
Abstract
Many leading hospitals and medical centers in the United States are located in large urban centers. This has meant that the post–World War II growth of the U.S. health care sector has been deeply intertwined with wider changes in the political economy of American cities. Through an examination of Boston’s Tufts-New England Medical Center (T-NEMC) and the surrounding Chinatown neighborhood, this article explores the implications of this relationship by assessing the spatial, economic, and community consequences of the growth of a major urban academic medical center. It treats the history of health care and health care policy as a key part of urban history, using the T-NEMC case to tell a larger story about the role of local and federal policy in transforming urban health care institutions.. T-NEMC deployed federal urban renewal and hospital construction programs to finance an ambitious expansion program designed to allow it to compete with Boston’s many prestigious medical centers. T-NEMC faced determined opposition from Chinatown residents who forged political alliances that helped them gain concessions from the medical center, including housing, schools, and health care and community centers—even as their neighborhood was transformed. Ultimately, T-NEMC’s larger strategy proved problematic. It took on excessive debt during the period of its expansion and then, in the 1990s, failed to form critical network alliances with other hospitals. The story of health care redevelopment in Boston thus proves to be deeply enmeshed in the changing political economy—and politics—of health care in the United States.
Throughout the recent debate over health care reform, pundits of all political persuasions frequently noted that the health care sector now accounts for nearly 18 percent of U.S. Gross Domestic Product. Most such observers, however, direct attention solely to characteristics of the health care system at the national level: fee-for-service medicine, tax exemptions for employer-provided health insurance, Medicare and Medicaid financing, and excessive costs and inferior quality compared with other nations. These issues are of critical importance, but this approach misses a central dimension of the health care sector’s significance, one which defines its role both in the lives of Americans and in the economy as a whole. This factor is the physical, spatial, and economic character of the sector as it exists in communities around the United States and, particularly, in large cities. Since World War II, the rapid expansion of the U.S. health care system has played an often determinative role in shaping the spatial organization of cities, defining the provision of urban public services, and not least, providing a primary source of jobs in many metropolitan areas. This has meant that the growth of the U.S. health care sector has been deeply intertwined with wider changes in the political economy of American cities.
By the end of the twentieth century, the “eds and meds” sector accounted for 34.7 percent of jobs in the nation’s twenty largest cities. Every one of these twenty cities had at least one hospital, college, or university among its top ten employers, and five of the cities had between four and six such institutions in their top ten. In many large cities, hospitals alone played a critical role as employers. Looking just at the mid-Atlantic region, hospitals accounted for six of the top ten private employers in Washington, D.C.; three of the top ten in Baltimore; and five of the top ten in both Philadelphia and Boston. 1 These statistics illuminate a broader trend: as manufacturing has declined in the United States, and particularly in cities, hospitals have increasingly replaced factories at the core of the urban economy. Such numbers alone, though, tend to obscure another dimension of this change: actions taken by the U.S. state enabled the physical expansion of urban health care institutions, and then played a crucial role in financing such institutions’ health care and research activities through both direct spending and indirect tax expenditures.
This study begins, then, with a simple premise: that in recent decades, health care policy has, in effect, also been urban policy. This is a point that has been lost amid the rancor of the health care debate. Like journalists and politicians, policy historians and social scientists have typically conceived of health care policy as a purely national issue, disconnected from either space or place. Policy scholars have carefully explored the development of the mixed, public–private health care sector in the United States, as well as the failure of the resulting system to achieve either universal coverage or effective cost control. Yet almost none have recognized the place-based, urban dimensions of health care, or noticed that the evolution of the U.S. health care system is as much a part of urban history as it is of the wider history of American political development.
Urban historians and social scientists have done little better, offering extensive studies of urban community development efforts but ignoring the implications of the massive medical institutions that have grown up in most major U.S. cities. Such historical neglect merely inverts the health policy experts’ blindness to the urban implications of health care. In turn, existing historical scholarship on hospitals tends to focus on their role in the history of medicine, rather than on their function as urban institutions. 2 The result is that we know relatively little about the details of how the urban health care sector arose or of how its emergence shaped the spatial, economic, and political character of cities.
The barriers between urban history and health care history can be removed by situating the emergence of the urban health care sector, and urban hospitals and medical centers in particular, amid both the changing political economy of U.S. cities and the wider growth of health care as a major component of the national economy during the postwar decades. This study offers a preliminary attempt at such analysis. After a brief assessment of federal policies that have shaped and facilitated hospital growth, it moves to a local frame through an examination of Boston’s Tufts-New England Medical Center (T-NEMC) and the surrounding Chinatown neighborhood. Boston has long been one of the nation’s leading urban centers of medical treatment, research, and education, and in the final decades of the twentieth century, it become a city that was in many ways anchored by its urban medical institutions. By exploring the spatial, economic, and community consequences of the growth of a major academic medical center in such an urban setting, this study thus treats the history of health care and health care policy as a key part of urban history. It finds that hospital expansion in Boston, while linked to federal policies and shaped by the needs of individual institutions, helped to build a new urban political economic order: the hospital city. Health care institutions such as the T-NEMC helped to reshape the local, regional, and even national economy while also contributing to the transformation of urban communities that were already undergoing rapid economic, demographic, and cultural change. By the 1970s, however, this transformative role increasingly came into conflict with the imperative to control the growth of costs within the health care system.
Hospitals and Federal Policy: Hill-Burton, Urban Renewal, and Federal Housing Administration (FHA) Mortgage Insurance
Five federal programs contributed to the expansion and modernization of urban hospitals during the post–World War II period, three of them directly and two indirectly. The direct policies included the Hill-Burton loan and grant program, the urban renewal program, and the FHA’s hospital mortgage insurance program. The indirect policy area consisted of the Medicare and Medicaid programs, which reshaped hospitals’ financing and operational functions after 1965. 3 Of these programs, only urban renewal was explicitly conceived of as an urban policy. Yet all five created intersections between urban hospitals’ roles as providers of medical care—especially for the urban poor—and their increasing importance as anchor institutions in postindustrial cities. It is these intersections that blur distinctions between policy areas to the point where the conclusion can be drawn that health care policy has operated as a critical but largely unrecognized form of urban policy in the United States.
Hill-Burton is the most widely recognized but—for large cities, at least—the least important of these federal programs. Passed in 1946 as the Hospital Survey and Construction Act, the Hill-Burton program was the only part of Harry Truman’s 1945 national health care proposal that became law. 4 The program primarily offered federal matching grants for the construction of new hospitals and nursing homes. From 1947 to 1971, it allocated $3.7 billion for hospital construction, which helped support approximately 30 percent of all such projects in the United States. As a result of the program’s 2-1 federal–local matching requirement, this covered about 10 percent of total construction costs. Initially, however, Hill-Burton focused resources on areas that lacked hospital facilities and did not make grants to regions with an average of more than 4.5 hospital beds for every 1,000 residents. Many larger cities, which already had existing hospitals, exceeded this cap. This meant that the bulk of Hill-Burton money went to small communities and rural areas rather than cities. Cities with populations greater than 250,000 received only about 13.3 percent of Hill-Burton funds, despite having 22 percent of the total U.S. population in the 1960 Census. This disparity declined slightly after a 1964 amendment permitted the program to make grants specifically for the modernization of existing, outmoded hospitals regardless of the per capita bed ceiling. Although such facilities were common in central cities, the urban–rural gap remained. As late as 1968-1970, larger cities still received only 18.1 percent of Hill-Burton funds. 5 Even with the funding disparity, 34.5 percent of the total inpatient beds the program funded were located in central cities. 6 Still, while Hill-Burton contributed to the emergence of the hospital as a new form of urban anchor, other federal programs played a more significant part in this process.
Although urban renewal contributed less than Hill-Burton to overall hospital growth in the United States, it would prove more important for the urban hospital sector. Scholars have long recognized that urban renewal redefined American cities during the postwar period, usually for the worse. Most studies have focused on how urban renewal destroyed intact, often minority neighborhoods, displaced residents, exacerbated segregation, and facilitated the expansion of high-end service industries even as manufacturing declined in the central cores of U.S. cities. Urban institutions such as universities and hospitals have frequently been identified as among the leading contributors to such negative consequences. 7 The basic fact of such institutions’ participation in urban renewal reflected tensions over core purposes that had been built into the program from its inception.
The Housing Act of 1949, which provided the legislative basis for the program, explicitly stated that its purpose was to provide “a decent home and a suitable living environment for every American family.” To gain the support, or at least the acquiescence, of the urban business and real estate interests who were well represented in Congress, advocates of low-income housing had to tie this goal to the related but not identical objective of clearing “blighted” areas from the urban core. As a result, urban renewal (known before 1954 as “urban redevelopment”) offered local governments a federal “write-down” subsidy that covered two-thirds of the local cost of assembling and clearing blighted land that could then be made available for redevelopment. This write-down was intended to bring the effective costs of the project into line with the local market rate at which the land could be resold for development. The legislation also required that projects merely be “predominantly residential.” This language opened the possibility of including commercial and institutional developments along with housing as part of urban renewal projects. 8
Amendments to the legislation in 1954 further loosened the constraints on nonresidential components of urban renewal. By the late 1950s, universities and hospitals around the United States began to take advantage of the federal urban renewal write-down to undertake expansions of urban campuses and medical facilities.
9
After 1959, however, linking institutional expansion to urban renewal became far simpler. Under Section 112 of the 1959 amendments to the housing act, Congress made universities eligible for urban renewal funds with no requirement that such projects be linked to housing. Two years later, hospitals received the same privilege at the request of the American Hospital Association. Julian Levi, who oversaw an early urban campus expansion program at the University of Chicago and served as a primary drafter of Section 112, explained to the House Subcommittee on Housing that universities could not
live with the 51-percent residential requirement . . . because what we need are campus facilities . . . you can’t because the moment you try to use the urban renewal tool, you are confronted with the fact that your project isn’t eligible and the only way you can make it eligible is to put housing back; and if you put housing back, you defeat the whole purpose of the operation.
10
Levi’s comment about “the whole purpose of the operation” reflects the institutions’ effort to shift the core functions of urban renewal further away from its original, if always nominal, housing goal and toward an explicit emphasis on rebuilding cities through institutional expansion.
Section 112 had one other important feature. It allowed cities to claim any expenditures made by universities or hospitals for urban renewal–related purposes as “grants-in-aid” that counted toward the required local contribution to the 2-1 federal–local matching grant ratio. If those grants-in-aid exceeded the necessary local expenditure, the federal government would provide credits of equal value toward ongoing or future urban renewal projects in the city. 11 This did two things. First, it created an incentive for cities to expand their institutional urban renewal programs to reduce immediate local costs (as the institutions would make the expenditures) while also generating subsidies for the city’s overall urban renewal program. By 1961, officials with the Urban Renewal Administration even became concerned that some local redevelopment authorities had come to view Section 112 as a way “to undertake these projects without local contribution.” 12 Second, it erased whatever weak distinction still remained between public and private in urban renewal and, more broadly, in the economics of urban land. Private institutional purposes, under this conception, were presumed to be inseparable from the public good. Over the following decade, this unexamined assumption would drive urban hospital expansion programs in the United States. Despite their broad implications, these changes to the Housing Act generated little controversy, and Congress passed the amendment without debate. 13
Congress may not have noticed what it was doing, but urban political and institutional leaders certainly did. By 1964, the Housing and Home Finance Agency (HHFA) reported that 154 urban renewal projects around the United States, involving 120 colleges and universities and seventy-five hospitals, had already taken advantage of Section 112’s institutional provisions. 14 This included both major urban medical centers such as the Detroit Medical Center and Baltimore’s Johns Hopkins Hospital as well as smaller institutions such as Tuscaloosa Druid City Hospital and Des Moines Mercy Hospital. 15 Neither HHFA nor later the Department of Housing and Urban Development (HUD) compiled detailed information about such projects, but a 1964 study of Boston by Julian Levi demonstrated that the existing plans of colleges, universities, and hospitals in that city alone could generate almost $31.7 million in Section 112 credits. Additional projects would generate even more. 16
Both Hill-Burton and urban renewal involved various forms of direct federal expenditures to subsidize construction. By the late 1960s, however, hospitals increasingly began to finance a greater percentage of construction costs through debt rather than by raising capital. 17 This led to two significant shifts in federal policy, which in turn served to reinforce the debt trend. First, Congress added a Hill-Burton loan program in 1970—previously Hill-Burton had provided only grants—and then transitioned the entire Hill-Burton operation to loans four years later. Second, the federal government began to guarantee hospital mortgages. The role of the FHA’s home mortgage insurance program in promoting suburbanization in the post–World War II United States is well known. Yet few historians or policy scholars recognize that, beginning in 1969, the FHA also provided mortgage insurance for hospitals. Just as in housing, the availability of federal mortgage insurance reduces the risk to a lender in the event that a hospital defaults on its loan. This lower risk means that the lender will offer the loan at a lower interest rate, which significantly reduces the cost of credit to the borrower and, in turn, the overall cost of a project.
Authorized by Section 242 of the Housing and Urban Development Act of 1968, this program remains in operation today (in slightly modified form). As of January 2010, it had guaranteed $15.7 billion of hospital mortgages. In contrast to Hill-Burton, Section 242 has been a heavily urban program. Approximately $7.48 billion of the guarantees have gone to cities that ranked among the fifty largest in the United States in the previous census. Many additional guarantees have gone to smaller but still distinctly urban places, as well as the suburbs of major cities. Until recently, it has also been heavily oriented toward the Northeast and Midwest. New York City alone has secured more than a third of the total guarantees, or $5.7 billion, far more than any other city. If a number of very large loan guarantees undertaken since 2005 are excluded, the remaining cities in the top ten recipients include Buffalo, Boston, Jersey City, Philadelphia, Patterson, Detroit, Chicago, and Atlantic City, with only Miami, in sixth position, located in the Sunbelt. 18 Although the program has guaranteed only a relatively small portion of overall U.S. hospital construction during this period—about 4.5 percent of total private hospital construction—its role in these urban areas has been far more significant. 19
These outlines of key federal hospital aid programs merely sketch the core structure of public policy in this area. They capture little of how these programs actually worked in U.S. cities, or of what the “on-the-ground” impact of hospital expansion has actually been in urban communities. As a result, the best means to assess the wider relationships between these policies and the growth of the urban health care sector is through a case study of the experience of a major urban medical center—the Tufts-New England Medical Center (T-NEMC), located in Boston’s South Cove neighborhood. Since the 1950s, T-NEMC has interacted with each of the major federal policies that have facilitated the expansion of urban hospitals. It has also frequently come into conflict with residents of the surrounding South Cove community of Chinatown. As such, it provides a potential archetype for how federal policies have facilitated urban hospital expansion. Boston itself is an important element in this choice of case studies, as it provides a prototype of the new “health care” city posited by this article. Even before World War II, Boston underwent a dramatic industrial decline, but emerged as a leading regional and national health care center with one of the highest rates of health care–related employment in the United States. The city thus offers an example of both the potential benefits and the potential dangers posed by hospitals and academic medical centers acting in the role of urban anchor.
Public Policy and the Academic Medical Center
During the early nineteenth century, Boston residents filled in tidal flats along both sides of the “neck,” a narrow isthmus that connected the city of Boston to Roxbury on the mainland. The filled area on the south side of the neck retained the name it had borne when still a body of water: the South Cove. In the ensuing decades, the South Cove filled with neighborhoods of three- and four-story residential buildings, which underwent waves of immigrant succession. By the 1950s, pockets of older Irish, Lebanese, and Syrian communities remained in the South Cove, but the area had become the core of Boston’s Chinatown. Boston’s Chinese immigrant community had first formed in the area during the 1870s, but had remained small until after World War II. As other immigrant groups began to move to Boston’s suburbs and as the U.S. government relaxed immigration restrictions following the Chinese revolution, Chinatown gradually expanded through much of the South Cove neighborhood. 20 Although poor, the Chinese American community in the South Cove remained cohesive, with a strong sense of group identity and vibrant ethnic organizations and institutions. The neighborhood, however, also faced significant stresses. Most of its population was low income, it had rates of tuberculosis 11.5 times higher than the citywide average, and much of its housing stock had begun to deteriorate. Built of wooden frame construction, many of the South Cove’s older buildings rested on wooden piles driven deep into the mud below. Subject to subterranean tidal flows beneath the fill, these pilings had experienced decades of daily dry–wet cycles that had left many rotten and structurally unsound. 21
Furthermore, the South Cove had already been deeply affected by urban reconstruction efforts, as the new Central Artery highway and the Fitzgerald Expressway had sliced wide swaths of clearance along the South Cove’s southern and eastern edges. Between 1940 and 1960, these highways eliminated approximately 353 housing units in the area. 22 The highway projects caused massive displacement in Chinatown and led to significant overcrowding in the South Cove’s remaining residential structures. Much to the chagrin of mid-century planners, who preferred carefully zoned, clearly differentiated single-use districts, the South Cove also had a heterogeneous mix of commercial stores (including Boston’s main low-end furniture district), restaurants, and wholesaling and manufacturing facilities. Two of Boston’s major theaters, the Wilbur and the Metropolitan, sat along the South Cove’s northern edge on Kneeland Street. Throughout the area, dilapidated properties had been demolished by their owners and replaced by parking lots. The South Cove would clearly meet the Housing Act’s definition of “blight.” 23 (See Figure 1).
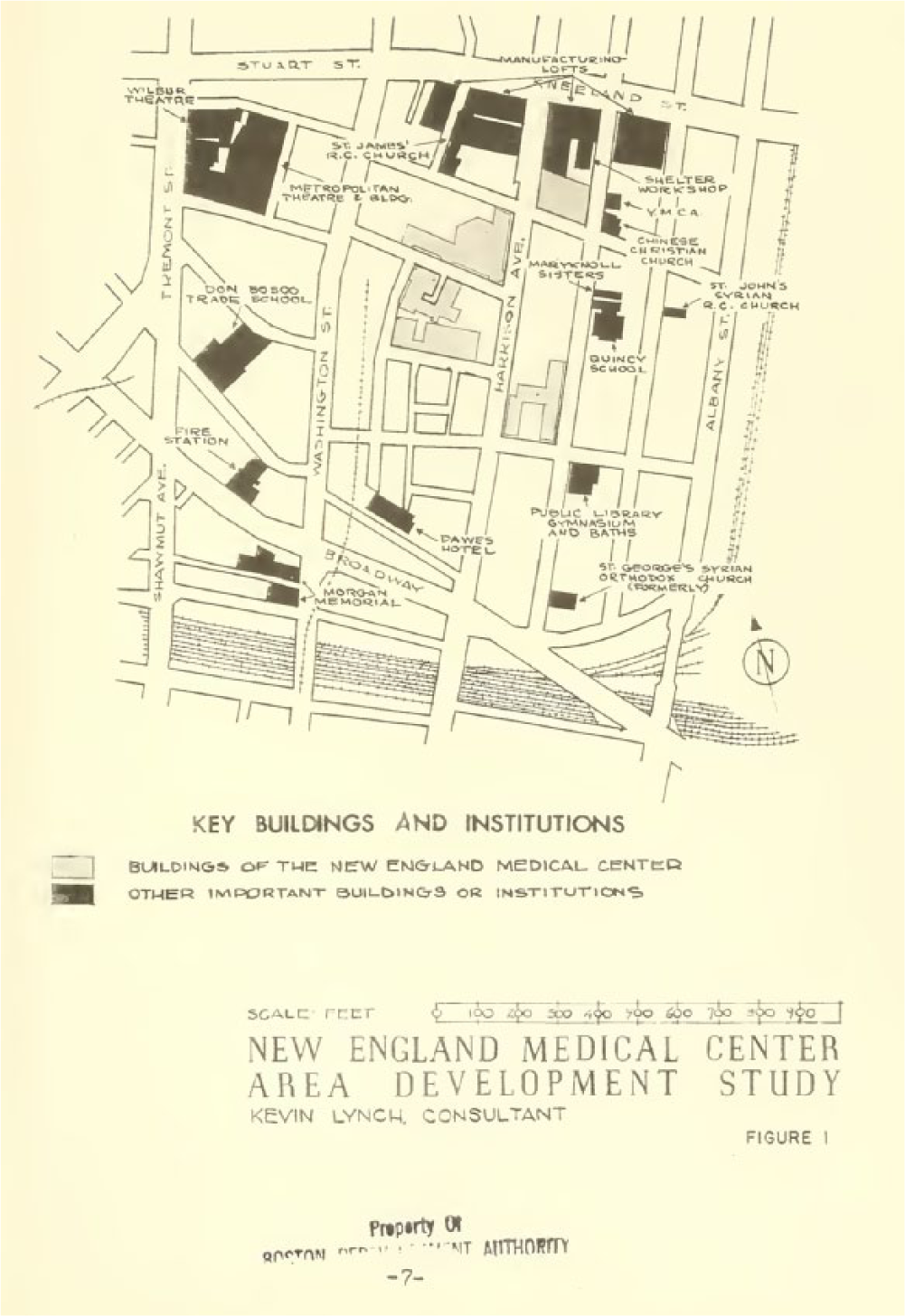
1955 map prepared by planning consultant Kevin Lynch, showing buildings of the New England Medical Center and other significant buildings in the South Cove/Chinatown neighborhood. The Massachusetts Turnpike and Central Artery-Fitzgerald Expressway would soon be built along the southern and eastern boundaries of the area.
Amid this district sat a major player in Boston’s medical community, the T-NEMC (referred to hereafter as “the medical center”). In the early 1960s, the medical center existed mainly as a coordinating body for four constituent institutions. These included the Boston Dispensary, an outpatient clinic that traced its origins to the colonial period (Sam Adams had been among its founders); the Boston Floating Hospital, a children’s hospital that until the 1920s existed as a ship-board hospital that sailed young patients out onto Boston Harbor in a quest to escape the supposedly ill humors of Boston’s unhealthy air; the New England Center Hospital, which provided specialty and diagnostic referrals around the region; and the Tufts University Medical and Dental School. 24
By the time Congress expanded Section 112 in 1961, the possibility that hospitals might employ urban renewal had already generated extensive discussions at the medical center. The Center’s main interests at the time consisted of achieving better coordination among its constituent medical institutions, delineating its overall mission more clearly, and obtaining space for the physical expansion necessary to become a major national medical center. Spread across multiple buildings of varying ages in the northern part of the South Cove, the medical center faced a mix of spatial constraints and opportunities. On its northern edge, manufacturing lofts, the two theaters, and an office building hemmed it in; on its western edge, a commercial district ran along Washington Street; to the south and east stood the older, low-income residential areas, including Chinatown on the east, with the expressways beyond in both directions. Parking lots were interspersed throughout the area, creating tempting openings for growth but too spread out to be easily assembled into large buildable properties. 25 Nonetheless, with the aim both of providing short-term parking for visitors and staff and of facilitating long-term expansion, the medical center had acquired empty lots as well as existing, occupied buildings. 26
Faced with these issues, medical center leaders at least theoretically considered moving to the Boston suburbs during the early- and mid-1950s. Opting for a less extreme course in 1955, they hired renowned city planning expert Kevin Lynch to study the situation and develop a tentative plan for future growth. At this point, the center’s leadership saw expansion directly into Chinatown as their easiest path.
Lynch, however, produced a planning document that was rather remarkable for its time. Although he urged the medical center to develop a master plan, coordinate all real estate acquisition among its constituent units, and push the city to designate the South Cove as a redevelopment area, Lynch also noted that the Chinese American community “is anchored here and has an obvious need for decent housing and adequate recreation in the vicinity.” As a result, he called for “cooperative endeavor with local groups . . . with the Chinese community in particular.” 27 Studying the center’s options for growth, Lynch suggested not a full-out push into the nearby residential areas—many of which he felt should be rebuilt for housing rather than institutional use—but instead that the center focuses its growth mostly to the west in the direction of downtown and the Boston Common. Its expansion should halt, though, at the major artery of Tremont Street, beyond which lay the Bay Village neighborhood in which a private rehabilitation effort had already begun—and seemed to be succeeding. 28
Lynch’s recommendations slowed the medical center’s march into Chinatown, while lack of progress in Boston’s overall urban renewal program constrained its broader options. In 1960, however, Boston elected John Collins as its new mayor. Collins had campaigned on a promise to launch an ambitious urban renewal program, and he soon recruited Edward Logue, the director of New Haven’s widely lauded but clearance-heavy urban renewal program, to supervise the new initiative. 29 For medical center administrators, the arrival of Logue in conjunction with the expansion of Section 112 marked a new opportunity to realize goals of institutional expansion and coordination.
In January 1961, the center hired planner Hermann H. Field as the director of a new Medical Center Planning Office. A graduate of the Harvard School of Design and a former campus planner at Cleveland’s Western Reserve University, Field had been imprisoned in communist Poland from 1949 to 1954 after being arrested while searching for his brother Noel Field, a former State Department official, wartime relief worker, and high-ranking Soviet spy who had been arrested as a suspected double agent in Hungary. 30 With his dramatic Cold War role behind him, Field settled into his role as an institutional planner for the T-NEMC.
Edward Logue directly encouraged the hiring of a planning director, as he had grown increasingly interested in the role that Boston’s medical and educational institutions could play in the city’s urban renewal program. 31 “In every project,” remarked a federal Urban Renewal Administration official after a 1961 field visit to Boston, “Logue wants a partner.” In particular, Logue wanted hospitals to acquire all properties necessary for their renewal programs directly so that their expenditures could be counted as local grants-in-aid that would generate Section 112 credits for the Boston Redevelopment Authority. In the summer of 1961, Logue commissioned Julian Levi, who in addition to orchestrating the University of Chicago’s expansion had been a primary architect of the 112 program, to conduct a survey of the potential 112 credits available to Boston’s many higher education and medical institutions. 32 Levi’s preliminary study convinced Logue that institutional property acquisition might generate enough credits for Boston “to finance its urban renewal program without local cash contributions.” 33 Such a financing structure would allow Logue to advance his program without having to ask local political leaders, or voters, for matching funds.
The benefits of this relationship flowed back to the institutions as well. In return for the generation of Section 112 credits through their property purchases, institutions such as T-NEMC gained three things: access to urban renewal write-downs of their acquisition costs, to city eminent domain powers for the acquisition of properties from recalcitrant property owners, and, finally, to city assistance in developing new parking facilities. Parking garages, in particular, could be financed through their own revenue generation capacity and would in turn produce additional in-kind noncash contribution credits for the Authority. 34
The need for such expanded parking facilities preoccupied hospital planners, in Boston and other cities, throughout the postwar decades. This focus reflected the growing centrality of the automobile in both American culture and public policy. The federally funded expressways that cut through the South Cove’s southern edge had a direct impact on neighborhood demolition, but the automobiles that these roads brought to the growing medical facilities required a place to park—leading to further demands on urban space in Chinatown and to a further impetus for cooperation between the medical center and the redevelopment authority. Reflecting this car-generated pressure, medical center physician-in-chief Dr. Samuel Proger observed at a meeting of the medical center’s executive committee that “many of the Medical Centers and Universities are now or are planning to erect garages because of the impossible situation of acquiring sufficient land for open parking.” 35 This “impossible situation” meant that medical institutions had a strong incentive to work with the redevelopment authority. Both nuanced (Section 112) and overt (the 1956 Interstate Highway Act) expressions of federal urban policy thus drove redevelopment decisions at the local level. Over the following decades, such policy structures contributed significantly to the physical and economic growth of Boston’s health care sector—and, specifically, to the expansion of its hospitals and academic medical centers.
Medical Center Planning and the Chinese Community
Hermann Field immediately undertook a detailed survey of the center’s options, as well as of conditions in the South Cove. 36 Effectively, Field’s planning office also completed much of the work necessary for the redevelopment authority to file a Survey and Planning Application for federal renewal planning funds. By the end of 1962, Field had also drafted a preliminary development plan for the medical center itself. Federal approval of these documents would allow the authority to gain access to nearly $1.5 million in Section 112 credits for previous medical center expenditures that could be applied to the adjoining New York Streets Urban Renewal Project. Levi’s survey, meanwhile, showed that as much as $3 million in additional credits might be available through a South Cove project due to expenditures that the medical center had made in the area during the 1950s and early 1960s. 37
These Section 112 credits proved critical. Upon arriving in Boston, Logue initially had not viewed the South Cove as a priority. If urban renewal were to proceed in the area at all, Logue envisioned it as an attachment to a nearby project focused on Boston’s downtown retail core. The downtown project, however, had temporarily stalled, blocking progress on the medical center’s plans and placing the South Cove 112 credits at risk because they could only be claimed if they had been made during the seven years preceding approval of a federal “Loan and Grant Contract” for an urban renewal area. 38 The fact that the soon-to-expire Section 112 credits could be applied to Logue and Collins’s ambitious and expensive plans for central Boston pushed the South Cove project forward as a top priority. In the summer of 1961, an Authority staff member who had been assigned to assist Julian Levi explained this to Field’s assistant Elliot Rothman: “He noted that we should not underplay or overplay our 112 credits. Logue needs them.” 39 Julian Levi himself played a critical part in convincing Logue to move forward, pressing him to take action before the credits were lost and urging him to either launch a project for the South Cove alone or join the area to the existing South End project, which, unlike the downtown project, seemed close to enactment. 40 Levi also made the related point that for Boston as a whole, the availability of the credits and the inclusion of related commercial and housing developments in the project would offset the property tax loss resulting from expansion of the tax-exempt Medical Center. 41
In late 1961, Logue agreed to proceed with the Survey and Planning Application for federal planning funds. This led directly toward the designation of the South Cove as an urban renewal area, and moved it, as Field reported to the medical center’s executive committee, “from a low to a high priority consideration” within the redevelopment authority. The authority in turn approved the medical center’s Development Plan in November 1962, followed by the Survey and Planning Application in December. 42
At this point, the Chinese American community balked. Before the Survey and Planning Application could be submitted to the HHFA, City Council had to approve it. This required a series of public hearings during the first months of 1963. At these hearings, community representatives from the Chinese Community Benevolent Association (CCBA; at the time, the leading community organization in the area) expressed opposition to any further medical center expansion into Chinatown. As a result, council proved hesitant to move forward. To break the impasse, Logue and Field negotiated an agreement with the CCBA that set aside specific tracts east of the medical center for low-income housing to be built by a new, community-controlled development corporation.
The agreement acknowledged that the Chinese community “has suffered severe dislocation and reduction in its land area,” and it specified that high-income housing could not be built in the Chinatown’s existing residential areas. It also required the redevelopment authority to consult with the CCBA over all aspects of the South Cove renewal plan, including the selection of developers. Perhaps most strikingly, it required the redevelopment authority to obtain the approval of both the CCBA and a newly formed community “Urban Renewal Committee” before it submitted the final urban renewal plan to either city or federal officials. All of these aspects of community input and control represented a significant departure from the reliance on top-down, authoritative expertise that had previously characterized urban renewal. With the agreement in place, City Council approved the Development Plan and the Survey and Planning Application on May 23. 43 After completing the lengthy federal review process, the application received HHFA approval in September 1964, and the formal urban renewal plan was completed in 1965. (See Figure 2). Field’s planning office, meanwhile, became a semipermanent part of the medical center—and of the wider apparatus of urban renewal in Boston. By 1967, Field oversaw a staff of twenty-eight and a $400,000 budget. 44

Aerial image, circa 1969, of the South Cove Urban Renewal (dashed white line) including the Tufts-New England Medical Center area (cross-hatched area) in relation to downtown Boston, the Prudential Center, Boston Common, and the Central Artery.
The experience with the Chinese American community’s objections, however, left Field with a new appreciation of the importance of working with the medical center’s neighbors. “Very commonly,” he told Architectural Forum in 1968, “the hospital is in the ambivalent position of treating the community’s sick while acting as if the community itself did not exist.” 45 While significant, Field’s insight should not be overstated. It did not extend to the medical center’s administration, and it did not produce a perfect process of community-institutional engagement as the urban renewal program proceeded over the following quarter century. Instead, it established the precedent, embedded in the 1963 agreement with the CCBA, that the Chinese American community would enter into both planning and political processes to defend its interests, and that its voice would be heard.
In part, such relationships reflected a larger shift in urban renewal policy in Boston, brought on by the unpopularity of massive clearance projects during the 1950s such as that in Boston’s West End. By the early 1960s, opposition to urban renewal in the Allston–Brighton and Charlestown neighborhoods raised the possibility that a political backlash against urban renewal might lead to the election of city officials hostile to Logue’s agenda. In an attempt to prevent this, Logue worked with the Ford Foundation’s Gray Areas program (an important precursor to the federal War on Poverty) to set up mechanisms for community participation in urban renewal. Although never fully successful in reconciling neighborhood interests with those of the redevelopment authority, the Gray Areas project nonetheless created a precedent for involving community groups in the urban renewal planning process and helps contextualize both the agreement with the CCBA and Hermann Field’s revelation about the value of neighborhood participation. 46
At times, the relationship between the medical center and the community reverted to the original pattern of confrontation followed by negotiation. During the late 1960s, a younger generation of Chinese American activists challenged not only the medical center and the redevelopment authority but also the established organizations of their own community such as the CCBA. In May of 1971, a group known as the Free Chinatown Committee circulated flyers charging that the medical center
has brought Chinatown to the edge of total destruction . . . this self-interest-seeking institution, in alliance with the city, has stripped us of our land and has destroyed at least 650 of our homes without replacing a single unit of housing.
The committee demanded that the medical center provide job training and hiring programs, “adequate and free health care,” and expanded community service and recreational facilities. It also called for “an end to all and any further T-NEMC [the medical center] expansion now and a commitment to replace, with low-income housing, all housing destroyed by previous expansion.” 47 The question of community, and specifically ethnic, control over the outcome of the renewal process underlay these demands. The activists who made up the Free Chinatown Committee sought not only to block further medical center expansion but also to ensure that resources such as the long-delayed Tai Tung Village housing development (the low-income housing promised in the 1963 agreement) and the new Josiah Quincy Elementary School Complex (which included housing, health care, day care, and social service components as well as a school) would be solely controlled by the Chinese community. An increasingly frustrated Hermann Field wrote angrily that “the Chinese no longer see a South Cove community. ‘Community’ to them means only and exclusively Chinese, and the other groups are irrelevant.” 48 What Field missed was the evidence—in the slow pace of low-income housing construction, in the existing schools that had long discouraged expressions of Chinese culture, in the willingness of the state to build highways through residential neighborhoods, and in the medical center’s long effort to facilitate its own expansion through control over land, buildings, and planning—that convinced the Chinese activists that they had few options other than direct control.
Soon, more moderate groups joined the Free Chinatown Committee in pressing the medical center to deliver on its promises. The South Cove Young Men’s Christian Association (YMCA) board, for example, narrowly passed a resolution stating “that the New England Medical Center has not met its moral obligation to the community,” while the Chinese American Civic Association issued a request not only for job training and hiring programs at the medical center but also for office equipment for its community services center, community aides at its senior center, and access to buildings owned by the medical center in which it might run its programs. 49
Medical Center Executive Director David Everhart and Tufts Medical School Dean William Maloney responded to this combined pressure with a statement acknowledging “the Community’s impatience, as well as the anger and frustration of the young members of the community represented by the Free Chinatown Committee.” Pledging to improve communication and work more closely with the community, Everhart and Maloney even offered “an immediate commitment of personal time and involvement.” Reclaiming the initiative from the Free Chinatown Committee, the moderate Chinese American Civic Association embraced this offer and agreed to resume work with the medical center. Everhart and Maloney, however, also pointed to “the limited resources available,” indicating that there would be limits to the medical center’s willingness, or ability, to serve the community’s needs. Over the following years, the community did at last gain some benefit from the relationship with the medical center: Tai Tung Village moved to completion, and other low- and moderate-income housing projects followed. The Quincy School Complex opened in 1976. 50
Still, conflicts over land use continued through the 1970s and 1980s. The community managed to win many of these battles, either through the political process or through the courts. In 1970, Chinese American activists had successfully fought a Medical Center proposal to build a parking garage on a site they felt would better serve as a community center. In 1987, the city rejected another Medical Center parking garage proposal that community groups opposed, and the following year, the Massachusetts Superior Court upheld the Authority’s designation of a community group as the redeveloper of four key land parcels over the medical center’s objections. 51 At other points, however, the medical center and the community joined forces when their interests coincided.
One such case involved the city’s 1973 decision to designate an area just to the north of Chinatown and the medical center as an official “adult entertainment district.” Known colloquially as the “Combat Zone,” the area quickly filled with strip clubs and pornography stores and became a center of prostitution. Medical center administrators worked with community groups to oppose the Combat Zone and to push for its elimination. Seeking to fend off broad attacks on the policy, Mayor Kevin White staged a midnight tour of the district, stopping to buy drinks for strippers in the clubs. 52 Despite the unified position of the center and the community against it, the Combat Zone remained in place until gentrification gradually drove its denizens away in the 1990s. 53 Less colorfully, but more significantly, the medical center assisted the urban renewal program’s inclusion of affordable housing projects aimed at Chinatown residents. It also provided funding and staffing for the South Cove Community Health Care Center. 54
The Health Care Sector and the Transformation of Boston
Despite the community’s relative success in exerting checks on the long-term redevelopment process, the medical center achieved its core objectives. Beginning in the late 1960s, it undertook an extended rebuilding effort—much of it vertical—that effectively created the first-class medical complex that its administrators had envisioned in the 1950s. Working from the basic approach outlined in the 1965 urban renewal plan, the medical center in 1975 completed construction of a new building for the Tufts University Dental School, as well as the new Proger Health Services Building, which housed the center’s main inpatient services. Consistent with wider trends in hospital finance during the period, the medical center took on debt to finance the Proger building. 55 These projects involved a complicated relationship with the displacement issue. The direct construction footprint for the buildings took advantage of a number of already vacant lots and required the demolition only of a series of commercial properties that housed low-cost furniture stores. These businesses had high turnover rates and provided relatively little employment. Other components of the expansion during this period involved the removal of garment firms from loft buildings along Kneeland Street so that the space could be renovated for medical center administrative offices and research labs. The direct footprint of the medical facilities, however, represented only part of the medical center’s impact. Kevin Lynch, Logue, and Field had all argued vociferously that the center’s expansion required, and even depended on, accommodation of the automobile. This focus on parking remained central to Medical Center planning for decades. With the new hospital and dental buildings of the 1970s and 1980s came large associated parking garages in adjoining buildings. The first garage, built in conjunction with the Proger and Dental School buildings, occupied a full block that at the time of the Lynch study had contained thirty-one housing units. 56
These choices about land use, and, particularly, about the removal of existing residential and commercial uses in service of the medical center’s growth, demonstrated one of the core dilemmas posed by the emergence of the hospital as an urban anchor. Health care, medical education, and biomedical research clearly offered better future prospects for Boston than garment manufacturing or low-cost retail—as Edward Logue, Hermann Field, and the medical center maintained. Since the medical center already occupied space in some of the former garment lofts, this transition had already begun. 57 Nonetheless, the process of land-use change involved a series of active, distinct policy choices about the kind of neighborhood Chinatown would be, and about how the growing health care sector would relate to its surroundings. The construction of this urban future depended on particular configurations of urban policy to make it possible. Eminent domain, urban renewal write-downs, local in-kind contribution credits for private investment, and, above all, the sanction of private, institutional growth plans by public authority created the conditions from which this new urban political economy could emerge. Creation of the new hospital city involved an erasure of any clear boundaries between public and private authority.
New policy tools, and with them, new risks, evolved to facilitate continued expansion of the hospital city. With the core project of the Proger Building completed, the medical center next undertook the rebuilding of the Boston Floating Hospital, which housed its pediatric services. The existing building had been constructed after the original Floating Hospital ship burned in 1927. By the 1970s, it had become badly outdated. Since 1964, the Floating Hospital’s operating license had required a waiver from the Massachusetts Department of Health “because of the inadequacy of the physical facility.” In 1976, the Department of Licensure warned that the building’s many violations of the state Life Safety Code might soon “jeopardize the Center’s Medicare and Medicaid reimbursement.” The following year, Boston Health Planning Council inspectors identified twenty-four serious areas of inadequacy, ranging from inadequate ceiling clearance for the installation of central air conditioning to congested operating rooms and laboratories to undersized patient rooms with inadequate bathroom facilities. Floor levels of the Floating Hospital did not align with other Medical Center buildings, which required “space consuming connecting ramps,” and surgeons even had to walk down a flight of stairs from their changing rooms to the operating rooms. 58 Replacement of the facility seemed imperative.
Initial planning for such a project, however, indicated that construction and related costs would exceed $55 million. With the medical center still carrying $3.4 million in debt from the just completed Proger Building, financing for a new project, no matter how badly needed, proved problematic. As a result, the medical center turned in 1976 to the FHA’s Section 242 mortgage insurance program, as did many other northeastern urban hospitals during the period. Gaining access to the federal mortgage guarantee, though, required an intricate and time-consuming process that eventually occupied more than three years. Since the late 1960s, many states, Massachusetts among them, had required hospitals to go through a state “determination of need” process before they could undertake any significant new construction projects. This requirement was intended to avoid overinvestment in hospital facilities so that expansion did not outstrip regional demand. Section 242 in turn required completion of the determination of need process prior to the start of the federal approval process. 59 In the case of the proposal for a new Floating Hospital, determination of need procedures delayed the project for nearly fifteen months in 1976 and 1977 after the Health Planning Council for Greater Boston concluded that the project “did not represent the provision of adequate health care services at the lowest reasonable aggregate cost.” Hospital cost control had emerged as a critical health care policy issue by 1976, and the Boston region as a whole already had a hospital bed-to-population ratio that far exceeded both state and national guidelines. Even though the Floating Hospital project would merely replace the old building’s pediatric beds, with no significant overall increase in beds, the excessive existing ratio meant that the project could be rejected. The growth of the hospital city had now come into conflict with the increasingly pressing imperative to limit health care cost growth.
During the appeals process that followed, however, a combination of the site inspections described above and a staff analysis that emphasized the Floating Hospital’s key regional role finally won the Health Planning Council’s support. 60 In November 1978, Health Planning Council Director Joanne Bluestone explained that the project was justified because of “the uniqueness of the pediatric populations served by the [the medical center]—patients from city areas which have federal medically underserved status and patients referred from throughout the region for tertiary care.” As a result, the Council endorsed the medical center’s application for federal financing assistance. 61 Convinced by the Health Planning Council’s revised analysis, the Massachusetts Department of Public Health issued the required Certificate of Need and the state Health Planning Agency offered its approval as well. 62
Review of the project by the FHA and the Department of Health, Education, and Welfare occupied nearly two more years and involved a detailed assessment of the hospital’s cash flow, its revenue sources, and the overall soundness of the proposed financing that the FHA would insure if it approved the medical center’s application. This process revealed the medical center’s dependence on Medicare and Medicaid payments, which together accounted for 39.5 percent of receipts in fiscal year 1978. It also demonstrated that only about 3.5 percent of all care (in patient billings) provided by the center went to free care for individuals lacking some form of third-party coverage or the ability to pay out-of-pocket. 63
Finally, in late September 1979, the Department of Health, Education, and Welfare’s (HEW) regional office in Boston recommended approval to HUD, allowing the project to move forward. 64 This slow state and federal approval process, which led some hospital administrators to avoid using Section 242 altogether, had a valuable payoff. A 1978 estimate suggested that the presence of FHA insurance on the medical center’s $55.56 million mortgage loan for the Floating Hospital project would allow the hospital to receive a rate of interest between 1 and 1.5 percent lower than on a conventional loan without such federal insurance. Over the life of the loan, this lower interest rate would save the hospital a minimum of $10 million in debt service. 65 Finally, after three years of construction, the new ninety-six bed Floating Hospital building opened in 1982. Over the following four years, medical center completed a series of significant renovations of its ambulatory care facilities as well as the construction of a Magnetic Resonance Imaging Center. In conjunction with the opening of the Floating Hospital, these projects completed the phase of medical center planning and expansion that Hermann Field and Edward Logue had initiated twenty-five years before.
Health Care Policy and Urban Policy in Conflict: Excess Cost and the Hospital City
A final irony must be noted in evaluating the role of public policy in the development of the urban health care anchor for the postindustrial city: at the time that the Tufts-New England Medical Center’s expansion projects were planned, they had a distinctly dual nature. Linked to Edward Logue’s urban renewal program through the Section 112 credits, the medical center’s redevelopment and expansion constituted part of a broader political economic agenda that sought to transition the city from its industrial past to a new economy based on advanced research and service provision (across a range of sectors). Yet at the same time, the expansion of the medical center was rarely thought of as an explicit economic development measure. From Hermann Field’s internal planning operation to the Health Planning Council’s deliberations over bed ratios to HEW’s assessment of Medical Center cash flow viability, the projects were instead considered mostly in the context of health care issues: quality of care, cost control, and relation to medically underserved communities. 66 Although the relationship to the surrounding Chinatown community mattered, perhaps to an uncommon degree, this had as much to do with managing the political process and creating housing as it did with generating neighborhood economic development. Neither Edward Logue, nor John Collins, nor Hermann Field, nor their immediate successors saw the medical center as a driver of economic development and employment.
As a result of this disjuncture, by the late 1970s the role of hospitals as employers created direct conflicts with the push toward hospital cost containment. As the regional office of HEW’s Division of Health Resources Development considered the medical center’s application for Section 242 mortgage insurance in mid-1979, a federal official questioned the center’s high levels of employment relative to “the average for New England teaching hospitals” and wondered “why [Full-Time Employees] would be projected to increase when a major objective of the building program is to increase efficiency.” Employment simply was not the goal. “An explanation,” the HEW loan officer concluded, “is necessary.” 67 In a policy environment focused on economic development, in which officials saw the medical center clearly as the economic driver that it had become, no such explanation would have been required.
At times, the consequences of structural economic change intersected directly with the imperatives of cost control. In the late 1970s, the Social Security Administration lowered the income classification of the Boston metropolitan area based on the region’s declining per capita income; this action led to steep cuts in regional Medicare and Medicaid hospital reimbursement rates. Declining per capita income, of course, reflected the broader economic transformation underway in cities like Boston. One federal analyst recognized this, assuring the director of the Medicare Bureau that
it can be reasonably assumed that the lower per capita income is an accurate reflection of the economic condition in that area. In Boston’s case, it appears that the lower per capita income group is a realistic reflection of that city’s relative standing in the country.
68
From the perspective of cost control, this justified cutting rates, even if the policy hurt urban hospitals—the very institutions that held the most promise for reversing the decline in per capita income. That, however, was not the Social Security Administration’s (SSA) concern.
Although the New England Medical Center had the resources to sustain itself through such uncertainty, a number of smaller institutions in Boston found their very existence threatened. 69 In such cases, the role of health care policy as a form of implicit urban policy proved deeply problematic. Along with inadequate access to health care and insurance coverage, the chief underlying problem of the U.S. health care system has been its inability to control costs. Yet it has been those excess expenditures that have funded the growth of the new urban health care anchor, the economic sector that has provided the chief replacement for manufacturing at the core of urban economies. The rise of the hospital city has been based on one of the key structural problems of the wider health care system.
The Medical Center as Urban Anchor
Whether explicitly conceived as an economic development policy or not, the growth of the New England Medical Center after 1960 had significant economic implications in postindustrial Boston. As early as 1972-1973, studies of the medical center’s economic impact found that it had major effects in expenditures, employment, and construction both in Boston itself and in the metropolitan area. 70 By the mid-1980s, the medical center had nearly 2,500 employees, with a payroll of almost $60 million. By 1997, the center had 4,995 employees and had become the city’s seventh largest private employer (although only its third largest hospital employer), and one of five hospitals among the city’s top ten employers. By that date, the health services sector accounted for 14.5 percent of all jobs in Boston, up from 11 percent ten years before. 71 Meanwhile, the city’s industrial sector continued to decline: between 1969 and 2002, Boston lost 76,631 manufacturing and wholesaling jobs. 72 Although its foundations rested on the U.S. health care system’s high levels of spending and lack of effective cost controls, the hospital city had been established.
During this period, the medical center’s entrenched pattern of cautious negotiation with the Chinese American community continued. In 1983, the center entered into a partnership with the CCBA in which it provided $100,000 to create a program that would train residents for health care jobs, including at the medical center. In exchange, the CCBA agreed to accept components of the center’s development program that it had previously resisted. 73 This agreement made explicit the long-standing trade-off between institutional growth and the community’s capacity to capture some of the economic benefits of health care sector’s expansion. It has continued to the present. In 1990, the medical center agreed to shape its master plan in accord with a plan developed by a consortium of community groups working under the umbrella of the Chinatown-South Cove Neighborhood Council. 74 More recently, a two-decade long struggle against the medical center plan’s for an 850-car parking garage concluded with the construction instead of the Metropolitan—a twenty-three story, mixed-income tower that reserved 46 percent of its units for affordable housing and included space for four community agencies that offer child care services, youth programs, job training, and English as a Second Language services. 75
These community benefits resulted from a number of key features of the institutional expansion process in Chinatown and the South Cove. First, both the medical center and the Chinese American community had a long-standing presence in the area, and both were recognized from the time of Kevin Lynch’s report as having legitimate interests in any changes that would take place. Second, Hermann Field’s planning operation within the medical center built on Lynch’s work and, from an early point in the process, articulated a goal of considering community interests and providing opportunities for input from the center’s neighbors. This position was of course neither universally nor consistently honored by the medical center, and its master plans often proceeded with the primary aim of maximizing its own interests. Yet the suggestion alone brought the issue into discussion and, when combined with community and at times political pressure, frequently led the medical center to accommodate the community’s interests as it expanded. At times, it even embraced a position of community partnership. In 1970, Field observed that “our concepts of how we should relate to the community have changed under pressure from the community, but we have been able to change.” 76 Third, more tentatively, the erasure of clear boundaries between the public and private planning process had significant consequences. Hermann Field’s private planning office within the medical center completed much of the basic planning for the public South Cove Urban Renewal Project. When the Authority accepted such participation from the acknowledged institutional stakeholder in the area, it opened the possibility for including as well the acknowledged community stakeholder. While this outcome remained contingent on political configurations within the redevelopment authority and city government that lie beyond the scope of this article, it nonetheless suggests that the lack of clear public–private boundaries may have helped to open the possibility for productive conflict that led to eventual cooperation, if not full partnership.
Tufts Medical Center, as it is known today, has nearly 5,000 employees and remains among Boston’s largest private employers. Just as significantly, the hard-won community–Medical Center partnerships in housing, medical care, community health, health services–related job training, and other areas have continued. Although it retains the exemption from the city’s property tax, since the late 1970s the medical center (and other Boston universities and hospitals) has made a “payment in lieu of taxes” to the city of Boston. In 2009, this payment exceeded $1 million. Without the tax exemption, however, the medical center would have paid the city $15.8 million in property taxes. 77 Employment is just one of the functions of the hospital city, and the political economy of local taxation suggests a key cost of reliance on hospitals and medical centers as anchors for the postindustrial city. Such institutions provide jobs and offer key health services (to those who have access to health care), but their direct contributions to city tax bases, and hence to the provision of other important public services, remain limited. 78
In many respects, Tufts Medical Center embodies the urban health care sector that has expanded so greatly since World War II and that this article places at the core of the political economy of the postindustrial hospital city. This outcome is the result of both tacit and direct public policies, including excess health care spending. What, then, does this admittedly provisional case suggest about the record of federal urban policy in the second half of the twentieth century? In part, it must be recognized that many of the standard critiques of U.S. urban policies, and particularly urban renewal, are still applicable. As a result of institutional expansion and highway construction, Boston’s Chinatown lost more than half its total acreage between 1960 and 1975 alone. The neighborhood’s boundaries have shifted notably, much of its population experienced displacement, and community institutions were destroyed. Yet the community has also benefited from new affordable housing, new schools and community facilities, increasingly significant economic spillovers in terms of both direct job and training opportunities in the medical center and greater customer base for neighborhood businesses (from Medical Center traffic and from a nearby cultural district revitalized through the urban renewal project), and a planning process that became increasingly responsive to community needs. These positive qualifiers to the traditional critique of urban policy are of course dependent on the particular factors involved in one case study in one city. A full evaluation of the hospital city will depend on a far broader assessment of how such contingencies played out around the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received financial support from the Bankard Fund for Political Economy for research conducted in the preparation of this article.