
Abstract
This study uses structural equation modeling to determine whether there are direct and indirect relationships between childhood trauma and recidivism for 230 women from two state prisons in North Carolina. The researchers obtained a random sample from all women scheduled to be released between 30 and 120 days from data collection. Findings indicated that childhood trauma was not significantly related to recidivism for this sample, but there was an indirect relationship with depression being the intervening variable accounting for the relationship between childhood trauma and recidivism. Results lend support to the importance of addressing incarcerated women’s trauma before release, while also assessing for depression and using empirically supported interventions to treat depression when applicable.
Although the national incarceration rate has declined since its peak in 2009, rates for women continue to increase compared with their male counterparts, and women comprise the fastest growing incarcerated population in the United States (Carson & Anderson, 2016). Women’s rate of incarceration has increased more than 700% in the past four decades; currently, more than 205,000 women are held in jails and prisons across the country. The War on Drugs “tough on crime” policies such as mandatory minimum sentencing structures are generally acknowledged to have fueled mass incarceration overall and to have specifically catalyzed the dramatic growth of women’s incarceration (Moore & Elkavich, 2008). Although these policies were designed to standardize sentencing outcomes, they remove the context from criminal offending behavior and obscure many of the social structures that disproportionately affect women and complicate women’s intersection with crime (Travis & Western, 2014).
Experiences of childhood trauma are hypothesized as a potent pathway to prison for many justice-involved women (e.g., Brennan, Breitenbach, Dieterich, Salisbury, & van Voorhis, 2012; Daly, 1992). In some analyses, childhood trauma (e.g., physical, sexual, and emotional abuse) is an indirect predictor of either incarceration for justice-involved women or recidivism for women on parole or probation (Salisbury & van Voorhis, 2009), with these effects often being mediated by mental health issues, substance use disorders (SUDs), and experiences of intimate partner violence (IPV). While there has been important research on pathways from childhood trauma to criminal justice involvement for women (Broidy, Payne, & Piquero, 2018; DeHart, Lynch, Belknap, Dass-Brailsford, & Green, 2014), there are no known studies examining pathways from childhood trauma to recidivism for women released from prison using mental health issues and SUDs as potential mediating variables. The current analysis extends the hypothesis that childhood trauma, mental health issues, and SUDs negatively affect justice-involved women by examining the impact of these issues on recidivism after release from prison.
The current study examines childhood trauma as a pathway to recidivism within 3 years of release among a probability sample of incarcerated women released from state prison. Structural equation modeling (SEM) was used to estimate the direct and mediated effects between childhood trauma and recidivism in the context of a range of covariates that have been linked to recidivism in other samples. Little is known about pathways to recidivism for incarcerated women, and whether experiences of childhood trauma, along with mental health issues and SUDs, affect recidivism rates. Understanding the influence of childhood trauma, mental health issues, and SUDs on recidivism may help prison mental health workers use validated trauma and behavioral health assessments to more accurately determine a woman’s risk for recidivism if research indicates there is a positive relationship. Understanding the context of incarcerated women’s experiences prior to coming to prison could direct the use of empirically supported, individualized intervention and treatment approaches to decrease mental health and SUD symptomatology, increase coping and well-being, and ultimately decrease the risk for reincarceration after release. Specifically, prisons could integrate universal trauma, mental health, and SUD screenings and create policies implementing individualized care within a trauma-informed care paradigm.
The Long Reach of Childhood Trauma for Incarcerated Women
The overwhelming majority of incarcerated women (approximately 80%) report experiences of interpersonal violence across the lifespan (Bloom, Owen, & Covington, 2004; Komarovskaya, Loper, Warren, & Jackson, 2011). Between 65% and 75% of incarcerated women report having experienced some form of interpersonal childhood trauma (Carlson, Shafer, & Duffee, 2010; Cook, Smith, Tusher, & Raiford, 2005; Kennedy, Tripodi, Pettus-Davis, & Ayers, 2016). Specifically, more than 57% of incarcerated women report having experienced childhood physical abuse (CPA), approximately 55% of women report childhood sexual abuse (CSA), and roughly three quarters of women report experiences of childhood emotional abuse (CEA; Cook et al., 2005; Renn et al., 2017). While rates of lifetime traumatic experiences are similar for incarcerated men and women, incarcerated women report higher rates of childhood victimization compared with their male counterparts, and they have significantly higher rates of lifetime traumatic experiences than nonincarcerated women. Recent research has assessed unique pathways to the criminal justice system for women.
The Gendered Pathways Perspective (GPP) emerged in the last decades of the 20th century to describe and explain women’s criminal offending behavior (e.g., Daly, 1992; Owen, 1998; Richie, 1996). The GPP addresses the unique social and psychological realities of women and identifies common pathways to describe women’s intersection with the criminal justice system. Overall, Salisbury and van Voorhis (2009) suggested that results from GPP research indicate that women engage in criminal offending behavior based on factors which are (a) not typically seen among male offender populations (e.g., prostitution, IPV, and coercion); (b) more prevalent among female offender populations (e.g., CSA); or (c) common among both male and female offender populations, but have distinctly gendered effects for women (e.g., drug use, intimate relationships, poverty, and economic marginalization; Belknap & Holsinger, 2006; Bloom, Owen, & Covington, 2006). These factors underscore how women’s criminal behavior can be viewed as survival of both victimization and poverty (DeHart et al., 2014; Kennedy & Mennicke, 2017).
Experiences of childhood trauma (i.e., CPA, CSA, and CEA) increase the risk for a range of negative mental health, substance use, criminological, and adult victimization outcomes (Golder, Engstrom, Hall, Higgins, & Logan, 2015; Golder et al., 2014; Johnson & Lynch, 2013; Kennedy, Mennicke, Feely, & Tripodi, 2018). Regardless of how childhood trauma is conceptually and operationally defined (e.g., singular experiences of CSA, or cumulative experiences of multi- or poly-victimization), it is significantly associated with a range of mental health issues from anxiety disorders (Lindert et al., 2014), to depression (Lindert et al., 2014), to hallucinations and psychosis (Marwaha & Bebbington, 2015). These associations are amplified for incarcerated women, and estimates suggest that nearly 74% of incarcerated women meet criteria for one or more psychiatric disorders with anxiety, depression, posttraumatic stress, and psychosis being the most prevalent (Kennedy et al., 2016). Analyzing the role of anxiety, depression, and psychosis as potential variables mediating the relationship between child abuse and recidivism for women released from prison is important because literature indicates that these mental health variables are significantly associated with childhood trauma (Golder et al., 2015; Huebner, DeJong, & Cobbina, 2010; Kennedy, Tripodi, & Pettus-Davis, 2013), they disproportionately affect incarcerated women when compared with the general population (Stanton, Kako, & Sawin, 2016), and, in some cases, they directly predict recidivism (Mallik-Kane & Visher, 2008). Understanding how anxiety, depression, and psychosis intersect with childhood trauma and affect the risk for recidivism after release will guide the implementation of empirically supported interventions in the prison setting to reduce the negative impact of symptoms on women’s lives and improve their success after release.
Experiencing childhood trauma increases the risk for developing an SUD and being arrested for drug-related crimes (DeHart et al., 2014). Incarcerated women who self-report experiences of childhood trauma are significantly more likely to meet criteria for a SUD when compared with women with no history of abuse (Kennedy et al., 2016; Tripodi & Pettus-Davis, 2013). Increased frequency and severity of childhood trauma significantly elevates the odds of current drug use among incarcerated women, which may indicate a cumulative relationship between experiences of abuse and problematic substance use as coping mechanisms (Fuentes, 2014; Holtfreter & Wattanaporn, 2013; Huebner et al., 2010).
Taken together, experiences of childhood trauma, mental health issues, and drug use all increase risk for experiencing IPV within adolescent and adult intimate relationships (Carlson & Shafer, 2010; Zust, 2009). Qualitative investigations of incarcerated women’s experiences of abuse across the lifespan indicate that early abuse alienates women from school, employment, and family, which increases their reliance on peers and intimate partners who engage in crime or use substances or violence in their relationships (DeHart, 2008; Fuentes, 2014). Economic marginalization and lack of family support often exposes incarcerated women to poverty and homelessness, which complicates their relationships and needs upon reentry after release from prison and may constrain their choice to remain with a violent partner (Zust, 2009).
Women’s Criminal Recidivism
Although childhood trauma has been identified as a prominent pathway to prison for some women, the relationship between childhood trauma and recidivism for women released from prison is less clear. Based on the extensive GPP literature base, it is important to consider whether the same pathways lead to recidivism for a sample of incarcerated women to provide effective and individualized interventions before release. We anticipate that the identified pathways to prison (i.e., childhood trauma, mental health issues, SUDs, and IPV) will be replicated when examining pathways to recidivism. This hypothesis is grounded on research suggesting that childhood trauma, mental health issues, and SUDs are highly prevalent among incarcerated women (Kennedy et al., 2016; Lindert et al., 2014; Marwaha & Bebbington, 2015). Furthermore, the presence of mental health issues (Holtfreter & Wattanaporn, 2013) and SUDs (Huebner et al., 2010; Mallik-Kane & Visher, 2008) strongly predict recidivism. Multistate recidivism analyses suggest that 58% of incarcerated women are rearrested, 38% are reconvicted, and 30% are reincarcerated within 3 years of release from prison (Deschenes, Owen, & Crow, 2007). Direct tests of the relationship between childhood trauma and criminological outcomes (e.g., incarceration, recidivism, or probation failure) are uncommon, and the results from existing analyses are mixed (Gehring, 2016; Salisbury & van Voorhis, 2009). It is currently unknown whether women released from prison who have experienced childhood trauma are more likely to return to prison than women in prison who have not, and if so, whether these relationships are mediated by mental health issues and/or SUDs.
The purpose of this study is to empirically test the influence of childhood trauma on reincarceration for women released from one of two state prisons in North Carolina. Although several path analyses have examined pathways to incarceration for women on probation and parole (e.g., Brennan et al., 2012; Gehring, 2016; Salisbury & van Voorhis, 2009), there is a dearth of research that specifically examines the relationship between childhood trauma and recidivism for incarcerated women after release from prison. Findings from the current analysis will contribute to the GPP theoretical literature by exploring the gendered-factors that increase women’s risk for recidivism after release from prison. Better understanding women’s pathways to recidivism may direct policy and practice innovations to address the unmet needs of this vulnerable population.
To fill this gap in the literature, we used SEM to assess the potency of childhood trauma as a predictor of the 3-year recidivism rate for a probability sample of incarcerated women. Using this analytic technique allowed us to consider the relationship between childhood trauma and recidivism in the context of anxiety, depression, psychosis, SUDs, and IPV (physical, sexual, and psychological victimization), and other demographic and criminological factors known to influence recidivism. Specifically, we sought to answer the following research questions:
Method
Participants and Procedures
A probability sample of 230 incarcerated women was obtained from the census of all women housed at two state prisons in North Carolina. One of the prisons contained all security levels and housed just over 1,300 women; the other was a minimum-security prison that housed approximately 200 women. The sample was randomly selected using a sampling frame of all eligible women in the two prisons who had a scheduled released date within 30 to 120 days from the date of interview, and then the research team narrowed the sampling frame by conducting stratified random sampling based on the women’s home county in North Carolina. Data collection occurred in six intervals from December 2010 to June 2012. Research team members obtained data from the participants by interviewing them, reading questions from the scales and measures aloud, and circling or writing down their responses. All research procedures were reviewed and approved by Florida State University, University of North Carolina, and the North Carolina Department of Correction (now the North Carolina Division of Adult Correction and Juvenile Justice within the North Carolina Department of Public Safety).
Eligible participants were at least 18 years old, able to speak English, and cognitively functioning to the degree that they were able to provide informed consent and indicate that they understood the nature of the study and what being a participant entailed. Overall, 277 women were asked to participate in the study and 230 provided informed consent and joined the study, an 83% response rate. In all, 149 participants were recruited from the larger prison (minimum-, medium-, and maximum-security level); 81 women were recruited from the smaller prison (minimum-security level). There were no statistically significant differences between women recruited from the two prisons on any of the variable included in this study.
Women in the sample were, on average, 33.7 years old (SD = 9.9). Just over 54% of the participants identified as White/Caucasian, 40% of women identified as Black/African American, 2.6% identified as Hispanic/Latina, 1.7% of women identified as Native American, and less than half a percent identified as Asian/Pacific Islander. The racial makeup of the sample is descriptively similar to the larger population of women held in state prisons in North Carolina. The mean length of the index incarceration (when women were interviewed) was 20.8 months (SD = 25.5). On average, women had two felony convictions which occurred prior to the index incarceration (SD = 2.3, range = 0-15).
The majority of women self-reported experiences of child abuse. Approximately 40% of women in the sample had experienced CPA, approximately 46% had experienced CSA, and approximately 83% had experienced CEA. A majority of the women interviewed were identified with one or more of the three mental health issues measured. Just over 60% of women met criteria for a current anxiety disorder and nearly 75% of women met criteria for current depression. More than 37% of women had experienced at least one symptom of psychosis in their lifetime, and 19% of women were currently experiencing at least one symptom of psychosis. In addition to mental health issues, more than 75% of the women interviewed met criteria for a SUD in the year prior to the index incarceration.
Measures
Independent Variables
Childhood trauma was assessed with a 20-item version of the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994). The CTQ measured abuse and neglect on five subdomains: physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect. Participants were asked about the frequency of childhood abuse experiences (birth through age 18) on a 5-point Likert-type scale (0 = never true, 1 = rarely true, 2 = sometimes true, 3 = often true, 4 = very often true). Mean frequency scores for each of the three abuse subdomains (i.e., physical, sexual, and emotional) were computed; neglect items were not included in the current analysis. The CPA subdomain included items like “I got hit so hard by people in my family that I had to see a doctor or go to a hospital”; CSA items included “Someone tried to touch me in a sexual way, or tried to make me touch them” and “Someone molested me”; and CEA items included “People in my family called me things like stupid, lazy, or ugly.” The short form version of the CTQ was validated among four large and varied independent samples; the five-factor solution was supported with excellent model fit (Bernstein et al., 2003). The measure demonstrated strong internal consistency among the pooled samples, and the subscale alphas ranged from adequate (α = .70) to excellent (α = .94). For this study, the global CTQ had high internal consistency (α = .94); the subscales ranged from good (α = .85) to excellent (α = .97).
Potential Mediating Variables
Mental health issues
The Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) was used to determine the presence of three mental health issues: anxiety, depression, and psychosis. The MINI assesses for 23 Axis 1 diagnoses consistent with the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). The MINI was found to be reliable and valid when compared with the Composite International Diagnostic Interview (CIDI) and the International Statistical Classification of Disease–10 (ICD-10) (Sheehan et al., 1997). Only the Anxiety, Depression, and Psychosis subscales were used for the current analysis. The MINI uses a dichotomous yes/no response option where the first question assesses the presence of a lifetime mental health symptom and a follow-up question establishes whether the respondent is currently experiencing that symptom. A dichotomous variable (0 = no, 1 = yes) was created for each of the three mental health issues to represent the presence of current (past 30 days) anxiety, depression, and psychosis. MINI scoring instructions were followed to identify whether participants met criteria for a current anxiety disorder (anxiety) and major depression (depression), and had experienced any current symptoms of psychosis (psychosis). Anxiety, depression, and psychosis were included in this study as potential mediating variables because research indicates women in prison who experience higher frequencies of childhood victimization are more likely to experience these mental health symptoms. Understanding if they help predict recidivism will potentially help develop correctional-based programming based on individualized needs.
SUDs
The presence of a SUD in the year prior to the index incarceration was assessed using the Substance Abuse Module (SAM; Cottler, Robins, & Helzer, 1989). The SAM is a 38-item measure which screens for the presence of substance use using DSM-IV criteria to establish the presence of any alcohol abuse, alcohol dependence, drug abuse, or drug dependence. The reported reliability kappa values range from .82 to .84 (Cottler et al., 1989). For the current study, women were instructed to reflect on the year prior to the index incarceration when responding to items. A dichotomous variable (0 = no, 1 = yes) was created to represent the presence of any SUD in the year prior to the index incarceration. Participants were identified as having met criteria for a SUD if they met the criteria for alcohol abuse, alcohol dependence, drug abuse, or drug dependence.
IPV
Physical, sexual, and psychological IPV experienced in the year prior to the index incarceration were measured using the Abuse Behavior Inventory (ABI; Shepard & Campbell, 1992). Physical IPV (six items) items included hitting, strangling, and attacking with a weapon; sexual IPV (three items) included coerced and forced sex; and psychological IPV (20 items) included controlling behaviors, put downs, and name-calling. All items were measured using a 5-point frequency scale (0 = never, 1 = rarely, 2 = occasionally, 3 = frequently, 4 = very frequently). Initial validation was conducted with a sample of 78 female victims and 100 male abusers; preliminary psychometrics were strong (Shepard & Campbell, 1992). Zink, Klesges, Levin, and Putnam (2007) revalidated the measure with 392 women drawn from primary care settings. Analyses indicated strong internal reliability (global α = .92) and high concordance with established measures. Furthermore, additional testing conducted by Postmus, Stylianou, and McMahon (2016) supported the stability and validity of a distinct three-item Sexual Violence subscale (α = .85) embedded within the physical IPV domain. We replicated this method for current analyses. The measure demonstrated excellent psychometric properties in the current sample: Global α = .97, Physical IPV subscale α = .93, Sexual IPV subscale α = .93, and Psychological IPV subscale α = .96. A dichotomous variable (0 = no, 1 = yes) was created for each of the three IPV subdomains to represent presence of any physical IPV, sexual IPV, or psychological IPV in the year prior to the index incarceration.
Dependent Variable
Recidivism is defined as whether the participant was reincarcerated at a North Carolina state prison within 3 years of release from the index incarceration. This includes reincarceration stemming from the commission of new crimes or for violating the terms of a community supervision condition. Administrative data were obtained from the North Carolina Department of Public Safety. The 3-year reincarceration rate for this sample was 17.8%. The mean time from release to reincarceration for those participants who were reincarcerated was 665 days.
Demographic and Criminological Covariates
The research team controlled for three variables associated with increased recidivism. These variables are age at time of release from prison, race time since release from prison, and number of prior felony convictions. Age at time of release was operationalized in years.
Race
Due to the relatively homogeneous racial identities of women in the sample (94% of the sample identified as White/Caucasian or Black/African Americans), a dichotomous variable identified women as White or belonging to any non-White racial minority group (0 = White, 1 = non-White minority). Research team members asked participants to identify their race.
Time since release from prison
Time since release from prison was operationalized as the number of days that elapsed between the official release date and the date when data were collected on recidivism. These data were gathered from the state administrative database provided by the North Carolina Department of Public Safety.
Number of previous felony convictions
The number of total previous felony convictions in the state of North Carolina prior to the index incarceration was counted, regardless of whether those felony convictions resulted in one or more episodes of probation or incarceration. Felony convictions associated with the index incarceration were not included in this variable. The number of previous felony convictions for each research participant was also gathered from the state administrative database provided by the North Carolina Department of Public Safety.
Data Analysis
Descriptive statistics of, and correlational analyses between, key constructs were conducted using SPSS, version 22. Table 1 contains descriptive information for participant demographics and variables in the model. To test the effects of childhood trauma, we used SEM in Mplus 5.21 (Muthén & Muthén, 2015). We conceptualized childhood trauma as physical, sexual, and emotional abuse and used a latent variable in model; all other variables were observed. A measurement model was needed to establish adequate model–data fit for latent variables. The latent variable is saturated because childhood trauma is a three-factor latent variable (Kline, 2011). To evaluate model–data fit, we used the full model with the latent variable of childhood trauma as well as observed variables. Model fit was established using a chi-square (χ2) goodness of fit test, with nonstatistically significant results indicating good model fit. Other fit indices were examined, including the comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square of approximation (RMSEA), and the standardized root mean square residual (SRMR). Good model fit on these additional indices is suggested by established critical values. The critical value for the CFI and TLI is .90, with values above .95 representing excellent fit; the RMSEA must be at or below .08 to demonstrate acceptable fit, with values below .05 preferred; and for the SRMR, a value of less than .10 is acceptable (Hu & Bentler, 1999; Kline, 2011). To evaluate the mediating effect from childhood trauma to recidivism through mental health variables and interpersonal violence, we used bootstrapping procedures using 95% bias-corrected bootstrap confidence intervals (CIs) based on 15,000 bootstrap samples.
Characteristics of the Sample
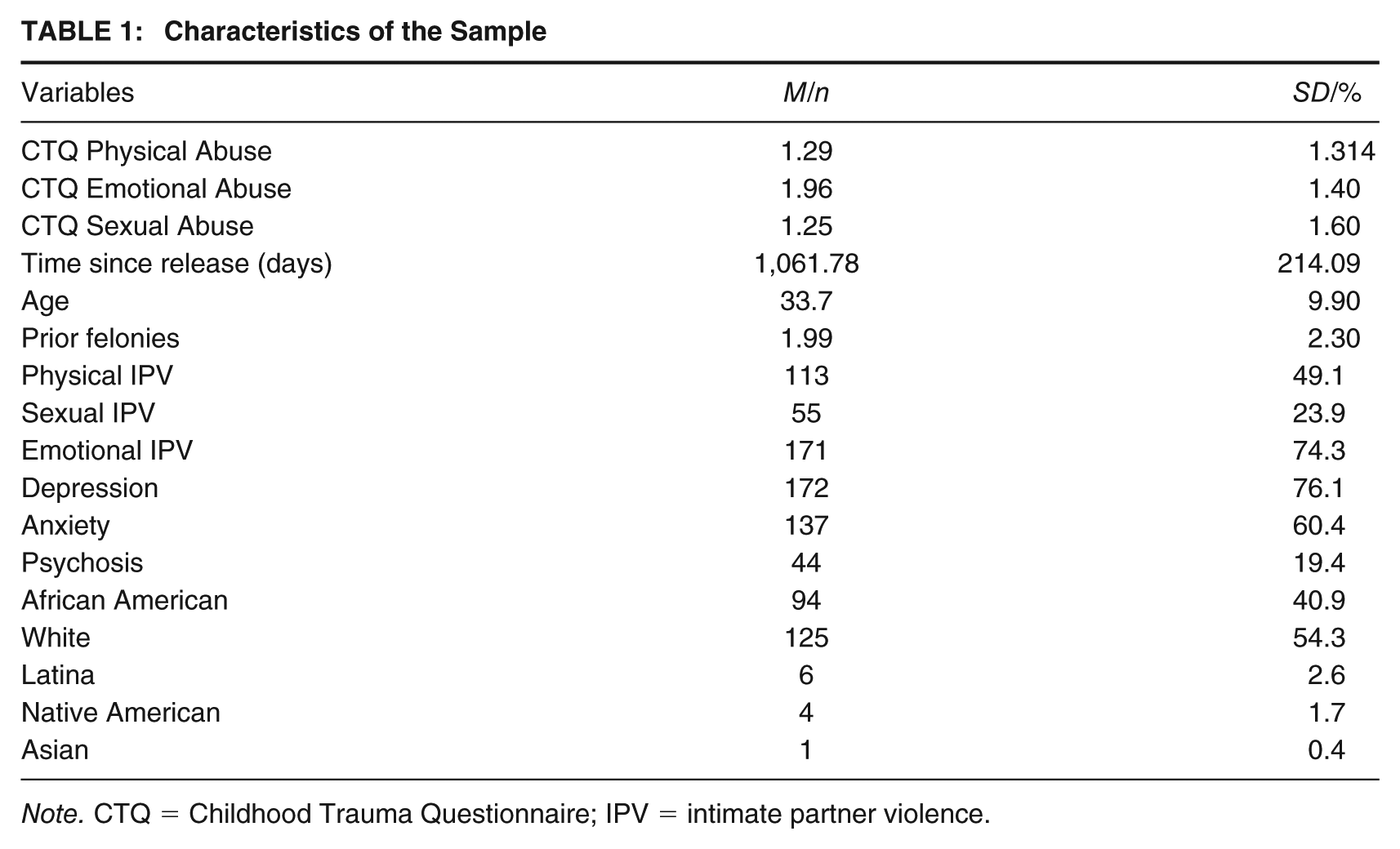
Note. CTQ = Childhood Trauma Questionnaire; IPV = intimate partner violence.
Missing data were examined prior to conducting inferential analyses. Levels of missing data were relatively low (up to 6%) on self-reported variables. Administrative data had no missing values. It is important to address missing data to maximize statistical power and minimize biased parameter estimates. Although higher proportions of missing data are associated with reduced quality of statistical inferences (e.g., Little, Jorgensen, Lang, & Moore, 2014), scholars suggest that such bias is ameliorable even when missingness nears 80%. Reducing this bias instead depends on the mechanism of the missing data and application of the appropriate missing data treatment (Little et al., 2014). Therefore, rather than excluding cases with missing values from the analyses, missing values were replaced using full information maximum likelihood methods (Muthén & Muthén, 2015). This is the preferred method given the overall low prevalence of missing values and the types of variables included in the analysis (Schafer & Graham, 2002).
Results
Correlation Analyses
An intercorrelation matrix is presented in Table 2. Of note, CPA, CSA, and CEA are all significantly correlated with one another, they are correlated with the mental health variables with the exception of CEA and depression, and they are not correlated with recidivism. Meeting the criteria for a SUD is correlated with CPA and CSA, but not correlated with reincarceration. Depression correlated with the majority of other variables, including psychosis, SUDs, physical IPV, sexual IPV, and race. The correlation between depression and reincarceration was noticeable, but not significant with an alpha level of .05 (p = .06). Reincarceration is significantly correlated with number of previous felonies and age.
Correlation Matrix for Observed Variables
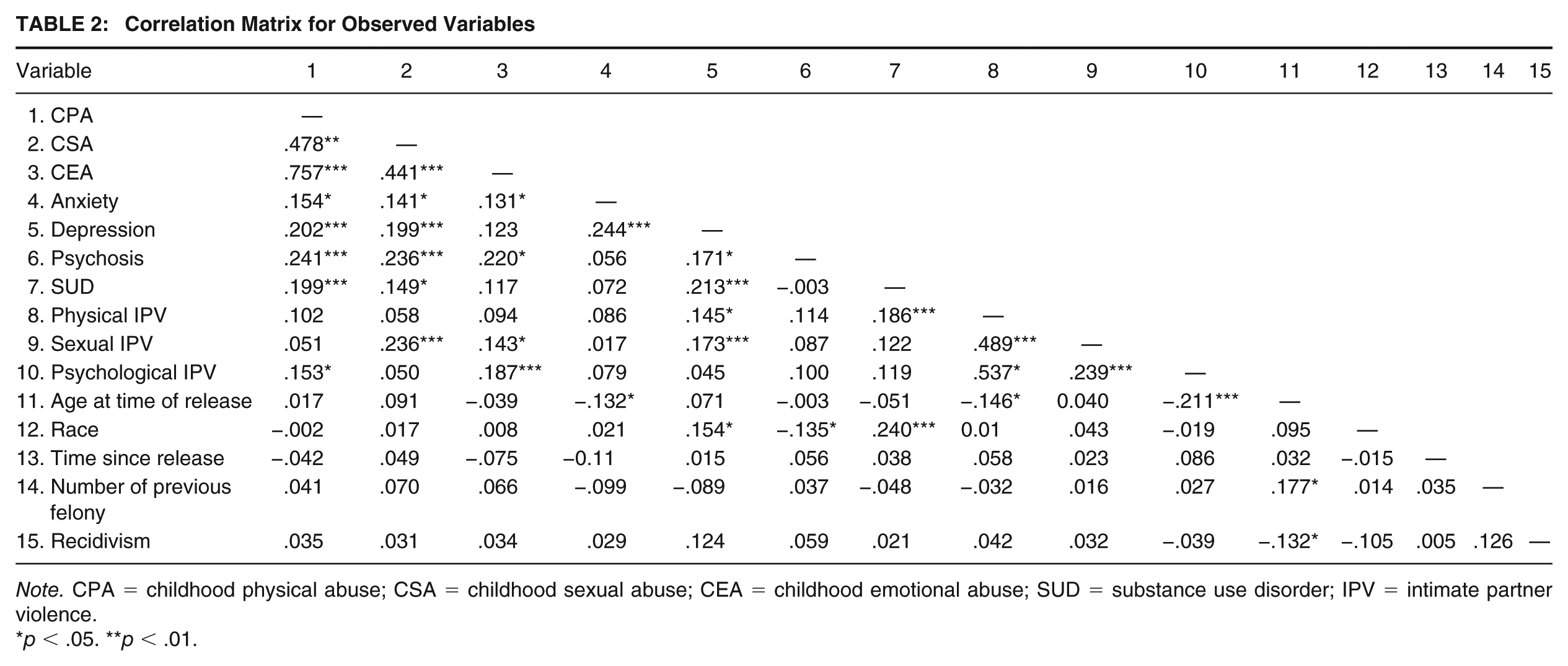
Note. CPA = childhood physical abuse; CSA = childhood sexual abuse; CEA = childhood emotional abuse; SUD = substance use disorder; IPV = intimate partner violence.
p < .05. **p < .01.
SEM
We used SEM to test the associations between childhood trauma, mental health, IPV, and recidivism. Childhood trauma was created using a latent variable with physical, sexual, and emotional trauma as indicators. Loadings of the three indicators to the childhood trauma latent variable were .61 for CPA, .54 for CSA, and .61 for CEA.
Our final model (see Figure 1) was used to estimate paths from the childhood trauma latent variable to the three observed mental health variables (i.e., anxiety, depression, and psychosis), the observed substance use variable (i.e., year prior to incarceration SUD), IPV (physical, sexual, and psychological), and the observed recidivism variable (i.e., reincarceration). We correlated error terms between physical IPV and both emotional and sexual IPV, as well as error terms between depression and SUD. Additional paths were estimated from the mental health, substance use, and IPV variables to reincarceration. Likewise, the effects of the four control variables (i.e., age at time of release, race, time since release from prison, and number of previous felony convictions) were also estimated to assess their effects on reincarceration. The model was constructed to allow for testing of both the direct and indirect effects linking childhood trauma to recidivism. The final model demonstrated excellent model–data fit. The χ2(60) = 90.136 value was not statistically significant (p = .073). Both the CFI and TLI values exceeded the critical value of .90 (CFI = .957; TLI = .935), with the CFI value indicating excellent fit (>.95). Likewise, the RMSEA value was .05, below the critical value of .08 and equal to the preferred value. Guidelines outlined by Kline (2011) indicate the ratio of observed variables to sample size should be above 10:1. The ratio of observed variables to sample size for this model is 15:1, suggesting adequate statistical power.
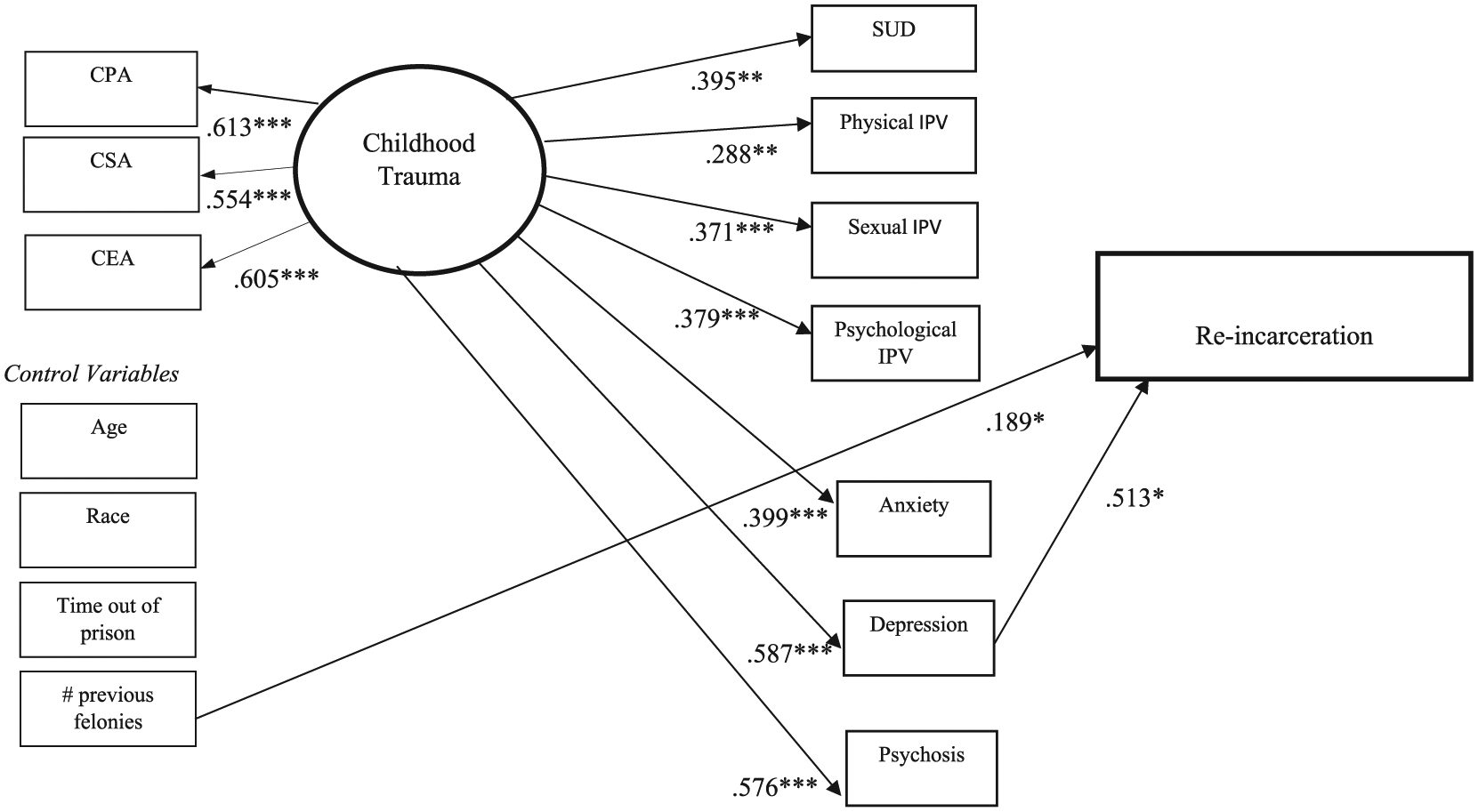
Model Examining Indirect Effects of Childhood Trauma on Reincarceration Through Substance Use, Mental Health, and IPV
The standardized parameter estimates are presented in Figure 1. The latent child abuse variable was significantly associated with the three mental health variables, substance use, and IPV. Specifically, childhood trauma was associated with meeting criteria for anxiety (β = .40, p = .001), depression (β = .59, p = .001), psychosis (β = .58, p = .001), and SUD (β = .36, p = .001) in the year prior to the index incarceration. Childhood trauma was also associated with physical IPV (β = .288, p = .001), sexual IPV (β = .371, p = .001), and psychological IPV (β = .399, p = .001).
We also tested the indirect (mediating) effects of victimization in adulthood, mental health, and SUD linking childhood trauma to recidivism. Childhood trauma had a significant, indirect effect on reincarceration through depression (β = .301, 95% CI = [.019, .582]) such that women who experienced greater childhood trauma were more likely to meet criteria for depression and those who met criteria for depression were more likely to be reincarcerated within the 3-year follow-up window. We found that other mental health diagnoses such as psychosis (β = .033, 95% CI = [−.181, .248]) and anxiety (β = .022, 95% CI = [−.091, .135]) did not significantly mediate childhood trauma and reincarceration. Indirect effects of adults’ IPV including psychological (β = −.07, 95% CI = [−.333, .193]), sexual (β = −.04, 95% CI = [−.276, .195]), and physical (β = .058, 95% CI = [−.214, .331]) were also not significant. Finally, we tested SUD as a mediating variable, and it was also not significantly associated with reincarceration (β = −.017, 95% CI = [−.133, .121]). The structural model accounted for 21.4% of the total variance in reincarceration (R2 = .24)
Discussion
Results indicate that experiences of CPA, CSA, and CEA intersect with both criminal offending and mental health issues, amplifying the risk of recidivism for abused women who met criteria for current depression. Although direct effects between childhood trauma and reincarceration were not identified in the current analysis among this sample of incarcerated women, the indirect pathway of childhood trauma to reincarceration through depression is noteworthy. Previous research analyzing women’s pathways to prison suggests that child abuse often leads to mental health issues and SUDs (DeHart, 2008; Golder et al., 2014), which creates and complicates women’s criminal offending behavior and ultimately culminates in arrest and conviction. For women under community supervision, this pathway also leads to subsequent arrest and incarceration (Salisbury & van Voorhis, 2009). Higher frequency child abuse has also been found to be associated with earlier onset of criminal behavior, chronic offending, and both violent and property offenses (Broidy et al., 2018). Results from the current analysis contribute to GPP literature by identifying depression as a potent mediator of the relationship between childhood trauma and recidivism. Understanding the significant relationships between childhood trauma, adult IPV, and both mental health and SUDs along with recognizing the association between depression and recidivism has important practice and policy implications.
This finding provides support for the growing impetus to design, implement, and assess gender-responsive and trauma-informed interventions within the prison milieu, with an emphasis on assessing participants for depression and intervening when applicable (e.g., Kubiak, Kim, Fedock, & Bybee, 2015; Saxena, Messina, & Grella, 2014; Tripodi, Mennicke, McCarter, & Ropes, 2019; Wolff, Frueh, Shi, & Schumann, 2012). Gender-responsive interventions for women in prison are generally trauma-informed and developed to address pathways to prison that disproportionately affect women, such as elevated rates of child abuse in general and sexual abuse in particular (Bloom et al., 2006; Gobeil, Blanchette, & Stewart, 2016; Holtfreter & Wattanaporn, 2013). Women who participate in gender-responsive and trauma-informed interventions often report significant decreases in mental health symptoms (e.g., depression and posttraumatic stress), anger and in-prison behavioral infractions, and sometimes recidivism after release (Gobeil et al., 2016; Tripodi, Bledsoe, Kim, & Bender, 2011). In fact, Gobeil et al. (2016) found that women who participated in correctional interventions were between 22% and 35% more likely to remain out of the criminal justice system after release, and that gender-responsive and trauma-informed programming had a greater effect on success than nongender-responsive programming. Scholars have previously suggested that people released from prison with mental health issues are more likely to be reincarcerated than those without mental health issues (Huebner et al., 2010; Skeem, Manchak, & Peterson, 2011). For the current sample, meeting criteria for current depression predicted recidivism, although current anxiety, psychosis, or SUD did not. Extant literature, however, suggests that SUD (Huebner et al., 2010) and psychosis (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009) are associated with recidivism.
Results from the current study support the development and implementation of additional gender-responsive and trauma-informed interventions in prisons to address incarcerated women’s disproportionate experiences of childhood trauma and subsequent mental health and SUDs, and to help break the cycle of incarceration and reincarceration among this population. Specifically, our results suggest that focusing on the connection between childhood trauma, depression, and criminal offending behavior may help incarcerated women improve coping and well-being, and ultimately reduce their risk for reincarceration after release.
If future studies find similar results, correctional-based mental health workers should consider assessing women in prison for trauma and related mental health issues with a specific focus on depression. Furthermore, treatment for depression could then be integrated into gender-responsive and trauma-informed interventions when applicable. Numerous empirically supported interventions have demonstrated success in addressing trauma as a means to reduce experiences of depression. These interventions include Eye Movement Desensitization and Reprocessing (Shapiro & Laliotis, 2015), Skills Training in Affect and Interpersonal Regulation Narrative Story Telling (Cloitre, Garvert, & Weiss, 2017), and Cognitive Processing Therapy (Williams, Galovski, Kattar, & Resick, 2011), all of which have been shown to be trauma-informed, effective, and efficacious treatments for depression. Future research should examine how to translate these interventions into the prison setting.
One primary strength of this study is its use of probability sampling. The research team had access to a sampling frame of all women at the two participating prisons who were between 30 and 120 days from release at the time of data collection. The researchers used stratified random sampling—sampling by county to which they are being released—to obtain the sample. Considering the 83% response rate and use of probability sampling, the research team is comfortable generalizing results from the sample to all women close to release from the two participating prisons. A second strength is the study’s assessment of both direct and indirect effects of child trauma on recidivism for women released from prison. Although the direct analysis indicated no statistically significant relationship between child trauma and recidivism for this sample, the model showed an indirect relationship between child trauma and recidivism through depression, which enabled the researchers to recognize the potential importance of screening women in prison for depression and integrating empirically supported interventions for depression into trauma-informed care programs when necessary if future studies replicate our findings. A third strength is that women were screened for mental health issues close to release rather than when admitted to prison, providing a more accurate analysis on the influence of mental health on recidivism.
One limitation to this study is the relatively small sample size, especially when considering the unexpectedly low 17.8% recidivism rate. Only 41 women in the sample were reincarcerated within 3 years. In contrast, Huebner et al. (2010) reported an 8-year women’s recidivism rate of 47%, with the overwhelming majority of recidivism (87%) occurring within 3 years after release. Using a larger sample size may result in higher rates of recidivism and the relationships between core constructs here may not be replicated. For example, the nonsignificant relationship between SUDs and reincarceration in the current analysis runs contrary to nearly every prior study assessing this relationship. It is possible that this surprising finding is a result of the low 17.8% recidivism rate and the lack of variability in the SUD data; 75% of the sample met the criteria for a SUD. In addition, we only had data on whether the participants were reincarcerated to a state prison in North Carolina. Recidivism rates may have been higher if we knew whether individuals were reincarcerated to other prisons or to county jails. A second limitation concerns measurement. Participants were retrospectively asked to recall whether they experienced childhood trauma by answering questions from the CTQ. It is possible that some of the participants misremembered aspects of their childhood. In addition, there is a possibility of social desirability bias because a member of the research team read questions from the measurement out loud to the participants and circled the participants’ responses in front of them. A third limitation is that the research team did not have access to validated risk assessments for the participants, prohibiting the ability to control for risk for recidivism with multiple variables associated with recidivism. Future research analyzing the pathways to recidivism should obtain validated risk assessments and control for these risks. Finally, we have no data on women’s lives postrelease, and therefore, we cannot speak to events that may have occurred which affected their mental health in general, and specifically their experience of depression and how that intersected with reincarceration. In addition, we were unable to control for postrelease changes in substance use, IPV, parenting or marital status, education, and employment—all of which have a documented relationship with recidivism.
Conclusion
The results of this study contribute to the GPP literature by analyzing pathways from childhood trauma to recidivism for a sample of incarcerated women, and support gender-responsive programming in prisons because of the influence of child abuse on mental health, SUDs, and adult victimization, and indirectly on recidivism with depression as the intervening variable. Gender-responsive programming is becoming more prevalent in women’s prison because of the recognition that women in prison have disproportionate levels of child abuse that is associated with mental health and SUDs. Results from this study not only support the continued growth of gender-responsive programs but also suggest the importance of using validated measures to assess for depression and to integrate empirically supported interventions to address depression with gender-responsive and trauma-informed programs.
Footnotes
Authors’ Note:
Special thanks to the North Carolina Division of Prisons, and both the administration and staff at the two prisons where data collection took place. This study was supported by a grant from the National Institute of Mental Health (Grant P30 MH079920).