
Abstract
Mental illness and substance use disorder are prominent among jail and prison inmates. Developing more effective mental and behavioral health treatment approaches for incarcerated criminal offenders is a critical step toward reducing rates of recidivism and relapse following release. Specifying subgroups of offenders who differ in cognitive, affective, behavioral, and demographic characteristics could facilitate more targeted and effective treatment approaches. Accordingly, this study utilized model-based cluster analysis to identify subgroups of offenders in a large sample of incarcerated male offenders (n = 2,388) using broad personality traits. Six subgroups of offenders emerged based on personality scales related to positive affect, negative affect, and behavioral control. Subsequent analyses revealed significant differences between groups on measures of cognitive ability, affect dysregulation, antisociality, substance use, and impulsivity. These findings provide insight into potential treatment and intervention strategies to target the specific needs of distinct subgroups of incarcerated offenders.
More than 2 million individuals in the United States are incarcerated in jails and prisons and more than half of these incarcerated individuals have a history of mental health problems and/or substance use problems (D. James & Glaze, 2006; Mumola & Karberg, 2007; Teplin, 1994). Accordingly, enhancing mental health and substance abuse services is a major goal of the U.S. Department of Justice (2016). To develop more effective mental health and substance use treatment programs for criminal offenders, however, it is essential to gain a better understanding of factors contributing to mental health and substance use problems within this population.
One of the primary challenges in treating these issues is the substantial heterogeneity of underlying risk factors among offenders. Substance abuse and criminal behavior have been linked to a variety of interrelated psychological factors, including mental illness, impulsivity, negative affect, lack of empathy, and antisocial personality (Bock & Hosser, 2014; Hemphill, Hare, & Wong, 1998; Krueger et al., 1994; Leistico, Salekin, DeCoster, & Rogers, 2008). This heterogeneity suggests that effective intervention efforts may vary considerably depending on the individual. For example, while some offenders with substance abuse disorders and high levels of impulsivity may benefit from remediation programs targeting behavioral inhibition, other offenders with substance abuse disorders and co-occurring anxiety and/or depression may more readily benefit from cognitive or emotion-focused treatments. Identifying subgroups of offenders who differ in the aforementioned cognitive and affective risk factors could thus facilitate more targeted and effective treatment approaches.
One method of differentiating subgroups within a population is model-based cluster analysis (MBCA), a statistical technique that determines the underlying structure of a data set and identifies whether, and how many, subpopulations exist. Multiple studies have used MBCA and its derivatives in clinical and incarcerated samples to differentiate personality types (e.g., Megargee, 1977; Mokros et al., 2015; Sellbom, 2014). For instance, Megargee and colleagues used the Minnesota Multiphasic Personality Inventory (MMPI; Butcher, Graham, Ben-Porath, Tellegen, & Dahlstrom, 2003) to demonstrate 10 personality types occurring within a prison population, many of which varied on measures of interpersonal functioning, negative affectivity, and impulsivity. One of the 10 types, for example, was characterized by high levels of depression and social isolation, whereas another type of offender group was characterized as generally well adjusted and free from major psychological problems.
Although different variables have been used to differentiate offender groups, several studies have used Multidimensional Personality Questionnaire–Brief Form (MPQ-BF; Hicks, Markon, Patrick, Krueger, & Newman, 2004; Miller, Greif, & Smith, 2003; Patrick, Curtin, & Tellegen, 2002). The MPQ-BF assesses a broad range of personality dimensions (i.e., negative emotionality, positive emotionality, and constraint) that relate to criminal risk factors such as psychopathology (Dougherty, Klein, Durbin, Hayden, & Olino, 2010; Eisenberg et al., 2000; Watson, Clark, & Carey, 1988), substance use (L. M. James & Taylor, 2007; McGue, Iacono, Legrand, Malone, & Elkins, 2001), and antisociality (Krueger et al., 2002; Romero, Luengo, & Sobral, 2001). Moreover, MBCA with MPQ-BF has been used to differentiate subgroups of individuals within populations of chronic substance users (Taylor, Reeves, James, and Bobadilla, 2006), veterans with posttraumatic stress disorder (PTSD; Miller et al., 2003), and psychopathic criminal offenders (Hicks et al., 2004; Hicks, Vaidyanathan, & Patrick, 2010; Poythress et al., 2010). However, to date no study has employed MBCA with MPQ-BF within a large, diverse pool of criminal offenders in an effort to elucidate mental health treatment needs.
Thus, this study has two primary goals: (a) Use MBCA with a broad range of personality traits in a large, diverse sample of criminal offenders to identify subgroups with distinct psychological characteristics; (b) determine how the subgroups differ in terms of relevant treatment variables (e.g., affective dysregulation, antisociality, substance use, impulsivity, cognitive ability) and suggest potentially relevant clinical intervention strategies based on these characteristics.
Method
Participants
Participants included 2,388 adult males incarcerated at medium-security prisons in Wisconsin. Individuals were eligible for participation if they were between the ages of 18 and 55, had no documented diagnosis of a psychotic disorder or PTSD, were not currently taking psychotropic medications, had a fourth grade reading level or above, and scored a 70 or above on a standardized measure of intelligence (Wechsler, 1981). Inmates with complete MPQ data were selected from a larger database of eligible participants. 1 All procedures were approved by an institutional review board and were carried out in accordance with the latest version of the Declaration of Helsinki.
Procedure
Each participant first completed two interview sessions and then a packet of questionnaires which assessed personality, substance use, and psychological functioning (individual measures described below). Participants were reminded at the beginning of each session that their participation was voluntary and confidential. All participants provided informed, written consent prior to beginning data collection and were paid at an hourly rate for their participation. All participants completed the MPQ and Psychopathy Checklist–Revised (PCL-R); missing data for other questionnaires are listed below. Occurrences of missing questionnaire data were either due to participants leaving the institution prior to completing questionnaires or due to electing not to complete them.
MPQ-BF
The MPQ-BF (Patrick et al., 2002) is a 155-question, self-report measure of personality traits. The MPQ-BF trait scales are highly correlated with the full MPQ and are consistent with its higher order factors (Patrick et al., 2002). The MPQ-BF consists of 11 primary trait scales (entered for cluster analysis) and three higher order factors (positive affect, negative affect, and constraint; see Table 1 for descriptions of all 11 scales). For these 11 scales, Cronbach’s alpha ranged from .70 to .82. The MPQ-BF also includes two scales designed to detect invalid response patterns. A total of 121 participants (5% of sample) were excluded due to invalid MPQ-BF profiles (Patrick et al., 2002).
MPQ Scales and Descriptions

Note. Descriptions provided reflect high scores on each scale. MPQ = Multidimensional Personality Questionnaire.
Antisociality
Psychopathy
The PCL-R is a 20-item scale of psychopathic traits (e.g., pathological lying, callous/lack of empathy, impulsivity, criminal versatility; Hare, 2003). Trained undergraduates and professional research staff completed the PCL-R based on information obtained during structured interviews and reviews of institutional files. Each item is rated on a 0 (not present) to 2 (present) scale; thus, PCL-R scores range from 0 to 40. Interrater reliabilities were available for 173 participants and yielded a high intraclass correlation (r = .96).
Criminal History
The number of violent and nonviolent charges and convictions (summed) was based on both self-report and legal documentation in institutional files. Violent crimes consisted of charges/convictions for assault/battery, sexual assault, robbery, weapon-related offenses, homicide, and kidnapping. Nonviolent charges/convictions included theft, drug, fraud, obstruction of justice, arson, breach of bail, and driving offenses.
Affect Dysregulation
Depression
The Beck Depression Inventory (BDI-II) is a 21-item self-report measure measuring attitudes and symptoms of depression (A. Beck, Steer, & Brown, 1996). Respondents score the severity of their experience of depression symptoms (e.g., low mood, low motivation, sleep disturbances) over a 2-week period on a 0 to 3 scale, with higher scores indicative of more severe symptomatology. BDI-II total scores range from 0 to 63. BDI-II analyses included data from 1,036 respondents.
Anxiety
The State-Trait Anxiety Inventory (STAI) is a 40-item self-report measure assessing state (e.g., I am tense) and trait anxiety (e.g., I worry too much; Spielberger, 1968). All items are rated on a 4-point scale (1-4) measuring the degree to which the respondent agrees that the statement describes themselves. STAI scores range from 20 to 80. STAI analyses included data from 989 respondents.
Posttraumatic Stress
The Posttraumatic Stress Disorder Checklist–Civilian Version (PCL-C) is a 17-item self-report measure evaluating symptoms of PTSD (e.g., feeling distant or cut off from people; feeling very upset when something reminded you of a stressful experience from the past; Weathers, Litz, Herman, Huska, & Keane, 1994). Participants are asked to assess the degree to which they have experienced each symptom on a 1 to 5 scale over the last month, with total scores ranging from 17 to 85. PCL-C analyses included data from 1,058 respondents.
Impulsivity
The Urgency, Premeditation, Perseverance, Sensation Seeking, Positive Urgency (UPPS-P) Impulsive Behavior Scale (Lynam, Smith, Whiteside, & Cyders, 2006) is a 59-item self-report instrument that measures five distinct dimensions of impulsive behavior, including negative urgency (e.g., It is hard for me to resist acting on my feelings; scores range from 12 to 48), positive urgency (e.g., When I am very happy, I can’t seem to stop myself from doing things that can have bad consequences; scores range from 14 to 56), lack of premeditation (e.g., My thinking is usually careful and purposeful; scores range from 11 to 44), lack of perseverance (e.g., I generally like to see things through to the end; scores range from 10 to 40), and sensation seeking (e.g., I’ll try anything once; scores range from 12 to 48). Each item is rated on a 1 to 4 scale, with higher values representing higher levels of impulsivity. UPPS-P analyses included data from 932 respondents.
Substance Use
Substance Use Chronicity
The Addiction Severity Index–Lite (ASI-Lite; Cacciola, Alterman, McLellan, Lin, & Lynch, 2007) includes a semistructured interview that focuses on types of substance tried (nicotine, alcohol, cocaine/crack, heroin, other opiates, inhalants, hallucinogens, stimulants, methadone, methamphetamine), total months of regular use of each substance (i.e., three or more times per week), and route of administration. A raw total score, which refers to the cumulative number of years using all substances (excluding nicotine), was calculated for each subject. This is calculated by summing the total number of months a person has been using substances divided by 12. ASI-Lite analyses included data from 937 respondents.
Substance Use Disorder
The Structured Clinical Interviews for the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994; SCID; First, Spitzer, Gibbon, & Williams, 1997) assesses the presence of various substance use disorders, including alcohol, marijuana, cocaine, and opiate (i.e., heroin and opiate prescription medication). Symptoms of substance use disorders (e.g., using more of the substance than intended over a period of time) are rated on a 1 (absent) to 3 (threshold) scale. The total number of symptoms that meet a clinically significant threshold (i.e., scores of 3) is summed to determine a diagnosis. A dichotomous variable was created representing the presence or absence of each substance use diagnosis. SCID analyses included data from 1,178 participants.
Cognitive Ability
Intelligence
Intelligence was assessed using the Wechsler Adult Intelligence Scale–Revised (WAIS-R; Wechsler, 1981; n = 976) or the Shipley Institute of Living Scale (SILS; Zachary & Shipley, 1986; n = 1,219). Regardless of the assessment tool used, all participants completed a measure of crystallized/learned knowledge (e.g., defining vocabulary words), as well as a measure of fluid reasoning (e.g., solving visual puzzles).
Education and Reading
Reading level was measured using the reading skills test of the Wide Range Achievement Test–Third Edition (WRAT-3; Wilkinson, 1994). Participants were asked to read a series of words in order and were assessed on their ability to accurately pronounce each word. Total scores are standardized based on the participant’s age group and range from <45 to >155. WRAT analyses included data from 1,101 participants. The last grade level that participants completed in school was used to assess education level and was assessed during the initial screening session.
Working Memory
Digits Backward (Wechsler, 1945) requires a participant to listen to a string of numbers (ranging from 2 to 12 in length) and repeat them to the administrator in the reverse order. Total scores range from 0 to 24. Digits Backward analyses included data from 1,613 participants.
Data Analyses
MBCA was performed on the MPQ-BF data using the computer package mclust (Fraley, Raftery, Murphy, & Scrucca, 2012) in the statistical language R, version 2 (R Core Team, 2013) and the expectation maximization algorithm to classify offenders into subtypes. The goal of MBCA is to use a fit criterion to estimate the number of subgroups within a sample. MBCA thus avoids common criticisms of other clustering techniques (e.g., k means) because the number of clusters is based on the best fit model, rather than a predetermined number. MBCA compares different models with varying assumptions (volume, shape, and orientation) about the structure of the data, and a fit index is calculated for each model to determine the best fit model. The models range from very simple (e.g., all parameters are held constant) to the least parsimonious (e.g., all parameters are allowed to vary). If the best fitting model indicates a one-cluster solution, then the observed data are multivariate, normal, and do not contain a mixture of subgroups. The fit index used, the Bayesian information criterion (BIC), maximizes the best fit model while minimizing the number of parameters being estimated. The smallest BIC value indicates the best fit model. In the current sample, 10 models were compared to determine the optimal subgroup structure.
After group identification, linear regression with planned contrast analyses was conducted to compare the groups on the MPQ variables used to create them and additional variables of interest. Chi-square analyses were used to examine group differences in substance use diagnosis. Because there were 15 between-group contrasts per variable, Bonferroni corrections were made for each variable. Bonferroni corrections yielded a corrected p value of .0033 (.05/15) to identify significant group differences within each model. Due to skewed distributions in the violent and nonviolent crime data, Box-Cox power transformations (log) were performed for these analyses. Effect sizes for contrast analyses are presented as r contrast values (Rosnow, Rosenthal, & Rubin, 2000). A standard correlation coefficient effect size (r) reflects a point biserial correlation between two groups. Because more than two groups were compared within one regression model for all contrast analyses, the partial correlation effect size with all noncontrast variation removed (r contrast) is reported. Participant information for all groups is provided in Figures 1 to 5. Demographic data for each group are provided in Table 2.
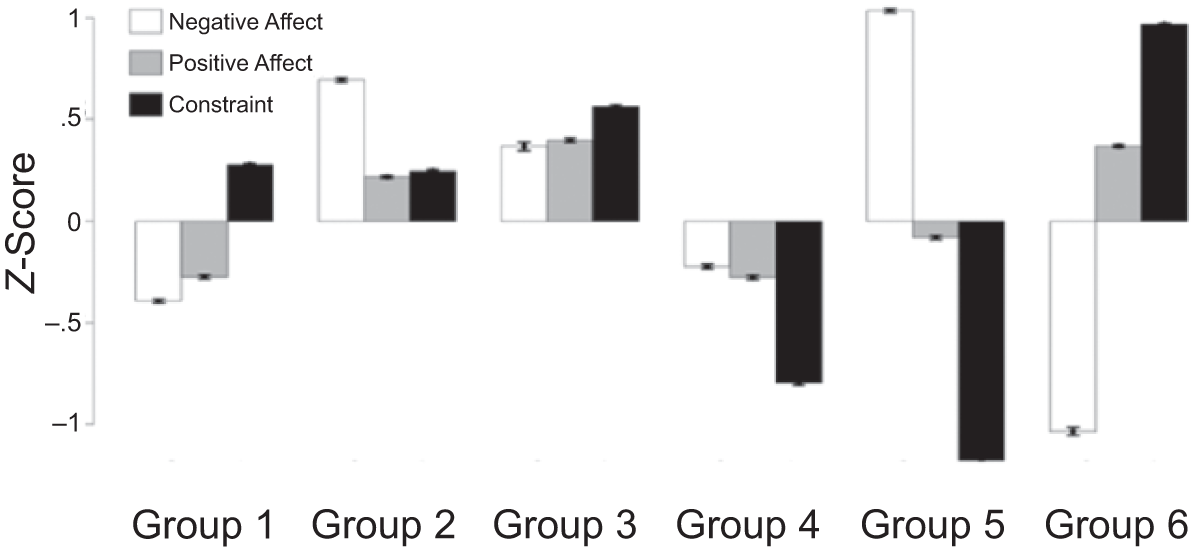
Z-Score Profile of the MPQ-BF Scales Associated With Subgroups of Offenders
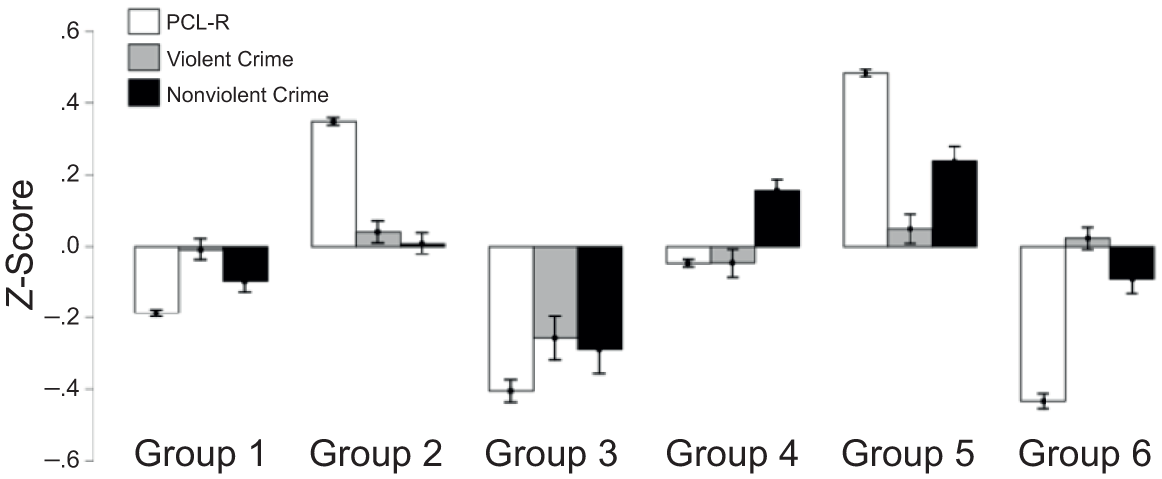
Z-Score Profile of the Antisociality Variables Associated With Subgroups of Offenders

Z-Score Profile of the Affect Dysregulation Variables Associated With Subgroups of Offenders
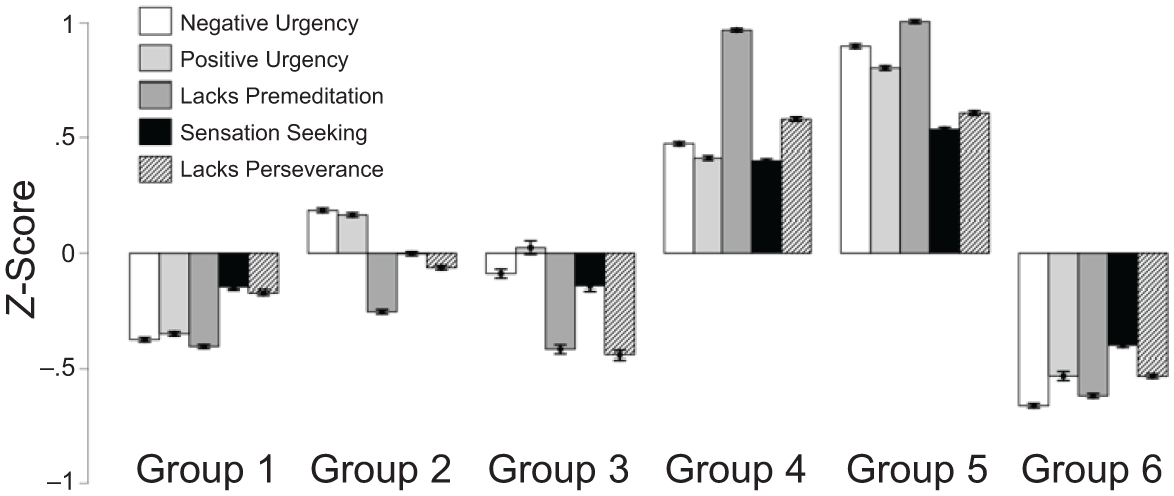
Z-Score Profile of the Impulsivity Variables Associated With Subgroups of Offenders

Z-Score Profile of the Substance Use Variables Associated With Subgroups of Offenders
Demographic Information
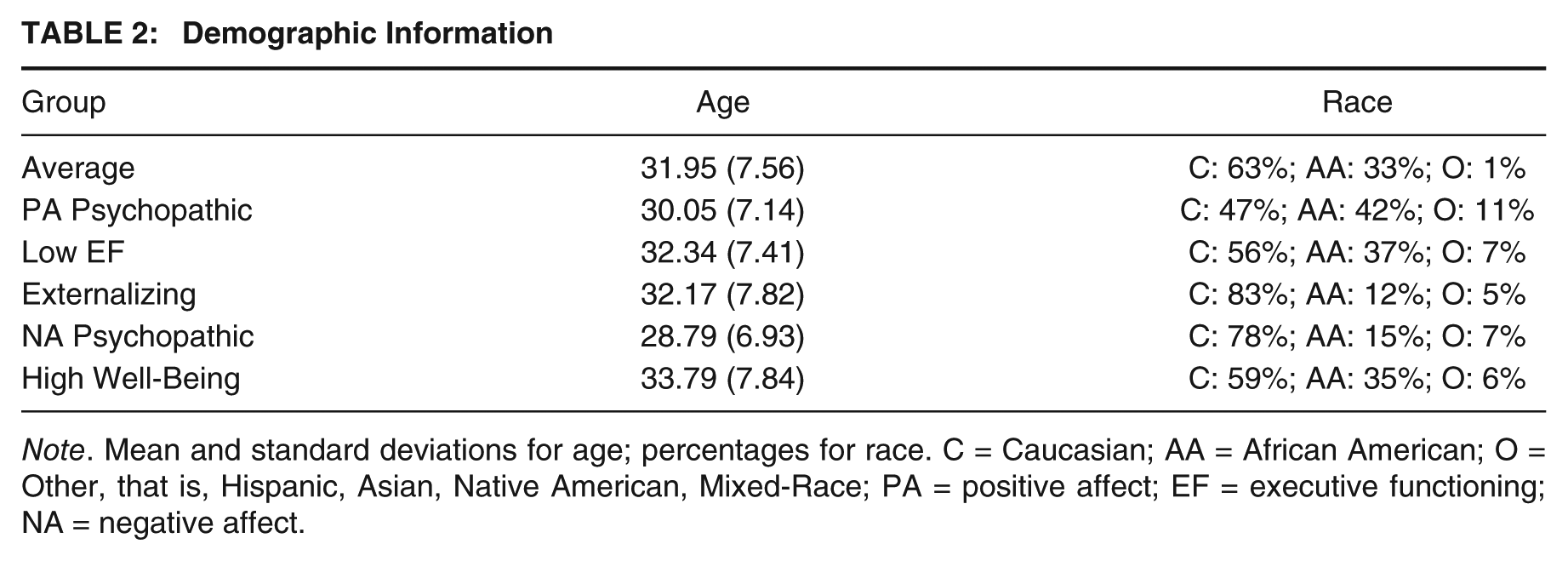
Note. Mean and standard deviations for age; percentages for race. C = Caucasian; AA = African American; O = Other, that is, Hispanic, Asian, Native American, Mixed-Race; PA = positive affect; EF = executive functioning; NA = negative affect.
Results
MBCA Analyses
The best fit model for the offenders (BIC = −68,923.97) yielded a six-cluster solution (Group 1, n = 549; Group 2, n = 484; Group 3, n = 105; Group 4, n = 404; Group 5, n = 337; Group 6, n = 410) with equal shape and orientation. Two thirds of the sample had a high probability of correct cluster assignment (≥80%). Low cluster assignment probability results from individuals who endorse a variety of traits used to model the clusters, thus making it difficult to assign them to a specific cluster. Data from statistical analyses are included in Tables 3 to 8. Summaries of group differences are provided below and presented in Figures 1 to 6.
MPQ Group Differences

Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients. PA = positive affect; EF = executive functioning; NA = negative affect; df = 2,275.
Group Differences in Antisociality
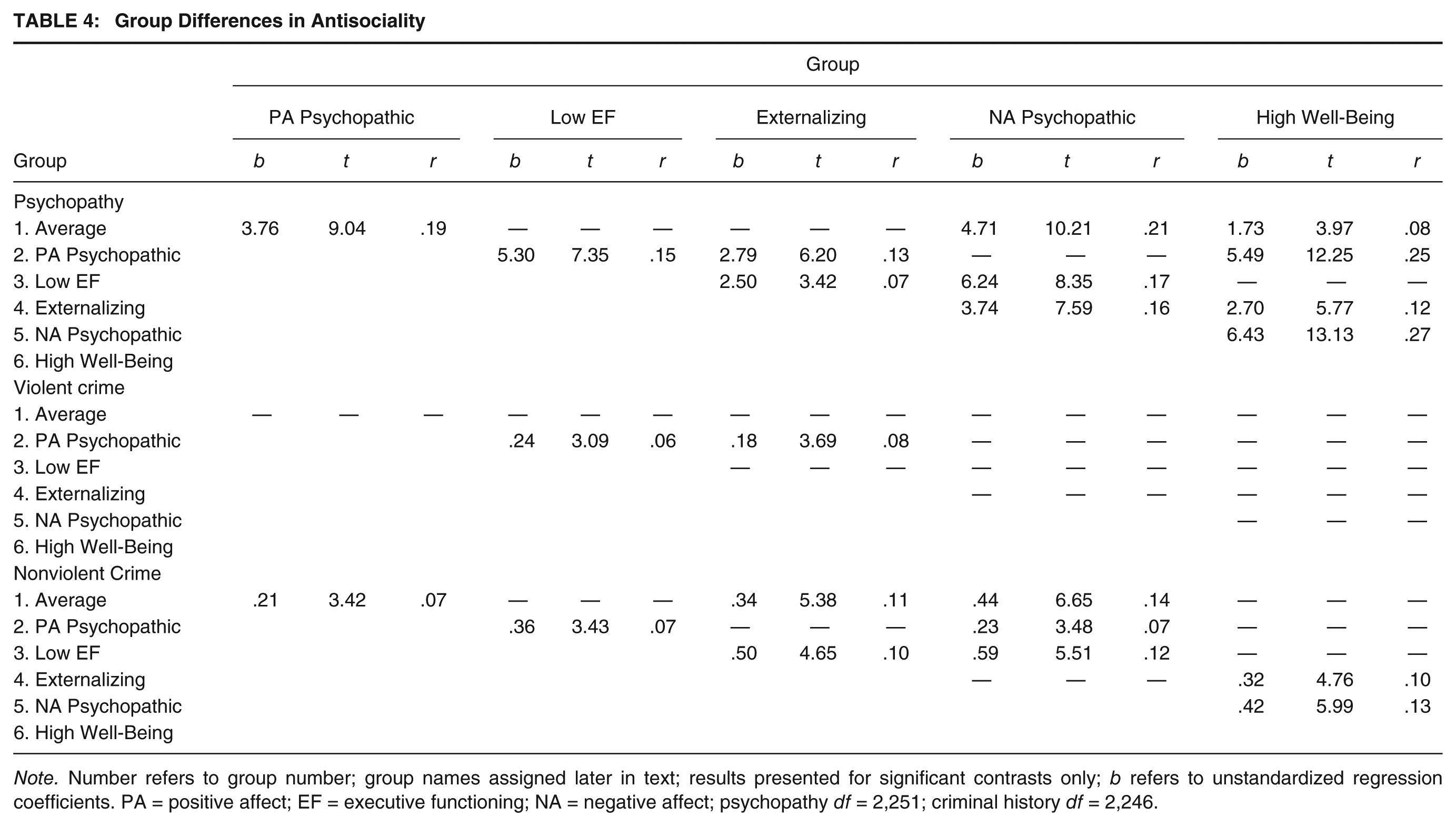
Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients. PA = positive affect; EF = executive functioning; NA = negative affect; psychopathy df = 2,251; criminal history df = 2,246.
Group Differences in Affect Dysregulation
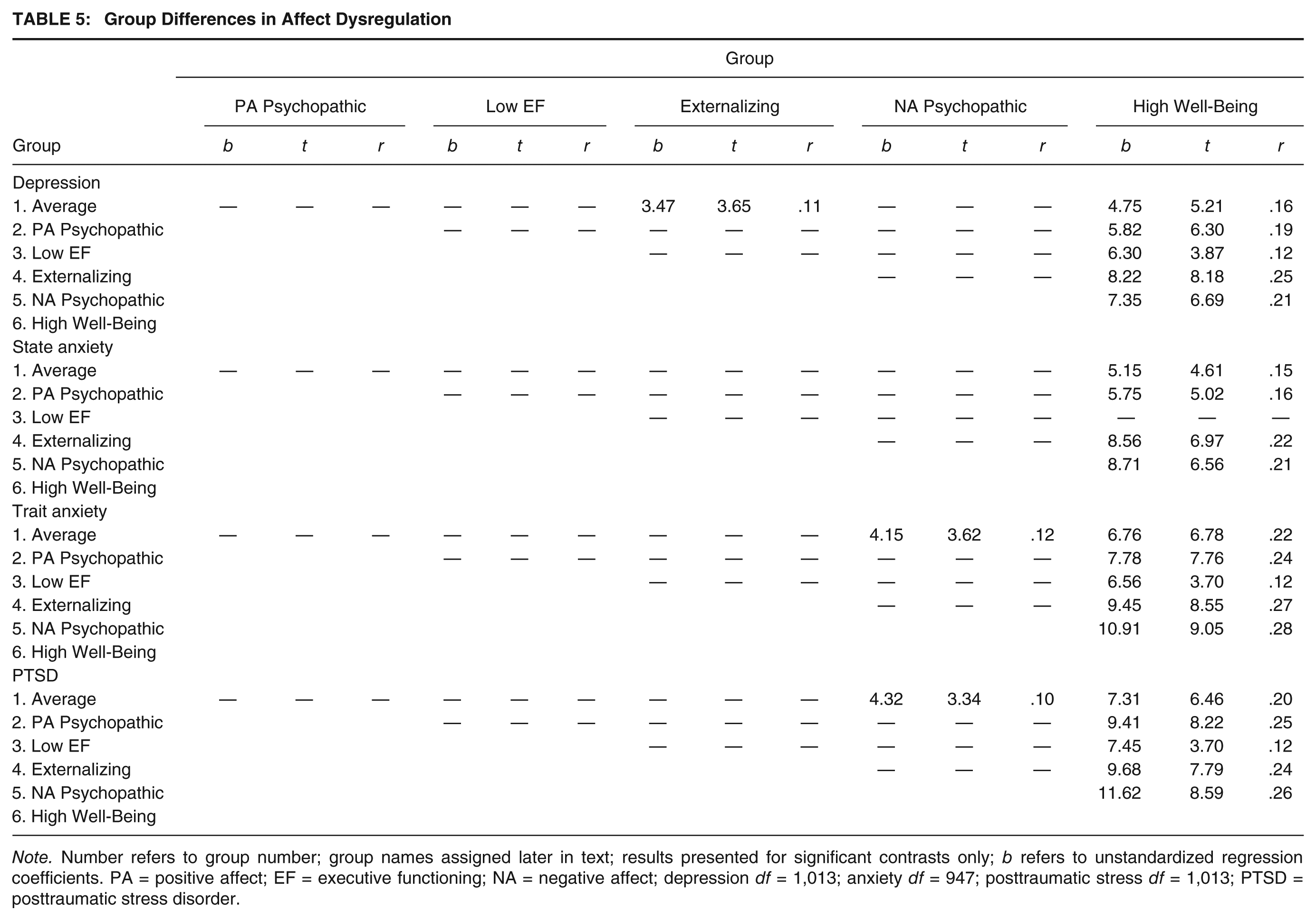
Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients. PA = positive affect; EF = executive functioning; NA = negative affect; depression df = 1,013; anxiety df = 947; posttraumatic stress df = 1,013; PTSD = posttraumatic stress disorder.
Group Differences in Impulsivity
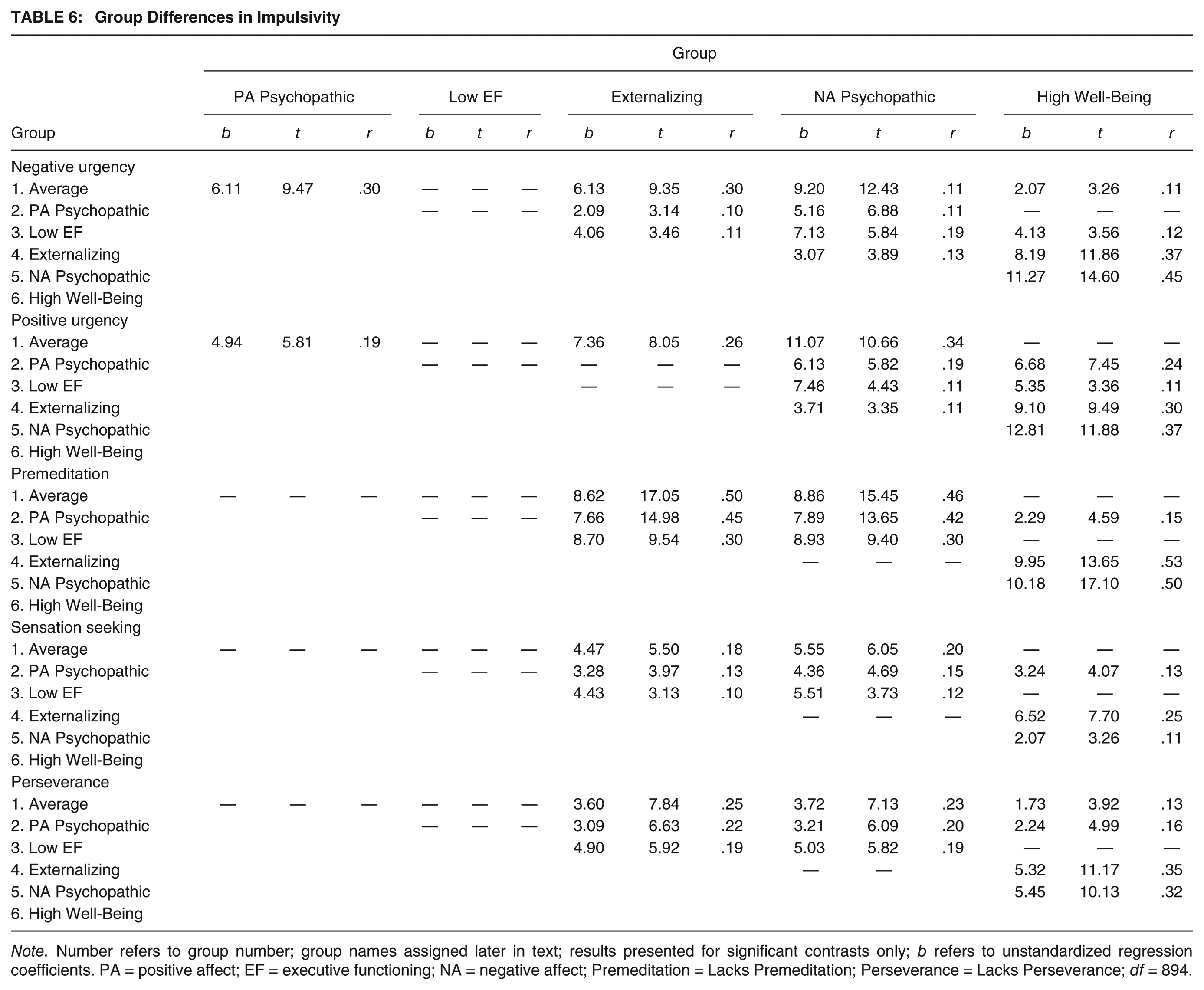
Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients. PA = positive affect; EF = executive functioning; NA = negative affect; Premeditation = Lacks Premeditation; Perseverance = Lacks Perseverance; df = 894.
Group Differences in Substance Abuse

Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients; z and p values provided for substance use disorder chi-square analyses; PA = positive affect; EF = executive functioning; NA = negative affect; df = 987
Group Differences in Cognitive Ability
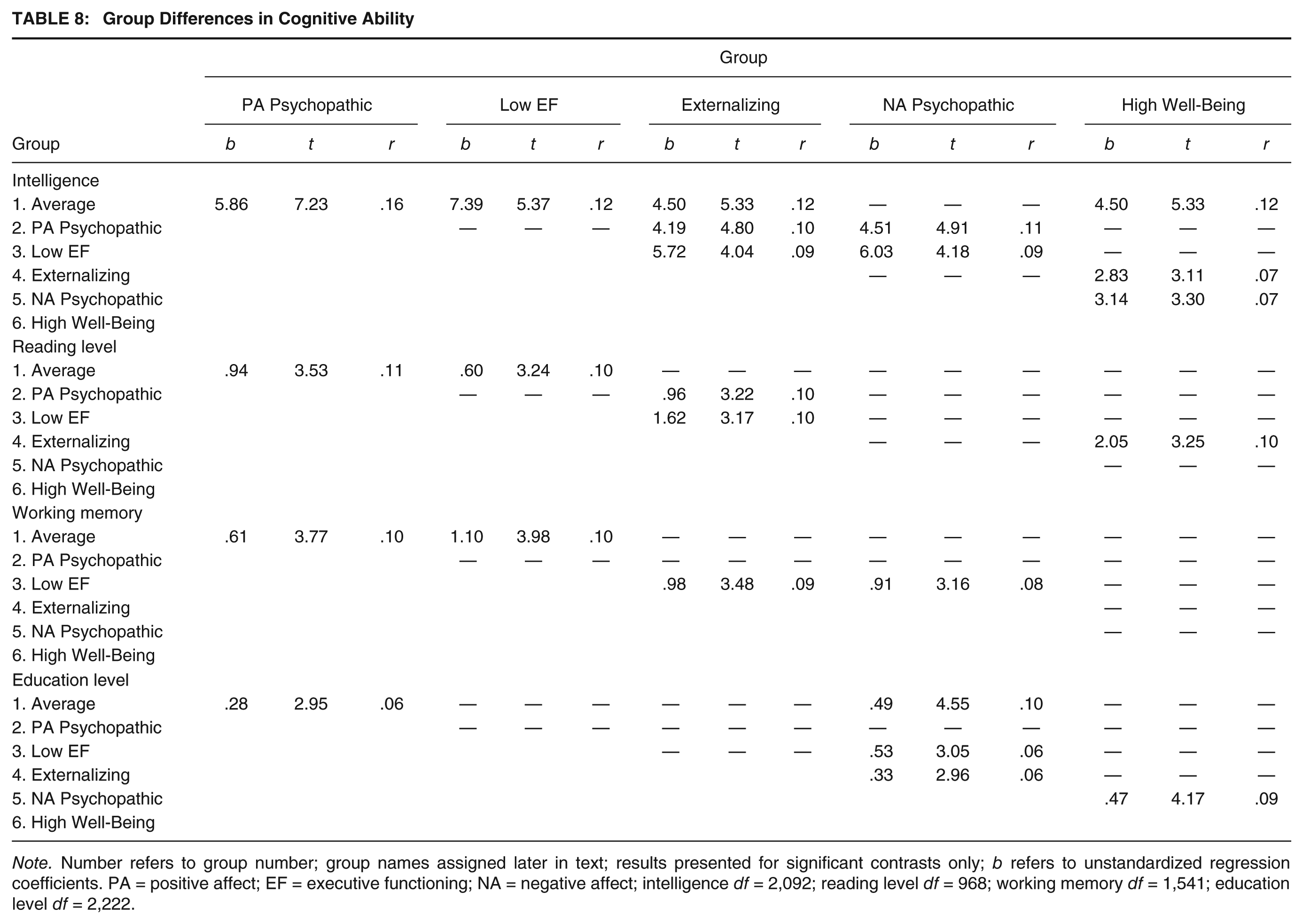
Note. Number refers to group number; group names assigned later in text; results presented for significant contrasts only; b refers to unstandardized regression coefficients. PA = positive affect; EF = executive functioning; NA = negative affect; intelligence df = 2,092; reading level df = 968; working memory df = 1,541; education level df = 2,222.
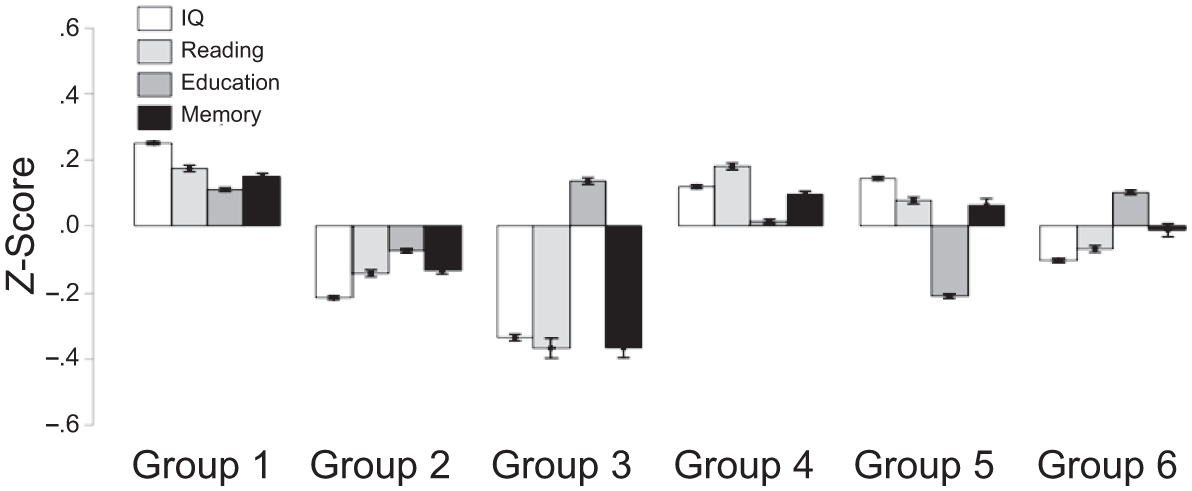
Z-Score Profile of the Cognitive Variables Associated With Subgroups of Offenders
Differences Between Groups on MPQ Scales
Specific MPQ profiles of each group are presented in Figure 1. A summary of group characteristics is provided here: near-average scores (within .5 SD of sample mean), moderately high/low scores (.5-.75 SD from sample mean) and high/low scores (≥.75 SD above mean). Group 1 is characterized by near-average scores on all three MPQ dimensions (positive affect, negative affect, and constraint). Group 2 is characterized by near-average scores on positive affect, moderately high scores on negative affect, and near-average scores on constraint. Group 3 is characterized by near-average scores on positive affect, near-average scores on negative affect, and moderately high scores on constraint. Group 4 is characterized by near-average scores on positive affect and negative affect and moderately low scores on constraint. Group 5 is characterized by near-average scores on positive affect, high scores on negative affect, and low scores on constraint. Group 6 is characterized by high scores on positive affect, low scores on negative affect, and moderately high scores on constraint. See Table 3 for details on statistical differences between groups for each MPQ dimension.
Differences Between Groups on Behavioral, Psychological, and Environmental Variables
To summarize, Group 1 was characterized by a low number of charges/convictions for violent crimes. Individuals in Group 1 had the highest IQ and reading level compared with the other groups and tended to perform better on working memory tasks. Group 2 scored very highly on the PCL-R and had the greatest number of charges/convictions for violent crimes. In addition, Group 2 members were characterized by high levels of alcohol and marijuana use disorders, low IQ, and low reading level. Group 3 members had very few criminal convictions and generally had the lowest cognitive ability across all measures (i.e., IQ, reading level, and working memory). Group 4 was characterized by high levels of substance use and moderate levels of general antisociality (i.e., criminal convictions and PCL-R scores). Group 5 scored particularly high on the PCL-R and had the greatest number of charges/convictions for nonviolent crimes. Group 5 was also characterized by high levels of anxiety, PTSD, impulsivity, and substance use (i.e., opiate and cocaine use disorders). Finally, Group 6 was characterized by low PCL-R scores, low levels of affect dysregulation (i.e., depression, anxiety, and posttraumatic stress), impulsivity, and substance use.
Based on these characteristics, the following group names were assigned to better reflect group membership: Group 1: Average; Group 2: Psychopathic-Positive Affect; Group 3: Low Executive Functioning; Group 4: Externalizing; Group 5: Psychopathic-Negative Affect; Group 6: High Well-Being.
Discussion
In a sample of more than 2,000 adult male prison inmates, six distinct subgroups were identified based on measures of broad personality traits. Moreover, the personality differences among groups were linked to substantial differences in psychopathology, criminality, substance use, cognitive ability, and impulsivity. Specifically, Group 1 (Average) offenders scored near the sample’s mean across most measures of personality, psychopathology, criminality, substance use, and impulsivity, but scored higher than most groups on cognitive ability. Group 2 (Psychopathic-Positive Affect) offenders scored highly on measures of positive affect and psychopathy, committed the greatest number of violent crimes, and demonstrated the most severe alcohol and marijuana use. Group 3 (Low Executive Functioning) offenders scored very highly on measures of positive affect, but poorly on executive function and cognitive ability. Group 4 (Externalizing) offenders scored slightly lower than the sample mean across all measures of personality, yet demonstrated severe substance use and impulsivity. Group 5 (Psychopathic-Negative Affect) offenders showed the most severe scores on measures of negative affect, psychopathology, substance use, psychopathy, and impulsivity. Group 6 (High Well-Being) offenders scored the highest on positive affect and showed the lowest levels of psychopathology, substance use, criminality, and impulsivity. Overall, this combination of results strongly supports the utilization of personality traits to differentiate offender subtypes and identifies unique treatment-relevant variables associated with each offender subtype.
The markedly divergent affect scores displayed by the Psychopathic-Negative Affect and High Well-Being groups highlight the importance of considering both positive and negative affect in mental health and treatment settings for offenders. The high positive affect scores within High Well-being individuals suggest that this group of offenders have an optimistic disposition and endorse having strong social bonds. Being engrained in a social community has been identified as a protective factor from criminally reoffending (Lodewijks, de Ruiter, & Doreleijers, 2010), and similarly, being socially isolated has been identified as a risk factor to reoffend (McGrath, Lasher, & Cumming, 2012; Quinsey, Harris, Rice, & Cormier, 1998). Furthermore, individuals with social supports tend to more closely adhere to treatment programs (DiMatteo, 2004; Voils, Steffens, Bosworth, & Flint, 2005) and have more successful treatment outcomes (Dobkin, Civita, Paraherakis, & Gill, 2002). The very high scores on the social closeness scale among High Well-Being members may have promising implications for their amenability to treatment efforts and may suggest that this group is at a lower risk to reoffend than other groups. This is an important consideration, given that the High Well-Being group consisted of more than 400 offenders in the current sample (17%), suggesting that a substantial proportion of incarcerated offenders may be at a low risk to reoffend. Future research should continue to explore the role of positive affect and close social ties as protective factors within the incarcerated population.
Psychopathic-Negative Affect offenders, in contrast, displayed very high scores on negative affect, suggesting that these offenders feel slighted by others and are prone to aggressive behavior. Negative affect has been consistently associated with the initiation of and severity of substance use (Brady & Sinha, 2005; Kassel, Stroud, & Paronis, 2003; Mason, Hitch, & Spoth, 2009). For instance, Epstein et al. (2009) reported that feelings of sadness and anger robustly predicted the craving of heroin among heroin users. Furthermore, Baker, Piper, McCarthy, Majeskie, and Fiore (2004) posited that a primary motivation for the initiation of drug use is avoidance of or escape from negative affectivity. In accordance with this body of work, Psychopathic-Negative Affect individuals showed more chronic substance use than the other offender groups, specifically with heroin and cocaine. It is possible that the high levels of negative affect displayed by Psychopathic-Negative Affect offenders play a causal role in their substance abuse, although given the cross-sectional nature of this study, causation cannot be concluded. Similarly, the very high impulsivity, and particularly the urgency scores, among Psychopathic-Negative Affect offenders suggests that Psychopathic-Negative Affect offenders tend to act impulsively in an effort to avoid feelings of strong negative affect (e.g., Verdejo-García, Bechara, Recknor, & Pérez-García, 2007).
This characterization has strong treatment implications, as Psychopathic-Negative Affect offenders may readily benefit from treatment programs that facilitate the development of adaptive coping skills and emotion regulation. Dialectical Behavioral Therapy (DBT; Linehan, 1987), in particular, may be beneficial for this offender group given its emphasis on learning to tolerate states of negative affect and distress. DBT has been shown to be effective at reducing aggression and antisociality within offender samples (Evershed et al., 2003; Trupin, Stewart, Beach, & Boesky, 2002) and improve emotion regulation skills among individuals with personality pathology (Panos, Jackson, Hasan, & Panos, 2014; Rosenfeld et al., 2007). Given the high psychopathy scores within the Psychopathic-Negative Affect group, DBT may be a promising future direction for treatment providers working with offenders with extreme levels of negative affect and/or personality pathology.
Whereas Psychopathic-Negative Affect offenders may be motivated to use substances in an effort to alleviate states of high negative affect, it is plausible that the sensation seeking and impulsive behavior that characterizes Externalizing offenders contributes to their frequent substance use. Sensation seeking behavior has also been identified as a risk factor for the utilization of drugs (Crawford, Pentz, Chou, Li, & Dwyer, 2003). Thus, behavioral treatment models that emphasize self-regulation may be highly beneficial for Externalizing offenders. For instance, there is evidence that cognitive-behavioral therapy (CBT; J. S. Beck, 1995) is effective at improving self-regulatory responses among individuals with attention deficit hyperactivity disorder (ADHD; Mongia & Hechtman, 2012; Weiss et al., 2012). Similar tactics may be beneficial for Externalizing offenders, although future research is needed to substantiate this idea.
Average offenders scored near the sample mean across measures, suggesting that this group may represent the typical inmate population. In accordance with this interpretation, the Average group was the largest of all subgroups (n =549, 23%). Interestingly, this group scored the highest on measures of cognitive ability, suggesting that this group may be amenable to higher level cognitive-based programs targeting antisociality, generally. There is some evidence that CBT effectively reduces antisocial behavior among adolescents and adults (Davidson et al., 2009; Lipsey, Landenberger, & Wilson, 2007; McCart, Priester, Davies, & Azen, 2006). The use of cognitive-behavioral models of treatment may therefore help reduce the risk of recidivism among the Average offender population.
Low Executive Functioning offenders scored highly on measures of positive affect, but the lowest on measures of intelligence and executive function compared with other groups. Given the association between poor executive functioning and criminality (e.g., Morgan & Lilienfeld, 2000), improvement of executive function skills may be an important area of intervention for Low Executive Functioning members. There is increasing evidence that mindfulness-based treatment programs can improve executive function impairments in attention, emotion regulation, and cognitive control (Tang, Yang, Leve, & Harold, 2012; Teper & Inzlicht, 2013; Teper, Segal, & Inzlicht, 2013). With this in mind, the utilization of mindfulness-based programs with Low Executive Functioning offenders may lead to meaningful improvements in broad-range executive function and, potentially, decreased criminal risk.
Although this study had several notable strengths, including the large offender sample size, it is not without limitations. The data utilized for this study stemmed primarily from self-report measures. Accordingly, it will be important to examine behavioral and psychophysiological differences among offender groups to substantiate potential mechanisms contributing to the personality and psychopathological differences observed between offender types. In addition, because this study utilized only adult men, we are unable to address the heterogeneity and treatment needs in female offenders or juvenile offenders. The exclusion criteria utilized may also limit the applicability of the current findings, given the exclusion of individuals with psychosis, PTSD, and low IQ. Future studies should employ similar methodology in more heterogeneous samples in an effort to specify effective targets for intervention within these samples. Finally, despite the large sample size, we did not have data from all subjects for all utilized measures. Nonetheless, the sample sizes across groups for each measure were large enough for statistical comparisons. For example, for the UPPS-P, which was the measure completed by the lowest number of participants (n = 932), group size ranged from 35 to 175 subjects in each of the six groups, for between-group comparisons.
In sum, this study identified six offender subtypes within a large, incarcerated population using measures of broad personality traits. The offender groups differed on important treatment-related variables, including mental health, criminality, cognitive ability, impulsivity, and substance use. These findings provide insight into potential treatment and intervention strategies to target the specific needs among incarcerated offenders. Considering the heterogeneity among criminal offenders and identifying specific treatment needs for these offenders are crucial first steps toward reducing criminal recidivism and substance abuse, and improving mental health outcomes within the incarcerated population.
Footnotes
Acknowledgements
The authors thank the many individuals at the Wisconsin Department of Corrections who made this research possible and are especially indebted to Warden Judy Smith, Warden Randy Hepp, and Dr. Kevin Kallas.