
Abstract
This study aimed to characterize lifetime criminal involvement among homeless people with mental illness in Canada (N = 1,682). A latent profile analysis yielded five classes. Most participants fell within the Fewer Needs (75.5%) group, characterized by less complex psychosocial histories and few criminal charges. Participants with Extensive Criminogenic Needs (5.0%) and Acute and Extensive Criminogenic Needs (5.0%) had more charges for justice administration, violent, and mischief/public order offenses and were more likely to have been charged before their first homelessness episode. Participants with Needs Associated with Homelessness (10.6%) and Needs Associated with Drugs (3.8%) were similar, although the former had the longest history of homelessness and the latter had more drug-related charges and were most likely to have drug use disorder. This typology, which sheds light on the cumulative needs associated with different patterns of lifetime criminal involvement among homeless people with mental illness, could guide prevention initiatives and intervention strategies.
Homeless adults with mental illness are overrepresented in the criminal justice system (for a review, see Roy et al., 2014). People with mental illness are at increased risk of criminal justice involvement (Fazel et al., 2016; Fisher et al., 2011). Furthermore, individuals released from correctional institutions are at increased risk of residential instability (Geller & Curtis, 2011; Kushel et al., 2005), and homelessness increases one’s vulnerability for contacts with the criminal justice system, through poverty-driven offending, increased surveillance, and the penalization of everyday life activities, such as sleeping or urinating in public spaces (Geller & Curtis, 2011; Hiday & Wales, 2011; Nijdam-Jones et al., 2017; Roy, Crocker, Nicholls, Latimer, & Isaak, 2016).
Several mechanisms linking homelessness, mental illness, and criminal justice involvement have been proposed. Skeem et al. (2011) proposed a model to account for the association between criminal behavior and mental illness. Their model, based on three main mechanisms, overlaps with Hiday and Wales’s (2011) five-group typology of people who have mental illness and who come into contact with the justice system. The first mechanism suggests that, for some, poverty and social disadvantage explain the lion’s share of the association between mental illness and criminal behavior, notably through neighborhood disadvantage and victimization (Kubrin & Stewart, 2006; Seto et al., 2018). Hiday and Wales (2011) suggested that this reflects a group of individuals who tend to commit acquisitive and mischief/public order offenses motivated by inadequate living conditions, and another group whose concomitant substance abuse increases the risk of offending as well as the risk of being arrested for offenses related to drugs and their procurement.
The second mechanism proposed by Skeem et al. (2011) suggests that mental illness is associated with poor satisfaction with employment and relationships, which in turn favors the development of antisocial traits or attitudes and procriminality that contribute to criminal behavior (Bonta et al., 2014; Skeem et al., 2014). Hiday and Wales (2011) have also accounted for a similar pathway with a subgroup of individuals with mental illness whose criminal motivations arise primarily from antisocial traits, antisocial cognitions, and the influence of antisocial peers. Individuals for whom these mechanisms are relevant would be expected to display a range of criminal behavior, sometimes including violent crimes.
Finally, the third mechanism suggests that, for a small subgroup of individuals with mental illness, untreated psychiatric symptoms are a direct cause of criminal behavior and violence (Junginger et al., 2006; Peterson et al., 2014). Hiday and Wales (2011) hypothesized the existence of two groups for whom mental illness is the primary driver behind criminal justice involvement: one group of individuals who are arrested primarily for mischief/public order offenses as a result of often harmless behaviors stemming from psychiatric symptoms occurring in public areas, and another who commit violent offenses driven by high levels of psychiatric symptomatology, such as hallucinations and delusions, and who are more likely to be found not criminally responsible due to mental illness.
The nature and patterns of offending may point to unique criminogenic needs and distinct criminal pathways among subgroups of individuals with mental illness who become entangled with the criminal justice system (Hiday & Wales, 2011; Skeem et al., 2011). Rehabilitation efforts aimed at individuals with mental illness convicted of crimes focus on the importance of incorporating the concept of criminogenic risk, using, for example, the Risk-Need-Responsivity (RNR) framework (Epperson et al., 2014; Skeem et al., 2015). The most important criminogenic risk/needs factors identified to date, referred to as the Central Eight, are criminal history, procriminal attitudes and cognitions, procriminal companions, antisocial personality pattern, education and employment, family and marital relationships, and substance abuse (Bonta et al., 2014; Skeem et al., 2015). According to the RNR model, individuals with different profiles of criminal justice involvement would have different criminogenic needs and warrant different interventions, both in nature and in intensity (Bonta & Andrews, 2007; Skeem et al., 2015). The risk principle highlights the importance of matching the intensity of interventions to the level of risk of the individual (Andrews, 2011; Bonta et al., 2000; Latessa et al., 2010). Moreover, the need principle focuses on the importance of assessing and targeting criminogenic needs in treatment, whereas the responsivity principle stresses the need for tailoring these interventions to individuals’ particular strengths and vulnerabilities (Bonta & Andrews, 2007; Skeem et al., 2015). In essence, it is vital to identify individual characteristics to better target needs and reduce criminal behavior.
Previous studies have attempted to characterize profiles of criminal justice involvement of those with mental illness. Using cluster analysis, Roy and colleagues (2016) generated profiles of self-reported criminal justice system contacts among participants in the 6-month period prior to their enrollment in the At Home/Chez Soi (AH/CS) study of homelessness. The first cluster comprised participants with multiple justice contacts, who were more likely to have depression and substance dependence, including a subgroup of individuals with frequent criminal justice involvement for nonviolent events, and more severe psychiatric symptomatology. A second cluster of participants were arrested, often for a disturbance, but were diverted from the criminal justice system and not charged. Finally, a third cluster comprised participants with a single arrest and associated charge, who were most likely to have severe substance misuse and low impulse control. Similarly, when examining 5-year jail bookings and psychiatric hospitalizations in a sample of 161 homeless individuals with mental illnesses, Harding and Roman (2017) identified four distinct profiles of frequent system users with cluster analysis: (a) the largest group comprised the average frequent user in terms of episodes of homelessness, jail admissions, or psychiatric hospitalization; (b) the second group was persistently homeless/rapidly cycling users, and had the most felony convictions; (c) the third group had the worst mood as well as the most issues in terms of alcohol and drug abuse; and (d) the smallest cluster were lifetime cyclers who had the most jail bookings. Although these findings provide a portrait of the criminal justice involvement of individuals who are homeless, 6 months to a few years may be too short a period to identify clear profiles and their associated characteristics. Because the effects of criminal justice involvement are far reaching and cumulative (Lopes et al., 2012; Muftić et al., 2016), examining lifetime criminal justice involvement and modeling its heterogeneity may assist in the identification of need profiles, providing critical insights into the nature and intensity of potential prevention and treatment initiatives.
Aims and Hypotheses
The aim of this study is threefold: (a) to describe the lifetime criminal justice involvement of a cohort of individuals with mental illness who are homeless; (b) to delineate distinct lifetime criminal justice involvement profiles; and (c) to compare these profiles across clinical and psychosocial characteristics. We had no hypothesis regarding the number of profiles that would emerge, but based on the extant literature, we expected to find qualitatively and quantitatively distinct profiles in type and number of prior criminal charges (Hiday & Wales, 2011; Skeem et al., 2011). Specifically, we expected to find one profile of individuals with higher rates of substance abuse characterized by a higher number of drug charges, another profile comprised individuals with a higher prevalence of violent offending along with more complex psychosocial histories, one profile with a higher number of mischief or public order offenses along with more severe psychiatric symptomatology, and one profile characterized by a greater history of homelessness along with petty and diverse criminal involvement. Finally, we hypothesized that the largest group would be composed of individuals with little prior criminal justice involvement.
Method
Sample and Procedure
This study uses a sample of participants recruited for the Montreal, Vancouver, Toronto, and Moncton sites of the AH/CS Housing First research and demonstration project of people living with mental illness who were homeless (for published study protocol, see Goering et al., 2011). We included the 1,682 participants who provided consent for the research team to access criminal records (Moncton: n = 230; Montreal: n = 468; Toronto: n = 549; Vancouver: n = 435), representing a participation rate of 94.2%. Participants had to be (a) legal adults, (b) absolutely homeless or precariously housed, and (c) have at least one serious mental disorder, specifically psychotic disorder, mood disorder with psychotic features, manic or hypomanic episode, major depressive episode, panic disorder, or posttraumatic stress disorder (PTSD), as determined by Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria on the Mini International Neuropsychiatric Interview (MINI; Lecrubier et al., 1997) at study enrollment. Participants were recruited between October 2009 and July 2011 in community agencies and various institutions that deliver services to people who are homeless and provided written informed consent. Appropriate institutional review boards across all four sites approved the research protocol, and additional ethics approvals were obtained for administrative justice data.
Measures
Indicator Variables
Official criminal records were obtained from the Royal Canadian Mounted Police (RCMP) Fingerprint Service. Criminal records included lifetime criminal charges (Canadian criminal code number), court outcome (verdict), and sentencing up to study enrollment. Files included youth criminal charges insofar as individuals had also been charged as adults. If an individual was charged as a minor and was not subsequently charged as an adult, their criminal record was not sent to the research team, and they would be coded as having no record. Records in paper format from all four sites were sent to Montreal, where they were coded and entered by 21 different raters who held or were completing an undergraduate degree in psychology or criminology. All raters coded four files to assess interrater agreement, which was strong with greater than 91.5% agreement for all sites across the various items, and kappa values ranging from .74 to .95 (Landis & Koch, 1977).
Charges were classified into 16 categories based on Uniform Crime Reporting number (Canadian Centre for Justice Statistics Policing Services Program, 2008) and then further aggregated into five charge categories for the purpose of analyses: violent, mischief/public order, drug-related, acquisitive, and administration of justice. Charges for violent offenses included violations causing death and attempting the commission of a capital crime, sexual assaults, assaults, violations resulting in the deprivation of freedom, other violations involving violence or the threat of violence (such as robbery), and violations pertaining to offensive weapons. Charges for mischief/public order offenses included disturbing the peace, property crimes involving mischief, disruptive behavior, and traffic violations such as impaired driving, street racing, and dangerous driving without due care and attention. Charges for drug-related offenses included those pertaining to the Controlled Drugs and Substances Act and the Food and Drugs Act. Charges for acquisitive offenses included acquisitive property crimes (e.g., theft, fraud), as well as offenses relating to prostitution, gaming, and betting. Finally, charges for administration of justice offenses included failure to comply with conditions, failure to attend court, and breach of probation. Charges that could not be classified into the five broad charge types, such as attempting to commit an undetermined crime, were classified as “other” and were not used to create the indicator variables. Although over a quarter of justice-involved participants had at least one of these charges (see Table 2), they represented only 2.3% (n = 561) of the total number of charges. We computed the total number of lifetime charges for each category and Winsorized at the 98th percentile to facilitate convergence of the model (Tabachnick & Fidell, 2013; Wilcox, 2005).
Correlates
Self-reported sociodemographic information was collected through an interviewer-administered questionnaire designed for the AH/CS study (see Goering et al., 2011, for details). Specifically, we collected self-reported information pertaining to gender, age at baseline, ethnicity (which we recoded as Indigenous, White, or other), work history (having worked at least 1 year in the past), education (high school completion), lifetime duration of homelessness (in months), and history of psychiatric hospitalization indicating greater clinical needs (having had at least two psychiatric hospitalizations within a 1-year period over the course of the past 5 years). Self-report in a research context has been found to be reliable in this population (Lemieux et al., 2017). Psychiatric disorder was assessed using the MINI (Lecrubier et al., 1997) at study enrollment by experienced interviewers with social science degrees who could benefit from a consultant psychologist when in doubt. Specifically, we examined the presence (or absence) of psychotic disorder, PTSD, manic episodes, as well as drug and alcohol use disorder (understood as abuse and/or dependence), as they have been found to be associated with criminal involvement (Bonta et al., 2014; Christopher et al., 2012; Douglas et al., 2009). Impulsivity was assessed using Item 17 of the Multnomah Community Ability Scale (MCAS), an observer-rated measure of community functioning (Barker et al., 1994; Dickerson et al., 2003). Interviewers rated participants on a 5-point scale at baseline, where a higher score indicated greater impulse control. Finally, we created a variable called “pre-homelessness justice involvement,” in reference to the sequence of onset of first episode of homelessness (self-reported at baseline) and first criminal charge (from official criminal records). When these two events occurred at the same age, we coded these individuals as having no prehomelessness justice involvement.
Statistical Analyses
Justice involvement was examined using descriptive statistics with Stata MP version 13. Latent profile analysis (LPA) was conducted on Mplus version 8, using lifetime number of charges in the five aforementioned categories as indicator variables. Model selection was determined by interpretability along with several standard statistical indicators (entropy, Bayesian information criterion, and bootstrapped likelihood ratio test). A three-step approach to LPA was used to examine the characteristics of each latent class in terms of the covariates listed above (Asparouhov & Muthén, 2014). Significance level was set at α = .01. Additional details pertaining to statistical analyses are available in the Supplemental Appendix (available in the online version of this article).
Results
Sample Characteristics
The majority of the sample (n = 1,682) self-identified as male (69.1%) and White (58.1%), and the mean age at study enrollment was 41 years (SD = 11.3). Less than half (47.6%) of the participants had completed high school, and over two thirds (69.5%) had worked at least 1 year continuously in their lifetime. In terms of mental illness, major depressive episode (44.4%) and psychotic disorder (38.2%) were the most common diagnoses. Alcohol use disorder was identified in 36.6% of the sample, whereas half (52.7%) of the sample had a drug use disorder (see Table 1).
Sociodemographic and Clinical Characteristics of the Sample (N = 1,682)
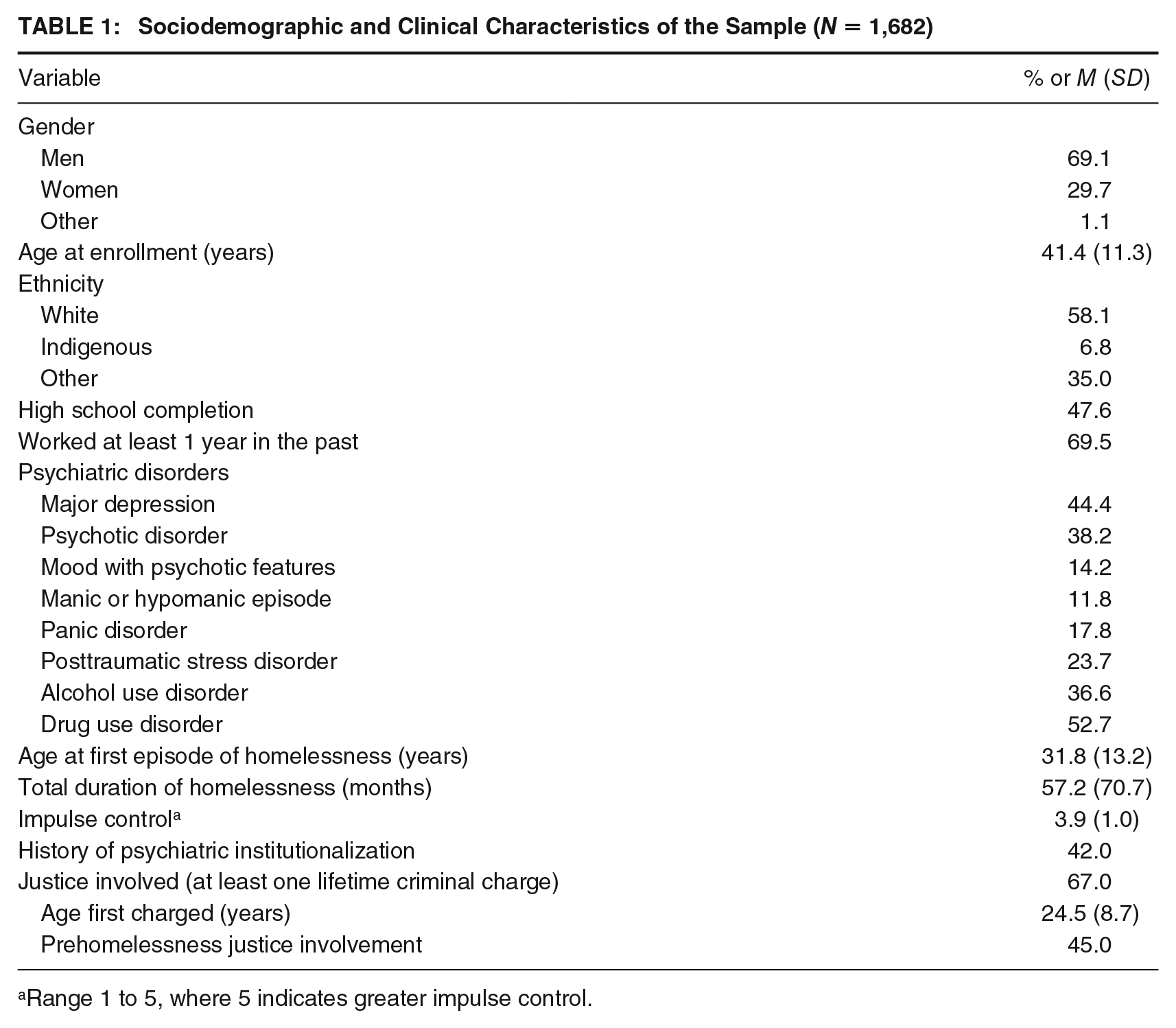
Range 1 to 5, where 5 indicates greater impulse control.
Lifetime Criminal Justice Involvement
Two thirds of participants (n = 1,127, 67.0%) had an official criminal history (i.e., at least one criminal charge), with an average of 21 charges (SD = 23.4) and a median of 12 charges (range = 1–143) over their lifetime. A quarter (24.5%) of justice-involved participants had a criminal charge before the age of 18, with an average number of charges as a minor of 1.2 charges (SD = 3.2; Mdn = 0; range = 0–26). The average age for first lifetime criminal charge was 24.5 years (SD = 8.7), and almost half (45.0%) had a criminal charge preceding their first homelessness episode.
Table 2 presents the distribution of charges as per the 16 Uniform Crime Reporting categories, all ages considered, among participants with at least one charge. Among those with a criminal record, 90.2% (n = 1,016) had at least one guilty verdict, 17.6% (n = 198) had at least one acquittal, 81.3% (n = 916) had their charges dropped at least once, and 3.0% (n = 34) of individuals had at least one verdict of not criminally responsible on account of mental disorder (NCRMD). Across the sample, there were 23,854 charges: 69.6% resulted in guilty verdicts, 28.3% were dropped, 1.7% ended in an acquittal, and less than 1% resulted in an NCRMD verdict. The most frequent charges were for acquisitive property crimes (28.9%), offenses related to the administration of justice (23.1%), and assaults (13.7%).
Description of Charges Among Justice-Involved Participants (N = 1,127)

Note. Percentage represents those having at least one of each type of offense.
Identification of Profiles of Lifetime Criminal Justice Involvement
LPA was used to investigate the plausibility of two- to seven-class solutions. The five-class model was selected, as distinct profiles emerged which were theoretically interpretable. Table 3 describes the five-class solution in terms of mean number of charges for each charge category. Class 1 was comprised of 1,273 individuals (75.7%), Class 2 of 178 individuals (10.6%), Class 3 of 84 individuals (5.0%), Class 4 of 84 individuals (5.0%), and Class 5 of 63 individuals (3.8%). Class 1 was characterized by lower means than for the total sample in all charge categories. Class 2 had no defining charge type: for all five categories, participants had neither the highest nor the lowest charge means. Class 3 had the highest means for both violent and mischief/public order charges, and also had a high mean for administration of justice charges. Class 4 had the highest means for acquisitive and administration of justice charges, as well as high means for violent and mischief/public order charges. Finally, Class 5 had the highest mean for drug-related charges.
Mean Number of Charges (With Standard Deviation) of Each Category in Overall Sample and Each Class

Comparison of Criminal Justice Involvement Profiles Across Clinical and Psychosocial Characteristics
Table 4 shows significant differences between the classes on all variables, except those pertaining to mental illness. Prehomelessness justice involvement, total duration of homelessness, as well as drug and alcohol use disorder were the clinical variables most likely to differ significantly between the classes. Participants in Class 1 (n = 1,273) were younger (M = 41.0, SE = 0.34), more likely to be women (35.0%), to have completed high school (53.0%), to have worked at least 1 year in the past (72.3%), and to display better impulse control (M = 3.98, SE = 0.03). This class had the smallest proportion of individuals with drug use disorder (45.6%) and had the shortest mean duration of lifetime homelessness (M = 33.3 months, SE =1.61). Because we suspected heterogeneity within this first class, given that it includes individuals who were charged with few but sometimes violent offenses (see Supplemental Appendix, available in the online version of this article, for details), we separated those who were charged with at least one violent offense (n = 488) from those who were not (n = 785). As these subgroups did not emerge empirically, we did not conduct any hypothesis testing and instead used this knowledge to better understand Class 1. Those with at least one violent offense showed a higher prevalence of psychotic disorder (43.7% vs. 35.4%) and of previous psychiatric hospitalization (49.2% vs. 41.6%). Nearly half of all (15 of 34) those found NCRMD in their lifetime belonged to the subgroup with at least one violent offense compared with six in the group with no violent offenses.
Mean (With Standard Deviations) or Proportion Comparisons of Covariates for Each Class

Note. PTSD = posttraumatic stress disorder; NCRMD = not criminally responsible on account of mental disorder.
Significant difference between Fewer Needs and Needs Associated with Homelessness at p < .01. bSignificant difference between Fewer Needs and Extensive Crimino-genic Needs at p < .01. cSignificant difference between Fewer Needs and Needs Associated with Drugs at p < .01. dSignificant difference between Fewer Needs and Acute and Extensive Criminogenic Needs at p < .01. eSignificant difference between Needs Associated with Homelessness and Extensive Criminogenic Needs at p < .01. fSignificant difference between Needs Associated with Homelessness and Needs Associated with Drugs at p < .01. gSignificant difference between Needs Associated with Homelessness and Acute and Extensive Criminogenic Needs at p < .01. hSignificant difference between Acute and Extensive Criminogenic Needs and Extensive Criminogenic Needs at p < .01. iSignificant difference between Acute and Extensive Criminogenic Needs and Needs Associated with Drugs at p < .01. jSignificant difference between Needs Associated with Drugs and Extensive Criminogenic Needs at p < .01. kSample too small, Fisher’s exact test conducted.
Participants in Class 2 (n = 178) had the longest mean duration of lifetime homelessness (M = 134.7 months, SE = 7.50) and the lowest impulse control (M = 3.46, SE = 0.10), as well as high rates of drug (76.5%) and alcohol (49.1%) use disorders. They did not differ significantly from participants in Class 1 in terms of employment history and had the second highest proportion of individuals with past stable employment (66.9%). Participants in Class 3 (n = 84) were the oldest (M = 45.8 years, SE = 0.96), were most likely to be male (90.1%), had the highest rate of alcohol use disorder (52.8%), and had a high proportion of prehomelessness justice involvement (71.9%). Participants in Class 4 (n = 84) were characterized by the highest proportion of individuals self-identifying as Indigenous (14.5%), the highest proportion of prehomelessness justice involvement (83.0%), and had a high proportion of individuals with alcohol use disorder (52.5%). They were very similar to participants who belonged to Class 3, and the two groups did not significantly differ on any of the variables. Class 5 (n = 63) had the highest proportion of individuals identifying as an ethnic minority other than Indigenous (38.0%), were least likely to have completed high school (23.5%), and less likely to have worked at least 1 year in the past (55.4%). They were the most likely to have a drug use disorder (83.1%) but least likely to have an alcohol use disorder (29.7%).
Discussion
This study identifies profiles of lifetime criminal justice involvement and their associated characteristics among a large sample of people with mental illness experiencing homelessness. This approach allows the extrapolation of need profiles associated with the cumulative effects of justice involvement. This improved understanding will be helpful for program development and evaluation, allowing service providers and decision makers to better target the needs of this marginalized population and inform population health policies and treatment.
Lifetime Criminal Justice Involvement
The first objective of the study was to describe the lifetime criminal justice involvement in this population. We found that over two thirds of the sample had a history of criminal justice involvement, which is in line with previous studies (Omura et al., 2014; Roy et al., 2014; Saddichha et al., 2014). This proportion is substantially greater than that of the general population (10%; Government of Canada, 2017). Tests of proportions show that guilty verdicts are more frequent in our sample than in the general offending population (70% vs. 63%, p < .001), whereas acquittals are less frequent (2% vs. 4%, p < .001; Maxwell, 2017). This finding, which is consistently observed in the literature (Fazel & Baillargeon, 2011; Fazel & Danesh, 2002; Huxter, 2013), suggests that the overrepresentation of homeless and mentally ill people within the criminal justice system might be a reflection of their increased likeliness to plead guilty, possibly due to difficulties in mounting a strong defense, in understanding the long-term implications of a criminal record and/or because of limited social and financial resources.
The most common charges in our sample reflected acquisitive property crimes (29%), administration of justice offenses (23%), and assaults (14%). In comparison, the most common criminal offenses in the general population are administration of justice offenses (23%), theft (10%), impaired driving (10%), and common assault (i.e., Level 1%–9%; Maxwell, 2017). Other than impaired driving, justice-involved homeless people with mental illness, as a group, are similar to the general offending population with regard to their type of charges. The high proportion of acquisitive property offenses is consistent with the findings from previous studies among individual with mental illness convicted of crimes to the effect that they are more likely than those without a mental illness to engage in property and acquisitive offenses as a means of survival and contradicts the notion that individuals with mental illnesses are dangerous and violent (Greenberg & Rosenheck, 2008; Hiday & Moloney, 2010).
Profiles of Criminal Justice Involvement as a Way to Identify Level of Need
The second and third objectives of the study were to identify distinct profiles of lifetime criminal justice involvement among people with mental illness who were homeless, and to compare them across clinical and psychosocial characteristics. We hypothesized the existence of specific profiles according to the existing theoretical models and prior research on the mechanisms explaining the criminal involvement of individuals who have mental illnesses (Hiday & Wales, 2011; Skeem et al., 2011). Generally consistent with our expectations, five profiles emerged from our analyses which point toward the existence of unique needs which can be differentially addressed to prevent societal harm, criminalization, and provide individuals with appropriate services.
As expected, the largest of the five groups, Class 1, included individuals with less complex psychosocial histories, indicative of less criminogenic and clinical needs, such as greater educational achievement, employment stability, and lesser criminal involvement compared with the four other groups (Bonta & Andrews, 2007; Bonta et al., 2014; Skeem et al., 2015). Overall, this indicates that the majority of individuals who are homeless do not have an extensive criminal career. We labeled this class Fewer Needs. Although individuals in the Fewer Needs group have less criminogenic and psychosocial needs than individuals from the four other classes, they still have important needs: They are homeless, mentally ill, and may have experienced multiple episodes of victimization and trauma (Edalati et al., 2017). Therefore, interventions for this subgroup could include rapid housing initiatives and emergency financial assistance coupled with trauma-informed care, so as to reduce exposure to vulnerability factors which may eventually lead to criminal involvement (Edalati et al., 2017; O’Donnell, 2019; Palmer et al., 2019; United States Department of Housing and Urban Development [HUD], 2016).
Classes 2 and 5 were characterized by greater social precariousness relative to the other classes, illustrated by longer periods of homelessness and more difficulty with employment coupled with moderate rates of general criminal involvement. Class 2 was labeled Needs Associated with Homelessness, as it was mainly characterized by chronic homelessness. Class 5 was defined by a greater number of drug charges, along with higher rates of drug use disorder, and was accordingly labeled Needs Associated with Drugs. Given their socioeconomic precarity as well as general criminal activity, individuals in these two groups may be more likely to benefit from initiatives such as Housing First coupled with forensic assertive community treatment or intensive case management (Cuddeback et al., 2013; Leclair et al., 2019; Morrissey et al., 2007; Woodhall-Melnik & Dunn, 2016). Moreover, individuals with Needs Associated with Drugs may benefit additionally from integrated dual disorder treatment (Peters et al., 2017) and drug treatment court (Wilson et al., 2006) to link them to appropriate services and decrease the criminalization of their substance use.
Finally, participants from Classes 3 and 4 were most likely than the other groups to have come into contact with the justice system prior to their first episode of homelessness and be charged with violent and mischief/public order offenses, suggesting that criminal justice involvement may be indicative of antisocial traits (Bonta & Andrews, 2007; Bonta et al., 2014; Skeem et al., 2015). As such, antisocial beliefs, possibly secondary to early trauma (see Edalati et al., 2017), as well as a lack of resources may both contribute to the justice involvement of participants of these two subgroups. These individuals are also more likely to be charged with administration of justice offenses, in line with previous studies which found that breach of conditions is most likely in individuals with extensive criminal histories (Grattet et al., 2009). These breaches contribute to the “revolving door” phenomenon, as administration of justice offenses are most likely to result in custodial sentences (Burczycka & Munch, 2015). This has led to initiatives specifically catering to individuals with mental illness convicted of crimes that take into account criminogenic needs, which have been found to reduce recidivism, arrests, and subsequent incarceration time (Abracen et al., 2016; Skeem et al., 2017). Because individuals in both these groups are farther along their justice trajectories, they are unlikely to be offered early diversion services. However, measures can be taken to stop the revolving door cycle. For instance, they could benefit from postjail diversion programs, such as APIC (Assess, Plan, Identify, Coordinate) and Critical Time Intervention models to reduce the risk of further homelessness and recidivism, as well as from interventions using the RNR framework (Osher & King, 2015; Pinals, 2017; Skeem et al., 2015). We thus labeled Class 3 Extensive Criminogenic Needs and Class 4 Acute and Extensive Criminogenic Needs, as individuals of the latter group did not significantly differ from the former on any characteristics, but showed a greater level of need, as per their much higher rates of charges relating to acquisitive crimes. In addition to interventions that address antisociality and other criminogenic needs, individuals with Acute and Extensive Criminogenic Needs may benefit from initiatives aimed at increasing resources, such as Housing First and supported employment (Talbot et al., 2017; Woodhall-Melnik & Dunn, 2016).
We also expected a group with a high number of mischief/public order offenses along with worse psychiatric symptomatology (Hiday & Wales, 2011; Skeem et al., 2011), although it did not emerge. A potential explanation may be that we only examined charges under the Criminal Code, while research suggests that most mischief and public order offenses are managed through police interactions that result in informal arrangements (e.g., the individual is requested to leave the area) or through the enforcement of municipal or other local by-laws (Charette et al., 2011; M.-E. Sylvestre, 2010). Self-report justice data revealed that 89% of the participants in the present study had at least one contact with police forces over the course of the study (Goering et al., 2014), although this may include help-seeking and information requests. Exploratory analysis of our data regarding police contacts in the Montreal site suggests that 52% of police interactions as a suspect do not result in a formal arrest. This indicates that many of these justice interactions may be dealt with through alternative strategies, such as diversion, ticketing, or support services.
None of the profiles identified significantly differed in terms of psychiatric characteristics. While the criminalization of mental illness is often cited as an explanation for the overrepresentation of individuals with a mental illness in the criminal justice system (Abramson, 1972; Hiday & Wales, 2011; Munetz & Griffin, 2006), studies have shown that individuals with mental illnesses convicted of crimes do not differ much in terms of criminogenic needs when compared to those without mental illness (Skeem et al., 2011, 2014). However, individuals with mental illness are disproportionately affected by poverty, mainly because they are more likely to be unemployed and underemployed, making them more prone to collect disability income (Harvey et al., 2009; Marwaha & Johnson, 2004). Individuals with mental illness thus face greater challenges in meeting their basic needs such as housing and have diminished capabilities allowing them to change their situation (J. Sylvestre et al., 2018). They are also more likely to have comorbid substance use problems (Kieres-Salomoński & Wojnar, 2015; Swendsen et al., 2010). These are the factors that are most likely to lead to criminal involvement, beyond mental illness (Fazel et al., 2009; Skeem et al., 2014; Swartz & Lurigio, 2007). Of note, in the current study, exploratory analyses in the Fewer Needs category revealed that individuals with at least one violent offense may experience more psychiatric difficulties, also reflected in the larger proportion of not criminally responsible verdicts. Although this subgroup did not emerge empirically, this may point toward the existence of a small group of individuals whose violent crimes are driven by symptoms of severe mental illness (Hiday & Wales, 2011; Skeem et al., 2011). Recent research has shown that people suffering from schizophrenia and other psychotic disorders are more prone to committing violent criminal acts than the general population (Penney et al., 2016; Witt et al., 2015). This is especially true of individuals with comorbid substance use disorders (Ogloff et al., 2015). However, mental illness itself is not a significant cause of crime and explains a very small proportion of societal violence (Darrell-Berry et al., 2016; Varshney et al., 2016). Regardless, when in crisis, individuals with severe mental illness may benefit from early intervention and assessment from community mental health services (Abreu et al., 2017). This is especially true of people found not criminally responsible due to mental illness, who are often already well known of civil psychiatric services before they offend (Crocker et al., 2015).
Strengths, Limitations, and Future Directions
The present study is the largest to empirically delineate and examine profiles of lifetime criminal justice involvement among homeless individuals with mental illness. Unlike past studies with similar samples (Benda et al., 2003; Harding & Roman, 2017; Roy, Crocker, Nicholls, Latimer, Gozdzik, et al., 2016), we examined lifetime criminal justice involvement. Considering lifetime criminal justice involvement along with historical criminogenic factors may contribute to our understanding of criminal justice involvement as well as better predict future needs and behavior (Bonta & Andrews, 2007).
Some limitations must be taken into account when interpreting the results. First, because this study only included criminal charges, there is likely an underrepresentation of public order and acquisitive offenses (e.g., loitering and panhandling), which are often covered by municipal by-laws. Second, police have considerable discretion and may opt to transport an individual with severe symptoms of mental illness to the hospital rather than arrest and charge them, when there are no victims and no one to press charges. These events would therefore not be accounted for in official criminal records. Third, the use of administrative data only offers insight into instances wherein individuals were charged with offenses; “successful” offending (i.e., when one manages not to get caught) might not be adequately taken into account. Finally, our sample did not include the full spectrum of mental disorders which may be linked to criminal justice involvement, such as disruptive, impulse control, and conduct disorders (American Psychiatric Association, 2013; Bonta et al., 2014; Skeem et al., 2014).
Further research should validate these typologies. In addition, future studies may want to use these profiles to evaluate the differential effectiveness and cost-effectiveness of psychosocial interventions such as Housing First. Another valuable approach may be to model longitudinal trajectories of lifetime criminal justice involvement, with time-dependent covariates to better understand the complex interaction of individual, psychological, and social/contextual risk factors at the time of each contact with the justice system.
Conclusion
This five-profile typology provides a means of better understanding the cumulative needs associated with variable patterns of lifetime criminal justice involvement among people with mental illness who are homeless. Our study generally supports the typologies and theoretical mechanisms suggested by Skeem et al. (2011) as well as Hiday and Wales (2011) who both emphasize the association between mental illness, socioeconomic situation, and criminal justice involvement. These results lend support for targeted interventions, such as early intervention and assessment from community mental health for participants with Fewer Needs, housing interventions for participants with Needs Associated with Homelessness, postjail diversion program and interventions using the RNR framework for participants with Extensive Criminogenic Needs and Acute and Extensive Criminogenic Needs, and drug treatment court or integrated dual disorder treatment for participants with Needs Associated with Drugs. Future studies should explore whether individuals from the various profiles benefit uniquely from different types of psychosocial and rehabilitation programs.
Supplemental Material
Appendix-900305 – Supplemental material for A Typology of Lifetime Criminal Justice Involvement Among Homeless Individuals With Mental Illness
Supplemental material, Appendix-900305 for A Typology of Lifetime Criminal Justice Involvement Among Homeless Individuals With Mental Illness by Ashley J. Lemieux, Marichelle C. Leclair, Laurence Roy, Tonia L. Nicholls and Anne G. Crocker in Criminal Justice and Behavior
Footnotes
Authors’ Note
This work was supported by a Mental Health Commission of Canada grant awarded to Eric A. Latimer. Over the course of this study, Ashley J. Lemieux was granted doctoral research scholarships from Fond de Recherche du Québec–Société et Culture (FRQ–SC), and from Équipe Vulnérabilité, intégration sociale et violence (VISEV), as well as a McGill University Department of Psychiatry for Graduate Excellence Fellowship in Mental Health Research. Marichelle C. Leclair would like to acknowledge the financial support of FRQ-SC in the form of an MSc fellowship, and VISEV as a bursary. Laurence Roy would like to acknowledge the Fonds de recherche Québec–Santé (FRQ-S) for her Junior 1 Chercheurs-boursiers salary award. Tonia L. Nicholls would like to acknowledge the Canadian Institutes of Health Research (CIHR) for her New Investigator salary support and her Foundation Award. Anne G. Crocker received consecutive salary awards from CIHR and FRQ-S, as well as a McGill University William Dawson Scholar Award during this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.