
Abstract
Adverse childhood experiences are traumatic early life experiences that can lead to poorer mental, physical, and social outcomes. Children in military and veteran families can face unique challenges compared with civilian families. This study utilizes data from 2017–2019 National Survey of Children’s Health to examine 56,655 children living in military, veteran, and civilian families to predict the prevalence of adverse childhood experiences. Findings indicate that children living in veteran families (compared with civilian families) have higher odds of witnessing parents use violence and witnessing parents with alcohol or substance use problems. Children in military families had higher odds of divorce and lower odds of experiencing parental death. It is also noted that children living in military, veteran, and civilian families are similar across other ACEs including the incarceration of a parent, child as victim of violence, living with family with mental illness, unfair treatment because of race, and difficulty covering basics like food and housing.
Introduction
There are currently 1.2 million children living in families where one or both parents are current members of the United States Armed Services (USAS) (American Association of School Administrators, 2022) and 2.1 million more children living in families where one or both parents have served in the past (Hanson, 2016). Children of current USAS members and those living in veteran families can face unique challenges compared with families with non-military civilian parents (Sullivan et al., 2019), including high residential mobility, family separation, and poorer mental and physical health of parents (Cramm et al., 2019). Military deployment and subsequent family reintegration have been identified as unique family stressors (Balderrama-Durbin et al., 2015). Children experiencing parental deployment have been shown to have higher resting heart rates and evidence of increased diagnosis of stress-related disorders like posttraumatic stress disorder compared with children in non-deployed military and non-military families (Barnes et al., 2007). Rates of child abuse and neglect are also found to be higher in military families as the result of deployment and reintegration-related parental stress (Gibbs et al., 2007; Mmari et al., 2010; Rentz et al., 2008). On the other hand, military families are likely to live on or near their assigned duty station providing critical instrumental support and social support for families and children.
Children exposed to high levels of stress, neglect, and abuse can develop an impaired stress response system putting them at risk for poor health and social outcomes. A link between a child’s physical environment, their brain structure, and their physical health, social development, and learning outcomes has been established by child health researchers (Shonkoff et al., 2012). In stressful situations, a quick release of stress hormones prepares children for “fight or flight.” When children are exposed to repeated stressors, however, the stress response can become exaggerated and stress hormones can build up to toxic levels (Shonkoff et al., 2012). Exposure to toxic stress is linked with impaired neuroendocrine system development, delays in child development, impaired linguistic and cognitive skills, difficulty with social and emotional development (Shonkoff et al., 2012), poor physical health (Bright et al., 2016), poor mental health and lower utilization of important primary care services (Baron-Lee et al., 2015; Bright et al., 2016). Research has also linked toxic stress to difficulties in school (M. S. Hinojosa et al., 2019). The constellation of high stress experiences that include abuse, neglect, and household dysfunction are called adverse childhood experiences (ACEs) (Anda et al., 2006; Felitti et al., 1998).
The literature on ACEs among USAS families is limited. Some studies ask USAS members about ACEs, but only for themselves, not their children. These studies indicate that USAS members have a higher likelihood of reporting ACEs when they were children compared with civilian counterparts (Blosnich et al., 2014; Katon et al., 2015; Murphy & Turgoose, 2022). Other studies provide information about ACEs, but only certain experiences like child abuse and neglect and do not include the constellation of other ACEs like family dysfunction. Studies like this find that children are more likely to be the victim of child abuse and neglect during parental deployment (Gibbs et al., 2007). Other studies focus on the mental and behavioral health of children in military families with a focus on family separation, finding more mental health and behavioral problems during parental deployment, but no mention of ACEs (Barker & Berry, 2009; Chandra et al., 2010; Chartrand et al., 2008; Fairbank et al., 2018). One recent study expanded this literature by taking a national data set to compare military, veteran, and civilian families to understand the mental health and treatment outcomes of children. This study found that certain mental health triggers for civilian children—frequent moves, parental separation, and poor parental health—were not in place for children in active-duty military families suggesting better mental health outcomes for children in military families (M. S. Hinojosa et al., 2022). Although informative, none of these studies provide information about the national prevalence of ACEs in military, veteran, and civilian families.
This study aims to fill an important gap in our understanding of the ACEs of children living in military and non-military families by contributing to the literature in three important ways. First, this study utilizes a national sample of children living in the United States. Having a national perspective is necessary as older studies tend to focus on children at particular sites, such as in individual states, or on military installations. Second, we explore multiple ACEs using measures that have generally not been available to studies utilizing only clinical data, child maltreatment data, or data available from solely USAS sources. Finally, this study measures the prevalence of ACEs in civilian families, veteran families, and current military families and makes comparisons. As noted, previous research tends to omit a non-military comparison group. Thus, the purpose of this study is to identify the prevalence of ACEs in a national sample of children living in current military families, veteran families, and civilian non-military families living in the United States.
Adverse Childhood Experiences
Adverse childhood experiences (ACEs) are the collective name for those early life experiences that are experienced as traumatic. ACEs refer to the experience of domestic violence; parental abandonment through separation or divorce; living with a parent with poor mental health; being the victim of physical, sexual, and/or emotional abuse; emotional and physical neglect; having an important member of the household in carcerated; and/or living in a household in which an adult is experiencing alcohol and drug use problems (Anda et al., 2006). Any of these ACEs can have profound effects on children’s health and social outcomes. Children exposed to one or more ACEs are more likely to drink alcohol and/or use illicit drugs in childhood (Anda et al., 1999). Children with ACEs are more likely to be obese, sexually promiscuous, are less likely to maintain supportive social networks, and are at higher risk of school failure (Anda et al., 1999, 2006). School age children with any ACEs are more likely to be diagnosed with multiple physical, mental, and developmental health conditions including attention-deficit/hyperactivity disorder, anxiety disorder, autism, developmental delays, depression, and dental problems compared with children without ACEs (Bright, Alford, et al., 2015; Bright, Knapp, et al., 2015). Children with ACEs are also more likely to lack access to routine health care that could help ameliorate the effects of their health conditions (Baron-Lee et al., 2015). The research is clear that children exposed to ACEs are at higher risk for health problems and health risk behaviors such as alcohol and substance misuse, autoimmune disease, heart problems, and obesity and diabetes when they become adults (Anda et al., 2006).
Children with parents who are current or former USAS members face unique challenges compared with children living in civilian non-military families. As part of normal military duty, there is a greater risk for parental absences and the stressors associated with post-deployment family reintegration, and greater potential for parental mental illness and/or physical injury. USAS members have a higher likelihood of developing a number of debilitating chronic physical health conditions relative to their civilian counterparts, including activity-limiting cardiovascular diseases and musculoskeletal disorders (R. Hinojosa, 2019a, 2019b; R. Hinojosa & Hinojosa, 2016). They also have a higher likelihood of having a diagnosed mental health disorder due to exposure to stressful events, especially as they relate to military combat zone deployments (Castaneda, 2008; Kessler et al., 1995; Lester et al., 2016). Children exposed to parental mental health problems are at greater risk for developing traumatic stress disorders (Felitti et al., 2019; Smith, 2004). Research has also shown that when a parent or primary caregiver suffers from negative physical health, there is an associated increased risk of poor child mental health outcomes (Chandra et al., 2010; Hisle-Gorman et al., 2019; Kieffer-Kristensen et al., 2011; Rivara et al., 2014).
Children in military families face increased risks of abuse, neglect, and household dysfunction as parents leave for duty or deployment and as the result of the parental stressors associated with reintegration back into the family (M. S. Hinojosa et al., 2019; R. Hinojosa et al., 2012). For example, researchers studied Texas State reports of child abuse and neglect and found them to be higher during the period just prior to parental deployment and just after parental reintegration into the family (Rentz et al., 2007). A study using national military medical treatment center data found that children in military families where a parent was deployed had higher rates of mental health diagnoses compared with non-deployed military parents (Mansfield et al., 2011).
There are a few reasons why we might expect children in military families to experience higher numbers of ACEs. First, studies of military personnel indicate that adults who had served in the military report higher rates of ACEs when they themselves were children (Larson & Welch, 2007). Research finds that the experience of trauma can be intergenerational where people who have experienced trauma are more likely to parent in ways that transmit the trauma to their children either directly or indirectly (Isobel et al., 2018). Research also indicates that children of people who have served in the USAS are more likely to serve in the USAS when they reach adulthood (Pew Research Center, 2011). This has implications for military families as the recruitment pool of people and families may contain trauma experiences.
There are also a few reasons why we might expect more resilience among military families. Researchers have focused in recent years on how families draw strength and demonstrate resilience in the face of adversity. Resilience refers to the actions families take to adapt to adversity and overcome difficulty (Oshri et al., 2015). One important element of family functioning, especially as it is related to ACEs, is family resilience and social support. The USAS has recognized this important element of families and provides support for service members and their families. Approximately one-third of active-duty military members live on the military base at which they are stationed and the rest live in the community nearby (U.S. Department of Housing and Urban Development, 2015). This provides a sense of community and a shared sense of belonging and allows families to access military community supported child care, education, health care, and social support networks. In a recent study using the National Survey of Children’s Health (NSCH), researchers showed that regardless of parental deployment status, USAS parents had children with better mental health outcomes compared with their non-military civilian counterparts. This held true even when adjusting for the effects of multiple residential moves, parent health status, and deployment away from home. The researchers concluded that even with the known challenges faced by USAS families, children in military families tend to have better access to high-quality health care, health insurance, and more tightly integrated social support networks. These positive aspects of military family life may, in fact, promote greater overall resilience and have been found to ameliorate the impact of ACEs-related problems in children (Easterbrooks et al., 2013).
This study will use the NSCH to ensure a national sample comparison of ACEs and the children of current military parents, children of military veterans, and the children of non-military civilian parents. This study will also explore multiple ACEs, including domestic difficulties, parental abandonment, poor parental mental health, physical, sexual and/or emotional abuse, emotional and physical neglect, parental incarceration, and parental substance use disorders. The goal of this research is to better understand the prevalence of ACEs in a national sample of children living in military and non-military families in the United States.
Method
Data and Participants
The National Survey of Children’s Health (NSCH) conducted annually by the US Census Bureau was used to conduct these analyses. The NSCH was created and administered to report on the physical and emotional health of U.S. children. The NSCH sends it surveys to random U.S. households that are identified as having at least one child between the age of 0 to 17. A family member who knows the most about the child is asked to respond to either a mailed or web-based survey about the selected child. Households with children 5 years of age or younger or households that had children with special health care needs were oversampled. Most of the respondents were parents, guardians, or foster parents of the children and therefore we will use the term “parents” to refer to this group for the remainder of the article. The 2017, 2018, and 2019 years of the NSCH were pooled to increase the sample size of the main population of interest, military, and veteran families for a final analytic sample of n = 56,655. All analyses were weighted according to NSCH instructions for complex sampling strategies to make the findings generalizable to the U.S. population.
Dependent Variable: Adverse Childhood Experiences
The NSCH asks nine ACE questions. This includes a child experiencing the following: (1) parent or guardian divorced, (2) parent or guardian death, (3) parent or guardian time in jail, (4) adults slap, hit, kick, or punch others, (5) being a victim of violence, (6) living with a mentally ill family member, (7) living with a person with an alcohol or drug problem, (8) being treated unfairly because of race or ethnicity, (9) not having enough money to cover basics like food or housing. All ACE survey items were coded 1 = experienced the ACE and 0 = did not experience the ACE. The one exception was the question asking about having enough money to cover basics, which was originally coded as a Likert-type scale question. This item was recoded so that 1 = experienced somewhat often or very often and 0 = experienced rarely or never. The current poverty rate for children living in the United States is 16%, and the choice to collapse the two items “somewhat often” and “very often” was supported because 17.02% of the weighted sample fell into this category (Creamer et al., 2021). In addition to examining each ACE individually, this analysis also sums up all nine ACE responses into a count index of ACEs for each child. This index ranges from 0 indicating no ACEs, to 9 indicating that the child had experienced all nine ACEs.
Independent Variables
Child Variables
Child Mental Health: Parents were asked if their child was diagnosed with one of the following four mental health disorders: anxiety disorder, attention-deficit hyperactivity disorder, behavioral disorder, or depression. These variables were summed into a single variable where 0 = no mental health disorders reported and 1 = one or more mental health disorders reported.
Child Mental Health Treatment: Parents reported whether their child had received treatment for a mental health condition in the past 12 months. This variable is coded 1 = yes, treatment was received and 0 = no treatment was received. A variable identifying if the child has access to insurance is included so that 1 = child has access to public insurance, 2 = child has access to private insurance, and 3 = child has access to both public and private insurance.
Family Variables
Military, Veteran and Civilian Families: Parents of the sample child were asked if they had served in the U.S. Armed Forces. If neither parent had ever served in the military, the family was identified as a civilian family. If one or more parent had served on active duty in the past but were not currently serving, the family was labeled a veteran family. If one or more parents were currently serving on active duty or active reserve duty (either deployed to theater or not) the family was labeled a military family. Family structure is coded so that 1 = two parents in the home, either biological or stepparents, 2 = single parent households including single moms and single dads, 3 = other family type which includes guardians, foster parents, and grandparents. Parent education is coded so that 1 = parent has high school degree or less, 2 = some college education or an associate degree, 3 = a college degree or graduate/professional degree. Parent physical and mental health was measured through two items on the questionnaire. Parents reported the state of their current mental and physical health. Responses were coded so that 1 = excellent or very good health, 0 = good, fair, or poor health. The omitted groups for the regression analysis were civilian families, two-parent family type, high school diploma or less for parents, good/fair/poor mental and physical health of parents.
Parent emotional support was measured by a set of eight survey items. Parents were asked to indicate which and how many of the eight types of emotional support they received related to parenting and general well-being. Parents reported on whether they had received emotional support from a health care provider, a spouse, their family, their church, through a health condition support group, a peer support group, a professional counselor, or some other source of emotional support. Responses were summed into an index ranging from 0 to 8 where 0 = no emotional support utilized and 8 = parent utilizes all types of emotional support. Family resilience was measured by four survey items. Parents were asked which of the following types of things they did when the family faces problems: the family stays hopeful, the family draws strength from one another, and the family works together and talk to each other to create solutions. Responses are coded so that 3 = the strategy is utilized all the time, 2 = the strategy is utilized most of the time, 1 = the strategy is utilized some of the time, and 0 = the strategy is utilized none of the time. A summative scale was created that ranged from 0 to 12, with 0 indicating no resilience strategies utilized and 12 indicating all resilience strategies utilized. A reliability test indicates that the three items have high internal consistency with a Cronbach’s alpha score of 0.8866.
Control Variables
Child’s sex was coded 0 = male and 1 = female. The race of the child was collected and organized by NSCH and was coded as 1 = White, 2 = Black/African American, 3 = Other race which includes Asian American and Multiracial. A separate ethnicity category was included where 1 = Hispanic/Latino and 0 = Non-Hispanic/Latino. For the regression analysis, the omitted categories include male child, White race, and non-Hispanic ethnicity. Child age was measured in years and ranged from 0 to 17. To test for the possibility that ACE exposure may follow a curvilinear pattern, a quadratic term was created by squaring the age variable (age2).
Analytic Strategy
The purpose of this study was to use the 2017, 2018, and 2019 pooled data from the National Survey of Children’s Health to understand the probability of a child experiencing ACEs when they are part of a military family, a veteran family, or a civilian family. All analyses were conducted using Stata 16 SE. The data were weighted using the Stata code provided in the methodology report published by the NSCH (U.S. Census Bureau, 2019). To calculate the odds of a child experiencing any of the ACEs within civilian families, veteran families, and military families, nine logistic regressions were run, one for each ACE serving as the dependent variable. Next, a negative binomial regression was run to predict the count of ACEs between civilian, veteran, and military families. Negative binomial regression was the most appropriate analysis because the ACE scale showed evidence of overdispersion (Long & Freese, 2014). Overdispersion in the dependent variable occurs when the mean is smaller than the variance. In this study, the dependent variable was the count of ACEs each child has. This count ranged from 0 to 9 with most of the data (95.59%) clustered around 0, 1, 2, and 3. Table 1 displays the weighted proportions of this variable. One clear indicator of overdispersion is that the mean of the ACE scale is smaller than the variance. In this case, the unweighted mean of the ACE scale is 0.659 and the variance is 1.369. The general rule is that if the variance is twice that of the mean, this is evidence of overdispersion (Hoffman, 2016). A second way to identify evidence of overdispersion is to examine the dispersion parameter (sometimes called the alpha parameter) within the fully specified negative binomial regression model. If the dispersion parameter equals zero (parameter is not significant at the p < .05 level), then the negative binomial regression reverts to a Poisson regression (best for count data with normal dispersion). If the dispersion parameter is greater than zero (parameter is significant at the p < .05 level), then the negative binomial model is run (Hilbe, 2011). In our model, the dispersion parameter (0.389 with a 95% confidence interval [CI] of [0.32, 0.46]) was significantly different from zero, indicating that negative binomial regression was the best model for these data.
Weighted Descriptive Statistics for ACEs, Family Type, Child, Family, and Sociodemographic Variables.
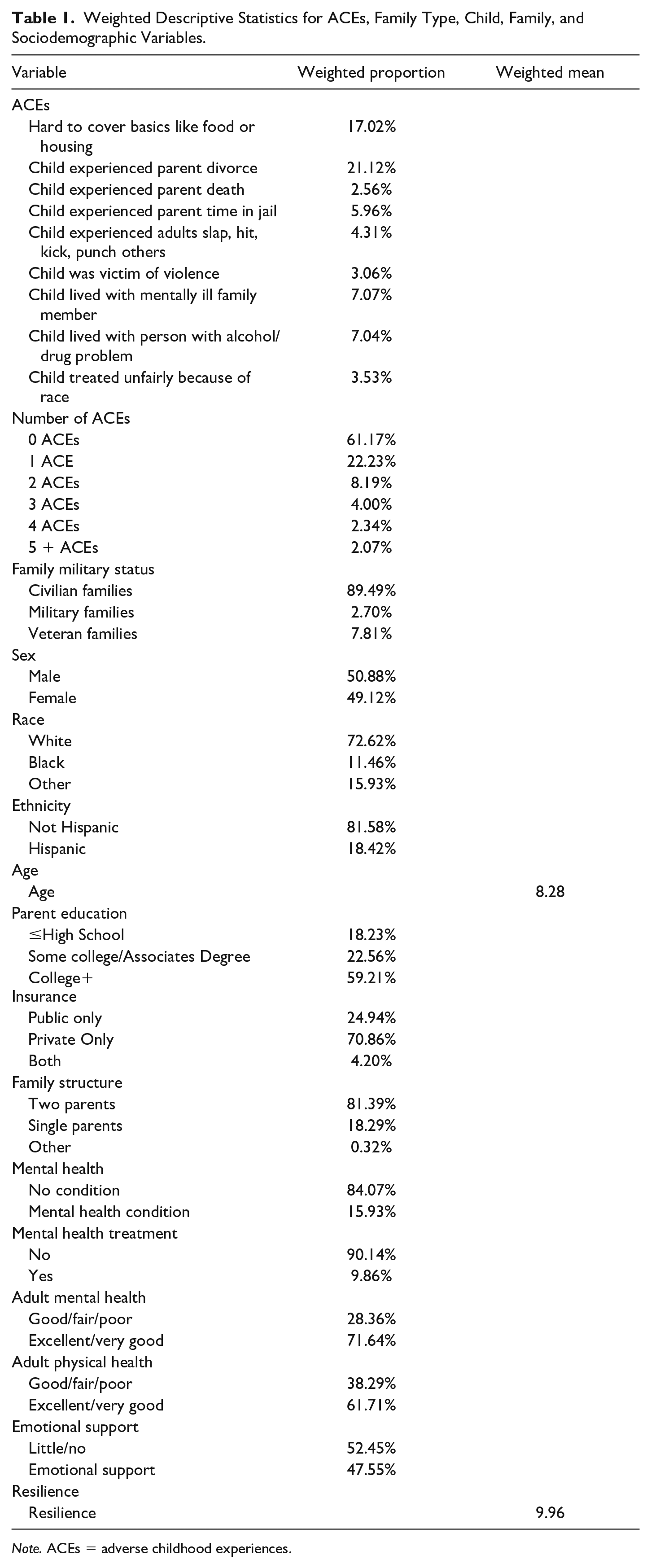
Note. ACEs = adverse childhood experiences.
To ensure that our logistic regression models are performing well, we employed ROC (receiver operating characteristic) statistics to test the sensitivity and specificity of our predictions in our logistic regressions. Sensitivity is the chance that we correctly predicted the “right” answer or the rate at which our model predicted correctly that a child experienced an ACE. Specificity is the chance that we correctly predicted the “wrong” answer or the rate at which our model predicts that a child did not experience an ACE when they truly did not. The ROC statistic is a number ranging between 0 and 1, with 0.5 indicating that our model is no better than chance alone (think of a 50% chance of seeing “heads” when flipping a fair coin). The closer to 1 the ROC number, the better the model. Most scientists use and ROC of 0.7 or higher to indicate an acceptable model (Carter et al., 2015). In our analysis, all models had an ROC of .78 or higher indicating strong, well-fitting models.
Results
Table 1 displays the descriptive statistics for all variables included in our models. These include sociodemographic variables (sex of the child, race/ethnicity of the child, parent educational level, age of the child, and family structure), child health variables (mental and physical health, mental health treatment, and health insurance status), and family variables (parent emotional support, family functioning, and parent health).
Civilian families were most common at 89.49%, followed by veteran families (7.81) and military families (2.70%). Half of the children in the sample were male (50.88%) and 72.62% were White non-Hispanic. A little over 11% were Black, non-Hispanic and 15.93% identified as other race. Eighteen percent were Hispanic/Latino. The average age was 8.28 years. Most parents had some college or a college degree or higher (81.77%) and most children were living in two-parent biological or stepparent families (81.39%). About 16% of parents reported that their child had a mental health condition and 9.86% reported treatment for a mental health condition in the past 12 months. Most parents reported excellent or very good mental health (71.64%) and physical health (61.71%). More than half of parents reported little or no emotional support (52.45%), and the average resilience score was 9.92 on a scale from 0 to 12, indicating higher levels of resilience.
The purpose of this study was to understand the odds of experiencing ACEs among military, veteran, and civilian families. The first set of logistic regression models examine the probability of experiencing each individual ACE controlling for all sociodemographic, child, health, and family factors. Table 2 displays the results of nine logistic regression models. Each model is fully adjusted for all child, family, and sociodemographic variables. In each logistic regression model, civilian families are the omitted category, which means that the odds ratios produced for veteran and military families are in comparison to civilian families.
Logistic Regression for Individual ACES by Family Type Adjusted for Child, Family, and Sociodemographic Characteristics.
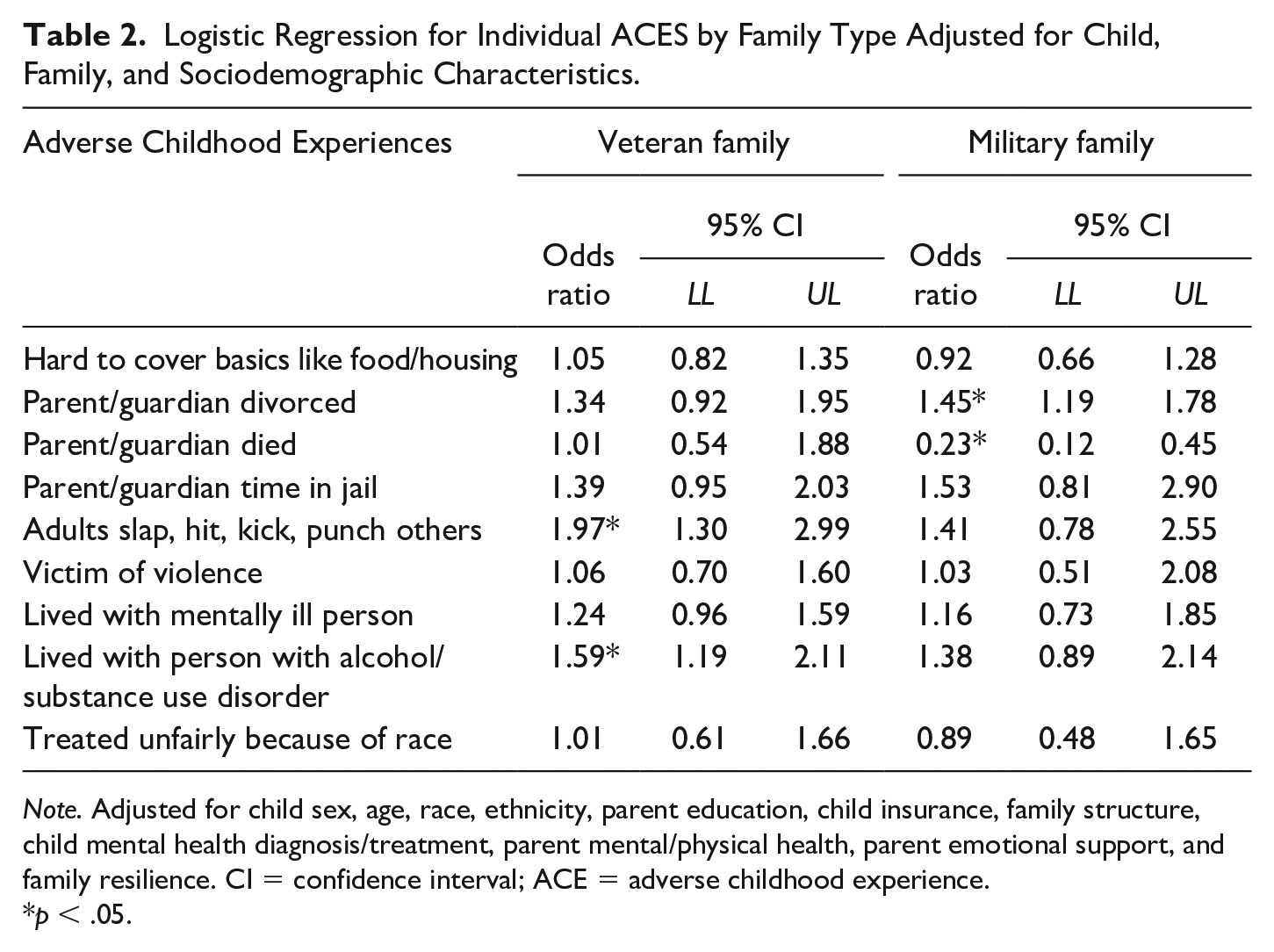
Note. Adjusted for child sex, age, race, ethnicity, parent education, child insurance, family structure, child mental health diagnosis/treatment, parent mental/physical health, parent emotional support, and family resilience. CI = confidence interval; ACE = adverse childhood experience.
p < .05.
Children in veteran families are 97% more likely to report witnessing adults slap, hit, kick, or punch one another compared with civilian families controlling for child/family factors and sociodemographic variables (odds ratio [OR] =1.97, 95% CI [1.30, 2.99]). Children in veteran families are also 59% more likely to experience an adult in the home with an alcohol or substance use problem compared with civilian families controlling for child/family factor and sociodemographic variables (OR = 1.59, 95% CI [1.19, 2.11]). Children in military families have 45% higher odds of divorce compared with civilian families controlling for all other factors (OR = 1.45, 955 CI [1.19, 1.78]). Children in military families have an odds of parent death that is 77% lower than the odds of parent death in civilian families controlling for child/family factors and sociodemographic variables (OR = 0.23, 95% CI [0.12, 0.45]).
Children in civilian, veteran, and military families differed across four ACE categories—divorce, parent death, experiencing adults punching/slapping/hitting, and experiencing adult substance use. To further illustrate the significant differences in these four ACEs, predicted probabilities for each event were calculated. Predicted probabilities are the expected proportion of children experiencing the ACE given their family type holding all other variables constant. This is the probability of an event (ACEs) for each family type given the data controlling for all other variables in the model. Using this information, we can estimate the percent of each family type predicted to experience each ACE event. The predicted probabilities were calculated using Stata SE 16.0 using the margins command. The control variables (child, family, and sociodemographic characteristics) were all set at their mean and the expected probability of children experiencing each ACE given the data are summarized.
Figure 1 illustrates that 25.31% of children in military families were expected to experience divorce holding all other variables at their mean compared with 24.25% of veteran families and 20.58% of civilian families. Less than 1% (0.67%) of children in military families are expected to experience a parent death holding all other variables at their mean compared with 2.62% of children in civilian families and 2.64% of children in veteran families. When it comes to family violence like experiencing adults punch, hit, slap, or kick another, 7.13% of children in veteran families experienced this compared with 5.41% in military families and 4.03% in civilian families when holding all other variables constant at their mean. Finally, 9.81% of children in veteran families report experiencing an adult living with them that has alcohol or other substance use problems compared with 8.78% of military families and 6.74% of civilian families. While there were differences in family type among four of the ACEs measured, it is worth noting that there were five ACEs where military, veteran, and civilian families were statistically similar. There was no difference between family types as it related to (a) experiencing discrimination based on the child’s race; (b) parental incarceration, (c) child as victim of violence, (d) child living with seriously mentally ill family member, and (e) difficulty covering the basics like food and housing.
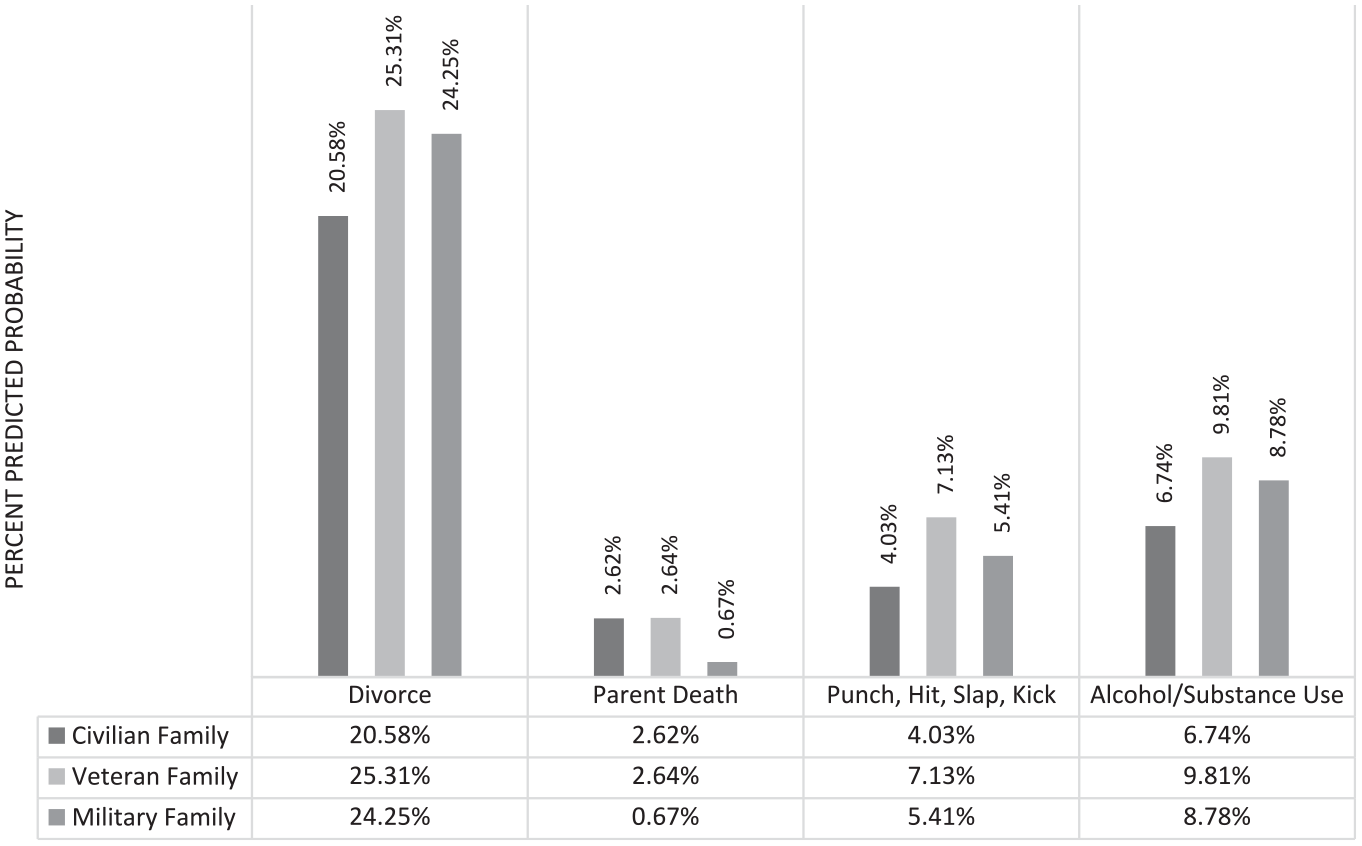
Predicted Probability of ACEs by Family Type.
To understand how the count of ACEs are distributed among different family types controlling for all child, family, and sociodemographic factors, a negative binomial regression model was executed. The dependent variable in this analysis is the summative ACE scale that is treated as a count variable so that a score of 0 corresponds to experiencing no ACEs and a score of 9 corresponds to experiencing every ACE on the list.
Table 3 displays the results of the negative binomial regression. We report the incidence rate ratio (IRR) in the text. Controlling for all variables in the model, the ACE incidence rate ratio for veteran families was 24% higher compared with children in civilian families (IRR = 1.24, 95% CI [1.12, 1.37]).
Negative Binomial Regression for Count of ACEs by Family Type, Child, Family, and Sociodemographic Predictors.
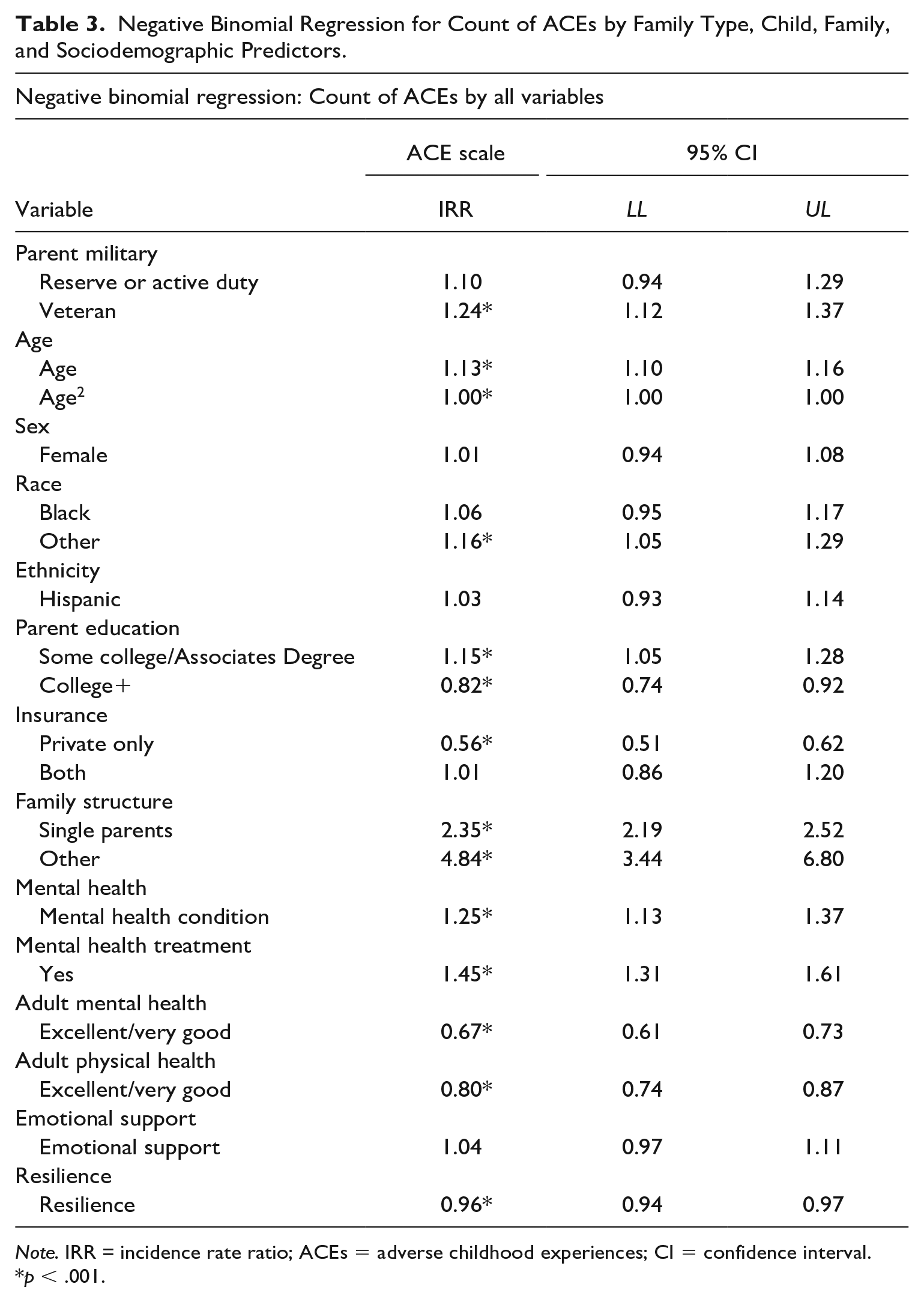
Note. IRR = incidence rate ratio; ACEs = adverse childhood experiences; CI = confidence interval.
p < .001.
This model also allows for the examination of child, family, and sociodemographic predictors of the count of ACEs. The model identified age, race, insurance status, parent education, child mental health conditions and treatment, family structure, parent mental health, parent physical health, and family resilience as significant predictors of the count of ACEs.
For every one unit increase in age, there was a 13% increase in the incidence rate (IRR = 1.13, 95% CI [1.10, 1.16]), or count of ACEs. Children identified as Other Race were 16% more likely to have higher counts of ACEs (IRR = 1.16, 95% CI [1.05, 1.29]), but there was no significant difference between Hispanic/Latino and Non-Hispanic/Latino children. Children with private health insurance had ACE counts that were 44% lower compared with children with public health insurance (IRR = 0.56, 95% CI [0.51, 0.62]). Children in families where parents had some college had slightly higher ACE counts (IRR = 1.15, 95% CI [1.05, 1.28]) compared with parents with a high school diploma or less. Children with parents holding a 4-year college degree or higher had lower ACE counts (IRR = 0.82, 95% CI [0.74, 0.92]) compared with parents with a high school diploma or less. Children with a mental health condition had 25% higher ACE counts (IRR = 1.25, 95% CI [1.13, 1.37]) and children utilizing mental health treatment had 25% higher ACE counts (IRR = 1.45, 95% CI [1.31, 1.61]) compared with children with no mental health problems or treatment. Family structure had the strongest effect on the count of ACEs among children with a 135% higher ACE count (IRR = 2.35, 95% CI [2.19, 2.52]) for single parents and 384% higher ACE count (IRR = 4.84, 95% CI [3.44, 6.80]) for other family structures such as guardians, grandparent, and foster parent families. Children living with parents experiencing excellent or good mental health had a 33% lower count of ACEs (IRR = 0.67, 95% CI [0.61, 0.73]) or fewer ACEs count compared with parents with good, fair, or poor mental health. Children with parents reporting excellent or very good physical health had a 20% lower count of ACEs compared with parents with worse physical health (IRR = 0.80, 95% CI [0.74, 0.87]). Children in families with higher levels of family resilience had a lower count of ACEs. For every one unit increase on the resilience scale, there was a 4% decrease in the count of ACEs (IRR = 0.96, 95% CI [0.94, 0.97]).
Discussion
Adverse childhood experiences like abuse, neglect, and household dysfunction are important stressors that many children face in family life. Children experiencing ACEs are at risk for developing high levels of stress hormones in their bodies. This high level of stress, often called toxic stress, in children is linked to stress-related disorders, mental, physical, and social problems for children when they are young and throughout the life course. Given the additional stressors that military members face, this study investigated the odds of experiencing ACEs among children living in military, veteran, and civilian families. The current literature on ACEs among children in military families is limited to retrospective studies conducted on adult military members, or studies using USAS data without a civilian or veteran control group. This study utilized national level data from children in the United States to examine ACEs in military, veteran, and civilian families to understand the current prevalence of ACEs. Results indicated a higher prevalence of three of the ACEs and lower prevalence for one of the ACEs between current military families and veteran families compared with civilian families.
Children living in military families had higher odds of experiencing divorce compared with civilian families. The expected prevalence of divorce among veteran families was 24% compared with 20% among civilian families. This study did not find a statistically significant difference between veteran families and civilian families. The higher divorce rate may be due to the stress of deployment and reintegration of the military family member as part of their work duties, mental health of military member, and non-military-related stressors like social support and work–family conflict (Pflieger et al., 2018). Research also indicates that military families marry earlier and have more children than their civilian peers which could lead to higher rates of divorce (Lundquist & Smith, 2005). Children in military families also have a lower prevalence of parental death. Based on the regression models, 2.6% of civilian families experience a parent death compared with 0.7% of military families. This finding runs counter the narrative that being in the USAS puts Americans at higher risk for fatalities. The lower death rates, however, could simply be related to the fact that once a military parent dies, the family status transitions to civilian or veteran status.
Findings from this study indicate that children living in veteran families were more likely to experience a family member with an alcohol or substance use problem. The expected percent of alcohol or substance use problems among children in civilian families was 6.7% compared with 8.8% for children in veteran families. This is in line with current research that identifies a higher prevalence of alcohol and substance use problems among veterans compared with military members and civilians (Boden & Hoggatt, 2018). Higher prevalence of substance use could be related to the unique challenges to military family life and trauma faced in the line of duty.
Children in veteran families are more likely to witness adults slap, kick, and punch others compared with civilian families. About 7% of children in veteran families have experienced this compared with 4% for civilian families. This is consistent with a recent meta-analysis which found that veteran families had higher prevalence of intimate partner violence compared with active-duty military families (Kwan et al., 2020). To ameliorate deployment stressors, most military families have access to Family Readiness Groups (FRGs), community support groups that provide social, educational, and (some) financial support promoting family resilience during their family members’ deployment (Army, 2020). Veteran families do not have access to these same resources, potentially making them more likely to engage in substance use or lash out with violent behavior. The data used in this study do not provide information about the experience of veteran parents as it relates to how or why they were discharged from the military. There is the potential that the veterans in the sample were discharged from active duty because of substance use problems or intimate partner violence.
There is some evidence that active-duty military families may have some protective factors in place to assist with family stress. For example, military families often live on or near military installations and have access to opportunities and interventions on base that can build resilience in the children and families (Huebner, 2019). Children may attend day care programs or schools that are sponsored by the Department of Defense, and they can access health care through both military treatment facilities as well as civilian medical practices relieving stress from families. The National Defense Authorization Act (NDAA) of 2010 created support programs for military families that have a child (or an adult dependent) with a special health care need. They can also receive military assignment locations where specialty care, health evaluations, case managers, individual service plans and support for care coordination are available. This is especially good for children with chronic health conditions and special needs. These things are not readily available for children and parents in veteran families, potentially leading to higher prevalence of family violence and alcohol/substance use problems. That said, civilians do not have these extensive support networks and appear to be doing better than military and veteran families, so the impact of military service cannot be denied.
Other research has found that the mental health of children in military families tends to be better even when they experience stressful events known to impact non-military children like frequent residential moves, parent illness or injury, and parent deployment (Hinojosa et al., 2022). For example, among children in current military families, the odds of reporting a mental health condition stayed the same regardless of the number of times the family moved residences. But among children in civilian families, increased numbers of residential moves were associated with higher odds of reporting mental health conditions. A similar pattern was seen when examining parent mental health. When parent mental health was worse, children’s report of mental health conditions was higher but only for civilian families and veteran families. Children in current military families had lower odds of mental health conditions regardless of parent’s mental health status. This finding runs counter to the national narrative of consistent sacrifice for families and children for military members, and while this study did not focus on ACEs, it did identify a specific advantage of being in a military family.
While making an important contribution, this study does have a few limitations. First, this study was not able to include important ACEs like physical and sexual abuse against the child. Parents served as primary reporters of their child’s experiences with ACEs, and therefore the NSCH chose not to include these ACEs as parents would not likely report these levels of abuse for fear of potentially incriminating themselves. Second, this is a national-level data set that was designed to provide information on the state of child health, well-being, development, and health care utilization in the United States. Since the purpose of the data was not to understand the experiences of military, veteran, and civilian families, we are missing some key information that could help us draw conclusions. It would be useful to know the status of veteran parents in the survey. For example, the circumstances of their discharge from the military could give important information about why we see higher odds of substance use and intimate partner violence. There are also potential consequences (or real fear of consequences) for military families to divulge that their child has been the victim of a traumatic experience within the family. Partners may have been reporting information about their child’s experiences with their military spouse, which could have led to bias, inaccurate reporting, or underreporting in the reporting of ACEs. Despite these limitations, this study provides an insight into the national prevalence of ACEs among military, veteran, and civilian families.
This study is meant to be an exploratory examination of different factors that could lead to children experiencing higher rates of ACEs. The purpose of this study is to identify the prevalence of ACEs in military families compared with non-military families controlling for other important sociodemographic and health-related factors. Future research on childhood trauma as it relates to military service should focus on understanding the ways that trauma affects families and children. The U.S. Department of Veteran Affairs has focused in recent years on trauma-informed care for military members with posttraumatic stress disorder, but this work could be expanded to offer services to spouses and children. Having better data about military families could also aid our understanding of how military service impacts child health outcomes and experiences with trauma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.