
Abstract
Several meta-analyses have examined the Central Eight risk factors for reoffending in the general forensic population. To our knowledge, this is the first meta-analysis to focus exclusively on the predictive validity of risk factors for recidivism in forensic outpatients. A multilevel meta-analysis was conducted of studies in which static and dynamic risk factors were investigated as predictors of violent and/or general recidivism in forensic outpatients. Twenty-seven studies were included, with 543 effect sizes in a unique population of 116,982 adult offenders. The Central Eight risk domains were found to be predictive of violent and general recidivism; however, these factors predicted recidivism with small-to-moderate effects. Overall, in the same domain, the dynamic risk factors were more strongly related to recidivism than the static risk factors. This knowledge may be used to guide future outpatient treatment.
Introduction
Since several studies have demonstrated the limited rehabilitative effect of prison sentences, forensic outpatient treatment has become increasingly important (Mears, Cochran, & Bales, 2012; Nagin, Cullen, & Jonson, 2009). Our knowledge of effective intervention to reduce delinquent behavior is mainly based on research on mixed populations (inpatients, prisoners, and offenders under varying degrees of probation supervision). To optimize the effect of treatment of the growing group of outpatients (Bales, Burkes, Scaggs, & Clark, 2015), it is important to enhance our understanding of which risk and criminogenic factors should be targeted in treatment to reduce reoffending. The aim of the present study was, therefore, to meta-analytically examine the most important risk and needs factors for forensic outpatients. However, the term outpatient is defined in a number of different ways across various studies. For instance, offenders in some studies were labeled as forensic outpatients when they were solely under intensive community supervision, whereas in other studies forensic outpatients received varying interventions, including drug treatment, cognitive-behavioral therapy, or family treatment (Lawrence & Lyons, 2011; Patenaude, 2013; Ploeg, 2008; Subramanian & Shames, 2013). Moreover, the term “parolees” or “probationers” is also used to describe a population that can be interpreted as forensic outpatients in the sense that they have been offered the same interventions mentioned above. The common denominator seems to be that all of these patients live in the community. Hence, in this article, the term “forensic outpatients” will be used to describe the population of offenders who have received community supervision and/or any treatment intervention while living in the community.
In the last decade, the central focus in offender treatment has been the risk–need–responsivity (RNR) principles, as these principles prescribe the basics of effective outpatient forensic care. The RNR model is an offender rehabilitation model developed by Bonta and Andrews (2017). In this model, the Risk principle states that high-risk offenders should be treated more frequently and for longer than low-risk offenders. The Need principle describes the focus of the treatment, which should target dynamic (changeable) risk factors, while the third principle (Responsivity) describes the required qualities of the therapist (general responsivity) and the tailoring of the treatment to the specific (dis)abilities of the patient (specific responsivity). Bonta and Andrews (2017) studied the effect of adhering these principles to forensic treatment on recidivism, concluding that recidivism rates decreased as the number of principles applied in the treatment protocol increased. Adherence to all three RNR principles had a greater rehabilitative effect for outpatients compared with clinical patients (r = .35 for community-based treatment and r = .17 for custody; Bonta & Andrews, 2017).
To adequately implement the risk and needs principles, knowledge of the most predictive static and dynamic criminogenic risk factors for recidivism is necessary. Static risk factors are features of the offenders’ histories that predict recidivism but are not amenable to intervention, such as prior offenses. By contrast, dynamic risk factors are potentially changeable factors, such as Substance Abuse and Criminal Network. Given that dynamic risk factors are considered to be responsible for the increase in risk, they have also been referred to as criminogenic needs (Bonta & Andrews, 2017). Five (meta-analytic) studies of predictors of recidivism among general offenders (Olver, Stockdale, & Wormith, 2014), youthful offenders (Grieger & Hosser, 2014), mentally disordered offenders (Bonta, Blais, & Wilson, 2014), racial minorities (Gutierrez, Wilson, Rugge, & Bonta, 2013), and drug offenders (Wooditch, Tang, & Taxman, 2014) found support for the eight strongest static and dynamic predictors of recidivism, also referred to as the Central Eight risk/needs factors. In more detail, the Central Eight risk/needs factors are as follows: a History of Antisocial Behavior (early involvement in criminal activity, a large number and variety of prior offenses, rule violations); Antisocial Personality Traits (impulsive or aggressive behavior, callous disregard for others); Antisocial Cognitions (attitudes, values, and rationalizations condoning antisocial behavior); Antisocial Friends (social support from friends with antisocial attitudes and/or who are involved in criminal activity); Family/Relationships (lack of social support of family members and/or a turbulent and violent relationship with a romantic partner); School/Work (quality of interpersonal relationships at school or work and low performance and involvement); Leisure (low levels of involvement and satisfaction in anticriminal leisure pursuits); and Substance abuse (problems with alcohol and/or drugs; Bonta & Andrews, 2017).
In other meta-analytic studies, moderator effects were found. Specifically, Substance Abuse and Personal/Emotional Problems were more predictive of recidivism in women than in men (Olver et al., 2014), while lack of Leisure was a better predictor of recidivism among ethnic/racial majority offenders than among offenders from ethnic/racial minority groups (Gutierrez et al., 2013; Olver et al., 2014; Wilson & Gutierrez, 2014). The offender’s age was also found to significantly moderate the relationship between the predictive value of risk factors and recidivism, that is, as age increases, the predictive effect of risk factors decreases (van der Put, Deković, Stams, Hoeve, & van der Laan, 2012). Interestingly, Spruit, van der Put, Gubbels, and Bindels (2017) found a U-shaped relationship between risk factors and recidivism across age, with an increased effect among offenders below the age of 40 and a decreased effect among offenders aged 40 years and over. Given the relevance of gender, race/ethnicity, and age to the relationship between risk factors and recidivism, these variables were included in the current meta-analysis as moderators.
Aim of the Current Meta-Analysis
The central aim of this multilevel meta-analysis was to identify the risk and needs factors for the prediction of general and violent recidivism among forensic outpatients.
In several ways, this study adds to the existing body of forensic knowledge in general and to findings from previous meta-analyses of forensic populations in particular. First, it focuses on a more homogeneous forensic population (i.e., outpatients) instead of the more general forensic population of in- and outpatients (Olver et al., 2014), or a subgroup of severely mentally disordered offenders who are typically treated in inpatient forensic clinics (see, for example, Bonta et al., 2014). A more homogeneous forensic outpatient sample was achieved through excluding studies of former inpatients or ex-detainees. The difference between inpatients and outpatients emerges in their offense history and recidivism rates. Compared with forensic outpatients, forensic inpatients have committed more severe violent offenses, often leading to physical injuries, and suffer more from major mental disorders such as psychotic and personality disorders (Ministry of Security and Justice, 2017). Although outpatients also suffer from personality disorders, the prevalence of psychotic disorders is much lower, while the incidence of impulse control and substance abuse disorders is much higher (Henrichs, Bogaerts, Sijtsema, & Klerx-van Mierlo, 2015; Spruit et al., 2017). This could explain why the recidivism rates reported in previous meta-analyses (in which the proportion of inpatients was relatively large) vary widely from 39% to 55.5% for general recidivism and 13.7% to 31.6% for violent recidivism, with the lowest recidivism percentages being found among general offenders and the highest among ethnic/racial minorities (Gutierrez et al., 2013; Olver et al., 2014).
On average, studies of outpatient populations report recidivism rates closer to the lower end of the inpatient range noted in the abovementioned studies. For example, a study by Rhodes, Dyous, Kling, Hunt, and Luallen (2013) found an overall recidivism percentage of 24.9% among offenders on federal community supervision. Accordingly, the current meta-analysis may shed some light on the differences in recidivism rates when focusing solely on an outpatient population. Second, the outcomes of the present study will contribute to more meaningful practices in terms of the applicability of the RNR principles to outpatient forensic care. Moreover, by including gender, race/ethnicity, and age as moderators in this specific group of offenders, some light will be shed on their relevance in terms of responsivity, and thus on how the treatment response may be optimized. Third, a distinction is made between the static and dynamic nature of risk factors within specific risk domains. Previous studies have shown the importance of the changes in the dynamic risk factors as a means of monitoring treatment progress (Lewis, Olver, & Wong, 2012), and findings have suggested a relation between positive changes in the dynamic risk factors and lowered recidivism rates (De Vries Robbé, De Vogel, Douglas, & Nijman, 2014). However, the findings from these studies are of limited use for the formulation of specific treatment goals in clinical practice as they represent an aggregated score of dynamic risk factors (total dynamic risk score and total static risk score). More specifically, the outcomes tell us about the importance of change in dynamic risk factors and recidivism, but little about which specific dynamic risk factors bring about changes in recidivism and should thus be targeted in treatment. Hence, the comparison of unique static and dynamic risk factor scores will provide more useful information on their relative importance for the prediction of recidivism and formulation of specific treatment targets.
In line with previous (meta-analytic) studies on the predictors of recidivism (Bonta et al., 2014; Grieger & Hosser, 2014; Gutierrez et al., 2013; Olver et al., 2014; Wooditch et al., 2014), it was expected that the same risk factors for general recidivism and violent recidivism would emerge for outpatients as for the general forensic population, as outpatients are a part of this general population. However, the strength of the predictive value could differ due to the fact that effect sizes are influenced by recidivism base rates. When base rates deviate from 50%—for instance, in the case of low-base-rate events such as sexual recidivism, where base rates are often below 10%—effect sizes remain small, with r < .20 (Babchishin & Helmus, 2016). In general, outpatients recidivate at a lower rate than inpatients. Hence, smaller effect sizes were expected for predictors of general and violent recidivism among outpatients.
Method
Study Inclusion Criteria
Several criteria were used to govern the inclusion of primary studies. First, these studies needed to examine offenders who were 18 years of age or older, male or female, not incarcerated, and either treated in a forensic outpatient treatment setting or supervised by a probation officer in the community. Studies were included when incarceration preceded outpatient treatment and/or community supervision. We further noted that there were some differences in the definitions of “outpatient” and “treatment,” as well as in related terminology, between the countries in which the primary studies were conducted; only studies in which community sentencing was operationalized as an imposed outpatient/community-based treatment (such as a psychological or addiction treatment, probation, or supervision) were chosen for inclusion. In this operationalization, treatment length and/or movement restrictions could vary between primary studies, as community sentences are imposed by court judges working in different jurisdictions. In all samples of offenders, the offenders were allowed to have jobs, to live in a private home (i.e., not institutionalized), and to move freely without supervision. Offenders in the samples of primary studies could have been imprisoned at some point in their past or could have received treatment for mental illness. However, studies were excluded when the patients had been released from forensic inpatient treatment or when offenders had been released from prison without outpatient treatment or supervision.
Second, the included studies had to define recidivism as a new arrest, reconviction, or violation of judicial conditions. Third, the studies needed to examine at least one static or dynamic risk factor for recidivism of any offense type. As mentioned in the “Introduction” section, static risk factors are features of the offenders’ histories that predict recidivism, but that are not amenable to intervention; by contrast, dynamic risk factors (such as having criminal friends) are changeable and can be targeted in interventions. Moreover, studies examining risk factors for child sexual abuse (and not other types of offenses) were excluded, as risk factors for sex offending differ from other types of offending behavior (Mann, Hanson, & Thornton, 2010). An additional reason to exclude risk factors for sexual offending is that these factors are not incorporated in the Central Eight risk factors proposed by Bonta and Andrews (2017), which form the focus of the current meta-analysis.
Risk factors could not be included when statistical information needed for calculating effect sizes was missing. Hazard ratios were not included, as these ratios refer to differences between groups in time until an event occurs, which cannot be transformed into a correlation. Fourth, only quantitative research was included, except for studies reporting on results of survival analyses, responsivity factors (e.g., treatment motivation), and predictors of sexual recidivism. Studies focusing on the validation of a risk assessment instrument were only included when associations between individual items and recidivism were reported. Finally, we only included studies written in English, Dutch, or German.
Literature Search
In our search for relevant primary studies, we applied three strategies (see Figure 1). First, all electronic databases (n = 413) accessible through the library of the University of Amsterdam were searched (the complete list of databases is available upon request). The most important databases we exhaustively searched were the following: ERIC (Education Resources Information Center), Pubmed, Web of Science, Medline, Cochrane Library, PsycINFO, PiCarta, JSTOR (Journal Storage), and Hein Online. In this electronic search, the syntax component “forensic outpatient” OR “forensic community based” OR “probation” OR “parole” OR “post release” AND “adult” OR “adult offender” OR “adult delinquent” was combined with the following syntax component: “risk factor” OR “predict*” OR “criminogenic need” OR “recidivis*” OR “re-offen*” OR “reoffen*” OR “repetition” OR “recurrence.” This electronic search resulted in 15,482 hits consisting of primary studies covering a wide variety of topics and samples. To narrow down these hits to studies that were eligible for inclusion, the first and third author proceeded with reading titles, abstracts, and (if necessary) full article texts. Of the 15,482 primary studies that were initially found, 2,563 studies appeared to be relevant after following deduplication and screening of the titles. After reading the study abstracts, 2,097 studies were disregarded, leading to a sample of 466 primary studies. The full texts of these studies were then evaluated against all inclusion criteria. In the end, eight studies were included in the qualitative synthesis and 27 primary studies were included in the meta-analysis.

Predictors of Recidivism in Forensic Outpatients Meta-Analysis Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram
In our second search strategy, we manually screened the reference lists of the studies that were eligible for inclusion in the previous step. We also examined reference lists from other studies that are relevant in the context of the present review, such as Greiner, Law, and Brown (2015), Ostermann (2015), and Wikoff, Linhorst, and Morani (2012). In our final search strategy, we contacted several experts in risk factors for recidivism and requested published and unpublished studies that would be eligible for inclusion.
Coding of Studies
To code the studies, we developed an electronic coding form. All static and dynamic risk factors for general and violent recidivism that could be retrieved from the included studies were clustered into various “risk domains,” which are groups of risk factors that are (more or less) similar in nature. A total of 16 risk domains were created for general recidivism, whereas 11 risk domains were created for violent recidivism (see Table 1). In the analyses, the risk domains were divided into dynamic and static risk factors and analyzed separately. The dynamic risk factors are as described in Table 1, whereas the static risk factors mainly refer to historical events in a particular domain. For descriptive purposes, information was collected on the following: country where the study was conducted, type of index offense, average age of the sample, recidivism outcome measure, gender (percentage of males in samples), percentage of mentally ill offenders, and race/ethnicity (percentage of subjects belonging to the racial/ethnic majority). The measure of recidivism outcome was also included in the present study, as Andersen and Skardhamar (2017) concluded that the difference in the occurrence of rearrests, reconviction, or reimprisonment has an effect on the comparability of studies. Rearrests occur more often than reconviction, which can result in a power difference that affects the strength of effect sizes. Therefore, recidivism outcome measure, gender, and race/ethnicity were tested as potential moderators of the effect of each risk domain. The percentage of mentally ill offenders in samples could not be tested as a potential moderator because only three studies provided this information. After both the first and third author coded seven of the 27 studies independently, an overall interrater reliability was calculated for each included study. This reliability ranged from good (κ = .80) to very good (κ = 1) according to the criteria put forward by Landis and Koch (1977).
Risk Domains and Examples of Static and/or Dynamic Risk Factors Classified in Each Domain
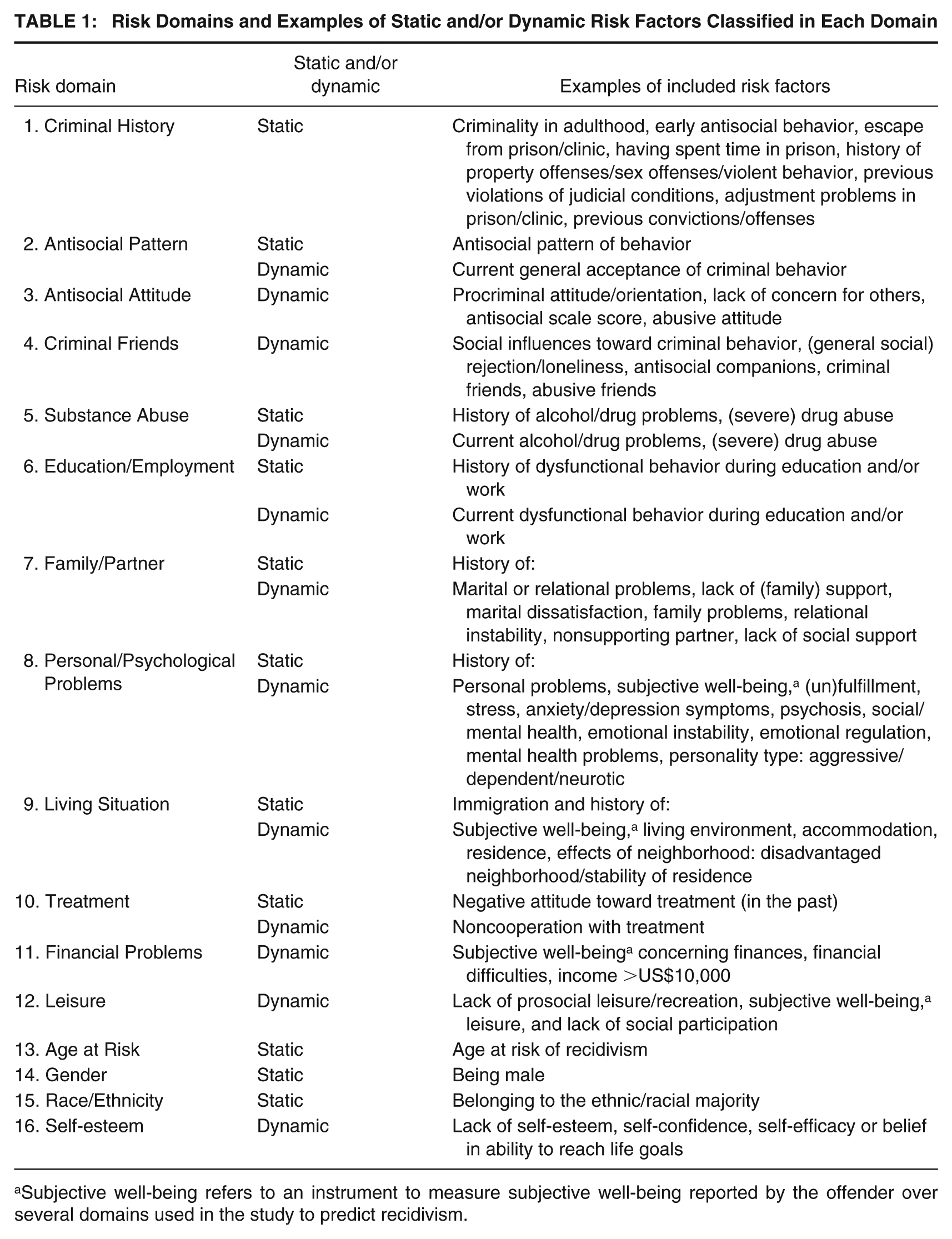
Subjective well-being refers to an instrument to measure subjective well-being reported by the offender over several domains used in the study to predict recidivism.
Statistical Analyses
Several formulas were used to transform the reported effect sizes (Cohen’s d, odds ratios, and area under the normal curve [AUC]) to Pearson’s correlation coefficients (r). The Rosenthal (1994) formula was used to transform Cohen’s d to r, whereas the Borenstein, Hedges, Higgins, and Rothstein (2009) formula was used to transform the odds ratio to Cohen’s d and the Ruscio (2008) formula was applied to transform AUC to r. Each effect size represented the relationship between a risk factor and recidivism. Effect sizes were transformed into z scores and checked for outliers to control for any disproportionate influence of outliers on the results. The standardized effect sizes all fell within the range of −3.29< z >3.29 (Tabachnik & Fidell, 2013), implying that no outliers were identified.
Most studies reported multiple effect sizes that could be classified under a single risk domain. Extracting more than one effect size from a single study violates an important assumption of meta-analysis, namely that all reported effect sizes should be independent. To deal with the dependency of effect sizes, a three-level random-effects meta-analytic model was used to analyze the combined effect sizes in each risk domain (Assink & Wibbelink, 2016). In this model, three levels of variance were accounted for: sampling variance of the observed effect sizes (Level 1), variance of effect sizes within studies (Level 2), and variance of effect sizes between studies (Level 3).
For the analyses, the “rma.mv” function of the “metafor” package (Viechtbauer, 2010) was used in the program R Studio (Version 3.2.2; R Core Team, 2015). The data set was built in SPSS version 20. For each risk domain, an overall effect was estimated in an intercept-only model. Two one-sided log-likelihood ratio tests were performed to determine whether the variance of effect sizes within studies (Level 2) and between studies (Level 3) was significant. The Level 1 variance was treated as known and calculated using the formula of Cheung (2014, p. 2015). In the event of significant variance within a risk domain, either at Level 2 or at Level 3, we proceeded with testing variables as potential moderators of the overall effect of a risk domain. For these moderator analyses, the intercept-only models were extended by including potential moderators (i.e., recidivism outcome measure, gender, and race/ethnicity) as covariates. In the moderator analysis, all categories of moderators were tested simultaneously using an omnibus test (F test). When the F test was significant, the regression coefficient (slope) of each category was tested via t test to determine the category for which the moderating effect was found. In the case of a continuous variable (moderator), the significance of the omnibus test is equal to the significance of the t test. In the case of a nonsignificant omnibus test (nonmoderating effect), it was not expected that the unexplained Level 2 and/or Level 3 variance would substantially decrease.
Bias and Sensitivity Analyses
To examine whether bias (such as publication bias; Rothstein, Sutton, & Borenstein, 2005) influenced our results, we applied the trim-and-fill method (Duval & Tweedie, 2000) using the “trimfill” function of the “metafor” package (Viechtbauer, 2010) in the program R Studio (Version 3.2.2; R Core Team, 2015). In this method, effect sizes were plotted against the standard error, and in the event that the “funnel” was asymmetric, outlying effect sizes were recoded to fit the normal distribution of effect sizes, while “missing” effect sizes were imputed to restore the symmetry of the funnel. Next, we added the “missing” effect sizes to the data set to reestimate the overall effect of each risk domain for which an asymmetric funnel plot was obtained.
Results
Twenty-seven studies were included, reporting on a total of 543 effect sizes and in which a total of 116,982 (N) unique offenders participated. Six study samples comprised only female offenders (n = 2,782, 2.4%), eight study samples comprised only male offenders (n = 5,583, 4.8%), and 13 study samples comprised both male and female offenders, of which 86.4% (n = 93,852) were men. The average age of the participants was 33.5 years (SD = 3.8, range = 20.5-40.0). Only three studies (n = 530) provided information on the mental illnesses of the offenders; therefore, the mental illnesses of participants were not tested in the moderator analyses.
Sixteen studies were conducted in the United States, seven in Canada, two in Western European countries, and two in Australia. In 16 studies, forensic outpatient treatment consisted of supervision (combined with treatment) by probationary institutes, while offenders received forensic community-based/outpatient treatment in the remaining 11 studies. The offenders received forensic outpatient treatment for any form of delinquent behavior, except sexual offending behavior, as studies of sex offenders were excluded from the present analysis. The average general recidivism rate was 35.0% (SD = 13.7, range = 16.6-62.4), while the average violent recidivism rate was 17.1% (SD = 3.1, range = 12.6-20.3). The average follow-up time was 3.8 years (SD = 2.7, range = 0.7-10.2). Average effect sizes are reported in terms of r. The criteria for interpreting these effect sizes, given a 50% base rate, are ≤.10 for a small effect, ≤.24 for a medium effect, and ≤.37 for a large effect (Rice & Harris, 2005). For base rates other than 50%, these criteria for small, medium, and large effects can be calculated using the conversion formulae (after Rosenthal, 1994) provided by Rice and Harris (2005). Using these formulae, the criteria for small, medium, and large effect sizes for a 35.0% base rate for general recidivism are .095, .232, and .357, respectively. For a 17.1% base rate for violent recidivism, these criteria are .075, .185, and .288, respectively.
Risk Domains for General Recidivism
The average effect sizes of the 13 risk domains for general recidivism were significant, implying that these risk domains were positively associated with general recidivism (see Table 2). An Antisocial Pattern of behavior correlated most strongly with general recidivism (r = .324) and showed a medium effect size. Ten out of the remaining 13 risk domains were significantly associated with general recidivism and yielded an effect that was small in size. The domain of race/ethnicity (i.e., belonging to an ethnic/racial majority) yielded a significant but very small effect size, with r = .077. When domains contained both static and dynamic risk factors and correlated significantly with general recidivism, only the dynamic risk factors contributed to a significant correlation with general recidivism. Only static risk factors in the Criminal History domain correlated significantly and moderately with general recidivism (r = .202). Table 2 provides an overview of the variance of the effect sizes within the same study (Level 2 variance) and the variance of the effect sizes between studies (Level 3 variance). When significant Level 2 and/or Level 3 variance was found within a risk domain, different variables may moderate the association between the risk domain and general recidivism.
Overall Effect Sizes (Correlations) for the Risk Domains for General Recidivism
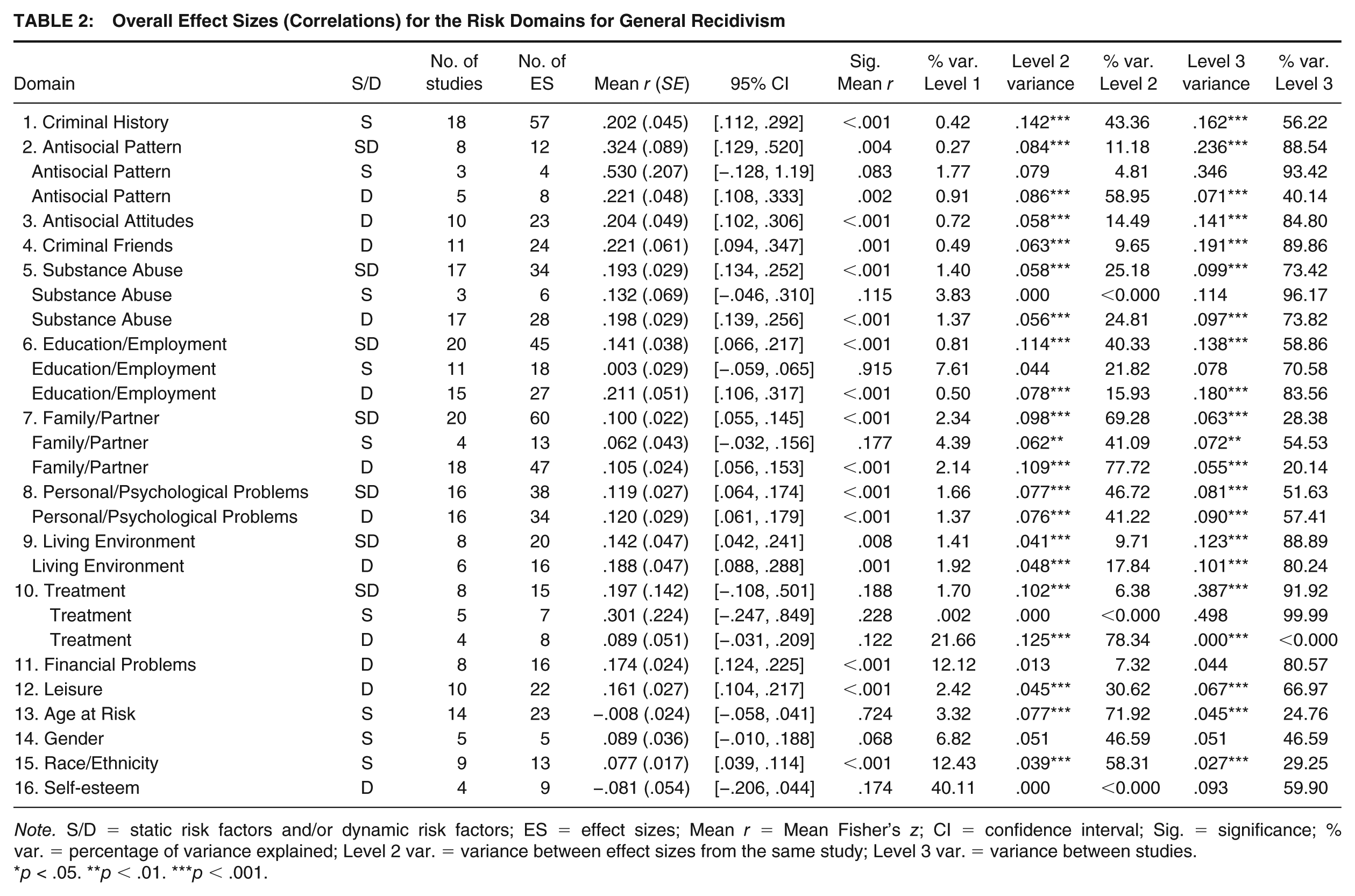
Note. S/D = static risk factors and/or dynamic risk factors; ES = effect sizes; Mean r = Mean Fisher’s z; CI = confidence interval; Sig. = significance; % var. = percentage of variance explained; Level 2 var. = variance between effect sizes from the same study; Level 3 var. = variance between studies.
p < .05. **p < .01. ***p < .001.
Risk Domains for Violent Recidivism
For violent recidivism, 11 out of the 16 risk domains were tested in the study (see Table 3). We found significant effects for the following risk domains: Criminal History, Antisocial Pattern, Antisocial Attitudes, Criminal Friends, Substance Abuse, Education/Employment, Family/Partner, Personal/Psychological Problems, Living Environment, and Leisure. We found that all risk domains except Financial Problems correlated significantly with violent recidivism, with the strongest effect being found for Antisocial Pattern (r = .27). Using the adjusted interpretation guidelines, we found a medium effect for the following risk domains on violent recidivism: Antisocial Pattern, Living Environment, Criminal History, and Education/Employment. We found a small effect for the following risk domains: Antisocial Attitudes, Criminal Friends, and Substance Abuse. For the Family/Partner domain, we found only a very small effect.
Overall Effect Sizes (Correlations) for the Risk Domains for Violent Recidivism

Note. S/D = static risk factors and/or dynamic risk factors; ES = effect sizes; Mean r = Mean Fisher’s z; CI = confidence interval; Sig. = significance; % var. = percentage of variance explained; Level 2 var. = variance between effect sizes from the same study; Level 3 var. = variance between studies.
p < .05. **p < .01. ***p < .001.
Moderators for General Recidivism
As shown in the Supplemental Material (available in the online version of this article), gender, race/ethnicity, and type of recidivism outcome (rearrest or reconviction) were tested as moderators of the effect of risk domains on general recidivism. Gender seemed to moderate the effect of static risk factors in the Family/Partner and Substance Abuse domains, as well as the effect of dynamic risk factors in the Self-esteem domain. Race/ethnicity moderated only the effect of the Treatment domain. As the percentage of the ethnic/racial majority increased in samples, the effect of the Treatment domain increased. However, after a Bonferroni adjustment (p < .002), none of the abovementioned moderating effects were upheld.
Moderators for Violent Recidivism
The moderator analyses showed that the effects of Antisocial Pattern, Antisocial Attitudes, having Criminal Friends, and lack of Education/Employment on violent recidivism were moderated by gender and race/ethnicity (see Supplemental Material). As before, after a Bonferroni adjustment (p < .004), none of the abovementioned moderating effects were upheld. Finally, type of recidivism outcome (rearrest or reconviction) did not moderate the effect of any of the examined risk domains for violent recidivism. There was no difference between general recidivism and violent recidivism in terms of the strength of the risk domains.
Publication Bias
The results of the trim-and-fill analyses are presented in the Supplemental Material. After the trim-and-fill analyses were completed, the effect of most of the risk domains became smaller, but did not change in terms of relative strength (small-to-moderate effects were found after trim and fill). However, the effects of most risk domains for violent recidivism decreased. Only the effects of Criminal Friends, Substance Abuse, and Education/Employment domains increased. Again, the relative strength of the effect sizes (small effects) did not change.
Discussion
The central aim of this multilevel meta-analytic study was to shed light on the relative strength (expressed in effect size) of risk and needs factors for the prediction of general and violent recidivism in an outpatient offender population. In general, the present findings were supportive of Bonta and Andrews’s (2017) study in which the Central Eight risk factors were related to general and violent recidivism. Breaking down the Central Eight risk domains into static and dynamic factors, the present study showed that two static risk domains, namely, Criminal History and Antisocial Pattern, were the strongest predictors of both general and violent recidivism. This finding corroborates the results of previous meta-analyses (Bonta et al., 2014; Collins, 2010; Olver et al., 2014). However, when risk domains included both static and dynamic risk factors, the dynamic risk factors were more strongly predictive of general and violent recidivism compared with the static risk factors. This was found for Substance Abuse, Education/Employment, Family/Partner, and Personal/Psychological Problems. As far as we know, this is the first study of forensic outpatients that directly compares specific static and dynamic risk factors within the same risk domain (e.g., history of substance abuse compared with current substance abuse). Previous studies targeting this issue have presented an additional predictive effect of the total score on dynamic risk factors on top of the total score on static risk factors in a subgroup of severely mentally ill offenders who had been released from mandatory inpatient treatment (De Vries Robbé et al., 2014), and despite small effects similar results were found for sexual offenders (Hanson, Helmus, & Harris, 2015; van den Berg et al., 2018). Moreover, the small effect sizes found in the meta-analysis by van den Berg and colleagues (2018), as well as in the present study, could have been the result of the fluctuating number of studies, relatively long follow-up time, and low base rates, as pointed out by Babchishin and Helmus (2016). An adjustment of the interpretation guidelines for recidivism base rates (Rice & Harris, 2005) yielded more medium effect sizes for the prediction of violent recidivism in the present study.
In the RNR model, the relevant risk domains found in the current study were labeled as dynamic, indicating that they describe the current situation and are changeable through intervention. Nonetheless, these factors become static in nature when they describe the offenders’ situation in the past. From our results, it can be concluded that it is not the dynamic risk factors per se that should be focused on in research, but rather the changes in these factors. A number of studies underline this conclusion; for instance, Pelissier, Jones, and Cadigan (2007) showed that substance abuse treatment had a positive effect on sobriety after successful completion of treatment, resulting in lower recidivism rates. Based on this new knowledge and previous studies of treatment effects among forensic (out)patients, more attention should be paid to (changes in) dynamic risk factors (Douglas & Skeem, 2005; Kraemer et al., 1997). With this in mind, substance abuse is of special interest, mainly because of its high prevalence among offenders. A study of a Dutch forensic outpatient sample showed that the prevalence of substance-related disorders was 61.5% among general violence offenders and 30.9% among intimate violence offenders (Kraanen, Scholing, & Emmelkamp, 2012). Moreover, 29.9% of these offenders had been intoxicated while committing an offense. Another Dutch study of sex offenders pointed out that substance abuse was a consistent predictor of general recidivism across age groups (Wilpert, van Horn, & Boonmann, 2018), while forensic outpatients with mental illness and substance abuse issues were found to have the highest dropout and recidivism rates compared with offenders with only substance abuse problems or other mental illnesses (van Horn, Eisenberg, Souverein, & Kraanen, 2018). Despite the high prevalence of substance abuse among the forensic outpatient population, we found only a small effect of substance abuse, in line with the findings of Bonta and Andrews (2017).
Apart from research on treatment that focuses on substance abuse, very few studies on the relationship between changes in other dynamic risk factors and recidivism have been published. In a study by Vedel, Emmelkamp, and Schippers (2008), a decrease in intimate partner violence was found in men who were continuing to abstain from substance abuse following cognitive-behavioral therapy. Howard and Dixon (2013) studied the relationship between changes in risk factors and general and violent recidivism among 196,493 English and Welsh offenders. They found that, after treatment, the total risk factor scores decreased for all offenders, although this decrease was larger among nonrecidivists. Specifically, they found the strongest relationship between changes in substance abuse and recidivism. In addition, changes in accommodation, employability, and (criminal) attitude were all significantly associated with recidivism. By contrast, changes in recognizing the impact of offending and psychiatric treatment were not associated with recidivism. Although it could be concluded from the latter finding that treatment does not effectively reduce recidivism, the item in question only refers to being in treatment and not to how actively an offender participates in treatment (e.g., motivation for treatment). Wooditch and colleagues (2014) did study the effect of being in treatment and found a risk-reducing effect of treatment that focused on changes in the dynamic risk factors, such as substance abuse, stable accommodation, employment, leisure, social support of prosocial friends, and establishing meaningful family and partner relationships.
Moderators
According to the responsivity principle of the RNR model (Bonta & Andrews, 2017), race/ethnicity and gender should be indicators used to accommodate treatment to the client’s cognitive abilities and learning style (the responsivity principle) and should also be regarded as noncriminogenic factors. However, the present results do not confirm this assumption: Gender and race/ethnicity had either no or a negligibly significant predictive value for general and violent recidivism, and no moderator effects of gender, race/ethnicity, or recidivism outcome (rearrests or reconviction) were found.
The studies in the current meta-analysis included intelligence and age as possible predictors of recidivism, but did not provide usable information on both factors to facilitate their inclusion as possible moderators. In theory, adapting treatment methods to patients’ characteristics (e.g., gender, race/ethnicity, intelligence, and age in outpatient facilities; Responsivity) should increase the effectiveness of outpatient treatment (Bonta & Andrews, 2017). However, researchers do not often include these factors as moderators in their studies. The current limited number of studies that include these moderators hinders the formulation of specific advice on responsivity in outpatient offenders as far as gender, race/ethnicity, intelligence, and age are concerned.
Limitations and Future Research
Publication bias caused by human error and the article acceptance practices of journals is a widely recognized problem in meta-analyses (Thornton & Lee, 2000). The protocoled searches and coding schemes used in this study minimized registration errors to the greatest possible extent. However, even when combined with the efforts of the authors to contact the authors of unpublished research, it is unlikely that all available research was included in this meta-analysis. Therefore, a trim-and-fill analysis was used to detect any effect of possible publication bias. The results showed minor changes in the strength of the effect sizes of the risk domains, from which it can be concluded that the results of this meta-analysis are a reliable representation of the results found until now. Despite this, the predictive validity of static and dynamic risk factors in forensic outpatients is influenced by low base rates and the small number of available studies (Babchishin & Helmus, 2016; Rice & Harris, 2005). Although the results point toward the conclusion that the effect sizes of this study underline the predictive validity of the static and dynamic risk factors, it should be noted that this is the first study to address this issue in an exclusively outpatient offender population. Hence, the present results need to be replicated in future and should be interpreted carefully for the time being.
The key results of this meta-analysis confirm the predictive value of the Central Eight risk domains for general and violent recidivism among forensic outpatients. Forensic outpatient treatment should thus focus on the dynamic risk factors of the following domains: Antisocial Pattern and Attitudes, Substance Abuse, Criminal Friends, Education/Employment, Family/Partner, Personal/Psychological Problems, Living Situation, Leisure, and Financial Problems. Future research should explore the relationship between changes in these dynamic risk factors and recidivism, along with the possible moderating effects of age, race/ethnicity, gender, and intelligence. Moreover, new meta-analysis on predictors of recidivism should be performed on the forensic residential and specified forensic outpatient subpopulations, preferably also in countries outside of Northern America.
Supplemental Material
CJB826109_Supplemental_Material_CLN – Supplemental material for Static and Dynamic Predictors of General and Violent Criminal Offense Recidivism in the Forensic Outpatient Population: A Meta-Analysis
Supplemental material, CJB826109_Supplemental_Material_CLN for Static and Dynamic Predictors of General and Violent Criminal Offense Recidivism in the Forensic Outpatient Population: A Meta-Analysis by Mara J. Eisenberg, Joan E. van Horn, Judith M. Dekker, Mark Assink, Claudia E. van der Put, Jan Hendriks and Geert Jan J. M. Stams in Criminal Justice and Behavior
Footnotes
Authors’ Note:
This work was partly funded by Dutch Kwaliteit Forensische Zorg (KFZ Call 2015-39) [Quality Forensic Care] of the Ministry of Security and Justice, The Netherlands. The Ministry of Justice had no involvement in decisions concerning the study design, data collection, analysis, and interpretation of the data, nor in the writing and publication of the report. J. M. Dekker is now at Pameijer, Rotterdam.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.