
Abstract
Evidence from previous studies indicates that racial discrimination is significantly associated with depression and that African Americans with higher levels of socioeconomic status (SES) report greater exposure to racial discrimination compared to those with lower SES levels. Coping strategies could alter the relationship between racial discrimination and depression among African Americans. This study first examined whether greater levels of SES were associated with increased reports of racial discrimination and ratings of John Henryism, a measure of high-effort coping, among African Americans. Second, we examined whether high-effort coping moderated the relationship between racial discrimination and depression. Data were drawn from the National Survey of American Life Reinterview (n = 2,137). Analyses indicated that greater levels of education were positively associated with racial discrimination (p < .001) and increased levels of racial discrimination were positively related to depression (p < .001), controlling for all sociodemographic factors. Greater levels of John Henryism were associated with increased odds of depression but there was no evidence to suggest that the relationship between discrimination and depression was altered by the effects of John Henryism.
Major depression is a psychiatric disorder that is highly prevalent and debilitating in the United States and worldwide (Kessler & Üstün, 2004; Williams et al., 2007). Depression is estimated to be the fourth most common cause of disability worldwide (Üstün, Ayuso-Mateos, Chatterji, Mathers, & Murray, 2004) and is associated with poorer socioeconomic status (SES; Adler et al., 1994; Brown & Adler, 1998; Dohrenwend et al., 1992; Link, Lennon, & Dohrenwend, 1993). Many African Americans are socially and economically disadvantaged (Mezuk et al., 2011; Walsemann, Gee, & Geronimus, 2009; Walsemann, Geronimus, & Gee, 2008) and numerous studies indicate that African Americans are exposed to substantial levels of stress and adversity over the life course (Turner & Avison, 2003; Turner & Lloyd, 2004). Exposure to stress is an important factor in the development of mental disorders within the mental health literature (Farley, Steeh, Krysan, Jackson, & Reeves, 1994; Mirowsky & Ross, 2003; Schulz et al., 2006; Turner & Lloyd, 1999, 2004). Racial discrimination is a potent stressor, related to both increased levels of depressive symptoms (Brody et al., 2006; Gibbons, Gerrard, Cleveland, Wills, & Brody, 2004) as well as increased odds of depression (Hudson et al., 2012; Kessler, Mickelson, & Williams, 1999). A key component in the relationship between exposure to stress and development of mental illness is coping. High-effort coping, defined as “sustained cognitive and emotional engagement,” is described as a problem-focused coping strategy (James, Hartnett, & Kalsbeek, 1983). It is possible that high-effort coping strategies may be used by African Americans of higher SES when individuals appraise stressful situations that are sometimes related to racial discrimination, such as job loss or being passed over for promotion, as situations that can be altered by hard work (Geronimus & Thompson, 2004). However, high-effort coping may be a “mental health cost” paid by African Americans who maintain greater levels of sustained effort and energy expenditures in order to cope with stress (Cole & Omari, 2003).
It is likely that many African Americans who do possess greater levels of SES have had to overcome substantial odds to gain higher levels of education and gain entry into more prestigious, higher paying occupations. Scholars have argued that African Americans must engage in an arduous process of upward social mobility to improve their SES (Cole & Omari, 2003; Heflin & Patillo, 2002; Neckerman, Carter, & Lee, 1999). In fact, many African Americans, even those who appear to be solidly middle class, begin their lives in poverty (Heflin & Patillo, 2002; Patillo-McCoy, 1999). Hertz (2005), using data drawn from the Panel Survey of Income Dynamics (PSID), revealed that 42% of African Americans born into the bottom 10th of the income distribution remained in that same income bracket as adults. In 2006, a third of African Americans younger than 18 years were living in poverty and until 1996, the percentage of African Americans younger than 18 years living in poverty was consistently 40% or greater (Macartney, 2011). Despite efforts to overcome, often, humble beginnings, findings from several studies suggest that African Americans of higher SES contend with numerous stressors related to overt and covert racial discrimination manifested in many forms, including racial residential segregation, diminished returns for investments in social and cultural capital, and limited advancement in occupational settings due to “racialized” glass ceilings (Cole & Omari, 2003; Hochschild, 1995; Williams, 2003).
The adoption of high-effort coping strategies may be a plausible coping response for African Americans who encounter stressors such as racial discrimination in settings such as school and the workplace. Feagin and McKinney (2003) interviewed African American respondents who described distress and pain resulting from discriminatory workplace encounters with White coworkers. It would certainly seem that these kinds of discriminatory experiences would threaten mastery and self-esteem, two established risk factors for depression, of African Americans, thereby increasing African Americans’ vulnerability to depression (Broman, Mavaddat, & Hsu, 2000; U.S. Department of Health and Human Services Office of the Surgeon General, 2001).
Racial discrimination is independently associated with poorer mental health in African Americans (Clark, Anderson, Clark, & Williams, 1999; Kessler et al., 1999; Schulz et al., 2000; Schulz et al., 2006; Williams, Neighbors, & Jackson, 2008). Results from several studies indicate significant, positive associations between perceived racial discrimination and impaired psychological well-being and decreased self-esteem (Karlsen & Nazroo, 2002; Watkins, Hudson, Howard Caldwell, Siefert, & Jackson, 2010; Williams, Takeuchi, & Adair, 1992; Williams, Yu, Jackson, & Anderson, 1997). Findings from a variety of multidisciplinary studies indicate that African Americans with more socioeconomic resources report greater exposure to racial discrimination compared with those with lower levels of education and income (Cole & Omari, 2003; Dawson, 1994; Forman, 2003; Higginbotham & Weber, 1992; Hochschild, 1995). It is posited that African Americans of higher SES are more likely to work and live in integrated settings compared with poorer African Americans. Thus, higher SES is associated with increased exposure to racial discrimination among African Americans (Brayboy-Jackson & Stewart, 2003; Forman, 2003; Hudson et al., 2012; Williams, 2003).
To an increasing degree, researchers have investigated the intersection between SES, racial discrimination, and mental health (Forman, 2003; Hudson et al., 2012; Hudson, Puterman, Bibbins-Domingo, Matthews, & Adler, 2013; Williams, 1999). African Americans of higher SES experience a variety of race-related stressors, ranging from interpersonal racial discrimination and residential steering to lower levels of compensation and limited advancement in occupational settings (Cole & Omari, 2003; Forman, 2003; Hochschild, 1995; Williams, 2003). In a qualitative study conducted by sociologist Karyn Lacy (2007), her metropolitan Washington, D.C., middle-class African American respondents describe elaborate schemes used to construct “public identities” to signal their middle-class status to Whites in order to indicate that they belong in certain settings, such as shopping in upscale retail stores or seeking housing in predominantly White neighborhoods (Lacy, 2004). Although Lacy did not formally examine depression, she observed that her respondents seemed to have been harmed psychologically by the construction and practice of delicate racial and class interactions. Evidence from a study of middle-class African American men conducted by Sellers, Bonham, Neighbors, and Amell (2009) indicates a significant inverse association between racial discrimination and favorable self-rated mental health. In fact, they concluded that racial discrimination could be more hazardous to mental health than to physical health.
In addition to direct interpersonal experiences of racial discrimination, African Americans are compensated at lower levels than Whites, notwithstanding similar levels of education and work experience (Williams, 2003). While these kinds of discrepancies may be structural in nature, it is possible that African Americans attribute their successes and failures to their individual efforts (Smith, 2007). Findings from a qualitative study conducted by sociologist Sandra Smith (2007) indicate that despite structural barriers to gaining employment, such as racial discrimination from employers, lack of access to jobs, and fewer marketable skills due to poor educational preparation, African Americans in her study attribute a large portion of their difficulties in finding work to their own personal deficits and missteps. Considering these findings, is it possible that African Americans, especially those of higher SES, use high-effort coping strategies when faced with stressors such as difficulties with employment or achieving promotion? If African Americans of higher SES attribute their socioeconomic success to hard work, personal sacrifices, and ability to overcome obstacles, high-effort coping strategies may be used in this population. Yet it is unclear whether efforts to use individual agency to overcome obstacles that may be structural in nature, have negative effects on mental health.
The transactional model of stress and coping has been widely used to model the stress process (Pearlin, Lieberman, Menaghan, & Mullan, 1981; Pearlin & Schooler, 1978; Wenzel, Glanz, & Lerman, 2002). Wenzel et al. (2002) state that stressful experiences are “person-environment transactions,” in which the impact of an external stressor is mediated by a person’s appraisal of the stressor and the psychological, social, and cultural resources at their disposal. During the appraisal process, individuals evaluate their perceived control over the threat as well as their perceived control over emotional reactions. A key component of the stress paradigm is coping (Pearlin et al., 1981; Pearlin & Schooler, 1978; Wenzel et al., 2002). Disengaging coping strategies such as distancing, cognitive avoidance, and denial shift attention away from stressors. These strategies are considered maladaptive because they can lead to disruptive thoughts and prolong feelings of distress over time (Carver et al., 1993; Carver, Lawrence, & Scheier, 1999; Schwartz, Lerman, Miller, Daly, & Masny, 1995). “Emotion-focused” strategies are considered most adaptive when a stressor is not malleable to change. Conversely, “problem-focused” coping strategies are suggested when a stressor is appraised as controllable (Wenzel et al., 2002). Wenzel et al. (2002) emphasize the protective effect that “problem-focused” coping offers over emotional regulation.
Unlike system justification theory, which suggests an econometric perspective in which individuals see overarching social and economic stratification as an aspect of volitional control and natural order, the literature suggests that adoption of high-effort coping strategies implies the use of sustained individual effort, such as working long hours or not taking time off work, in order to cope with stress (Geronimus & Thompson, 2004; Jost, Banaji, & Nosek, 2004). As mentioned earlier, avoidance coping strategies such as denial coping might be an effective coping response to stressors that are apprised as not amenable to change (Carver et al., 1993; Meyer, Schwartz, & Frost, 2008; Schwartz et al., 1995). For instance, researchers have observed that the development of depressive symptoms such as fatigue and pessimism is a plausible reaction in the face of failed attempts to reach personal goals or when personal goals are unattainable (Nesse, 2000). Keller and Nesse (2006) found that feelings of guilt, rumination, fatigue, and pessimism were associated with failed efforts. Yet for many African Americans, especially those from socioeconomically disadvantaged backgrounds, hard, individual work may be perceived as the only way to achieve upward socioeconomic mobility and the socioeconomic benefits of investing in human capital (e.g., pursuit of higher education and training programs) and striving in the face of stressors may be worth great efforts. It is possible that individuals who engage in high-effort coping continue to strive despite individually and institutionally mediated racism. It is not clear whether African Americans, particularly those of greater SES, cope by striving in a high-effort manner and the mental health effects of such striving are unknown.
Social epidemiologist Sherman James posits that African Americans could use John Henryism, a “high-effort” coping strategy to cope with external stressors (James et al., 1983). James’s construct of John Henryism is based on the American folklore of an African American steel-driver named John Henry who famously raced a steam-powered machine during the construction of a rail road (Bronder, Speight, Witherspoon, & Thomas, 2014; James et al., 1983). As legend has it, John Henry won the race against the machine but soon dropped dead with a hammer in his hand. John Henryism is defined as a strong behavioral predisposition to cope actively with psychosocial and environmental stressors (Angner, Hullett, & Allison, 2011; Bennett et al., 2004; James, 1994; James et al., 1983). James (2002) further describes John Henryism as . . . a cultural adaptation on the part of newly freed people faced with the daunting task of creating for themselves, an American identity. To be authentic, that identity had to make possible a coherent expression of core American values such as hard work, self-reliance, and freedom.
James argues that in the face of psychosocial stressors, African Americans may use high-effort coping due to their increased exposure to psychosocial stressors, particularly in response to race-related obstacles such as racial discrimination (James, 1994, 2002; James et al., 1983). According to James, high-effort coping strategies are characterized persistent, sustained efforts to cope with racial barriers. Furthermore, James argues that high-effort coping may be deleterious to health because considerable energy is expended to cope with psychosocial stressors and individuals have greater perceived control over the outcome of a stressful situation.
John Henryism was initially developed to examine hypertension among African Americans, and thus, the majority of research to date has primarily tested the relationship between John Henryism and hypertension (Bonham, Sellers, & Neighbors, 2004; Clark, 2003; Dressler, Bindon, & Neggers, 1998; James et al., 1983; McClure & Myers, 1999; Merritt, Bennett, Williams, Sollers John, & Thayer, 2004). While the John Henryism construct has been empirically tested in a variety of different studies, there are gaps in previous explorations.
There are very few previous studies that have investigated the relationship between John Henryism and mental health, particularly depression (Bronder et al., 2014; Neighbors, Njai, & Jackson, 2007). One study conducted by Neighbors et al. (2007) explored the relationship between John Henryism and depressive symptoms using the National Survey of American Life (NSAL). They found that John Henryism was not significantly associated with depressive symptoms among African Americans. However, this study did not test the relationship between SES and John Henryism nor did it examine whether SES played a significant factor in the relationship between John Henryism and depressive symptoms.
The vast majority of studies that examine John Henryism have primarily focused on poor or low-income samples (Bonham et al., 2004). Bonham et al. (2004) indicate that more research is needed on samples of varying SES, particularly among African Americans, not just low SES samples. For instance, it is possible that African Americans who possess greater levels of SES are likely to use high-effort coping when faced with psychosocial stressors. Higher SES African Americans may apply great amounts of pressure on themselves to succeed, working very hard as a coping strategy to overcome structural and individually mediated racial discrimination. For many African Americans who have greater levels of SES, it is through investments in human capital (e.g., pursuing higher education) and sheer effort, rather than social capital or family wealth that has propelled them into a higher social class (Conley, 1999; Patillo-McCoy, 1999; Shapiro, 2004). And due to immense lack of wealth in the African American community as well as changes to the overall labor market, the social and economic position of many African Americans is tenuous (McBrier & Wilson, 2004; Patillo-McCoy, 1999; Wilson, 1996).
Light et al. (1995) conducted a study to determine whether high job status and John Henryism were related to hypertension among a sample of African Americans and Whites. Compared with White men in high-status jobs, they found that African Americans and White women who held high-status jobs reported higher John Henryism scores. Additionally, Light et al. found that African Americans who held high status jobs and were more likely to use high-effort coping had higher diastolic and systolic blood pressure levels. Bronder et al. (2014) examined the relationship between John Henryism and psychological distress in a community sample of 314 Black women. They found a negative relationship between John Henryism and depressive symptomatology and suggested that John Henryism was predictive of better mental health status in their sample. They also tested whether SES, specifically income and education, moderated the relationship between John Henryism and depression. Their results indicated that SES did not moderate this relationship. Bonham et al. (2004) examined high-SES African American men to explore the relationship between John Henryism and self-rated health. Using a sample of 399 African American men who were members of a national fraternal organization, they found a positive relationship between John Henryism and favorable self-rated physical health. The authors concluded that for the high-SES African American men in their study, John Henryism is beneficial to health.
Focus of the Present Study
Given the unique stressors that African Americans face, particularly as they accumulate more socioeconomic resources, a more comprehensive evaluation of the relationship between SES, racial discrimination, John Henryism, and depression is warranted. Previous research indicates that John Henryism is associated with poorer physical health (Bennett et al., 2004; James et al., 1983; James, Keenan, Strogatz, Browning, & Garrett, 1992). Depression is a highly prevalent mental disorder and is typically associated with poorer SES (Dohrenwend et al., 1992; Kessler, Berglund, et al., 2005; Kessler, Chiu, Demler, & Walters, 2005). However, the relationship between SES and mental health is not consistent. For instance, Salami and Walker (2013) found that higher SES was associated with greater depressive symptoms and anxiety. Additionally, findings from previous research that have examined the relationship between John Henryism and mental health outcomes are mixed. Some researchers have found positive relationships between John Henryism and mental health, which would suggest that John Henryism is deleterious to health (Neighbors et al., 2007). Other studies had found negative relationships between John Henryism and poorer mental health, which could indicate a health enhancing effect (Bronder et al., 2014). Few studies have examined the relationship between John Henryism and depression and even fewer studies have examined how SES and racial discrimination may affect these relationships. This study takes advantage of a national, probability-based sample of African Americans to examine these relationships, uses a fully structured lay interview to assess depression according to International Classification of Diseases, 10th Revision and Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria, and seeks to better understand the complex relationships between John Henryism, depression, SES, and racial discrimination.
The hypotheses of this article were as follows:
Method
Sample
Data for this article were drawn from the NSAL Reinterview (Jackson et al., 2004). Data were collected between 2001 and 2003 and used an in-home, face-to-face interview design with computer-assisted personal interviewing software. Interviews lasted an average of 2 hours and 20 minutes. Study eligibility criteria for participation in the NSAL included that respondents were 18 years of age or older and that they spoke English. The NSAL used a national probability sampling process in which data were collected using a stratified and clustered sample design, and weights were created to account for unequal probabilities of selection, nonresponse, and poststratification (Heeringa et al., 2004; Kessler & Üstün, 2004). The sample size for each racial/ethnic group was calculated based on the prevalence estimates of mental disorders in their respective populations but was primarily based on the rates of native-born African Americans and Whites (Jackson et al., 2004). The final African American sample of the NSAL includes 3,570 African Americans, with a response rate of 71%. The weighted NSAL sample of African Americans represented the population of this racial group in the continental United States.
All NSAL respondents were invited to complete a self-administered questionnaire that was mailed to participants’ residences. The NSAL Adult Reinterview (RIW) included measures that were not available in the original NSAL, namely the John Henryism Active Coping Scale developed by Sherman James, which was used to measure high-effort coping and is described in further detail below. We limited analyses to the RIW African American Sample. Of the 3,570 African American NSAL respondents who participated in the original, face-to-face interview, a total of 2,137 completed the self-administered RIW for a response rate of 60%. Several factors, namely female gender, unemployment, higher levels of education, and participating in the original NSAL interview post–September 11, 2001, were associated with higher response rates on the RIW. Weights were created and used to account for these nonresponse variations. The final sample, which included respondents who answered all relevant items used for this analysis was n = 2,137. This study was approved by the institutional review board at the University of Michigan.
Measures
Dependent Variable
Lifetime incidence of depression was the primary outcome for this study. The World Mental Health Composite International Diagnostic Interview (CIDI) is used to assess depression in the NSAL (Kessler, Berglund, et al., 2005; Kessler, Chiu, et al., 2005; Kessler & Üstün, 2004). The CIDI is a fully structured lay interview that assesses mental disorders according to the International Classification of Diseases, 10th Revision and DSM-IV criteria to assess a broad range of psychiatric disorders. The CIDI includes question items on respondents’ symptoms of depression, severity of symptoms in addition to the amount of impairment, and the length of time respondents report depressed feelings. Williams et al. (2007) compared the validity of CIDI diagnosed depression versus the Structured Clinical Interview for DSM-IV, which is a diagnostic interview that must be administered by a clinician. Comparisons of the CIDI and the Structured Clinical Interview for African American NSAL respondents in the clinical reappraisal sample indicated fair concordance for African Americans (κ = 0.43; 95% confidence interval [CI] = 0.26-0.59; Williams et al., 2007). Respondents who met criteria for life course depression were designated as “1” and those who did not meet criteria for depression were designated as “0” in logistic regression models.
Independent Variables
Racial discrimination was measured using the Everyday Discrimination Scale (Essed, 1991; Williams et al., 1997). The Everyday Discrimination Scale used in the NSAL is composed of 10 items that correspond to the stem question, “In your day-to-day life how often have any of the following things happened to you?” The scale included items such as “I am treated with less courtesy than other people,” “I sometimes receive poorer service than other people,” and “I am called names or insulted,” with a 6-point Likert-type response scale (6 = almost every day, 5 = at least once a week, 4 = a few times a month, 3 = a few times a year, 2 = less than once a year, and 1 = never; α = .86). Respondents were asked if they had experienced any of these events anytime in their life and to what they attributed these experiences. Respondents could indicate whether they received poorer treatment due to personal characteristics such as race, body weight, sexual orientation, and gender. We limited analyses to reports of discrimination attributed to race.
The John Henryism Scale for Active Coping was used to assess high-effort coping and is measured in the NSAL using an adapted version of the 12-item, Likert-type, John Henryism Scale for Active Coping (James et al., 1983). The scale is composed of 12 items with higher scores indicating more high-effort coping when faced with difficult psychosocial stressors. The scale measures the behavioral predisposition to cope actively and persistently with difficult psychosocial stressors and barriers. The question stems included items such as, “Sometimes I feel that if anything is going to be done right, I have to do it myself”; “I don’t let my personal feelings get in the way of doing a job”; “Once I make up my mind to do something, I stay with it until the job is completely done”; “When things don’t go the way I want them to, that just makes me work even harder.” Responses to the items range from 1 to 4 with higher scores reflecting higher levels of active coping: 1 (completely false) to 4 (completely true). Possible scores ranged from 0 to 45 for the NSAL RIW African American sample, with higher scores indicating more high effort coping when faced with difficult psychosocial stressors. Cronbach’s alphas for internal consistency for this sample were .87 for African Americans. There have been no discrepancies found in validity between African American men and women on the scale (James, 2002).
Several sociodemographic and SES variables were also included in analyses. Gender was self-reported and dichotomous, with female as the reference category. Age was a continuous variable of respondents’ reported age at the time of the interview. Family income to poverty ratio (reported family income divided by the 2003 U.S. poverty level) was measured as a continuous variable. Respondents’ highest level of education was collected as a continuous variable in years of education. Household size was a continuous variable that indicates the number of individuals who reside in respondents’ households, including adults and children. Age and gender were controlled for in models because they are both associated with depression and could be confounding factors. We controlled for household size because SES, particularly income, is influenced by household size.
Analysis Strategy
All analyses were completed using SAS Version 9.2 software, which has capabilities to handle the complex survey design of the NSAL (Heeringa et al., 2004). Linear regression was used to examine the relationship between SES indicators and racial discrimination as well as the association between SES and John Henryism. Multivariable logistic regression was used to determine the relationship between racial discrimination and depression, controlling for age, gender, and household size. Interaction terms were created to examine whether John Henryism moderated the relationship between racial discrimination and depression. The analyses described below account for probability-based sample weighting and analyses incorporate the design effects in the estimation of standard errors and test statistics.
Results
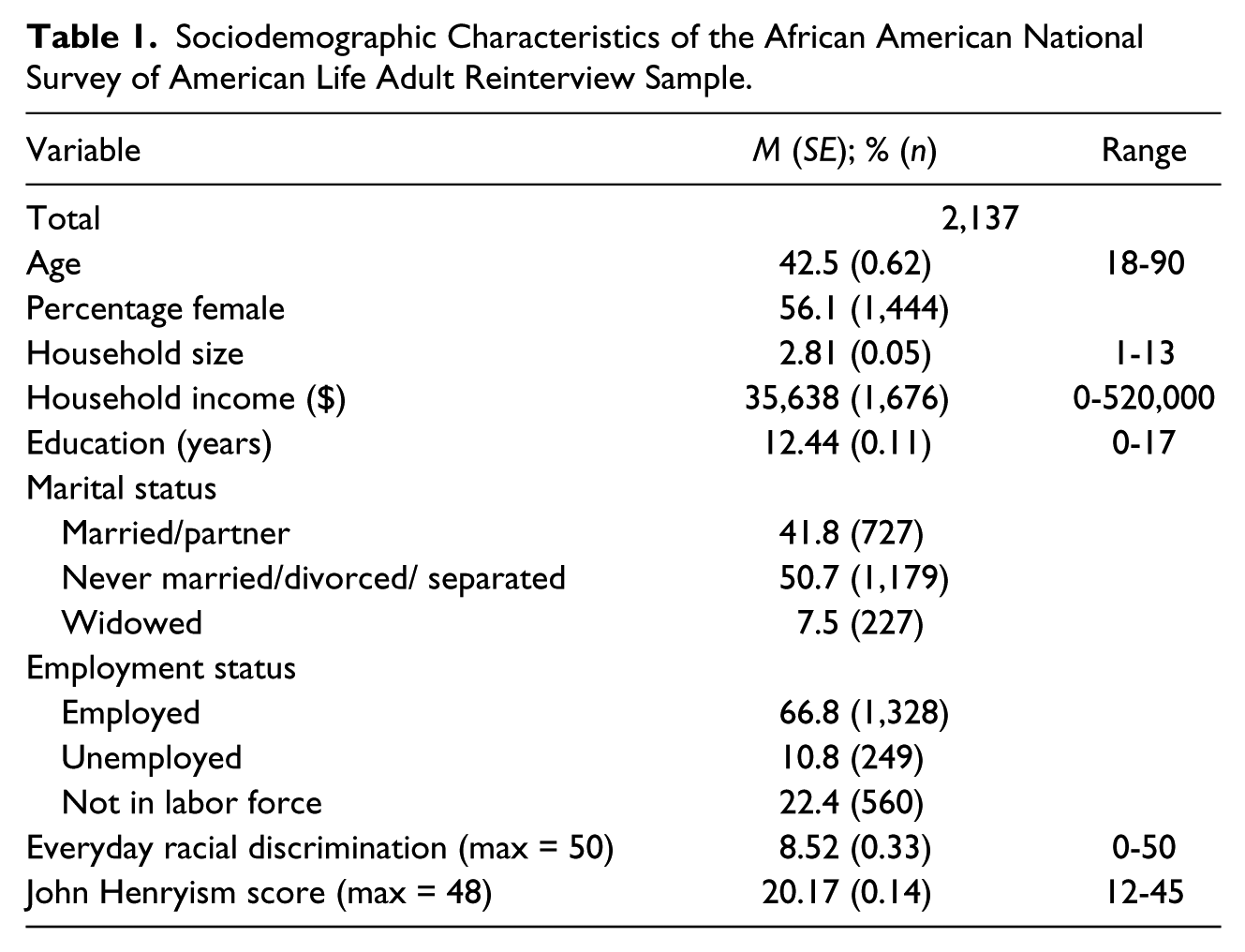
The sociodemographic characteristics of the sample are displayed in Table 1. The average age of the sample of African Americans was 42.5 years (SE = 0.62) and women represented 56% of the sample. Forty-two percent of the sample reported that they were married or lived with a romantic partner and 67% of respondents reported that they were currently employed. Respondents reported an average of 12 years of education and an average household income of $35,638. The average everyday racial discrimination score was 8.52 (SE = 0.33). Scores ranged from 0 to 50 (the maximum score was 50). The mean John Henryism score was 20.17 (SE = 0.14). Scores ranged from 12 to 45 (the minimum score is 12 and the maximum score possible on the scale is 48).
Sociodemographic Characteristics of the African American National Survey of American Life Adult Reinterview Sample.
It was hypothesized that higher levels of SES would be positively associated with greater reports of racial discrimination and higher John Henryism scores. Table 2A displays the bivariate relationship between SES and racial discrimination. There was a significant positive relationship between education and racial discrimination (p = .02) but there was no significant relationship between income, relative to poverty, and racial discrimination. There was no evidence to support the hypothesis that greater levels of SES be would be associated with increased levels of John Henryism. Analyses indicated that there were no statistically significant relationships observed between SES and John Henryism. This relationship is displayed in Table 2B.
Relationship Between (A) Socioeconomic Status (SES) and Everyday Discrimination and (B) Socioeconomic Status and John Henryism.
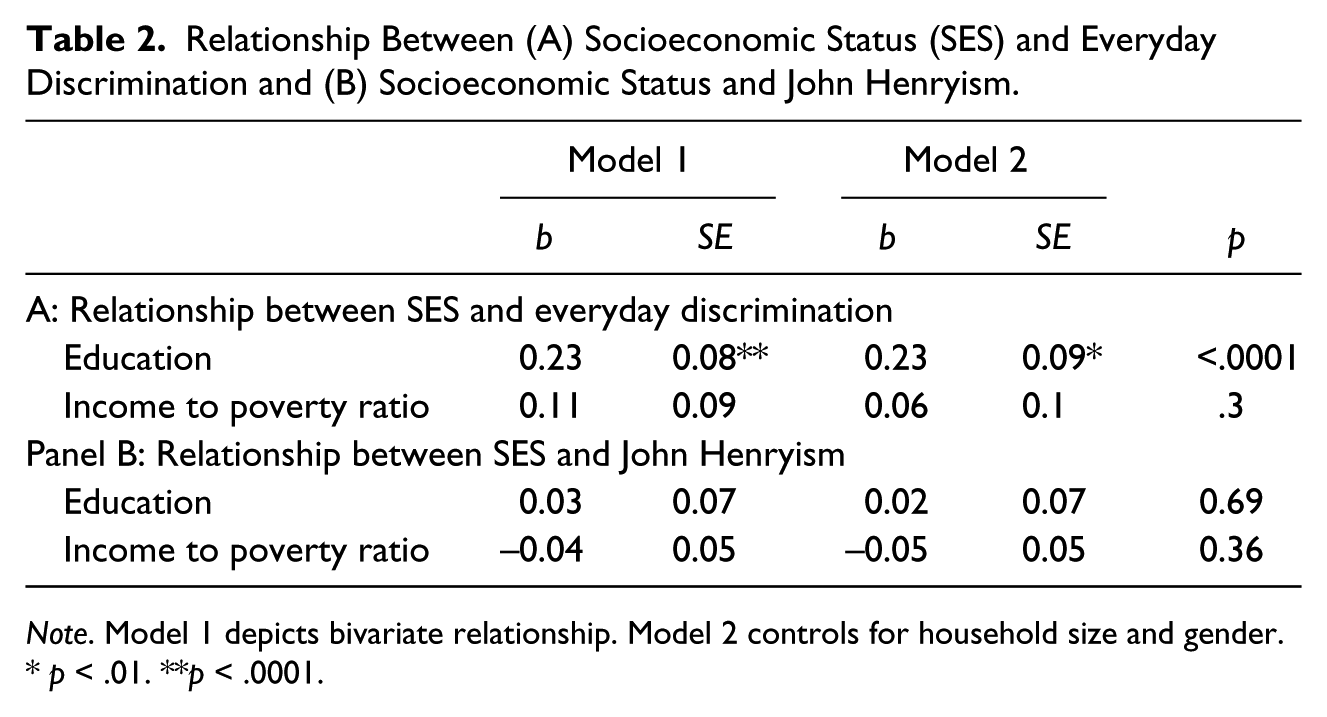
Note. Model 1 depicts bivariate relationship. Model 2 controls for household size and gender.
p < .01. **p < .0001.
It was hypothesized that both racial discrimination and John Henryism would be associated with greater odds of depression. Table 3 presents the findings for the bivariate and multivariable logistic regression analyses that were used to examine the relationship between everyday racial discrimination and depression. There was a significant bivariate association between everyday discrimination and greater odds of depression (odds ratio [OR] = 1.04; CI = 1.03-1.06). This relationship remained significant after adjusting for covariates in the multivariable logistic regression model (OR = 1.05; CI = 1.03-1.06). Next, Table 4 depicts the bivariate relationship between John Henryism and depression. There was a significant association (OR = 1.04; CI = 1.01-1.07). This relationship held once we adjusted for covariates in the multivariate model (OR = 1.04; CI = 1.02-1.07).
Major Depressive Episode by Socioeconomic Status and Everyday Racial Discrimination.
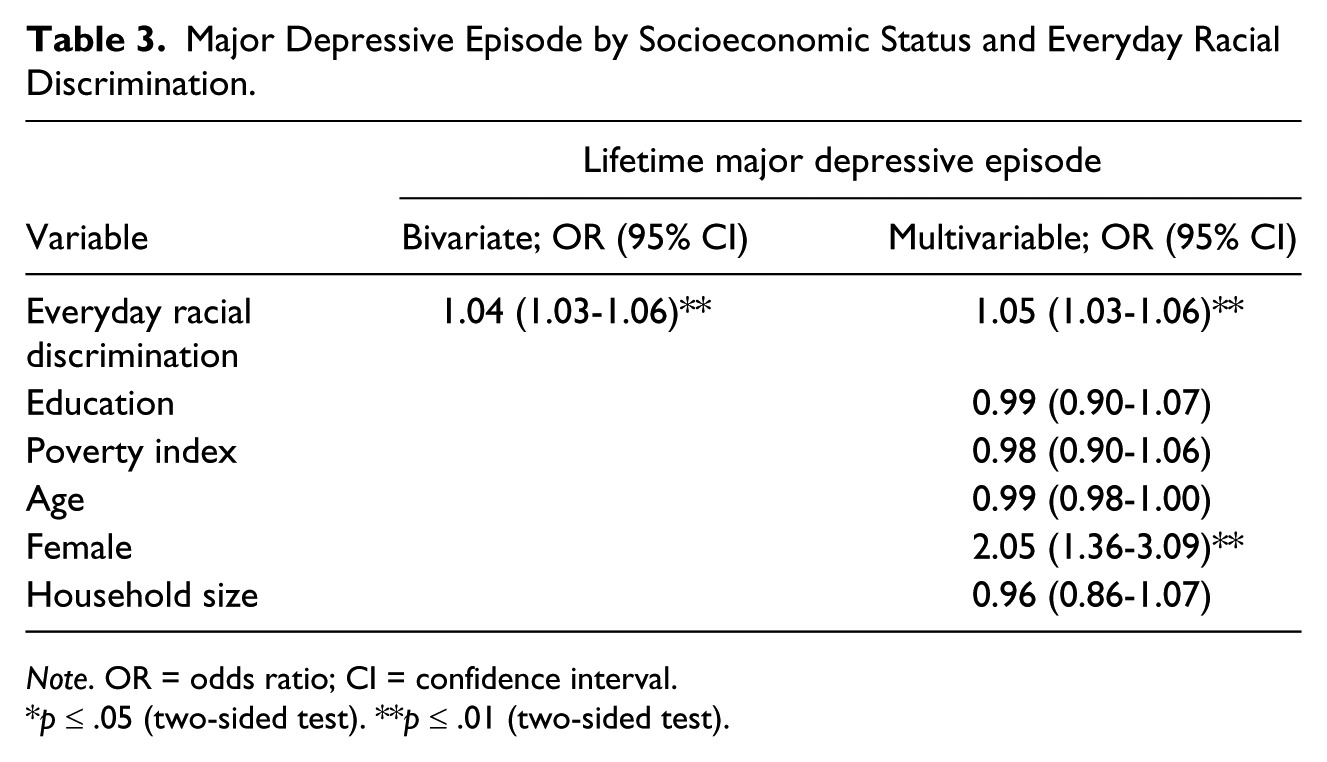
Note. OR = odds ratio; CI = confidence interval.
p ≤ .05 (two-sided test). **p ≤ .01 (two-sided test).
Major Depressive Episode by Socioeconomic Status and John Henryism.
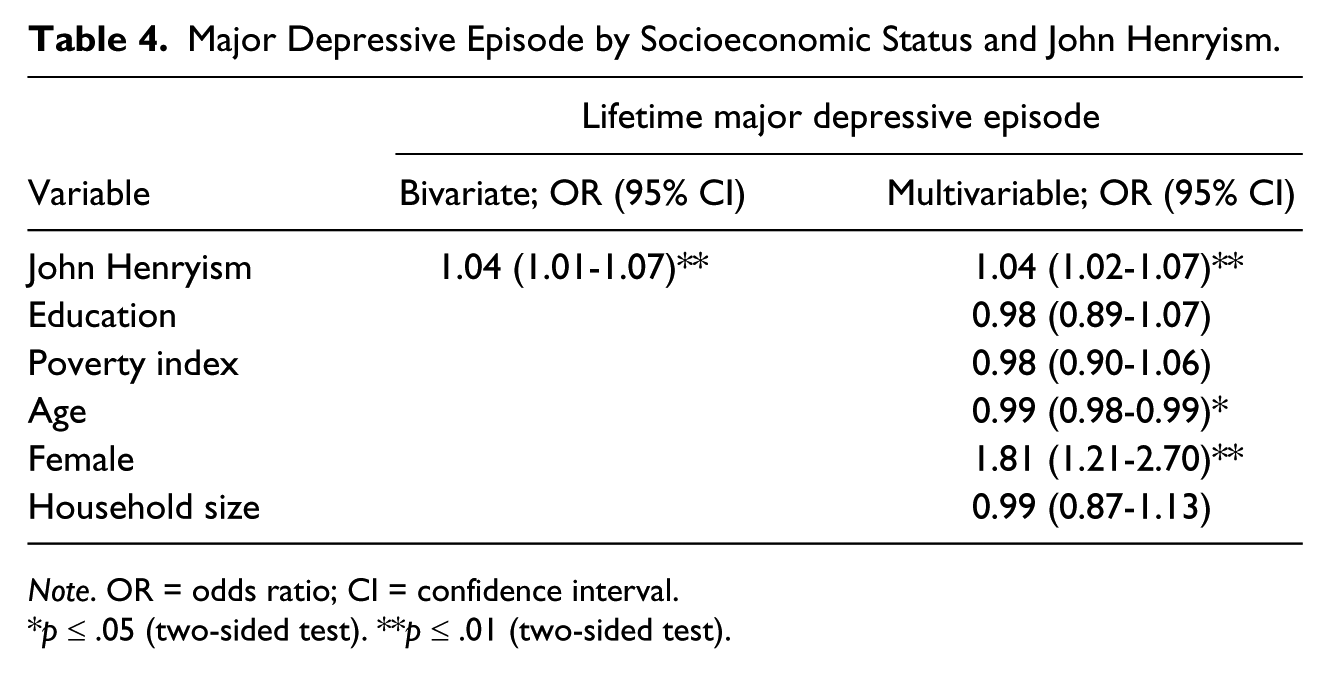
Note. OR = odds ratio; CI = confidence interval.
p ≤ .05 (two-sided test). **p ≤ .01 (two-sided test).
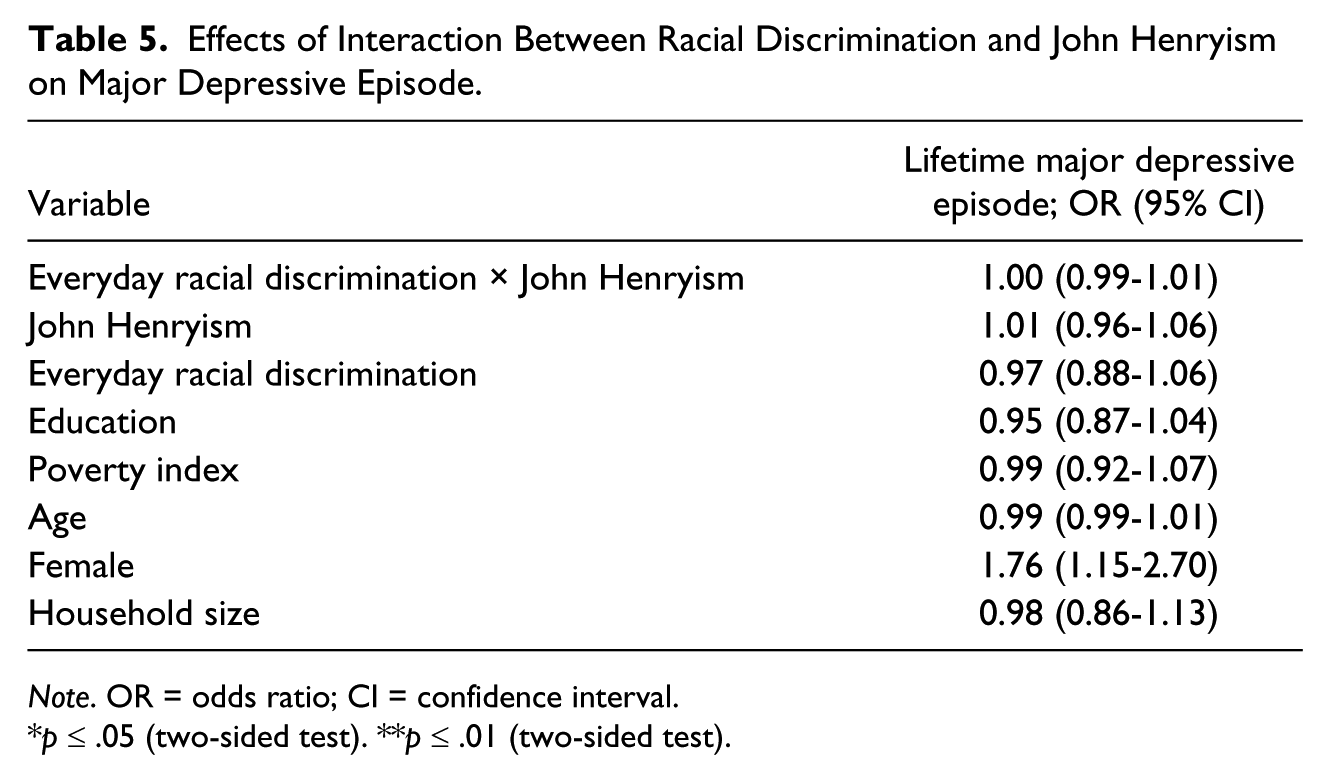
Finally, it was hypothesized that the relationship between racial discrimination and depression would be moderated by John Henryism. There was a significant bivariate relationship between racial discrimination and John Henryism (r = 0.08, p < .001; table not shown). As previously mentioned, there were also significant relationships between both John Henryism and depression and between racial discrimination and depression. However, the interaction between racial discrimination and John Henryism was not statistically significant (see Table 5). This finding suggests that the association between racial discrimination and depression was not attenuated by the effects of John Henryism.
Effects of Interaction Between Racial Discrimination and John Henryism on Major Depressive Episode.
Note. OR = odds ratio; CI = confidence interval.
p ≤ .05 (two-sided test). **p ≤ .01 (two-sided test).
Discussion
The primary aims of this study were to examine the relationships between SES and racial discrimination and between SES and John Henryism among African Americans. We also examined whether racial discrimination and John Henryism were associated with greater odds of depression, and whether John Henryism moderated the relationship between racial discrimination and depression. First, we found that racial discrimination was significantly associated with greater odds of depression and African Americans. African Americans who reported higher levels of education were more likely to report experiences of racial discrimination. Although this association has been found before in previous studies, these findings, observed in a nationally representative sample of African Americans, lend additional empirical support to results from previous studies.
Contrary to our hypothesis, we did not observe a significant association between greater levels of SES and increased John Henryism scores. However, there was a significant positive association between John Henryism and greater odds of depression. These findings differ from previous studies that have examined the relationship between John Henryism and depression (Bronder et al., 2014). In the stress process, individuals appraise whether they have the coping resources to handle a stressor. It is possible that hard work is deemed as the key to upward social mobility among African Americans. As such, when faced with unfair treatment and other stressors, African Americans who use high-effort coping could negatively affect their mental health. The foundational research on John Henryism that has shown a positive relationship between greater levels of John Henryism and cardiovascular outcomes (Bennett et al., 2004; James et al., 1992; James et al., 2006). Angner et al. (2011) found that higher John Henryism scores were associated with lower levels of happiness in African American men. The observed relationship between John Henryism and depression in this study suggests that engaging in high-effort coping is associated with greater likelihood of depression among African Americans.
Also contrary to our hypothesis, we did not find evidence that John Henryism moderated the relationship between racial discrimination and depression. One reason for this could be that the measure of racial discrimination used here did not adequately capture the types of experiences that individuals would use high-effort coping to address. For instance, the items in the Everyday Discrimination Scale focused on individually mediated forms of racial discrimination. So it is possible that “microagressions” or broader structural level racism may not have been captured by this measure (Chae, Nuru-Jeter, Lincoln, & Francis, 2011; Kwate & Meyer, 2011). Additionally, the positive association observed between depression and John Henryism could indicate that greater levels of high-effort coping are not likely to protect against the development of depression.
Limitations and Conclusions
Strengths of this study include the use of a nationally representative sample of African Americans and use of the CIDI to assess depression. Yet there are several key limitations to consider when interpreting results. First, it is possible that depressed individuals are more likely to interpret certain experiences as discriminatory. This could explain the positive association between racial discrimination and increased odds of depression. Therefore, we could not determine whether depression influenced respondents’ perceptions of racial discrimination. Similarly, since the NSAL is a cross-sectional study, longitudinal data are needed to determine the temporal relationship between, not only racial discrimination but also John Henryism and depression. Although analyses revealed statistically significant associations between racial discrimination, John Henryism, and depression, the odds ratios were relatively small. One possible explanation is that the measure of racial discrimination used here underestimate discriminatory experiences and do not adequately capture the frequency, intensity, or psychological impact of racial discrimination among African Americans. There are multiple levels of racism, including individual, institutional, and internalized (Jones, 2000). However, we were only able to examine one level, individual-level perceptions of racial discrimination, and additional insights may be gained from the use of a measure that focuses on institutional-level racism. Additionally, this study only examined two factors that could affect depression, racial discrimination, and John Henryism. Another important coping mechanism to consider that was not examined is social support. The stress and coping model suggests that once individuals appraise a stressor, they will first turn to social support to cope with the stressor (Wenzel et al., 2002). Social support has been implicated as a significant coping factor, particularly for African Americans, in the stress and coping literature (Bronder et al., 2014; Cassel, 1976; Thoits, 1995; Wheaton, 1985). For instance, we did not observe an association between SES and John Henryism. It is possible that social support provided individuals with the resources necessary to cope with stress and minimizes the use of high-effort coping strategies. Future research efforts are needed to examine these relationships in different racial/ethnic groups and across gender.
In their report, Mental Health: A Report of the Surgeon General (U.S. Department of Health and Human Services Office of the Surgeon General, 2001), the Substance Abuse and Mental Health Services Administration called for more research to investigate how African Americans cope with stress, especially race-related stressors such as racial discrimination, and how coping strategies used by African Americans are related to the occurrence of mental health problems (Townsend & Belgrave, 2009; U.S. Department of Health and Human Services Office of the Surgeon General, 2001). More investigations of the potential interactions between SES, exposure to race-related stressors, and coping mechanisms and how these factors are related to depression among African Americans are needed (Williams et al., 2008). Continued research efforts should explore other coping mechanisms and factors that could protect the mental health of African Americans against stressors like racial discrimination.
The findings garnered from this study indicate that John Henryism is associated with greater odds of depression among African Americans. It is possible that African Americans who engage in high-effort coping strategies could have greater likelihood of experiencing depression. This finding is alarming, considering results from previous studies that indicate John Henryism is also related to poorer physical health (Bennett et al., 2004; Fernander, Duran, Saab, & Schneiderman, 2004; Haritatos, Mahalingam, & James, 2007; James, 2002; James et al., 1992). High-effort coping could be simultaneously harming the mental and physical health of African Americans. Thus, African Americans who engage in high-effort coping could run the risk of embodying the very legend of John Henry (Angner et al., 2011).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (Grants U01-MH577165; R01MH068804-04), with supplemental support from the Office of Behavioral and Social Science Research at the National Institutes of Health, the University of Michigan, and the Center for Research on Ethnicity, Culture and Health funded through the National Institute of General Medical Sciences (5R25GM058641-10). Additional support was provided by the Kellogg Health Scholars Program, the University of California, San Francisco, Center on Social Disparities in Health, and the University of California, San Francisco Health Disparities Working Group.