
Abstract
The Africultural Coping Systems Inventory (ACSI) assesses African Americans’ culturally relevant stress coping strategies. Although its factor structure, reliability, and validity of the scores have been examined across ethnic groups of African descent, psychometric properties have not been investigated in an African American clinical sample. Thus, it is unclear if the ACSI is useful for research with African Americans with distress. To assess the ACSI’s psychometrics, we used data from 193 low-income African American women who in the past year encountered interpersonal trauma and attempted suicide. We tested four models: one-factor, four-factor, four-factor hierarchical, and bifactor. None of the models were optimal, suggesting possible revisions to ACSI items. Yet the bifactor model provided a better fit than other models with items loading onto a general factor and onto specific factors. Internal consistency of the scores was above the recommended criterion (i.e., .70), and the ACSI general factor was related to depressive symptoms, suicidal ideation (but not alcohol abuse), providing some support for its concurrent validity. Future directions, limitations, and clinical-counseling implications are discussed.
African Americans’ culture-specific coping practices include participating in spiritual and religious practices and rituals, like prayer and meditation; seeking and receiving support from extended family and kin networks; and connecting with culturally sanctioned social groups and community resources (A. G. M. Brown et al., 2017; Utsey, Bolden, Lanier, et al., 2007; Utsey, Bolden, Williams, et al., 2007). These practices largely reflect West African coping principles, such as spirituality (i.e., communion with spiritual realms), collectivism (i.e., prioritizing the goals of the family and ethnic group), and communalism (i.e., focus on human relationships and the value of each community member; Asante, 1992; Cokley, 2005; Jones, 2003; Montgomery et al., 1990; Parham, 2002). To capture these processes, Utsey et al. (2000) used Africentric frameworks to develop the Africultural Coping Systems Inventory (ACSI), a scale to measure African Americans’ culture-specific coping responses to stress.
The ACSI has been validated using both exploratory and confirmatory factor analysis (CFA) techniques (Utsey et al., 2004; Utsey & Ponterotto, 1996). Psychometric findings have supported the ACSI’s multidimensionality and revealed four subscales: (a) Cognitive and Emotional Debriefing, defined as one’s adaptive reactions to environmentally based and racially charged stressors; (b) Collective Coping, characterized as one’s comfort derived from social connections with others or groups; (c) Spiritual-Centered Coping, identified as one’s resilience due to harmony with the universe and/or one’s higher power; and (d) Ritual-Centered Coping, described as one’s use of rituals to preserve balance (Utsey et al., 2000). Subscale scores have exhibited acceptable to good internal consistency, with coefficients ranging from .71 to .84 in African American samples (Utsey et al., 2000; Utsey et al., 2004).
Moreover, ACSI scores have exhibited criterion-related validity. Several ACSI subscale scores have related to adaptive coping processes in African American college students (Utsey et al., 2000) and quality of life in non-students (Utsey, Bolden, Lanier, et al., 2007). Yet its findings with African American women have been mixed. For instance, one study found that Africultural coping did not moderate the associations between race- and gender-based discrimination and psychological symptoms for African American women, whereas another study found that cognitive-emotional coping styles partially mediated the relation between gendered racism and psychological distress (no mediating effects were found for spiritual-centered, collective, and ritual-centered coping; Greer, 2011; Thomas et al., 2008). Also, in the context of low levels of racial tension, women who used more Africultural coping reported more stress than those who used less Africultural coping, whereas in the context of higher levels of racial tension the opposite pattern was observed (Shahid et al., 2018). Thus, closer inspection of Africultural coping’s performance across African American subgroups is warranted.
Utsey et al. (2004) also bolstered the research on the ACSI by examining its psychometric performance across ethnically diverse African descent populations. Given that the ACSI captures coping behaviors presumed to reflect African-centered epistemologies, Utsey et al. (2004) hypothesized that its factor structure would replicate across ethnically distinct groups. To test this hypothesis, they used CFAs to assess the structural invariance of the ACSI across three ethnically diverse samples: (a) 202 African Americans, (b) 143 African Caribbeans, and (c) 117 continental Africans (i.e., born in Africa). Contrary to expectations, although the pattern of coefficients for the four-factor structure was comparable across the samples, the variance and covariance parameters varied markedly. Also, model fit indices were higher for African Americans than the other two groups. Regarding internal consistency, data from the Caribbean and continental African samples yielded some Cronbach’s alpha estimates in the questionable range (.60 ≤ α < .70), whereas responses from African Americans resulted in acceptable to good estimates (α’s = .70-.82). These findings suggest that subscale items measured the same construct mainly in African Americans. Although these findings could have resulted from small sample sizes for both the Caribbean and continental African samples, it could be that the ACSI may be most relevant to African Americans and may not reflect the distinct experiences of individuals outside this ethnic group.
In addition to examining the ACSI’s psychometric properties across ethnically diverse samples, it is also imperative to investigate its psychometrics in subgroups nested within ethnic groups. Although African Americans generally have been included in psychometric evaluations of the ACSI, no studies have used African American women clinical samples specifically. This is concerning given that African American women with clinical diagnoses represent a particularly vulnerable and at-risk population who can benefit from adaptive coping strategies (Warren-Findlow & Issel, 2010). In particular, African Americans with major depressive disorder were more likely to be chronically depressed and to exhibit worse impairment (Williams et al., 2007), and this pattern was especially true for African American women (Centers for Disease Control and Prevention, 2016). Moreover, suicide rates are steadily rising in African American women aged 45 to 64 years (Curtin et al., 2016). Furthermore, although problem drinking was less likely to be observed in African American women relative to White women and African American men, people with a mental illness reported pronounced alcohol or drug use concerns (Cobb & Assari, 2019). Therefore, it could be that mental health status engenders unique within-group differences among African Americans that differentially influence coping, and thus differentially shape the psychometrics of the ACSI. For instance, on the one hand, given that stressful situations prompt the use of culture-specific coping, African American women with psychiatric symptoms may be more prone to use and require the benefits of multifaceted Africultural coping practices. On the other hand, women with clinically significant distress may be less likely to utilize coping practices that attenuate mental health symptoms, partially explaining their symptomatology. Yet the psychometric utility of this scale and its relation to clinical indicators of depression, suicide, and alcohol abuse have not been systematically examined, restricting the field’s understanding of Africultural coping as a clinically viable protective factor for African American women with elevated psychopathology.
Psychometric evaluations of the ACSI in African American women clinical samples can also benefit from the use of innovative methodological approaches. The ACSI’s factor structure has been assessed via a correlated-traits model approach, but no studies have utilized a bifactor model despite the fact that bifactor models have been recommended over unidimensional and correlated-traits models. Bifactor models allow researchers to simultaneously explore a latent common trait and additional subtraits (Reise et al., 2010), enhancing the nuanced examination of both common variance shared by factors and unique variance specific to each factor (Gonzalez & MacKinnon, 2018; Reise et al., 2010; Reise et al., 2016). Using this specific approach with the ACSI may lead to additional theory building regarding Africultural coping, and it can improve the empirical clarity pertaining to disentangling general Africultural coping from specific coping strategies (i.e., spiritual, ritual, collective, and cognitive and emotional debriefing) in relation to health and wellness outcomes among people of African descent.
The Current Study
The current study represents an effort to expand research on the ACSI by investigating its factor structure, reliability, and validity in low-income African American women who in the past year encountered interpersonal trauma and attempted suicide. To test the ACSI’s factor structure and to select the most theoretically sound and best fitting model, we followed CFA recommendations by testing different models (T. A. Brown, 2014; Worthington & Whittaker, 2006). We tested the commonly supported four-factor model alongside other models: one-factor (all scale items load onto one factor), four-factor hierarchical (four subscales load onto one, higher order factor), and a bifactor model (scale items load onto subscales and onto a general factor that accounts for shared variance). Because the bifactor model has not been tested before with this measure, our hypothesis about model fit was exploratory. In addition, because ACSI subscale scores have exhibited good internal consistency in African Americans, we presumed that subscale scores would exhibit good internal consistency (α ≥ .70) in an African American women clinical sample. Also, because the ACSI theoretically represents people’s adaptive response to stressors, and adaptive coping is believed to reduce symptomatology, we hypothesized that subscale scores would significantly and inversely relate to behavioral health symptoms (e.g., alcohol abuse, depression, and suicidal ideation), supporting concurrent-related validity. This investigation addresses the ACSI’s clinical utility among African American women with pronounced symptomology and the potential interrelations among Africultural coping and behavioral health outcomes in this vulnerable and at-risk population.
Method
Participants
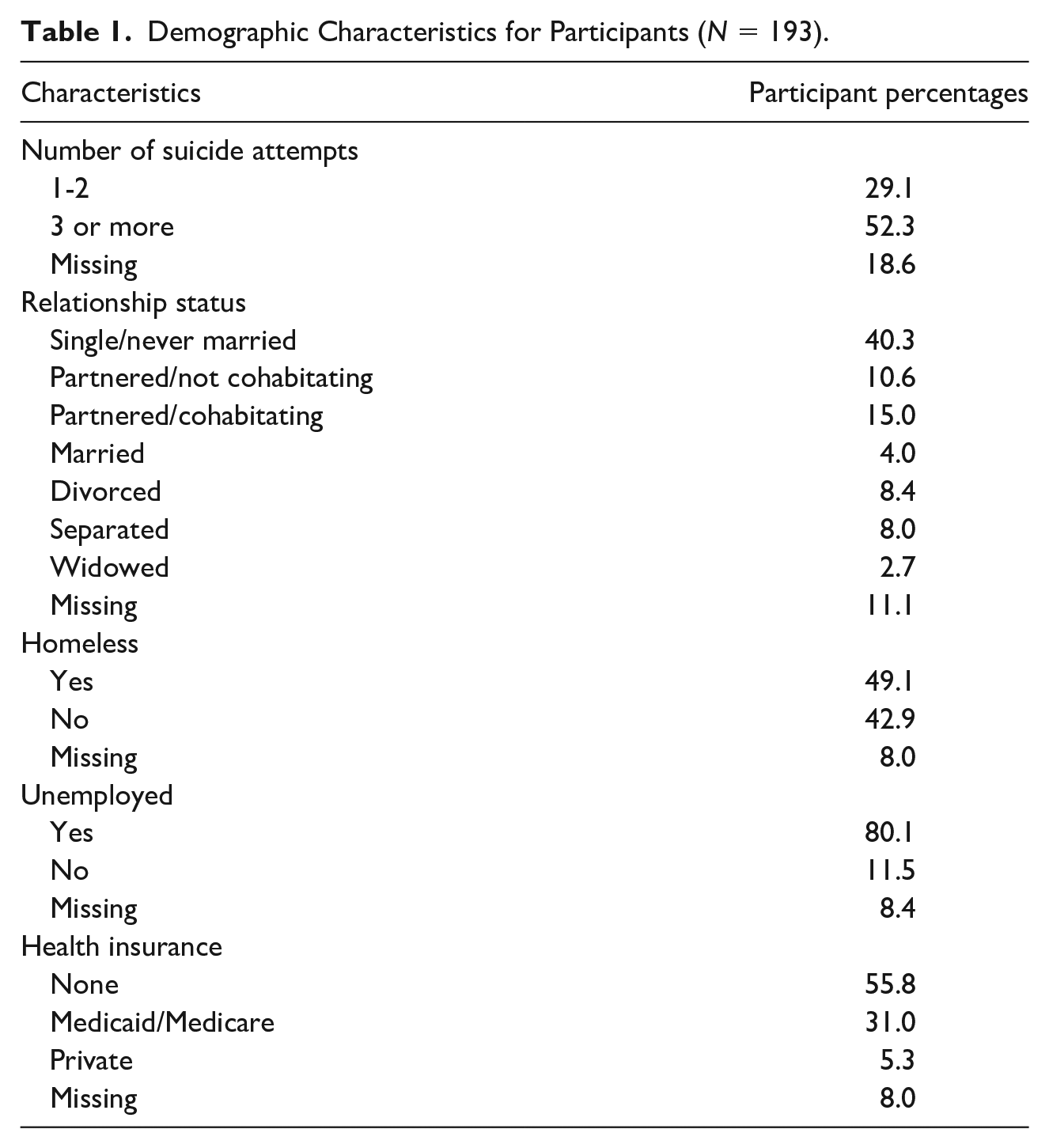
Table 1 includes information about the sample’s key sociodemographics. The sample consisted of 193 African American women aged 18 to 59 years (M = 36.72, SD = 11.17). Many women reported being single/never married (40.3%), homeless (49.1%), unemployed (80.1%), and having no health insurance (55.8%). All women reported at least one suicide attempt in the past year, and about half of the sample (52.3%) reported attempting suicide three or more times during their lifetime.
Demographic Characteristics for Participants (N = 193).
Procedure
Data were collected from 2008 to 2018. Recruitment took place in clinics within a university affiliated public hospital that mostly serves patients who are underinsured, low-income, and racial/ethnic minorities. Research personnel—trained undergraduate and graduate students who represented diverse gender identities and racial and ethnic backgrounds—approached people and screened them to determine study eligibility: (a) self-identification as an African American woman, (b) experience of intimate partner violence in the past year (Universal Screening Tool for Domestic Violence; Dutton et al., 1996), (c) suicide attempt in the past year, and (d) acceptable cognitive functioning (Folstein et al., 2001; Mini-Mental State Exam). Women were excluded if they were acutely psychotic (Kaslow et al., 2010; Psychotic Screener) or reported a life-threatening medical condition that would hinder participation in the study. Research personnel read aloud all study questionnaires to study participants. Study measures were administered in the same order for each participant, and study assessments took approximately 3 hours to complete. Participants were paid $25 at the end of the assessment.
Measures
Demographic questionnaire
The 26-item demographic questionnaire asked about participants’ age, socioeconomic background, and relationship status.
Africultural Coping Systems Inventory
The 30-item ACSI was used to measure four dimensions of culture-specific coping: (a) Cognitive and Emotional Debriefing (11 items; e.g., “Hoped that things would get better with time”); (b) Collective Coping (8 items; e.g., “Asked for suggestions on how to deal with the situation during a meeting of your organization or club”); (c) Spiritual-Centered Coping (8 items; e.g., “Prayed that things would work themselves out”); and (d) Ritual-Centered Coping (3 items; e.g., “Lit a candle for strength or guidance in dealing with the problem”; (Utsey et al., 2000). As part of the ACSI, participants were asked to describe a stressful situation from the past week. With this event in mind, they used a 4-point Likert-type scale (0 = did not use, 1 = used a little, 2 = used a lot, 3 = used a great deal) to denote which strategies they used to cope. For each subscale, items were summed, and higher scores indicated more use of that coping strategy. Existing psychometric information for the ACSI is presented in the literature review above.
Brief Michigan Alcoholism Screening Test
Alcohol abuse was assessed via the 10-item Brief Michigan Alcoholism Screening Test (bMAST; Pokorny et al., 1972). This measure has been used across clinical and research settings to measure lifetime drinking behaviors, and a sample item is, “Have you ever been arrested for drunk driving or driving after drinking?” Participants answered “yes” or “no” to each of the questions. For Items 3, 8, and 9, participants received zero points if they responded “no” and five points if they responded “yes.” For all other items, participants received zero points if they answered “no” and two points if they answered “yes.” Once points were assigned to all items, points were summed, with the total score range falling between 0 and 29 and with higher values representing more issues with alcohol. In a recent systematic evaluation of the bMAST across studies and samples, this measure exhibited adequate internal consistency of the scores (α ≥ .70). In addition, it has demonstrated good internal consistency of the scores across African American clinical samples (α’s ranging from .84 to .88; (Bliss et al., 2008; Watson-Singleton et al., 2019). Good internal consistency for the measure was obtained in the current study (α = .87). It has also demonstrated diagnostic validity with a diagnostic accuracy rate of about 80% (Minnich et al., 2019), supporting its construct validity.
Beck Depression Inventory
The 21-item Beck Depression Inventory (BDI-II) measured severity of depressive symptoms during the past two weeks (Beck et al., 1996). Item scores ranged from 0 to 3, and total scores range from 0 to 63. Item scores were summed, and higher scores indicated more depressive symptomatology. Example items include, “I am sad all the time,” and “I do not expect things to work out for me.” Across studies, the BDI-II scores have exhibited excellent internal consistency (α = .90) and strong test-retest reliability (α’s ranging from .73 to .96), including among low-income African Americans who have attempted suicide (α = .94; (Joe et al., 2008; Wang & Gorenstein, 2013). The Cronbach’s alpha estimate in the current study evidenced excellent internal consistency (α = .92). A recent comprehensive analysis of the BDI-II’s factor structure revealed that the best fitting model represented a general depression factor and three specific factors (i.e., cognitive, somatic, affective; (McElroy et al., 2018). Therefore, the authors recommended that the BDI-II be viewed as a unidimensional scale that was scored as such. It has also demonstrated good specificity with an accuracy rate of about 92% in correctly classifying those without major depressive disorder (Cahill et al., 2006; Wang & Gorenstein, 2013).
Beck Scale for Suicidal Ideation
The 21-item Beck Scale for Suicidal Ideation (BSS) measured participants’ desire to die, reasons for living, and suicidal intent (Beck & Steer, 1991). Items are rated from 0 to 2 with total scores ranging from 0 to 42. Item scores were summed, and higher scores denoted more suicidal ideation. An example items are “(0) I would try to save my life if I found myself in a life-threatening situation”; “(1) I would take a chance on life or death if I found myself in a life-threatening situation”; “(2) I would not take the steps necessary to avoid death if I found myself in a life-threatening situation.” Its internal consistency of the scores has been excellent in African American clinical samples (α = .90; Watson-Singleton et al., 2018), and good internal consistency was found in the current sample (α = .85). Additionally, the BSS scores have exhibited concurrent validity, such as being positively related to current ideation (Β = 2.52, standard error [SE] = .13, p < .001), hopelessness (Β = .69, SE = .07, p < .001), and thwarted belongingness (Β = 5.01, SE = .37, p < .001; Guiteirrez et al., 2019).
Data Analysis
To assess competing models of the ACSI’s factor structure in this sample, we conducted CFAs using Mplus version 8 (Muthen & Muthen, 2017). ACSI item raw scores were used. There was less than 5% missing data for any item, and missing data were handled with the full information maximum likelihood, which uses all available information by estimating population parameters that would likely produce the estimates from the sample data. Mahalanobis distance tests were conducted to determine multivariate outliers; no significant outliers were detected.
All analyses were performed using the robust maximum likelihood estimator (i.e., maximum likelihood estimation with robust SEs), which is appropriate for nonnormally distributed variables and noncomplete data (Muthen & Muthen, 2017). To determine model fit, we used the Akaike information criterion and the Bayesian information criterion, both of which serve as indicators of model fit and parsimony (Kline, 2016). There are no recommended cutoffs for Akaike information criterion and Bayesian information criterion values, but lower values indicate better fit (Kline, 2016). Also for the sake of completeness, additional fit indices were included, such as chi square, root mean square error of approximation (RMSEA < .08 for adequate fit), comparative fit index (CFI > .95 for good fit), Tucker-Lewis index (TLI > .95 for good fit), and standardized root mean square residual (SRMR < .08 for good fit; Hu & Bentler, 1999). We also included a chi-square difference test with a Satorra-Bentler scaling correction (which is necessary when using the robust maximum likelihood estimator) to directly compare goodness of fit between models, where a p value < .05 indicates a statistically significant difference in goodness of fit (Jiang & Yuan, 2017). In addition, internal consistencies of the scores for the factors associated with the best fitting model were calculated via Cronbach’s alpha as well as coefficient omega (proportion of variance attributable to all sources of common variance) and omega hierarchical values for bifactor models (proportion of variance in total subscale score that can be attributed to the two general factors; Revelle & Zinbarg, 2009). Finally, validity analyses were performed via correlations between the ACSI latent factors and behavioral health total scores: alcohol abuse, depressive symptoms, and suicidal ideation.
Results
Descriptive Statistics
Descriptive analyses (mean, standard deviations, minimum, maximum, skewness, and kurtosis) were performed to aid data cleaning and to ensure data entry accuracy. For ACSI subscales, the ranges, means, and standard deviations are as follows: the Cognitive and Emotional Debriefing subscale ranged from 0 to 33 (M = 17.52, SD = 6.25); Spiritual-Centered Coping ranged from 0 to 24 (M = 14.65, SD = 5.96); Collective Coping ranged from 0 to 24 (M = 12.12, SD = 5.53); and Ritual-Centered Coping ranged from 0 to 9 (M = 2.45, SD = 2.65). Skewness for subscales scores ranged from −.456 to .969, with no scores outside of the recommended cutoff of ±1.0. Kurtosis scores ranged from −.693 to −.098. Supplemental tables of the descriptive statistics and correlation matrix are available on request.
CFA
Building on previous literature, we compared four models of the ACSI’s underlying structure: (a) four-factor correlated model in which items loaded onto four latent factors representing the ACSI subscales; (b) one-factor model in which all items loaded onto a single latent factor; (c) a hierarchical factor model in which items loaded onto four latent subscale factors which in turn loaded onto a single, latent variable; and (d) bifactor model in which items loaded onto both a general factor and four uncorrelated factors representing the subscales. Ultimately, none of the models fit well. Across all models, the bifactor model had the best fit to the data across all fit indices; however, it only exhibited acceptable model fit on two of the four fit indices. RMSEA of .053, 95% confidence interval [.044, .061] and SRMR of .056 were lower than the minimum criterion value of .08 or less, which indicated acceptable model fit. Values for the other two indices were not acceptable: the CFI (.873) and TLI (.850) were less than the minimum criterion of .90 for acceptable model fit.
Furthermore, in the bifactor model, most items loaded dominantly onto the general factor. Also, the Cognitive and Emotional Debriefing, Spiritual-Centered Coping, and Ritual-Centered Coping factors were relatively well-defined, revealing unique contributions (i.e., factor coefficients ranging from .295 to .777) to the conceptualization of Africultural coping. Yet the Collective-Centered Coping items almost all loaded exclusively onto the general factor, suggesting that this subscale may not add to the conceptualization of Africultural coping beyond a general score, at least in this sample (Table 2).
Confirmatory Factor Analyses Results for All Alternative ACSI Models (N = 193).
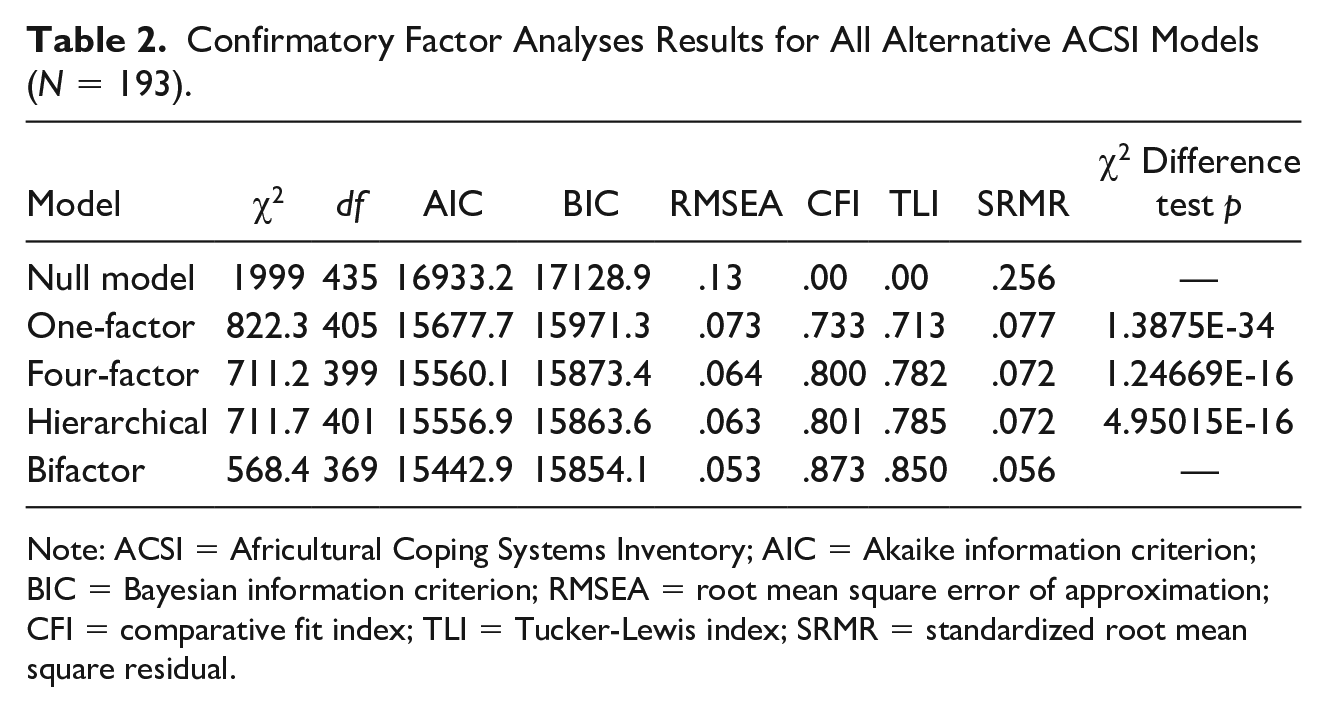
Note: ACSI = Africultural Coping Systems Inventory; AIC = Akaike information criterion; BIC = Bayesian information criterion; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; SRMR = standardized root mean square residual.
Across all models, ACSI item scores revealed high levels of residual variance, meaning that much of their variance was not explained by any latent factor. In the best fitting model, 9 of the 30 items had less than 30% of their total variance explained. Although the items loaded significantly onto at least one latent variable, the majority of their variance went unexplained. This pattern is likely the reason for the misfit of all models to the data. Information about factor coefficients, residual variance, and R2, for the bifactor model can be found in Table 3.
Factor Coefficients of the Africultural Coping Systems Inventory Bifactor Model (N = 193).
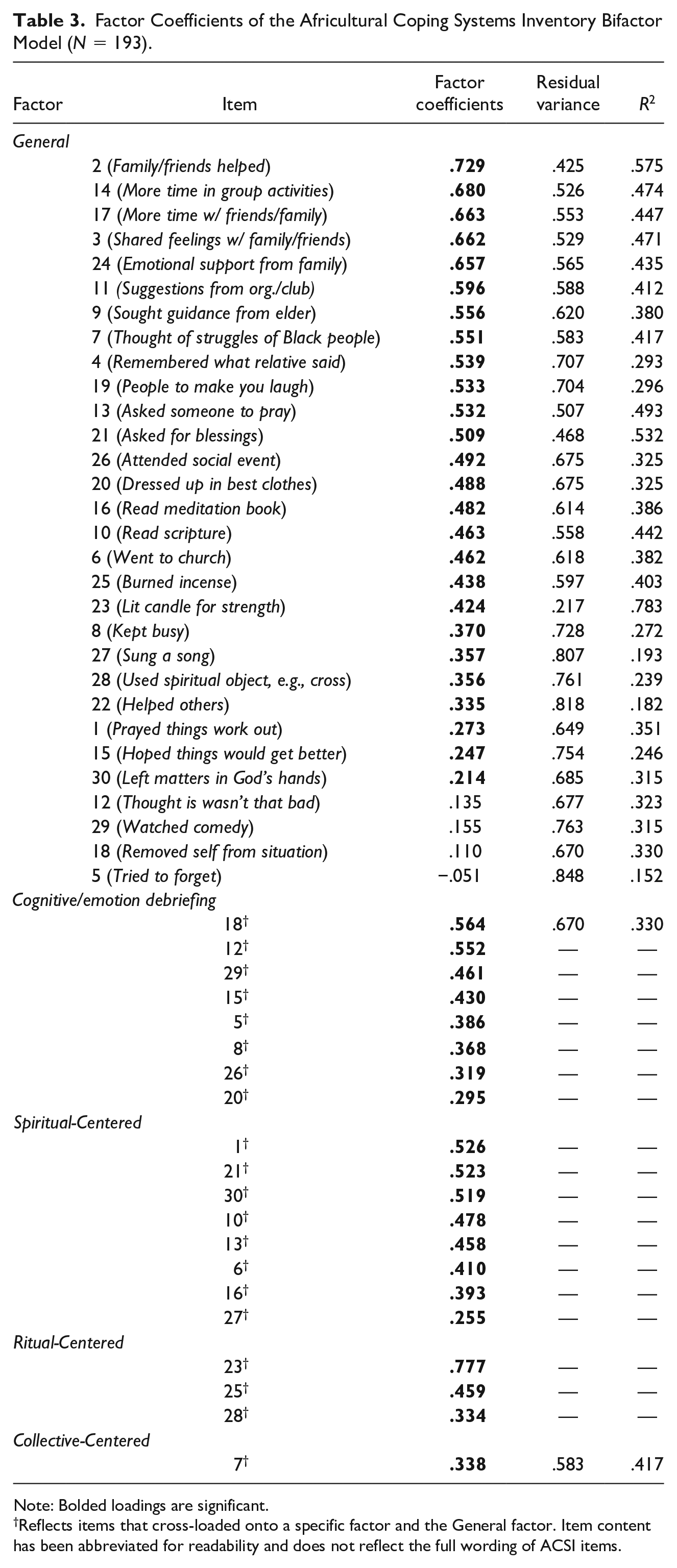
Note: Bolded loadings are significant.
Reflects items that cross-loaded onto a specific factor and the General factor. Item content has been abbreviated for readability and does not reflect the full wording of ACSI items.
Reliability
We calculated the internal consistency for each subscale: Cognitive and Emotional Debriefing (α = .76), Collective-Centered Coping (α = .80), Spiritual-Centered Coping (α = .81), and Ritual-Centered Coping (α = .70). Consistent with our hypothesis that ACSI scores for the subscales would exhibit good internal consistency (α ≥ .70), all Cronbach’s alpha coefficients fell between .70 ≤ α < .90, indicating acceptable to good internal consistency. Also, we assessed other indices of reliability given that Cronbach’s alpha coefficients can be less reliable for bifactor models (Rodriguez et al., 2016). Coefficient omega levels, which account for the strength of the association between factor items (McDonald, 1999; Revelle & Zinbarg, 2009), ranged from .72 to .92 (M = .81). Values in this range typically suggest a highly reliable multidimensional composite of the scores (Watkins, 2017), which could mean that subscale scores reflected the combination of general Africultural coping and the four specific factors. However, the exactness of the total and subscale scores cannot be disentangled due to the combination of general and specific variance in the computation of ω (Watkins, 2017).
Omega hierarchical values were assessed given that they solely reflect the variance of the general factor, and these values were more widely spread (ωH = .09-.77, M = .42). Although there are no specific guidelines for omega coefficients, high ωH coefficients suggested that the general factor was the main source of systematic variance in the test score, whereas low ωH coefficients indicated that specific factors explained the bulk of reliable variance (Rodriquez et al., 2016). Overall, the coefficient values in this study indicated that although specific factors moderately accounted for a proportion of the variance, a higher proportion was explained by the general coping factor. Thus, these reliability estimates indicated that the general factor was the most internally consistent, whereas the four subscale factors varied more considerably. Internal consistency coefficients for the ACSI subscale scores can be found in Table 4.
Descriptive Statistics and Internal Consistency Coefficients for Africultural Coping Subscales (N = 193).
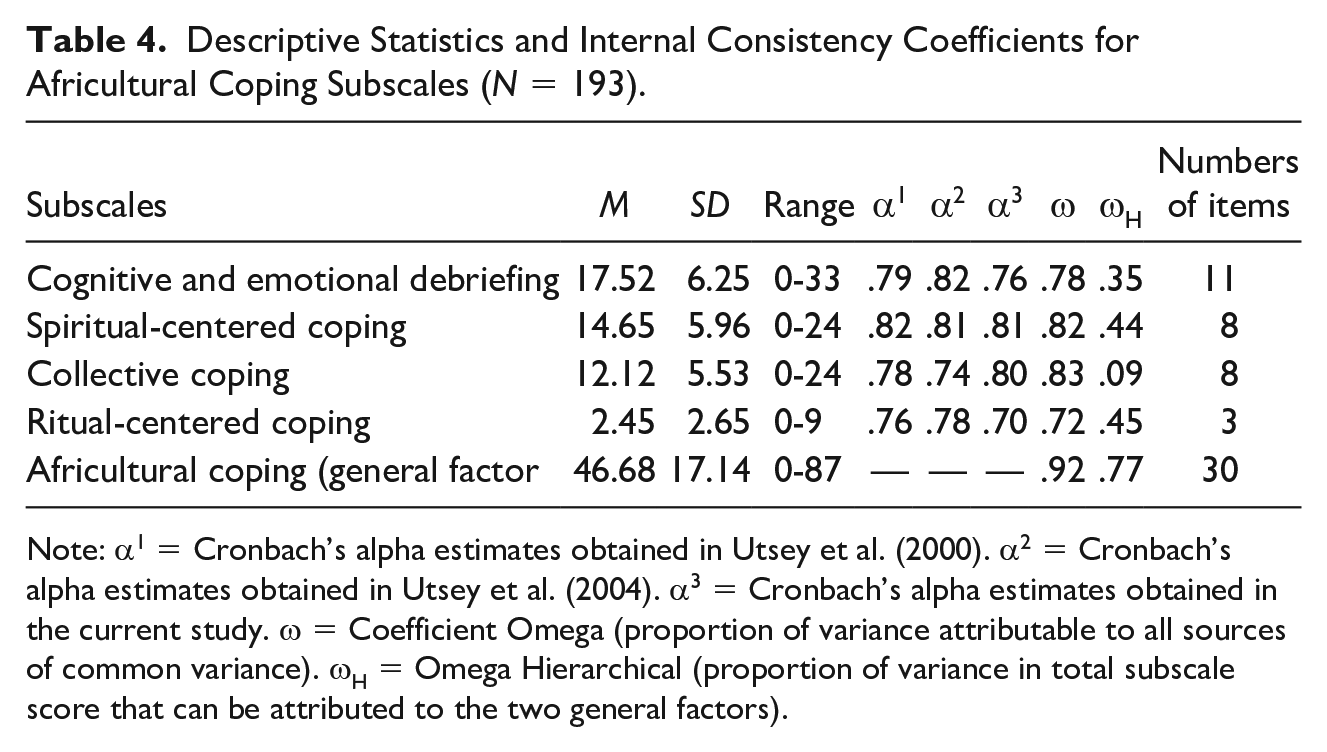
Note: α1 = Cronbach’s alpha estimates obtained in Utsey et al. (2000). α2 = Cronbach’s alpha estimates obtained in Utsey et al. (2004). α3 = Cronbach’s alpha estimates obtained in the current study. ω = Coefficient Omega (proportion of variance attributable to all sources of common variance). ωH = Omega Hierarchical (proportion of variance in total subscale score that can be attributed to the two general factors).
Validity
In addition to model fit and reliability, we assessed this measure’s concurrent validity by measuring its associations with current psychological symptomatology, specifically alcohol abuse, depressive symptoms, and suicidal ideation. Because the bifactor model supported a general factor and specific factors, we investigated the relations among both the general factor and the specific factors on the outcomes of interest. This analysis provided information about if the specific factors differentially predicted outcomes beyond the shared variance with the general factor. We found that neither the general factor nor specific factors were related to alcohol abuse, as had been expected. Also, none of the specific factors were related to depressive symptoms or suicidal ideation as expected. However, as predicted the general factor was negatively associated with depressive symptoms (r = −.21, p = .02) and suicidal ideation (r = −.25, p < .001). Thus, higher levels of general Africultural coping was associated with decreased depressive and suicidal symptomatology in this sample. These results can be found in Table 5.
Intercorrelation Between ACSI Specific and General Factors and Health Symptoms (N = 193).
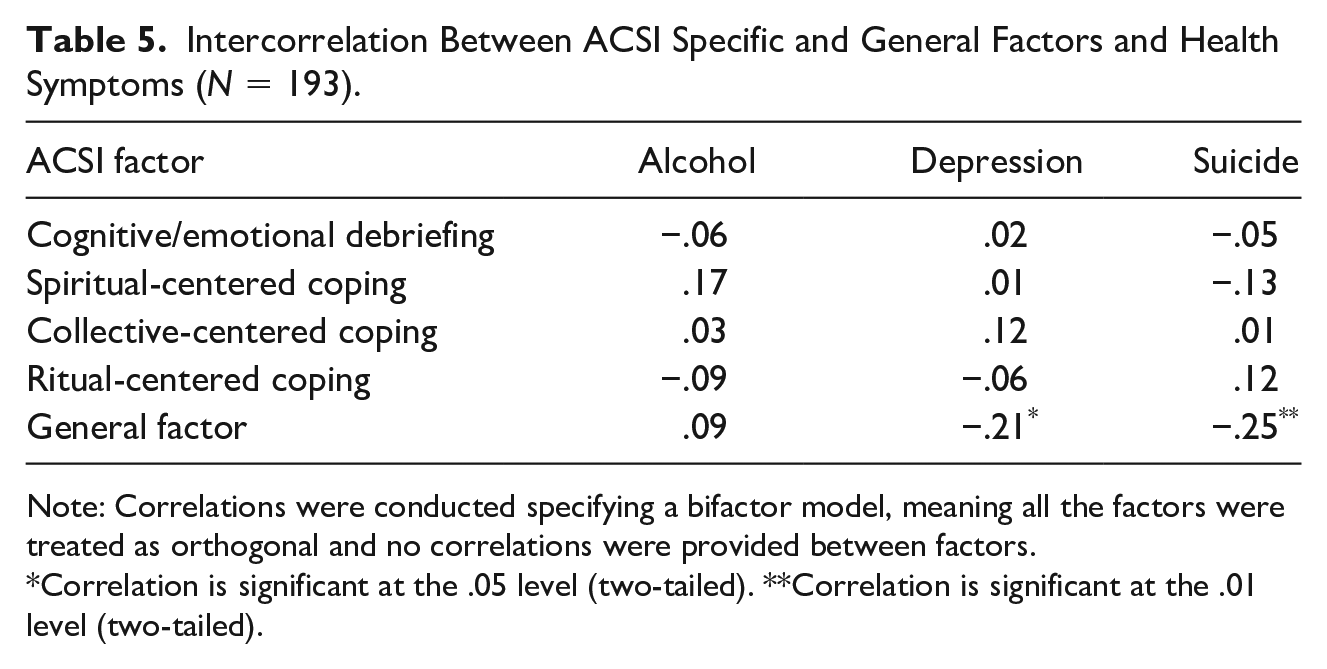
Note: Correlations were conducted specifying a bifactor model, meaning all the factors were treated as orthogonal and no correlations were provided between factors.
Correlation is significant at the .05 level (two-tailed). **Correlation is significant at the .01 level (two-tailed).
Discussion
This study was the first to investigate the psychometric properties of a culture-specific coping measure, the ACSI, in a clinical sample of African American women. This study, which included low-income African American women with past interpersonal trauma and suicide attempts, extends knowledge of the relevance of this measure for different subgroups of African descent persons and attends to the meaningful heterogeneity that exists among this population. Furthermore, the focus on African American adult women with clinically elevated symptomatology is a noteworthy feature as they represent a subpopulation that may particularly benefit from the use of culturally specific methods of coping (Warren-Findlow & Issel, 2010). Overall, results revealed that none of the models were acceptable, but the bifactor model had the best fit to the data relative to all other models. The bifactor model suggested the presence of a general Africultural coping factor along with well-defined specific factors for cognitive and emotional debriefing, spiritual-centered coping, and ritual-centered coping. In contrast, almost all of the collective-centered coping items loaded onto the general factor and did not contribute uniquely to the conceptualization of Africultural coping. Yet given that the bifactor model only evidenced acceptable model fit on two of four fit indices, these findings must be interpreted with caution. Also, high levels of internal consistency of the scores were obtained for the general factor and each of the ACSI’s specific factors. With regard to concurrent validity, only the general factor was significantly related to depressive symptoms and suicidal ideation. Thus, in this clinically distressed sample of African American women, it appears that global reliance on culturally relevant coping rather than utilization of any specific form of Africultural coping, is associated with lower levels of psychopathology. However, the positive gains of Africultural coping did not extend to alcohol abuse in this sample.
The first psychometric property examined was the factor structure of the ACSI scores. Because the utilization of the bifactor model was a novel aspect of the current study, we did not have a specific a priori hypothesis about which model would fit best. We found that none of the factor structures tested for the ACSI in this clinical sample of African American women were acceptable. The worse fit was the one-factor model and the best fit was the bifactor model, with two out of four fit indices being satisfactory. The four-factor and hierarchical models were substantially lower in fit than the bifactor model, indicating that a four-factor and hierarchical approach do not best capture the conceptualization of Africultural coping. The bifactor model indicated that each of the four dimensions of Africultural coping relate at the general construct level (i.e., culture-specific coping). Also, in contrast to previous research in which a four-factor model revealed the presence of four distinct factors, the bifactor model supported three distinct factors (i.e., Cognitive and Emotional Debriefing, Spiritual-Centered Coping, and Ritual-Centered Coping) that accounted for unique variance alongside a commonly shared, general factor that accounts for shared variance. Moreover, the fit indices of the bifactor model differ slightly from the indices found in Utsey et al. (2004); although the RMSEA of .053 in the current study was comparable to the RMSEA value (i.e., .05) found in Utsey et al. (2004), our CFI value of .873 was less than Utsey’s reported CFI of .93 (i.e., Utsey did not report TLI and SRMR values). These differences may be due to sampling variability or may highlight possible limitations of the ACSI. Either way, additional factor analytic research on the ACSI is warranted.
Despite the fact that the fit of the bifactor model was not adequate overall, the bifactor model may have potential given its better fit than the other models and the fact that bifactor approaches are recommended when evaluating psychology-related constructs (Reise et al., 2010). Specifically, additional studies can build on these findings to revise and improve the scale for use. For instance, the findings from the current study demonstrated issues with some ACSI items that may be contributing to model fit concerns. For instance, Items 8 (“To keep from thinking about the situation I found other things to keep me busy:” Cognitive and Emotional Debriefing), 22 (“Read passage from a daily meditation book:” Spiritual-Centered Coping), 27 (“Sought out people I thought would make me laugh:” Cognitive and Emotional Debriefing), and 28 (“Got dressed up in my best clothing:” Cognitive and Emotional Debriefing) had factor coefficients less than .40 on both the general factor and their respective specific factors. Also, most items had high levels of residual variance (greater than or equal to .50), indicating that considerable amounts of their variance were not explained by any latent factor, which could also have contributed to model misfit. Thus, revising or deleting these items may improve model fit. Last, future research is needed to assess if the absence of a specific Collective-Centered Coping factor is a function of a bifactor analysis of ACSI scores or the function of the clinical nature of the sample. For instance, African American adults with elevated levels of depressive symptoms and/or suicidal ideation have endorsed lower levels of social support (Kaslow et al., 2005). Thus, individuals’ symptomatology could have influenced their endorsement of collective coping practices and thus influenced this subscale’s factor analytic performance in the current study.
The second psychometric property that was evaluated was internal consistency. We expected that subscale scores would exhibit good internal consistency (α ≥ .70) in this clinical sample of African American women, and this hypothesis was supported. In the current investigation, the internal consistency coefficients ranged from adequate to good for all ACSI subscale scores. These estimates aligned with previous studies (Utsey et al., 2000; Utsey, Bolden, Lanier, et al., 2007). Additionally, both the omega coefficients and omega hierarchical coefficients, the indices used for internal consistency in bifactor models, indicated that variance was explained by both the general factor and the specific factors. Although the exactness of the variance attributed to either the general or specific factors cannot be disentangled (Watkins, 2017), omega coefficients support the multidimensionality of the ACSI scores, which is consistent with its conceptualization as a multidimensional construct. Yet, omega hierarchical coefficients suggested that the general factor is the most internally consistent compared with the specific factors, suggesting that the general factor raw score is likely to be a more appropriate measure of its respective factor relative to the specific factors. Consistent with recommendations noted above, item revision and/or deletion could improve the extent to which specific factor raw scores serve as reliable measures of their particular factors. Moreover, in future studies, test-retest reliability of the scores should be assessed to ascertain if Africultural coping is more trait-like versus state-like; trait-like constructs typically remain stable over time, whereas the opposite is true for state-like constructs (Schmidt et al., 2003). Although coping strategies may vary across time points given changing stress levels, consistent use of Africultural coping, even during times of low stress, may be vital in moving from crisis and stress intervention to crisis and stress prevention. Thus, it is theoretically and empirically advantageous to consider if individuals consistently use Africultural coping and to evaluate if consistent use aids optimal health.
The third aspect of the ACSI’s psychometric properties we focused on pertained to its concurrent validity in relation to behavioral health. Specifically, because the ACSI reflects adaptive coping in response to stress, we anticipated that higher levels of Africultural coping would inversely relate to alcohol abuse, depressive symptoms, and suicidal ideation. This hypothesis was partially supported, and this study yielded new findings regarding the relations between the ACSI scores and behavioral health outcomes in a clinical sample. Although the specific factors did not predict current psychopathology, higher scores on the general factor were associated with lower levels of depressive symptoms and suicidal ideation. This finding contrasts recent results with a sample of African American women college students in which specific forms of Africultural coping styles (spiritual-centered, cognitive-emotional coping) inversely related to levels of suicidal ideation and behavior (Morrison & Hopkins, 2019). One possible reason for this difference could be the nature of the sample. The sample examined by Morrison and Hopkins (2019) included 87% of people who reported no suicidal ideations within the last year and 62% of whom reported no suicidal ideations during their lifetime, whereas everyone in the current sample had a suicide attempt in the past year, with many having more than one suicide attempt in their lifetime. Therefore, spiritual-centered and cognitive-emotional coping may be inversely related to suicidal ideation and behavior among people already at minimal risk for suicidal thoughts and behaviors but unrelated to suicide among those at greater risk. Despite these differences, findings from the current study highlight the psychological benefits of drawing on Africultural coping in the face of extreme distress for high-risk African American women.
In addition, culture-specific coping may facilitate African Americans’ efforts to reclaim peace, harmony, and emotional and spiritual balance (Myers & Speight, 2010; Utsey et al., 2000). As a result, future studies should examine the relations among the ACSI scores and positive psychology-focused variables (Seligman, 2019). One factor that fits within a positive psychology framework is suicide resilience, or the ability to utilize personal and external supports to forego suicidal behaviors when confronted with thoughts of suicide (Osman et al., 2004). One study with an African American clinical sample supported relations among suicide resilience and intrapersonal strengths, like self-efficacy and spiritual well-being (Kapoor et al., 2018). Thus, future studies should assess if Africultural coping nurtures suicide resilience and reduces suicidal gestures among African American women at risk for suicide.
Limitations and Future Directions
The findings from the current study contribute to the growing understanding of the psychometric properties of the ACSI across various African American samples; yet, several limitations are worth noting. First, limited demographic diversity (e.g., lack of socioeconomic and gender diversity) hinders inferences about the findings’ external validity and generalizability. Studies that focus on a variety of clinical versus nonclinical samples as well as that include demographically diverse African Americans are critical, especially given that social positions and contexts (e.g., socioeconomic status, region) can influence coping styles (Hudson et al., 2016). Such studies can include the examination of the psychometrics of the ACSI in additional African American women samples as well as among African American men; such investigations can advance the assessment of culturally relevant protective factors in these samples (Gayman et al., 2018). In particular, African American men face unique barriers, like masculinity norms, that could thwart the use of Africultural coping (Hudson et al., 2016; Hudson et al., 2018). Second, the data were cross-sectional, and we cannot infer whether Africultural coping influences psychological symptoms or whether psychological symptoms contribute to the use of Africultural coping strategies. Third, all questionnaires were administered in the same order, which could have produced an order effect. Order effects can inadvertently influence patterns and styles of responding to questionnaire items, ultimately undermining the validity of survey data. Fourth, we did not examine other culturally relevant coping styles, like John Henryism and Strong Black Woman (SBW) schema. John Henryism promotes high-effort coping in response to discrimination (James, 1994) and has been linked to elevated blood pressure among African Americans and lower levels of depressive symptoms in African American women (Bronder et al., 2013; Subramanyam et al., 2013). The SBW schema, an intersectional coping style that fosters emotional suppression and self-reliance in African American women, has been associated with disordered eating, depressive symptoms, and low perceived support (Abrams et al., 2019; Harrington et al., 2010; Watson-Singleton, 2017). As a result, studies are needed to investigate if John Henryism and SBW schema are related to the ACSI and if they differentially impact outcomes among African Americans. Fourth, data were collected over a 10-year span; due to this extensive passage of time, participants recruited toward the end of the study could have differed from participants recruited at the study’s inception. Therefore, data collected within a narrower window are needed to replicate these findings to ensure validity.
Clinical-Counseling Implications
It is imperative to establish the validity of the ACSI with clinical samples in order to fully elucidate its implications in clinical settings. Yet using the measure as an interview or counseling tool could enrich assessment, conceptualization, and treatment. With regard to assessment, providers can use the ACSI to collect information about individuals’ Africultural coping. Higher scores on coping can be treated as a client strength, whereas lower scores on coping dimensions may illuminate potential opportunity for treatment. In addition, use of the ACSI can help put clients’ beliefs and behaviors in context. For instance, adequately understanding clients’ use of spiritual- and ritual-centered practices can protect against overdiagnosing some disorders (e.g., schizophrenia; Gurak et al., 2018), whereas knowledge of cognitive and emotional debriefing patterns, like the tendency to minimize the expression of distress, can protect against underdiagnosis of other disorders (e.g., major depressive disorder; Weaver et al., 2015). Furthermore, collecting client data via the ACSI can promote culturally relevant case conceptualizations that situate clients’ coping strategies within sociocultural contexts. This qualitative approach may be helpful in understanding the usefulness of the scale as well as how the items operate with a clinical population. Moreover, using the ACSI during assessment and conceptualization can be used to optimize interventions with African American women by bolstering culturally normative coping strategies. Taken together, a more nuanced consideration and integration of Africultural coping in clinical and counseling settings can enhance how African American women’s psychological experiences are understood and treated.
Supplemental Material
ACSI_Correlation_Matrix – Supplemental material for Africultural Coping Systems Inventory: Psychometrics in a Clinical Sample of African American Women
Supplemental material, ACSI_Correlation_Matrix for Africultural Coping Systems Inventory: Psychometrics in a Clinical Sample of African American Women by Natalie N. Watson-Singleton, Devon LoParo, Yara Mekawi, Joya N. Hampton-Anderson and Nadine J. Kaslow in Journal of Black Psychology
Supplemental Material
Descriptives_of_ACSI – Supplemental material for Africultural Coping Systems Inventory: Psychometrics in a Clinical Sample of African American Women
Supplemental material, Descriptives_of_ACSI for Africultural Coping Systems Inventory: Psychometrics in a Clinical Sample of African American Women by Natalie N. Watson-Singleton, Devon LoParo, Yara Mekawi, Joya N. Hampton-Anderson and Nadine J. Kaslow in Journal of Black Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute of Mental Health (1R01MH078002-01A2, Group interventions for abused, suicidal Black women) awarded to the last author (Kaslow). Joya Hampton-Anderson was supported by the AIM Youth Mental Health Foundation Clinical Science Fellowship during the writing of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.