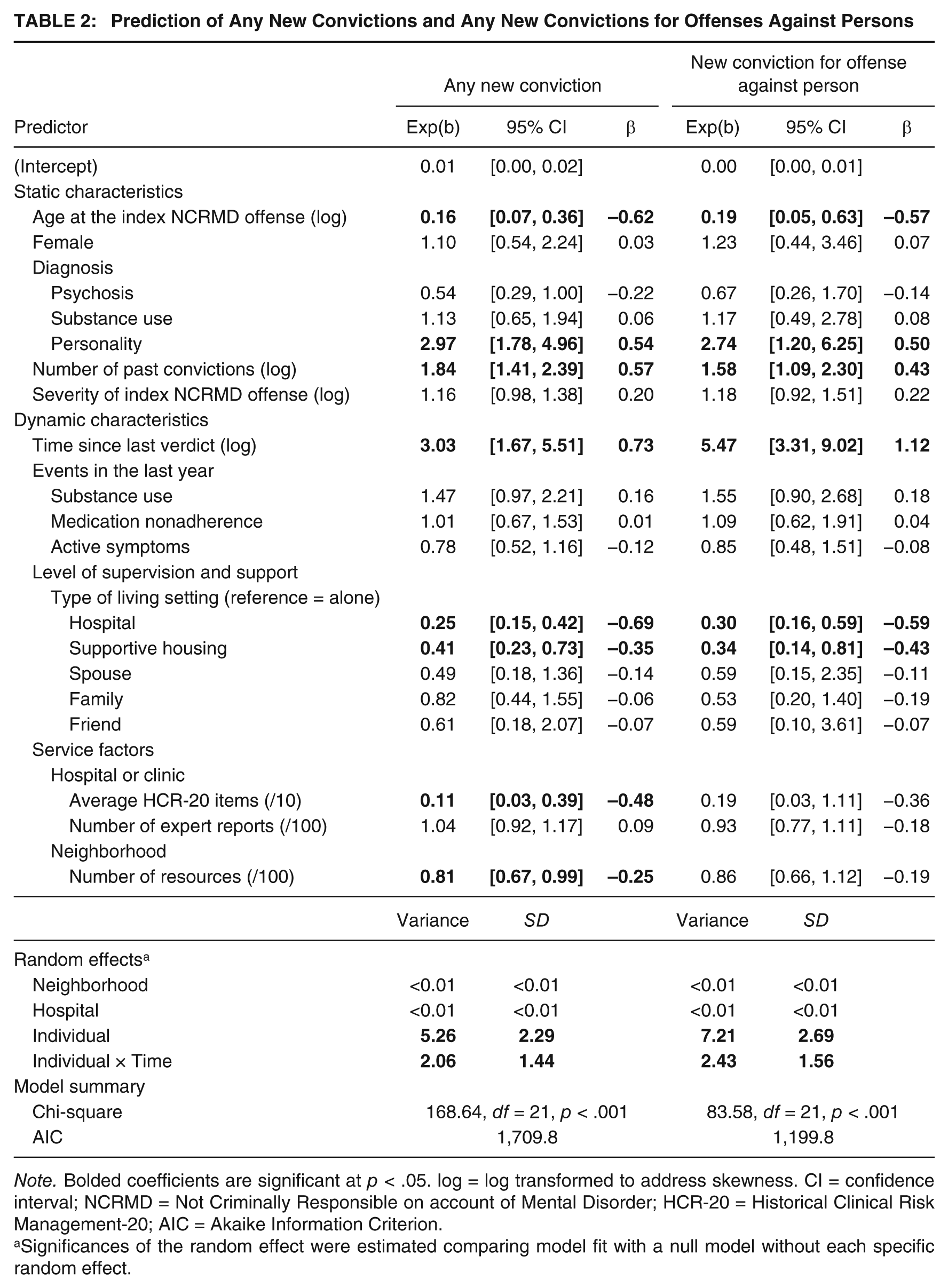
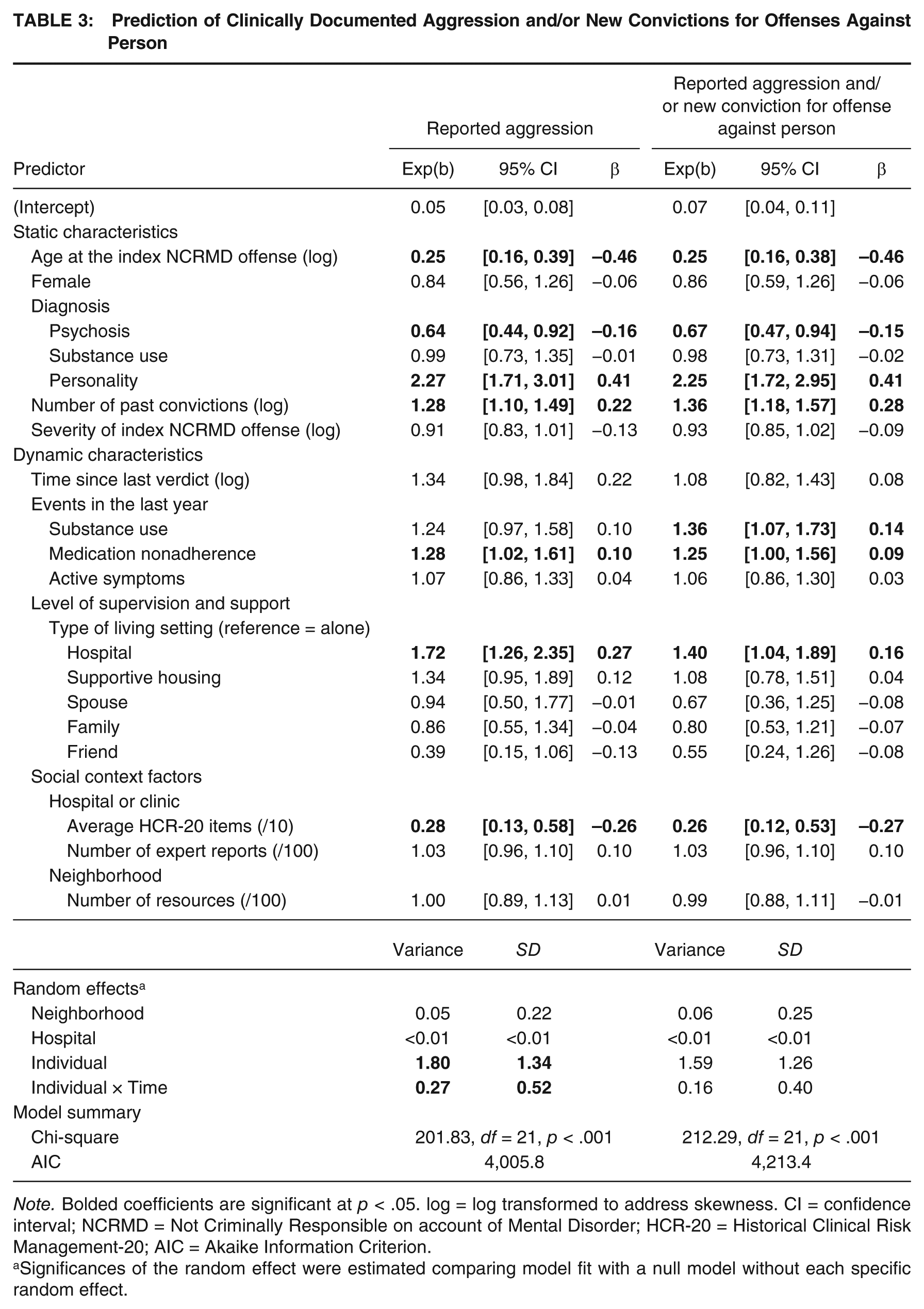
Tables 2 and 3 present the results of the discrete time event history analysis for the different outcomes, namely, any criminal conviction, criminal conviction for offenses against the person, clinically documented aggression against others (which often did not result in new criminal charges), and the combination of these two latter outcomes. A positive standardized coefficient β means an increase and a negative coefficient means a decrease in risk of recidivism. The nonstandardized coefficient, Exp(b), can be interpreted as an odds ratio.
Prediction of Any New Convictions and Any New Convictions for Offenses Against Persons
Note. Bolded coefficients are significant at p < .05. log = log transformed to address skewness. CI = confidence interval; NCRMD = Not Criminally Responsible on account of Mental Disorder; HCR-20 = Historical Clinical Risk Management-20; AIC = Akaike Information Criterion.
Significances of the random effect were estimated comparing model fit with a null model without each specific random effect.
Prediction of Clinically Documented Aggression and/or New Convictions for Offenses Against Person
Note. Bolded coefficients are significant at p < .05. log = log transformed to address skewness. CI = confidence interval; NCRMD = Not Criminally Responsible on account of Mental Disorder; HCR-20 = Historical Clinical Risk Management-20; AIC = Akaike Information Criterion.
Significances of the random effect were estimated comparing model fit with a null model without each specific random effect.
Individual Characteristics
Age was one of the most robust predictors for all outcomes (β = −0.62, –0.46). As expected, older NCRMD patients were less likely to reoffend. Gender and whether a patient was diagnosed with a substance use disorder were unrelated to reoffending. Patients diagnosed with a personality disorder were approximately 2 to 3 times more likely to engage in clinically documented aggression than patients without that diagnosis. Those with more extensive criminal histories were more likely to reoffend. Patients diagnosed with a psychotic spectrum disorder had 1.56 times fewer clinically documented incidents of aggression than patients who did not have this diagnosis (e.g., those who had mood or anxiety disorder diagnoses).
Dynamic Factors
Events in the Last Year
Although substance use, medication nonadherence, and active symptoms were unrelated to new convictions, medication nonadherence was associated with 1.28 times the likelihood of clinically documented aggression, and substance use increased by 1.36 times the rate of aggression when combining criminal conviction for offenses against persons and clinically documented incidents.
Service Factors
Level of Supervision
Being detained in hospital, in comparison to living alone, decreased the likelihood of new conviction by a factor of 4 for any convictions and a factor of 3.33 for convictions against persons, but increased by a factor of 1.72 the likelihood of clinically documented aggression. Living in supportive housing also reduced the likelihood of any new conviction by 2.44 and conviction for crimes against persons by 2.94, in comparison to living alone.
Hospital
Although the number of Review Board reports completed by an institution did not predict the likelihood of the composite aggression outcome, an increase of 10 items of the average comprehensiveness of these reports at the hospital level (i.e., number of HCR-20 items mentioned) decreased by 9.09 times the likelihood of any new conviction and by 3.57 times the likelihood of clinically documented aggression.
Neighborhood
The number of mental health resources near patients’ residences was negatively associated with the likelihood of any recidivism only. Compared with other travel distances we examined, the effect was strongest (though still modest) at the 45-min travel distance mark; an increase of 100 resources in this radius decreased by 1.23 times the likelihood of having a new conviction.
Gender Comparison
As there is evidence that trajectories and outcomes can differ for men and women found NCRMD (Nicholls, Crocker, Seto, Wilson, & Côté, 2015), and there has been debate about the extent to which risk variables are common or unique for males and females (e.g., de Vogel, de Vries Robbé, van Kalmthout, & Place, 2012), models were run independently for men (n = 1260) and women (n = 231). When comparing nonoverlapping confidence intervals from the model coefficients, only one major difference was observed: The likelihood of clinically documented aggression was higher for women than for men living with a friend. Results of this comparison are available in the Supplemental Material, available with the online version of this article.
Discussion
This study is novel with respect to sample size, the number of observations, the distinction between criminal recidivism and clinically documented incidents of aggression, and the use of geographic analysis to take neighborhood factors into account. Replicating and extending prior research (Hiday, 1995; Silver, 2000), our results revealed that static individual, dynamic individual (Wilson, Desmarais, Nicholls, & Hart, 2013) as well as dynamic extra-individual factors were associated with official recidivism and/or clinically documented aggression among a large sample of persons found NCRMD.
Individual Factors
Some of our results were consistent with prior findings, including past work using the same National Trajectory Project sample. For instance, younger age, having a personality disorder diagnosis, and number of prior convictions were associated with a greater risk of recidivism (Bonta et al., 2014; Charette et al., 2015), whereas gender (Nicholls et al., 2015) and severity of the index offense (Bonta et al., 2014; Charette et al., 2015) were not. These findings are also generally consistent with the Risk-Need-Responsivity framework for correctional rehabilitation (Andrews & Bonta, 2010). Younger age and prior criminal history are robust predictors of criminal behavior, including aggression (e.g., Sweeten, Piquero, & Steinberg, 2013). There is a marked gender difference in violence, but past research suggests this difference is smaller among individuals with serious mental illness or with intellectual disabilities (e.g., Hodgins, 1992; Robbins, Monahan, & Silver, 2003; for a review see Nicholls, Cruise, Greig, & Hinz, 2015).
Many of these factors were also related to clinically documented aggression, in a similar manner: Being younger, having a personality disorder diagnosis, and having more prior convictions were associated with a greater likelihood of clinically documented aggression, and with the composite aggression outcome combining new convictions for offenses against persons and clinical reports. Individuals diagnosed with a psychotic disorder were significantly less likely than those without such a disorder to have clinically documented aggression, but did not differ in criminal recidivism. This result is consistent with research showing that a diagnosis of schizophrenia is associated with a lower likelihood of violence among individuals with mental disorders, compared with other psychiatric diagnoses, even though schizophrenia is associated with a small increase in risk of violence compared with the general population (Harris et al., 2015).
Dynamic Factors
Individual Factors
We advanced previous work on dynamic risk factors by looking at changes over multiple hearings, during an extensive observation period. Many past studies of putatively dynamic risk factors either have looked at putative factors assessed at one time only, making them static factors from a statistical point-of-view (Douglas & Skeem, 2005), or have assessed dynamic factors 2 or 3 times (e.g., Wilson et al., 2013). In this study, medication nonadherence was related to more clinically documented aggression, but not to criminal recidivism, whether for any new offenses or new offenses against the person. This might reflect a more direct effect of medication nonadherence on the clinical outcome, or it might reflect greater clinical team scrutiny, wherein patients who are monitored more closely will be known to be adhering to medication (or not) and will also be more likely to be reported if they are aggressive. Contrary to prior research by Bonta et al. (2014) and Skeem and Mulvey (2002), we found that a diagnosed substance use disorder was unrelated to reoffending. However, researchers have demonstrated that substance use disorders are drastically underdiagnosed in forensic patients (Ogloff, Lemphers, & Dwyer, 2004; Ogloff, Talevski, Lemphers, Wood, & Simmons, 2015). For example, Ogloff et al. (2004) found that only 8% of 130 Australian forensic patients had a diagnosis of substance use disorder on file, yet 75% met diagnostic criteria for lifetime substance use disorder based on a structured clinical interview. In sum, the findings suggest that it is likely to be important to assess and treat substance use disorders, but further research on underdiagnosis in forensic contexts and using measures of substance use that do not rely on diagnosis is required.
Service Factors
We also advanced previous research by considering dynamic service factors, namely forensic client residence and the risk assessment reports by the service to which the client was registered. Residence had different associations, with individuals living in hospitals or supportive housing being less likely to have any criminal recidivism, whereas those living in hospitals were more likely to have any clinically documented aggression. The most parsimonious explanation for the first association is that individuals who are already in a structured environment, especially as an inpatient, are more likely to be detected for aggression and simultaneously are less likely to be criminally charged because there are other options available, including a return to hospital or an increase in supervision. A parsimonious explanation for the second association is that clients living in hospitals are more closely monitored around the clock, so any aggression is more likely to be reported and recorded.
Individuals registered with services producing repots mentioning fewer risk items were more likely to have any criminal recidivism and to have clinically documented aggression. This is consistent with our opinion that the number of risk items mentioned in reports is an index of comprehensiveness of the clinical assessment, inasmuch as services that pay more attention to risk factors may be more effective at risk management, discharge planning, and other risk-related decisions, thereby reducing new convictions or clinically documented aggression.
Neighborhood Factors
A particularly interesting neighborhood factor was presence of community mental health resources within a 45-min drive, which predicted any criminal conviction but not clinically documented aggression. The first part of this finding relates to past work showing that neighborhood resources influence the likelihood of crime, and again supports the importance of adequate access to community resources in supporting recovery as inpatients return to the community (Hiday, 1995; Melnychuk et al., 2009). However, we cannot rule out alternative explanations, such as individual choice in where to live posthospitalization, or correlations between mental health resources and other neighborhood characteristics, such as average income, rental accommodation options, and social service availability. The second part may be related to the fact that much clinically documented aggression occurs within hospitals, and thus the presence of community mental health resources would be expected to have less of an effect on this outcome.
Strengths and Limitations
Strengths of this study include the large, multijurisdictional sample, follow-up period, and number of observations. We examined truly dynamic factors that could change from hearing to hearing, and we considered extra-individual service and neighborhood factors that are often unexamined in forensic follow-up studies. In addition, our random effects model could account for differences in opportunity to reoffend (e.g., detained in hospital for at least some of the follow-up period), differences in level of clinical observation (e.g., inpatient vs. living in supportive housing vs. living independently), and in number of observations (e.g., someone who was released, then rehospitalized would have more hearings, all other things being equal, than someone who had only annually scheduled hearings).
Given that we drew upon a cohort from the three largest provinces in Canada, we are confident the results are relevant to other persons found NCRMD. Given the similar common law origins of the NCRMD and Not Guilty by Reason of Insanity verdicts in Canada, the United States, the United Kingdom, and other Commonwealth countries, we anticipate that our findings regarding the outcomes of individuals with mental disorders under quasi-judicial review are relevant internationally, as well.
Limitations of the study include the reliance on coding data from archived documents. As already noted, file data quality and quantity varied over site and time, which is a common issue in retrospective file-based studies. Clinical teams and Review Boards might have considered other important factors, but if they were not recorded in files or coded for the NTP, they could not be included in this analysis. Also, not all client aggression was necessarily detected or recorded by clinicians; for example, clinicians might not record what they judged to be less serious aggression, such as shoving another patient.
Other limitations reflect how we operationalized some variables. We suggested that the number of HCR-20 items mentioned in the experts’ reports to the Review Boards is a credible indicator of risk assessment practices. Some might argue that this is a poor indicator of comprehensiveness because a thorough risk assessment or case formulation might mention only the most salient factors. In our view, mentioning factors that were absent is helpful for future report readers, who then do not have to wonder if the risk factor was considered but judged to be irrelevant, or was not considered at all and, therefore, not mentioned.
The number of community mental health resources within a set travel distance does not tell us anything about the quality of those resources, or actual access. Having many resources within a 45-min drive is not helpful if the person cannot afford public transit or taxis, or cannot drive, and having resources nearby is not helpful if the person is not interested in using the service, waiting lists are long, or the person is ineligible for the services. We recognize that 45 min is an arbitrary distance; we also examined resources within 15, 30, and 60 min.
Another limitation is that we had to combine data from all three provinces to have a sufficient sample size for our complex statistical analysis. However, prior research has shown there are provincial differences in patient characteristics and in trajectories and outcomes that could have affected the results of this study. For example, Charette et al. (2015) reported that Quebec had the shortest disposition times under Review Boards for persons found NCRMD, and the highest recidivism rates, suggesting that the criminal justice system is more likely to be involved in offending by persons with mental disorders in Quebec than in the other two provinces.
A final limitation is that we only had dynamic information about persons found NCRMD while they were under the jurisdiction of a Review Board; we did not have this information for anyone who had been absolutely discharged. We did not follow individuals after their absolute discharge, unlike our previous study of official recidivism, where we could look at criminal outcomes up to the end of our data collection (Charette et al., 2015).
Implications for Policy and Practice
Perhaps, the most important implication for forensic policy and practice is that considering extra-individual factors can be helpful in risk assessment and risk management. Consistent with results from others (Hiday, 1995; Melnychuk et al., 2009; Silver, 2000), and with the social-ecological model described by Bronfenbrenner (1977), risk assessment and management focused primarily or entirely on static and individual factors might benefit from considering dynamic and social factors as well. Our results suggest that these factors do have associations with outcomes, and understanding how and why these variables predict aggression could be helpful in guiding individual as well as social interventions. If mentioning HCR-20 items is indeed an indicator of risk assessment comprehensiveness—an assumption on our part—then more systematic training and quality improvement efforts might have an effect on violence risk management. Future risk assessment developments incorporating extra-individual factors might improve on the performance of existing risk measures that rely on individual factors.
As noted already by Salem et al. (2015) and others, where patients go after they are discharged from hospital is important. Thus, policies that affect the availability of affordable housing, professional supports, and access to high quality community mental health resources could have many benefits, including the reduction of rehospitalizations, general recidivism, and violence, all of which carry hefty individual, social, and economic costs. Our results—in addition to work by Melnychuk et al. (2009) and others—suggests that investments in housing and resources, including where housing and resources are located, could have big impacts on the outcomes of forensic clients as they return to the community.
Future Directions
An important future direction is prospective research following a cohort of persons found NCRMD as they leave hospital and return to the community, collecting data about their individual characteristics, dynamic changes over time on relevant factors, more services and neighborhood factors as well as potentially protective factors that mitigate risk to reoffend. Prospectively, collected data involving persons found NCRMD would address some of this study’s limitations, including information from self-report and observers, better operationalizations of the variables of interest, and multiple measures of service factors such as treatment involvement, availability, and quality as well as of multiple measures of neighborhood factors such as type of housing, actual involvement with community resources, income and employment, and local crime rates.
We focused on access to community mental health resources in this study, but neither resources nor persons found NCRMD are distributed randomly. Melnychuk et al. (2009) showed that persons found NCRMD were more likely move back to areas associated with social stresses, including lower average incomes and education, higher unemployment, and a higher ratio of rental properties, which suggests less residential stability and lower community cohesion. Relatedly, Vaughan et al. (2015) found that police calls for “emotionally disturbed persons” in a medium-sized Canadian city were disproportionately from a few locations, in close proximity to the city’s sole hospital, many public health units, addiction services, pharmacies, and walk-in clinics, and a majority of alcohol points-of-sale and criminal justice services. These police calls could include persons who have been found NCRMD in the past, who currently have an NCRMD status, or who may be found NCRMD in the future.
We did not have the data in this study to rule out alternative explanations for our results regarding neighborhood factors. For example, our result about access to community mental health resources may be less about those resources and more about where persons found NCRMD are likely to move postdischarge from hospital, which may be related in turn to proximity to things such as pharmacies, walk-in clinics, or alcohol points-of-sale. Moreover, selection of residence is rarely determined solely by the individual, as they may have to choose from a limited set of authorized housing or remain close to the hospital from which they were discharged to attend regular appointments.
It would also be very valuable to carry out similar research in other jurisdictions. Although NCRMD law has similar origins as other criminal responsibility defenses invoking serious mental illness, how the law is applied can vary across jurisdictions, and even within jurisdictions (Crocker et al., 2015a). Moreover, some of our findings might not hold in jurisdictions where most community mental health resources are not publicly funded, and thus access is constrained not only by travel time, but by cost.
Supplemental Material
CJB765047_Supplemental_Material – Supplemental material for Individual, Service, and Neighborhood Predictors of Aggression Among Persons With Mental Disorders
Supplemental material, CJB765047_Supplemental_Material for Individual, Service, and Neighborhood Predictors of Aggression Among Persons With Mental Disorders by Michael C. Seto, Yanick Charette, Tonia L. Nicholls and Anne G. Crocker in Criminal Justice and Behavior
Footnotes
Acknowledgements
Dr. Nicholls acknowledges the support of the Michael Smith Foundation for Health Research and the Canadian Institutes of Health Research (CIHR) for consecutive salary awards. Dr. Crocker received consecutive salary awards from CIHR, FRQ-S, and a William Dawson Scholar award from McGill University while conducting this research.
This research was previously presented at the 2014 meetings of the International Association of Forensic Mental Health Services and the American Psychology-Law Society.
This research was consecutively supported by grant 6356-2004 from Fonds de recherche Québec—Santé (FRQ-S) and by a grant from the Mental Health Commission of Canada. Dr. Charette acknowledges doctoral fellowship support from the Social Sciences and Humanities Research Council of Canada.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.