
Abstract
This study examined the impact of perceived social support on mental health and psychosocial functioning in combat veterans after military deployment, including veterans with post-traumatic stress disorder (PTSD) and veterans with comorbid PTSD and alcohol use disorder. Veterans (n = 139; female = 23) completed self-report and clinician-administered measures of social support, mental and physical health, functional impairment, and quality of life. The cohort was divided into high, medium, and low perceived social support based on averages of the total score from the Multidimensional Scale of Perceived Social Support. Relative to the low perceived social support group, the high perceived social support group reported fewer symptoms of PTSD, anxiety, and depression. The high perceived social support group also reported a more diverse and embedded social network, less disability, and better quality of life. Of note, the high and low perceived social support groups did not differ on age, gender, education, race ethnicity, or combat trauma exposure. These findings highlight that perceived social support may play an important role in the treatment of postwar veterans as they transition back to civilian life.
Background
The wars in Afghanistan and Iraq together make up the longest sustained lengths of U.S. combat operations (Congressional Research Service, 2019). However, less than 1% of the population of the United States is directly impacted by these combat operations. Although post–9/11 veterans have not received the hostile public sentiment that some Vietnam veterans endured, most civilians know very little about their experiences or concerns. Furthermore, these wars are unique from previous wars in their reliance on the National Guard and Reserves; longer duration of deployments; the frequency of multiple redeployments; types of injuries sustained; and broader effects of these conflicts on the service members, their families, and their communities (Institute of Medicine, 2013). Additionally, while the majority of the U.S. military is non-Hispanic White (57%), Black and Latino adults are increasingly represented. In 2017, 16% of U.S. military members were Black and 16% were Hispanic/Latino, 4% were Asian, and an additional 6% were identified as “other” or unknown (Barroso, 2019).
Approximately three quarters of post–9/11 veterans were deployed and are twice as likely as those who served before them to have deployed (Parker et al., 2019). Over a third of veterans (35%) indicate they knew and served with someone who was seriously injured and 30% knew and served with someone killed in battle. Among combat veterans, 57% report witnessing someone from their unit affiliation being seriously wounded or killed (Parker et al., 2019). While most combat veterans do not go on to develop the signature wounds of post-traumatic stress disorder (PTSD; estimates range from 1 to 30%) or traumatic brain injury (prevalence estimated at 22%), there are still significant postdeployment challenges encompassing both clinical issues (such as substance abuse, anxiety, and depression) and functional concerns including potentially stressful transitions to family, work, and/or academic settings (Institute of Medicine, 2013). Additionally, rates of PTSD are higher in diverse previously deployed post–9/11 veteran populations with increased risk of a positive screen for PTSD among veteran affairs (VA) health care users (OR = 2.71), African Americans (OR = 1.61), those who served in the Army (OR = 2.67), and those on active duty (OR = 1.69; Dursa et al., 2014). For many veterans, the impact of war is experienced beyond their combat deployment and into the transition from military to civilian life (Sayer et al., 2010).
Following deployment, a significant minority of combat-exposed veterans develop biopsychosocial impairments including physical and mental health issues, substance use, social support challenges, functional impairments, and quality of life concerns (e.g., Hoge et al., 2004; Kehle et al., 2011; Seal et al., 2007). Notably, perceived social support is one of the strongest predictors of overall adjustment after experiencing a trauma, making it a potentially significant protective factor for combat-exposed veterans (Brewin et al., 2000; Ozer et al., 2003). Perceived social support is defined as one’s perceptions of available emotional, informational, or tangible supports including a sense of belonging (Glanz et al., 2015). According to the National Center for PTSD’s Field Operations Guide for Psychological First Aid, the main types of social support are emotional support, social connection (i.e., feeling like you fit in and have things in common with others), feeling needed (i.e., feeling valued, useful, productive, and appreciated), reassurance of self-worth (i.e., people having confidence in you and your abilities), reliable support, advice and information, physical assistance, and material assistance (Brymer et al., 2006). Research indicates that perceived social support enhances mental and physical health in diverse nonclinical populations (e.g., college students, unemployed workers, new mothers, widows, parents of children with serious illnesses; Ozbay et al., 2007). Numerous cross-sectional/retrospective studies also indicate that social support and PTSD have a negative relationship in which combat veterans with greater levels of perceived social support have less severe PTSD symptoms and those with more severe PTSD symptoms report lower social support (e.g., Barrett & Mizes, 1988; Boscarino, 1995; Duax et al., 2014; Wilcox, 2010).
For example, Pietrzak and colleagues (2009a) demonstrated that combat veterans’ perceived social support was associated with lower traumatic stress and depressive symptoms. Others have investigated whether specific sources of social support moderate psychosocial outcomes for combat veterans. Various studies indicate that perceived social support from peers and significant others is associated with lower PTSD symptom severity (Wilcox, 2010), emotion dysregulation and depression (Cox et al., 2017), and less frequent utilization of VA clinical settings, suggesting a lower need for clinical intervention (Lehavot et al., 2013). Platt et al. (2014) found that perceived social support predicted less PTSD in the context of prior trauma and that social network diversity interacted with perceived social support to predict PTSD outcomes.
Additionally, results from Avery and McDevitt-Murphy (2014) showed that lower levels of postdeployment social support were associated with increased PTSD symptom severity, regardless of unit social support during deployment. Gros and colleagues (2016) investigated the relationships between PTSD, co-occurring substance use disorders, and social support among predominately post–9/11 VA treatment-seeking sample of veterans. Results indicated that increased social support was associated with less severe PTSD symptoms and, interestingly, increased alcohol use. However, other investigators report no relationship between alcohol use and social support (Avery & McDevitt-Murphy, 2014; Ren et al., 1999; Sacco et al., 2014) or only a small negative relationship between the two (Boscarino, 1995).
Collectively, these results suggest that perceived social support has a strong negative association with mental health outcomes in combat-exposed veterans (Avery & McDeritt-Murphy, 2014; Bryan & Heron, 2015; DeViva et al., 2016; Laffaye et al., 2008; Pietrzak et al., 2009b; Wilcox, 2010) and supports a social causation model that focuses on the positive impact of social support on stress and well-being (Cohen & Willis, 1985). However, most studies of perceived social support show only that it correlates with better mental health, and there is less evidence for a causal link. Other longitudinal studies support a social selection model suggesting that PTSD symptoms can erode social support over time (Carter et al., 2016; King et al., 2006; Laffaye et al., 2008). Perhaps social support has a different impact on the course of PTSD than on PTSD onset, although the relationship between PTSD symptoms and social support remains unclear (Laffaye et al., 2008). King and colleagues discovered that male combat veterans with more severe PTSD symptoms 2 years postdeployment had lower positive social support at a 5-year follow-up. However, there are other studies that suggest higher social support is prospectively associated with decreases in PTSD symptom severity (Kaniasty & Norris, 2008; Shallcross et al., 2016).
In a sample of 521 National Guard Soldiers, Shallcross and colleagues discovered that PTSD symptoms and social support reciprocally influence one another over time. They found PTSD-specific symptoms both eroded and were positively influenced by social support in this National Guard Soldier population. Also, in a nonmilitary Mexican population of victims from a natural disaster, Kaniasty and Norris (2008) found that in the 12–18 months following the trauma, participants benefited from social support, but social relationships were also hampered from trauma symptoms. However, social support had a positive impact on trauma symptoms from 6 to 12 months and 18 to 24 months, suggesting that higher social support resulted in decreases in PTSD symptom severity.
As noted above, the relationship between social support and trauma is complicated. Furthermore, individual characteristics that predict who might respond to social support are not well established due to the practical challenges of recruiting and studying the post–9/11 veteran population. The post–9/11 veteran designation includes a wide range of subjects who have deployed to a war zone. This population is heterogeneous and includes veterans with varying degrees of trauma exposure, levels of help seeking, and time since initial deployment (Institute of Medicine, 2013). There is also limited representation of the five military branches, with Army and Reserve personnel being overrepresented. The heterogeneity of both the veteran population and the research settings they are recruited from may hinder generalizations about which veterans respond to social support after combat operations. For example, Milliken et al. (2007) reported significant differences in probable PTSD prevalence between the National Guard members (24.5%) and active-duty service members (16.7%) in the 4–10 months following deployment. At a 5-month follow-up Post-Deployment Health Reassessment (PDHRA), many new cases of PTSD were identified among service members who initially reported subthreshold symptoms. In fact, investigators found there were twice as many new cases of PTSD than were identified at the initial Post-Deployment Health Assessment, suggesting either delayed onset or delayed reporting of symptoms. Notably, investigators found a similar increase in rates of depressive symptoms for both active-duty and reserve components, although reservists were more likely to be utilizing mental health services or to have been identified as needing a referral for mental health services. Perhaps the real difference between mental health prevalence rates in National Guard/reserve and active-duty component is related to less social embeddedness or fewer resources, given that the National Guard members have less access to resources, medical providers, and less fear of it impacting their career since they are part-time service members. The variable PTSD symptom prevalence and time-bound symptom manifestation among different military branches and components with similar demographic backgrounds highlight some of the challenges to accurate identification of those who may benefit from perceived social support.
Notably, most subjects from all the clinical studies cited have been White male veterans. Avery and McDeritt-Murphy (2014) reported the most diverse clinical sample with 65.2% veterans identifying as White (n = 45), 27.5% as Black (n = 19), 5.8% multiethnic (n = 4), and 1.4% as Asian (n = 1). However, a national survey of a nonclinical sample of post–9/11 veterans (N = 924) conducted by Muralidharan and colleagues (2016) revealed that Black male veterans (n = 38) reported lower support from family and friends while Hispanic male veterans (n = 49) had greater concerns about family disruption after deployment, both relative to their White counterparts (n = 350). Given the small sample sizes of ethnically and racially diverse veterans, the extant research does not illuminate the interface between social support and mental health outcomes in racially, ethnically, or socioeconomically diverse veteran populations. There may be cultural, ethnic, or socioeconomic variations in levels of perceived social support that remain unknown due to this knowledge gap. Additionally, the existing literature does not elucidate the role of perceived social support in mental health outcomes for female combat-exposed veterans.
Introduction
This study aims to further illuminate the role of perceived social support in impacting the mental health outcomes of combat-exposed veterans. While many of the studies cited have examined the impact of social support on PTSD and depression, few studies have also investigated the association between social support and readjustment issues including anxiety disorders and substance use disorders, which are frequent presenting concerns in VA clinical settings. In this study, we examined perceived social support to determine the extent to which it is associated with a broader range of mental health symptoms including postdeployment PTSD, anxiety, depression, alcohol misuse, quality of life, mental health disability, and social network variables. Based on previous findings, we expected veterans reporting higher perceived social support would be less susceptible to PTSD, depression, anxiety, and disability related to mental health and have a higher quality of life. We also incorporated structured clinical interviews such as the Clinician Administered Posttraumatic Stress Scale (CAPS-IV), Hamilton Depression Inventory (HAM-D), and Hamilton Anxiety Inventory (HAM-A). Previous investigations relied upon self-report scales, which—although efficient—may have over- or underestimated symptom severity (Althubaiti, 2016). Finally, unlike previous studies, we recruited a sample of post–9/11 veterans recruited from an urban VA medical center including approximately equal representations of African American, Latino, and White veterans. We also examined ethnic/racial differences to determine the extent to which perceived social support may differ for ethnic/racial groups represented.
Method
Participants and Procedures
Participants included 139 post–9/11 U.S. military veterans recruited from the Jesse Brown VA Medical Center (JBVAMC) in Chicago, IL, between 2012 and 2017 as part of a larger study. Recruitment occurred via advertisements placed in public spaces within the hospital, through clinic referrals, and through outreach to veteran communities. Participants were compensated hourly for their time in adherence to institutional review board (IRB) standards weighing benefits and risks. Participants completed a clinical assessment and self-report measures after concluding informed consent procedures. Initial exclusion criteria included being over the age of 55 (to reduce the likelihood of a neurodegenerative process impacting cognitive performance in the larger study); the presence of a clinically significant medical or neurological condition that would affect the ability to participate; psychotic disorder; the presence of organic mental syndrome, intellectual disability, or pervasive developmental disorder; current substance abuse; or suicidal/homicidal ideation at a level that would interfere with the study protocol. Participants completed a general demographic interview to assess for basic demographic characteristics such as age, level of education, sex, and race/ethnicity in addition to Clinician Administered PTSD Scale, Social Network Index, Multidimensional Scale of Perceived Social Support (MSPSS), and World Health Organization Quality of Life (WHOQOL). The developers of the MSPSS recommended using mean total scale score ranging from 1 to 2.9 to indicate low social support, a score of 3 to 5 to indicate moderate social support, and a score from 5.1 to 7 to indicate high social support (Zimet et al., 1988). The cohort was divided into three perceived social support groups based on these recommendations (low n = 22, moderate n= 52, high n = 65; see Table 1). This study was approved by the IRBs at JBVAMC as well as the University of Illinois at Chicago. The research was conducted in accordance with the Helsinki Declaration and the American Psychological Association ethical standards.
Demographic and Clinical Characteristics of the Sample.
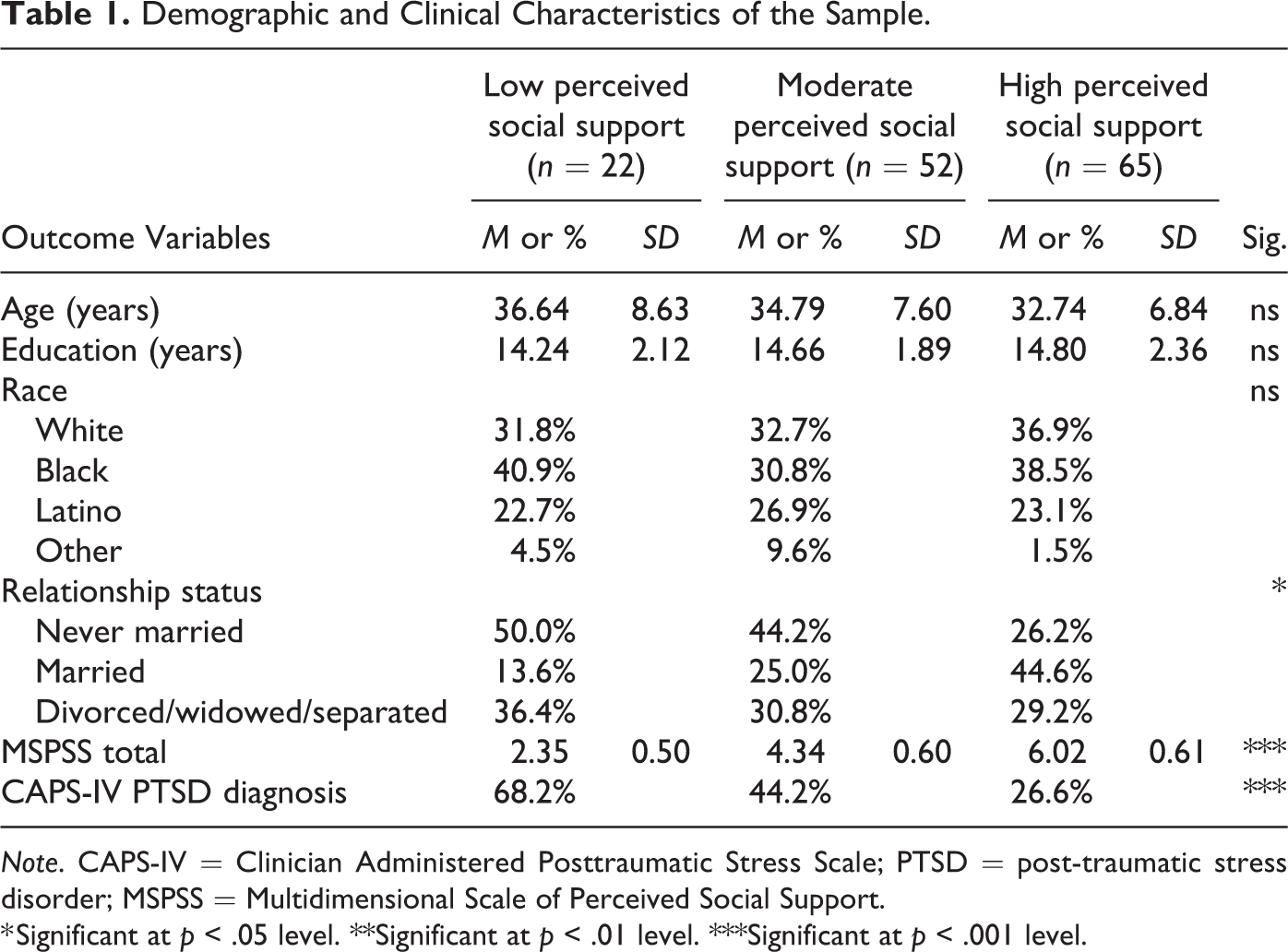
Note. CAPS-IV = Clinician Administered Posttraumatic Stress Scale; PTSD = post-traumatic stress disorder; MSPSS = Multidimensional Scale of Perceived Social Support.
* Significant at p < .05 level. **Significant at p < .01 level. ***Significant at p < .001 level.
Measures
In order to meet the study objective of understanding the impact of perceived social support on various outcomes, this study evaluates how grouping based on self-reported perceived social support (independent variable) is associated with a range of mental health, social network quality, and functional variables (dependent variables).
Social Support and Network
MSPSS
The MSPSS (Zimet et al., 1988) is a 12-item measure of subjectively assessed social support using the total score comprised of factor groups related to the source of support (i.e., family, friends, or significant others). Respondents indicated how much they perceived support from 1 (very strongly disagree) to 7 (very strongly agree) for each item. For example, “I get the help and support I need from my friends.” The total score has established internal consistency (Cronbach’s α .88; Zimet et al., 1988). In the present sample, the MSPSS total score had a Cronbach’s α of .93.
Social network index (SNI)
The SNI is a 12-item measure for identifying how many people one sees or talks to on a regular basis including family, friends, workmates, and neighbors. The scale was designed to capture three aspects of one’s social network: (1) the overall number of people in the network in contact at least every 2 weeks, (2) the number of different networks domains (embedded networks) in which an individual is regularly active (e.g., friends, family, work, church) at least once every 2 weeks (i.e., between 0 and 8), and (3) the number of social roles in which the respondent has regular contact (i.e., at least once every 2 weeks) with at least one person (i.e., between 0 and 12). To receive a point for a domain, a respondent must have at least four high-contact people within that domain.
Psychopathology (PTSD, Depression, Anxiety, Alcohol Use, Combat Exposure)
CAPS-IV
The CAPS-IV is a structured interview intended to assess for exposure to traumatic stressors and accompanying symptoms of PTSD related to those events. Current PTSD symptoms were assessed in relation to the war-zone trauma that was most upsetting at the time of assessment. Items are summed for a continuous score of PTSD symptom severity that ranges from 0 to 136, with higher scores indicating more severe PTSD (Blake et al., 1995
HAM-D and HAM-A
The HAM-D and HAM-A interviews offer high validity and reliability in measuring response to treatment on several psychological and somatic/physical symptoms of depression and anxiety. The HAM-D is an observer-rated scale using behaviorally anchored items rated on a 3- or 5-point scale and summed to obtain the total score. Scores greater than 24 are indicative of severe depression while scores less than 7 are indicative of the absence of depression (Rohan et al., 2016). The HAM-A is an observer-rated 14-item scale, with a total score ranging from 0 to 56 with rising severity values higher than 13 indicative of a case (Hamilton, 1959). In the present sample, Cronbach’s αs were .80 and .86 for the HAM-D and HAM-A, respectively. These instruments were chosen for their interview format rather than the alternative to self-report questionnaire format of Beck Inventories.
Alcohol use disorders identification test (AUDIT)
The AUDIT (Saunders et al., 1993) is a 10-item scale that was given to measure self-reported alcohol use as well as problems associated with alcohol use and overall hazardous drinking during the past 12 months. AUDIT scores in the range of 8–15 represented a medium level of alcohol problems whereas scores of 16 and above represented a high level of alcohol problems. The AUDIT total score was calculated and utilized as a dependent variable. Good internal consistency has also been reported for this measure (Cronbach’s α = .83; Daeppen et al., 2000). In the present sample, Cronbach’s α was .93.
Combat Exposure Scale (CES)
The CES is a 7-item measure of combat exposure severity that inquires about the frequency of various combat experiences such as witnessing someone hit by enemy fire or conducting combat patrols. The CES has demonstrated high internal consistency with a coefficient α of .85 and a test–retest reliability of .97 (Kean et al., 1989). In the present study, Cronbach’s α was .84.
Quality of Life/Disability
Sheehan Disability Scale (SDS)
The SDS (D. V. Sheehan et al., 1996) measures mental health-related disability and contains three 11-point items, and the respondent is asked to rate, on a numerical scale, the extent to which emotional problems have disrupted their work, social life, and family life/home responsibilities over the last month (ranging from 0 [not at all] to 10 [extremely]). Its validity and reliability have been investigated by several studies (K. Sheehan & Sheehan, 2008). In the present sample, Cronbach’s α was .97 for the SDS total score.
WHOQOL-BREF
The WHOQOL-BREF is a 26-item measure of both satisfaction and importance of various aspects of life including physical health, psychological health, social relationships, and environment (World Health Organization, 2004). Cronbach’s αs ranged from .79 to .87 within the present sample.
Data Analysis
Groups were initially compared on demographic and basic clinical characteristics (see Table 1) utilizing univariate analyses of variance (ANOVAs) and χ2 analyses. Planned comparisons for dependent variables included psychiatric symptoms, social network variables, and functional variables (see Table 2). Univariate ANOVAs were conducted for group comparisons on each dependent variable using a Bonferroni correction for post hoc comparisons. False discovery rates were utilized to correct for Type I error using the Benjamini and Hochberg (1995) procedure using p values for all 13 dependent variables.
Psychiatric, Social Network, and Functional Variables.
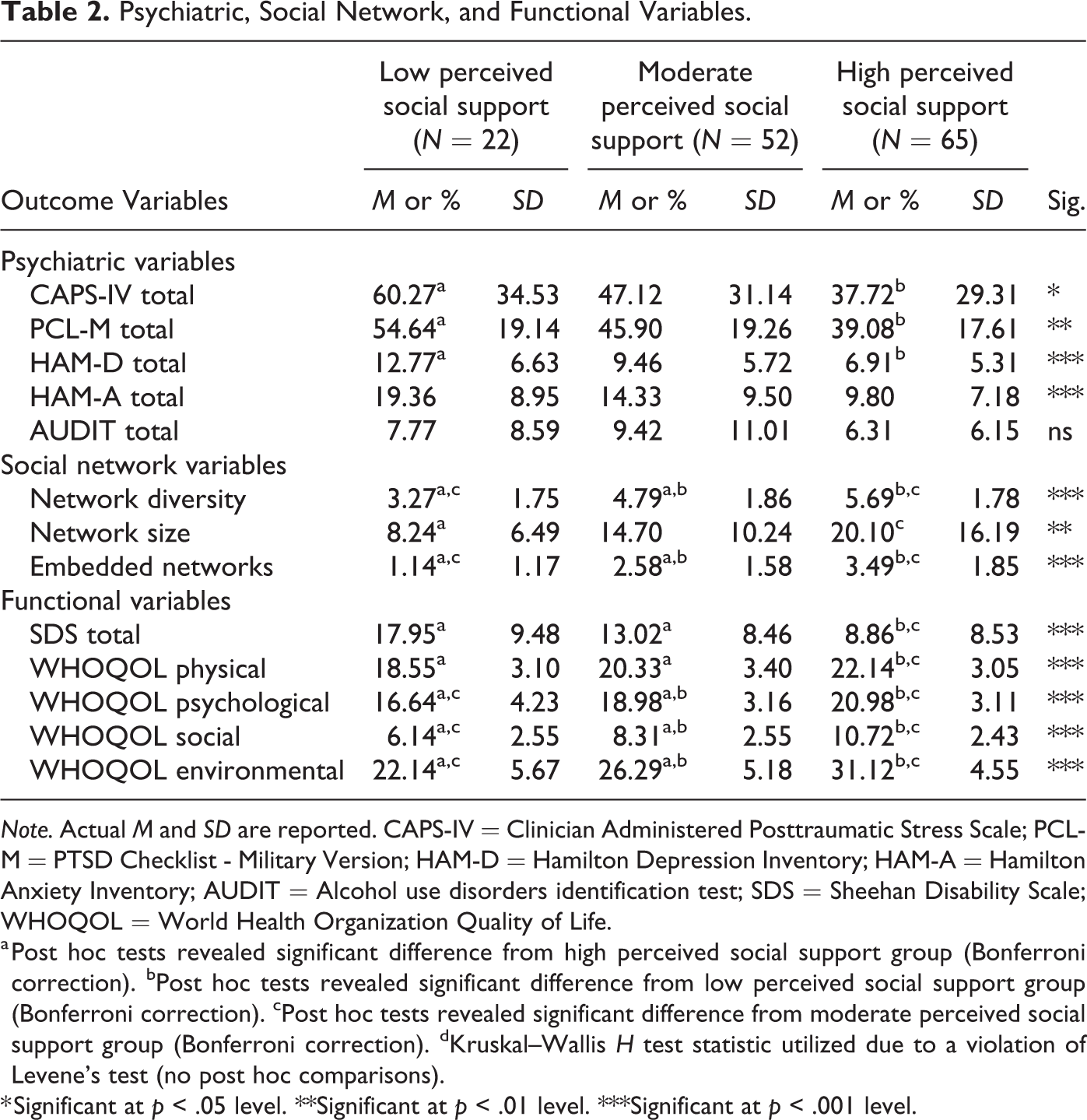
Note. Actual M and SD are reported. CAPS-IV = Clinician Administered Posttraumatic Stress Scale; PCL-M = PTSD Checklist - Military Version; HAM-D = Hamilton Depression Inventory; HAM-A = Hamilton Anxiety Inventory; AUDIT = Alcohol use disorders identification test; SDS = Sheehan Disability Scale; WHOQOL = World Health Organization Quality of Life.
a Post hoc tests revealed significant difference from high perceived social support group (Bonferroni correction). bPost hoc tests revealed significant difference from low perceived social support group (Bonferroni correction). cPost hoc tests revealed significant difference from moderate perceived social support group (Bonferroni correction). dKruskal–Wallis H test statistic utilized due to a violation of Levene’s test (no post hoc comparisons).
* Significant at p < .05 level. **Significant at p < .01 level. ***Significant at p < .001 level.
Results
No differences between groups were observed for age, sex, years of education, race, or combat exposure. However, those in the high perceived social support group were significantly more likely to be married. Descriptive statistics for demographic and clinical variables are provided in Table 1. Representation of all significant group comparisons and post hoc comparisons can be found in Table 2. False discovery rates were utilized to correct for Type I error using the Benjamini and Hochberg (1995) procedure, and all outcomes aside from alcohol use were significant at a corrected p < .046 cutoff. With regard to psychiatric symptoms, significant differences between perceived social support groups were evident for clinician-rated PTSD symptoms, F(2, 136) = 4.62, p = .011; partial η2 = .06, and clinician-rated depression, F(2, 135) = 9.26, p < .001; partial η2 = .12. Due to violations of Levene’s test for the equality of error variances, ratings for both alcohol use and clinician-rated anxiety were evaluated using the Kruskal–Wallis test. A Kruskal–Wallis H test showed that there was a statistically significant difference in anxiety scores between the perceived social support groups, χ2(2) = 18.87, p < .001, with a mean rank score of 96.77 for low perceived social support, 74.95 for moderate perceived social support, and 55.70 for high perceived social support. No significant differences were observed between groups for alcohol use. With regard to social network variables, significant differences between perceived social support groups were observed for social network diversity, F(2, 136) = 15.20, p < .001; partial η2 = .18; social network size, F(2, 133) = 27.40, p = .001; partial η2 = .10; and embedded social networks, F(2, 136) = 17.21, p < .001; partial η2 = .20]. Notably, no significant difference was observed between race demographics for perceived social support. When evaluating functional outcomes, significant perceived social support group differences were also observed for disability, F(2, 136) = 9.82, p < .001; partial η2 = .13; physical quality of life, F(2, 136) = 11.71, p < .001; partial η2 = .15; psychological quality of life, F(2, 136) = 15.26, p < .001; partial η2 = .18; social relationships, F(2, 135) = 31.87, p < .001; partial η2 = .32; and environmental quality of life, F(2, 136) = 31.11, p < .001; partial η2 = .31].
Discussion
This study assessed the impact of perceived social support on mental health and psychosocial functioning in post–9/11 veterans. As expected, results indicated that high perceived social support was associated with lower levels of PTSD symptoms, anxiety, depression, self-reported mental health-related disability, and greater quality of life. These findings are comparable to findings of other cross-sectional/retrospective studies (e.g., Duax et al., 2014; Gros et al., 2016; Wilcox, 2010), while using more sensitive PTSD diagnostic tools (e.g., CAPS-IV) and a perceived social support measure (i.e., Multidimensional Scale of Perceived Support). While other investigators (e.g., Wilcox, 2010) found a relationship between postdeployment perceived social support and PTSD that pertained to family, significant others, and military friendships, this study found the relationship also held true for nonmilitary friendships. These findings highlight the noteworthy relationship between social support, mental well-being, and psychosocial functioning in post–9/11 veterans. Prior research (i.e., Pietrzak et al., 2010) suggests that social support (as a moderator) can “buffer” negative effects of PTSD symptoms as well as generate broad positive effects on other symptoms and domains of functioning, such as anxiety, depression, disability, and quality of life. While our study did not employ perceived social support as a moderator variable, when considered in the context of prior studies, our findings may reflect a potential protective effect of social support. However, another interpretive possibility is that individuals with increased mental health problems prevent a barrier to the development of strong social support networks. These findings also suggest no relationship between alcohol use and perceived social support, which is consistent with prior research (Avery & McDevitt-Murphy, 2014) and may reflect a more complicated dynamic between types of social support and alcohol use (e.g., Beattie & Longabaugh, 1999). High perceived social support among veterans was also associated with greater size of social networks, more social network embeddedness, and more diversity in social relationships. This was an expected finding and has potential clinical implications for post–9/11 veterans.
While there is a groundswell of research into clinical interventions for combat-related PTSD (Watkins et al., 2018), less attention has been paid to nonclinical factors, interventions, or sources of support that may significantly impact mental health outcomes in this population. It has been well established that mental health stigma or veteran stigma may lead some combat veterans to delay or avoid utilizing traditional mental health treatment (Pietrzak et al., 2009a). Therefore, nonclinical means of support such as harnessing social support networks may serve as an alternative venue to foster resilience and recovery, particularly for veterans who have lower levels of readiness to engage in formal mental health treatment.
The Department of VA Veterans Healthcare Administration (VHA) operates the largest integrated health care delivery system in the United States of America. The VA’s depth and breadth of services for veterans is second to none and is probably the reason that 14 of the 20 veterans who committed suicide per day in 2013 or 2014 did not have any contact with the VA (U.S. Department of Veterans Affairs, Office of Suicide Prevention, 2017). The VHA provides a broad range specialized mental health care (PTSD clinical teams, primary care–mental health integration, Psychosocial Rehabilitation and Recovery Center, day hospital programs, inpatient services, general outpatient mental health services) and social support services (suicide prevention, recreational therapy, whole health coaching, wellness programming, homeless programming, caregiver support, peer support, community partnerships, etc.). This includes working with and improving the support of veteran families, caregivers, and supporters who are critical to veterans’ well-being.
Case Presentation
To illustrate how social support perceptions can change over time, we present a fictional case of a 28-year-old, married Latino veteran diagnosed with PTSD who distances himself from available social supports because “civilians don’t understand what I’ve been through.” This veteran is a composite of a number of cases treated by the authors (E.P. and H.M.P.) and will be given the pseudonym “Mr. Doe.” Mr. Doe was initially engaged by VA staff during a PDHRA conducted 90 days postdeployment. During the PDHRA, Mr. Doe was educated about his VA benefits (informational support) and expressed interest in filing a disability claim with the VA for a service-connected medical condition. Following the PDHRA, a VA case manager reached out to him by phone to follow up on his needs and began to help him initiate this claim (tangible support). In the course of assisting with the claim, the case manager was able to assess Mr. Doe’s other needs and learned that he needed a primary care appointment, which was scheduled for him. During the primary care appointment a week later, his physician completed basic screens for depression and posttraumatic stress and he endorsed these symptoms for the first time, after having initially denied them on questionnaires at the PDHRA.
Subsequently, the physician made a referral for a mental health intake and Mr. Doe was linked with a psychologist. During initial psychotherapy sessions, he endorsed symptoms of intrusion and hyperarousal but was mostly bothered by pervasive feelings of disconnection from those around him, including feeling misunderstood and emotionally distant or numb. He reported not communicating with his wife or any close friends or family members for fear that they would respond poorly to hearing about his wartime experiences or would ask him intrusive questions about these experiences, which he did not want to discuss. As the psychologist and Mr. Doe collaboratively considered treatment options, including trauma-focused therapies, the psychologist recommended a number of additional sources of support, including a process group for recently discharged post–9/11 combat veterans. In the context of the process group, Mr. Doe expresses feelings pertaining to his combat experiences for the first time and receives validating responses from peers (emotional support). After 2 months of attending the group, he begins to articulate a renewed sense of belonging and connection with his veteran peers.
As Mr. Doe continues to participate in trauma-focused work with the psychologist, he begins to show an increased willingness to communicate with nonveteran significant others, although not necessarily about his wartime experiences. Rather, he is more willing to attend family gatherings, social events, or school functions with his children and has received psychoeducation on effective coping strategies for hyperarousal symptoms that still sometimes occur in public settings. After 6 months of group and individual treatment, he still reports occasional nightmares and intrusive memories, but his avoidance symptoms have greatly decreased, and he has sustained social reconnection with veteran peers and nonveteran friends and family members. As part of his recovery process, he also began participating with other veterans in community service projects, such as volunteering at the local forest preserve and animal shelters.
Veterans may participate in evidence-based psychotherapy such as prolonged exposure (PE) or cognitive processing therapy. Both treatments are based on processing the emotional and cognitive aspects of the trauma. However, typically, the PTSD symptoms fluctuate throughout these treatments, and sustainable improvements can take much longer than expected due to avoidance in the form of “no shows,” “noncompliance,” and “cancellations” and yield mixed results (see Steenkamp et al., 2020). While sometimes PTSD symptoms don’t change dramatically, many veterans consider treatment a success due to improvements in quality of life, less disability, and increased perception of social support. Many continue to engage in other psychosocial interventions that reinforce and support these very social bonds and connections. This fictional case presentation shows us that there is no wrong door to access social support. Additionally, having a “new experience” in a robust social network can change perceptions of the individual veteran.
The work with Mr. Doe highlights how various forms of social support (i.e., informational, tangible, emotional) can have collective positive effects on veterans’ postdeployment readjustment, social network engagement, and quality of life. The changes reported in this fictional composite case are consistent with the work of Price and colleagues (2013) who showed that assisting veterans in enhancing their social support networks can complement engagement in formal mental health treatment, perhaps creating a positive synergistic effect on treatment engagement and mental well-being. They discovered that social support during treatment is associated with greater reductions in PTSD symptoms during PE treatment. More specifically, specific types of social support including emotional and informational support were positively related to increased treatment response. It should be noted in the study that PTSD symptoms did not moderate changes in social support.
Limitations/Conclusions
In conclusion, impaired social networks can be conceptualized as both the antecedent and the consequence of combat trauma. However, the perception that veterans have someone to talk to among friends, peers, or family; having someone to go to for advice, money, or other assistance; and feeling valued in one’s life can make a significant difference in overcoming war trauma and military transitions. There may be many routes to wellness, and social support is an important variable to consider in a multimodal, ecological approach to the treatment of postwar veterans.
Additionally, elucidating nonclinical supports or protective factors may be critical to supporting veterans of color, given evidence of racial and ethnic disparities found among African American and Latino veterans in the VA health care system. That is, evidence suggests that members of these populations are less likely to receive a minimal trial of any treatment in the 6 months after being diagnosed with PTSD (Spoont et al., 2015). While there may be myriad contributors to this disparity, assisting such veterans in cultivating social support networks could offer a protective effect amid other internal or external barriers to traditional mental health treatment. Future research should explore whether assisting veterans in enhancing their levels of social support—perhaps in the form of peer support or other social networking—impacts PTSD symptom severity.
The cross-sectional, correlational design limits interpreting directionality with regard to the relationship between mental health symptoms and perceived social support. Despite this, various explanatory models may help to illuminate the current findings. First, a longitudinal trajectory approach suggests that people have different responses to trauma across time, captured by four patterns: low stable post-traumatic stress or resilience (a large majority of the military population), gradual recovery of post-traumatic stress symptoms, delayed reactions, and chronic dysfunction (Bonanno, 2004; Bonanno, et al., 2012). The directionality and temporality of perceived social support may be multidimensional, and it is plausible that chronic PTSD symptoms could degrade actual sources of social support over time (King et al., 2006; Laffaye et al., 2008). Future research should examine how perceived social support and PTSD symptom clusters interact over time, as symptom clusters such as avoidance and emotional numbing may be critical factors illuminating the nuances of how combat veterans may benefit from perceived social support over the long-term following combat trauma.
Social support perception may also reflect the quality of secure adult attachments, which is a protective factor in coping with stress (Mikulincer et al., 2011). Adult attachment is an outgrowth of the early attachment relationship between the infant and caregiver; the former sets the stage for all future social connections. Therefore, attachment patterns may play an important role in the development and maintenance of PTSD. Future research should also examine how perceived social support, attachment style, and PTSD symptoms interact over time, as attachment patterns may be another critical factor shedding light on the nuances of how combat veterans may benefit from perceived social support over the long-term following combat trauma. Additionally, while this study added a more diverse sample of participants to the perceived social support knowledge base, there remains a relative dearth of literature illuminating the role of perceived social support in the mental health outcomes of persons of color and female combat veterans, which future researchers should investigate.
In summary, the present investigation provided data regarding associations between perceived social support and psychopathology across functional domains of disability and quality of life in post–9/11 veterans. The findings are consistent with other cross-sectional studies showing associations between perceived social support and positive readjustment after trauma (e.g., Bryan & Heron, 2015; DeViva et al., 2016; Peitrzak et al., 2010; Wilcox, 2010). Novel findings include the differential associations between the perceived social support on quality of life, mental health–related disability, and anxiety.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Department of Veterans Affairs (I01CX000913 to KLP).