
Abstract
Evaluations of juvenile adjudicative competence (AC) are frequently ordered, yet significant gaps remain in the field’s understanding of referred youth. Using a sample of 277 court-ordered evaluations of juvenile AC, this study provides further support for the relationship of age and intelligence with competence, but other factors remain inconsistent. In the current study, developmental immaturity was associated with competence. Youth showed highest rates of deficits in the functional capacities of rational appreciation, ability to assist counsel, and decision-making. Within factual understanding, the highest rates of deficits were seen for the understanding of charges, plea bargains, the trial purpose, and juvenile justice commitment. This study provides the first empirical estimate of the proportion of youth (9%–30%) who demonstrate factual, but not rational understanding, and highlights areas that may be underreported in reports to the court. Implications for evaluations and research are described, including a focus on mental health symptoms and rational appreciation.
Keywords
Evaluations of juvenile adjudicative competence (AC) have increased dramatically since due process rights were first recognized in the juvenile courts (In re Gault, 1967; Kent v. United States, 1966). As policy and practice changes have created a system in which juveniles face serious sanctions and an adversarial process, the competency of youth to participate in the adjudicative process has become a frequent and important question. Studies of community, juvenile justice, and evaluated youth have provided important information about the general competency-related capacities of youth; however, most research has focused on factors associated with competency and not examined competency-related functional abilities—that is, exactly what the youth can or cannot accomplish (Grisso, 2003). This article seeks to address this gap in the literature by examining the specific functional abilities of youth referred for competency evaluations and examining how historical and diagnostic factors relate not just to the overall opinion on competency but also the specific functional capacities that constitute competency. Results indicate what specific abilities remediation efforts should be prepared to address.
AC from Criminal to Juvenile Court
The need for an accused individual to be competent or able to participate in the legal process has deep roots in English law (Roesch & Golding, 1980) and can be seen in the early 19th century in American courts (United States v. Lawrence, 1835). It has long been recognized that adjudicating only those persons who are competent both protects their constitutional rights and preserves the real and perceived integrity of the courts (Drope v. Missouri, 1975; Youtsey v. United States, 1899). The U.S. Supreme Court, in Dusky v. United States. (1960, p. 402), specifically defined a competent defendant as one who has a “sufficient present ability to consult with his lawyer with a reasonable degree of rational understanding” and “a rational as well as factual understanding of the proceedings against him.” Scholars have broken this definition into four functional capacities that together comprise competence: factual understanding, rational appreciation, ability to assist counsel, and ability to make relevant decisions (Kruh & Grisso, 2009), with assisting and making decisions sometimes combined under the idea of reasoning. Although competence became relevant to youth as due process protections were extended to the juvenile courts in the 1960s (In re Gault, 1967; Kent v. United States, 1966), it was not until the “get tough” era of the 1990s, when more and younger youth began facing more adversarial processes and punitive outcomes, that the question of competence was increasingly raised in the juvenile courts (Bonnie & Grisso, 2000; Grisso, 2003). Despite this increase, attorneys may not raise the question of competence as often as they have actual concerns about a youth’s AC (Viljoen et al., 2010), suggesting juvenile AC is neither appropriately nor sufficiently addressed (Bryant et al., 2015; Grossi et al., 2016; Harvey, 2011).
Today, juvenile courts function very similarly to adult criminal courts, with adversarial proceedings and the potential for far-reaching consequences. Statutes specific to juvenile AC are common (37 states) but vary widely in what they include (Panza et al., 2020). Some statutes are informed by research and resulting best practice recommendations (Larson & Grisso, 2011). Other states have limited statutory guidance based largely on long-standing criminal court practice (Rapisarda & Kaplan, 2016). The latter can produce significant challenges because of the important differences between juveniles and adults in factors impacting AC. Similarly, while there is a large body of research identifying factors typically associated with adult incompetence, and thus established procedures and related restoration services (most commonly through psychotropic medication, Zapf & Roesch, 2009), for juveniles, the picture remains less clear. Youth may be found incompetent to stand trial for reasons of mental health disorder, cognitive deficits, developmental delays, normal developmental immaturity, or some combination thereof. Further complicating the picture, incompetent youth frequently present with a constellation of factors that do not rise to the level typically associated with inpatient treatment (Kruh & Grisso, 2009) nor would they be expected to respond as readily to medication. Current understanding of the factors associated with juvenile AC has been informed by two distinct veins of research.
Adjudicative Capacities of Juveniles
First, studies of community and the general population of juvenile justice youth (i.e., not youth whose competence was questioned by the court) have provided important information about the capacities of youth in this domain. Across studies, younger juveniles and those with lower IQ are more likely to have competency-related deficits (Ficke et al., 2006; Grisso et al., 2003; Viljoen & Roesch, 2005). Younger youth are also more likely to show deficits in appreciation of attorney-client privilege and the advocacy role of their attorney as well as the appreciation of the relationship between offense severity and possible consequences (Grisso, 1980, 1981; Grisso & Pomiceter, 1977; Peterson-Badali & Abramovitch, 1992). The difference in younger youth may be partially explained by lower future orientation (Kivisto et al., 2011). Similarly, lower IQ scores are associated with deficits in understanding, appreciation, and decision-making (Grisso et al., 2003). Processing speed, specifically, has been associated with understanding and appreciation aspects of juvenile AC and working memory with reasoning (Panza & Fraser, 2015). Furthermore, age and IQ appear to interact, whereby youth with low IQ and young age are at particular risk for deficits in AC (Ficke et al., 2006; Grisso et al., 2003; Viljoen & Roesch, 2005). These findings are particularly concerning, as juvenile justice youth score, on average, 1 SD below their peers on measures of IQ (Kivisto et al., 2011). Some measures of learning and academic functioning have been associated with AC-related abilities, although no clear patterns have been established (see Kruh & Grisso, 2009).
Although helpful, these studies examine youth adjudicative competence outside the context of real charges and use tools that do not examine case-specific decision-making or consider developmental issues specific to youth (Kruh & Grisso, 2009). In reality, juvenile competency evaluations occur within the stressful context of a legal case and extend beyond an interview of the youth to include collateral information and behavioral observations, such as interactions with the attorney (O’Donnell & Gross, 2012), factors highly relevant to demonstrated adjudicative competence. As such, the generalizability of these findings to actual evaluation contexts may have limitations.
AC in Referred Juveniles
The second vein of research has examined AC abilities more contextually, using youth referred and evaluated for competency to stand trial. Research consistently indicates that youth referred for evaluations of adjudicative competence appear similar to their juvenile justice peers, facing multiple charges and having a history of juvenile justice, special education, and mental health service involvement (Kruh & Grisso, 2009). Studies have also identified various factors that may distinguish competent and incompetent youth.
Most consistently, as in research with general youth samples, younger evaluated youth are more likely to be opined incompetent. Depending on the age categories examined, studies have found youth less than age 15 (Bath et al., 2015) or those aged 12 and younger most likely to be found incompetent (Baerger et al., 2003; Kruh et al., 2006; McCormick et al., 2021; McKee, 1998). When compared, incompetent youth are significantly younger than competent peers (Cowden & McKee, 1994). Similarly, intelligence is also associated with competence in referred youth. Youth at lower levels of intellectual functioning (Kruh et al., 2006) and those diagnosed with mental retardation/borderline intellectual functioning (McKee & Shea, 1999) or intellectual deficits (Bath et al., 2015; McCormick et al., 2021; Warren et al., 2019) are more likely to be opined incompetent to proceed.
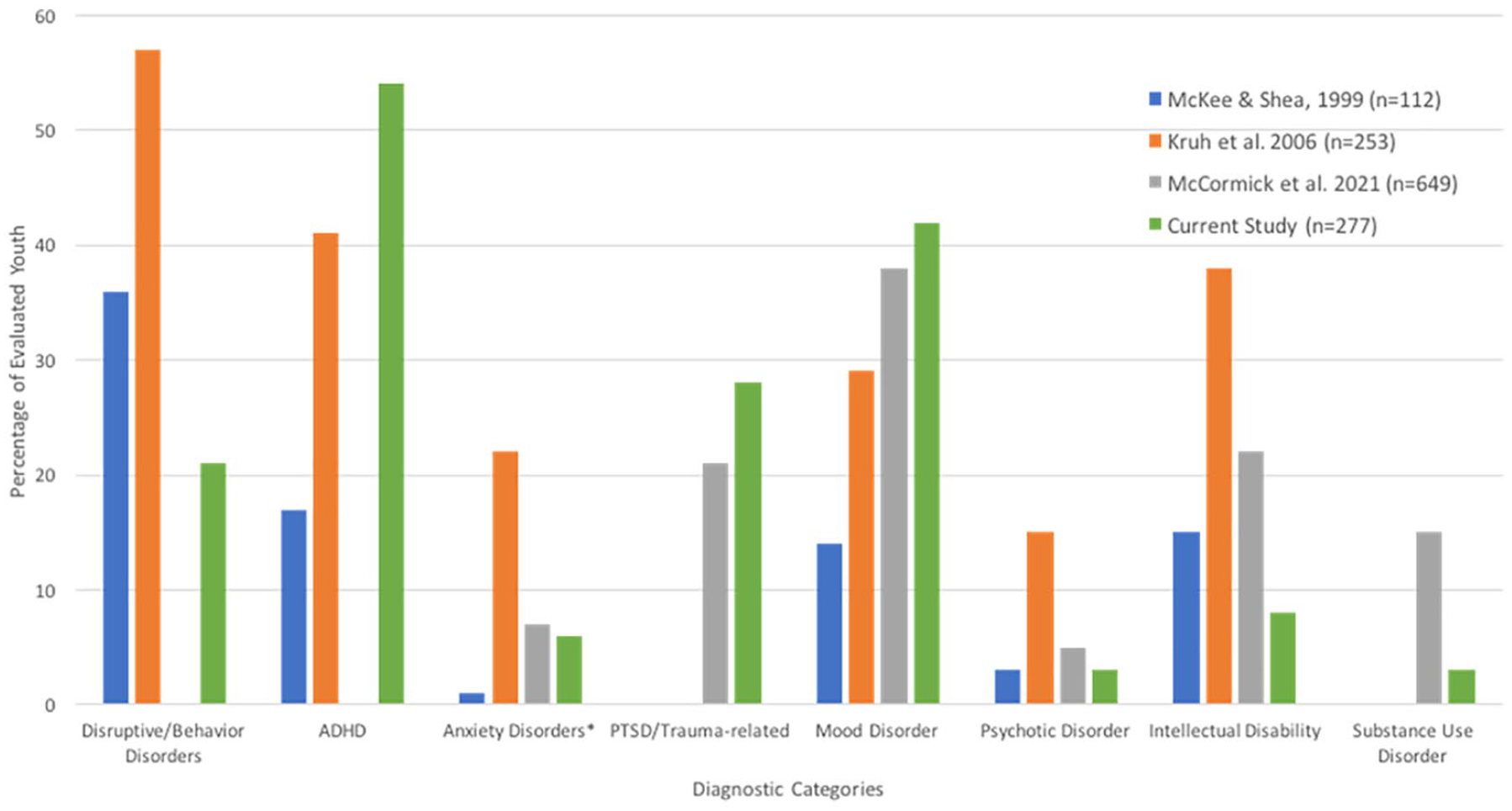
The relationship between other diagnostic categories and juvenile competence is less clear. In adults, the presence of a psychotic disorder (Pirelli et al., 2011) is a strong predictive factor for incompetence. In studies of referred youth, however, where one study found youth aged 16 to 17 with a diagnosed psychotic disorder more likely to be found competent (Bath et al., 2015), Kruh et al. (2006) found a psychotic disorder diagnosis was associated with incompetency. One explanation may be that the types and rates of disorders present in referred youth vary widely. For example, across studies, the percentage of referred youth diagnosed with psychotic disorders has ranged from 3% to 28% and those with attention-deficit hyperactivity disorder (ADHD) from 17% to 41% (Bath et al., 2015; Kruh et al., 2006; McKee & Shea, 1999). Differences are likely influenced by evaluation location (in-patient vs. outpatient settings) and jurisdictional differences in the disorders considered acceptable bases for questioning or determining incompetence. However, further clarity on the relationship between mental health functioning and competency is needed to inform policy and develop practices to address the mental health needs of incompetent youth.
Existing research has yielded inconsistent results with other explored factors. Previous outpatient mental health treatment has been significantly associated with incompetence in some studies (Baerger et al., 2003) and with competence in others (Bath et al., 2015), whereas other research found no relationship (Cowden & McKee, 1994; Kruh et al., 2006). Similarly, a history of special education was associated with incompetence in some studies (Baerger et al., 2003; Cowden & McKee, 1994). Another study found most referred youth had a history of special education and the absence of that history may be associated with competence (Kruh et al., 2006). Other factors such as prior arrests have been associated with competency in one sample (McKee & Shea, 1999) but not in others (Cowden & McKee, 1994) or with any consistency.
Together, this body of research confirms the importance of considering age and intelligence when evaluating juvenile AC. It also highlights a key complication in understanding juvenile AC: a precise understanding of how the larger constellation of mental health symptoms, cognitive deficits, developmental deficits, developmental delays, and developmental immaturity may influence competence remains elusive.
The lack of research on developmental immaturity (DI), beyond the proxy of age, in youth referred for evaluation of juvenile AC is a particular limitation. Although best practice recommendations are that DI be noted as an acceptable predicate, or basis, for incompetence in youth (Larson & Grisso, 2011) and 15 of 37 states with juvenile specific AC statutes explicitly include DI as an accepted predicate for incompetence (Panza et al., 2020), the field has not yet developed a reliable way to measure the construct (Cunningham, 2020), particularly in clinical evaluations. What we know about DI, in particular associated deficits in abstract thinking, risk appraisal, and reasoning (see Kemp et al., 2017; Shulman & Cauffman, 2013), has clear implications for youth’s AC. Attorneys note DI as a common source of concern about youth’s AC (Viljoen et al., 2010), and research from one jurisdiction suggests evaluators note DI as a factor influencing AC even when not specifically established in statute as an acceptable predicate (McCormick et al., 2021), especially for youth 12 and younger.
Additional descriptive research is needed to help clarify the current literature and to develop a more representative picture of referred youth across jurisdictions. Furthermore, very little research with referred youth has looked beyond the overall determination of competence to examine the specific functional abilities underlying competence. Using a modified set of functional abilities required for competence (McGarry & Curran, 1973), McKee (1998) found youth, particularly those less than 13, were less often opined to possess the functional abilities associated with competence than older youth and adults. Knowing and defining charges, the adversarial process, trust in attorney, willingness to disclose facts, and ability to consider a plea-bargain were all observed less frequently in youth. Yet, most studies have not broken youth abilities down to the level of functional deficits, leaving evaluators with little information on what deficits may be of most concern when conducting their evaluations.
The Present Study
The current study was designed to address several gaps in the current literature by examining a large sample of youth referred for an evaluation of AC in two jurisdictions of one state and using the forensic evaluation report as the source of information. These reports reflect youth functioning at the time competency was questioned in the context of the real court demands and stressors and as such is an important source of information. They are also the source used by judges to inform ultimate court competency determinations. This study provides additional descriptive data on who is referred for juvenile AC evaluations and what factors are associated with competence, placing those data in the context of existing studies.
We expected evaluated youth would have high rates of Intellectual Disability (ID), special education history, and mental health treatment history. We also expected age, ID, and inpatient treatment history (as a measure of symptom severity) would be associated with incompetence in referred youth. Due to the range of potential severity encompassed by any diagnostic classification, we did not expect that diagnosis per se would be associated with AC. We expected DI would be noted more often for younger youth and sought to provide descriptive information on the proportion of youth for whom DI was noted as a key factor influencing competence.
Second, this study provides descriptive information on the specific functional deficits exhibited by youth referred for evaluation of juvenile AC. It also examines the relationship between youth characteristics and the four broad functional capacities of AC: factual understanding, rational appreciation, ability to assist counsel, and ability to make relevant decisions. We expected youth would show more marked deficits in rational appreciation and decision-making than in factual understanding. Because previous research has not examined relationships between these specific functional capacities and clinical or historical factors, these are novel exploratory analyses. We also examined the relationship between factual understanding and other functional deficits. We expected that factual understanding would be necessary but not sufficient for other functional abilities that are more cognitively complex (Rogers et al., 2004). This study provides a first empirical estimate of the portion of youth who demonstrate factual understanding but not rational appreciation of a specific area of knowledge.
Method
Sample
Court-Ordered Evaluations of Juvenile AC
De-identified evaluations of juvenile AC, referred to as “competence to stand trial” in state statute, were gathered from two Massachusetts (MA) counties with the most court-ordered competency referrals in the state. The study was approved by the Administrative Office of the Juvenile Court and the supervising IRBs for both the court clinics and the author’s institution. MA is uniquely suited to serve as a source of information because of its court clinic model and related state regulations that require court clinic evaluators (doctoral-level psychologists or psychiatrists) to be certified as Certified Juvenile Court Clinicians (CJCC). Evaluators complete specialized training and a committee-review process to ensure reports meet established standards. This process means the content and format of evaluations are more consistent than might be typical in other jurisdictions. A total of 371 reports on 277 youths were deidentified and collected from the court from the study period (June 1, 2009–June 1, 2014). For youth evaluated more than once during the study period, only the initial evaluation was included in the current study (N = 277). The collected reports represented 93% of ordered evaluations of juvenile AC in the two county court clinics during the study period.
Youth whose reports were included in the study were 83% male and ranged in age from 8 to 19 (M = 14.78, SD = 2.18). Information on race and ethnicity was included in reports for only a portion of participants (35% and 39%, respectively; see Riggs Romaine et al., 2017 and Riggs Romaine & Kavanaugh, 2019) and was coded for the current study as two separate variables (i.e., a youth described as a “black Hispanic male” was coded as Black for race and Latino/Hispanic for ethnicity). Of those reported, 44 were Black/African American, 37 were White, 13 were two or more races, and 2 were Asian (181 missing). For ethnicity, 78 participants were described as Latino/Hispanic and 28 as not Latino/Hispanic (171 missing). Most youth included in the study were referred by their defense attorney (66%) and spoke English (88%). Their most serious open charges ranged in severity from attempted murder to low-grade miscellaneous offenses (e.g., disorderly person and delinquent trespassing). More than half (58%) had a most serious offense of assault/assault and battery. Most also had a history of special education (76%, although only 8% of the full sample were diagnosed with an intellectual disability) and mental health treatment (88%, 44% of the full sample had been psychiatrically hospitalized). Records of the official court determination regarding competence were not available. For this reason, evaluators’ concluding opinions (including ultimate-issue opinions and also conclusory penultimate statements) were used as the dependent variable of AC. Research has consistently found very high agreement between evaluator opinions and judicial determinations of competence (Harvey, 2011; Kruh et al., 2006; Zapf et al., 2004).
Forensic Evaluators
The included reports were written by 23 different evaluators, each of whom contributed 1 to 41 reports (M = 12.04, SD = 12.18, Mdn = 9, Mode = 1) to the total sample. Reports were completed by evaluators holding a PsyD (53%), PhD (38%), or MD (8%). Per state statute, all evaluators were certified or in the certification process to become a CJCC and were working in one of the two selected juvenile court clinics at the time the evaluation was completed.
Coding Procedures
A team of nine trained research assistants (graduate and undergraduate students) who were blind to study hypotheses read reports and coded them using a structured coding scheme to pull variables from the narrative evaluations. The structured coding scheme, a detailed worksheet that included the item/factor to be coded, categorical codes, and definitions, was reviewed by a panel of experts in juvenile AC to check that relevant functional abilities were included. The coding scheme was reviewed and updated with expert feedback before initial training and coding began.
All coders were trained by the author, coding multiple reports together, reconciling differences, and creating a coding manual with detailed instructions for each item. When consistent coding was achieved, coders began rating assigned cases. One of every four reports was double-coded by two independent raters. Data were collected at the most detailed level possible (e.g., years and months of age, specific diagnoses) and grouped later for the purposes of analysis and comparison to existing research (e.g., age range of 8–12, mood disorders).
Data Retrieval
Many variables of interest in the current study had to be retrieved from the lengthy, written evaluations of juvenile AC but did not require rating by the coder. Descriptive and demographic information was collected including age, race/ethnicity, current grade level, mental health diagnoses, treatment history, out-of-home placements, history of child-protective service involvement, education history (including special education placement), and charges. Specific open charges were grouped by level of severity using 19 categories, based loosely on the FBI’s uniform crime index, which ranged from murder as most serious to the least serious miscellaneous category (e.g., city ordinance violation, vandalism, and driving while disqualified).
Data Coding
Other variables, including the specific functional abilities of interest in this study, required the coder to categorize information the evaluator provided in the report. The coding sheet captured descriptions of the youth’s evidenced understanding and appreciation of the functional abilities listed in Table 4. The description provided in the text of the report was coded into nominal categories. Descriptions of factual understanding were coded as (0) Able to demonstrate, (1) Able with provided education, (2) Mixed, (3) Not able to demonstrate, or (4) No information given. Descriptions of appreciation were coded as (0) No information given, (1) Adequate appreciation/Absence of deficits noted, or (2) Deficits noted. Descriptions of the evaluator’s conclusory opinions on factual understanding, rational appreciation, ability to assist counsel, and ability to make relevant decisions were coded as (0) Adequate, (1) Mixed, (2) Inadequate, or (3) No information given. Adequate interrater reliability was established for these items. The prevalence-adjusted bias-adjusted kappa (Byrt et al., 1993) was calculated to account for the expected and observed prevalence problem (i.e., when ratings fall under one category at much higher rates over another; Hallgren, 2012) for many coded variables. Kappa values of .75 and greater are generally defined as reflecting excellent agreement, .60 to .74 as good agreement, and .40 to .59 as fair agreement (Cicchetti & Sparrow, 1981). The reliability data reflect excellent agreement for 37.5% of items, good agreement for 37.5%, and fair agreement for the remaining 25% of coding items.
Statistical Analysis Plan
The primary questions of interest in this study relied on descriptive statistics and measures of association between categorical variables. Descriptive statistics were used to determine the proportion of participants characterized by clinical and individual factors, and the findings compared with those from previous research. In many analyses, age was considered as a categorical variable to allow comparison to previous research (e.g., Grisso et al., 2003; Kruh et al., 2006). Categorization of continuous variables can reduce statistical power (Naggara et al., 2011), so age was used as a continuous variable for any analyses that were not compared with previous research, and the impact of categorization was examined for regression analyses.
Descriptive statistics were also used to provide data on the prevalence of specific functional abilities in the current sample. Consistent with previous research, chi-square analyses were used to examine the association between individual factors and AC (both evaluator’s conclusions and the four functional capacities). Point-biserial correlations were used for continuous predictor variables. After assessing collinearity, a multivariate logistic regression equation was used to examine the effects of each significant factor on AC while controlling for the effects of the other factors and to determine the percentage of cases accurately classified by the model.
Results
Youth Referred for AC Evaluations
Figure 1 shows the percentage of youth in each diagnostic category and places the current sample in the context of other research on youth referred for AC evaluations. The current sample had proportionally more youth diagnosed with ADHD, mood disorders, and anxiety and trauma-related disorders (the latter two were grouped together as anxiety disorders in previous research using Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000] categories) than previous samples, but proportionally fewer youth diagnosed with psychotic disorders and intellectual disabilities.
Diagnoses of Evaluated Youth Across Studies
Factors Related to AC and AC Capacities
As in previous research, gender, χ2(1, N = 268) = 1.73, p = .189, and offense severity, r(267) = −.1, p = .105, were not associated with competence, and age (categorized as shown in Table 1) was significantly associated with competence opinions, χ2(3, N = 268) = 21.21, p < .001, V = .28. Only 20% of youth aged 9 to 12 were opined competent, whereas 46% to 65% of the other age groups were opined competent. As expected, age was also associated with all four broad functional capacities: factual understanding, χ2(6, N = 252) = 18.89, p = .004, V = .19; rational appreciation, χ2(6, N = 206) = 26.98, p < .001, V = .25; ability to assist counsel, χ2(6, N = 217) = 17.33, p = .008, V = .20; and ability to make relevant decisions, χ2(6, N = 243) = 16.35, p = .012, V = .18 (see Table 2).
Factors Discriminating Competence
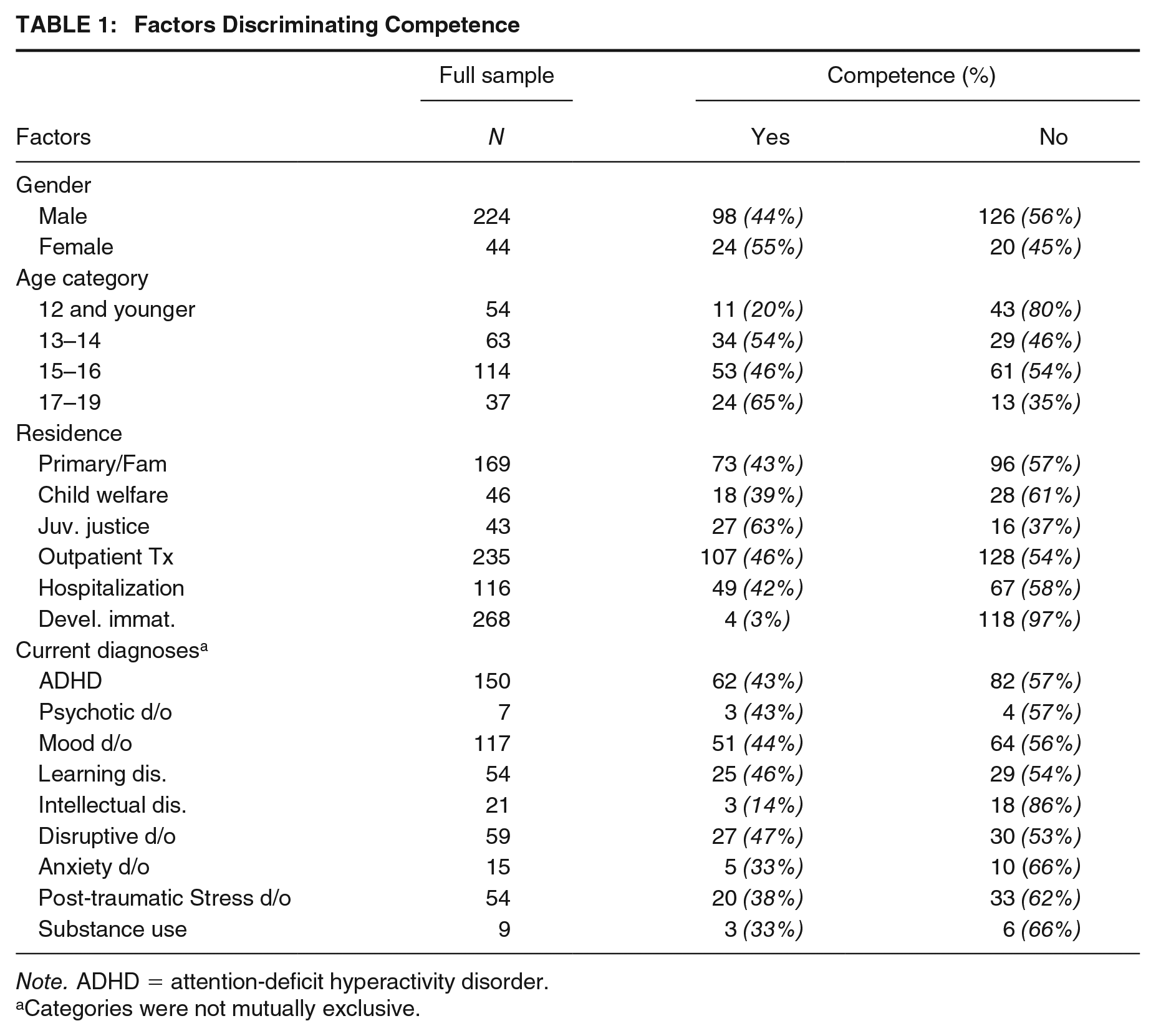
Note. ADHD = attention-deficit hyperactivity disorder.
Categories were not mutually exclusive.
Factors Discriminating Functional Capacities
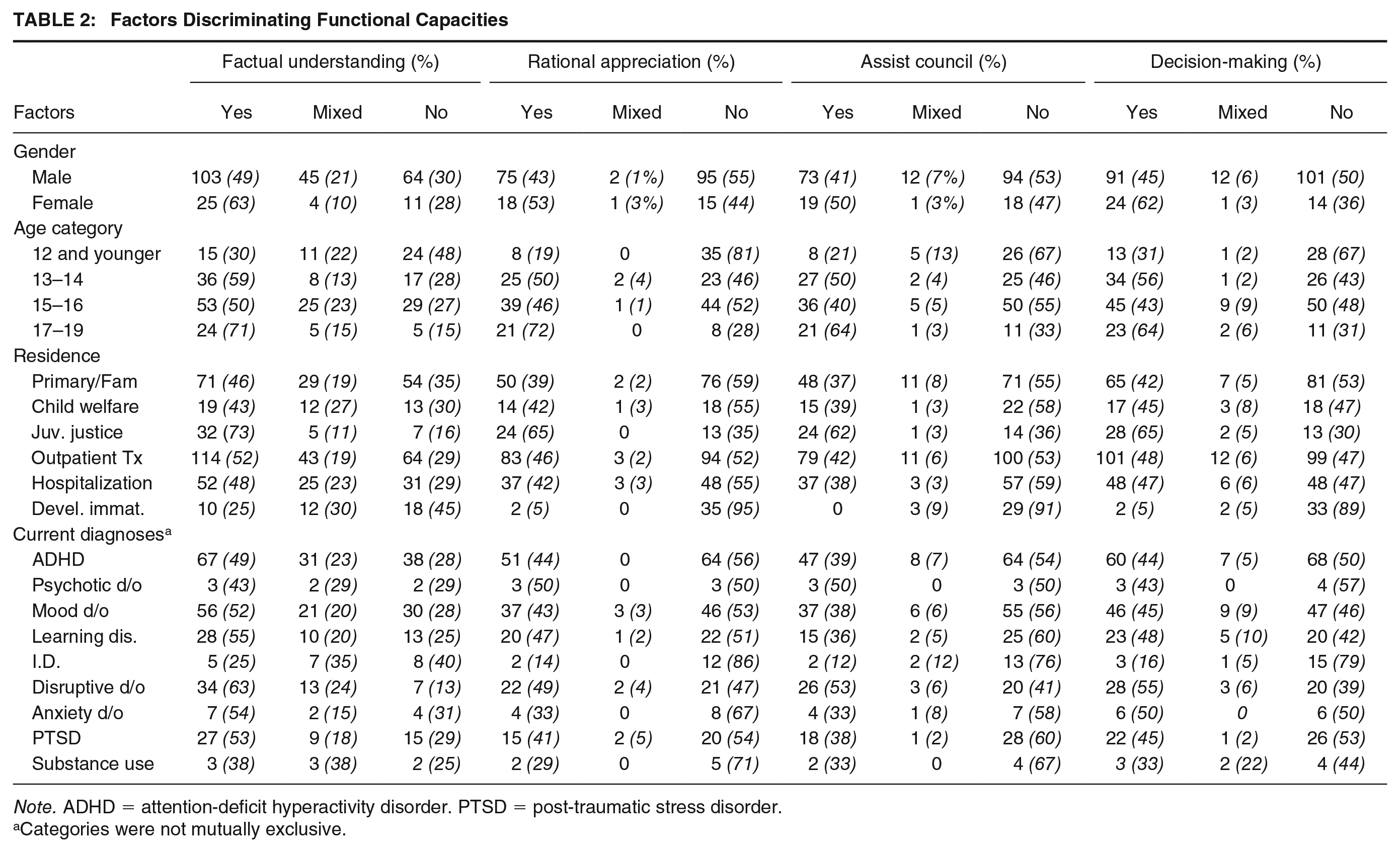
Note. ADHD = attention-deficit hyperactivity disorder. PTSD = post-traumatic stress disorder.
Categories were not mutually exclusive.
In the current sample, variables not associated with competence or any functional capacities were special education (past or current placement), history of outpatient treatment, and history of psychiatric hospitalization. Placement at the time of evaluation was associated with both competence, χ2(2, N = 258) = 6.29, p = .043, V = .16, and factual understanding, χ2(4, N = 242) = 12.43, p = .014, V = .16. Youth placed in the custody of the state’s juvenile justice agency were more likely to be opined competent (63%) than youth in placement with the state’s child welfare agency (39%) or those living with a parent/primary caregiver or family member (43%). Youth in juvenile justice custody were less likely to have problems in factual understanding (16%) than youth in child welfare (30%) or caregiver/family custody (35%). Importantly, placement at the time of evaluation was also associated with age, F(2, 264) = 16.46, p < .001. Tukey’s honestly significant difference (HSD) test revealed youth placed in juvenile justice custody (Mage = 16.11, SD = 1.05) were significantly older than youth placed with caregivers/family (Mage = 14.24, SD = 2.35), p < .001, 95% confidence interval (CI) = [1.06, 2.67].
Current psychotic disorders, mood disorders, PTSD and trauma-related disorders, and learning disabilities did not differentiate competent and incompetent youth, nor did they distinguish groups on any of the four functional capacities (see Table 2). Current ADHD diagnosis was associated only with rational appreciation, χ2(2, N = 181) = 6.32, p = .042, V = .17. Youth with a current ADHD diagnosis were more likely to have inadequate rational appreciation (55% vs. 50%) and less likely to show mixed abilities (0% vs. 5%). A disruptive disorder diagnosis was associated only with factual understanding, χ2(2, N = 215) = 9.31, p = .010, V = .21, where youth with a diagnosed disruptive disorder were more likely to demonstrate adequate factual understanding than their peers. A current diagnosis of intellectual disability (including borderline intellectual functioning, intellectual disability and diagnoses of mental retardation and mild mental retardation under DSM-IV-TR criteria) was significantly associated with competency opinions, χ2(1, N = 229) = 8.80, p = .003, V = .20. Half of youth without an intellectual disability diagnosis were opined not competent, compared with 86% of youth with an intellectual disability diagnosis. Current intellectual disability was also associated with all four functional capacities: factual understanding, χ2(2, N = 215) = 6.82, p = .033, V = .18; rational appreciation, χ2(2, N = 176) = 7.50, p = .023, V = .19; ability to assist counsel, χ2(2, N = 187) = 6.65, p = .036, V = .19; and ability to make relevant decisions, χ2(2, N = 209) = 8.39, p = .015, V = .20. A similar pattern was observed for each functional capacity, a greater percentage of youth with an intellectual disability diagnosis had inadequate abilities in each domain. In one third of study reports where IQ was included, IQ score was significantly associated with competence, r(99) = .28, p < .01.
Statements relevant to developmental maturity were included for only 17% of the sample. DI was noted as a cause of incompetence in 13% of youth, and those youth were significantly younger than the rest of sample, t(275) = 8.63, p < .001, d = 1.57. Specific aspects of developmental immaturity were rarely noted. Only five reports included mention of time perspective (three of those five noted an orientation to short-term consequences), and only 16 reports included description of how the youth weighed risks and benefits (half noted an orientation toward reward). Still, presence of noted developmental immaturity differentiated competent and incompetent youth, χ2(1, N = 268) = 28.17, p < .001, V = .32, and was associated with all four functional capacities: factual understanding, χ2(2, N = 252) = 12.66, p = .002, V = .22; rational appreciation, χ2(2, N = 206) = 30.77, p < .001, V = .39; ability to assist counsel, χ2(2, N = 217) = 27.70, p < .001, V = .36; and ability to make relevant decisions, χ2(2, N = 243) = 32.37, p < .001, V = .37.
The factors associated with AC in the current study (age, current ID diagnosis, noted DI, and current placement) were entered in a binary logistic regression equation. Although age was related to DI, r(277) = −.35, p < .001, and placement, r(277) = .33, p < .001, they are not so collinear as to prevent entry in the model. This model was statistically significant, χ2(7) = 48.11, p < .001, explained 26% (Nagelkerke R2) of the variance, and correctly classified 68% of cases. Youth with a current ID diagnosis were 10.19 times as likely to be opined not competent, and those with noted immaturity were 6.82 times as likely to be opined not competent (see Table 3). Increasing age was associated with an increased likelihood to be found competent, but the placement was not a significant predictor when controlling for the effect of age. When age was included as a continuous variable, the model remained significant, χ2(5) = 42.49, p < .001. The percentage of variance explained decreased (Nagelkerke R2 = .24), but the model continued to accurately classify 68% of cases.
Logistic Regressions Predicting AC Based on Age, ID, Immaturity, and Placement
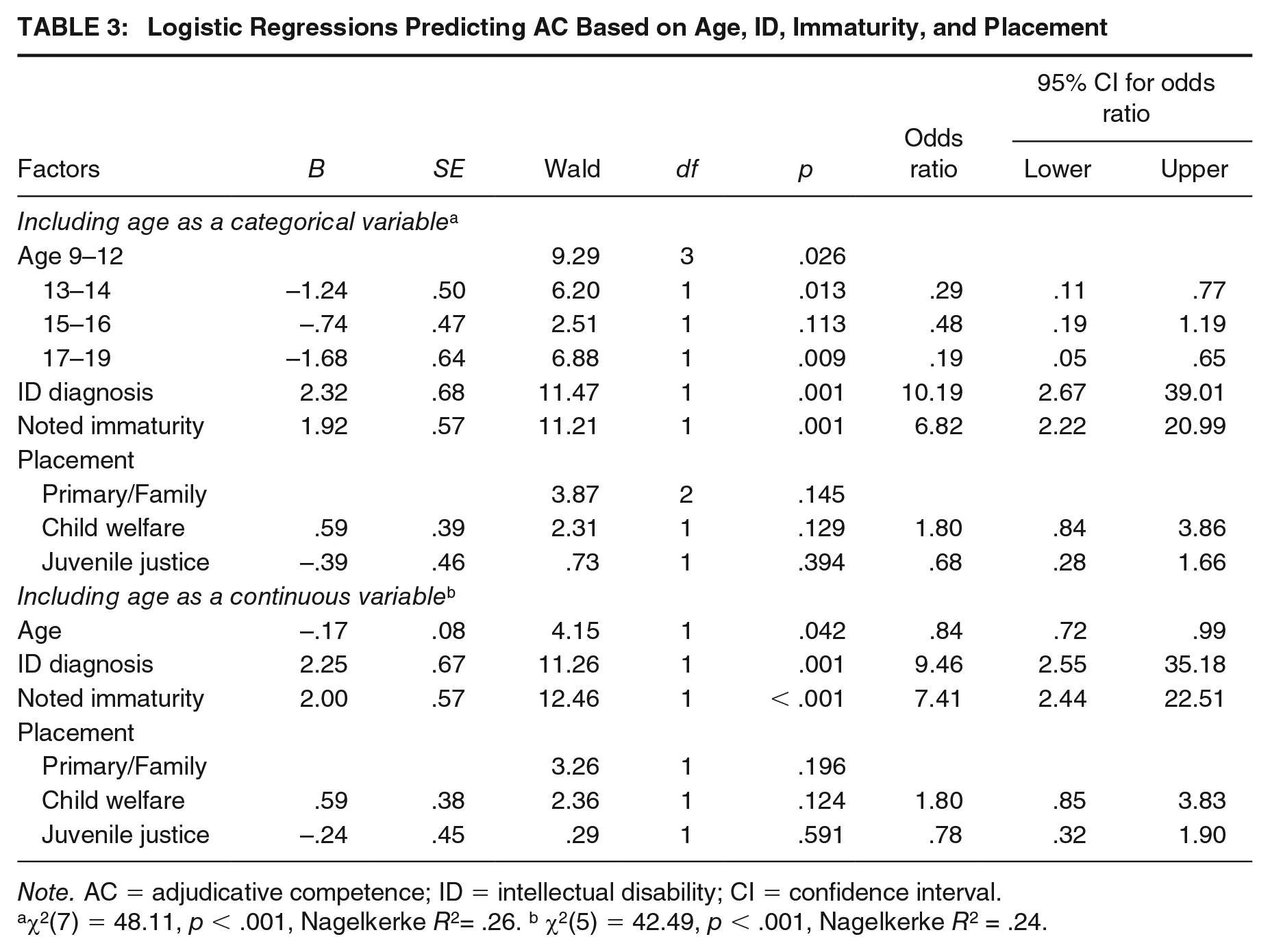
Note. AC = adjudicative competence; ID = intellectual disability; CI = confidence interval.
χ2(7) = 48.11, p < .001, Nagelkerke R2= .26. b χ2(5) = 42.49, p < .001, Nagelkerke R2 = .24.
Specific Functional Abilities in Referred Youth
In addition to the four broad functional capacities, we examined youth’s performance on the specific functional abilities that contribute to the larger functional capacities. For any given item, information was not included in the report (i.e., was coded as “no information given”) for 3% to 82% of youth in the sample. Items with more than 40% missing data are included separately in Table 4 and were not interpreted in the following comparisons because of the high rates of missing data. They do, however, provide data on which functional deficits tend to be missing from the written report. The highest rates of adequate understanding were seen for the ability to adequately define the roles of courtroom personnel and provide factual information about charges and pleas (see Table 4). As expected, fewer youth had documented adequate abilities to rationally appreciate the purpose of a trial, the implications and consequences of different pleas, and the role of legal participants. It was the minority of reports that provided information on time perspective and abilities to comport behavior in the courtroom.
Specific Competence-Related Abilities in Referred Youth

Functional abilities with >40% missing data were not statistically compared due to high rates of missing data.
In Table 4 “Able” includes both (a) youth who could immediately respond to the evaluator’s question on this topic and (b) youth who required education on the topic, but later demonstrated adequate understanding. This second group who required and benefited from education comprised 8% to 71% of youth eventually described as “Able” to demonstrate the specific ability. Youth needed and benefited from education most on plea bargains (71%), continuance without a finding (a common determination in these jurisdictions, 68%), and the role of the prosecutor (55%). Fewer youth demonstrated adequate understanding after education for other items, including those that begin to incorporate an element of appreciation or reasoning: severity of charges (8%), commitment to the juvenile justice system (19%), and how judges make determinations (21%).
Finally, we examined the relationship between factual understanding and rational appreciation. Information on any one aspect of appreciation was missing for 17% to 53% of youth (see Table 4). Cases with no information included on the relevant aspect of appreciation were excluded from the analyses. Table 5 presents the number of youth in each category and the results of chi-square analyses. As expected, a relationship was observed between factual and rational understanding such that factual understanding was necessary but not sufficient for rational appreciation. Having all adequate understanding (i.e., demonstrating all relevant abilities) of charges (able to report the charges, their severity, and the behavior charges refer to) differentiated youth with and without adequate appreciation of charges. Sixty-eight percent of youth with an all-adequate understanding of charges also had an adequate rational appreciation of their charges. Only 15% of youth who did not demonstrate this all-adequate factual understanding were determined to have an adequate rational appreciation of their charges.
Relationship Between Factual Understanding and Rational Appreciation
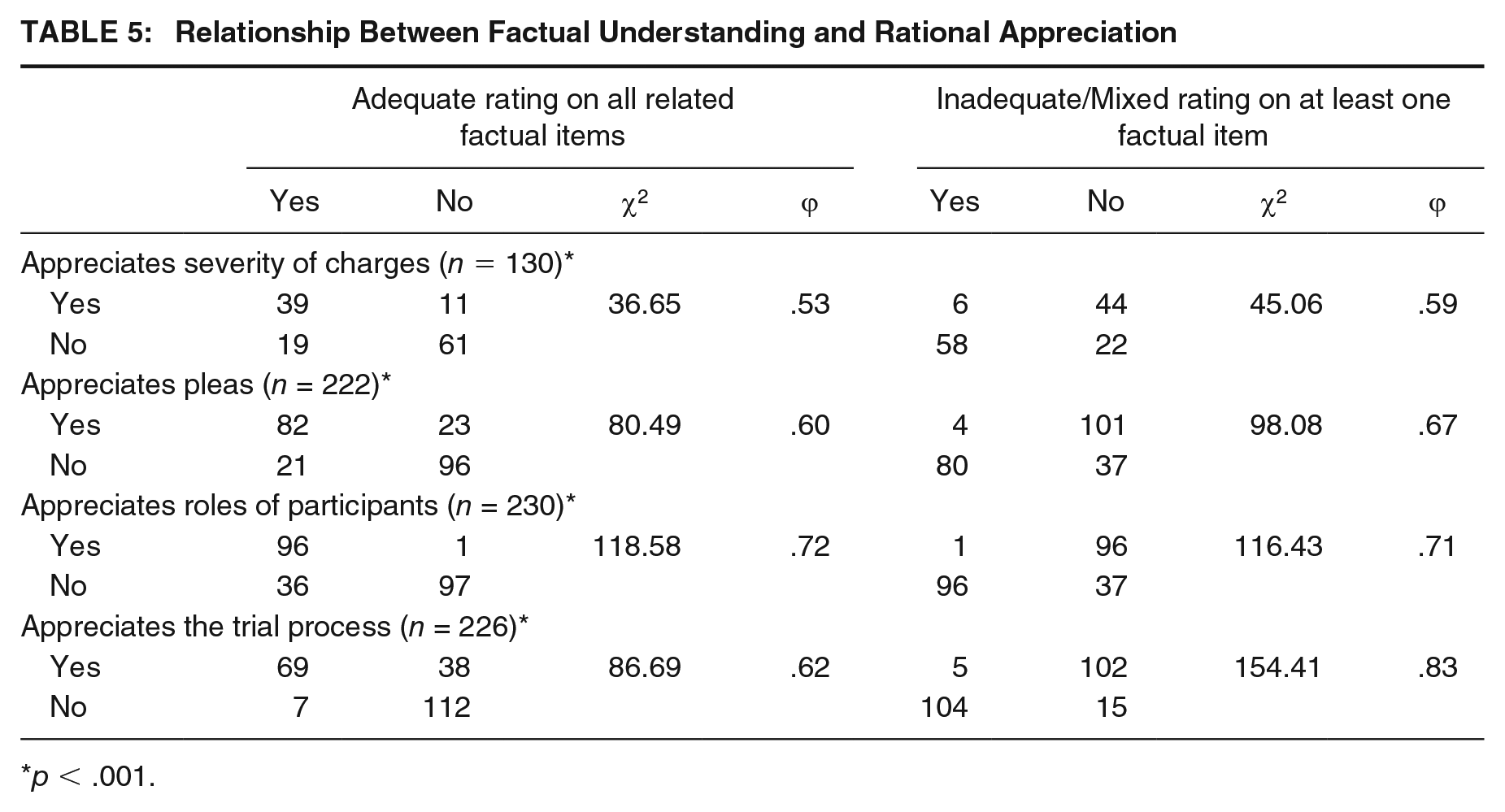
p < .001.
In addition to examining youth with all adequate factual understanding of charges, we also compared youth who did and did not have any one or more component rated as inadequate (i.e., any one or more relevant deficits). Youth who could not demonstrate understanding for one or more factual questions regarding charges were more likely to be described as having deficits in their appreciation of charges (45%) than youth who did not (5%). Similar patterns were observed when the factual understanding of pleas (guilty, not guilty, and plea bargains), participants (defense attorney, prosecutor, and judge), and trials (purpose, roles within the trial, and how determinations are made) were compared with rational appreciation in each area. For each aspect of rational appreciation, youth with adequate factual understanding were significantly more likely to show adequate rational appreciation. For each area, 9% to 33% of youth with all adequate factual responses still showed deficits in the relevant rational appreciation.
Discussion
The current study examined specific functional abilities exhibited by youth whose AC was questioned and evaluated by the juvenile court. It provides an empirical snapshot of referred youth in one jurisdiction at one point in time that is useful both to inform local practice and to add to the emerging picture of juvenile AC nationally over time (Kruh et al., 2006). Results highlight the consistently observed relationship between AC and both age and intelligence in this sample of referred youth. Findings also provide empirical support for expected patterns in juvenile AC between factual and rational understanding and give a first evidence-based estimate of the prevalence of youth who may have a factual understanding but not possess the rational appreciation abilities required by the Dusky standard.
Factors Associated With Competence
Results highlight the wide range of presenting psychiatric problems in referred youth. This sample from 2009 to 2014 included proportionally more youth diagnosed with ADHD and mood disorders, and proportionally fewer youth with psychotic disorders than seen in previous research. More than half of the youth were determined not competent by evaluators. Largely consistent with past research, mental health diagnoses per se did not differentiate competent and incompetent youth in this sample, with the exception of ID. Importantly, ID was defined broadly in this study and included youth noted to have borderline intelligence or mild mental retardation (under DSM-IV-TR diagnostic categories). Lower levels of intelligence have been consistently associated with AC across studies (Bath et al., 2015; Kruh et al., 2006; McCormick et al., 2021; McKee & Shea, 1999; Warren et al., 2019), and in the current study, youth meeting this broad definition of ID were 9.6 times more likely to be found incompetent than youth without an ID. Other mental health diagnoses did not differentiate competent and incompetent youth, nor did history of inpatient treatment. Previous research demonstrated associations between psychotic disorders and competence. Current results were likely influenced by the very small number of youth (n = 7) with a psychotic disorder diagnosis. In the current study, most evaluations were conducted on an outpatient basis as youth requiring a hospital level of care for more severe psychiatric symptoms were typically evaluated through a different local mechanism and would not be included in this sample. The low prevalence of psychotic disorders in this sample was likely influenced by this local policy, and, thus, we do not draw any generalizable conclusions.
As in previous research, in the current study age was consistently associated with competence, with younger youth more likely to be found incompetent. Specifically, youth aged 9 to 12 were 3.4 times more likely to be found incompetent than youth aged 13 to 14 and 5.3 times more likely than youth aged 17 to 19. It is worth noting this observed relationship is not linear. Kruh et al. (2006) also found a varying relationship with age in a sample of referred youth, such that 15- to 16-year-olds were most likely to be found competent and showed the greatest difference when compared with younger youth. Across studies, results consistently demonstrate the greatest competence deficits in younger youth. The impact of developmental immaturity (DI) on competence-related abilities may be most substantial for youth in the youngest age ranges and more variable and influenced by other factors including mental health symptoms, cognitive functioning, and individual differences in maturation in the mid and older age ranges.
In the current study, placement at the time of the evaluation was associated with competence, with youth in juvenile justice custody (in most cases, a juvenile justice detention facility) more likely to be found competent than their peers residing with family or in a child welfare placement. Some previous research has found the opposite (Baerger et al., 2003), and other studies have found no relationship between living situation or guardianship with competence (Kruh et al., 2006; McKee & Shea, 1999). In the current study, the observed differences in factual understanding appear to be due to age, as youth in juvenile justice custody were significantly older.
Developmental immaturity, specifically, has received increased attention since the study time period. Jurisdictions differ in their policy, training, and acceptance of DI as a possible cause of incompetence. Recent research suggests evaluators may note DI concerns, most often for youth aged 12 and younger, at similar rates regardless of policy (McCormick et al., 2021). Regarding the current sample, MA does not require specific predicates for incompetence, but during the study time period, local case law had opened the door to consideration of DI by an included footnote in a rare appellate decision considering juvenile AC (Abbot A. vs. Commonwealth, 2009). Nonetheless, DI was rarely noted in this sample of evaluations and when it was noted, it was to describe problematic immaturity. The codable information in the reports gives an estimate of how often evidence of DI was noted as part of the evaluator’s causal explanation of functional deficits but does not provide consistent information on maturity across the sample.
When the significant factors identified in this study (age, current ID diagnosis, noted DI, and current placement) were entered together, the logistic regression model accurately predicted 68% of youth as competent or not competent. This is lower than, albeit similar to, previous research (Baerger et al., 2003; Kruh et al., 2006). What is interesting are the different factors identified and used in each study. Age, included categorically, is the only common factor across all three studies. Some factors that showed strong association in one study showed no significant relationship with competence in the other two studies. One challenge may be the broad nature of the categories used. Intellectual deficits, psychological disorders, and even categorical IQ scores reflect an array of underlying abilities and deficits. Previous research has demonstrated how different aspects of cognitive functioning (e.g., working memory and processing speed) impact different aspects of competence abilities (Panza & Fraser, 2015). Similarly, a youth may be in special education for a range of psychological and behavioral problems, each with very different implications for competence-related abilities. Together, these analyses highlight the importance of age and intelligence in predicting competence but also point to the difficulty in using other available broad categories to refine that prediction. In research with adults, active psychotic symptoms have been even more predictive of competency findings than the diagnosis of a psychotic disorder (Kois et al., 2013). Future research could examine juvenile’s functioning at the symptom level (e.g., inattention or current psychotic thinking, rather than ADHD or a psychotic disorder) to see if that may better capture specific factors influencing competence.
Specific Abilities and Functional Capacities
Across the sample, there was a subset of functional abilities where youth showed relative strengths and higher rates of adequate understanding. This included the roles of individual trial participants, charges, charge severity, and the behavior referred to by the charges. Youth tended to benefit from education in these areas as part of the evaluation, particularly regarding the role of the prosecutor.
In a second subset of functional abilities, youth demonstrated marked challenges. These included more complex ideas, such as the plea bargaining process, juvenile justice commitment (which in this jurisdiction includes similarly complex if-then contingencies), and rational appreciation of roles and how they are performed by trial participants.
There was a third subset of functional abilities that remain largely unknown. More than half of reports (and in some cases 73%–98% of reports) had no information on specific functional abilities including common verdicts, abilities in the courtroom, and aspects of DI that influence decision-making (e.g., time perspective and orientation to reward). It is possible evaluators did not include information about these higher level abilities if they had already concluded the youth had marked deficits in other functional capacities, in particular factual understanding. However, it is important for reports to address the full array of a youth’s deficits and for evaluators to offer opinions on the youth’s abilities in each of the four functional capacities. This will allow the court to consider the entirety of the legal standard when reaching a competency determination and when considering the likelihood of remediation. Specifically, if only factual understanding is noted as a deficit, judges may be left to assume that remediation of the noted factual deficits will be sufficient to achieve AC.
In addition to describing specific functional abilities, this study is the first to look at how different factors relate to the four broad functional capacities of factual understanding, rational appreciation, ability to assist counsel, and ability to make relevant decisions. Both age and current ID diagnoses were related to all four functional abilities. If a factor is associated with factual understanding, we would expect it to also influence the subsequent abilities that are more cognitively demanding and rely on a factual understanding of the terms and roles (e.g., without knowledge of what a defense attorney does, it is impossible to appreciate that role and how it interacts with other court persons in a trial; see Rogers et al., 2004 for discussion of the cognitive complexity model). It is particularly interesting to look at the factors related to only some of the functional abilities. Placement at the time of evaluation was only related to factual understanding and may reflect differences in who gets placed where for pretrial evaluation, with younger and more fundamentally impaired youth (i.e., youth with less factual understanding) more likely to remain placed at home. ADHD was related only to rational appreciation. It may be that youth with ADHD symptoms are less able to use the factual understanding they do possess to form a rational appreciation and may fall in that group of youth who demonstrate adequate factual understanding but not rational appreciation. The percentage of youth who demonstrated factual understanding but not rational appreciation ranged from 9% on appreciation of the trial process to 33% on the severity of charges.
Limitations
A major limitation of the current study is the lack of information on the race/ethnicity of the evaluated youth. The absence of this information was not anticipated when planning the study methodology and raised interesting questions about if and how race/ethnicity is reported in the body of a forensic report. These questions have been explored fully elsewhere (see Riggs Romaine et al., 2017; Riggs Romaine & Kavanaugh, 2019). Careful consideration of this complex issue is emerging in forensic literature, and practical considerations were recently published by the AP-LS Practice Committee (2021). As practice in forensic evaluations continues to develop, this may remain a problem for some time in research using completed psychological evaluations as the source of information. Researchers may need to seek information from sources of information outside the forensic report (e.g., court databases) to provide this important demographic information. Future research should examine differences in functional abilities as well as differences in evaluators’ perceptions of functional abilities in youth of different races/ethnicities.
This study also presents data from two jurisdictions in one state that does not have a predicate requirement for AC. As a result, the reports that served as the source of information could differ meaningfully in the information reported, and the need for evaluators to reconcile diagnostic ambiguity, from reports pulled from jurisdictions with firm predicate requirements. In the current sample, reports varied in the extent to which evaluators relied on historical mental health diagnoses from records or noted clear conclusions on current diagnostic presentation. This could have impacted our ability to see relationships between current mental health diagnoses and competence-related abilities.
Using evaluation reports as the source of information brings some inherent limits. Evaluators differ in the information they include, and coders are limited by what is presented in the report. In the current study, only one third of youth had an actual IQ score reported, and information on the race and ethnicity of evaluated youth was even more severely limited. Data about the youth and specific competence-related abilities were frequently missing from reports. Demographic and historical information not included may reflect the evaluators’ determination of relevance. In accordance with best practice principles, evaluators must determine the relevance of information and include only relevant information in reports (Heilbrun, 2001). As such, missing data do not necessarily indicate the information was not known or considered by the evaluator. Similarly, missing information on competency-related deficits, such as the high rates of missing information on certain verdicts or the ability to track courtroom events, may reflect information that was not asked by the evaluator but may also reflect information that was determined not relevant for this youth due to the pervasive deficits observed in more foundational areas.
Despite limitations, forensic evaluations of youth whose competence was questioned remain an important source of information. They reflect the youth’s functioning and abilities in the precise time and stressful circumstances relevant for AC. They also reflect the information available to the judge when making competence determinations. Research of this type additionally provides important information on the specific AC deficits in referred youth, suggesting what areas may be most in need of remediation efforts. Nationally, the need for more and different remediation efforts has been noted (see Heilbrun et al., 2019) and a better understanding of the specific functional deficits presented by incompetent youth is key to designing and evaluating remediation programs.
Implications for Policy and Practice
Although the current study relies on reports from one state, it provides a first empirical look at specific functional deficits and when interpreted in the context of previous research has important implications for the forensic evaluation of juvenile AC.
Evaluators and the systems that work with referred youth, including evaluation, remediation, and placement, should expect to see a range of mental health presentations. More recent studies have found a greater prevalence of mood disorders and ADHD and less of the traditionally expected psychotic disorders and intellectual deficits. This likely reflects the growing understanding of the range of mental health symptoms that may interact with development and impact competence-related abilities.
Evaluators, researchers, and policy makers must also carefully consider the utility of diagnoses in different contexts. With the exception of intellectual deficits, mental health diagnoses do not consistently provide an indication of the youth’s competence abilities. Information on the mental health disorders common in referred youth provides helpful normative information for evaluators and can help policy makers plan for remediation needs and interventions. However, nomothetic data on relationships between diagnoses and AC is of limited use to evaluators. Best practices in juvenile AC evaluations include determining functional deficits first, before considering what mental health, developmental or other factors may cause the observed deficits (Kruh & Grisso, 2009). This requires consideration of more specific symptoms and functional abilities than broad diagnoses. Although mental health diagnoses are likely to remain a focus of evaluation, particularly in states with established predicate requirements, it may be more useful for research to focus on symptoms and severity rather than diagnostic categories. The nature and severity of symptoms (e.g., inattention and distraction rather than ADHD) may provide more useful information to distinguish which aspects of psychological functioning most impact competence-related abilities. Future research should empirically examine the relationship between presenting symptoms and functional abilities. In the current study, the information presented in reports on specific symptoms varied widely and tended to focus on behavioral observations (e.g., limited eye contact, description of speech). Using theory and the available empirical evidence, it may be possible for clinical researchers to identify key categories of symptoms to track and assess their relationship with competence abilities.
When assessing youth functional capacities relevant to competence, evaluators should expect that about 9% to 30% of youth who demonstrate adequate factual understanding will nonetheless have deficits in their rational appreciation. These remain first estimates that will need to be clarified and replicated in future research. Nonetheless, findings from the current study highlight the notable portion of youth who fall in this category. This is particularly important to consider because reports more reliably included information on factual understanding than rational appreciation. As noted, evaluators may not include discussion of rational appreciation because the youth has already clearly demonstrated deficits and it does not necessarily indicate the topic was not considered and assessed by the evaluator. However, it does mean no information was presented to the trier of fact in the written report. Table 4 includes the rates of missing information for each topic area. It may be helpful for evaluators to consider if and how they include information on different competence areas for different youth. Although evaluators may reasonably conclude a competency interview with an impaired youth before fully assessing each aspect, it may still be helpful to clearly document their conclusions about a youth’s current abilities in each of the four relevant capacities. In the current sample of reports, given the high rates of missing information in some areas (e.g., continuance verdicts, the youth as decision-maker), it is unclear if and how they were assessed. Evaluators and those supervising the evaluation process may find it helpful to consider their own practices in addressing these areas in the written report.
Finally, results also highlight the importance of providing education in the evaluation process. Evaluations of AC focus on the youth’s ability or capacity to meet the functional demands (Kruh & Grisso, 2009) and not necessarily their current factual knowledge. In the current study, large proportions of evaluated youth benefited from education on processes (e.g., plea bargains, continuance without a finding) and roles, including that of the prosecutor. Evaluators should be prepared to provide this type of education and assess the impact via the youth’s subsequent understanding and appreciation.
Footnotes
Authors’ Note:
Thanks to Dr. Thomas Grisso and Dr. Ivan Kruh for their helpful review and formative input on early drafts of this manuscript