
Abstract
Decades of research suggest certain risk factors, including individual characteristics, increase an individual’s likelihood of being victimized. Measuring these risk factors then becomes crucial for movement forward in victimology. Recent research suggests the increasing need to measure the concepts of sex assigned at birth, gender identity, and sexual identity, all of whom have been linked to risk of victimization. However, it remains to be seen how these concepts are currently being measured, how their measurement has evolved, and if these concepts are being measured regularly, especially in large-scale national data efforts. This study seeks to examine the changes, or lack thereof, in measurement of the concepts of sex, gender identity, and sexual identity in seven major social surveys used in victimology research. Changes to wording, responses, and the number of questions regarding each of these concepts is discussed along with suggestions for improving measurement and implications for victimization research.
Introduction
Concerns over measurement, operationalization, and methodology have always been a part of victimization research, and more broadly, research in criminal justice and criminology. The ability to collect more individualized and nuanced data has increased over time due to technological and computational advancements, and so have the calls for more inclusive data collection methodologies (see Magliozzi et al., 2016; Saperstein & Westbrook, 2021; Sullivan, 2020). Data that are representative of multiple populations, especially underrepresented populations, are crucial to the progress of research in victimology. Studies have shown that underrepresented populations including sexual and gender minorities (SGMs) are at an increased risk of experiencing victimization (for examples see; Martin et al., 2011; Porter & Williams, 2011; Snyder et al., 2018; Walters et al., 2013). A sexual minority often refers to a person whose sexual identity is something other than heterosexual or straight, such as gay, lesbian, bisexual, queer, pansexual, or asexual, among others (Aspinall, 2009). A gender minority is commonly defined as someone who identifies as transgender, gender nonbinary, gender fluid, or some other identity than the gender corresponding with their sex assigned at birth (Wade & Ferree, 2015). Major theories in victimization such as routine activities theory and lifestyles theory both acknowledge the role of individual characteristics in determining victimization risk (Cohen & Felson, 1979; Hindelang et al., 1978). Given that 5.6% of adults in the United States identified as a SGM in a recent survey (Jones, 2021), adequately capturing the diversity within these populations should be an integral part of measurement, especially among national and longitudinal data sets seeking to examine risk factors, correlates, and outcomes of victimization.
Although many one-time, cross-sectional, victimization studies have begun to embrace SGM inclusivity (see DeKeseredy et al., 2021; Edwards et al., 2015; Langenderfer-Magruder et al., 2016; Martin et al., 2011; Porter & Williams, 2011; Ray et al., 2021; Walters et al., 2013), it is yet to be examined if larger data efforts, including multiyear national-level data collection, are following suit and measuring these concepts. A few studies (Aspinall, 2009; Westbrook et al., 2021; Westbrook & Saperstein, 2015) have examined major surveys to determine how gender, sex assigned at birth (hereafter referred to as “sex”), and sexuality have been conceptualized and measured over time. Although none of these studies focused on victimization, they serve as a guiding framework for how major surveys are measuring these vital concepts. Thus, this study builds on this research to examine seven major surveys that include measures of victimization to see how the concepts of sex, gender identity, and sexual identity are currently measured, and how they have evolved over time. These changes, or lack thereof, are discussed in the context of victimization research and possible future directions for measurement.
While variation in definitions of the key concepts of (sex, gender identity, and sexual identity) exist across disciplines, there is a general consensus in how they are broadly defined. Sex is typically defined as male or female sex that is assigned to a child at birth and documented on one’s birth certificate, commonly based on the child’s external genitalia (American Psychological Association [APA], 2015). “Intersex” is an umbrella term adopted in the 90’s to include individuals whose sex traits or reproductive anatomy do not fit into the male/female dichotomy, although it is important to note that many individuals who are intersex are assigned male or female sex at birth (see InterAct.org, 2021). “Gender identity” is commonly defined as the internal feeling or self-identification of one’s gender, such as male, female, or gender nonbinary among others, which may, or may not correspond with sex (Wade & Ferree, 2015). “Transgender” is commonly understood to represent those whose gender identity does not align with their binary sex category (Wade & Ferree, 2015). For example, someone assigned male at birth who identifies as a woman, or a transwoman, would be considered transgender. Related, “cisgender” refers to those whose gender identity aligns with their sex assigned at birth. Finally, “sexual identity” generally refers to a person’s self-identification derived from their sexual and/or emotional attraction to another person, such as heterosexual, lesbian, gay, bisexual, or asexual (APA, 2015; Aspinall, 2009).
Literature Review
Opportunity Theories of Crime and Individual Characteristics
The most commonly studied theories in victimization research are Cohen and Felson’s (1979) routine activities and Hindelang et al., (1978) lifestyles theories. Both theories have similar foundations, asserting that victimization is most likely to occur when there is a convergence in time and space of key factors including proximity to motivated offenders, exposure to risky environments, target attractiveness, and the lack of capable guardians (Cohen and Felson, 1979; Hindelang et al., 1978). Demographics and individual characteristics, such as sex, age, race/ethnicity, and other factors, are thought to influence the lifestyles individuals lead and the activities they engage in, which in turn are thought to differently expose individuals to risk of victimization.
Recently, victimization research has turned to explore in-depth differences among specific demographics that may influence lifestyles and activities, including differences in victimization risk by gender and sexual identity. Specifically, risk among individuals who are transgender and distinctions within sexual identity outside of the “gay/straight” binary have been examined. However, this research remains difficult without large-scale data sets that measure these concepts. The current existing research demonstrates the importance of measuring and exploring these concepts within victimization research. Although full review of the literature in the areas of sex, gender identity, and sexual identity in victimization is outside the scope of this paper, a summary of research in these areas concerning victimization is discussed to highlight the significance of measuring these concepts.
Sex Assigned at Birth and Gender Identity
There is no shortage of research examining disparities in victimization risk based upon sex. For decades, studies in victimology have examined differences between males and females, finding that females are at higher risk for experiencing sexual victimization, stalking, and intimate partner violence (IPV), while males are at higher risk for assault and robbery (see Cass, 2007; Fisher et al., 1998; Krebs et al., 2007; Snyder, 2015; Snyder et al., 2018). However, historically, these studies have not taken into account the potential difference in risk for variations in sex and gender identity. It is almost automatic to ask a question about binary sex in a victimization survey (e.g., male, female), but not as common to include a question on gender identity. This is possibly due to the common assumption that these constructs are the same (i.e., males always identify as men and females always identify as women).
However, recent research provides evidence that the assumption of sex and gender identity as always being identical is misguided, with estimates of around 1 million Americans identifying as transgender (Meerwijk & Sevelius, 2017). Furthermore, Cantor and colleagues (2019) reported that 1.7% of college students identified as transgender or gender nonbinary, suggesting a significant number of people do not identify as having a cisgender gender identity. Even though these estimates may seem small and thus not significant enough to measure, these populations still encompass millions of individuals, suggesting that while a large proportion people identify as cisgender, measuring these concepts distinctly is still vital. These findings coupled with the results from Westbrook and Saperstein (2015) provide clear evidence for issues related to the measurement of gender identity and sex. Specifically, many surveys are still treating the concepts of sex and gender identity as synonymous, with gender identity seen as something that is static for an individual and readily apparent for all people (Westbrook and Saperstein, 2015). Alternatively, even if researchers acknowledge the difference in these concepts, time, survey costs, and other constraints may hinder the addition of these questions (Smyth & Olson, 2020).
These issues have several ramifications directly related to the future of victimization research. Confounding the terms of sex and gender identity muddies the waters for understanding who might be at greatest risk of experiencing victimization. Indeed, more recent studies that have included measures of both sex and gender identity have found differences in risk. For example, Griner et al. (2020) used a pooled sample of over 80,000 college students and found that transgender students were significantly more likely to experience sexual victimization and have been in a sexually abusive relationship compared to cisgender students. Martin-Storey et al. (2018) used a sample of over 4,200 college students and found that students who were transgender or gender nonbinary reported higher rates of sexual harassment and unwanted sexual behavior (47% and 28%) compared to cisgender men (20% and 8%) and women (32% and 18%), respectively.
Furthermore, in a meta-analysis with 85 articles that examined IPV in transgender populations, Peitzmeier and colleagues (2020) reported that transgender individuals were between two and three times more likely to experience IPV compared to cisgender individuals. Other studies have reported similar results using various transgender samples and victimization types including IPV, sexual assault, stalking, and other forms of violence (see Coulter et al., 2017; Garthe et al., 2021; Hoxmeier, 2016; Johnson et al., 2016; Whitton et al., 2019 for examples). Overall, it is clear based on these studies that differences in victimization risk exist by sex and gender identity.
It is important to note that of the studies that used national level data, such as Griner et al. (2020), the number of students who identified as transgender was only 204, highlighting the importance of the need for large-scale studies to measure these concepts to allow for any meaningful statistical comparison. In addition, Coulter et al. (2017) combined multiple years of data to achieve a sample size of 177 transgender individuals. Peitzmeier and colleagues (2020) also highlighted this issue in their discussion noting, “. . . few studies examined demographic correlates of IPV within transgender communities. Twenty-eight unique data sets had more than 150 transgender participants and could support subgroup and risk factor analyses” (p. e11). In other words, few data sources existed that allowed for any subgroup statistical analysis. A common response to this issue has been to combine transgender, a gender identity, with sexual identity, creating a single “SGM” category. While this research has provided important insight into the victimization among transgender and sexual minority populations, it does not allow subsample analysis to unpack differences in risk that may exist within these populations. Thus, large-scale data are needed to fully understand nuances that may exist.
Finally, much of the research with larger samples that has been published in this area focused on college students (Coulter et al., 2017; Griner et al., 2020), largely ignoring the general population. However, the limited research that has been conducted on victimization among specifically transgender populations often finds a higher risk than their cisgender counterparts (Brown & Herman, 2015). This may be due to college-level studies adding questions related to sex and gender identity earlier than other surveys more focused on the general population.
Sexual Identity
Another demographic measure that has started to gain traction in victimization research is sexual identity, supported by research that suggests a growing number of people now identify as a sexual minority. For example, Cantor and colleagues (2019) reported that nearly 17% of college students identified as gay, lesbian, bisexual, asexual, queer, or questioning. A recent Gallup poll found that among adults in the United States, 5.6% identified as lesbian, gay, bisexual, or transgender (LGBT; Jones, 2021). Considering this, several victimizations studies have started to include a sexual identity variable in some form, and this concept may be further along in measurement than sex and gender identity.
Research suggests that the inclusion of sexual identity is an important factor when considering victimization risk. Several studies have found differences in risk of IPV among sexual minorities (Edwards et al., 2015; Martin et al., 2011; Porter & Williams, 2011; Walters et al., 2013; Whitfield et al., 2021) reporting that those that identified as a sexual minority were at higher risk for experiencing IPV compared to their heterosexual peers. Similar results have been reported for other types of victimization including sexual assault, physical assault, stalking, and other forms of violence, finding that individuals who identified as a sexual minority often experienced victimization at higher rates than their heterosexual counterparts (Bender & Lauritsen, 2021; Davis et al., 2021; Johnson et al., 2016; Kammer-Kerwick et al., 2021). The message from these studies is clear: victimization research needs to consider sexual identity when examining risk, and considering policy and prevention.
Current Study
Overall, a growing body of research suggests that including SGM variables is vital to the advancement of victimization research. Thus, this study seeks to examine how several major social surveys have measured the concepts of sex, gender identity, and sexual identity in the past and how these concepts may have changed over time. This study has three major goals. First, using the work of Westbrook and Saperstein (2015) as a guide, seven major surveys that included victimization variables were selected to examine the measurement of sex assigned at birth, gender identity, and sexual identity. Second, each of these surveys was examined in detail to explore how each of these concepts has been measured over time including any changes to these concepts in terms of wording, options, and count. Third, this information will be discussed and used to guide future survey development in the area of victimology.
Method
The seven surveys were identified from the Inter-university Consortium for Political and Social Research’s (ICPSR) data on the most frequently downloaded data sources, providing a list of top-utilized surveys. Surveys were selected based on their potential impact, given the frequency of their use in the area of victimization, acknowledging this is not an exhaustive list of surveys, especially outside of the United States, that could have been included. The names of the surveys included were the National Survey of Adolescent Health (Add Health), the National Crime Victimization Survey (NCVS), the National College Health Assessment (NCHA), the General Social Survey (GSS), the Youth Risk Behavior Surveillance System (YRBSS), the Crime Survey for England and Wales (CSEW), formerly known as the British Crime Survey (BCS), and the National Intimate Partner and Sexual Violence Survey (NISVS). The GSS was the longest running survey starting in 1972, while the most recent survey, the NISVS, started in 2010.
Surveys were selected based on the following criteria: (1) the use of a national or large-scale sample; (2) the survey is currently still being administered or was not discontinued; (3) the survey included questions directly related to measuring victimization; (4) the survey had been administered at least twice; (5) the survey was tied to an organization that is in charge of its administration (e.g., Centers for Disease Control and Prevention [CDC], American College Health Association [ACHA], U.S. Census Bureau). The surveys did not have to be solely focused on victimization to be selected, but did have to include at least two questions devoted to measuring some form of victimization. For example, the YRBSS mainly focuses on youth health, but includes questions about bullying victimization and assault. General information for each survey was recorded including when the survey was first administered, how it is administered, and other general characteristics of the survey.
Procedure
Once selected, codebooks or the actual survey questionnaire for each year of the survey were obtained and coded by year for the three concepts (sex, gender identity, and sexual identity). The codebooks or survey questionnaires were obtained through multiple sources including survey websites when available, the ICPSR depository, and other online sources. In total, over 100 codebooks and surveys were analyzed spanning several decades. Each survey codebook or questionnaire was hand-coded for five data items: (a) how many questions in the survey directly measured sex, gender identity, and sexual identity; (b) the exact wording and responses for each of these questions including the original wording of questions from first survey administration; (c) any changes in wording and responses for these questions including the addition of new questions; (d) year of any changes made to these questions or responses; and (e) any additional references to sex, gender identity, or sexual identity throughout the survey. Each codebook or survey was examined in its entirety and this information was entered into an Excel spreadsheet, which was then used to summarize patterns and changes across surveys.
To locate these concepts, we used pre-existing conceptualizations of sex, gender, and sexuality as a guideline for inclusion. Manifest coding techniques (in this case, a keyword search) were employed to identify questions that attempted to explicitly measure the concepts. Keyword search terms included words and phrases such as, “sex, gender, sexuality, trans, woman, man, female, male, gay, lesbian, same-sex, straight, heterosexual, homosexual, intersex.” Most of the survey items were identified through this process, but some of the older surveys and codebooks were not searchable, so the entire document had to be examined by hand.
Table 1 includes general characteristic information for each surveys including the first and last years of administration, how often the survey is administered, the population under study, how the data are collected, and the organization responsible for administering the survey. All of the surveys were national level, with one survey (the CSEW) taking place outside of the United States. Most of the surveys contained an interview component, with the NCHA having one form of administration that takes place completely online and one in person.
Survey Characteristics
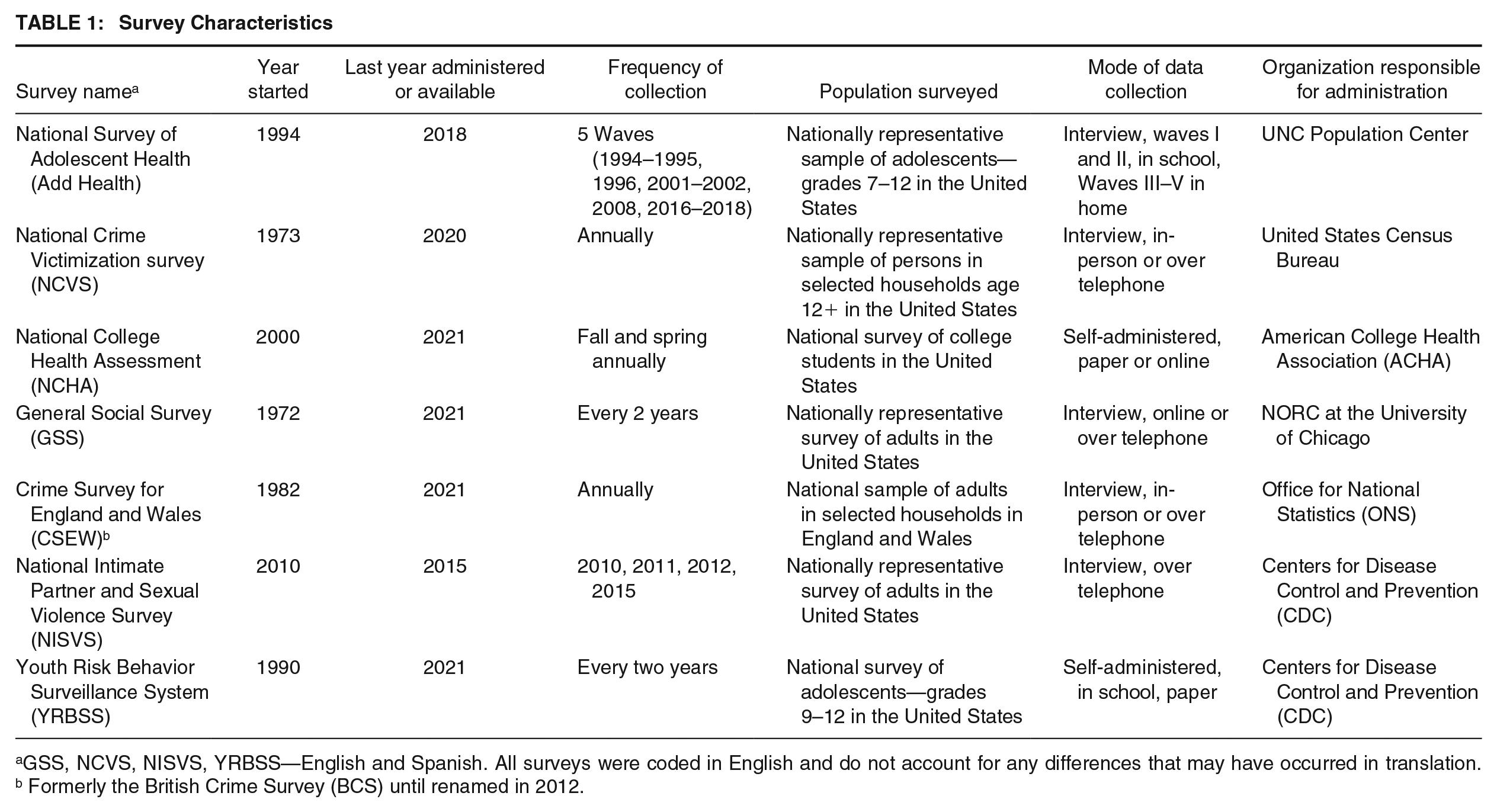
GSS, NCVS, NISVS, YRBSS—English and Spanish. All surveys were coded in English and do not account for any differences that may have occurred in translation. b Formerly the British Crime Survey (BCS) until renamed in 2012.
Results
The Measurement of Sex Assigned at Birth
All of the surveys examined included questions intended to measure sex from their inception. Table 2 provides the original wording for these questions, the current number of questions related to the concepts of sex, gender identity, and sexual identity included in each survey, and how wording for these particular questions has changed over time. The years and types of change are also noted. In general, specific question wording related to sex and changes to these questions over time varied by the survey. Typically, surveys included a question that simply said, “Code respondent sex,” (National Opinion Research Center [NORC], 1972, p. 35) or “What is your sex?” with the responses of “male” and “female” (ACHA, 2000, p. 8). None of the surveys contained other options such as “intersex” or “don’t know” the first year they were administered.
Measures of Sex Assigned at Birth, Gender Identity, and Sexual Identity Across Surveys and Time
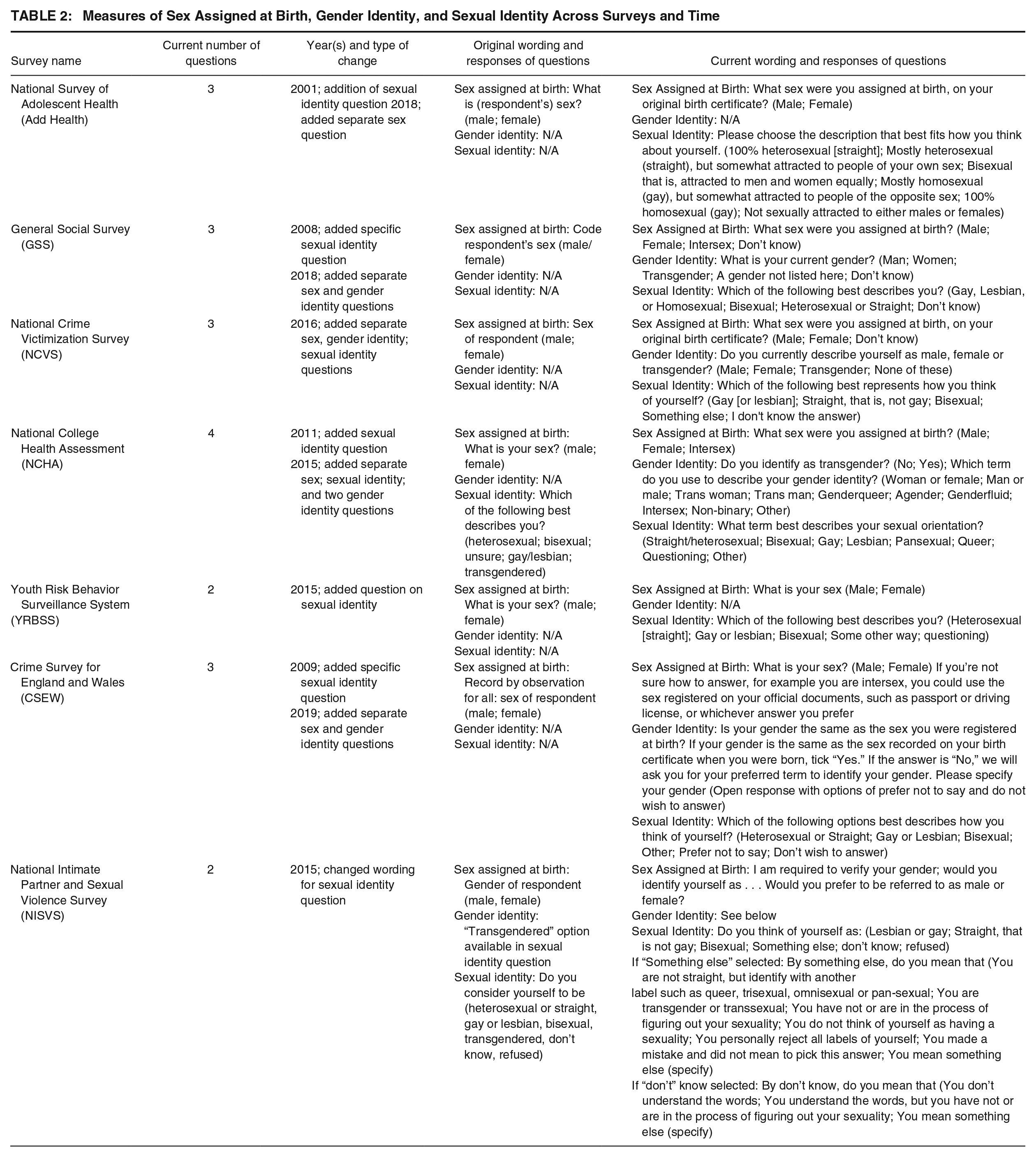
Notably, several surveys including the Add Health Wave I: In-Home Questionnaire administered in 1994 and 1995 had original wording for the interviewer to select the sex of the respondent instead of asking the participant directly with options of “male” and “female.” Interviewers were instructed to, “Ask if necessary” (Harris, 2018, p. 847). This was also true for the 1973 NCVS up until 2016, with the note of, “Ask if not apparent,” (United States Department of Commerce & U.S. Census Bureau, 2015, p. 2) and the CSEW, called the BCS at the time in 1982, specifically noted that the interviewer should, “Record by observation for all” (Home Office Research and Planning Unit, 1982, p. 52). The GSS starting in 1972 used similar phrasing of coding the respondents’ sex until 2014 when the wording used both the terms of “sex” and “gender” for this question asking the interviewer to “Select gender of chosen respondent,” but calling the variable “sex” in the codebook (NORC, 2014, p. 46). This wording changed again in 2018 when sex was separated from gender; however, the gender question included the variable name of (Sexnow) in the codebook, still confounding the concepts of sex and gender (NORC, 2018, p. 294). The NISVS also used the terms interchangeably with the phrase “Gender of the respondent” used to measure sex, and the options of “male” and “female” (CDC, 2011, pp. 2–3). In the 2008 version of the NCHA, the original “What is your sex?” question was replaced with one that asked, “What is your gender?” with the options of “female, male, and transgender” also confounding sex and gender identity (ACHA, 2008, p. 11). This changed in 2015 when the survey moved to four separate questions: one on sex, one specifically asking about identifying as transgender, one on gender identity, and one on sexual identity.
Overall, the specific wording of sex and gender identity questions changed the least across time with some surveys, like the YRBSS, not altering the wording of these questions at all. In addition, when compared to changes in questions directly related to sexual identity, sex questions also appeared to take a bit longer time to update, with the GSS not updating these questions to reflect a separation in sex and gender identity until 2018. This change occurred a few years earlier in the NCVS (2016), with the wording of “What sex were you assigned at birth, as on your original birth certificate?” (U.S. Census Bureau, 2016, p.8) and a year earlier in 2015 for the NCHA with the addition of wording reflecting sex assigned at birth (ACHA, 2015, p. 11). Overall, four surveys added wording related to sex assigned at birth or on a birth certificate, but only two surveys (NCHA, GSS) added the option of “intersex” for this question and two (GSS, NCVS) contained a “don’t know” or “refused” option. The NISVS took a different approach compared to the rest of the surveys in 2015. The sex question was reworded to say, “I am required to verify your gender, would you identify yourself as . . .,” then asking, “Would you prefer to be referred to as male or female?” confounding sex and gender identity (CDC, 2015, p. 18).
Within the Add Health Wave V: Mixed-Mode Survey administered between 2016 to 2018, they offered three choices for gender identity, “male, female, or unspecified” that mirrored options for self-reported sex, “male” or “female.” The Wave V codebook suggested that approximately 28 respondents in Add Health were included in the “unspecified” gender identity (Harris, 2018, p. 7). However, because the measure did not explicitly include expansive options for respondents and “unspecified” is not a gender identity, the survey is considered functionally as having only a single measure of gender that is still largely conflated with sex.
The Measurement of Gender Identity
None of the surveys included a question directly about gender identity from inception. However, the NISVS in 2010 did have a “transgendered” option in their sexual identity question (which will be discussed in the next section). The NCHA added a question on gender identity in 2015, when it stopped combining sex and gender identity into one question, the earliest of all the surveys. This question read, “Which term do you use to describe your gender identity” with the options of “woman, man, trans woman, trans man, genderqueer, or other identity” also with a box to specify something else (ACHA, 2015, p. 11). In addition, a question specifically about identifying as transgender was added with the options of “yes or no” (ACHA, 2015, p. 11).
In their most currently available versions, only four surveys (NCVS, NCHA, GSS, CSEW) included a question directly on gender identity and only the NCHA separated this into two questions. One asked respondents to describe their gender identity and another specifically asked if they identified as transgender. The selections for these questions also varied with the NCHA having the most options for this question; “woman or female, man or male, trans woman, trans man, genderqueer, agender, genderfluid, intersex, non-binary, or other” (ACHA, 2019, p.11). The other two had significantly fewer options; GSS—man, women, transgender, a gender not listed here, and don’t know; NCVS—male, female, transgender, and none of these (NORC, 2018, p. 294; U.S. Census Bureau, 2019, p.356; respectively).
Overall, the questions for many of the surveys remained unchanged until very recently with gender identity added in 2016 for the NCVS and 2018 for the GSS. The NCHA was the first to add a separate gender identity question in 2015. In 2019, the CSEW added a separate question on gender identity, asking “Is your gender the same as the sex you were registered at birth? If your gender is the same as the sex recorded on your birth certificate when you were born, tick yes. If the answer is no, we will ask you for your preferred term to identify your gender” (Office for National Statistics [ONS], 2019, p. 270). This was followed by a question for those responding “no” that asked, “Please specify your gender” with an open response box also including options of “prefer not to say” and “do not wish to answer” (ONS, 2019, p. 270). The NISVS combined the concepts of gender identity and sexual identity, and as of its last administration in 2015 did not contain a standalone question on gender identity. The remaining two surveys, Add Health and YRBSS, also did not contain questions at last administration (2018 and 2021, respectively) that directly asked about gender identity.
The Measurement of Sexual Identity
Perhaps the questions that saw the most changes in wording, options, and availability were questions related to sexual identity. Two surveys, the NCHA and the NISVS, included a question about sexual identity from their inceptions in 2000 and 2010, respectively. Original options for this question in the NCHA included, “Which of the following best describes you?” with the options of “heterosexual, gay/lesbian, bisexual, transgendered, or unsure” (NCHA, 2000, p. 6). The original wording in the NISVS was as follows, “Do you consider yourself to be. . .” with the options of “heterosexual or straight, gay or lesbian, bisexual, transgendered, don’t know, or refused” (CDC, 2011, p. 72).
In their most recently available versions, all of the surveys included direct questions about sexual identity with inclusive options. Most of the wording of these questions was similar with the NCVS asking, “Which of the following best represents how you think of yourself?” (U.S Census Bureau 2019, p. 349) or “Which of the following best describes you?” from the GSS (NORC, 2018, p. 294) used as common phrasing. Again, the NCHA had the most response options for this question: “straight/heterosexual, bisexual, gay, lesbian, pansexual, queer, questioning, or other” (ACHA, 2019, p.11). It is notable that some surveys combined sexual identities, often not separating those who identified as lesbian from those who identified as gay. For example, the GSS listed the following options for sexual identity: “gay, lesbian, or homosexual, bisexual, heterosexual or straight, or don’t know,” with the selection of “gay, lesbian, or homosexual” as one option (NORC, 2018, p. 294). The YRBSS took a similar route with the options of, “heterosexual (straight), gay or lesbian, bisexual, or not sure” with gay and lesbian being grouped into one option (CDC, 2019, p. 16). The CSEW also combined gay and lesbian (ONS, 2019, p. 271). The NCVS had two separate sexual identity questions based on how the respondent answered the sex question. If “female” was selected then the options for sexual identity were, “lesbian or gay, straight that is not lesbian or gay, bisexual, something else, or I don't know the answer. For males, the same responses were given minus the lesbian option” (U.S. Census Bureau, 2019, pp. 7–8).
Furthermore, Add Health (starting at Wave III administered between 2001–2002, through Wave V, administered between 2016–2018) was the only survey that provided options that allowed the respondent to acknowledge they may not firmly fit into one category of sexual identity. These responses included, 100% heterosexual (straight), mostly heterosexual (straight), but somewhat attracted to people of your own sex, bisexual that is, attracted to men and women equally, mostly homosexual (gay), but somewhat attracted to people of the opposite sex, 100% homosexual (gay), not sexually attracted to either males or females with the question asking respondents to, “Please choose the description that best fits how you think about yourself” (Harris, 2018, p.116).
The NISVS took a distinct approach to both the location and wording of this question in its first administration. The question on sexual identity was located in a “relationships” section at the end of the survey, not with the rest of the demographic questions. It was not moved until 2015 when it was placed in the demographic section. In addition, this question combined the concepts of sexual identity and gender identity asking, “Do you consider yourself to be. . .” with the options of, “heterosexual or straight, gay or lesbian, bisexual, transgendered, don’t know, or refused” (CDC, 2010, p.72) in its original survey from 2010. This changed in 2015 when a series of new questions were added. The first question read, “Do you think of yourself as. . .” with the options of “lesbian or gay, straight, that is not gay, bisexual, something else, don’t know, or refused.” If “something else” was selected by the respondent they were asked, “By something else, do you mean that. . .” with the options of, you are not straight, but identify with another label such as queer, trisexual, omnisexual or pan-sexual, you are transgender or transsexual, you have not or are in the process of figuring out your sexuality, you do not think of yourself as having a sexuality, you personally reject all labels of yourself, you made a mistake and did not mean to pick this answer, you mean something else (specify). If “don’t know” was selected by the respondent, they were then asked, “By don’t know, do you mean that . . .” with the options of, “you don’t understand the words, you understand the words, but you have not or are in the process of figuring out your sexuality, you mean something else (specify)” (CDC, 2015, p.5). This is the only survey that used this multistep approach to seemly attempt to measure sexual identity and get at gender identity through the inclusion of a transgender option.
Discussion
Summary of Results
Overall, every survey made some change in wording, the number of responses, or amount of survey questions regarding sex, gender identity, and sexual identity. The YRBSS had the least number of changes, adding one question on sexual identity in 2015. The NCHA arguably had the most changes, consistently adding more response options to questions and adjusting wording to questions. It also was one of the first in 2015 to add separate questions on sex and gender identity. Other surveys, such as the NCVS, Add Health, GSS, and the CSEW took longer for this separation (2016, 2018, 2018, and 2019, respectively). Surveys tended to add questions on sexual identity first (as early as 2001 in Add Health) and then add questions on gender identity later. While the surveys have made advances in measuring these concepts, concerns and room for improvement remain, especially when considering the role these factors may play in explaining differences in victimization risk.
Implications and Recommendations
These findings have several implications for future research in victimization. First, surveys should include separate measures of sex, gender identity, and sexual identity. Smaller scale studies have found that SGM individuals are often at higher risk for experiencing victimization when compared to their non-SGM counterparts. However, these studies often cannot conduct subsample statistical analysis due to small sample sizes. This not only erases these identities as separate, but also presents the assumption they are uniform in risk, introducing bias into measurement. The measurement of these concepts in larger studies can potentially solve these issues, allowing for a more exact analysis of potential disparities in victimization.
The ACHA provides an example of how some larger-scale surveys have adapted to achieve this goal, providing evidence that this is a necessary change. Snyder et al. (2018) using ACHA data found that male college students who were gay were more than three and a half times (3.61) and females who were bisexual were over two times more likely to experience sexual assault than their heterosexual counterparts. This demonstrates the potential impact these larger data sets can have in examining risk that is more specific, allowing for analysis that separates sexual identity, rather than having to combine it into one or two categories.
Currently, several surveys including the GSS, NISVS, CSEW, and the YRBSS combine the identities of gay and lesbian into one survey selection, which makes it difficult, if not impossible, for any analysis among individuals without making assumptions and compromising validity (e.g., only males identify as gay). This is evidenced by two recent studies that used the NCVS and YRBSS. Violent victimization rates in NCVS data were found to be higher for gay and lesbian individuals (38.6 per 1000) compared to heterosexuals (19.4 per 1000); (Bender & Lauritsen, 2021) and Johns and colleagues (2020), with YRBSS data, reported that students who were lesbian, gay, or bisexual, were at significantly greater risk of violent victimization when compared to heterosexual students. However, it is unknown if the rates would differ between gay and lesbian individuals or if one group was driving the victimization rate, since these were combined in measurement. Thus, surveys like the GSS, NISVS, and the CSEW, should separate sexual identity categories and should not tie them to questions about sex (e.g., NCVS and YRBSS). They should also expand the number of options available (for example, the addition of queer, pansexual, or unsure/questioning options) to better reflect different types of sexual identity and allow for analysis within these groups. Considering it is not uncommon to make changes to measurement, as was frequently found, and this would not require additional questions, these are simple changes that could be made to these surveys.
Second, although great strides have been made in many of the surveys examined, there are still concerns that exist, especially with gender identity. Not all of the surveys contained a question on gender identity. The YRBSS also did not include a question on gender identity, severely limiting the ability to examine how transgender and nonbinary youth may or may not differ in victimization risk from their cisgender peers. Furthermore, Add Health, arguably one of the most well published data sets across the social sciences, still does not include an inclusive question on gender identity, limiting its ability to examine this important demographic in terms of specific victimization risk.
Based on these findings, it is imperative to separate the constructs of sex and gender identity. As noted by Sullivan (2020), without this separation, “we lose the ability to understand differences and to design evidence-based policies tackling problems facing girls and boys, women and men” (p. 522). Separating sex and gender identity can allow an important distinction to be explored in victimization research; the examination of differences in risk by these two concepts. It may be that victimization risk is impacted more by one demographic (e.g., sex) than the other, or that they both contribute to risk. Furthermore, the distinct measurement of each concept potentially allows for the analysis of variations in outcomes such as mental health, substance abuse, and other negative impacts often experienced by victims. Then, as argued by Sullivan (2020), this data can then be used to inform policy, prevention, further research, and provide vital information for practitioners.
Second, at a minimum, surveys should include a question asking if a person identifies as transgender, ideally as a separate question solely focused on gender identity including other options such as nonbinary. Transgender should not be included as an option in questions that ask about sexual identity. Taking a two-step approach to sex and gender may be the most accurate way to capture these concepts. Saperstein and Westbrook (2021) tested different types of measures to capture gender identity and sex, finding that measuring these concepts with a two-step approach offered the most detail; first asking about sex at birth, then a follow-up question about gender. This is also the recommendation of the Gender Identity in U.S. Surveillance (GenIUSS, 2014) group; they suggest a two-step approach, with the first question asking about sex and the second asking about current gender identity (acknowledging that gender identity might be fluid) with suggested response options of “male, female, trans male/trans man, trans female/trans woman, genderqueer/gender non-conforming, or different identity (please state)” (p. 3). The addition of these variables can allow for important research questions among the transgender community to be examined. Namely, are there differences in risk among those within the transgender community? Research has found transgender people to be at high risk of victimization (e.g., Peitzmeier et al., 2020), but often lacked the ability to examine subgroups within this population. Consistent inclusion and measurement will allow for this comparison, adding to the literature and potential policy recommendations in this area.
Third, the notion that gender identity might be fluid or change over time, presents another challenge to researchers trying to measure this concept. One suggestion to address this issue is including scales or gradations to capture femininity and masculinity in terms of gender expression. Gender expression includes our appearance, gender roles, emotional expression, and behaviors (Hoffman, 2001). Notably, an individual’s gender expression does not always align with their gender identity (Tabler et al., 2021). Gender expression scales typically provide a range and allow the respondent to select how masculine, androgynous, and/or feminine they see themselves (Wylie et al., 2010). Often recommended as two items, these scales first attempt to capture how the respondent sees themselves and the second attempts to capture how most people see them on a scale that ranges from “not at all” feminine to “very” with the same options for masculine and androgynous (Magliozzi et al., 2016; Saperstein & Westbrook, 2021). Add Health did include a single-item measure of gender expression measured at Wave V with Tabler et al. (2021) finding that 2% of cisgender men and 6% of cisgender women reported a gender expression that was androgynous or gender nonconforming. Another option is to allow respondents to place themselves on a wider continuum like the one used in Bittner & Goodyear-Grant, (2017) with masculine and feminine poles ranging from 0% to 100%.
The inclusion of more continuous measures of gender expression can add nuance to our understanding of gender diversity (Tabler et al., 2021). When interacting with others, we often do not know others’ identities, instead relying on externalized cues in the form of expression such as speech, appearance, and behavior to make assumptions about someone’s identity. Thus, some forms of victimization, such as hate crimes, may be rooted more in expression than identity (Tabler et al., 2021). Victimization in schools, for example, has been shown to be affected by an individual’s gender expression (Gordon et al., 2018), and even among cisgender identifying individuals, higher scores of gender expression nonconformity were correlated with higher levels of everyday discrimination (Tabler et al., 2021).
Finally, questions on sexual identity should seek to be as inclusive as possible with response options. This would include not combining any identities, such as gay and lesbian and offering more response options such as pansexual, asexual, and queer. In the United Kingdom context, for example, it is common to see response options limited to heterosexual/straight, gay/lesbian, bisexual or other (see Aspinall, 2009). The Williams Institute provides a recommendation on how to measure sexual identity inclusively. They suggest three different questions, one asking about sexual identity (e.g., gay, lesbian, bisexual, queer, etc.), one asking about sexual behavior (e.g., the gender or sex of sex partners), and one on sexual attraction (e.g., who they are attracted to; Badgett, 2009). In addition, similar to the notion that gender identity is fluid, it should also be acknowledged that sexual identity can be fluid. Surveys could address this issue by including wording that asks the respondent how they “currently” identify, recognizing that this may change. Furthermore, for panel or longitudinal surveys, questions on current sexual identity and gender identity could be asked with each administration to document any changes that may occur with these identities. This information could then be used to further examine how victimization risk may change over time across and within identities. These questions should be placed in the demographics section of the survey. In some surveys, such as Add Health, sexual identity is included in sections on sexual activity and other behavioral health questions. Someone’s sexual identity can vary extensively from sexual behavior and sexual partners. Placing expansive gender and sexual identity questions in demographics sections is an inclusive practice that reaffirms the centrality of these concepts to people’s self-perceptions, alongside variables like race/ethnicity and age, avoiding the tendency to conflate identity with behavior.
One additional suggestion similar to gender identity is to add gradation scales that allow for respondents to identity on a scale where they may fall. The only survey in the current study that included something like this was Add Health, with the addition of percentages and variation (e.g., 100% heterosexual [straight], mostly homosexual (gay), but somewhat attracted to people of the opposite sex) in their sexual identity question (Harris, 2018). Further complicating the issue is how attraction relates to sexual identity. Individuals may identify as heterosexual, yet experience same-gender attraction, and these people would not be identified with a singular measure of sexual identity, suggesting multidimensional scales may be needed (Aspinall, 2009; Wolff et al., 2017). Adding questions to address identity, attraction, and sexual behavior can help to unpack these relationships.
It is acknowledged that researchers may still need to combine categories or response options when doing analyses but allowing for the measurement of these concepts can help SGM individuals not to feel “erased” and encourage representation. Oversampling, or intentionally sampling to include a specific population (Vaughan, 2017), may be one way to mitigate this issue. Larger surveys are more likely to have the resources to target these populations to diminish potential sample size issues. One way oversampling can be conducted is through screen questions. Victimization surveys, such as the NCVS, often use these types of questions to “screen” participants into different parts of a survey. Similarly, a survey design could contain a component that asks survey participants a preliminary screen question about their sexual and gender identities, continuing to survey until a threshold or quota of SGM individuals are reached. Participants that identify as cisgender or heterosexual could be screened out after reaching the threshold, allowing more data collection for SGM individuals expending fewer resources. It may also be possible to “pool” estimates across years in surveys (Daigle et al., 2016), as long as the measurement has stayed the same, to obtain larger samples sizes as utilized in Griner and colleagues (2020). Finally, Kalton (2009) suggested sharing costs across surveys, something the CDC could easily do among the numerous surveys it conducts each year. Considering large-scale data efforts often serve as a bell-weather for other research, these surveys have the opportunity to set the standard for how the concepts of sex, gender identity, and sexual identity are measured.
One major and ongoing barrier, however, is that survey sample weights are often based on population estimates generated from federal data; yet some of these data resources do not include inclusive gender and sexuality measurements. For example, the U.S. Census Bureau (2020) ultimately decided to exclude gender and sexual identity measures in the 2020 census, only capturing cohabiting same-sex couples. It is critical that researchers endorse adoption of inclusive measures and encourage federal organizations to adapt their instruments. Additional research is also needed to explore the measurement of these concepts in additional cultures, languages, and countries. Only one survey that originated outside of the United States was included in the current study, limiting the ability of generalization to other countries. The comparison of surveys originating from other countries, especially those that do not have English as their primary language, may provide further insight into cultural differences in these concepts and their measurement. It may be that other countries are ahead of the United States in measurement of these concepts (see Aspinall, 2009; Sullivan, 2020), or that similar problems exist, providing a fruitful avenue for future research.
Conclusion
As victimization research continues to advance, so must the ability to measure more specific inclusive variables, especially among groups shown to be at high risk for victimization, such as SGM individuals. This effort should be led by large, national-level data sets, to achieve the ability to examine risk across and within SGM individuals. The current study examined the change in measurement of sex, gender identity, and sexual identity across seven major surveys, finding that many of the surveys are making headway in measuring these concepts. However, concerns remain in many of these data sets including the confounding of variables, the exclusion of gender identity, and the lack of options in sexual identity.
Footnotes
Authors’ Note:
Carlos M. Gonzales is now in the Department of Sociology & Criminology at Pennsylvania State University. We have no conflicts of interests to disclose.