
Abstract
As the COVID-19 pandemic has spread and continued, much attention has been focused on the physical costs of the virus. That said, early research has also demonstrated an impact on mental health, including depression. At the same time, there has been a documented increase in hate crime victimization during the pandemic. Importantly, hate crime victimization—and fear of victimization—has also been demonstrated to increase depressive symptoms. Following this, we posit that hate crime victimization, and fear of victimization, may play a significant role in COVID-19-related depressive symptoms. We test these hypotheses using results from a sample of 3,117 participants who responded to a survey administered in May 2020. Results indicate that not only do a higher perceived personal risk of COVID and experiences with hate crime predict higher depressive symptoms but that hate crime experiences mediate the relationship between perceived risk of COVID and depressive symptoms.
The novel coronavirus disease (COVID-19) was declared a global pandemic by the World Health Organization (WHO) in March 2020. Since this declaration, the pandemic has continued to spread, infecting over 250 million worldwide and resulting in the deaths of more than 5.4 million people (WHO, 2022). While the pandemic is still ongoing at the time of this writing, the deleterious impacts of the pandemic will likely continue long after the disease itself has subsided. Fear of the disease, changes to individual plans for the future, financial losses, mandatory lockdowns, and a host of other factors are likely to continue for some time and may have a significant negative impact on individual mental health, exacerbating anxiety and depression (Bueno-Notivol et al., 2021; Ettman et al., 2020).
Concurrent with the growth and spread of the pandemic has been the spread of fear-related bigotry and prejudice. As the virus initially spread, prominent political figures, including former President Donald Trump, blatantly ignored WHO guidelines for avoiding disease-related stigmatization and disparagingly referred to the disease as the “Wuhan virus,” the “Chinese virus,” and the “Kung Flu.” Recognizing the potential political legitimization effect—and other negative impacts—of this rhetoric, the Federal Bureau of Investigation (FBI) issued a warning regarding an anticipated increase in hate crimes against Asian Americans. Others have suggested that these effects are likely to reverberate to other racial and ethnic groups as well, as pandemic-related fears serve to exacerbate in-group/out-group divisions and facilitate prejudices (e.g., Van Bavel et al., 2020). Indeed, early research has indicated that reported hate crimes, which are criminal offenses motivated, in whole or in part, by bias or prejudice against an individual because of their race, religion, gender, sexual orientation, or other group characteristic, have been occurring at an alarmingly high level during the COVID-19 pandemic (Gover et al., 2020; Lantz & Wenger, 2020; Tessler et al., 2020). Even those who do not experience hate crime victimization frequently report that they know someone who has been victimized or report changing their own behavior to avoid victimization (Lantz & Wenger, 2020). Unfortunately, prior research has also demonstrated a robust relationship between hate crime victimization—both direct and vicarious—and depression as well (e.g., Bell & Perry, 2015; Craig-Henderson & Sloan, 2003; Herek et al., 1997).
In summary, a growing body of research has indicated a direct association between the COVID-19 pandemic and (a) reported mental health issues, including depression and (b) bias-motivated victimization. At the same time, a separate body of research has demonstrated a similar significant association between hate crime victimization and negative mental health symptoms. If both the pandemic and hate crimes are independently related to negative mental health symptoms, but the pandemic has itself also led to increases in hate crime, it follows that hate crime victimization and fears of such victimization play an important role in explaining and exacerbating the mental health consequences of the pandemic. Yet, these relationships have not been examined jointly. As such, in the current study, we seek to address this gap by considering the joint relationship between the COVID-19 pandemic, hate crime victimization, and individual mental health. Specifically, the present research examines three primary research questions. First, are concerns regarding the pandemic independently related to self-reported depressive symptoms? Second, are experiences with hate crime victimization and fear of hate crime victimization similarly related to depressive symptoms? Finally, do concerns about hate crime victimization partially account for, or exacerbate, any of the observed negative health consequences of the pandemic?
Background
Exposure to uncontrollable events has often been linked to depression (Kendler et al., 2003; Kendler & Gardner, 2016; Seligman, 1972). Prior research on disease outbreaks, in particular, has indicated that such events are associated with increased levels of depression (Hawryluck et al., 2004), and the scope of the current COVID-19 outbreak is unprecedented. Indeed, one meta-analysis of studies conducted during the COVID-19 pandemic by Bueno-Notivol et al. (2021) found a pooled prevalence rate of depression of roughly 25%, a rate significantly higher than the estimated prepandemic prevalence of depression. Another study conducted by Ettman and colleagues (2020) compared nationally representative data from surveys conducted before and during the pandemic, and found that the prevalence of depressive symptoms was higher in every category (e.g., medium, severe, etc.) during COVID-19, in comparison to before. These differences were, moreover, substantial such that the prevalence of depression symptoms was roughly threefold higher during COVID-19, increasing from a prevalence of 8.5% to 27.8%. These effects have been attributed to the widespread impacts of the pandemic, including individual health concerns, the unpredictability of the disease, the loss of individual freedoms, changes in future plans, social distancing and social isolation associated with mandatory lockdowns, conflicting information, and financial loss, among others factors (e.g., Brooks et al., 2020; Bueno-Notivol et al., 2021; Huremović, 2019; Kawohl & Nordt, 2020; Marroquín et al., 2020; Pfefferbaum & North, 2020; Shigemura et al., 2020).
COVID-19 and Hate Crime Victimization
At the same time, research and other figures have suggested that the COVID-19 pandemic has had significant impacts on prejudice, bias, and hate crime victimization in the United States as well (see Tessler et al., 2020). High-profile incidents of bias victimization have been documented across the country. In Texas, for example, one man stabbed a Burmese American family because he thought they were Chinese and infecting people with the coronavirus. One of several documented incidents in New York involved a man who poured acid on an Asian woman; in another incident, a Korean woman was punched in the face (Lee & Yadav, 2020). Corroborating these reports as indicative of a more general phenomenon, Asian American organizations like the “Stop AAPI Hate” forum have recorded hundreds of instances of anti-Asian hate crimes (Jeung et al., 2021; Jeung & Nham, 2020; Ren & Feagin, 2021).
Researchers have offered several explanations for these hate crimes, including the role of scapegoating, wherein individuals respond to the threat of disease by “othering” that threat (Muzzatti, 2005; Reny & Barreto, 2022). The perpetration of hate crime, in particular, is frequently used to “do difference” or “other” potential hate crime victims. Specifically, this literature posits that hate crimes extend marginalization against those who are perceived as different (Perry, 2001). This research has also suggested that the state can facilitate and legitimize hate crimes by enabling a divisive political environment through the use of inflammatory rhetoric (Koopmans & Olzak, 2004; Piatkowska & Lantz, 2021), like that espoused by Trump. Most explanations and mechanisms, however, are rooted in fear in some way or another.
Prior research has suggested that the threat of disease is associated with heightened fear and increases in ethnocentrism and intolerance toward out-groups (Faulkner et al., 2004; Van Bavel et al., 2020). Prejudice, moreover, tends to be exacerbated when fear is heightened (Clissold et al., 2020; Schaller & Neuberg, 2012). In this way, Clissold et al. (2020) argued that global health crises, like the current pandemic, have the unfortunate tendency of exposing and exacerbating existing societal prejudices (see also Gover et al., 2020). Following this, some scholars have argued that these recent increases in hate crimes are unlikely to be exclusive to those targeting the Asian population but rather to extend to other racial and ethnic minorities as well (Wenger & Lantz, 2021a). This recent research observed, for example, that while social distancing practices related to lockdowns and other policies reduced the risk of hate crime victimization in general during the pandemic, this victimization risk was higher among racial/ethnic minority respondents who identified as essential workers and those who were unable to socially distance. As such, the profound impacts of the COVID-19 pandemic on discrimination and hate crime victimization have the potential to reverberate throughout not only the Asian American community, but other racial/ethnic minority populations as well, particularly those who continued to work or were essential workers during the pandemic.
Hate Crime Victimization and Depression Symptoms
Taken together, recent research has suggested that both individual depressive symptoms and the potential for hate crime victimization have increased during the COVID-19 pandemic. Importantly, however, other hate crime research has been devoted to the study of the unique harms associated with hate crime victimization, including increased depressive symptoms. Indeed, these unique harms are the primary justification for hate crime laws, which generally punish those who commit hate crimes more severely than those who commit other types of crime. This research generally argues that hate crimes, in comparison to other crimes, are associated with greater physical trauma (e.g., Lantz & Kim, 2019; Malcom & Lantz, 2021), broader community trauma (e.g., Bell & Perry, 2015; Iganski, 2001; Perry & Alvi, 2012), and—most important for the present research—psychological trauma (e.g., Fetzer & Pezzella, 2019; Herek et al., 1999). Herek et al. (2002) further noted that these impacts are not solely because of the excessive brutality associated with hate crimes; even minor forms of hate crime victimization can induce these negative psychological impacts given that such incidents suggest the possibility for further attacks in the future.
More specifically, research has shown that hate crime victimization is often associated with significant adverse consequences for victim mental health; hate crime victims report significantly more emotional and psychological distress, including depression, even compared with victims of other crimes (e.g., Craig-Henderson & Sloan, 2003; Herek et al., 1997, 1999; McDevitt et al., 2001; Tiby, 2009). Hate crime victims also frequently report significant fears of revictimization and often make changes to their behavior to avoid this revictimization (Craig-Henderson, 2009; D’Augelli, 1992; Herek et al., 1999; Pilkington & D’Augelli, 1995). These adverse symptoms also tend to be more intense in nature and to last longer than those experienced by other victims. Herek et al. (1997), for example, found that victims of anti-gay hate crime reported higher levels of depression up to 5 years after the primary victimization, compared with non-hate crime victims.
Other research has extended this consideration of psychological trauma, suggesting that hate crime victimization may have significant negative impacts on the larger community as well. In this context, prior research has described hate crimes as “message crimes,” which are intended to send a broader message of intimidation to both individual victims and those who identify with or share that victim’s same characteristics (Bell & Perry, 2015; Garcia et al., 1999; Iganski, 2001; Lim, 2009; Weinstein, 1992). Researchers have referred to these impacts more broadly as “in terrorem” effects (e.g., Iganski, 2001; Perry & Alvi, 2012; Weinstein, 1992). This research suggests that when individuals hear about an incident of victimization in which the victim was targeted because of some shared characteristics, they often exhibit symptoms similar to the primary victim (Herek et al., 1997). Learning that someone was targeted for an immutable characteristic that one shares can have a profound impact on mental well-being (Levin & McDevitt, 1993), and people who learn that someone was targeted because of shared characteristics, or membership in a shared social group, experience despair and depression (Craig-Henderson & Sloan, 2003). Put simply, when confronted with the victimization of others, one is confronted with the difficult truth that such an incident could have happened to anyone with those same targeted characteristics.
While quantitative studies on this topic are limited, a number of researchers have identified these impacts among focus groups or using qualitative interview techniques. Lim (2009), for example, conducted a series of interviews among Asian Americans and found that hate crimes had a significant negative impact on the Asian community at large, in that learning of anti-Asian incidents made respondents feel vulnerable and unsafe. Respondents similarly indicated more acute awareness of their own risk of potential victimization after hearing about community victimization. In another study, Noelle (2002) conducted interviews among a small sample of LGB (lesbian, gay, and bisexual) respondents following the notorious hate-motivated murder of Matthew Shepard. In conducting these interviews, Noelle identified a vicarious traumatizing effect; like those respondents in Lim’s (2009) sample, the respondents indicated an increased sense of vulnerability and risk following community victimization. More importantly, this sense of vulnerability was also accompanied by increases in respondents’ reported depression and reduced self-esteem. Some respondents even indicated that the murder of Shepard fundamentally challenged their perceptions of the “meaningfulness of the world and worthiness of self” (Noelle, 2002, p. 32). Most recently, Bell and Perry (2015) conducted focus group interviews among LGB community members and found similar effects, in that respondents indicated increased feelings of sadness, isolation, anxiety, and depression, among other emotions, after hearing about anti-LGB hate crimes.
Current Research
Taken together, research has suggested that (a) the breadth and scope of the COVID-19 pandemic are likely associated with individual depression; (b) the COVID-19 pandemic has been associated with similar increases in out-group prejudice and hate crime victimization; and (c) hate crime victimization is also associated with significant increases in individual depressive symptoms. As such, these patterns suggest a need to consider the joint relationship between the COVID-19 pandemic, hate crime victimization, and individual depression. Following this, the goal of the present research is to examine these relationships within the context of three primary research questions. First, are individual concerns regarding COVID-19 related to self-reported depressive symptoms? We hypothesize that greater perceived concern regarding COVID-19 will be positively associated with depressive symptoms (Hypothesis 1). Second, are experiences with hate crime related to depressive symptoms? We hypothesize that individuals who report hate crime experiences will report greater depressive symptoms than those who do not report such experiences (Hypothesis 2). Finally, do experiences with hate crime victimization partially account for, or exacerbate, the observed relationship between the COVID-19 pandemic and depressive symptoms? We hypothesize that experiences with hate crime will mediate (Hypothesis 3) and moderate (Hypothesis 4) the association between personal concern regarding COVID-19 and depressive symptoms.
Method
The data for this study come from an opt-in web-based survey designed to assess experiences with hate crime and prejudicial attitudes during the COVID-19 pandemic which was administered using Prime Panels by CloudResearch in May 2020 to 4,188 American adults throughout the United States. 1 CloudResearch is a research firm with access to more than 50 million participants throughout the world across various research platforms which each have their own participant pool. 2 CloudResearch determines inclusion criteria based on researchers’ sampling requests and then contacts potential participants via email or a dashboard if they fit the inclusion criteria. Participant compensation is determined by the particular research platform they are affiliated with (Cloud Research, 2020). The survey used in the current study was designed to be approximately representative of the U.S. population in terms of race/ethnicity and gender by using a targeted quota sampling strategy which ensured the sample reflected the U.S. population in terms of race/ethnicity according to the American Community Survey (ACS) 5-year estimates of the racial composition of the United States. We also included an oversample of an additional 300 Black, 300 Hispanic, and 300 Asian respondents to increase the racial/ethnic diversity of the sample. While not all questions included in the full survey are pertinent to the research at hand, respondents took an average of 15 min to complete the full survey. All study procedures were approved by the Florida State University Institutional Review Board and all participants received a statement of informed consent prior to taking the survey.
Survey data, in comparison to official data sources, have the advantage of including both those hate crimes that are reported to the police and those that are not. This is particularly important given recent research that has demonstrated both a reluctance among hate crime victims to notify the police (Lantz et al., 2019) and declining reporting rates in the United States (Myers & Lantz, 2020). We are aware of no other data sources that would allow the analyses conducted in the current study, but we acknowledge the limitations of our survey collection strategy. First, opt-in surveys may be biased due to differences between participants and the general public which are unobserved. However, some recent research suggests that non-probability opt-in surveys have the potential to be as effective as probability-based designs (e.g., Ansolabehere & Schaffner, 2014; Kennedy et al., 2016; Simmons & Bobo, 2015). In addition, our quota sampling strategy, in which we matched our sample to the general population using race and ethnicity, reduces the bias introduced by the opt-in nature of the survey (Rivers & Bailey, 2009). Nevertheless, our findings must be interpreted in light of this potential limitation. In addition, we recognize that the data obtained from these results may not necessarily be generalizable to the population as a whole. Given the rapid onset and constraints imposed by the COVID-19 pandemic, however, we believe these results represent an important starting point for considering the relationships that we examine. We use listwise deletion for missing data, resulting in a final sample size of 3,117.
Measures
Descriptive statistics for all variables are shown in Table 1. The primary dependent variable of interest in the current study is respondents’ depressive symptoms. We measure depressive symptoms using a modified 7-item version of the Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977). 3 The CES-D is a well-validated scale; modified versions of the scale are commonly used (Frisco et al., 2013; Wenger & Frisco, 2021) and studies have found versions of the scale with as a few as four of the items to be reliable (Grzywacz et al., 2006). Respondents were asked how often in the past week they (a) did not feel like eating, (b) had trouble keeping their minds on what they were doing, (c) felt depressed, (d) felt that everything they did was an effort, (e) felt their sleep was restless, (f) felt sad, and (g) felt they could not get going. Response options ranged from 0 (never or rarely) to 3 (most or all of the time) and we sum these responses to create a final measure ranging from 0 to 21, with higher values indicating more depressive symptoms (α = .90). The average value of depressive symptoms across our sample is 5.37.
Descriptive Statistics

Note. Standard deviations not shown for binary variables.
Our primary independent variables are perceived risk of COVID, hate crime victimization, fear of victimization, and vicarious victimization. Perceived risk of COVID is an ordinal measure based on a question asking respondents: “What level of threat do you think COVID-19 poses to you or your family?” Respondents answered on a 5-point Likert-type scale from very low (= 0) to very high (= 4). The mean of the variable is 2.33, corresponding to a response between moderate and high. Hate crime victimization is measured using a series of questions that asked respondents how often they experienced each of seven incident types during the 1 to 2 months prior to the survey because of their race/ethnicity. The incident types included: “been threatened with physical violence,” “had your personal property damaged or destroyed,” “had objects thrown at you,” “been chased or followed,” “been spat upon,” “been punched, hit, kicked, or beaten,” and “been assaulted or wounded with a weapon.” Respondents who said they had experienced any of these victimization types during the 1- to 2-month reporting period were coded as having experienced hate crime victimization (= 1) while respondents who reported no such experiences were coded as not having experienced hate crime victimization (= 0). Approximately 24% of respondents experienced a hate crime victimization during the 1 to 2 months prior to survey administration.
Our measure of fear of victimization is based on a question that asked respondents: “has the possibility of harassment or violence because of your race/ethnicity affected in any way how you yourself act or behave?” Respondents who answered yes are coded 1 on the dummy measure and respondents who answered no are coded 0. About 22% of respondents reported this fear of victimization. Finally, our measure of vicarious victimization is based on a question that asked respondents how many people they know personally have been verbally harassed, threatened with violence, or physically attacked because of their race/ethnicity. This measure is coded as a dummy measure equal to 1 if the respondent reported knowing at least one other person who had been a victim and coded 0 otherwise. Almost half of the respondents (46%) reported this type of vicarious victimization.
In addition to our primary measure, we control for several other respondent characteristics that might be related to our dependent and primary independent variables. Respondent age is measured in years based on the respondent’s birth date and survey date. Respondent gender is based on a question asking respondents which gender identity they identify with most. Respondents who responded “male” or “transgender male” are coded as male (= 1) while respondents who responded “female” or “transgender female” are coded as female (= 0). 4 Other responses (gender variant, other, and prefer not to answer) are coded as missing due to the low sample size. Respondent race/ethnicity is based on three questions from the survey asking respondents whether they are of Spanish, Latino, or Hispanic origin, which racial category describes their race (with the option to select more than one) and then which racial category they identify with most (if they indicated more than one racial category in the prior question). All respondents who answered yes to the first question are coded as Hispanic. The remaining respondents are coded as non-Hispanic Black if they indicated Black as one of their racial identities and, if asked, as the racial category they identified with most; coded as non-Hispanic White if they indicated White as one of their racial identities and, if asked, as the racial category they identify with most; coded as Asian if they indicated Asian as one of their racial identities and, if asked, as the racial category they identify with most; and coded as other race if they did not fall into one of these groups (White is the reference category in all models; see Table A.1 of the Supplemental Appendix [available in the online version of this article] for descriptive statistics by racial/ethnic group).
Respondent employment is coded as 1 if the respondent indicated they were employed at the time of the survey (either as they were before the pandemic or remotely) and 0 if the respondent was unemployed at the time of the survey (either because they were prior to the pandemic or became unemployed during the pandemic). Respondent education is a 7-point ordinal scale, ranging from some high school or less to a doctoral or other terminal degree, representing the highest grade of school that the respondent has completed. Respondent nativity is coded as 1 if the respondent indicated that they were born in the United States and coded 0 if they were born outside of the United States. Finally, because of the potential for lockdown procedures and other experiences with social isolation to influence both the risk of hate crime victimization and depressive symptoms, we control for the extent of social distancing engaged in by the respondent at the time of the survey. Total social distancing is coded as 1 if the respondent reported that they were not socializing with friends and family in person and coded as 0 if they reported socializing in person in some capacity. A correlation matrix of all analytic variables is presented in Table 2.
Correlation Matrix

p < .05. **p < .01. ***p < .001.
Analytic Strategy
To examine our first research question regarding whether concerns related to COVID-19 are related to depressive symptoms, we estimated a linear regression model with respondent depressive symptoms regressed on the perceived risk of COVID and all of our control variables. We then estimated a second linear regression model in which we added hate crime victimization, fear of victimization, and vicarious victimization as predictors to address our second research question regarding whether experiences with hate crime are related to depressive symptoms. To answer our third research question regarding whether hate crime experiences partially account for, or exacerbate, the relationship between perceived risk of COVID and depressive symptoms, we conducted both mediation and, separately, moderation analyses. Figure 1 graphically displays our theoretical mediation model. Because we have three mediators (hate crime victimization, fear of victimization, and vicarious victimization), we conducted two sets of mediation analyses. In the first, we used the medeff command in Stata 15 to test each mediator separately. In the second, we tested all three mediators simultaneously using seemingly unrelated regression (with the sureg command; Preacher & Hayes, 2008) to calculate direct effects and the nlcom command to calculate indirect effects. Although there are other methods for conducting mediation analyses, we are aware of no other method which allows for testing for multiple binary mediators. In addition, we used the bias-corrected and accelerated bootstrapping method for calculating the confidence intervals for the indirect effects (Preacher & Hayes, 2008). Finally, moderation analyses were conducted by testing for interaction effects between perceived risk of COVID and each of our victimization variables.
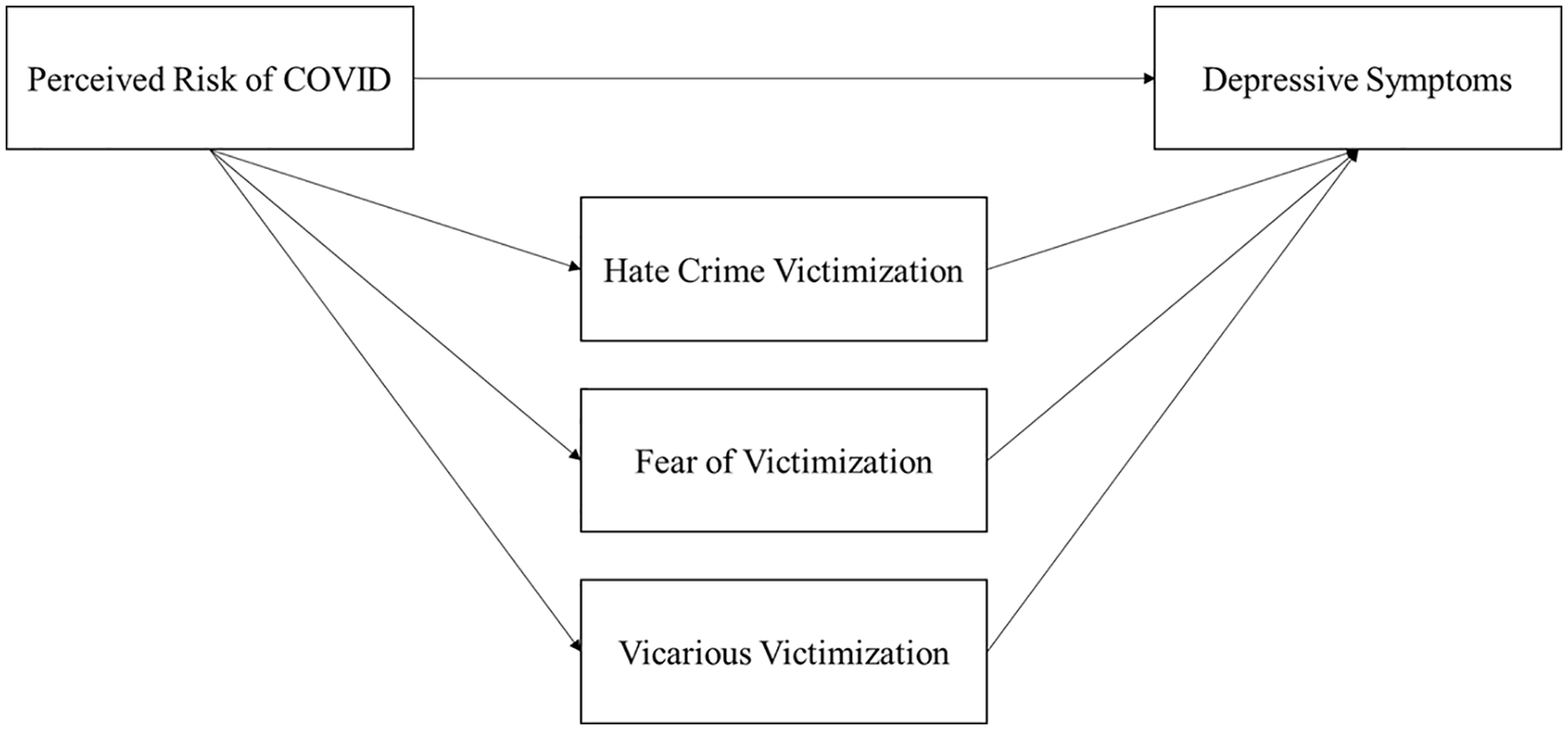
Theoretical Mediation Model
Results
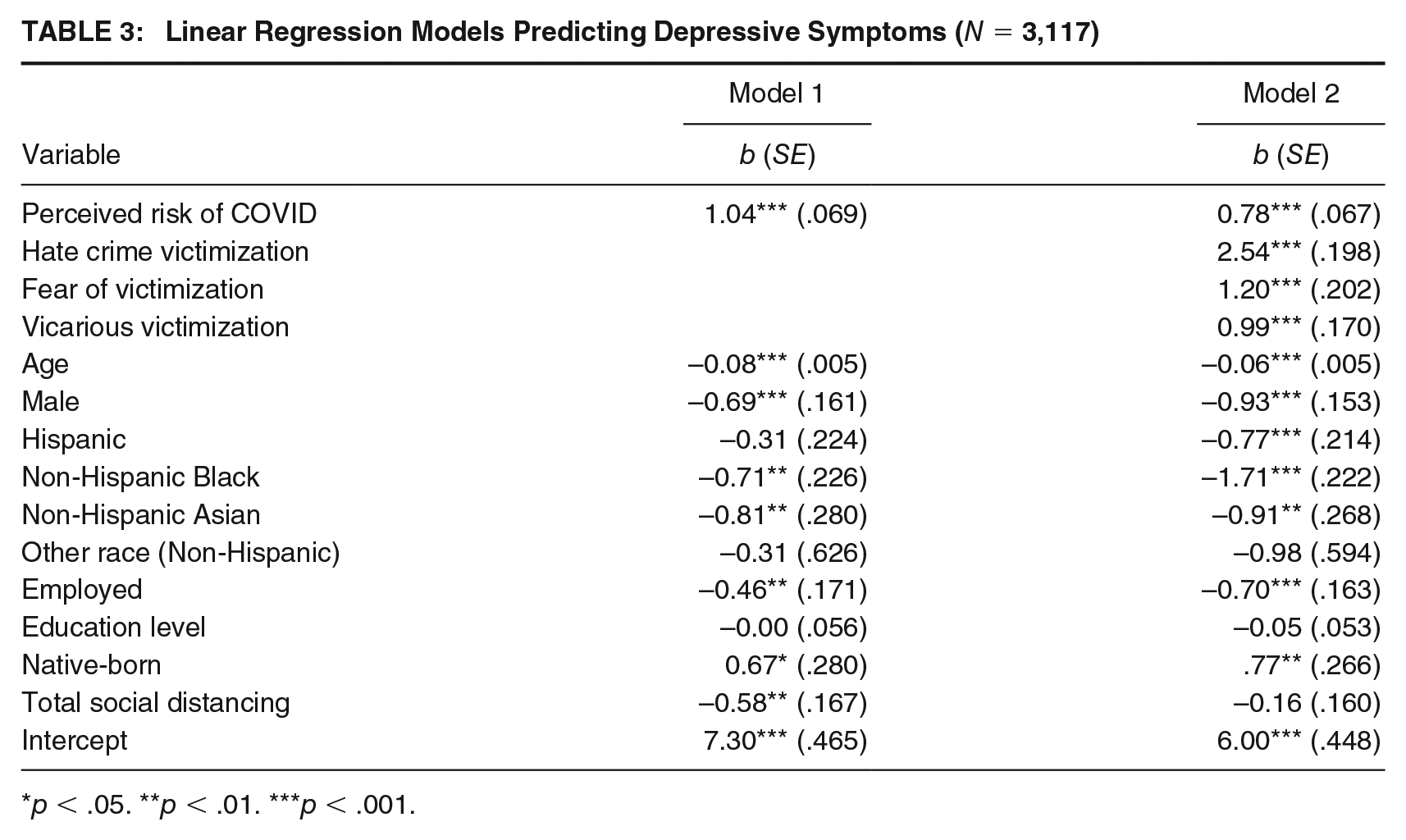
Results of our first regression model predicting depressive symptoms are shown in Model 1 of Table 3. As seen in the table, perceived risk of COVID was positively associated with depressive symptoms, providing support for our first hypothesis. Specifically, a one-unit increase in perceived risk of COVID was associated with a 1.04-unit increase in depressive symptoms (p < .001). Regarding control variables, older respondents, male respondents, those who are employed, and those who engaged in total social distancing were found to have lower depressive symptoms. In addition, non-Hispanic Black and Asian respondents had lower depressive symptoms than White respondents, and native-born respondents had higher depressive symptoms than those who are foreign born.
Linear Regression Models Predicting Depressive Symptoms (N = 3,117)
p < .05. **p < .01. ***p < .001.
To test our second hypothesis, we introduced the three victimization variables in Model 2 of Table 3. As suggested by our hypothesis, hate crime victimization, fear of victimization, and vicarious victimization were also positively associated with depressive symptoms. Specifically, hate crime victims scored 2.54 units higher on the depressive symptoms scale than respondents who were not the victim of a hate crime. Those who reported fear of victimization scored 1.20 units higher on the depressive symptom scale than those who did not report fear of victimization, and those who reported vicarious victimization scored .99 units higher on the depressive symptoms scale than those who do not report vicarious victimization.
Notably, the regression coefficient for the perceived risk of COVID is smaller in Model 2 than in Model 1 (b = .78, p < .001), providing preliminary support for our investigation of possible mediation effects. As described in the analytic strategy, we began our mediation analysis by testing for a mediation effect of each victimization type separately to see whether each independently mediates the relationship between perceived risk of COVID and depressive symptoms. Results revealed a significant indirect effect for all three victimization variables, suggesting that all three are independent mediators (see Table A.2 of the Supplemental Appendix for full results). However, given that Model 2 of Table 3 reveals an independent effect of each victimization variable when all three are included in the regression model, our primary mediation analysis tested for mediation of all three variables together. Results of this mediation analysis are presented in Figure 2.
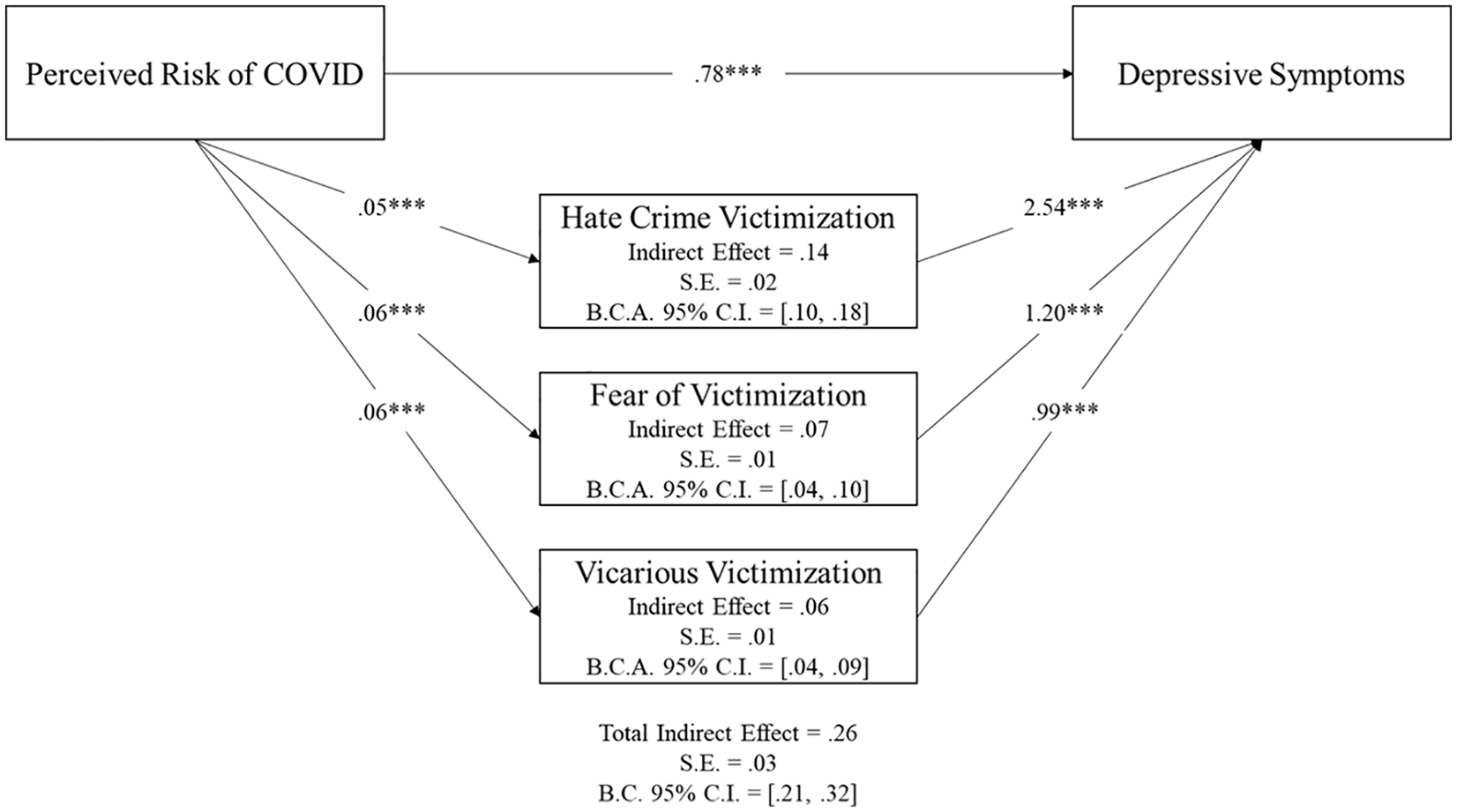
Multiple Mediation Model Depicting the Effect of Perceived Risk of COVID on Depressive Symptoms as Mediated by Hate Crime Victimization, Fear of Victimization, and Vicarious Victimization (N = 3,163)
As shown in the figure, while the perceived risk of COVID had a direct relationship with depressive symptoms even after controlling for the mediating variables, it also operated indirectly through all three mediating variables. In other words, the perceived risk of COVID was significantly associated with higher odds of experiencing hate crime victimization, fear of victimization, and vicarious victimization, and each of these experiences increased depressive symptoms, providing support for the mediation portion of our third hypothesis. Each of the three indirect effects is significant at the p < .01 level. Moreover, the total indirect effect of perceived risk of COVID on depressive symptoms jointly through the three mediators is significant as well (total indirect effect = .26, p < .001), and 25.4% of the total effect of perceived risk of COVID on depressive symptoms is mediated by hate crime victimization, fear of victimization, and vicarious victimization, collectively. Thus, our results provide support for our third hypothesis.
Finally, to test our fourth hypothesis and examine whether the three victimization experiences also moderate the relationship between perceived risk of COVID and depressive symptoms, we tested for two-way interactions between perceived risk of COVID and each of the three victimization variables. However, none of these interactions were significant and results are thus not shown here. In other words, hate crime experiences mediate, but do not moderate, the relationship between perceived risk of COVID and depressive symptoms.
Discussion
As the COVID-19 pandemic has raged across the United States and the world, research has documented a corresponding increase in mental health concerns and hate crime victimization. Moreover, there is reason to expect hate crime victimization itself to adversely impact individual mental health outcomes. Within this context, the current study suggested that personal concerns about the risk of COVID-19 could negatively impact individuals’ depressive symptoms, that various hate crime experiences could negatively impact individuals’ depressive symptoms, and that these experiences with hate crime could either mediate or moderate the relationship between perceived risk of COVID and depression. Our results highlight three important findings.
First, perceptions of greater personal risk of COVID-19 were associated with higher depressive symptoms. This finding is in line with prior research on mental health outcomes related to disease outbreaks generally (Hawryluck et al., 2004) and the COVID-19 pandemic specifically (Bueno-Notivol et al., 2021). Although we do not have pre-COVID measures and cannot directly assess the causal direction of this association and acknowledge that it is possible that preexisting depressive symptoms may also lead to increased fear of the pandemic, these effects provide some evidence for the devastating impact of the pandemic on individual mental health. Moving forward, researchers, policymakers, and mental health experts should focus efforts on combating and addressing the negative consequences of the pandemic for individuals’ depressive symptoms.
Second, hate crime victimization, fear of victimization, and vicarious victimization each had independent positive associations with depressive symptoms, thus providing an important contribution to research on the psychological and public health impacts of hate crime more generally. While hate crime legislation is ostensibly justified on the grounds that such crimes have a greater psychological impact on victims than other crimes, a number of scholars have argued that the empirical support for this argument has been lacking—primarily due to data limitations (Bell & Perry, 2015; Iganski, 2001; Perry, 2006). This research is among the first to quantitatively demonstrate a direct relationship between hate crime victimization, fear of victimization, vicarious hate crime victimization, and individual mental health, in the form of depressive symptoms. Taken together, these results suggest that anti-bias legislation and other efforts to address the mental health consequences of hate crime victimization must extend beyond individual victims by providing assistance and resources to others within the victims’ community as well.
Finally, and most importantly, our analyses revealed that experiences with hate crime mediate, but do not moderate, the relationship between perceived risk of COVID-19 and depressive symptoms. In other words, experiences with hate crime victimization, fear of victimization, and vicarious victimization may not exacerbate the impact of COVID-19 on depressive symptoms, but they do help explain—to some extent—the increased levels of depression reported during the pandemic. Therefore, while addressing the mental health costs of the pandemic must be a central aspect of the public agenda moving forward, one aspect of this focus must be on the psychological costs related to bias-motivated victimization and fears associated with potential victimization. As Craig-Henderson and Sloan (2003) noted, one of the most important aspects of treatment for hate crime victims is to help them to reclaim a sense of normalcy. Unfortunately, there are even more barriers to this return to normalcy for those who are victimized within the context of a global pandemic.
Importantly, neither the consequences of the pandemic or hate crime victimization are evenly distributed across populations but are concentrated among those belonging to racial/ethnic minority groups, and among those who were “essential workers” or were otherwise unable to socially distance during the early months of the pandemic. We think it is important to consider these results within this context. Lockwood and Cuevas (2020) recently argued that because of historical contexts of discrimination, the mental health consequences of hate crimes may be particularly pronounced among racial and ethnic minority victims. Future research, therefore, should consider the potential for race-specific variation in the relationship between hate crime victimization and depressive symptoms. These results have particularly important implications for these populations and efforts to address COVID-19-related depression should not be designed without regard for these disparities. Furthermore, prior research has shown that hate crime victimization varies across space and exhibits spatial clustering (Wenger & Lantz, 2021b). As such, the mental health consequences found in the current study might not only be concentrated among certain populations but also within certain communities. Future research should examine spatial variation in hate crime victimization, fear of victimization, and vicarious victimization during the COVID-19 pandemic, in particular, to determine whether resources to address such harms should be geographically concentrated as well.
Conclusion
The COVID-19 pandemic has wrought severe negative consequences for groups across the United States and the rest of the world. Much of the initial research on these consequences has focused on outcomes for physical health, but more recent research has focused on outcomes for mental health as well. These negative physical and mental health outcomes have happened alongside high levels of hate crime victimization and fear of victimization. The current study examined the combined impact of the COVID-19 pandemic and experiences with hate crime on individual depressive symptoms and found that experiences with hate crime partially mediate the relationship between the COVID-19 pandemic and depressive symptoms. Therefore, any plans for a return to “normalcy” postpandemic will require not only addressing the direct consequences of the pandemic itself but also the indirect consequences through hate crime victimization, fear of victimization, and vicarious victimization.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548221104738 – Supplemental material for The Role of Hate Crime Victimization, Fear of Victimization, and Vicarious Victimization in COVID-19-Related Depression
Supplemental material, sj-docx-1-cjb-10.1177_00938548221104738 for The Role of Hate Crime Victimization, Fear of Victimization, and Vicarious Victimization in COVID-19-Related Depression by Marin R. Wenger, Brendan Lantz and Gabriella Gallardo in Criminal Justice and Behavior
Footnotes
Authors’ Note:
The authors gratefully acknowledge funding in the form of a Collaborative Collision Grant from the Florida State University Council on Research and Creativity.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.