
Abstract
This article addresses a policy paradox that characterizes many health care systems and the Israeli system in particular, that is, the existence of two parallel yet seemingly contradictory policy trends: reducing public financing for health care services while increasing governmental involvement in health-system management. The authors characterize this process as privatization through centralization; that is, to control welfare-state expenses and be able to reduce them, the government must first control the funding and management of welfare-state mechanisms and organizations. They develop a theoretical rationale for explaining this policy paradox and demonstrate it through analyzing the legislative changes that followed the legislation of the National Health Insurance Law in Israel.
Health care systems around the world face significant challenges that often lead to reforms, transformations, and institutional changes, many guided and directed by the World Bank (Atkinson, 2002; Gruber, 2007; Standing, 1999; World Bank, 1993). Such reforms usually include strategies of decentralization, privatization, cost sharing, and participation that are offered to, or imposed on, national governments. The implementation of health care reforms in a given national setting, however, often produces contradictory processes—a phenomenon that we term here a policy paradox.
This article addresses a policy paradox that characterizes many health care systems and the Israeli system in particular: the existence of two parallel yet seemingly contradictory policy trends—reducing the public share in financing health care services while increasing governmental involvement in health-system management. Although the former trend can be understood as a privatization strategy, the latter trend expresses increased centralization. Given that privatization in its broad sense refers to the act of reducing the role of government or increasing the role of private institutions in satisfying people’s needs (Savas, 2005; Starr, 1989), centralization is in effect the opposite of privatization. Therefore, these two strategies are usually considered contradictory, thereby producing a policy paradox. The explanation of this policy paradox is a central research question in this article.
In early 1995, Israel reformed its health care system by enacting a National Health Insurance Law (NHIL; NHIL, 5754-1994). Since then, all persons with resident status in Israel have had health insurance. Several studies describe the principles of the reform and the processes that led to its maturation (Chernichovsky & Chinitz, 1995; Chinitz, 1995; Horev, Babad, & Shvarts, 2003). The main goals of the reform were to provide universal health coverage, spell out residents’ entitlement to a basic package of health care services (a “health basket”), promote increased equity, assure the solvency of the health care system, give residents greater freedom of choice among health funds (the public nonprofit organizations [NPOs]—nonprofit health care providers—similar to American health maintenance organizations [HMOs] that deliver health care services under the NHIL), and absolve the Ministry of Health (MOH) of operational responsibility for the provision of health care services, thereby allowing MOH to devote more effort to monitoring and regulating the system. However, throughout the implementation process, health care policy was inconsistent with these goals, as manifested among other things in a plethora of legislative initiatives that changed the nature of the NHIL significantly.
A systematic examination of these legislative initiatives uncovers the policy paradox that characterizes Israel’s health care system. As we demonstrate below, during the NHIL’s 12 years of implementation, the public share in the financing of health care services has declined significantly (Bin Nun & Kaidar, 2007a; Horev, 2004) whereas the involvement of the government, through the ministries of Finance and Health, has not declined as the NHIL intended but rather has increased (Horev, 2004; Horev & Babad, 2005). These parallel processes of privatization and centralization constitute the policy paradox in the Israeli health care system.
To explain this policy paradox, we develop the following argument. Studies of welfare-state retrenchment and new institutionalism point to a strategy of privatization through centralization, that is, to reduce public funding of the welfare state, the government must first control the funding and management of welfare-state mechanisms and organizations (Pierson, 1995). Such control is often achieved through centralization and even nationalization of resources and management mechanisms. When control is achieved, the government can gradually reduce the funding of the welfare state. Similar dynamics exist in health care systems, which often experience privatization through centralization (Hacker, 2002).
This rationale does much to explain the policy paradox in the Israeli health care system, in which the government first took control of the funding of the system by means of earmarked taxes collected by the National Insurance Institute (the social-insurance mechanism)—a compulsory progressive health tax paid by each adult resident and a “parallel tax” paid by employers. We will show that the government then tightened its control of the health care system by pushing through various legislative amendments of the NHIL that regulated the powers, management, and supervision of the health funds, even though this was not part of the underlying rationale of the NHIL. All these measures have enabled the Ministry of Finance to gradually reduce the public share in the funding of health care services as part of its general and ongoing policy, yet not necessarily planned for the long term, of retrenching the welfare state.
A central argument in this respect suggests that the centralization strategy was primarily aimed at controlling expenses so that resources could be shifted and flexibly reallocated in case of an economic or military crisis. The analysis that follows shows that although bureaucrats at the Ministry of Finance may have had a general policy paradigm of reducing government intervention in the economy, most of their activities and initiatives toward the health care system have been related to short-term moves rather than being the results of long-term plan of retrenching the welfare state.
Thus, latent privatization processes in the Israeli health care system have occurred via incremental policy making, with the Ministry of Finance adopting an approach of “muddling through” in budget management and resource allocation (Lindblom, 1959; Wildavsky, 1984). However, the fact that this behavior is facilitated by centralization processes increases the potential for inefficiency. Practically speaking, it does not allow market forces to take part in the health care system although the government retreats mainly in the financial aspect. Consequently, residents are increasingly required to find their own solutions to the resulting shortage in health care services. They seek immediate solutions in semilegal or “black” markets, which, in turn, are institutionalized by the government, thus exacerbating the lack of long-term planning in the system.
This article does not attempt to offer a comprehensive model for explaining all social policies or even policies regarding the health system. Rather, our goal is to explain and demonstrate a specific mechanism which often typifies policy making in the areas of the welfare state. By explaining the mechanism of privatization through centralization and its specific characteristics in the Israeli context, we hope to shed light on the advantages and disadvantages of an essential dynamic in the area of social policy.
The article proceeds as follows. The next section first presents the central arguments that the new institutional literature bruits as explanations for transformations in welfare states in general and health care systems in particular. At the core of these transformations lie different forms of privatization. Then we offer main central explanations for the transformation of the Israeli health care system. The section titled “Privatization Through Centralization in the Israeli Health Care System as Expressed in Post-NHIL Legislation” reviews the main legislative initiatives in 1995 to 2008 to change and update the NHIL and explains the rationale of privatization through centralization in the Israeli health care system. The section titled “Discussion” concludes the analysis and explains the inefficiencies embodied in this strategy.
Health care Reforms and Welfare-State Retrenchment From a New Institutional Perspective
This section first presents the foundations of a new institutional analysis and its application to health care reforms and then reviews the main arguments regarding the transformation of the Israeli welfare state, focusing on the changing role of trade unions and the increasing dominance of the Ministry of Finance after the 1985 economic stabilization plan. To complete the theoretical setting, we present main arguments relating to the transformation of the Israeli health care system.
The New Institutional Approach and the Analysis of Health Care Systems
The new institutional approach focuses on the analysis of institutions, that is, their evolution and influence. Institutions are defined formally by laws, regulations, and authoritative decisions as well as informally by rules such as norms (North, 1990; Steinmo, 2001; Voos, 2001). Furthermore, processes of policy formation and implementation often include making and changing rules, meaning that the new institutional approach can be integrated into policy analysis.
A central focus in the new institutional research is the role of the state and its intervention in social and economic interaction. In this context, major research questions refer to the status and transformation of the welfare state, forms and strategies of privatization, and centralized versus decentralized governmental mechanisms (Pierson & Skocpol, 2002; Streeck & Thelen, 2005). The framework elaborated by the new institutionalism creates a well-equipped toolbox for the analysis of institutional reforms generally and health care–system reforms particularly.
The new institutionalism suggests two main approaches for the analysis of institutional change. The first, which dominates the literature, relies on a strong punctuated equilibrium model in which lengthy periods of institutional stability are interrupted by some sort of exogenous shock or crisis that leads to a more-or-less radical reorganization followed by institutional stability (Beissinger, 2002; Katznelson & Weingast, 2005; Pierson, 2004; Pierson & Skocpol, 2002; Streeck & Thelen, 2005). The crisis period that triggers significant institutional change is characterized as a critical juncture and is explained by using the concept of path-dependent analysis, that is, analysis of the processes, attitudes, and actions that create the conditions for institutional change (Mahoney, 2000; Pierson, 1995, 2004). To a large extent, these processes influence the specific characteristics of institutional change. An existing coalition of interests in favor of a certain status quo, for example, may create a “lock-in effect” that impedes significant institutional changes (Pierson, 1995). Furthermore, existing policy influences the nature of institutional change due to the impact of “policy feedback,” that is, central players’ experience with the existing policy.
In his comparative analysis of health care policy in Britain and the United States in the 1980s, Pierson (1995) shows that in Britain, the combination of positive policy feedback and a strong lock-in effect blocked many privatization initiatives of the Thatcher Government, whereas in the United States, opposite conditions allowed significant changes under the Reagan Administration.
The second approach toward the analysis of institutional change focuses on incremental transformative change (Hacker, 2004; Streeck & Thelen, 2005). Incremental and gradual changes may be minor ones that adapt or reshape an existing institution or major ones that completely revamp the institution and are therefore transformative. The comparative literature suggests several types of transformative institutional change: displacement, layering, drift, and conversion (Streeck & Thelen, 2005).
Hacker (2002, 2004), analyzing the main dynamics and changes in the American health care system since the 1980s, demonstrates the roles played by these four forces. In particular, he develops the mechanism of drift, arguing that it explains the evolution of the private provision of health care services in the United States.
Drift occurs when, despite external changes, the maintenance of existing institutional structures is neglected until they fail (Hacker, 2004). As a result, players are forced to find institutional alternatives. However, they attain this goal, not by reforming the rules, which remain unchanged in the face of evolving external conditions, but by marginalizing them. Hacker (2004) demonstrates how the American public health care system shrank due to the nondecisions of conservative politicians and administrators who deliberately avoided the financial adjustment of health-insurance programs to changing conditions, resulting in risk privatization.
In the past decade, the Israeli health care system has faced similar drift processes that signified the privatization trend in health care policy. However, this policy not only deviated from the original underlying rationale of the NHIL (Chernichovsky & Chinitz, 1995; Gross, Rosen, & Chinitz, 1998) but also became possible due to the nationalization of the funding mechanism through earmarked taxes collected by the National Insurance Institute—a compulsory progressive health tax paid by each adult resident and a parallel tax paid by employers. This was an early indication of the centralization trend that was subsequently expressed in ongoing legislative initiatives. Together, these trends make up the ostensible policy paradox of privatization through centralization—a strategy pointed out by Pierson (1995).
In analyzing the typical strategies used by advocates of welfare-state retrenchment, Pierson (1995) suggests three basic ground rules for the study of retrenchment. First, one should examine long-term as well as short-term spending cuts. Second, one should examine program structure as well as program spending. Third, one needs to study systemic retrenchment as well as programmatic retrenchment. Programmatic retrenchment is the result of spending cuts or the reshaping of welfare-state programs. Policy changes that alter the context of future spending decisions—in what may be termed systemic retrenchment—may be as important for the welfare state as changes in the structure of the spending program “within” the welfare state itself. This distinction is crucial in the study of welfare state retrenchment.
Pierson (1995) further elaborates on possible forms of systemic retrenchment. First, a government may attempt to defund the welfare state by constraining the flow of revenues to future administrations. Second, its policy may induce a change in public opinion, weakening popular support for the public provision of social services. If government policies whet the public’s preference for the private provision of these services, retrenchment may be facilitated by the public’s growing hostility toward public social programs.
The third form of systemic retrenchment includes modifications in political institutions, changing the way welfare-state decisions are made, and thus, potentially, changing policy outcomes. In this respect, Pierson (1995) suggests the following:
Retrenchment advocates possess two strategic options that might make institutional conditions more conductive to the pursuit of cutbacks: They may try to centralize political authority, hoping to increase their capacity to implement their own policy preferences; alternatively they might pursue decentralizing strategy, transferring authority over social policy to local governments. (p. 16)
We term the first of these strategies privatization through centralization and propose that it explains the ostensible policy paradox in which privatization and centralization coexist.
The fourth form of systemic retrenchment includes the weakening of prowelfare state interest groups. Groups that depend on government financing are likely to be highly vulnerable.
However, these strategies may reduce popular support for politicians and, in turn, increase political costs. Pierson (1995) addresses this point by identifying several strategies that politicians who wish to be reelected may invoke to reduce their risks. The first is obfuscation—manipulation of the information flow to reduce public awareness of retrenchment actions or their negative consequences. This goal may be basically achieved by minimizing the importance of negative consequences and by “implicit privatization,” in which benefits retain their real value but play a diminishing role in an expanding economy and by reducing the visibility of their actions and diminishing traceability. The second strategy is dividing the opposition. The third includes compensation for the victims of retrenchment policies, which limits attacks from the opposition.
Both types of strategies—retrenchment and minimization of costs— have been adopted by Israeli bureaucrats and politicians since the 1980s. They have been also intensively used in setting policy and the institutional structure of the health care system since the mid-1990s. We now present the major transformations in these areas; then, in the next section, we explain in detail the changes in the NHIL in the context of retrenchment of the welfare state.
Transformation of the Israeli Welfare State and the Israeli Health Care System
Researchers of Israeli society generally agree that since the 1980s, and more so since the late 1990s, Israeli governments have adopted socioeconomic policies that exhibit clear neoliberal characteristics, for example, shrinking the public sector and its roles, increasing the role and freedoms of the private sector and capital, downsizing social-security networks, reducing the government’s role in providing basic services such as education and health care, weakening the labor unions, privatization, reducing wages, and attempting to change laws that provide security for workers (Bareli, Gutwein, & Friling, 2005; Doron, 1999; Swirski, 1999, 2005). It is also generally agreed that although these processes trace their historical origins to the 1960s or even 1950s, they reflect a significant shift in the ideology and perceptions that guide policy makers in Israel.
These processes have been explained in several ways. A main explanation is the now-conventional view of students of Israeli society and politics: Since the late 1970s, Israeli society has experienced significant exposure to modern Western influences such as the free-market economy, individualistic values, and international companies as part of globalization. Generally speaking, too, Israeli society has become much more privately oriented than it was in previous decades (Arian, 1998; Avimelech & Tamir, 2002; Filk, 2000; Horowitz & Lissak, 1989; Mautner, 2000). To a large extent, many view these cultural changes as the core explanation for any social and political development in Israel. Policy changes in the direction of retrenchment of social services are often explained by the emergence of free-market ideologies and values that replaced the old welfare-state tradition (Doron, 1999). However, a recent study shows that the Israeli public justifies, to a large extent, state intervention in the supply of public services, supports public investment in services related to the welfare state, and recognizes the obligation to support those in need (Cohen, Mizrahi, & Yuval, in press).
Another current in research focuses on structural factors and social (class oriented) power struggles in explaining the retrenchment of the Israeli welfare state. Researchers usually trace the turning point in this direction to the economic stabilization plan that a National Unity Government implemented in 1985 on the basis of an agreement with representatives of the private sector (employers) and labor unions (Bareli et al., 2005; Ben-Bassat, 2001; Swirski, 2005). This agreement dramatically changed the power structure in Israeli society by reducing the power of trade unions, which under their federation (the Histadrut) also managed the country’s largest health fund, although increasing the state autonomy, that is, control of the Israeli economy by the Ministry of Finance (Grinberg, 1993). From that point onward, bureaucrats at the Ministry of Finance became dominant players in most policy-making processes and attempted to advance the neoliberal ethos that guided their professional education and has been regarded as part of their commitment to the professional community (Grinberg, 1996; Maman, 2002; Shalev, 2004). In so doing, the Ministry has made intensive use of a mechanism known as the Economic Arrangements Law (EAL). Ostensibly meant to reconcile various legislative provisions with the annual Budget Bill, the EAL is actually used to make significant changes in many policy areas, health care–system policy in particular (Horev & Babad, 2005). To pass the EAL, diverse legislative changes are rushed through, their social considerations are not given sufficient attention, and no public debate is held. In the main, the Knesset (parliament) Finance Committee discusses the bill as part of its state-budget debates and under time pressure to pass the budget before the deadline. Under these circumstances, legislators cannot give due consideration to the social implications of economic measures that affect the health care system. Given this context, the Israeli health care system has operated under significant political pressures and ongoing financial crisis.
The system is basically composed of four health care organizations operating under governmental regulation. Until the mid-1990s, it was dominated by Kupat Holim Clalit, the General Health Fund (hereinafter Clalit), established in 1911. Clalit was the major supplier of health care services, operating hospitals and clinics at all levels and in all parts of the country. Health insurance was paid for by means of union dues. Thus, adverse developments at the Histadrut drove the national health care system into a major economic crisis by the 1980s (Chernichovsky & Chinitz, 1995). After a very complex political process, the Knesset voted on June 15, 1994, to enact the NHIL. The insurance program instituted by the law included a basic package of care for every person holding resident status, thereby bringing most of the system’s finances under public auspices. Although the financing of the system was actually nationalized and done through governmental channels, the provision of health care services remained in the hands of the four health care organizations, which were financed on the basis of a capitation formula. These changes weakened Clalit’s dominance and triggered the privatization of services that were excluded from the basic package.
However, after more than 15 years of implementation, as research shows, only part of the social goals of the NHIL have been achieved, largely due to significant budget cuts and retrenchment of the welfare state. Such processes widened intersectoral disparities in the quality and quantity of health care services, meaning that the equality of services set forth in the NHIL has not been achieved. Chernichovsky, Elkana, Anson, and Shemesh (2005) demonstrate that there is a correlation between the relative level of the population’s health and sociodemographic characteristics. The impact is clearly expressed in the declining quality of services in peripheral geographic areas and for the weaker sectors of society (Gross & Barmeli-Grinberg, 2001; Heler, 2002; Nirel & Rosen, 2004; Swirski, 1999). Shoval and Anson (2000) also show that the new law did not significantly change the situation of the weaker sectors. Recent empirical data show that trust in Israeli health care organizations is modest, although Israeli citizens are relatively satisfied with the health services they receive (Mizrahi, Vigoda-Gadot, & Cohen, 2009).
These processes may be explained in the context of welfare-state retrenchment as described above. In the next section, we explain in detail the changes in the NHIL in this context.
Privatization Through Centralization in the Israeli Health Care System as Expressed in Post-NHIL Legislation
This section of our article offers a systematic analysis of the abundance of post-NHIL legislative initiatives and reveals the rationale of privatization through centralization that can partially explain health care policy in Israel. It also points to additional strategies that have been developed in the context of the new institutionalism to advance privatization processes.
Our analysis is based on open interviews with politicians, bureaucrats, decision makers, and academic scholars as well as analysis of primary and secondary textual sources, foremost detailed documentation of all legislative amendments to the NHIL from the time the Knesset passed the bill into law (June 15, 1994) to August 1, 2008. “Legislative amendments” are defined as all the additions, replacements, and corrections to the NHIL that were formally gazetted in the Israeli law book (Sefer Huqim).
Overall, there have been 403 legislative acts that may be considered amendments to the NHIL. Most of them (375) amended various sections of the law—368 in the law proper and 7 in the addenda. Twenty-eight additional adjustments were gazetted in the list of legislative acts (Reshumot) in matters related to the law. Among the 403 adjustments, 276 were indirect amendments, passed in the aforementioned shortcut legislative procedure (the EAL) or under economic-recovery laws. Figure 1 shows the distribution of amendments over the years and demonstrates that most of the amendments occurred between 1997 and 1999.
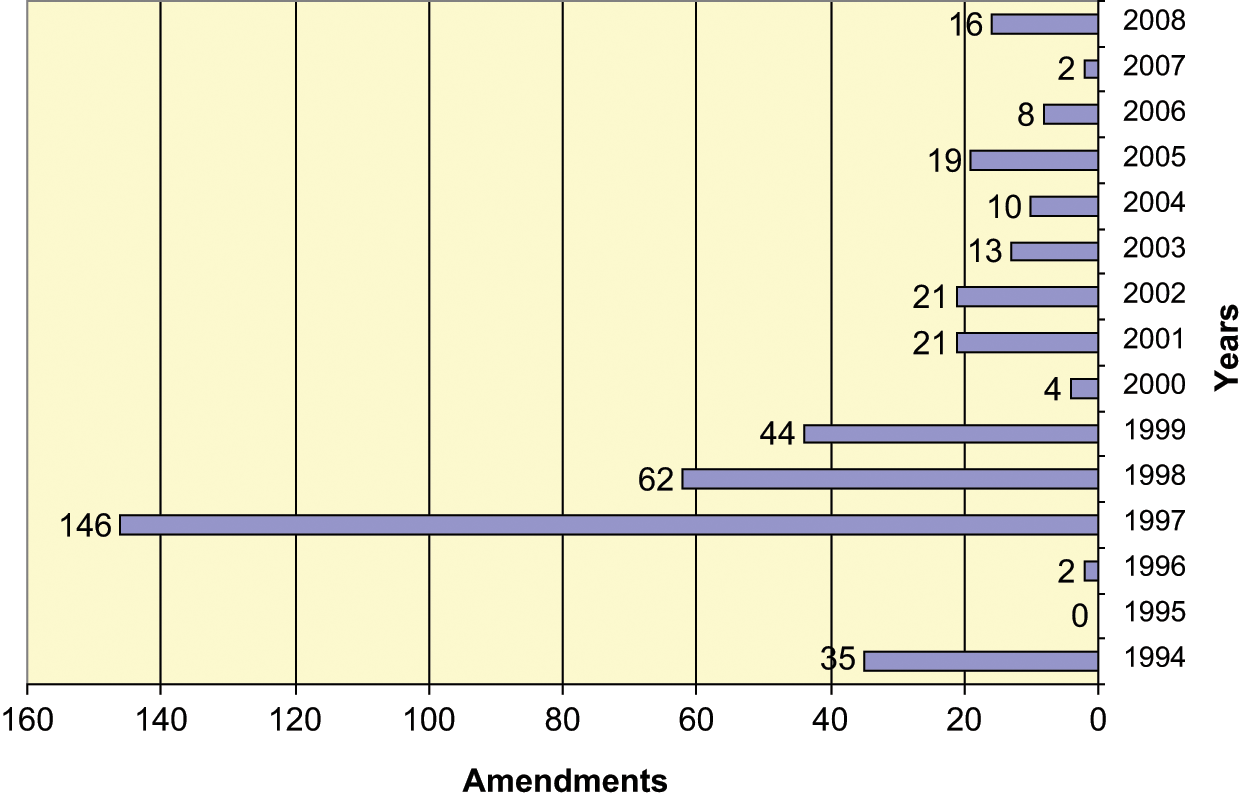
Amendments to the NHIL—by years
The health funds were main targets of the legislative initiatives. About 55% of the amendments concern the funds’ management, how they enroll members, the extra services they may provide (in addition to the health basket), and the invoking of sanctions against them. Importantly, our survey did not include the augmentation of the “basket” with new services and technologies. These legislative acts aside, 28.5% of the amendments related to sources of funding (members’ payments, health tax, etc.) and the apportionment of receipts. As we can find in Figure 2, the remaining amendments were divided among the following topics: the health basket (7.2%), health basket costs (2.2%), information and definitions (4.5%), and “other” (3.2%).
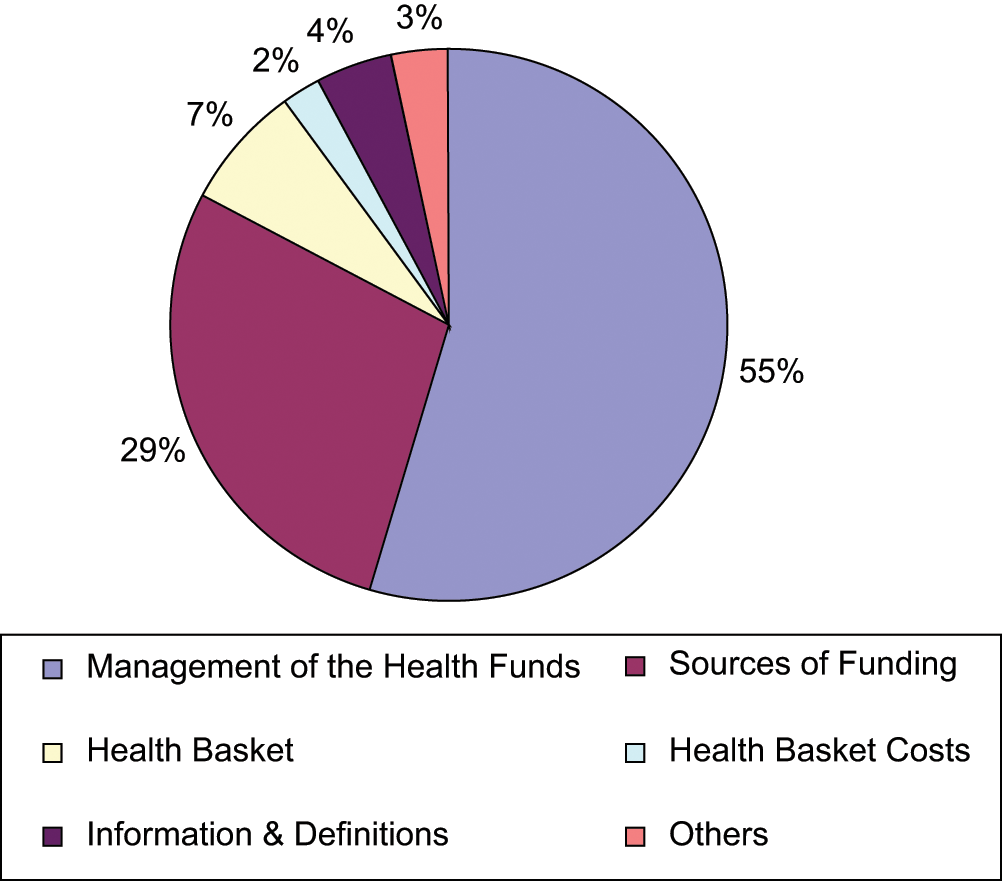
Amendments to the NHIL—by topics
The following analysis illuminates the centralization trends that the legislation reflects in regard to the financial sources of the health care system, the role of the ministries of Health and Finance in managing the system, and supervision of the health funds. It then sheds light on the corresponding privatization trends, expressed in reduced public financing of the health care system that elicits a risk privatization phenomenon, in which citizens have to solve their health problems in their own ways and at their own expense.
Centralization Trends in Legislative Amendments to the NHIL
The executive independence and operational autonomy of any health care organization depend primarily on an independent budget flow, that is, the existence of own financial resources. It follows that any legislation or policy measure that attempts to reduce independent financial resources expresses a centralization approach among legislators and policy makers. Indeed, major amendments to the NHIL relate to the financial resources of the health care system.
When the NHIL went into effect, the following sources of funding were established: health-insurance premiums (the health tax), parallel-tax receipts (an employers’ tax), an annual allocation from National Insurance to the MOH (for inpatient nursing care under the Long-Term Care Insurance Law), the share of the maternity-insurance premium under the National Insurance Law, the sums in the MOH budget for the provision of personal health care services, additional sums from the state budget to complement the funding of the health basket based on a given formula, and health funds’ revenues on account of services for which the law allows them to charge.
The most substantive change in respect to sources of funding was made under the 1997 EAL (NHIL, 5754-1994, Amendment 5). Before the NHIL went into effect, and afterwards until 1997, employers’ remittances to National Insurance under the Parallel Tax Law had been forwarded to the health funds as part of the funds’ current revenues, in addition to union dues (in the case of Clalit), premiums (charged by funds other than Clalit), and other sources. For the health funds, these payments were an earmarked source of funding with no strings attached. In 1997, the Parallel Tax Law was amended in ways that abolished the requirement of paying the tax (Parallel Tax Law 5733-1973, Amendment 16). A note to the proposed amendment explained that the Government, committed in any case to making up from its budget any gap between collection of health tax by National Insurance and the cost of the legislated package of insured services (the health basket), was responsible for ensuring that the health funds’ revenues be no smaller than the cost of the basket as determined in the law. The Ministry of Finance argued that the change reflected an intention to simplify National Insurance’s collection procedures and improve the flow of funding to the health funds. Thus, a greater share of sources would emanate from the state budget and the funds would not be dependent on seasonal and other effects of collecting from the public. However, in practice, this made the health funds more dependent on the MOH and eroded the sources available to them, in addition to obstacles and conditions that the funds had to surmount before the state agreed to forward those complementary resources from its budget.
In the terms of the retrenchment strategies discussed above (Pierson, 1995), this legislation may be understood as a restructuring strategy of centralizing financial resources to indirectly control the management and operation of health care organizations. However, although Pierson (1995) suggests that such a structural change is part of a well-planned strategy that aims to reduce public funding to welfare mechanisms in the long term, we have no indication that this was the case in the Israeli system. In fact, given the short-term calculations of most players in the Israeli scene (Mizrahi & Meydani, 2003), it is most likely that the Ministry of Finance bureaucrats simply wanted to control these resources to facilitate their reallocation in case of some future need. However, due to their short-term calculus, as we demonstrate below, they set in motion an incremental process of reducing the public share in funding for the health care system.
The legislative initiatives included additional aspects of centralization, such as maintaining the role of the MOH in providing many health care services and tightening supervision and control over health funds. These strategies and the relevant legislative acts are also explained below.
In addition to the basket of services that the health funds were required to provide, the NHIL set forth another list of medical services relating—mainly to prevention, mental health, nursing care, and rehabilitative and mobility equipment—to which members are entitled through the offices of the MOH. Interestingly, in regard to the basket of services for which the health funds are responsible, the law set forth explicitly the length of the adjustment (interim) period. The services under Health Ministry responsibility were treated differently. Here, the legislator settled for a general statement of intentions, explaining that the personal health care services that the state had been providing on the determining date, and those listed in the Third Addendum to the law, would be transferred to the health funds’ responsibility. However, no target date for the handover was specified. Instead, the legislator explained that until such a date would be set, the MOH would continue to provide the services at issue. Several attempts to regulate the matter by legislation failed. A series of amendments led to a state of affairs in which preventive services (e.g., early discovery of birth defects, inoculations, populations at risk, and family planning), psychiatry, and geriatric care remained within the purview of the MOH, as did health care services for schoolchildren (National Health Insurance, Amendment 20; NHIL, 5754-1994, Amendment 6; Recovery Program for the Israeli Economy 2003 Bill).
Centralization strategies were also manifested in legislation and amendments that tightened supervision and control over the health funds and other health organizations. Over the years since the NHIL went into effect, the state has become increasingly involved in managing the health funds’ affairs. Indeed, the largest mass of amendments during these years pertained to issues involving the funds’ ongoing management. Examples are adjustments relating to the funds’ institutions, their statutes, and the protection of members’ rights in the statutes. An entire section titled “Rules for the Management of Health Fund Affairs” was added to the NHIL in response to this need (NHIL, 5754-1994, Amendment 5). Adjustments relating to health funds’ statutes require authorization from the Minister of Health. The minister is empowered to reject any change in regulations that she or he considers detrimental to sound and independent management of the fund. For example, regulatory provisions concerning boards of directors, health-fund institutions, their composition, and their powers require the approval of the Minister of Health, whereas other changes need only be brought to the minister’s attention.
In the aftermath of this legislative change, the Minister of Health may forbid a health fund to accept new members until it corrects deficiencies in its statutes. A note attached to the bill before it was passed explained the purposes of the changes: to bring the funds’ statutes into line with the provisions of the law, to uphold the principle of the funds’ independence, to assure representation of members of the fund in the fund’s institutions, and to establish methods of appointment.
Other adjustments involving the management of health-funds affairs were enacted due to the legislator’s concern about the possibility that a health fund might run itself into financial danger. For this reason, since the original law went into effect, rules have been formulated to make sure that money from sources allocated to health funds by law would be used solely for the purposes of the law. Most adjustments of this kind pertain to contracting between health funds and outside corporations. For example, the law was amended to forbid a fund to acquire a controlling stake in another corporation and to contract with an outside party in a project unless the conditions and criteria set forth in various sections of the law are met (NHIL, 5754-1994, Amendment 5).
Legislative changes during the first years of national health insurance acted sweepingly to toughen the state’s enforcement powers against health funds relative to the powers granted to the state in the original law. One clause provided for the appointment of supervisory accountants for funds that overran their budgets or violated the rules set forth in the law.
The purpose of appointing a supervisory accountant for funds that breach their budgets was to monitor the funds’ income and outgo. The accountant was empowered to approve or strike down all new hiring and any change in the terms of employment of existing staff. The fund also needed the accountant’s approval for any financial or other commitment that it made. Apart from determining the accountant’s powers, the amendment authorized the ministers of Health and Finance to set conditions for his or her appointment. Once appointed, the accountant was required to present the ministers with regular reports on the financial situation of the fund.
Examples of other measures added to the law follow. The ministers of Health and Finance were allowed to limit the number of new members of any fund that failed to maintain a balanced budget (NHIL, 5754-1994, Amendment 5). The Minister of Health was authorized to advertise the findings of any committee that she or he might appoint to look into health-fund affairs. If a deficiency found by such a committee was not corrected within 14 days, the minister was allowed to fire an “official” (who in the previous wording of the law was called a “member of the management”), suspend the fund’s advertising and marketing activities, delay advance remittances, and freeze the fund’s development plans. As stated, all these powers were additional to those in the original law.
Privatization Trends in Amendments to the NHIL
Given these centralization trends, our systematic analysis of the amendments to the NHIL shows the existence of corresponding privatization trends expressed in the reduction of public finance for the health care system. The result is a phenomenon of risk privatization, in which residents have to solve their health problems in their own ways and at their own expense.
As explained above, the most substantive change in respect to sources of funding was made in 1997, when the Parallel Tax Law was amended in a way that rendered the tax inoperative (Parallel Tax Law 5733-1973, Amendment 16). This legislation placed control of funding sources in the government’s hands, and since then the Ministry of Finance has imposed gradually significant cuts in the health care system budget. This incremental policy, though not clearly indicated in any legislation, led to a significant downscaling of public funding for the health care system and a parallel increase in the share of private funding (Bin Nun & Kaidar, 2007b). Again, we claim that this incremental policy of reducing public health care funding and latent privatization was not necessarily planned for the long term. Rather, as derived from our interviews, it seems to be the result of ad hoc short-term decisions made by bureaucrats (Chernichovsky, 2007; Gafni, 2008; Galantee, 2008; Horev, 2008; Oron, 2008; Shani, 2008; Sharp, 2008; Shemer, 2008).
This behavior, although also characteristic of bureaucrats at the MOH, is especially typical of those at the Ministry of Finance, which has become the dominant player in Israeli health care policy making (Horev & Babad, 2005). It is these officials who have to find sources to cover deficits and pay for unplanned activities such as military operations and war.
Additional amendments to the NHIL that encouraged privatization trends pertain to the range of services provided by the public health care system, the taxation mechanism, and copayment mechanisms.
Since the NHIL was enacted, the sections that assure the goal of universal coverage have not been amended. However, another goal—establishing a standard package of medical services for all residents, most of which would be provided by the health funds—has been sterilized by a series of legislative changes. In 1998, the law was amended to allow health funds to add services and adjust members’ copayments after obtaining appropriate authorization (NHIL, 5754-1994, Amendment 7). Important services such as preventive dental care for schoolchildren and geriatric services were left outside the public health care orbit for most of the population, even though the legislator charged the Health Ministry with responsibility for providing them. In these respects, the package of services is not standard.
Legislative changes in several fields have aggravated the burden of copayments and made the payments more regressive, to the detriment of weak population groups. By the time the NHIL went into effect, patients were already being charged for medicines and some medical services such as visits to emergency centers, child-development treatments, and home visits. In early 1997, it was decided that copayments for the services listed in the law would be adjusted every April on the basis of a health care price index fashioned of components that were determined in the law (NHIL, 5754-1994, Amendment 5). In early 1998, the law was augmented with a section concerning changes in the health basket and payment for medical services. Each health fund was allowed to apply for an adjustment in the level of payments for medical services included in the law (NHIL, 5754-1994, Amendment 7). The authority to approve such applications was given to the Minister of Health per approval of the Knesset Finance Committee. Since then, approval has been given readily and the level of copayments has been rising significantly.
As for taxation mechanisms, the NHIL lists health-insurance premiums (health tax) as one of the funding sources. The premium is actually an earmarked tax that was supposed to replace the dues that members had paid their health funds until the law was enacted. The National Insurance Institute was placed in charge of collecting the new tax. A standard rate—4.8% of income—was established for most residents. An amendment passed shortly before the NHIL went into effect established new rules for the collection of the health tax. The amendment revised the original rules so that collection would be patterned not after the conventional principles and procedures in paying National Insurance contributions but after the charging of health-fund dues. This made it possible to charge health tax even on income that was exempt from National Insurance contributions, including benefits paid under law. In 2003, the health-tax base was broadened further by including two previously exempt groups: career soldiers (NHIL, 5754-1994, Amendment 21) and (albeit at a reduced rate) housewives (housewives for whom old-age pension contributions were made remained exempt; NHIL, 5754-1994, Amendment 22). It was also decided that fund members on early pension would pay the tax as ordinary workers would (NHIL, 5754-1994, Amendment 26). In a nutshell, since the NHIL went into effect, the collection of health tax has been expanded beyond the original provisions in terms of the number of persons liable.
In regard to the range of services provided by the public health care system, the NHIL instructed the ministers of Health and Finance (per approval of the Knesset Labor and Social Affairs Committee) to determine, on the implementation of the law, the cost of the health basket, that is, the budget that the state would allocate to the health care system to fund the services and pharmaceuticals included in the law. It was also determined that the cost of the basket would be adjusted each year by the rate of increase in the health care price index (computed in a manner established in the Fifth Addendum to the law) and that the ministers of Health and Finance would be entitled, per approval of the Knesset Labor and Social Affairs Committee, to change by administrative order the composition of the health care price index or to adjust the cost of the basket to the health funds in view of demographic changes. To this day, despite dissatisfaction among the health funds and a general consensus that the nonadjustment of the index has eroded the funds’ per-capita revenue, the Fifth Addendum has not been amended and no administrative order to recompose the health care price index has been issued. Furthermore, the section that awards the health funds a budget increase for demographic changes (population growth) has been implemented only in part, thereby speeding the erosion of the health funds’ per-capita revenue.
In 1997, the method of adjusting the cost of the basket was revised in a significant way (NHIL, 5754-1994, Amendment 5). The amendment, practically speaking, abolished the indexation mechanism for the sum allocated to the MOH for personal health care services in the ministry’s areas of responsibility. Since then, the budget for this matter has been subject, each year anew, to negotiations between the ministries of Health and Finance.
In fact, even though over the years the basket has been changed in other ways (e.g., new technologies have been added and the copayment rules have been modified), the law has not been adjusted concurrently in regard to how the cost of the package is calculated. Furthermore, there has been no long-term examination of the cost of the technologies that have been inserted into the basket and the consistency of these insertions with the predetermined budget for this purpose.
On August 1, 2008, an additional section in the law concerning changes in the basket and payment for medical services drove the system farther down the road to privatization. For the first time since 1998, the Knesset determined that health funds may not include “life-saving” or “life-prolonging” drugs in their supplemental services (i.e., those in addition to the basic basket; NHIL, 5754-1994, Amendment 38). Thus, these drugs may be accessed only via the private market.
In terms of the new institutional approach, as noted above, these dynamics have created a process of drift in which, despite external changes, the maintenance of existing institutional structures is neglected until they finally fail, forcing principals to find institutional alternatives. Indeed, Israelis have found alternative ways to handle the resulting shortage of services. By so doing, they initiated privatization processes that the government has institutionalized.
Thus, the legislative initiatives and amendments to the NHIL, as well as the policy measures that followed them, paint a clear picture of privatization trends in the Israeli health care system. Most of these initiatives and amendments include strategies of restructuring and neglect of financial maintenance that impose indirect and latent privatization (Pierson, 1995). In the discussion that follows, we suggest that the coexistence of centralization and privatization tendencies reflects the centrality of the Finance Ministry’s bureaucrats in policy-making processes in Israel and these bureaucrats’ two-pronged strategy in advancing their interests and policy paradigm: attempting to gain control over policy-making mechanisms, especially those related to financing and resource allocation, although managing the allocation of such resources through short-term decisions that correspond to the general policy paradigm of reducing government intervention in the economy.
Discussion
This article addresses a policy paradox that characterizes many health care systems and, in particular, the Israeli one. It is characterized by the existence of two parallel yet seemingly contradictory policy trends—reducing the public share in financing health care services while increasing governmental involvement in health care–system management. Although the former trend may be construed as a privatization strategy, the latter expresses greater centralization.
Our systematic examination of the legislative initiatives and amendments to the NHIL reveals the policy paradox that characterizes Israel’s health care system. During its 12 years of implementation, the public share in the financing of health care services has declined significantly (Bin Nun & Kaidar, 2007a; Horev, 2004) whereas the involvement of the government, via the ministries of Finance and Health, has not declined as envisaged in the NHIL but has increased (Horev, 2004). These parallel processes of privatization and centralization constitute the policy paradox in the Israeli health care system.
More specifically, the government first took control over the funding of the system by legislating earmarked taxes to be collected by the National Insurance Institute—a compulsory progressive health tax paid by each adult resident and a parallel tax paid by employers. We then showed that the government further tightened its control of the health care system by amending the NHIL in various ways that regulated the powers, management, and supervision of the health funds. All these measures allowed the Ministry of Finance to gradually reduce the public funding of health care services as part of a general and ongoing policy, not necessarily planned out for the long term, of retrenching the welfare state.
Indeed, our analysis demonstrates how the rationales developed within Pierson’s (1995) framework help to explain the policy paradox in a system where centralization and privatization coexist, as in the case of the Israeli health care system. The analysis also points to the central role of Ministry of Finance bureaucrats in managing the health care system and the two-pronged strategy with which they advance their interests and policy paradigm (Horev & Babad, 2005): attempting to seize the reins of policy-making mechanisms, especially those related to financing and resource allocation, while managing the allocation of such resources through short-term decisions that correspond to the general policy paradigm of reducing government intervention in the economy.
Some of the legislative changes and new regulations point to attempts by Ministry of Finance to make the health care system more efficient by means of the EAL mechanism. The intended purpose of this statute, enacted each year before the Knesset passes the state budget, is to amend existing legislation in matters that may otherwise rule out the attainment of state-budget goals. As the budget for the coming year must be passed on time, the Knesset uses a rush procedure to make these legislative changes. Admittedly, the EALs have served the Ministry of Finance well in its efforts to contain general-government expenditure, including spending on health care services. Expenditure for hospital services is a case in point. Each year, the EAL establishes rules for reckoning between health funds and hospitals on account of hospitals’ services to fund members. According to this method, an annual spending limit is set, beyond which the funds pay for hospital services at half the regular rate. Another attempt to cope with the steady increase in spending for hospital services was made in the 2003 Economic Recovery Program Law, which adjusted the Public Health Ordinance to widen the powers of the Director General of the MOH in fields such as hospital construction, the number of hospital beds, and the licensing of special medical aids. As for medicines, an attempt was made to limit expenditure by amending the Pharmacists Ordinance and allowing parallel imports of pharmaceuticals.
However, in many cases, the Ministry of Finance has used the EAL to make significant changes in health care–system policy that have no obvious connection with annual budget goals. These legislative changes are rushed through, their social considerations are not given sufficient attention, and no public debate is held. In the main, the Knesset Finance Committee discusses the EAL in the course of its state-budget debates and under deadline pressure to pass the budget. Under these circumstances, the legislators cannot give due consideration to the social implications of economic measures that affect the health care system. Furthermore, the various economic recovery plans included cuts in benefits that adversely affected the basic living conditions of weak population groups and the education system. Given this state of affairs, the public devotes most of its attention to basic problems of assuring adequate existence, employment, and education, leaving less concern for the effects of the economic measures on the health care system.
Yet, even though they proved as the dominant players in the Israeli health care policy arena, not all the attempts of the Ministry of Finance bureaucrats proved to be successful. Their repeated attempts, since 1998, to establish a fifth, private-oriented, sick fund as well as the attempts to impose a “flexible health care basket,” in which each sick fund would determine the services supplied in its basket, have failed time after time.
These strategies clearly show that although the Ministry of Finance bureaucrats may have a general policy paradigm of reducing the government intervention in the economy, most of their activities and initiatives in regard to the health care system are part of short-term moves rather than elements of a long-term plan to retrench the welfare state. As our analysis shows, there are several indications that the Ministry of Finance is primarily guided by short-term considerations.
Thus, processes of latent privatization of the Israeli health care system are advancing by means of incremental policy making in which the Ministry of Finance adopting an approach of “muddling through” in budget management and resource allocation (Lindblom, 1959; Wildavsky, 1984). However, the role of centralization processes in making this behavior possible increases the potential for inefficiency as market forces are not really allowed to take part in the health care system, although the government retreats mainly in the financial respect. As a result, residents are increasingly left to find their own solutions to the shortage of health care services. They seek short-term solutions that, in turn, are institutionalized by the government, thereby exacerbating the lack of long-term planning in the system. Further research will probe these aspects of the Israeli health care system.
Footnotes
Authors’ Note
This research is based on data collected by the authors following the research of Tuvia ![]() . Horev was kind enough to share his data with the authors (amendments until the year 2004) and also contributed to the article in helpful comments and suggestions. They gratefully thank him for his support. The analysis in this article and its implications are at the sole responsibility of the authors. Both authors contributed equally to this study.
. Horev was kind enough to share his data with the authors (amendments until the year 2004) and also contributed to the article in helpful comments and suggestions. They gratefully thank him for his support. The analysis in this article and its implications are at the sole responsibility of the authors. Both authors contributed equally to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Israel National Institute for Health Policy and Health Services Research (NIHP).