
Abstract
Perpetual debate regarding the delicate balance between access and innovation and the protection of the public health and safety dominate discussions of the United States Food and Drug Administration (“FDA”). Established chiefly as a command and control federal administrative agency, iterative changes in legislation have shaped the FDA's activity in drug, biologic, and medical device regulation over the course of the last one hundred plus years. The most recent fundamental reframing of the agency's authority and directive presented itself in the 21st Century Cures Act, reflecting an important role for patient perspectives in the regulatory process. This Article explores recent developments in patient-focused product development efforts at the FDA and offers modest insights on the increasing role of patients, and patient advocacy groups, in agency decision-making. The Article terms this era “21st century citizen pharma.”
I. INTRODUCTION
Over the last decade, medical, scientific, and legal commentators have noted the ushering in of the “citizen science” movement, describing the active involvement of a broad spectrum of stakeholders in the scientific process. This term contemplates the emergence of non-scientist contributions in traditionally highly expert fields, including genetic and genomic research. Patient advocacy groups have been leading the charge, supporting recent legislation and policy efforts to foster widespread recognition of innovative and information-generating partnerships to inform pharmaceutical and medical device development. Strategic alliances within industry, academia, and the public are also propelling these efforts into the mainstream.
The 21st Century Cures Act continues this trend, introducing statutory provisions that provide ample authority and discretion to the FDA to utilize more expansive sources and types of information and evidence to support medical product evaluation and approval. This legislation was driven largely by patient advocates and has significant potential to foster increased involvement of patient advocate groups across many aspects of the FDA process. This article examines this legislation, its implementation, and its potential long-term implications for medical product development as coupled with the “citizen science” movement, resulting in the new era of “citizen pharma.” 1
Part II of the article describes the historical development of the Food, Drug and Cosmetic Act (“FDCA”) as implementing a relationship strictly between the FDA and the regulated industry. As a command and control regulatory structure, congressional design has historically mandated direct communication between drug, biologic, and medical device sponsors and the FDA to inform product evaluation and approval. This part also describes iterative changes in the FDCA that have enhanced the FDA's ability to consult outside sources for information, and FDA's own initiatives to seek outside perspectives. Part III traces the basis and growth of the “citizen science” movement tied to patient advocacy, stemming from controversial litigation involving human tissue and property rights, and then examining the emergence of the patient advocate as a response to this case law. This part will examine several key areas of development emerging from lessons of the past, including the role of patient advocacy groups in maintaining biobanks, shaping policy, and introducing novel contractual and intellectual property agreements.
Part IV explores relevant provisions within the 21st Century Cures Act, enacted in December 2016, that support a broader role for citizen pharma. These include provisions providing for the analysis of patient experience data, real-world evidence (“RWE”), qualified data summaries, biomarker qualifications, and adaptive trial designs as tied to new drug evaluation, as well as select provisions pertaining to medical devices. Part IV also details current initiatives of the FDA to implement the 21st Century Cures Act provisions and more general efforts of broader stakeholder input in the drug and medical device approval process, citing real-time examples and partnerships. The article then concludes with several modest thoughts on the future of citizen pharma.
II. THE FDCA & BEYOND
The FDA is a creature of congressional design, tasked with oversight of at least one-fifth of all consumer products in the United States, 2 accounting for $1 trillion of spending per year. 3 The FDA is responsible for a spectrum of products as set forth in numerous federal statutes, the most complex being the FDCA, which is codified in Title 21 of the United States Code. 4 This section explores the structure of the FDCA and basic concepts regarding regulation of new drugs, biological products, and medical devices.
A. FDCA Structure —Classic Command and Control
The historic structure of the FDCA dates back to the original Pure Food and Drug Act, enacted by Congress in 1906 in the wake of outcry over food production methods sparked by Upton Sinclair's novel The Jungle. 5 The legislation was the first significant piece of consumer protection law introduced by Congress and signaled tremendous changes in the manner in which the government regulated medical products over the course of the next half century. Although the 1906 Act set forth chiefly post-market enforcement provisions relating to adulteration and misbranding of products once on the market, subsequent amendments in 1938, 1962, and 1976 fundamentally secured the FDA's role as gatekeeper to market entry in the realm of drugs and medical devices. By 1962, new drug sponsors were required to demonstrate both safety and efficacy via clinical trials in a new drug application prior to gaining market approval, 6 and by 1976, medical device sponsors were also subject to affirmative pre-market approval requirements for high-risk devices. 7 Likewise, biological products were subject to premarket approval on the basis of safety, purity, and potency, with similar clinical trial requirements and safety and efficacy review. 8 Such regulation epitomizes the classic “command and control” model, where regulation consists of standards, requirements, and enforcement actions for violations. 9 Essentially, the interaction in this command and control relationship is strictly one between the FDA as regulatory agency and the regulated industry.
However, there has been a distinct movement over the last several decades with regard to the role and voice of patient advocacy groups in regulation and input into product development and long-term market profile. One prime example of this is the Patient Centered Outcomes Research Institute (“PCORI”), established as part of the Affordable Care Act. 10 Another example is the “All of Us” precision medicine campaign, to which patients are donating samples and medical information for the purpose of identifying genomic information to guide targeted therapies. 11 Largely driven by legislation, these and other patient-focused efforts are informing medical care and research at many levels. Several FDA-specific initiatives are discussed below.
B. FDA Patient -Focused Initiatives Prior to the 21st Century Cures Act
Congress has by legislation imposed a number of duties on the FDA to engage and involve patients in the regulatory process. As early as 1988, the FDA created the Office of Health and Constituent Affairs, and recently introduced the FDA Patient Education Network to “educate patients, patient advocates, and their healthcare professionals about medical product regulations and … involve patients more effectively in regulatory decisions related to medical product safety and approval.” 12 The FDA maintains a patient webpage with resources and contact information. 13 The Center for Drug Evaluation and Research (“CDER”) also recently concluded a series of 22 patient-focused drug development meetings spanning 2012-2017, imposed by the Food and Drug Administration Safety and Innovation Act of 2012 (“FDASIA”). 14 Patients may also contribute through adverse event and product reporting for drugs, biologics, and medical devices via MedWatch, the online platform provided by the FDA. 15
By far, the FDA's Center for Devices and Radiological Health (“CDRH”) has taken the lead on incorporating patient perspectives into regulatory matters. There is a centralized webpage directing patients to CDRH resources and patient-focused initiatives related to medical devices, with links to guidance documents, Federal Register announcements, and reports. 16 In 2013, CDRH launched the Patient Preference Initiative to “develop a systematic way of eliciting, measuring, and incorporating patient preference information, where appropriate, into the medical device Total Product Life Cycle.” 17 A Patient Engagement Advisory Committee (“PEAC”) was established in September 2015 as required by the FDASIA. 18 The FDA also finalized a guidance document in August 2016 regarding the consideration of patient preference information (“PPI”) in medical device submissions. 19 The FDA defines PPI as one specific type of patient perspective that is “qualitative or quantitative assessment of the relative desirability or acceptability to patients of specified alternatives or choices among outcomes or other attributes that differ among alternative health interventions.” 20 The guidance document sets forth recommended qualities of patient preference studies, how and when to submit to FDA, inclusion of PPI in decision summaries and possibly device labels, and gives hypothetical examples. 21 And in November 2016, CDRH created the Patient & Care-Partner Network to “partner with patient organizations to provide a means for CDRH staff to formally engage with patients and care-partners.” 22
At the strategic level, CDRH has identified partnering with patients as a 2016-2017 priority, one of three priorities enumerated in their report.
23
The report highlights that “[p]atients are no longer passive bystanders in their health.”
24
Going further, the report states:
Patient groups have evolved from patient support, advocacy and basic disease research funding organizations, to being more active in medical product development and assessment. Patients are committed to contributing their views, data, and resources to increase patient-centric medical product innovation, assessment, and regulatory decision-making, and we are committed to assuring that our decisions and actions are informed by patient perspectives.
25
CDRH subsequently published a document entitled Value and Use of Patient-Reported Outcomes in Medical Device Assessment, which noted that the FDA was incorporating both PPI and patient reported outcomes (“PRO”) into regulatory decisions. 26 FDA has stated elsewhere that the use of PRO measures as primary and secondary endpoints in medical device clinical studies rose from 20 prior to 2009 to over 120 in 2014. 27
The FDA's CDRH is also a member of the Medical Device Innovation Consortium, a non-profit, public-private partnership that includes medical device companies, trade associations, patient groups, the National Institutes of Health, Centers for Medicare & Medicaid Services, PCORI, and other, non-profit, organizations. 28 The Consortium has published a framework for incorporating patient feedback. 29 In 2016—triggered by FDASIA—the FDA also established a cross-Center Patient Council to “better coordinate and integrate the role of patient perspectives into regulatory decision-making over the total product life cycle.” 30
Last, just following the enactment of the 21st Century Cures Act in December 2016, the FDA issued a final guidance document on factors to consider regarding benefit-risk in medical device availability, compliance, and enforcement decisions. 31 A draft had been introduced earlier in June 2016. This document includes information on measures of patient perspectives on benefits and tolerance, and means to include in agency assessments. 32
III. THE RISE OF “CITIZEN SCIENCE” AND THE PATIENT ADVOCACY MOVEMENT IN THE U.S.
The term citizen science has a range of meanings for different groups both internationally and in the U.S., although a quick sampling reveals common themes. The National Geographic Society defines it broadly as “the practice of public participation and collaboration in science to increase public knowledge.” 33 A federal government collaboration states that “[i]n citizen science, the public participates voluntarily in the scientific process, addressing real-world problems in ways that may include formulating research questions, conducting scientific experiments, collecting and analyzing data, interpreting results, making new discoveries, developing technologies and applications, and solving complex problems.” 34 Even the Oxford Dictionary has added the term, defining it as “scientific work undertaken by members of the general public, often in collaboration with or under the direction of professional scientists and scientific institutions.” 35 This Article uses the term broadly, as a public participation and collaboration in scientific endeavors involving legitimate research questions.
This participation and collaboration of the public with the scientific community in the pursuit of answers to research questions ties directly into the current approach of patient advocacy groups in the U.S. The patient advocacy movement over the last several decades is a response to failures of the legal system to recognize patient rights, autonomy, and perspectives in the scientific process. As the CDRH's 2016-2017 strategic priorities report notes, 36 patients are no longer passive consumers of healthcare; patients, and advocacy groups, seek an active role in research, development, commercialization, and market longevity of medical products. This Article connects the patient advocacy movement with the general rise of citizen science, particularly exploring the realm of drug and medical device development and product approval by the FDA. A brief overview of the early U.S. landscape, including literature and case law, coupled with an exploration of the current activity of patient advocacy is warranted here.
A. The Early U.S. Legal Landscape : Literature and Case Law
Bioethics literature is rife with scholarship addressing early examples of scientific misconduct with respect to removal and use of human samples without consent for financial gain. In each scenario, some type of relationship existed between the patient and the medical specialist or facility charged with misconduct, whether it was fiduciary in the traditional doctor-patient setting, or arose from a researcher-human subject interaction. In each scenario, there was also a complete lack of informed consent. It seems incomprehensible that in a post-Nuremburg Code world such situations would occur, but any legal or bioethics scholar is well aware of the unfortunate landscape in the U.S. For example, Rebecca Skloot conveys the story of Henrietta Lacks, a poor African American woman whose cells were extracted from a tumor biopsy in the early 1950s at Johns Hopkins Hospital, cultured, and developed into the HeLa cell line. 37 Another example is the Tuskegee Syphilis Study, a Public Health Service clinical study tracking the impact of untreated syphilis on African American men for four decades, ending only in 1972. 38
Several cases made their way through the courts starting in 1990. The first was the case Moore v. Regents of the University of California, a staple for any first year Property Law casebook. 39 There, John Moore underwent treatment for hairy-cell leukemia at the University of California, Los Angeles (“UCLA”) Medical Center. 40 Over the course of seven years, Moore travelled regularly for extraction of blood, skin, and bone marrow that he believed was critical for the monitoring and treatment of his condition. 41 Moore only later discovered that his physician, Dr. Golde, had isolated, patented, and commercialized a cell line derived from his samples. 42 Moore sued UCLA and Dr. Golde for lack of informed consent, breach of fiduciary duty, and conversion. 43 Moore urged the court that he deserved a portion of any profits derived from drug development resulting from his sample. 44 The Court refused to recognize that Moore had a property interest in the samples extracted from him, stating only that physician researchers may have a fiduciary duty to patients to disclose intent to use patient samples for research or commercial reasons that may not directly benefit the patient. 45 Moore settled the case and became a champion for patient rights, dying at age 56 from experimental therapy. 46 Interestingly, the strong dissent by Justice Mosk argued for an expansion of the term “inventor” in the patent law to include the source of the tissue as a recognition of the substantial nature of the contribution. 47
In 2000, a similar case arose involving the use of blood, urine, and tissue samples of children afflicted with Canavan disease, a rare genetic condition. 48 Plaintiffs, both the non-profit patient groups and individuals, alleged that the hospital and researcher did not inform them of the intent to patent and commercialize discoveries resulting from use of the samples, and to restrict access to diagnostic testing developed using the samples. 49 Six causes of action were asserted: lack of informed consent, breach of fiduciary duty, unjust enrichment, fraudulent concealment, conversion, and misappropriation of trade secrets. 50 All but the unjust enrichment claim were dismissed in 2003, and the case was ultimately settled out of court. 51 It was reported that the hospital would continue licensing the patent for use in clinical testing and would collect royalties, but would allow license-free use “in research to cure Canavan disease, including gene therapy research, genetic testing in pure research, and in mice used to research Canavan disease.” 52
Two additional cases contribute to the discussion, both involving academic medical research centers and faculty investigators. In Washington University v. Catalona, at issue was the ownership status of Dr. Catalona's biobank of approximately 10,000 blood and tissue samples acquired from prostate cancer patients over his 26 year tenure at the university. 53 Catalona sought to transfer the samples with him to his new institution and the University sought to retain ownership. 54 The Court, relying on contract law principles, held that in the absence of express terms in the consent forms, the University was the rightful owner (despite patient expectations and support for Dr. Catalona's continued use). 55 The 8th Circuit affirmed the decision in July 2007. 56 In Havasupai Tribe v. Arizona State University (“ASU”), 57 two lawsuits were filed against ASU relating to use of banked blood samples: one on behalf of individual plaintiffs, 58 and the other on behalf of the Havasupai Tribe. 59 The lawsuits alleged that ASU investigators used samples collected in the 1980s from tribe members specifically for diabetes research to subsequently study rates of schizophrenia and origins of the tribe, which directly conflicted with their origin story. 60 The parties settled in March 2010. ASU agreed to pay the tribe $700,000; return all samples in their possession; return all documents pertaining to the research; terminate all institutional review board approval for research involving the use of the samples; and, provide a list of entities to which samples were transferred. 61
Drawing momentum from the unsatisfactory outcomes in the aforementioned cases, patient advocacy groups have taken the lessons from the legal decisions and have shaped a new role for themselves.
B. The Emergence of the Patient Advocate as a Citizen Scientist
There is rapidly growing literature documenting and exploring the increasing role of patient advocates as tied to the citizen science movement. 62 This Article will not attempt to reprise that literature here, but will offer several key points. First, patient advocacy groups and collaborations have flourished over the last 20 years following the publication of the human genome. Momentum in genomics and the promise of precision medicine has reframed the importance and position of advocacy groups. The role of the advocacy group is now wide-ranging, from providing education and public outreach, facilitating collaborations with researchers, securing funding for research, and lobbying Congress and state legislators, to acquiring and maintaining patient biospecimens and corresponding medical information in biobank registries. 63 As part of this shifting role, some patient advocates have also strenuously pushed for a change in terminology from research subjects to research participants to reflect these important contributions. 64
Second, patient advocacy groups have implemented careful organizational structures and robust legal representation, and are keenly proactive in developing contractual agreements with researchers for access to samples and future commercialization rights, including licensing and intellectual property.
Third, many advocates are documenting and publicizing their active involvement as citizen scientists, touting their own contributions alongside scientists. For example, Sharon Terry, an executive director of a patient group called PXE International, and a mother of two children with pseudoxanthoma elasticum (“PXE”), a rare connective tissue disorder, claims she engaged in the bench science. 65 She reports “I extracted DNA, ran gels, read the gels and helped write the paper announcing the gene's discovery.” 66 She was also named co-inventor on the patent. 67 Likewise, Francis Collins collaborated with co-founder and medical director of the Progeria Research Foundation in the discovery of the disease gene, which was subsequently patented. In this instance, the patient advocate held a PhD and was an pediatrics instructor at a major children's hospital. 68
Finally, patient advocacy groups are leading the charge on legislative changes that support an increased role in drug and medical device research, development, and oversight. This is most evident in the 21st Century Cures Act, although the Act builds on prior achievements at both the state and federal level.
IV. THE 21st CENTURY CURES ACT AND PATIENT-FOCUSED DRUG DEVELOPMENT INITIATIVES
The 21st Century Cures Act was years in the making. The first iteration of the Act was introduced to the United States House of Representatives on May 19, 2015; 69 two days later, it was unanimously approved by the House Energy and Commerce Committee, 70 and passed the House on July 10, 2015. 71 However, it died in Senate committee. The bill was reintroduced, with significant additions and ultimately passed both the House and Senate, with only five Senators voting against it. 72 President Obama signed the legislation into law on December 13, 2016. 73 Legal commentators specializing in food and drug law note the significance of the legislation in breaking the typical cycle of FDA-focused statutory changes as only occurring every five years with reauthorization of user-fee legislation. 74 Various sources also trace the close involvement and support of patient advocacy groups, and the pharmaceutical industry, in the Act's ultimate success. 75 Coverage of the controversy surrounding the passage of the legislation can be found elsewhere. This section describes the relevant provisions of the legislation and details the FDA's activities in implementation.
A. The Enacted Legislation
The legislation directs the FDA to take action in a variety of ways regarding oversight of drugs and medical devices. Notably, the legislation also includes two key provisions directly fueled by widespread patient advocacy efforts over the last several years. First, drug manufacturers and distributors are required to make public their expanded access policies, otherwise termed compassionate use, for investigational drugs undergoing clinical trials. 76 While merely a transparency-driven reporting requirement, this provision relates generally to recent state trends in “right-to-try” legislation led by patient advocacy organizations; these laws have been enacted in 38 states. 77 Such laws preserve the right of terminally ill patients, under the care of a physician, to decide to seek investigational treatments that have succeeded in Phase 1 clinical trials but have not been approved by the FDA. 78 The FDA has its own compassionate use policy and reviews requests from terminally ill patients for access to investigational treatments. 79 However, the drug manufacturer or distributor must agree to distribute the investigational drug as well. 80 There are current discussions among policymakers to enact a federal right-to-try law, yet such an effort faces significant barriers. 81
Second, the legislation also addresses regenerative medicine therapies 82 (“RMT”) in great detail, directing the FDA to update regulations and guidance regarding RMTs, 83 consult with the National Institute of Standards and Technology and stakeholders to establish standards, 84 and grant accelerated approval for RMTs. 85 The legislation also categorizes medical devices used with RMT as moderate risk, unless the Secretary makes a determination otherwise. 86 The FDA has finalized two guidance documents and published two additional draft guidance documents regarding regenerative medicine in the wake of the 21st Century Cures Act. 87 One in particular covers the new legislative changes. 88 The guidelines follow an increase in FDA seizure actions against stem cell facilities and signals of future enforcement actions. 89
Overall, the 21st Century Cures Act introduces potentially significant changes to the FDA processes involved in product review and approval of drugs and medical devices, and gives discretion to the FDA to determine how to implement particular requirements. Figure 1 identifies provisions in which the legislation intersects particularly with the involvement of additional stakeholders and a broader array of information sources in drug and medical device development and regulatory review. Several provisions are extremely timely and relevant to citizen pharma, including the inclusion of patient experience data with drug approvals, new review mechanisms for use of biomarkers in clinical trial design for new drugs, use of RWE for support of new drug indications, and the creation of a breakthrough medical device category.
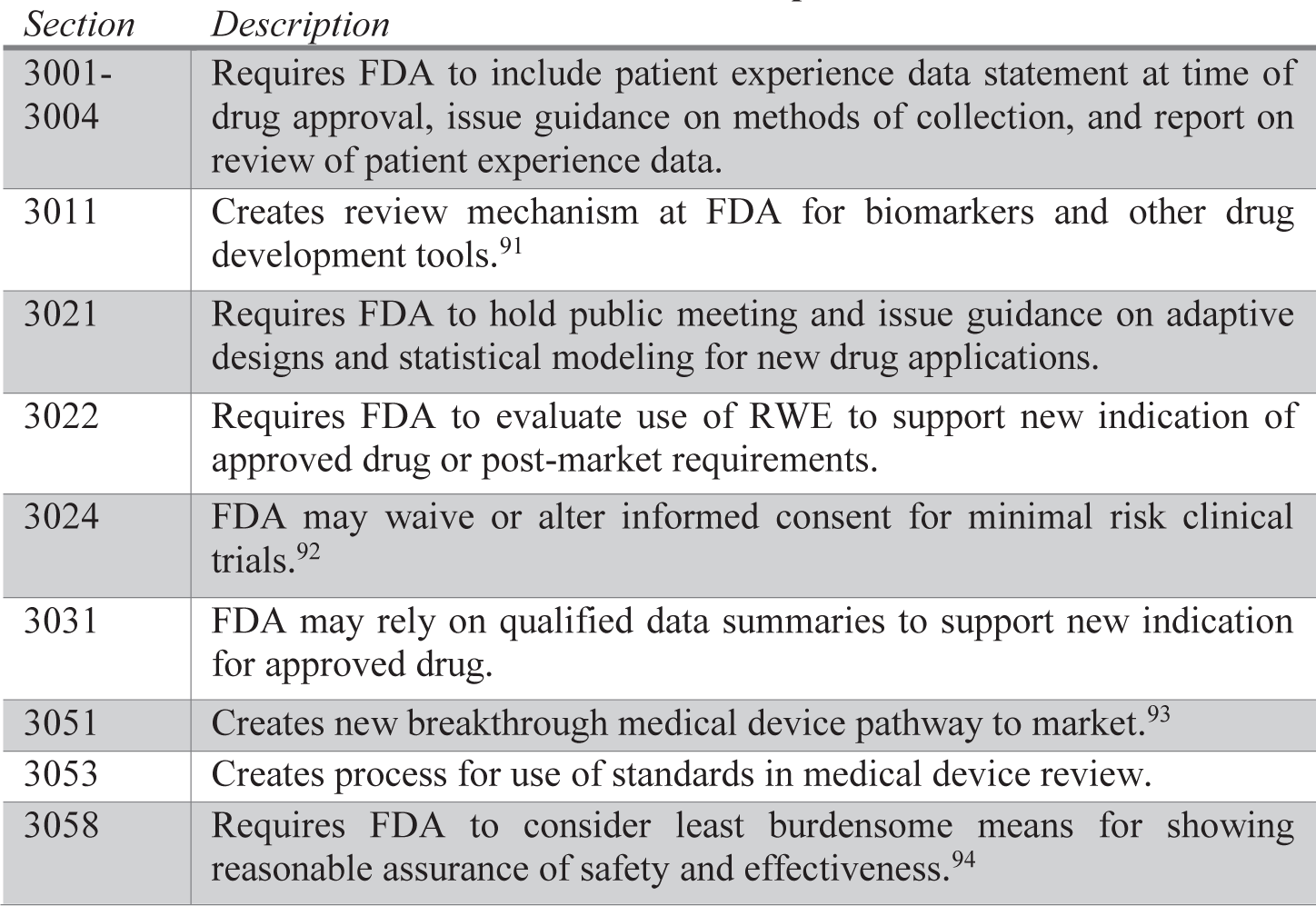
Select sections of the 21st Century Cures Act Relevant to Patient-Focused Product Development 90
The legislation requires the FDA to include patient experience data along with review of a sponsor application for approval. 95 This patient experience data is contemplated as data collected by any person that is “intended to provide information about patients' experience with a disease or conditions.” 96 This includes the impact of the disease or condition, or the accompanying therapy, and preferences regarding treatment. 97 The law also directs the FDA to issue guidance within 18 months of enactment on methods to collect such information from patients, use of such information in drug development, 98 and to publish a report on agency review of patient experience data and use in regulatory decision-making. 99 Many question how the agency will integrate patient experience data into product information that is circulated to consumers and healthcare professionals; some urge that it will require a separate label to facilitate consumer comprehension of the information. 100
Congress also requires the FDA to establish a system of qualification for drug development tools, where qualification assures that the tool “can be relied upon to have a specific interpretation and application in drug development and regulatory review.” 101 Congress urges the FDA to prioritize the qualification of drug development tools based on considerations of severity, rarity, or prevalence of the disease as well as public health priorities. 102 The law contemplates that the process involves a letter of intent, qualification plan, and full qualification package for FDA review. 103 Specific provisions direct the FDA to implement such a qualification process, along with expert consultation, for biomarkers. 104 A biomarker is defined as “a characteristic (such as a physiologic, pathologic, or anatomic characteristic or measurement) that is objectively measured and evaluated as an indicator of normal biologic processes, pathologic processes, or biological responses to a therapeutic intervention.” 105 Legal experts implore the FDA to fully utilize expert consultants in review of biomarker qualification requests, similar to advisory committees for substantive products. 106
Furthermore, the FDA is tasked with establishment of a program to utilize RWE in the assessment of new drug indications and post-market approval studies. 107 Congress defines RWE as “data regarding the usage, or the potential benefits or risks, of a drug derived from sources other than randomized clinical trials.” 108 The FDA is a given two years to establish a draft framework for such a program and begin implementation. 109 Congress enumerates required framework contents, including sources of RWE (such as “ongoing safety surveillance, observational studies, registries, claims, and patient-centered outcomes research activities”), gaps in data collection, standards and methodologies for collection of RWE, and priority areas. 110 In implementing the program, the FDA must consult with several entities, including regulated industry, medical professional organizations, academia, patient advocacy organizations, consumer organizations, and disease research foundations. 111
Finally, the legislation creates a breakthrough medical device category that accelerates device review and approval. 112 These provisions mimic the breakthrough therapy designation introduced in FDASIA applying to drugs and biologics. 113 FDASIA established an expedited review mechanism and mandatory timeframes for FDA response to applicant requests for breakthrough therapy designation; FDA published a guidance for industry in May 2014 detailing the process. 114 Several long-standing FDA policies likewise support accelerated timeframes for drug products, including Fast Track designation, accelerated approval, and priority review designation. 115 The provisions in the 21st Century Cures Act pertaining to medical devices similarly set forth a process for breakthrough status for medical devices. 116 The FDA had previously developed an Innovation Pathway, piloted in 2011, an expedited access pathway in 2015, and a Priority Review program as a means to facilitate faster development and review of promising medical devices. 117
B. FDA Implementation Activity
Subsequent to enactment of the 21st Century Cures Act in December 2016, the FDA has diligently worked to meet timeframes imposed within the legislation, as well as foster new connections with patient groups. At the organizational level, the FDA published a notice in the Federal Register in March 2017 requesting stakeholder input on the creation of a central Office of Patient Affairs, providing a single entry point for patients and to coordinate the FDA's patient-related activities across medical centers and offices. 118 The agency identified objectives for patient engagement activities and outlines the duties of the potential new office. 119 These include providing services to triage and navigate patient inquiries, hosting and maintaining systems for data that include and incorporate patient stakeholder knowledge shared with FDA, and developing a scalable and forward-looking communication platform with an emphasis on online channels. 120 Patient advocates continue to lobby for this central office, though the FDA has not shared any updates on the original call for input. 121
Notably, FDA Commissioner Scott Gottlieb appears to be fostering increased efforts to collaborate across individual product centers. The agency recently highlighted a cross-agency approach to the review of Kymriah, the first U.S. approved gene therapy product, announced in August 2017. 122 Both the Center for Biologics Evaluation and Research and the Oncology Center of Excellence, which cuts across the medical product centers at the FDA, worked to “pioneer and implement this more collaborative scientific model for drug review at FDA.” 123 The FDA press release describes this as a “historic action” that ushers in “a new approach to the treatment of cancer.” 124
In May 2017, the FDA published its plan for the issuance of patient-focused drug development guidance in light of the 21st Century Cures Act, 125 which stipulated that the FDA must issue such guidance as the first step in implementing the patient experience data collection system. 126 The agency has also hosted over 20 meetings to gain stakeholder input on the topic of patient-focused development, triggered initially by legislative directive. 127 The guidance document lays out the FDA's plan and target milestone dates, including public workshops and dates for seven guidance documents. 128 The document references an assortment of FDASIA and 21st Century Cures Act requirements. 129 The proposed funding for the FDA's efforts in this realm is $2.3 million in Innovation Account funding in FY 2018, increasing up to $4.2 million in FY 2025. 130
The FDA published a guidance document regarding the use of RWE in August 2017; a previous draft was published in July 2016. 131 The guidance discusses the spectrum of sources of RWE and the relationship of RWE data collection to the regimented structure and data collection mechanisms of clinical trials. 132 The FDA outlines select purposes for which data collected from RWE may be potentially useful to inform medical device performance, including: for hypothesis generation, as a historical control, as a concurrent control group, as evidence to identify or support clinical validity of a biomarker, as evidence to support the grant of certain product classifications, as evidence to expand the label to include other indications, and to conduct post-approval studies. 133 The guidance emphasizes that relevance and reliability of RWE are tantamount. 134
The FDA held the first meeting in mid-October 2017 of the PEAC, a committee founded by CDRH made up solely of patients, caregivers, and representatives. 135 The CDRH states that the it is “working with a diverse group of outside partners to encourage the inclusion of patient perspectives across the total medical device life cycle, from design and ideation of the medical device to the clinical trial process and through the postmarket evaluation.” 136 CDRH materials online urge that they are considering and working toward “how to integrate the patient voice, as a matter of science, into product development.” 137 The Charter of the PEAC was extended in November 2017 to be in effect until October 2019. 138
On October 25, 2017, the FDA issued its breakthrough devices draft guidance. 139 The guidance implements section 3051 of the 21st Century Cures Act (creating FDCA section 515B) as well as section 901 of the FDA Reauthorization Act of 2017. 140 As noted above, the provisions add to the FDA's existing expedited development and review policies for medical devices. The document establishes basic procedures, identifies relevant considerations for designation of a particular product, and details the role of a data development plan and effective communication with the FDA. 141 Relatedly, media reports in December 2017 draw focus to the FDA's recent additional efforts to speed medical devices approval by introducing enhanced evidence collection post-market. 142
The FDA also launched a Patient Affairs Staff in the Office of Medical Products in December, 143 as well as a Patient Engagement Collaborative. 144 The Patient Affairs Staff website features a useful chart depicting the evolution of patient engagement at the FDA and identifies key areas of focus. 145 The Collaborative will be a partnership between the FDA and the Clinical Trials Transformation Initiative (“CTTI”) “to create a new work group with patient advocacy organizations to talk about patient engagement at the FDA.” 146 CTTI is a patient-centered public-private partnership “to develop and drive adoption of practices that will increase the quality and efficiency of clinical trials.” 147 Relatedly, in July 2017, the FDA published guidance pertaining to provisions in the 21st Century Cures Act that provide authority to the FDA to permit exceptions for minimal risk clinical trials. 148
In all, the FDA has successfully delivered on various directives contained within the 21st Century Cures Act. The agency has built on prior initiatives and collaborations on the topic of patient engagement and perspectives in product development and review. The Gottlieb Administration is also prioritizing cross-center approaches and streamlining review times through novel mechanisms. The challenge will be translating thoughtful guidance and policy regarding non-traditional sources of data and data collection into the regulatory decision-making process.
V. CONCLUSION
Three months prior to the passage of the 21st Century Cures Act, the FDA approved Exondys-51 (eteplirsen), the first treatment for Duchenne Muscular Dystrophy (“DMD”), after prolonged disputes within the agency. 149 DMD is a severe form of muscular dystrophy associated with progressive muscle weakness and loss, manifesting in males between the ages of three and five. 150 Leading the charge on the approval of Exondys-51 was Director of the Center for Drug Evaluation and Research, Dr. Janet Woodcock, a vocal proponent of patient input. 151 The decision was controversial, as FDA staff and advisory committee members had urged that the drug had not been shown to be effective in clinical trials consisting of only 12 patients, with no placebo control group. 152 FDA Commissioner Robert Califf even issued a public memo describing the basis of the scientific disagreement underpinning the debate in an effort to defend Dr. Woodcock's decision. 153 The drug's approval was coupled with robust post-market clinical trial requirements under the guise of risk evaluation and mitigation strategies imposed on Sarepta Therapeutics. 154 The drug is projected to cost $300,000 a year and will treat approximately 13% of patients with DMD, those with a specific genetic mutation. 155
Although DMD is a rare disease, and Exondys-51 is tailored to a very narrow segment of the population, the debate and review of the drug was informed by intense patient participation. Public meetings in April 2016 were attended by hundreds of patient advocates, 85 of whom were slated to speak. 156 Reporters described the meetings as “emotionally charged” as young, wheelchair-bound patients described living with the disease. 157 In addition to calling for Exondys-51's approval, advocates implored the FDA to develop new standards for approving drugs for rare disorders, particularly those lacking any available treatments like DMD. 158 As one commentator said, the road to approval for Exondys-51 “was a test case for the increasing power of patient advocacy in drug development and approvals, which is why advocates for patients with other rare diseases, such as spinal muscular atrophy, were paying close attention.” 159
The recent efforts within the FDA, and legislation like the 21st Century Cures Act, have affirmatively invited patient voices into the regulatory process. It remains to be seen just how this process will be implemented, and how the agency will respond to increasing patient perspectives and patient-generated information as positioned against long-standing requirements for product approval. There are also critical questions regarding relationships between patient advocacy groups and the regulated industry, with many drug companies actively funding these groups or partnering with them on research initiatives. However, despite the uncertainty, these developments should enhance the scope of FDA's assessment of promising new treatments.
Footnotes
1
The use of the overarching term “pharma” here is intended to include several types of medical products regulated by the FDA that were addressed in the 21
3
U.S. F![]() ] (last updated Jul. 7, 2017).
] (last updated Jul. 7, 2017).
4
The FDA regulates food (including dietary supplements), cosmetics, human and animal drugs, biological products, medical devices, products emitting radiation, and tobacco products. 21 U.S.C. § 301-399(h).
5
Wallace F. Janssen, The Story of the Laws Behind the Labels, FDA C
6
A drug is defined as “(A) articles recognized in the official United States Pharmacopoeia, official Homoeopathic Pharmacopoeia of the United States, or official National Formulary, or any supplement to any of them; and (B) articles intended for use in the diagnosis, cure, mitigation, treatment, or prevention of disease in man or other animals; and (C) articles (other than food) intended to affect the structure or any function of the body of man or other animals; and (D) articles intended for use as a component of any article specified in clause (A), (B), or (C).” Federal Food, Drug, and Cosmetic Act § 201(g), 21 U.S.C. § 321(g) (2016). A “new drug” is one that adheres to the general definition of a drug, but is not generally recognized as safe and effective among experts that are qualified by scientific experience and training or has not been used for a material extent under particular conditions. Id. § 321(p). For new drugs, premarket approval is required through the new drug approval process. Id. § 355.
7
A medical device is defined as “an instrument, apparatus, implement, machine, contrivance, implant, in vitro reagent, or other similar or related article, including any component, part, or accessory, which is—(1) recognized in the official National Formulary, or the United States Pharmacopeia, or any supplement to them, (2) intended for use in the diagnosis of disease or other conditions, or in the cure, mitigation, treatment, or prevention of disease, in man or other animals, or (3) intended to affect the structure or any function of the body of man or other animals, and which does not achieve its primary intended purposes through chemical action within or on the body of man or other animals and which is not dependent upon being metabolized for the achievement of its primary intended purposes.” Id. § 321(h).
8
The FDA is tasked with regulation of biological products in the Public Health Service Act. New drugs are chemically synthesized, while biological products are naturally-derived and defined as a “virus, therapeutic serum, toxin, antitoxin, vaccine, blood, blood component or derivative, allergenic product, protein (except any chemically synthesized polypeptide), or analogous product, or arsphenamine or derivative of arsphenamine (or any other trivalent organic arsenic compound), applicable to the prevention, treatment, or cure of a disease or condition of human beings.” Public Health Service Act § 351(i), 42 U.S.C. § 262(i) (2018).
9
O
10
For a description of the legislative provisions creating PCORI, see A
11
About the All of Us Research Program, N![]() ].
].
12
About the FDA Patient Education Network, F![]() ].
].
13
For Patients, F![]() ].
].
14
Sue Sutter, FDA's 21![]() ].
].
15
Reporting Serious Problems to FDA, F![]() ].
].
16
CDRH Patient Engagement, F![]() ].
].
17
Patient Preference Initiative, F![]() ].
].
18
The PEAC held its first meeting in October 2017. See Section IV.B, infra.
19
20
Id., at 6.
21
Id. For an informative blog post detailing the final guidance on PPI and patient-centered activities at FDA, see McKenzie E. Cato & Allyson B. Mullen, FDA Finalizes Guidance Regarding Patient Preferences Information for Medical Device Submissions, H![]() ].
].
22
Establishment of the Patient and Care-Partner Connection; Establishment of a Public Docket; Request for Comments, 81 Fed. Reg. 78169 (Nov. 7, 2016).
23
24
Id.
25
Id. at 7.
26
27
2016-2017 S
28
See M![]() ].
].
29
30
Patient Affairs Staff, U.S. F![]() ].
].
31
32
Id.
33
Citizen Science, N![]() ].
].
34
See About, C![]() ]. The website emphasizes crowdsourcing as one key aspect of citizen science efforts.
]. The website emphasizes crowdsourcing as one key aspect of citizen science efforts.
35
Citizen Science Definition, C![]() ] (quoting the 2014 Oxford Dictionary).
] (quoting the 2014 Oxford Dictionary).
36
2016-2017 S
37
R
38
S
39
Moore v. Regents of the Univ. of Cal., 51 Cal. 3d 120 (Cal. 1990), cert. denied, 499 U.S. 936 (1991).
40
Id. at 125.
41
Id. at 126.
42
Id. at 127.
43
Id. at 128-29.
44
Id. at 148-49.
45
Id. at 131-32.
46
Dennis McLellan, Obituaries: John Moore, 56; Sued to Share Profits from His Cells, L.A. T
47
Moore, 51 Cal. 3d at 168-70.
48
Greenberg et al. v. Miami Children's Hosp. Research Inst., 264 F. Supp. 2d 1064 (S.D. Fla. 2003).
49
Id. at 1067-68.
50
Id. at 1068.
51
Press Release, Canavan Found., Nat'l Tay-Sachs & Allied Diseases Ass'n (Sept. 23, 2003) (on file with author).
52
Alessandra Colaianni et al., Impact of Gene Patents and Licensing Practices on Access to Genetic Testing and Carrier Screening for Tay-Sachs and Canavan Disease, 12 G
53
Wash. Univ. v. Catalona, 437 F. Supp. 2d 985 (E.D. Mo. 2006).
54
Id. at 993.
55
Id. at 997.
56
Wash. Univ. v. Catalona, 490 F. 3d 667 (8th Cir. 2007), cert denied, 552 U.S. 1166 (2008).
57
For an excellent account of the history and the procedural posture of the cases, see Katherine Drabiak-Syed, Lessons from Havasupai Tribe v. Arizona State University Board of Regents: Recognizing Group, Cultural, and Dignitary Harms as Legitimate Risks Warranting Integration into Research Practice, 6 J. H
58
Tilousi v. Ariz. State Univ. Bd. of Regents, No. CV2005-013190, 2006 WL 4642922 (Ariz. Super. Feb. 7, 2006).
59
Havasupai Tribe v. Ariz. State Univ. Bd. of Regents, 204 P.3d 1063 (Ariz. Ct. App. 2008).
60
Id. at 1066-67.
61
Drabiak-Syed, supra note 57, at 195.
62
See, e.g., Diana Bloom et al., The Rules of Engagement: CTTI Recommendations for Successful Collaborations Between Sponsors and Patient Groups Around Clinical Trials, 52 T
63
See, e.g., Judith G. Hall, The Role of Patient Advocacy/Parent Support Groups, 103 S. A
64
Oonagh Corrigan & Richard Tutton, What's in a Name? Subjects, Volunteers, Participants, and Activists in Clinical Research, 1 C
65
Sharon F. Terry et al., Advocacy Groups, supra note 63, at 160.
66
Eliot Marshall, Patient Advocate Names Co-Inventor on Patent for the PXE Disease Gene, 305 S
67
See Paradise, supra note 62 (providing an analysis of the patent law regarding inventorship).
68
Marshall, supra note 66.
69
H.R. 6, 114th Cong. (1st Sess. 2015).
70
71
H.R. 6.
72
Jennifer Steinhauer & Robert Pear, Sweeping Health Measure, Backed by Obama, Passes Senate, N.Y. T
73
21st Century Cures Act, Pub. L. No. 114-255, 130 Stat. 1033 (2016).
74
Michael McCaughan, FDARA, 21
75
See, e.g., Sy Mukherjee, Everything You Need to Know About the Massive Health Reform Law that Just Passed Congress, F
76
21st Century Cures Act § 3032.
77
Right to Try in Your State, G![]() ].
].
78
Id.
79
Jordan Paradise, FDA Guidance to Industry Streamlines Physicians' Compassionate Use Requests, H![]() ].
].
80
21 C.F.R. § 312 (2017); Paradise, supra note 79.
81
See, e.g., Michael Cipriano, Right-To-Try Legislation Must Change Language to Narrow Spectrum of Patients, Gottlieb Says, P
82
The Act defines “regenerative medicine therapy” as including “cell therapy, therapeutic tissue engineering products, human cell and tissue products, and combination products using any such therapies or products, except for those regulated solely under section 361 of the Public Health Service Act and part 1271 of title 21, Code of Federal Regulations.” 21st Century Cures Act, Pub. L. No. 114-255, § 3033, 130 Stat. 1033, 1103 (2016).
83
Id. § 3035.
84
Id. § 3036.
85
Id. § 3033.
86
Id. § 3034.
87
FDA Announces Comprehensive Regenerative Medicine Policy Framework, U.S. F![]() ].
].
88
89
Michael Cipriano, US FDA's Drug Seizures Seen as Most Significant Aspect of Stem Cell Crackdown, P
90
See Jordan Paradise, Cultivating Innovation in Precision Medicine through Regulatory Flexibility at the FDA, 11 N.Y.U. J.L. & L
91
For FDA's Biomarker Qualification Program and the list of qualified biomarkers, see Biomarkers at CDER, U.S. F![]() ] (last updated Oct. 11, 2017).
] (last updated Oct. 11, 2017).
92
U.S. F
93
The FDA has issued breakthrough devices draft guidance, implementing § 515B of FDCA created by § 3051 of the Cures Act and § 901 of FDA Reauthorization Act of 2017, Pub. L. 115-52. Breakthrough Devices Program; Draft Guidance for Industry and Food and Drug Administration Staff; Availability, 82 Fed. Reg. 49,373 (Oct. 25, 2017); U.S. F![]() .
.
94
95
Patient experience data is defined as data that “are collected by any persons (including patients, family members and caregivers of patients, patient advocacy organizations, disease research foundations, researchers, and drug manufacturers)” and “are intended to provide information about patients' experience with a disease or condition, including – (A) the impact of such disease or condition, or a related therapy, on patients' lives; and (B) patient preferences with respect to treatment of such disease or condition.” 21st Century Cures Act, Pub. L. No. 114-255, § 3001, 130 Stat. 1033, 1084 (2016).
96
Id.
97
Id.
98
Id. § 3002(a)-(b).
99
Id. § 3004.
100
Sue Sutter, Patient Experience Data May Require Separate Label, Genentech Suggests, P
101
Drug Development Tools Qualification Program, U.S. F![]() ].
].
102
21st Century Cures Act § 3011.
103
Id.
104
Id.
105
Id.
106
David E. Paul & Catherine Clements, Getting by with a Little Help from Their Friends: FDA Using External Experts to Enhance Biomarker Qualification and Enhance Precision Medicine, 72 F
107
21st Century Cures Act § 3022.
108
Id.
109
Id.
110
Id.
111
Id.
112
Id. § 3051.
113
Food and Drug Administration Safety and Innovation Act of 2012, Pub. L. No. 112-144, § 902, 126 Stat. 993, 1086-1087 (2012). Breakthrough therapy status signals that the drug is progressing through clinical trials subject to the statutory provisions provided for breakthrough therapies, not that the drug has been approved by the FDA. The FDA defines a breakthrough therapy as a drug “intended alone or in combination with one or more other drugs to treat a serious or life threatening disease or condition and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development.” Fact Sheet: Breakthrough Therapies, U.S. F![]() ]. This language tracks that used in the statute.
]. This language tracks that used in the statute.
114
115
A table within the FDA's breakthrough therapy guidance document compares the four expedited mechanisms. Id. at 11.
116
Congress directs the FDA to focus breakthrough status on medical devices “that provide for more effective treatment or diagnosis of life-threatening or irreversibly debilitating human disease or conditions … that represent breakthrough technologies … for which no approved or cleared alternatives exist … that offer significant advantages over existing approved or cleared alternatives, including the potential, compared to existing approved alternatives, to reduce or eliminate the need for hospitalization, improve patient quality of life, facilitate patients' ability to manage their own care (such as through self-directed personal assistance), or establish longterm clinical efficiencies; or … the availability of which is in the best interest of patients.” 21st Century Cures Act § 3051.
117
B
118
Enhancing Patient Engagement Efforts Across the Food and Drug Administration; Establishment of a Public Docket; Request for Comments, 82 Fed. Reg. 13,632 (Mar. 14, 2017).
119
Id. at 13,633.
120
Id. at 13,633-34.
121
Derrick Gingery, Patient Advocates Continue to Push US FDA for Central Office, 79 P
122
Brenda Sandburg, Novartis CAR-T Therapy's Swift Approval Aided by REMS and New US FDA Review Model, 79 P
123
Id. (quoting Commissioner Scott Gottlieb, M.D.).
124
FDA Therapy Brings First Gene Therapy to the United States, U.S. F![]() ]; see Michael Cipriano, FDA's Gottlieb Pushing ‘Seamless’ Clinical Trials for Faster Development, P
]; see Michael Cipriano, FDA's Gottlieb Pushing ‘Seamless’ Clinical Trials for Faster Development, P
125
126
21st Century Cures Act, Pub. L. No. 114-255, § 3032, 130 Stat. 1033, 1084 (2016).
127
Derrick Gingery, FDA Ends Regularly Scheduled Patient-Focused Drug Development Meetings, P
128
U.S. F
129
Id. at 3.
130
Sutter, supra note 14, at 17.
131
132
For a discussion of agency considerations leading up to issuance of the guidance, see Cole Werble, Real-World Evidence: Advice, Principles and Examples Emerge from FDA, P
133
Id. at 10.
134
Id. at 12.
135
Statement by FDA Commissioner Scott Gottlieb, M.D. on New Steps by FDA to Advance Patient Engagement in the Agency's Regulatory Work, U.S. F![]() ].
].
136
137
Statement by FDA Commissioner Scott Gottlieb, M.D., supra note 135; Patient Engagement Advisory Committee, U.S. F![]() ] (last updated July 25, 2017) (giving advice to the Commissioner or designee, on complex issues relating to medical devices, the regulation of devices, and their use by patients).
] (last updated July 25, 2017) (giving advice to the Commissioner or designee, on complex issues relating to medical devices, the regulation of devices, and their use by patients).
138
Advisory Committee; Patient Engagement Advisory Committee, 82 Fed. Reg. 50,882 (Nov. 2, 2017).
139
U.S. F
140
FDA Reauthorization Act of 2017, Pub. L. No. 115-52, § 901, 131 Stat. 1005, 1077-78 (2017).
141
U.S. F
142
See, e.g., Thomas M. Burton, FDA Plans New Medical Device Approval Process, W
143
Patient Affairs Staff, supra note 30.
144
Patient Engagement Collaborative, U.S. F![]() ] (last updated Dec. 22, 2017).
] (last updated Dec. 22, 2017).
145
Patient Affairs Staff, supra note 30.
146
Id.
147
Strategic Plan, C![]() ].
].
148
U.S. F
149
Sy Mukherjee, The FDA Just Made Its Most Controversial Drug Approval of the Year, F![]() ].
].
150
W. Douglas Biggar, Duchenne Muscular Dystrophy, 27 P
151
Jeff Buchanan, Bio Execs Talk Patient Advocacy, Duchenne Approval at BioForward Panel, E![]() ].
].
152
153
Mukherjee, supra note 149.
154
Weisman, supra note 152.
155
Id.
156
157
Weisman, supra note 152.
158
Id.
159
Buchanan, supra note 151.