
Abstract
This study recruited 567 African American youth (mean age = 15.27 years; 65.1% girls) to examine the role of parent and peer contexts on drug use among African American adolescents. Data were collected on demographics, drug refusal efficacy, drug use, and various psychosocial factors including family and peer factors. When controlling for age and gender, parental monitoring and peer risky behavior completely mediated the relationship between parental attitudes toward drug use and drug refusal efficacy and partially mediated the relationship between parental attitudes toward drug use and current alcohol use. Only peer risky behavior mediated the relationships between parental attitudes toward drug use and current tobacco and marijuana use. Results also revealed several salient moderating relationships. Implications for prevention programs are provided and include strengthening current parenting skills and focusing efforts on fostering the mother-adolescent relationship.
Nationwide, adolescent substance use persists at disturbing rates despite prevention efforts. However, for most drugs the prevalence of substance use among African American youth is lower than that of youth in other racial and ethnic groups. For example, in 2008, cigarette smoking among youth aged 12 to 17 years was more widespread among White and Hispanic youth than African American youth (10.6.%, 7.9%, 5.0%, respectively; Substance Abuse and Mental Health Services Administration [SAMHSA], 2009). Similarly, African American youth reported lower rates of alcohol use (10.1%) than Whites (16.3%), Hispanics (14.8.3%), and persons reporting two or more races (14.8%); however, African American youths’ rate of alcohol use was higher than Asian (5.7%) peers. Even though these rates were lower for African American youth than their White counterparts, substance use and abuse has a disproportionately negative impact on the African American community. In addition, African American adolescents experience legal and social consequences of substance use and abuse, such as higher rates of incarceration and academic problems, which are more serious than those experienced in their peer ethnic groups (Emshoff, Avery, Raduka, & Anderson, 1996; Wallace & Muroff, 2002). Consequently, the problem of substance use in African American adolescents raises important issues regarding how parents and peers might buffer negative patterns to prevent the grave consequences that often accompany substance use.
The purpose of this article is to present findings from a survey of African American youth that inquired about their drug use and their relationships with parents and peers. In addition, we present a developmental model based on family interactional theory. This model illustrates the linkages among parent and peer factors and African American youth drug use as we conceptualized these connections to develop our hypotheses. After discussing our methodology, we conclude with a discussion that focuses on the roles of parents and peers in drug refusal efficacy and the implications for additional research and practice in this area.
Parent and Peer Factors
Family interactional theory: the developmental model (FITTDM; Brook, Brook, & Pahl, 2006) is the primary theory used in this study. FITTDM was selected because its underlying concepts stem from social cognitive theory and social control theory, which are two theories commonly used to understand adolescent drug use. Furthermore, FITTDM was selected for use in this study because it has been refined to focus specifically on adolescent drug use, and because it has empirical evidence supporting its usefulness with African American youth (e.g., Brook et al., 2006). According to FITTDM theory, drug use is influenced by interrelationships between adolescents’ personalities (e.g., ego integration), previous drug use, parental characteristics (e.g., parental warmth, drug use), and quality of relationships with family members, peers, and the environment (e.g., neighborhood characteristics). Brook et al. (2006) proposed a pathway to adolescent drug use in which the parent directly influences his/her child’s conventional attitudes and subsequent behaviors as it relates to drug use. According to Brook et al. (2006), the parent internalizes society’s values and the absence of parental drug use creates a warm parent-child relationship that is free of conflict and leads to the adolescent’s identification with his/her parent, which, in turn, leads to a high-quality relationship between parent and child. Subsequently, the child internalizes the conventional parts of the parent’s personality, attitudes, and behaviors that lead to a conventional personality during adolescence. Accordingly, the adolescent’s conventional personality is therefore expressed in attitudes and behaviors that limit deviant peer affiliations and supports the adolescent’s own attitudes toward conventional behaviors.
Although FITTDM illustrates a complex interrelationship of risk factors at the individual, family, and social ecology of youth, we have adapted the model to highlight the influence of three dimensions of parenting: (a) parent attitudes toward drugs, (b) parent attachment, and (c) parent monitoring of their children’s activities (see Figure 1). In addition, we have adapted the model to highlight the influence of peer relationships on drug use and drug refusal efficacy (see Figure 1). These dimensions of parenting were the focus of the current study because few studies have examined these constructs as they relate to drug use among African American youth. In addition, Wallace and Muroff (2002) suggested that parental influence might be a stronger determinant of adolescent drug use than peer influence for African American youth as compared with youth of other races/ethnicities. The purpose of this article is to examine the aforementioned parenting constructs in relation to peer constructs. Peer influence is a strong and consistent predictor of drug use (Bahr, Hoffman, & Yang, 2005). Investigating parent influence, because it seems to be especially important for African American youth, may help explain how parents buffer against negative peer influence and may be useful in developing and refining preventive interventions for African American youth. Focusing on other constructs, such as genetics and adolescent personality, was outside the scope of the current study. For these primary reasons, the FITTDM model was adapted.
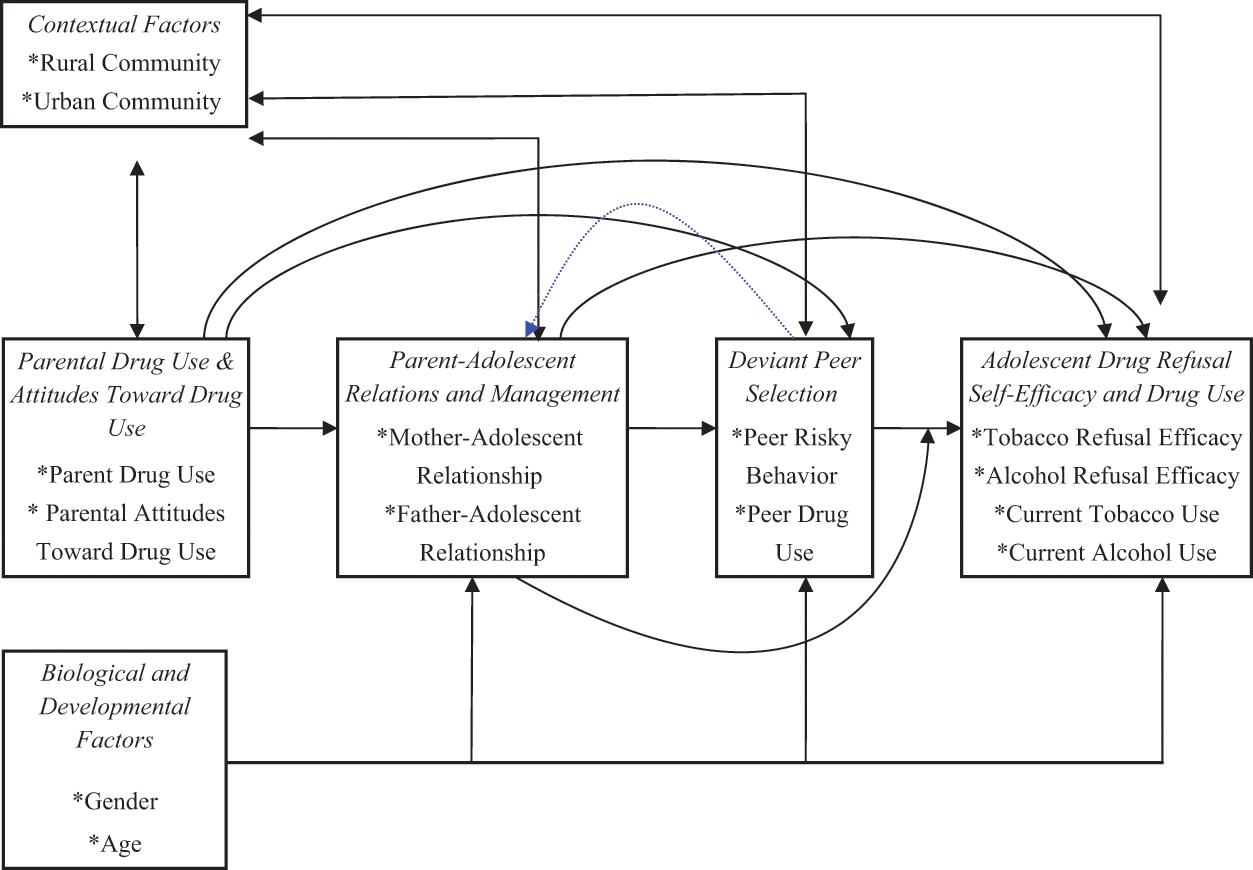
Adapted conceptual model of adolescent drug use
In general, the adapted conceptual model differs from the theory in several ways. First, since the present study focused on parents, peers, and adolescent drug use, we did not include genetic factors, parents’ marital status, adolescent personality, and adolescent drug abuse. Although marital status is a parent-related variable, we did not include it in the adapted model because studies have shown that it may not be predictive of drug use among African Americans (Belgrave, Townsend, Cherry, & Cunningham, 1997). Second, a few domains were renamed to clearly reflect the variables of interest in this study. FITTDM labels parental attitudes toward drug use as “parent personality.” In the adapted model, this construct is labeled “parental attitudes toward drug use” because this label provides a better description. FITTDM includes parent-adolescent relations and parental management in one domain, which is labeled as “parent-adolescent relations.” In the adapted model, this domain is labeled “parent-adolescent relations and management” to clarify the variables. In addition, the theory labels the peer domain “peers.” To be precise, this domain is labeled “deviant peer selection” in the adapted model. Third, the adapted model includes drug refusal efficacy as a proximal factor for drug use. Drug refusal efficacy was included in the adapted model because individuals must feel efficacious to put forth effort into refusing drugs (Corneille & Belgrave, 2007). Existing literature indicates that drug refusal efficacy may be a promising variable in predicting drug use (Clark, Nguyen, Belgrave, & Tademy, 2011). Fourth, FITTDM suggests that contextual factors bidirectionally affect adolescent personality and directly affect adolescent drug use but not other variables. Consistent with research, the adapted model suggests that contextual factors bidirectionally affect each domain. Fifth, FITTDM illustrates that genetic factors directly affect the parent drug use and personality, adolescent personality, and adolescent drug abuse domains and indirectly affect the parent-adolescent relations domain. In the adapted model, biological and developmental factors directly affect parent relations and management, deviant peer selection, and adolescent drug refusal efficacy and drug use. Additionally, parental attitudes toward drug use influence parent-adolescent relationships (e.g., warmth, attachment) and parenting management (e.g., monitoring, supervision). For example, parents who display favorable attitudes toward drug use often exhibit poor supervision of their children (Bahr, Maughan, Marcos, & Li, 1998). In addition, parental attitudes toward drug use and the parent-adolescent relationship interact such that adolescents with strong attachment and bonds with parents who hold favorable attitudes toward drugs may also engage in drug use. A combination of strong attachment to parents, high levels of parental monitoring, and a perception of parental disapproval of drug use may predict drug refusal.
Although the parent-adolescent relationship and parental monitoring skills are associated with adolescent drug use, the additional factor of deviant peer association also appears to affect this relationship. Peer influence is a typical component of development and includes peer conventional attitudes and behaviors (including attitudes toward drug use and drug use behaviors), peer acceptance and approval, and active and passive peer pressure. Parents who hold negative attitudes toward drugs may engage in more monitoring of their children’s activities and be more selective about with whom their child affiliates. In addition, the selection of risky peers is associated with weak parent attachment and poor parent monitoring (Brook et al., 2006). Adolescents who have weak parent attachment and are inadequately monitored may be more likely to engage in drug use than adolescents who have strong parent attachment and are adequately monitored. These relationships occur because these youth select peers who engage in similar types of risk behavior.
Gender, Age, and Drug Use
Age and gender directly and indirectly affect substance use; therefore, these two variables were examined as moderators of peer influence on drug use. Girls, especially African American girls, are less likely to use drugs than boys (SAMHSA, 2009). When drugs are used, girls (more so than boys) are likely to use drugs within the context of a relationship (i.e., to gain approval from friends or family members; Schinke, Di Noia, Schwinn, & Cole, 2006). Consequently, risky peers may exert greater influence on drug use among girls than boys. On the other hand, boys have more opportunities to affiliate with risky and deviant peers (i.e., because there is less monitoring of boys than girls), suggesting a greater opportunity and influence of risky peers on boys (Crosnoe, Erickson, & Dornbusch, 2002). Although research supports the influence of risky peers for both males and females, we speculated that risky peers would be a stronger influence on drug use and efficacy for adolescent females.
We were also interested in the moderating effect of age on the relationship between risky peers and drug use. Older adolescents are more likely to use drugs than younger adolescents; increase in drug use occurs across the three developmental age periods of participants in this study (early, mid, and late adolescence; SAMHSA, 2009). Therefore, risky peers may exert more influence at older ages than at younger ages. When adolescents are older, drugs are more accessible, there is more self-selection of friends and peers, and there is less monitoring. Therefore, we expected a greater influence of risky peers on substance use among older rather than younger adolescents.
Rationale for the Current Study
The present study builds on earlier studies and extends previous research in several salient ways. First, a more complete set of parental variables are examined than has been studied collectively in previous drug use research. In this study, the direct and indirect effects of two parental characteristics on adolescent drug refusal efficacy and use are examined. Second, previous studies have examined peer influences as a mediator in the parenting-adolescent drug use relationship. However, there has been less research on parenting practices as a moderator of the relationship between peer influence and drug refusal efficacy and use (e.g., Dishion, Capaldi, Spracklen, & Li, 1995; Kung & Farrell, 2000). This study examines whether parent-adolescent relations and parental monitoring moderate youth affiliation with risky peers and if this is linked to drug refusal efficacy and use. Third, most studies that focus on the effects of parenting styles and practices and adolescent drug use do so with a singular substance or do not examine the different substances used by adolescents. This study distinguishes which parent-adolescent relations and parental monitoring styles are risk or protective factors for different drugs, alcohol, tobacco, and marijuana use. Fourth, and possibly most salient, this study is innovative in examining a hypothesized buffering interaction among parents and peers that could have important implications for prevention programs. All hypotheses excluding the mediation hypothesis (Hypothesis 1) are exploratory.
Hypotheses
This study examined the role of parent and peer contexts on drug use among African American adolescents. The primary goal was to explore the parent-adolescent relationship, parental monitoring, and peer influence jointly on drug refusal skills and drug use. This study sought to test the following hypotheses:
Hypothesis 1: Consistent with FITTDM, (a) peer risky behavior will mediate the relationship between mother-adolescent relations and adolescent drug refusal efficacy and use, (b) peer risky behavior will mediate the relationship between parental monitoring and adolescent drug refusal efficacy and use, (c) mother-adolescent relations and monitoring will mediate the relationship between parental attitudes toward drug use and peer risky behavior, and (d) mother-adolescent relations and monitoring and peer risky behavior will mediate the relationship between parent attitudes toward drug use and adolescent drug refusal efficacy and use.
Hypothesis 2: Mother-adolescent relations and monitoring will moderate the relationship between peer risky behavior and adolescent drug refusal efficacy and use.
Hypothesis 3: Gender and age will moderate the relationship between peer risky behavior and drug refusal efficacy and use.
Method
Participants
The sample came from two waves of 5th-, 8th-, and 12th-grade students (N = 660) living in the Southeastern United States. This study uses data collected at Time 1 (baseline) during the spring of 2006, although data were collected at three assessment points. Eighty-six percent (n = 567) of the sample identified themselves as African American/Black, and only data from African American participants were used in the analyses. The mean age of the participants was 15.27 years (SD = 2.902), with a range of 9 to 21 years. Sixty-five percent of the sample was female.
Procedure
This study was approved by the university’s institutional review board. Data were collected in two public school systems in the Southeastern United States. Researchers recruited using a classroom-by-classroom method. During introductory meetings with students, data collection staff described the consent and assent process. Students were instructed to take consent forms home for their parents’ review and return forms to their school liaison. Completed and signed forms were later collected and secured by a school liaison until the data collection staff returned to collect study documents. An alternative consent form was given to students who were at least 18 years old, if they provided valid identification to verify their age. Participants were enrolled in the study upon consent from parents and after providing their assent.
Data were collected by trained researchers using a questionnaire. The questionnaire was administered in a designated area, often the cafeteria, but sometimes a media room, auditorium, multipurpose room, or private classroom. Researchers seated students far enough apart to ensure privacy. Researchers introduced themselves, provided a succinct overview of the study, and informed the students that their participation was voluntary and their responses were anonymous.
Measures
All measures had been used previously with the target population and were reliable and valid. The Parental Attitudes Toward Drug Use Measure assessed youth’s perception of their parents’ attitudes about their own drug use (Springer et al., 2004). The three-item measure uses a 4-point Likert-type scale with responses that range from not wrong at all to very wrong. An example of a scale item includes, “How wrong do your parents feel it would be for you to drink beer, wine, hard liquor (for example, vodka, whiskey or gin)?” Participants were instructed to respond regarding the behaviors of the parent that they identified earlier in the questionnaire as the person who they “see as a mother/father.” A Cronbach’s α of .73 was computed for this measure.
The Network of Relationship Inventory (NRI) assessed adolescents’ perceptions of their relationships with their mothers and fathers or guardians (Furman & Buhrmester, 1992). The youth’s perception of relationship with mother was used in this study. The NRI consists of 20 items. An example of an item is, “How often do you talk about personal things with your mother?” The items were rated on a 4-point Likert-type scale with responses that ranged from not at all to a lot, not a lot to all the time, or not at all happy to very happy. A Cronbach’s α of .76 was computed for the NRI.
Relationship subscale
Participants completed an abbreviated version of the Parental Monitoring Scale (PMS) originally developed by Silverberg and Small (1991) and further developed and validated by Li, Feigelman, and Stanton (2000). The abbreviated version had four rather than six items and had been previously used by the study investigators with a similar population. The abbreviated version was used to reduce the number of items in the questionnaire.
The PMS assesses parental monitoring by asking whether youth perceive a parent or guardian as usually aware of their activities after school. Participant responses to the PMS (Li, Stanton, & Feigelman, 2000) used a 3-point Likert-type scale with choices ranging from never to always. An example of an item from the PMS scale includes, “When you go out, how often do your parents know where you are going?” A Cronbach’s α of .70 was computed for this measure.
The eight-item Peer Problem Behavior Scale (John Snow Inc., 2000a, 2000b) was used to measure affiliation with risky peers. Participants responded to 12 items that assessed the type of peers with whom they affiliated. Examples of items included, “How many of your friends get suspended from school?” and “How many of your friends get good grades?” This measure also includes peer drug use (i.e., marijuana use, other drug use). The measure uses a 5-point Likert-type scale with responses choices of none, a few, some, most, and all. A Cronbach’s α of .77 was computed for this measure.
Past 30-day drug use
Scales from the Center for Substance Abuse Prevention Government Performance and Results Act (2005) were used as the primary measures for cigarette, alcohol, and marijuana use. Past 30-day use of substances were measured by a single item, “During the past 30 days, on how many days did you smoke cigarettes (or have at least one drink of alcohol, or use marijuana)?” Participants could check seven responses that ranged from 0 days to all 30 days.
The Specific Event Drug and Alcohol Refusal Efficacy Scale (SEDARE) was adapted from a measure developed by Conners, Bradley, Whiteside-Mansell, and Crone (2001). In this study, the SEDARE was adapted so that participants were asked about tobacco and alcohol use rather than alcohol and other drugs. This modification was made so that the drug refusal efficacy measure would relate to the study’s dependent variables for tobacco, alcohol, and marijuana use. Items addressing refusal efficacy for tobacco and alcohol use were compiled into a single scale. Participants responded to nine items that inquired about whether they would be tempted to smoke (cigarettes) or drink (alcohol) during certain potentially stressful or pressured events. Two sample items are “I would feel tempted to smoke if someone made fun of me for not doing it” and “If my boyfriend/girlfriend wanted me to drink, I would feel tempted.” The scale uses a 7-point Likert-type scale that ranges from 1 (not true) to 7 (very true). A Cronbach’s α of .87 was computed for this measure.
Results
Preliminary Analyses
Exploratory data analytic procedures were performed to ensure that the data met the appropriate assumptions for conducting multivariate analyses. To test hypotheses, main order, mediating, and interaction effects were examined. All variables were mean centered to reduce nonessential multicollinearity and improve the interpretability of findings (e.g., Aiken & West, 1991; Garson, 2008).
Descriptive Statistics on Measures
Most participants in the study reported not using substances over the past 30 days. More than 90% of the participants reported that they did not smoke cigarettes or marijuana during the past 30 days, and 79.8% of the participants reported that they did not consume alcohol during the past 30 days. Responses for drug refusal efficacy had a possible range from 9 to 67, with higher scores indicating lower levels of drug refusal efficacy. The mean score was 14.51 (7.71), indicating that most participants felt efficacious about refusing drugs.
Mean scores on the NRI indicated that participants felt they had positive and close relationships with their mothers. Scores ranged from 9 to 36, with a mean score of 29.51 (5.10). In addition, most participants reported high levels of perceived parent disapproval toward drug use. The mean was 10.87 (1.75) on a scale ranging from 3 to 12. Similarly, participants reported high levels of perceived parental monitoring with responses ranging from 3 to 12, with a mean score of 9.49 (1.89). Participants reported moderate levels of peer risky behavior (M = 16.2, SD = 4.82).
Hypotheses Testing
Hierarchical multiple regression analyses were used to examine the predictive value of parent and peer factors on drug refusal efficacy and use. Age and gender were controlled in the regression equation. A dummy variable was created for gender, and gender and age were always entered in the first step of the regression equation.
The present study used Baron and Kenny’s (1986) approach to test mediation models, and the Aroian version of the Sobel test was used to test partial mediators (Aroian, 1944; Sobel, 1982). Age and gender were entered in Step 1 of each analysis below. Hypothesis 1 was tested in three phases. During Phase I (denoted as Hypothesis 1a), parent-adolescent relationship and management variables (mother-adolescent relationship in Phase 1a, parental monitoring in Phase 1b) were entered as independent variables (M1), deviant peer selection (peer risky behavior variable) was entered as the mediator variable (M2), and drug refusal efficacy and drug use variables were entered as dependent variables (Y). In the second phase of the analysis (II; denoted as Hypothesis 1b), parental attitudes toward drug use was entered as the independent variable (X), mother adolescent relationship and monitoring variables were entered as mediator variables (M1) in IIa and IIb, respectively, and peer risky behavior was entered as the dependent variable (M2). During Phase III (denoted as Hypothesis 1c), the complete mediation model was examined. Parent attitudes toward drug use was entered as the independent variable (X), mother adolescent relationship, monitoring and peer risky behavior variables were entered as mediators (M1, M2), and drug refusal efficacy and use were entered separately as dependent variables (Y). Phases I and II were conducted to provide support of the full mediation model tested in Phase III.
Phase I: Mediation Analyses
During Phase I, parent-adolescent relationship and management variables (mother-adolescent relationship, parental monitoring) were entered as independent variables (M1), deviant peer selection variable (peer risky behavior) was entered as the mediator variable (M2), and drug refusal efficacy and drug use variables were entered as dependent variables (Y). Mother-adolescent relationship was entered as the independent variable in Phase Ia and parental monitoring was entered as the independent variable in Phase Ib. Age and gender were entered in Step 1 of each analysis.
Phase Ia: Mother-adolescent relationship and past 30-day tobacco, alcohol, and marijuana use and drug refusal efficacy
In examining Phase Ia, we did not find mediating effects of peer risky behavior in the relationship between mother-adolescent relationship and tobacco, alcohol, and marijuana use. In addition to the drug use outcomes, peer risky behavior was also predicted to mediate the relationship between mother-adolescent relationship and drug refusal efficacy. The analysis met the first requirement of mediation, that is, the mother-adolescent relationship must be significantly associated with drug refusal efficacy (M1 → Y; β = −.150, t(559) = −3.497, p = .001). The effect size for this model was .009. For the second requirement, mother-adolescent relationship must significantly predict peer risky behavior. This requirement was met (β = −.216, t(559) = −5.682, p = .000). The effect size for this model was .215. The third requirement was that peer risky behavior must be significantly associated with drug refusal efficacy while controlling for mother-adolescent relationship (M2 → Y). When entered simultaneously, peer risky behavior remained significant (R2 = .079,
Phase Ib: Parental monitoring and past 30-day tobacco use
Peer risky behavior was predicted to mediate the relationship between parental monitoring and past 30-day tobacco use. The first requirement of mediation was that parental monitoring needed to significantly predict past 30-day tobacco use (M1 → Y). This requirement was met (β = −.151, t(559) = −3.442, p = .001). The effect size for this model was .062. For the second requirement, parental monitoring must significantly predict peer risky behavior. This requirement was met (β = −.305, t(559) = −7.789, p = .000). The effect size for this model was .253. The third requirement was that peer risky behavior must be significantly associated with past 30-day tobacco use while controlling for parental monitoring (M2 → Y). When entered simultaneously, peer risky behavior remained significant (R2 = .120,
Phase Ib: Parental monitoring and past 30-day alcohol use
Mediation was tested as described in the “Phase I: Mediation Analyses” section. Peer risky behavior was predicted to mediate the relationship between parental monitoring and past 30-day alcohol use. The first two steps to determine mediation were satisfied. Parental monitoring predicted 30-day alcohol use (β = −.233, t(559) = −5.430, p = .000) and peer risky behavior (β = −.305, t(559) = −7.789, p = .000). During Step 3, when peer risky behavior and parental monitoring were entered simultaneously, peer risky behavior remained significant (R2 = .164,
Phase Ib: Parental monitoring and past 30-day marijuana use
Mediation was tested as described in the “Phase I: Mediation Analyses” section. Peer risky behavior was predicted to mediate the relationship between parental monitoring and past 30-day marijuana use. The first two steps to determine mediation were satisfied. Parental monitoring predicted 30-day marijuana use (β = −.119, t(559) = −2.708, p = .007) and peer risky behavior (β = −.305, t(559) = −7.789, p = .000). During Step 3, when entered simultaneously, peer risky behavior remained significant (R2 = .105,
Phase Ib: Parental monitoring and drug refusal efficacy
Mediation was tested as described in the “Phase I: Mediation Analyses” section. Peer risky behavior was predicted to mediate the relationship between parental monitoring and drug refusal efficacy. The first two steps to determine mediation were satisfied. Parental monitoring predicted drug refusal efficacy (β = −.245, t(559) = −5.544, p = .000) and peer risky behavior (β = −.305, t(559) = −7.789, p = .000). During Step 3, when entered simultaneously, peer risky behavior remained significant (R2 = .098,
Phase II: Mediation Analyses
During Phase II, a variable for parental attitudes toward drug use was entered as the independent variable (X), variables for parent-adolescent relationship and management (mother adolescent relationship, parental monitoring) were entered as mediator variables (M1), and a variable for peer risky behavior was entered as the dependent variable (M2). In Phase IIa, mother-adolescent relationship was entered as the mediator variable. In Phase IIb, parental monitoring was entered as the mediator variable. Age and gender were entered into Step 1 of each analysis.
Phase IIa: Parental attitudes toward drug use and peer risky behavior
Mother-adolescent relationship was predicted to mediate the relationship between parental attitudes toward drug use and peer risky behavior. The first requirement of mediation was that parental attitudes toward drug use needed to significantly predict peer risky behavior (X → M2). This requirement was met (β = −.239, t(559) = −6.292, p = .000). The effect size for this model was .227. For the second requirement—parental attitudes toward drug use—must significantly predict mother-adolescent relationship. This requirement was met (β = .195, t(559) = 4.684, p = .000). The effect size for this model was .075. The third requirement was that mother-adolescent relationship must be significantly associated with peer risky behavior while controlling for parental attitudes toward drug use (M1 → M2). When entered simultaneously, mother adolescent relationship (R2 = .258,
Phase IIb: Parental attitudes toward drug use and peer risky behavior
Mediation was tested as described in the section above. Parental monitoring was predicted to mediate the relationship between parental attitudes toward drug use and peer risky behavior. The first two steps to establish mediation were satisfied. Parental attitudes toward drug use predicted peer risky behavior (β = −.239, t(559) = −6.292, p = .000) and parental monitoring (β = .230, t(559) = 5.893, p = .000). During Step 3, when entered simultaneously, parental monitoring (R2 = .286,
Phase III: Full Mediation Model
During Phase III, the complete mediation model was examined. Parental attitudes toward drug use was entered as the independent variable (X), parent-adolescent relations and management and deviant-peer selection variables were entered as mediators (M1, M2), and drug refusal efficacy and use were entered separately as dependent variables (Y).
Phase III: Past 30-day tobacco use
The first requirement of mediation—parental attitudes toward drug use—must be significantly associated with past 30-day tobacco use (X → Y), which was met (p = .000). The effect size for this model was .119. The second requirement was that parental attitudes toward drug use must significantly predict the mediators mother-adolescent relationship, parental monitoring, and peer risky behavior. Mother-adolescent relationship was not included in this model because it failed to predict past 30-day tobacco use during the lower level analysis. The second requirement was met. Parental attitudes toward drug use predicted parental monitoring (p = .000) and peer risky behavior (p = .000), effect sizes of .181 and .227, respectively. The third requirement was that the mediators (i.e., parental monitoring and peer risky behavior) must be significantly associated with past 30-day tobacco use while controlling for parental attitudes toward drug use (M1M2 → Y). When entered simultaneously, peer risky behavior remained significant (p < .01; p = .000), but parental monitoring did not (p = .542). The independent variable for parental attitudes toward drug use remained significant (p = .000). Results indicated that requirements for complete mediation were not met. Instead, partial mediation (M2 → Y) occurred (X Step 1 B = −.138 and SE = .020, X Step 3 B = −.109). Peer risky behavior partially mediated the relationship between parental attitudes toward drug use and past 30-day tobacco use. The effect size for the final model was .156. Table 1 summarizes these findings.
Summary of Hierarchical Regression Analysis for Mediation Analysis of Full Model

Note: CI = confidence interval.
p < .01.
Phase III: Past 30-day alcohol use
Mediation was tested as described in the “Phase III: Full Mediation Model” section and subsection “Phase III: Past 30-day tobacco use.” Parental monitoring and peer risky behavior was predicted to mediate the relationship between parental attitudes toward drug use and past 30-day alcohol use. The first two steps to establish mediation were satisfied. Parental attitudes toward drug use predicted peer risky behavior (β = −.239, t(559) = −6.292, p = .000), parental monitoring (β = .230, t(559) = 5.893, p = .000), and past 30-day alcohol use (β = −.230, t(559) = −5.620, p = .000). During Step 3, when entered simultaneously, peer risky behavior (p < .01; p = .000), parental monitoring (p = .006), and parental attitudes toward drug use (p = .001) remained significant. Results indicated that requirements for complete mediation were not met. Instead, partial mediation (M1M2 → Y) occurred (X Step 1 B = −.114 and SE = .020, X Step 3 B = −.071). Parental monitoring and peer risky behavior partially mediated the relationship between parental attitudes toward drug use and past 30-day alcohol use. The effect size for the final model was .174.
Phase III: Past 30-day marijuana use
Mediation was tested as described in the “Phase III: Full Mediation Model” section. Parental monitoring and peer risky behavior were predicted to mediate the relationship between parental attitudes toward drug use and past 30-day marijuana use. The first two steps to establish mediation were satisfied. Parental attitudes toward drug use predicted peer risky behavior (β = −.239, t(559) = −6.292, p = .000), parental monitoring (β = .230, t(559) = 5.893, p = .000), and past 30-day marijuana use (β = −.161, t(559) = −3.871, p = .000). During Step 3, when entered simultaneously, peer risky behavior remained significant (p < .01; p = .000), but parental monitoring did not (p = .475). The independent variable for parental attitudes toward drug use remained significant (p = .013). Results indicated that requirements for complete mediation were not met. Instead, partial mediation (M2 → Y) occurred (X Step 1 B = −.066 and SE = .017, X Step 3 B = −.044). Peer risky behavior partially mediated the relationship between parental attitudes toward drug use and past 30-day marijuana use. The effect size for the final model was .107.
Phase III: Drug refusal efficacy
Mediation was tested as described in the “Phase III: Full Mediation Model” section. Parental monitoring, mother-adolescent relationship, and peer risky behavior were predicted to mediate the relationship between parental attitudes toward drug use and past 30-day marijuana use. The first two steps to establish mediation were satisfied. Parental attitudes toward drug use predicted peer risky behavior (β = −.239, t(559) = −6.292, p = .000), parental monitoring (β = .230, t(559) = 5.893, p = .000), mother-adolescent relationship (β = .195, t(559) = 4.684, p = .000), and drug refusal efficacy (β = −.116, t(559) = −2.693, p = .007). During Step 3, when the mediators were entered simultaneously, peer risky behavior (p < .01; p = .000) and parental monitoring (p = .001) remained significant, but mother-adolescent relationship (p = .801) did not. The independent variable for parental attitudes toward drug use became nonsignificant (p = .676). Thus, the requirement for complete mediation was met (M1M2 → Y). Peer risky behavior and parental monitoring mediated the relationship between parental attitudes toward drug use and drug refusal efficacy. The effect size for the final model was .089.
Does parent-adolescent relations and management moderate the relationship between peer risky behavior and drug refusal efficacy and use?
Prior to analysis, interaction terms of the independent and moderator variables were created. In hierarchical regression, age and gender were entered first. Second, the main effects of the independent variables were entered. Third, the main effects of the moderator variables were entered. Variables were centered to reduce nonessential multicollinearity, and interaction terms were loaded fourth.
Mother-Adolescent Relationship
Mother-adolescent relationship did not moderate the relationship between peer risky behavior and any of the drug use variables or the drug refusal efficacy variable.
Parental Monitoring
Parental monitoring moderated the relationship between peer risky behavior and past 30-day tobacco use (R2 = .159,
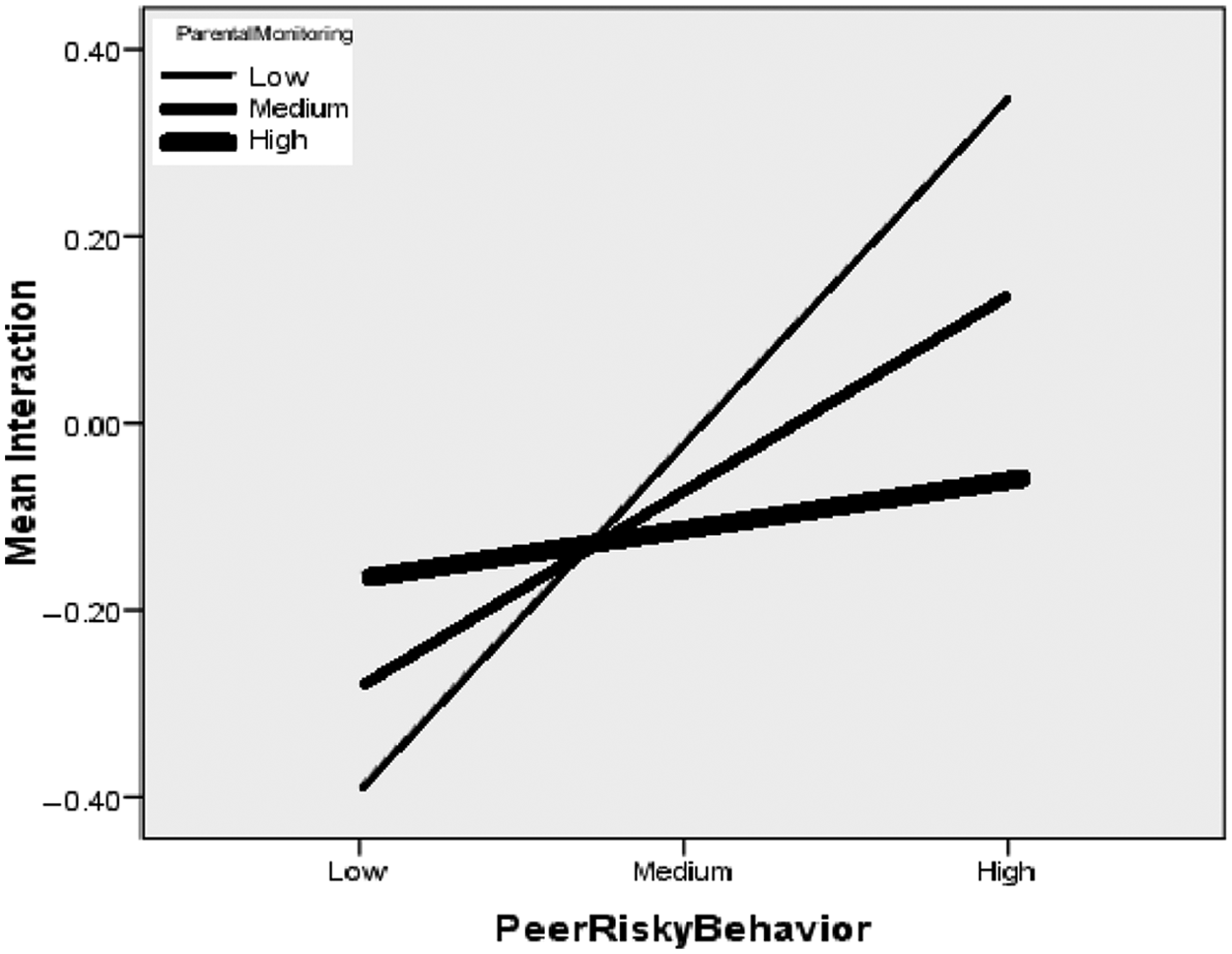
Peer risky behavior × Parental monitoring for past 30-day tobacco use
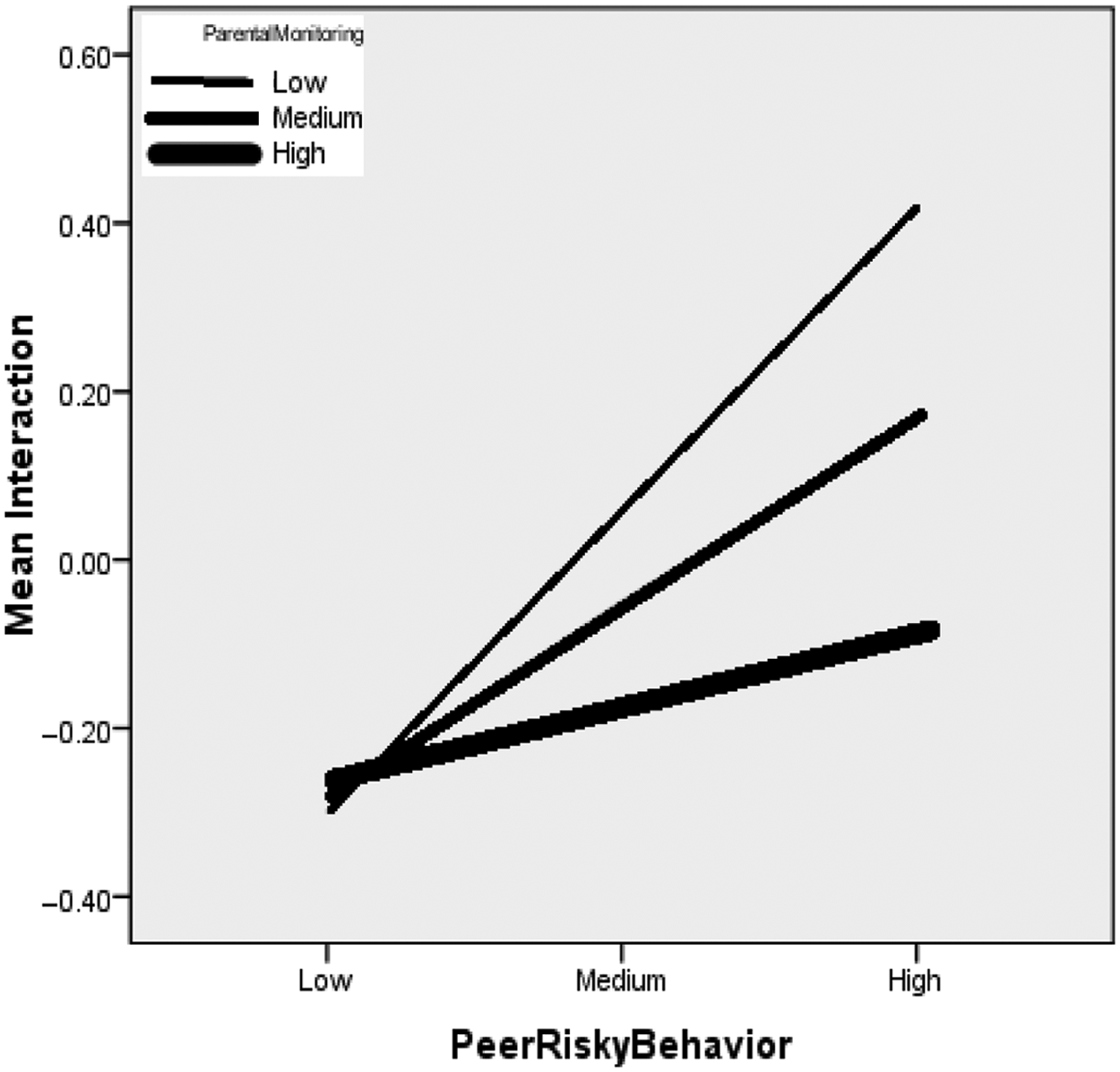
Peer risky behavior × Parental monitoring for past 30-day alcohol use
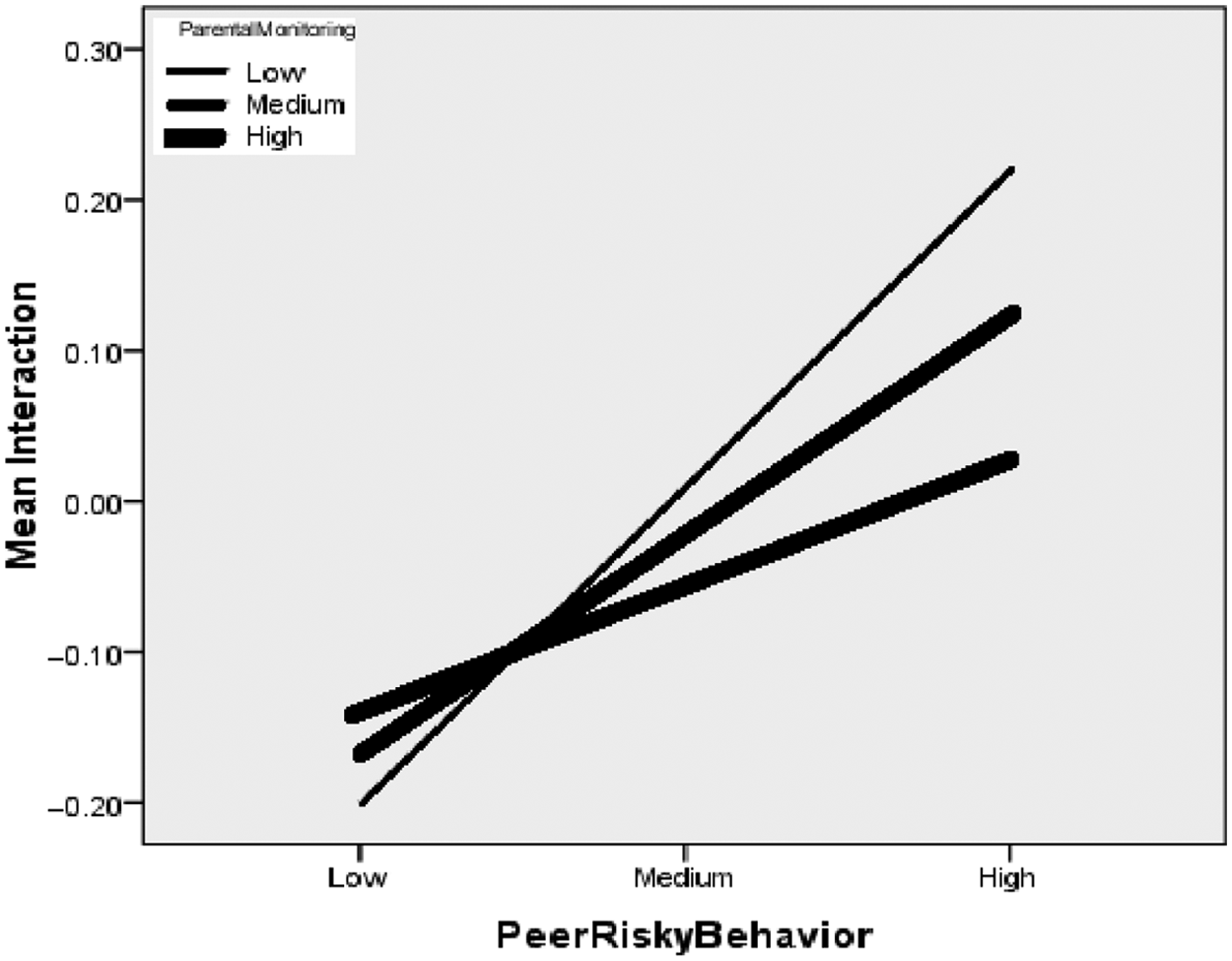
Peer risky behavior × Parental monitoring for past 30-day marijuana use
Does gender moderate the relationship between peer risky behavior and adolescent drug refusal efficacy and use?
Gender did not moderate the relationship between peer risky behavior and drug refusal efficacy (p = .159), past 30-day tobacco use (p = .863), or past 30-day alcohol use (p = .178). However, gender was found to moderate the relationship between peer risky behavior and marijuana use (R2 = .117,
Interaction of Peer Risky Behavior and Gender for Past 30-Day Marijuana Use
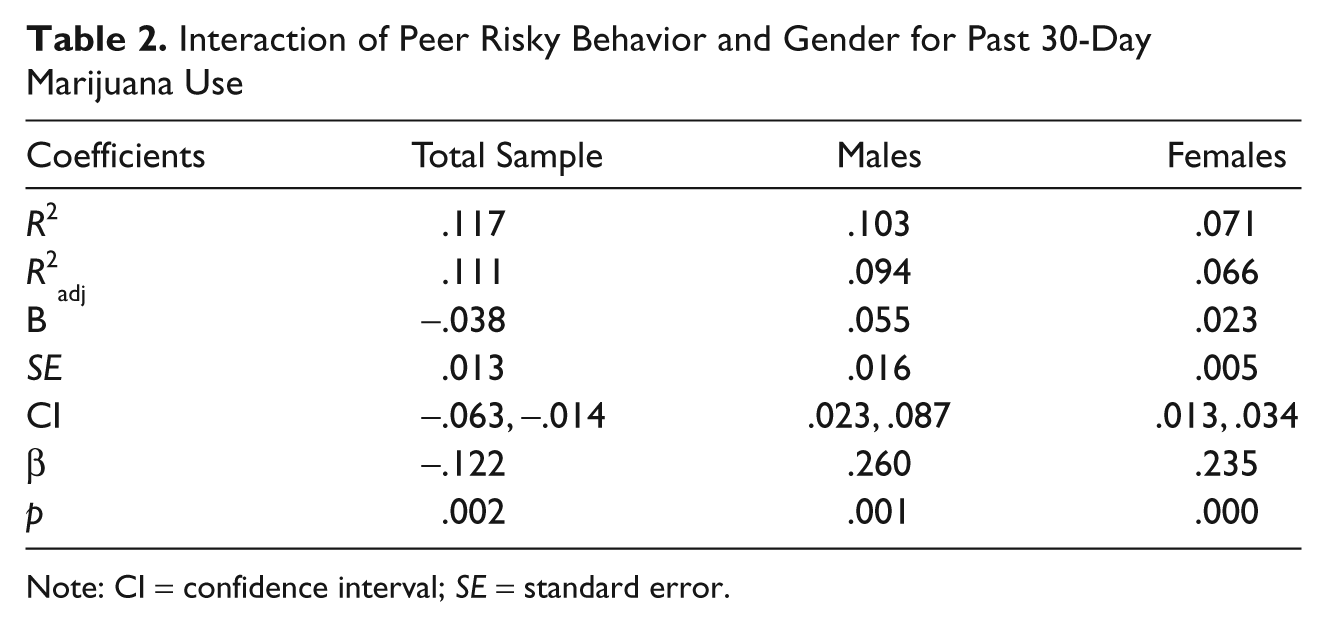
Note: CI = confidence interval; SE = standard error.
Does age moderate the relationship between peer risky behavior and adolescent drug refusal efficacy and use?
Age did not moderate the relationship between peer risky behavior and drug refusal efficacy (p = .220), past 30-day alcohol use (p = .309), or past 30-day marijuana use (p = .071). However, age did moderate the relationship between peer risky behavior and past 30-day tobacco use (R2 = .154,
Discussion
Researchers have documented the powerful role that parents play in adolescent development and behaviors such as drug use (Boyd, Aschraft, & Belgrave, 2006; Ennett, Bauman, Foshee, Pemberton, & Hicks, 2001). However, studies examining the mechanisms that explain the ways in which parental influences affect drug use and interact with peers to influence drug use behaviors among African American youth are less extensive. The findings from this study contribute to the current understanding of the role parents and peers play in drug refusal efficacy and drug use among African American adolescents. Most youth in the sample did not report drug use during the past 30 days. Brook et al. (2006) found that effects of parental attitudes toward drug use upon adolescent drug refusal efficacy were diminished by other parenting factors. Our findings are somewhat supportive of this finding. Parental monitoring and peer risky behavior partially mediated the relationship between parental attitudes toward drug use and current alcohol use and completely mediated the relationship between parental attitudes toward drug use and drug refusal efficacy. Only peer risky behavior mediated the relationships between parental attitudes toward drug use and current use of tobacco or marijuana. This finding suggests that parenting processes, both the mother-adolescent relationship and parental monitoring, did not affect tobacco and marijuana use in this sample. However, both peer risky behavior and parental monitoring mediated parental attitudes toward drug use and current alcohol use and, perhaps more important, drug refusal efficacy. Peer risky behavior was the only variable that consistently mediated all the drug use and drug refusal efficacy models. Nevertheless, the other important mediator, parental monitoring, played an important role in the use of alcohol and drug refusal. Consequently, the findings suggest that peer risky behavior and parental monitoring help explain the process by which parental attitudes toward drug use influence drug refusal efficacy and alcohol use. Parents who hold negative attitudes toward drugs may also engage in more monitoring of their children’s activities and be more selective about with whom their child affiliates.
This study also sought to determine the manner by which parenting variables interact with peer risky behavior to influence adolescent drug use. These hypotheses were exploratory. There was no support for the hypothesis that mother-adolescent relationship would reduce the influence of friends’ risky behavior upon drug refusal efficacy and use. However, parental monitoring reduced the influence of peer risky behavior on current tobacco, alcohol, and marijuana use (but not on drug refusal efficacy). This finding, consistent with the previous one, highlights the salient role of parental monitoring and is consistent with previous research (e.g., Dishion et al., 1995). Here, parental monitoring may be especially important when youth are in contexts in which their peers engage in deviant and problematic behaviors.
This study also examined the interaction of demographic characteristics (gender and age) and peer risky behavior on adolescent drug use. These hypotheses were exploratory. Despite expectations, gender did not moderate the relationship between peer risky behavior and drug refusal efficacy, current tobacco use, or current alcohol use. However, gender moderated the relationship between peer risky behavior and current marijuana use (but not other drugs). That is, this relationship was stronger for boys than girls and suggests that boys are more susceptible to using marijuana when their peers do so. In addition, findings indicated that age did not moderate the relationships between peer risky behavior and drug refusal efficacy, current alcohol use, or current marijuana use. However, age moderated the relationship between peer risky behavior and current tobacco use. That is, under conditions of high levels of peer risky behavior, younger participants were less likely than older participants to smoke cigarettes during the past 30 days. It is possible that the hypothesized interaction was only significant for tobacco use because of its accessibility. Because of tobacco’s legal status it may be more accessible to adolescents 18 years and older who can legally purchase tobacco products. In addition, youth younger than 18 years old may be able to access cigarettes from parents and older peers. In general, tobacco products are likely more available than alcohol, because the legal age to purchase alcohol is 21 years (most in the sample were younger than 21 years), and marijuana, which is an illegal drug regardless of age.
Limitations
This study yielded salient findings regarding the relationship between parents, peers, and drug refusal efficacy and use among African American adolescents. However, the findings of this study should be interpreted within the context of the study’s limitations. The limitations of the study include some shortcomings inherent in the research design, sampling methods, and measurement.
The present study used a cross-sectional design and causal inferences cannot be made with this design. Another limitation was the sample selection biases. This study required active parental consent. Some research has suggested that studies that require active parental consent may lead to participation by different types of students than those studies that require passive consent (e.g., Dent, Sussman, & Stacy, 1997) . Thus, these youth and the reported characteristics of their parents might be different from the general population of African American youth. For example, the study sample might be more prosocial and less likely to use drugs. This limitation is somewhat less of a concern because the participants were descriptively similar to participants in other studies (e.g., the study sample reported similar drug use prevalence rates and household structures as participants in other studies such as the Monitoring the Future national study).
A purposive sampling framework was used and, therefore, the findings cannot be generalized to adolescents outside the U.S. Midatlantic region.
The present study relied exclusively on youths’ self-report, which may contribute to response bias. In addition, many of the measures may have contained social desirability biases because participants were asked questions related to their own drug use behaviors and their parents’ attitudes toward parenting and parenting behaviors. The questionnaire was read aloud to fifth-grade students, which might have helped with students’ comprehension of the questions, but which could have led to additional bias.
Another limitation relates to the study’s measures. First, this study used a general measure of peer risky behavior that combined peer drug use, peer school suspension, and other peer problem behaviors. Measuring these peer problem behaviors in combination may have blurred the distinctions between these behaviors. It is possible that these peer risky variables contribute unique variance in adolescent drug use. Future studies may wish to consider looking at these constructs individually.
Another noteworthy limitation relates to model and theory building. Only a modest amount of variance associated with drug refusal efficacy and use was explained by the parent and peer variables as they were measured in this study. These findings suggest that (a) more sensitive measures might show greater effects (i.e., a measure of best friends’ drug use would be a more sensitive measure than perceived risky peer behavior); (b) other parent and peer variables should be included, such as parental drug use and father-adolescent relationship; and (c) it might be useful to explore alternative variables and theoretical frameworks, such as developmental factors (e.g., menarche, spermarche) and cultural factors (e.g., ethnic identity, religiosity).
Implications for Research and Knowledge Building
Several opportunities for research emerged from the present study. A first intriguing line of inquiry relates to the study’s outcome variables. The findings suggest that the paths to drug use are not the same across all drugs. Studies should continue to examine models across various drugs and refrain from combining multiple drugs into composite variables. As noted, the model poorly explained drug refusal efficacy. Notably, studies that have examined parents and peers and drug use have traditionally focused only on drug use. Hence, there is a paucity of studies that examine the relationships between parents, peers, and drug refusal efficacy. More studies are warranted to examine drug refusal efficacy. In this study, drug refusal efficacy was considered as a dependent variable. However, it is possible that drug refusal efficacy is a partial mediator or intervening variable in the relationships between psychosocial factors and drug use.
A second avenue of research relates to the lack of significant findings for the relationships between mother-adolescent relationship and the drug use variables. Findings regarding the association between mother-adolescent relationship and adolescent drug use are inconsistent. Some published studies have suggested that mother-adolescent relationship predicts adolescent drug use (e.g., Castro, Brook, Brook, & Rubenstone, 2006), some have suggested that there are modest effects (e.g., Bahr et al., 1998), and the present study yielded insignificant findings. Future studies should seek to replicate existing studies to determine under which conditions the relationship between mother-adolescent relationship and drug use is significant.
Implications for Prevention Programming/Practice
Given the consequences of drug use for African American adolescents, developing and modifying prevention and intervention programming is a noted national public health priority. Although the cross-sectional nature of these data limit this model as an exploratory model, and thus cannot indicate causality, the results of this study suggest several implications for prevention and intervention programming. First, prevention and intervention programming should seek to build current strengths, such as parenting skills and practices that appear to be effective in buffering against drug use among African American adolescents. Parenting behaviors—particularly parental attitudes toward drug use and parental monitoring—had direct effects on adolescents’ drug refusal efficacy and drug use. In addition, the results suggest that despite the strong influence of peers, parents retain substantial influence over the attitudes and behaviors of their adolescent children. Prevention programs should educate parents that their drug attitudes and behaviors are likely to affect their children’s attitudes and behaviors. Similarly, programs should teach parents that inconsistencies in their drug attitudes (e.g., negative attitudes) and behaviors (e.g., personal drug use) may contribute to their children’s drug use.
Furthermore, the findings of this study should dispel the myth that parenting practices are insignificant during adolescence. The results suggest that parental influence on adolescents’ behaviors remain extensive during adolescence. Notably, findings indicate that parental monitoring has indirect effects on drug refusal efficacy and drug use such that parental monitoring may reduce drug use by decreasing exposure to risky peers. It is possible that parental monitoring reduces initial affiliation with risky peer as well as reduces the influence of already established relationships with risky peers. Hence, the protective role of parents should be emphasized in programs. Programs that help parents to identify or create environments in which their children can be exposed to positive and prosocial peers are another implication from our findings.
Overall, our findings support the importance of prevention and intervention programs that strengthen parental attitudes and behaviors with regard to monitoring. These programs are likely to be effective because they make salient to parents the importance of monitoring for decreasing their child’s affiliation with risky peers while providing necessary structured supervision. At the same time, parental prevention and intervention programs should make salient to parents how their own attitudes and drug use behavior affect drug use by their children.
Footnotes
Acknowledgements
The authors extend appreciation to Deborah Butler (project director) and Dr. Aashir Nasim (convestigator) for their support of this research.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The authors wish to thank the Virginia Tobacco Settlement Foundation for funding of this project.