
Abstract
This study examined the associations between individual, institutional, and cultural race-related stress and somatic and cognitive anxiety. We adopted a risk and resilience framework to investigate the protective role of optimism and religious involvement in the race-related stress-anxiety link. A total of 171 African American young adults completed measures of race-related stress, optimism, religious involvement, and anxiety symptomatology. Institutional race-related stress was positively associated with cognitive and somatic anxiety. Optimism moderated the association between individual race-related stress and cognitive anxiety. Religious involvement enhanced the protective function of optimism in the association between individual and cultural race-related stress and cognitive anxiety. These results illustrate the utility of a multidimensional framework for understanding the impact of race-related stress on anxiety symptomatology. Moreover, the pattern of findings suggests that high religious involvement and high optimism may produce the most advantageous outcomes with respect to the association between race-related stress and anxiety in African American young adults.
Prior research indicates that racial discrimination is a normative experience for African American young adults (Banks, 2010; Banks & Kohn-Wood, 2007; Sellers, Caldwell, Schmeelk-Cone, & Zimmerman, 2003). Sadly, these experiences can have damaging effects on a wide range of mental health outcomes such as depression (Banks, Kohn-Wood, & Spencer, 2006; C. Brown, Abe-Kim, & Barrio, 2003; Sellers, Copeland-Linder, Martin, & Lewis, 2006), substance abuse (Guthrie, Young, Williams, Boyd, & Kintner, 2002; Martin, Tuch, & Roman, 2003), posttraumatic stress symptoms (Butts, 2002; Carter, Forsyth, Mazzula, & Williams, 2005), paranoia (Combs et al., 2006), generalized anxiety (Graham & Roemer, 2012; Rucker, West, & Roemer, 2010), and psychological distress (Sellers et al., 2003).
Despite the negative link between racial discrimination and favorable mental health outcomes, studies also report considerable heterogeneity in well-being outcomes (Bynum, Burton, & Best, 2007; Caldwell, Kohn-Wood, Schmeelk-Cone, Chavous, & Zimmerman, 2004; Neblett, Hammond, Seaton, & Townsend, 2010). Researchers have identified optimism and religious involvement as two factors that may protect the psychological well-being of African Americans against race-related stress and adversity (Danoff-Burg, Prelow, & Swenson, 2004; Utsey, Giesbrecht, Hook, & Stanard, 2008). In this study, we examined the protective nature of optimism and religious involvement in the association between individual, institutional, and cultural race-related stress and anxiety in a sample of African American young adults. Prior evidence suggests that race-related stress may trigger feelings associated with anxiety, such as paranoia and distrust (Lewis-Trotter & Jones, 2004). Moreover, epidemiological studies suggest that African Americans may have higher rates of anxiety disorder (Kessler, Mickelson, & Williams, 1999) and experience a more chronic course of anxiety symptomatology than European Americans (Breslau, Kendler, Su, Aguilar-Gaxiola, & Kessler, 2005).
Race-Related Stress and Anxiety Symptomatology
One particularly useful model for examining the linkage between racial discrimination and anxiety is Lazarus and Folkman’s (1984) model of stress and coping. This model posits that if the relationship between an individual and the environment is appraised by the person as taxing, it could endanger his or her well-being (Lazarus & Folkman, 1984). Thus, in this model of stress and coping, racial discrimination is characterized as a race-related stressor that exhausts the individual’s coping resources and ultimately influences the genesis of psychopathology, such as anxiety symptomatology (Harrell, 2000).
Building on Jones’s (1997) seminal tripartite model of racism, one might imagine that the impact of race-related stress varies as function of the level or type of racism or race-related stress in a given encounter. Jones characterized individual racism (commonly referred to as racial discrimination) as personal and degrading actions experienced by minorities (e.g., being called a racially derogatory name). Race-related stress at the individual level (e.g., being called a racial slur) might contribute to anxiety due to its jolting and unexpected nature. At the institutional level, Jones characterized racism by differential access to societal resources and services based on one’s race (e.g., unequal employment opportunities due to one’s racial group affiliation). One might imagine that the deprivation of social resources and services might foster a sense of lack of agency over stressors that threaten social status and lead to increased anxiety. Finally, Jones characterized culturalracism as cultural practices that laud one culture as superior to another (e.g., hearing or reading negative remarks about one’s ethnic group by a member of another ethnic group). Experiences of cultural race-related stress might conjure painful recollections of past discrimination and also engender feelings of powerlessness, impotence, and lack of control. In light of theory and evidence that suggests perceptions of uncontrollability are linked with anxiety symptoms (e.g., Lazarus & Folkman, 1984; Rucker et al., 2010), it seems plausible to believe that all three domains of race-related stress might be related to anxiety.
Several studies have examined the link between race-related stress and anxiety, though these studies are not without limitations. In a study by Kessler et al. (1999), day-to-day racial discrimination significantly predicted increased odds of being diagnosed with generalized anxiety disorder. Banks et al. (2006), Ong, Fuller-Rowell, and Burrow (2009), and more recently, Graham, West, and Roemer (2012) also found that perceived discrimination was associated with higher levels of anxiety symptomatology. In a study of discrimination, broadly defined, Soto, Dawson-Andoh, and BeLue (2011) found that experiences of non-race-based discrimination predicted generalized anxiety disorder for all racial groups, while experiences of race-based discrimination significantly predicted generalized anxiety disorder for only African Americans. While these studies suggest a strong positive association between racial discrimination and anxiety, they reflect two important limitations. First, the majority of studies have examined racial discrimination at the individual level to the exclusion of institutional and individual race-related stress. Such a focus fails to advance our understanding of how other forms of race-related stress may inform anxiety symptomatology and psychological well-being more broadly. Second, studies of anxiety symptoms have failed to differentiate between somatic and cognitive symptoms of anxiety. In light of evidence that African Americans are more likely to endorse somatic symptoms such as abdominal pain, chest pain, and headache than cognitive symptoms (e.g., fear and worry; Neal & Turner, 1991), more research is needed to examine if and how different types of race-related stress may relate to the somatic and cognitive symptoms of anxiety. Understanding differences in correlates of somatic versus cognitive anxiety will provide clinicians and researchers a stronger avenue for detecting anxiety-related problems and developing culturally informed interventions in African American clients.
Optimism as a Protective Factor
The risk and resilience framework (Garmezy, 1991, Zimmerman & Arunkumar, 1994) suggests that the presence of specific individual factors may increase or decrease African Americans’ vulnerability to racism-related stress. One such factor is optimism. Theory suggests that optimism may be an influential protective factor in the context of stress and adversity (Z. E. Taylor, Larsen-Rife, Conger, Widaman, & Cutrona, 2010), highlighting its potential value as a resilience factor in the context of race-related stress and psychological well-being. Expectancy-based theory posits that an individual’s belief in positive future outcomes will motivate an individual to adaptively cope and improve well-being in the face of stress and adversity (Carver & Schieier, 1998). Consistent with this suggestion, several studies find that optimism is associated with adaptive coping strategies that help individuals reduce, manage, or eliminate stress (Nes & Segerstrom, 2006). Moreover, several studies provide evidence that optimism has salubrious effects on psychological well-being for African Americans facing general life stress such as economic (Z. E. Taylor et al., 2010) and academic stress as well (Baldwin, Chambliss, & Towler, 2003).
While we are unaware of any studies to examine the protective role of optimism in the association between race-related stress and anxiety, a couple of studies demonstrate the protective nature of optimism in the relationship between race-related stress and psychological well-being. Utsey et al. (2008) found that optimism buffered the negative effect of race-related stress on psychological well-being. In another study, Danoff-Burg et al. (2004) suggested that the harmful effects of perceived racial discrimination experiences on psychological well-being were moderated by hope and optimism in late adolescent African Americans. Together, these studies suggest that optimism may protect African Americans from the deleterious effect of racial discrimination on various psychological well-being outcomes.
Religious Involvement and Optimism
A second, related protective factor is religious involvement. As far back as the early part of the 20th century, Freud (1928) indicated that the function of religion was to reprieve people of the burdens and difficulties of life. Since that time, scholars have identified religion as particularly important for helping African Americans to interpret racism-related stress and adversity (Cone, 1990). Many African Americans are religiously involved and engage in religious activities, such as attending church service and praying to God, to find strength and comfort in the context of stress (Graham & Roemer, 2012; R. J. Taylor, Chatters, & Levin, 2004). This body of research empirically supports the notion that religious involvement protects African Americans from the deleterious effect of race-related stress (Constantine, Donnelly, & Myers, 2002; Lewis-Coles & Constantine, 2006). In addition, African American liberation theology, in particular, metaphorically links Black oppression and racial adversity and discrimination to the oppression experienced by the Old Testament Israel and suggests that God will one day vindicate the oppressed just as God delivered biblical Israel from their oppressors. Previous theoretical (Hicks, 2004) and empirical work (e.g., Constantine & Sue, 2006; Peterson, 2000) suggests that religious involvement is protective when operating in tandem with optimism. S. Beck (1971) theorized that the image of an all-loving, forgiving, and merciful God was a source of “cosmic optimism” for believers. Sethi and Seligman (1993) reported a positive association between religious involvement and optimism while work by Mattis, Fontenot, Hatcher-Kay, Grayman, and Beale, (2004) noted a similar association between religiosity and optimism in African American adults. In light of the suggestion that religious involvement may go hand in hand or correlate with optimism, one interesting question is how religious involvement and optimism might operate together in the context of race-related stress and anxiety. Despite the apparent protective nature of optimism and religious involvement in the context of stress, we are unaware of any studies, to date, that have examined both factors together in the context of racial adversity and African American psychological well-being.
The Present Study
The purpose of this study is to address the aforementioned limitations of prior studies while increasing our understanding of the linkages among race-related stress, optimism, religious involvement, and anxiety. First, we are unaware of any study to examine the association between different domains of race-related stress and anxiety, while also differentiating between somatic and cognitive anxiety. The latter distinction may be an important one given the differential manifestation of anxiety symptoms for African Americans. Second, only a few studies have examined the protective role of optimism in the association between race-related stress and anxiety in African American young adults. Third, the current body of research on psychological well-being has not explored how religious involvement and optimism operate together within the context of race-related stress for African American young adults.
In light of these shortcomings, we sought to accomplish three aims. The first aim was to examine the association between specific types of race-related stress and two indices of anxiety symptomatology (i.e., somatic, cognitive). Consistent with the limited research on race-related stress and anxiety (Banks et al., 2006; Kessler et al., 1999), we hypothesized that different domains of race-related stress (i.e., individual, institutional, cultural) would be positively associated with cognitive and somatic symptoms of anxiety. The second aim of the study was to examine if optimism buffered the association between specific types of race-related stress on the different indices of anxiety symptomatology. Based on the accumulated studies that examine the protective role of optimism during stress (Baldwin et al., 2003; Z. E. Taylor et al., 2010), we hypothesized that the relation between race-related stress and anxiety would be more pronounced for individuals with lower levels of optimism. The third aim of the study was to examine if religious involvement would enhance the protective role of optimism within the context of individual, institutional, and cultural race-related stressors for African American young adults. In line with previous research (Mattis et al., 2004; Sethi & Seligman, 1993), we hypothesized that religious involvement would enhance the protective role of optimism in the association between race-related stress and anxiety symptomatology.
Method
Participants
Participants were 171 self-identified African American students enrolled at a midsized southeastern university. The age of the participants ranged from 18 to 24 years (M = 19.78 years, SD = 1.29) and 20.2% of participants identified as freshmen, 20.2% as sophomores, 26.6% as juniors, and 32.9% as seniors. One hundred thirty (76%) of the participants were females. Participants described their family’s socioeconomic status (SES) as either poor (5.3%), working class (24%), middle class (52%), upper middle class (18.1%), or wealthy (0.6%). The median family SES was middle class (Mdn = 3.00).
Measures
Demographic Information
Participants completed a demographic questionnaire assessing their gender, race/ethnicity, age, SES, parents’ educational attainment, and religious affiliation.
Multidimensional Measure of Racial Discrimination
The Index of Race-Related Stress (Utsey & Ponterotto, 1996) is a 46-item multidimensional measure of stress experienced by African Americans as a result of chronic exposure to racial discrimination. The measure consists of four subscales: individual, institutional, cultural, and collective race-related stress. The scale assesses lifetime prevalence with responses ranging from 0 (this has neverhappened to me)to 4 (event happened and I was extremely upset). The individual race-related stress subscale (α = .82) contains 11 items that assess the level of stress evoked by perceiving racism at a personal level (e.g., “Security people have followed you while shopping in some stores”). The institutional race-related stress subscale (α = 0.69) contains 11 items that assess the level of stress evoked by perceiving racism embedded in the policy of a given institution (e.g., “You think you did not receive a school award you deserved because you are black”). The cultural race-related stress subscale (α = .88) contains 16 items that assess the level of stress evoked by perceiving cultural practices of a dominant group being lauded as superior to those of African Americans (e.g., “You have heard bad remarks or comments about Black people spoken with little guilt by important White people”). The collective race-related stress subscale (α = .58) contains 8 items assessing the level of stress evoked by perceiving a collective organization of dominant group members (e.g., White supremacy groups) restricting the rights of Blacks (e.g., “You were physically attacked by a group of White/Non-Blacks”) Unfortunately, the collective racism subscale demonstrated low reliability in the study sample, and was not further analyzed. The four subscales have also demonstrated adequate to good reliability (αIndividual = .84, αInstitutional = .82, αCultural = .89, αCollective = .74) in a prior validation study (Utsey & Ponterotto, 1996).
Measure of Optimism
The Revised Life Orientation Test (LOT-R; Scheier, Carver, & Bridges, 1994) is a six-item measure that examines an individual’s level of dispositional optimism. The items making up the optimism index are scored on a 5-point Likert-type scale of 1 (strongly disagree) to 5 (strongly agree). Sample items include, “In uncertain times, I usually expect the best” and “I am always optimistic about my future.” To assess for construct validity, Scheier et al. (1994) conducted a principal component analysis and found a one-factor structure in the LOT-R scores. The results suggest that the LOT-R is a unidimensional measure of optimism. In regard to internal consistency, the LOT-R has demonstrated evidence for acceptable internal consistency in African American samples (Mattis, Fontenot, & Hatcher-Kay, 2003, α = .82; Utsey et al., 2008, α = .76). In the current sample, the LOT-R is a reliable measure of optimism (α = .82).
Measure of Religious Involvement
The Multidimensional Measure of Religious Involvement (MMRI; Levin, Taylor, & Chatters, 1995) is a 12-item measure of religious involvement for African Americans. The MMRI measures three indices of religious involvement: organizational, nonorganizational, and subjective religious involvement. A composite score of all three indices was examined in this study. Higher scores correspond to higher levels of religious involvement. A sample item of organizational religious involvement includes, “How often do you usually attend religious service?” A sample item of nonorganization religious involvement includes, “How often do you pray?” A sample item of subjective religious involvement includes, “How religious would you say you are?” The MMRI has proven to be a reliable and valid measure of religious involvement for African Americans (Chatters, Levin, & Taylor, 1992; Levin et al., 1995). In the present sample, the MMRI was a reliable measure of religious involvement (α = .87). Although internal consistency was not reported in the original validation study, a study by Jang and Johnson (2003) reported the internal consistency of the MMRI to be adequate (α = .74).
Measure of Anxiety
The Beck Anxiety Inventory (BAI; A. T. Beck & Steer, 1990) is a 21-item self-report inventory measuring the degree of anxiety in the respondent. Using a 4-point Likert-type scale of 1 (not at all) to 4 (severely—it bothered me a lot), the BAI measures the severity of anxiety symptoms (total score range: 0-63), with higher scores reflecting more severe anxiety symptoms. The BAI also measures two indices of anxiety symptomatology: somatic and cognitive symptoms (A. T. Beck & Steer, 1990). Chapman, Williams, Mast, and Woodruff-Borden (2008) examined the factor structure of the BAI in an African American sample. A confirmatory factor analysis found that a two-factor model (i.e., cognitive, somatic) provided the best fit for the African American sample. In regard to internal consistency, the somatic (α = .80) and cognitive (α = .70) subscales demonstrated evidence for acceptable internal consistency in the observed sample. Although internal consistency was not reported for cognitive and somatic anxiety in previous studies, the BAI scale has demonstrated excellent internal consistency in previous research (α = .92; A. T. Beck & Steer, 1990). The somatic subscale includes rating the degree of experiences with somatic symptoms pertaining to anxiety, such as “Face flushed” and “Hands trembling.” The cognitive subscale includes rating the degree of experiences with cognitive symptoms pertaining to anxiety, such as “Fear of loss of control” and “terrified.”
Procedure
This study was approved by the appropriate Institutional Review Board at the institution where the research was conducted. To recruit participants, contact information of self-identified African American undergraduate students was obtained from the university registrar’s office. Students on this list received information briefly describing the study and contact information for scheduling an appointment. The research team also posted fliers in buildings on campus.
At the onset of the study, each participant was greeted by a trained research assistant and told that the study examined individuals’ reactions to challenging situations. The participant was then asked to read and sign a consent form. After obtaining informed consent, the participant completed surveys consisting of measures of race-related stress, optimism, religious involvement, anxiety symptomatology, and other indices of psychological well-being in small group administrations. The questionnaires took approximately 45 to 60 minutes to complete. At the completion of the study, participants received 10 dollars for compensation.
Results
Preliminary Analyses
Preliminary analyses were conducted prior to the inferential multivariate regression analyses. Data were evaluated for the presence of outliers, skewness, and normality. Four outlier cases were removed due to extreme values in a number of measured variables. The skewness and kurtosis of each variable were in acceptable limits to proceed with the planned analyses. Next, we examined descriptive statistics and bivariate correlations for the measured variables in the study (Table 1).
Intercorrelations, Means, Standard Deviations.
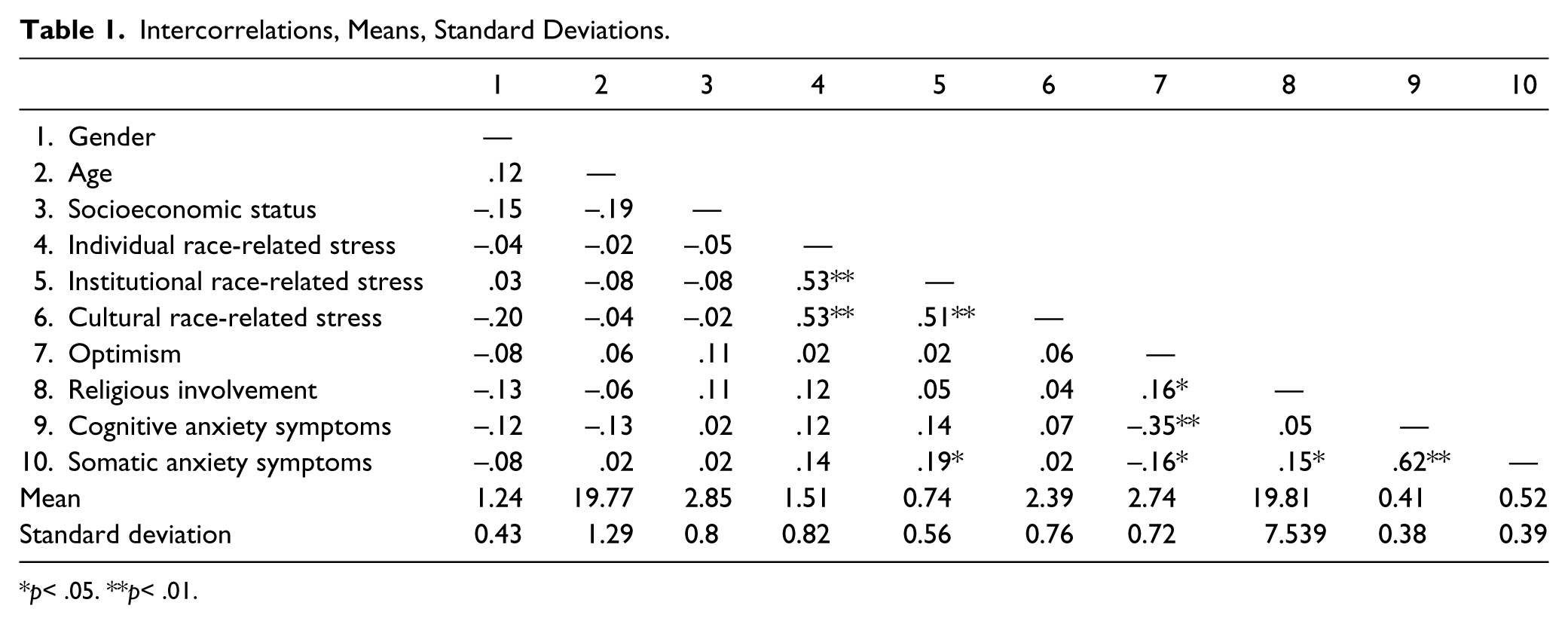
p< .05. **p< .01.
To investigate the study aims, six ordinary least squares regression analyses were conducted with cognitive or somatic anxiety as the dependent variable. To control for Type I error, we evaluated all six omnibus tests against a p value of .05/6 = .008. Predictors in each regression model included one type of race-related stress (i.e., individual, institutional, or cultural), optimism, religious involvement, two-way interactions between predictors, and three-way interaction between all the predictors. Of note, gender, SES, and age were excluded from the analyses as covariates since they were unrelated to cognitive or somatic symptoms of anxiety in the bivariate analyses. Continuous predictor variables were centered to reduce multicollinearity between the main effects and interactions.
Racial Discrimination Stress as a Risk Factor for Anxiety Symptomatology
The first aim of the study was to investigate the relationship between different domains of race-related stress (i.e., individual, institutional, and cultural) and different expressions of anxiety symptomatology (i.e., cognitive, somatic). Significant main effects of race-related stress were found for cognitive and somatic symptoms of anxiety. Individual race-related stress was not significantly associated with somatic and cognitive anxiety symptoms, while institutional race-related stress predicted more somatic anxiety (b = .14, p = .01) and cognitive anxiety symptoms (b = .12, p = .02) (overall model adjusted R2s = .58 and .70, respectively). Cultural race-related stress was not associated with somatic or cognitive anxiety symptomatology.
Optimism as a Protective Factor
The second aim of the study was to examine whether optimism buffered the positive association between race-related stress and anxiety symptomatology. A significant two-way interaction between individual race-related stress and optimism was found for cognitive anxiety (b = −.11, p = .04). Simple slope analyses found the slope representing the association between individual race-related stress and cognitive anxiety symptoms to be positive and significantly different from zero when participants endorsed low (b = .14, p = .01) and moderate levels of optimism (b = .06, p = .05). In contrast, the slope of the line representing the association between individual race-related stress and cognitive anxiety symptoms was not significantly different from zero when participants endorsed high levels of optimism (b = −.01, p = .83). Figure 1 plots the relationship between individual race-related stress and cognitive anxiety symptomatology at one standard deviation below the mean, the mean, and one standard deviation above the mean for optimism. Increases in individual race-related stress were linked with greater cognitive expressions of anxiety for participants endorsing low and moderate levels of optimism. However, there was no relationship between individual race-related stress and cognitive anxiety symptomatology for individuals endorsing high optimism. Optimism did not moderate other associations between race-related stress (i.e., institutional and cultural race-related stress) and anxiety symptomatology.
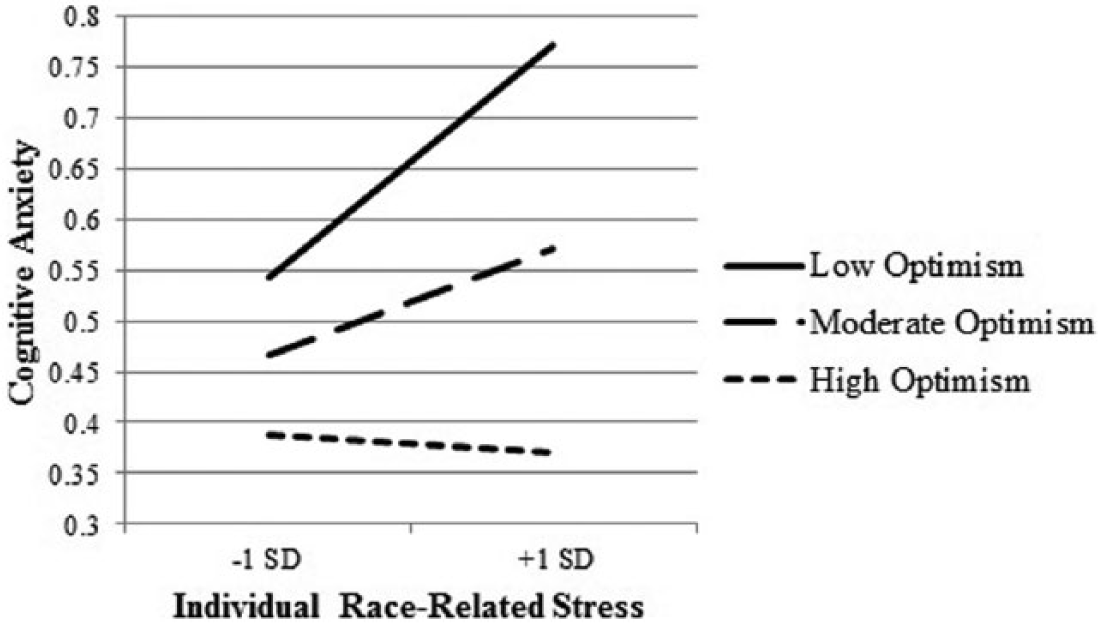
The relationship between individual race-related stress and cognitive anxiety symptomatology at one standard deviation below the mean, the mean, and one standard deviation above the mean for optimism.
Religious Involvement and Optimism as Protective Factors
The third aim of the study was to examine whether religious involvement would enhance the buffering effect of optimism in the association between race-related stress and anxiety symptomatology. The examination of three-way interactions among the various domains of race-related stress, optimism, and religious involvement revealed two significant three-way interactions. First, the Individual race-related stress × Optimism × Religious involvement interaction term significantly predicted cognitive expressions of anxiety symptoms (b = −.02, p = .01; overall model adjusted R2 = .70). Simple slope analyses found the slope representing the association between individual race-related stress and cognitive anxiety to be positive and significantly different from zero when participants reported high religious involvement and low optimism (b = .22, p = .01). Individuals with high religious involvement and low optimism also endorsed the highest levels of cognitive anxiety at high levels of individual race-related stress. The slope representing the association between individual race-related stress and cognitive anxiety was not significantly different from zero when participants reported low religious involvement and low optimism (b = .06, p = .26), low religious involvement and high optimism (b = .08, p = .23), and high religious involvement and high optimism (b = −.11, p = .13). Of note, individuals with high religious involvement and high optimism had the lowest level of cognitive anxiety at high levels of individual race-related stress. These findings are illustrated in Figure 2. Similar patterns were found for individual race-related stress and somatic anxiety (overall model adjusted R2 = .58) and for institutional race-related stress and cognitive anxiety, but these interactions failed to reach statistical significance (b = −.01, p = .08, b = −.02, p = .07, respectively). The three-way interaction was also nonsignificant in the model for institutional race-related stress and somatic anxiety; however, significant main effects were present for optimism and religious involvement in this model. Optimism predicted less somatic symptoms of somatic anxiety (b = −.11, p = .01), while religious involvement predicted more somatic symptoms of anxiety (b = .01, p = .03).

The relationship between individual race-related stress and cognitive anxiety symptomatology at one standard deviation below and one standard deviation above religious involvement and optimism.
The Cultural race-related stress × Optimism × Religious involvement interaction term significantly predicted cognitive expressions of anxiety symptoms (b = −.02, p = .03; overall model adjusted R2 = .69). Simple slope analyses found the slope representing the association between cultural race-related stress and cognitive anxiety to be positive and significantly different from zero when participants reported high religious involvement and low optimism (b = .15, p = .04). As with individual race-related stress and cognitive anxiety, individuals reporting high religious involvement and low optimism also endorsed the highest level of cognitive anxiety at high levels of cultural race-related stress. The slope representing the association between cultural race-related stress and anxiety was not significantly different from zero when participants reported low religious involvement and low optimism (b = −.01, p = .88), low religious involvement and high optimism (b = .11, p = .12), and high religious involvement and high optimism (b = −.05, p = .51). As with the pattern of findings for individual race-related stress and cognitive anxiety, individuals with high religious involvement and high optimism also had the lowest level of anxiety at high levels of cultural race-related stress. These findings are illustrated in Figure 3. The three-way interaction between cultural race-related stress, optimism, and religious involvement did not predict somatic anxiety symptoms (overall model adjusted R2 = .56); however, similar to the model for institutional race-related stress and somatic anxiety, significant main effects of optimism and religious involvement revealed that optimism predicted less somatic symptoms of anxiety (b = −.11, p = .01), and religious involvement predicted more somatic symptoms of anxiety (b = .01, p = .02).

The relationship between cultural race-related stress and cognitive anxiety symptomatology at one standard deviation below and one standard deviation above religious involvement and optimism.
Discussion
The first aim of the study was to examine the associations between race-related stress and anxiety symptomatology. In particular, the study explored the relationships between different types of race-related stress (i.e., individual, institutional, and cultural) and different types of anxiety (i.e., cognitive, somatic). The results indicated that the association between race-related stress and anxiety symptomatology depends on the type of race-related stress, individuals’ levels of optimism and religious involvement, and the type of anxiety symptomatology. Contrary to expectations, institutional race-related stress was the only form of race-related stress that was related to anxiety—both cognitive and somatic—symptoms, prior to consideration of the moderator variables (i.e., optimism and religious involvement).
Previous empirical studies report a positive association between individual race-related stress (e.g., overt racial slurs) and anxiety symptomatology (Banks et al., 2006; Kessler et al., 1999; Ong et al., 2009; Soto et al., 2011), and suggest that individual race-related stress is often jolting and unexpected in nature and possibly leads to traits of hypervigilance and overalertness (Ellison, Musick, & Henderson, 2008). However, we did not find support for this link in our study prior to considering levels of optimism and religious involvement. Two possible explanations for this discrepancy are (1) most studies reporting on the link between race-related stress and anxiety symptomatology do not consider third variables and (2) the majority of studies examining race-related stress examine the frequency of such experiences and not the extent to which individuals are bothered by such experiences, as did the measure in our study. A number of researchers have highlighted the importance of examining not only the frequency of race-related stress experiences but also the intensity of the experience when considering the impact and implications of race-related stress experiences (Landrine & Klonoff, 1996; West, Donovan, & Roemer, 2010; Williams & Mohammed, 2009). It may be the case that the frequency of individual race-related stress experiences is predictive while the intensity or amount of stress or bother resulting from individual race-related stress experiences is less predictive of anxiety symptomatology.
In understanding the pattern of findings for institutional race-related stress, Feagin (2006) argued that poorer well-being outcomes develop due to the lack of agency one has over managing stressors at an institutional level. Institutional race-related stress, in particular, leads to economic, legal, political, and social restrictions and disadvantages, which has negative implications on the quality of life for African Americans (Thompson & Neville, 1999). Lacking agency over institutional race-related stress is linked with increased anxiety as one is unable to control situations that negatively impact the quality of one’s life (Barlow, 2002; Broman, Mavaddat, & Hsu, 2000). This finding is particularly noteworthy when one considers the dearth of studies examining the psychological impact of institutional race-related stress relative to studies of individual race-related stress.
Finally, contrary to our hypothesis, cultural race-related stress was not associated with symptoms of anxiety (prior to consideration of the moderator variables). In making conceptual sense of this finding, several studies suggested that cultural race-related stress may be reframed as “positive and useful” and as opportunities for growth (A. P. Jackson & Sears, 1992; Myers, Montgomery, Fine, & Reese, 1996; Neblett et al., 2010). Thus, it may be that reading or overhearing negative remarks about one’s group motivates the pursuit of self-development and cultivates a sense of mastery over one’s life rather than anxiety.
The second aim of this study was to examine whether dispositional optimism moderated the association between different types of race-related stress and anxiety symptomatology. The results indicated that optimism moderated the association between individual race-related and cognitive anxiety symptoms. Consistent with the idea of optimism serving as a protective factor (Carver, Scheier, & Segerstrom, 2010; Peterson, 2000; Z. E. Taylor et al., 2010), the findings indicate that high levels of optimism nullify the negative association between individual race-related stress and cognitive anxiety symptoms. Carver et al.’s (2010) conceptualization of optimism posits that optimists expect positive outcomes in stressful situations, which in turn, evoke less cognitive anxiety symptoms, such as feeling nervous or feeling like the worst might happen.
Although optimism moderated the relationship between individual race-related stress and cognitive anxiety, most of the associations between race-related stress and anxiety were not moderated by optimism. A number of explanations may inform this pattern of findings. First, the present study examined an individual’s disposition toward optimism. However, Peterson (2000) noted that even dispositional optimists are pessimistic about certain situations. Thus, generally optimistic participants may still possess pessimistic beliefs about race-related stress. Second, there is a lack of research on optimism within the context of race-related stress. As racism has been alive and well in our society for hundreds of years, it may be especially difficult for victims of discrimination to cultivate optimism in the context of racism. Despite the majority of null findings, it is noteworthy to mention that optimism still functioned as a compensatory factor for many indices of psychological well-being (e.g., optimism predicted less somatic anxiety across all levels of institutional and cultural race-related stress). This suggests that optimism still plays some role in the psychological well-being of African American emerging adults across all levels of race-related stress.
The third objective was to examine whether religious involvement enhanced the protective role of optimism in the association between race-related stress and anxiety symptomatology. The study contained two instances when religious involvement enhanced optimism. First, religious involvement enhanced the protective role of optimism in the association between individual race-related stress and cognitive anxiety symptoms. Specifically, there was no association between individual race-related stress and anxiety symptomatology at high levels of religious involvement and optimism. At high levels of individual race-related stress, cognitive anxiety was lower at high levels of religious involvement and optimism than when optimism was evaluated as a sole moderator, and individuals with high optimism and religious involvement also exhibited the lowest levels of cognitive anxiety at high levels of individual race-related stress. Individuals who endorsed high religious involvement and low optimism, on the other hand, evidenced a positive association between individual race-related stress and cognitive anxiety. Although previous studies emphasize the protective role of religious involvement in the context of race-related stress (Constantine & Sue, 2006; Ellison et al., 2008), these results are consistent with a number of past studies to find a positive link between religious involvement and poor psychological well-being (e.g., J. S. Jackson, 1991; McAdoo, 1995) and further suggest that it is the combination of optimism and religious involvement that conveys protection. African American theology and religious involvement is shaped by racial oppression and may offer an important avenue to promote optimism in the context of individual race-related stress (Ward, 1995). In turn, the optimism cultivated from, and combined with religious involvement may be what makes religious involvement protective in the context of individual race-related stress (Mattis et al., 2003). Individuals who are religiously involved and optimistic may believe that external factors (e.g., God’s intervention) will remediate and prevent acts of interpersonal racism, while forgiving and showing sympathy to those who promote or engage in interpersonal racism (Mellor, 2004; Pargament, 1997). Cognitively reframing race-related stressors in this way could ameliorate the cognitive symptoms of anxiety elicited by individual race-related stress.
In the second instance, religious involvement enhanced the protective role of optimism in the association between cultural race-related stress and cognitive anxiety symptoms. Specifically, there was no association between cultural race-related stress and cognitive anxiety symptoms for individuals who endorsed high religious involvement and high optimism. Additionally, individuals reporting high levels of religious involvement and high optimism also endorsed the least amount of cognitive anxiety symptoms at high levels of cultural race-related stress. There was also a positive association between cultural race-related stress and cognitive anxiety for individuals who endorsed high religious involvement and low optimism. Consistent with the proposed framework, high levels of religious involvement, coupled together with high levels of optimism, is protective in the context of cultural race-related stress. Individuals exposed to negative messages about their culture may counter these messages by perceiving a close relationship with God (Ellison et al., 2008). Although speculative, individuals who sense having a close relationship with God are likely to feel a sense of elevated self-worth, self-esteem, and confidence in the context of cultural race-related stress (Ellison, 1993; Ellison et al., 2008). In turn, individuals may feel more optimistic and experience less fear and worry about future outcomes, which are symptoms of cognitive anxiety.
Limitations and Future Directions
The present study contributes to the growing body of research on race-related stress and anxiety symptomatology in a number of ways. However, several limitations will need to be addressed in future research. First, our study may not generalize to other samples of African American emerging adults. The participants in our current sample were undergraduate and graduate students from a prestigious academic institution in the southeastern region of the United States. Different sociodemographic contexts (e.g., age, SES) have been shown to influence religious involvement (R. J. Taylor et al., 2004), optimism (Peterson, 2000), and perceived race-related stress experiences (Prelow, Danoff-Burg, Swenson, & Pulgiano, 2004). Our sample was also predominantly female which may further threaten the external validity of the study. Second, the lack of significant findings for institutional race-related stress may be indirectly caused by the modest internal consistency (α = .69) of the institutional race-related stress subscale. Specifically, lower scale reliability may attenuate observed effect sizes, which in turn, decreases the likelihood of statistical significance in study findings (Furr & Bacharach, 2013). Third, the directionality of the observed findings remains unclear due to the cross-sectional data. For example, we are unable to determine if institutional race-related stress increased anxiety symptomatology, or if high-anxiety symptomatology increased institutional race-related stress. Similarly, it is difficult to ascertain the temporal ordering of optimism and religious involvement. Future studies should examine the key study constructs over time to develop a temporal understanding of the role of optimism and religious involvement in the context of race-related stress.
In addition to addressing the methodological limitations of the present study, future research could examine specific domains of religious involvement (e.g., prayer, church attendance) that are salutary for African American emerging adults in the context of race-related stress. Despite the developing body of research on religious coping for African Americans (Boyd-Franklin, 2010; D. R. Brown, Ndubuisi, & Gary, 1990; Levin & Taylor, 1998; Nooney & Woodrum, 2002), we are unaware of any studies that have examined specific religious expressions that buffer the deleterious impact of race-related stress for African American emerging adults. Second, as alluded to previously, the present study focused exclusively on dispositional optimism. However, research suggests that optimism may change based on situational and contextual factors (Luthans, 2002; Luthans & Youssef, 2007). Thus, it is conceptually plausible for optimism to operate dissimilarly in the context of race-related stress than other stressors (e.g., academic stress) for African American emerging adults. It would be wise for future studies to examine the role of state optimism in the context of race-related stress. Third, future research should strive to develop a more culturally sensitive understanding and assessment of anxiety for African Americans. Epidemiological studies suggest that African Americans endorse different types of anxiety disorders (Breslau et al., 2006) and symptomatology (Heurtin-Roberts, Snowden, & Miller, 1997; Neal & Turner, 1991) than White Americans. Although optimism and religious involvement were most protective in the context of cognitive symptoms in our study, these studies nonetheless suggest that behavioral and cognitive expressions of anxiety may be different for African Americans. In better understanding the relationship between discrimination and anxiety, researchers must employ an assessment of anxiety that adequately reflects anxiety symptoms relevant to African Americans.
Clinical Implications
Our study offers important insight into clinical practice with African American patients. First, this study highlights the influence of racial discrimination on the mental health of African Americans. Specifically, given the pervasiveness of race-related stress in the lives of African Americans (Sellers & Shelton, 2003; Swim, Hyers, Cohen, Fitzgerald, & Bylsma, 2003), counselors working with African American patients should not disregard the influence of race-related stressors in the genesis and maintenance of anxiety symptoms. In addition, as counselors facilitate the exploration of race-related stress for African American patients, counselors should apply a multidimensional conceptualization of racial discrimination. As illustrated by the study findings, institutional race-related stress experiences may be particularly worthy of future study as we seek to understand the impact of race-related stress on the expression and magnitude of anxiety symptomatology. Second, scholars have posited the notion that religious involvement and spirituality is an effective intervention tool in the mental health setting for African Americans (Boyd-Franklin, 2010; Hill & Pargament, 2008; Walsh, 2009). Counselors working with religiously involved African Americans should explore identity components of religious involvement (e.g., church attendance, prayer) that make religion psychologically salubrious, though our results also suggest that religious involvement in isolation may be insufficient for mitigating anxiety symptoms. Ultimately, the inclusion of race-related stress, optimism, and religious involvement in therapeutic conceptualizations of African American young adults may contribute to the development of culturally sensitive interventions in this population.
Conclusion
Individual, institutional, and cultural race-related stress emerged as correlates of cognitive anxiety symptoms, though the associations depended on the levels of optimism and religious involvement. Findings indicated that optimism may provide protection to African American young adults, particularly in the context of individual race-related stress and anxiety symptomatology, while optimism and religious involvement, in combination, may confer protection to African American emerging adults in the context of individual and cultural race-related stress. The results underscore the need for future research to examine underlying mechanisms that account for the salutary properties of optimism and religious involvement for African American young adults in the context of race-related stress. While the study findings highlight the negative implications of race-related stress for the well-being of African American young adults, study findings also suggest the potential benefits of cultivating optimism and incorporating or invoking religious involvement in mental health service delivery. This line of inquiry has the potential to inform counseling practice and research on how African Americans can successfully overcome and negotiate race-related stress and adversity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the Department of Psychology at the University of North Carolina at Chapel Hill (Account No. 68060).