
Abstract
I. INTRODUCTION
Advances abound in biotechnology and biomedicine, and cutting-edge clinical research is transforming medical practice by the minute. 1 While benefits are quite likely, biomedical research with people who suffer from mental illness 2 must include enhanced protections to guard against harms to this potentially vulnerable population. Notions of harmful, abusive practices in psychiatric research and practice bring to mind the infamous eugenics movement of the early twentieth century; 3 unfortunately, however, abuse is not merely a thing of the distant past. In 2003, a young man with severe mental illness allegedly was coerced by his psychiatrist, against the wishes of his mother, to participate in “the CAFÉ study,” a clinical trial comparing atypical antipsychotics, including Seroquel, in first-episode psychosis; the study was conducted within the University of Minnesota Department of Psychiatry and sponsored by AstraZeneca, the manufacturer of Seroquel. 4 In 2004, while still enrolled in the study and taking Seroquel, the young man committed suicide by violent and gruesome means. 5 The State of Minnesota commissioned a 2015 report that showed evidence of coercive enrollment, inadequate supervision of both subjects and study personnel, conflicts of interest, and numerous misrepresentations and unethical cover-ups. 6 Though some bioethics and mental health policy professionals have signaled that human research protections for mentally ill people are insufficient, 7 any efforts to remedy deficiencies repeatedly miss the mark. The United States has never promulgated regulations or prescribed strict guidance on concrete approaches to addressing mental health vulnerabilities in clinical research; rather, vulnerability determinations have rested “on a common tradition of interpreting the regulations.” 8 This practice continues despite recent changes to the Common Rule. 9
Shortcomings in the regulatory management of biomedical research with people who suffer from mental illnesses are evident, especially considering the inclination of researchers, in practice, to narrowly focus on a participant’s consent-based decision-making capacity. 10 An exclusive focus on a mentally ill person’s decision-making capacity—as measured by standardized assessment instruments such as the MacCAT-CR) 11 —when contemplating their vulnerability to coercion or undue influence ignores other sources of vulnerability for this population. These vulnerabilities include the lived experience of low self-esteem resulting from stigma, 12 sometimes being feared 13 or discriminated against, 14 and social isolation. 15 Other contributions to vulnerability in this population include underemployment or unemployment, 16 housing insecurity, 17 “limited availability of providers, the affordability of health insurance, and the cost of drugs.” 18 Additional sources of vulnerability may include the mental illness itself and psychotropic drugs used to treat the illness, both potentially altering the patient-participant’s authentic self through their effects on thought processes and choices. 19 Further, the power imbalance within the psychiatrist-researcher patient-participant relationship—sometimes referred to as “power-relational vulnerability” or deferential vulnerability 20 —is another source of vulnerability that may go unrecognized. 21 Given the history of stigmatization and abuse against mentally ill people, both outside 22 and within the research context, 23 regulations and guidance should impose heightened protections for this population to ensure proper enrollment and continued participation in biomedical research.
To say that all potential participants with mental illness are vulnerable to coercion or undue influence casts too wide a net. 24 Yet, an approach that views all vulnerabilities to coercion or undue influence emanating from mental illness as arising only in the context of decision-making capacity, at least as this term currently is assessed and applied in practice, 25 is far too narrow. A middle ground is needed to appropriately protect people with mental illness in biomedical research. This issue is complicated and will surely require complex solutions.
This Article does not set out to solve all the problems, but it is an effort to start a conversation, offer observations on the problematic application of the Revised Common Rule (“rCR”) in the context of mental illness, and make some initial recommendations. Further, this Article primarily addresses research with psychiatric patients who are not involuntarily hospitalized or experiencing active psychosis and whose decision-making capacities are not obviously compromised. 26 Part II of this Article provides a brief history of the Common Rule and relevant changes in the rCR, highlighting the lack of clarity on the meaning and parameters of “impaired decision-making capacity” and who is “vulnerable to coercion or undue influence” in the context of mental illness. Challenged here are assumptions that impaired decision-making capacity, as currently assessed and applied in practice, is and must be the rCR’s exclusive framework for assessing vulnerability to coercion or undue influence in potential participants suffering from mental illness. Part III discusses how the long-awaited changes to the Common Rule provide little clarity on who is vulnerable to coercion or undue influence outside four specifically named categories, what vulnerability of this type looks like, or how such vulnerability should be determined. Part IV maintains that absent firm leadership and guidance from the U.S. Department of Health and Human Services (“HHS”), expertise is needed regarding the unique circumstances of participants in psychiatric research. Part IV also contemplates sources of expertise, e.g., the psychiatrist who treats mental illness, the patient who suffers from and lives with mental illness, and the mentally ill person who already has served as a subject in biomedical mental health research. Part V suggests new language for binding guidance or further rule revisions. A final suggestion is to modify one scholar’s proposal to include research subjects in the research review process, proposing that if specific federal research regulations and guidance do not materialize, the next best alternative is to focus on who is at the institutional review board (“IRB”) table interpreting existing regulations.
II. THE COMMON RULE THEN AND NOW: CHANGES PROVIDE LITTLE CLARITY
A. Efforts to Solidify Protections
Despite several attempts between the 1970s and 1990s to provide greater protections in biomedical research for people suffering from “mental disorders,” 27 the Common Rule’s codification in 1991 28 made no mention of people who suffer from mental illness and only mentioned the “mentally disabled.” 29 In 1996, the National Bioethics Advisory Commission (“NBAC”) began working to study the issue of “mental disorders” in the context of research participation and to formulate possible solutions to address voids in protections. 30 In December 1998, NBAC issued its report, Research Involving Persons with Mental Disorders That May Affect Decisionmaking Capacity. 31 NBAC limited its inquiry to decision-making capacity, ignoring other types of vulnerability arising in mental illnesses or “mental disorders.” 32 NBAC’s first recommendation related to IRBs and how, in order to close gaps and extend appropriate protections to people suffering from “mental disorders,” IRBs should be tailored to properly represent these potential participants’ interests. 33 Specifically, Recommendation I states:
All IRBs that regularly consider proposals involving persons with mental disorders should include at least two members who are familiar with the nature of these disorders and with the concerns of the population being studied. At least one of these IRB members should be a member of the population being studied, a family member of such a person, or a representative of an advocacy organization for this population. 34
Official guidance based on these 1998 recommendations would have been appropriate, but federal regulators issued no guidance specifically limiting risks to which mentally ill participants might be exposed in biomedical research. 35
Due to the heterogeneity of people who suffer from mental illnesses, and the variability of mental illnesses even within diagnostic categories, a detailed, one-size-fits-all rule may have been beyond realistic expectation. 36 But the fact that a task is challenging does not warrant avoiding or abandoning attempts to address it. Nearly thirty years after implementation of the original Common Rule, and over twenty years since the NBAC report, rather than mending inadequacies, the recent changes under the rCR 37 have made an already flawed regulatory framework even more out of sync with safeguarding people with mental illness who may need heightened protections in biomedical research. One major shortcoming of the rCR is that it gives IRBs more responsibility and discretion in deciding what it means to have “impaired decision-making capacity,” to whom that criteria should apply, and under what circumstances. 38 This approach allows for inconsistencies based on who is sitting at the IRB table on any given day, at any given institution. As discussed later, the IRB can play a significant role in addressing what is lacking in the rCR, 39 so increased IRB responsibility should not be criticized. Yet, IRB discretion in carrying out increased responsibility ad hoc should be curbed, rather than expanded, through binding guidance or modified regulation.
B. Absence of “Mental Illness ” in Original and Revised Common Rule
Very early in the rulemaking process, drafts of what would become the original Common Rule referenced the “mentally infirm,” 40 though ultimately this term was deleted from the final rule. The term “mentally disabled” is the closest approximation to mental illness in the original Common Rule. 41 Who was “mentally disabled” or what constituted a mental disability was never properly defined under the original rule, and whether or not it was intended to include people with mental illness is unknown. 42 The Americans with Disabilities Act definition of “disability” includes a “mental impairment that substantially limits one or more major life activities of an individual,” 43 yet the term “mental disability” has many mainstream connotations, including congenital brain abnormalities and cognitive deficits from brain damage or neurodegenerative disease. 44 The mystery as to the meaning of “mentally disabled” in the Common Rule is moot, as this term was stricken in the recent revision, shown here:
45 C.F.R. § 46.107 IRB membership.
(a) … If an IRB regularly reviews research that involves a vulnerable category of subjects pregnant women, or handicapped mentally disabled
…
(£issues which
Other notable changes in the rCR include the addition of those with “impaired decision-making capacity” as one example of individuals who may be vulnerable to coercion or undue influence, as well as instruction regarding possible IRB composition. 46 Mental illness is mentioned nowhere. 47
C. Impaired Decision -Making Capacity : An Exclusive Lens For Viewing Mental Illness ?
The new but likewise vague concept “impaired decision-making capacity” now substitutes for “mentally disabled.” 48 The rCR groups individuals with impaired decision-making capacity with other categories of prospective subjects, “such as children, prisoners, … [and] economically or educationally disadvantaged” people, when describing the types of subjects meant to be included in those “vulnerable to coercion or undue influence.” 49
Before the Common Rule revisions, relevant literature and analyses of the propriety of enrolling mentally ill people in research rested primarily on concerns about decision-making capacity. 50 In both the original rule and the rCR, however, the use of “such as” in 45 C.F.R. §§ 46.107, 46.111 indicates that the list of vulnerable groups is neither exhaustive nor final. 51 The rCR allows for subjects who suffer from mental illness but who do possess traditional decisional capacity to not be considered vulnerable in the clinical research setting. But, intended or not, the rCR’s “such as” language also implies that factors besides impaired decision-making capacity may affect a person’s vulnerability to coercion or undue influence; that is, sometimes people who suffer from mental illness may fairly be considered a vulnerable, unnamed group under the rCR for reasons other than impaired decision-making capacity. Excluding bases outside traditional notions of decisional capacity, as it is assessed and applied in practice, in determining vulnerability to coercion or undue influence in this population makes simplistic and even harmful assumptions about the experience of mental illness. 52 A mentally ill person might possess traditional decision-making capacity based on a standard assessment and still be vulnerable to coercion or undue influence in biomedical research, and, thus, need additional, heightened protections. 53
D. Why “Impaired Decision -Making Capacity ” is too Limited
Under the rCR, specific categories of subjects deemed to be per se vulnerable to coercion or undue influence—children, prisoners, and economically and educationally disadvantaged people 54 —are readily discernable: a child is a person under age 18, a prisoner is an incarcerated person, and determining a person’s financial means and education level is a straightforward task. The same cannot be said of the category “individuals with impaired decision-making capacity.” 55 Categories of individuals vulnerable to coercion or undue influence can extend beyond those named in the rule; but, of those explicitly listed, “individuals with impaired decision-making capacity” is the one category with uncertain meaning. What about a person who has impaired decision-making capacity makes them vulnerable to coercion or undue influence? Where does mental illness fall within this category, if at all? Should “mental illness,” standing alone, qualify as a non-enumerated category left open under the “such as” language in 45 C.F.R. §§ 46.107, 46.111? 56 As stated above, if a person is mentally ill but has decision-making capacity, they may still be vulnerable to coercion or undue influence under the rCR.
Numerous sources of vulnerability to coercion or undue influence for those suffering from mental illness are less apparent than common understandings of impaired decision-making capacity, yet no less important. 57 Living with mental illness in a society that misunderstands, fears, and stigmatizes mental illness gives rise to all sorts of vulnerabilities to coercion or undue influence. 58 Some of the symptoms experienced by people suffering from mental illness include despair, guilt, 59 “ambivalence, diminished motivation, disengagement, or impulsivity,” 60 somatic disturbances, and suicidality. 61 Major depression causes “diminished ability to think or concentrate, or indecisiveness.” 62 In 1997, Professor Carl Elliott aptly wrote: “When a person is caught in the grip of depression, his values, beliefs, desires, and dispositions are dramatically different from when he is healthy. In some cases, they are so different that we might ask whether his decisions are truly his.” 63 In fact, because “symptoms can cloud a person’s judgment,” psychiatrists often “advise patients not to make major life choices while experiencing a depressive episode.” 64 Further, psychotropic drugs used to treat mental illness may affect thinking, behavior, values, judgment, and risk-taking assessments—in essence, these drugs may alter one’s personality, for better or worse—thereby distorting the potential research subject’s true self. 65 Furthermore, mental illness can lead to extreme isolation and loneliness, 66 and participation in biomedical research might provide an inappropriate or false sense of belonging and fellowship in a time of psychiatric crisis or ongoing distress. 67 Ultimately, “even the most well-informed and decisionally ‘fit’ individual cannot realize the spirit of informed consent if his or her ‘choice’ is inauthentic, symptom driven, compromised, or coerced.” 68
Many scholars concur that people suffering from mental illness or other conditions that impair decision-making capacity should not be enrolled in biomedical research without “sound scientific justification” for their inclusion. 69 Others believe that “[r]esearch decisional capacity” should not be determined by an assigned diagnosis or group membership, “but by characteristics unique to that person.” 70 Another body of literature questions whether people suffering from mental illness need any protection against their own potential decision-making deficiencies. 71 In all the above examples, the myopic emphasis on potential participants lacking or possessing decision-making capacity—and the narrow definition of decision-making capacity and common beliefs about its assessment in people with mental illness—ignores all other sources of vulnerability to coercion or undue influence in this population. Traditional decision-making ability may appear intact, but may be affected by other vulnerabilities to coercion or undue influence, including the mental illness, the influences of psychotropic drugs, and imbalances in power dynamics experienced between the patient-participant and psychiatrist-researcher. 72 These factors may go completely unrecognized in the widely accepted assessment of decision-making capacity in research, the MacCAT-CR. 73
The rCR leaves open how people with mental illness should be viewed in the context of vulnerability to coercion or undue influence. 74 To cabin the mentally ill subject’s vulnerability within traditional notions of decision-making capacity is short-sighted, though it is the trend in both the literature and in practice. 75 The rule’s indecisiveness, however, provides an opportunity to expand protections and finally close the gaps originally identified by NBAC. 76 Suggested solutions on how to accomplish this are set forth later in this Article.
III. WHAT IS VULNERABILITY TO COERCION OR UNDUE INFLUENCE, AND WHO IS VULNERABLE IN THIS CONTEXT?
A. Common Definitions
“Coercion” and “undue influence” find their origins in the law. 77 The concept of “vulnerability,” however, is rooted much more in ethics and social sciences than in law. 78 The Common Rule and the rCR do not define any of these terms, 79 but reaching a clear understanding of their meanings and implications in biomedical research is essential. Yet, many IRBs appear to use the terms “coercion” and “undue influence” interchangeably, without differentiation. 80 It has been argued that monitoring traditional notions of overt “coercion” and “undue influence” in research is insufficient, because other factors—social, cultural, economic, and political realities—may make research participation less voluntary and more a necessity. 81
1. Coercion and undue influence in relation to mental illness
Though “coercion” and “undue influence” are undefined in the Common Rule and rCR, on its website, HHS discusses the need for investigators to avoid engaging in coercion and undue influence. 82 Coercion is described as follows:
Professor Jill Fisher asserts that limiting the concept of coercion to intentional acts fails to address the societal factors that force individuals to make choices they might otherwise not, absent their adverse circumstances. 84 The concept is described as “structural coercion” that has the potential to undermine the propriety of enrolling certain subjects in research. 85 Presented in the context of a person becoming a research participant out of desperation for a cure, for the purpose of obtaining money, or accessing general health care, the idea of “structural coercion” easily relates to psychiatric patients in research. Structural coercion takes into account that “broader power dynamics” outside the researcher-subject relationship “might infringe on the voluntariness of consent” 86 and prospective research participants might actually “turn to research in order to mitigate the threat of structural violence.” 87 Again, Fisher presents structural coercion in the context of monetary incentives for participation, or participation to obtain basic health care or a miraculous cure, exploring the space where societal inequalities may limit opportunities and choices for potential research participants. 88 In this setting, there is something tangible, e.g., money, health care or experimental “treatment,” that the participant lacks and desperately needs. 89 Structural coercion aptly applies to people who live with mental illness, a population that experiences housing insecurity, underemployment and unemployment, and insufficient treatment options. 90 In the case of the psychiatric patient-participant, beyond a need for sources of income, mental health care and treatments, reasons for participating in research might include a sense of belonging to something, a yearning for human interaction, and even feelings of friendship (e.g., with study staff) 91 after years of social isolation.
HHS describes “undue influence” as arising in the context of inappropriate rewards, but also as present in other instances in more subtle form. 92 For example, HHS notes that where undue influence depends on a specific individual’s situation, “it is often difficult for IRBs to draw a bright line delimiting undue influence” and that the IRB must “use its discretion in determining which circumstances give rise to undue influence.” 93 This task becomes difficult because IRBs in most circumstances do not evaluate a particular participant’s vulnerability to undue influence, and influence or “justifiable persuasion” is not per se unacceptable in research enrollment. 94
The power imbalance between the patient-participant and psychiatrist-researcher may unduly influence a participant’s choices. 95 This possibility is not surprising, as common sense suggests that the psychiatrist holds sway over the patient’s decisions about psychiatric interventions. 96 For example, a participant in a qualitative study eliciting opinions from psychiatric patients about deep brain stimulation (“DBS”) testified: “I have a psychiatrist who I have been with for a long time who has been prescribing medications for me and treating me and, now if he were to advocate for [DBS], and he had good reasons, that would be more persuasive.” 97 This type of trust and deference can be expected to exist in most psychiatric clinician-patient and researcher-subject relationships, implicating concerns about voluntarism in consent. 98 Moreover, some scholars suggest an additional vulnerability: the distrust those suffering from mental illness often have in themselves. 99 True autonomy is hindered “when agents ‘doubt their own worth and ability to make appropriate choices.’” 100 Without considering this additional aspect of vulnerability—a lack of self-worth and self-trust—studies on how to counteract vulnerabilities of mentally ill participants will be incomplete and inherently flawed. 101
Other less recognized sources of undue influence include the influence of psychotropic medications and changes in personality and preferences due to mental illness. 102 While mental illness or psychotropic medication may not change participants’ decision-making ability, they may change the decision they make. 103 This scenario continues to be ignored under federal regulations designed to protect vulnerable people in human subjects research.
2. Vulnerability in relation to mental illness
The Common Rule and rCR point to “a vulnerable category” or “a category of subjects that is vulnerable to coercion or undue influence,” respectively, in three contexts: (1) IRB membership, 104 (2) equitable subject selection, 105 and (3) the potential need for additional safeguards in research involving vulnerable subjects. 106 Overall, the Common Rule did little to define vulnerability; instead, it “convey[ed] a consent-based conceptualization of vulnerability that lack[ed] internal clarity regarding its scope.” 107 This uncertain scope of vulnerability and the consent-based focus on decision-making capacity continue under the rCR. 108
For years scholars have attempted to forge meaning where little or no guidance exists. 109 The result is a disorganized, minimally useful literature focused on vulnerability. 110 The dictionary defines a “vulnerable” person as one capable of being physically or emotionally wounded, or open to attack or damage. 111 Worldwide, policies and guidelines on clinical research ethics rarely define “vulnerability,” but they generally “convey implicitly that vulnerability is fundamentally an inability to provide free and informed consent.” 112 Some assert that “mental illness creates an inherent vulnerability,” 113 while others maintain that such a notion risks overinclusion and furtherance of stigmatization and discrimination. 114
B. A Closer Look at the Origins of “Vulnerability ”
Authored by the National Commission, the Belmont Report was the first official influential writing to identify vulnerability as a factor requiring significant attention in clinical research ethics. 115 The report states that one necessary consideration in assessing justifiability of research with humans is:
(iv) When vulnerable populations are involved in research, the appropriateness of involving them should itself be demonstrated. A number of variables go into such judgments, including the nature and degree of risk, the condition of the particular population involved, and the nature and level of the anticipated benefits. 116
Under “Selection of Subjects,” the report states that research targeting particular groups gives rise to injustice. 117 These groups include:
racial minorities, the economically disadvantaged, the very sick, and the institutionalized … Given their dependent status and their frequently compromised capacity for free consent, they should be protected against the danger of being involved in research solely for administrative convenience, or because they are easy to manipulate as a result of their illness or socioeconomic condition. 118
The National Commission recommended requiring additional protections in human subjects research involving pregnant women, fetuses, neonates, prisoners, children, and the mentally infirm. 119 While every other category was listed explicitly as a vulnerable population in the final Common Rule, the rule did not prescribe heightened protections for institutionalized “mentally infirm” subjects due to “concern that [such protections] might block valuable and appropriate research.” 120 In its final 1991 iteration, the Common Rule mentioned subjects “‘likely to be vulnerable to coercion or undue influence,’ including mentally disabled persons,” 121 but, as noted above, did not define mental disability. 122
Since publication of the Belmont Report, legal and nonlegal policies and guidelines relating to clinical research ethics have expanded worldwide; along with this expansion, the meanings and conceptual scopes of vulnerability and vulnerable populations have branched in nuanced directions. 123 Scholars have put forth various interpretations. For example, one analysis suggests that vulnerability is an “additional susceptibility to research-related harm or risk, or that additional safeguards are needed to protect the potential participant from research-related risk or harm.” 124 Another approach imagines layers of vulnerability “which arise from interactions between an individual’s characteristics and their environment, and which interact with one another to create an inextricably context-dependent vulnerability.” 125
One of the more influential interpretations of vulnerability in human research divides vulnerability into six subcategories: “cognitive, juridic, deferential, medical, allocational, and infrastructural.” 126 Categories most relevant to people suffering from mental illness are cognitive vulnerability and deferential vulnerability. 127 Cognitive vulnerability that impairs decision-making capacity may be either permanent, as with Alzheimer’s disease or brain injury, or temporary, e.g., an episode of major depressive disorder. 128 Deferential vulnerability highlights that an individual could possess cognitive decision-making capacity but still be influenced by others’ opinions “such that they are not able to decide based on their own preferences and values.” 129 A power imbalance between the researcher and a subject suffering from mental illness could serve as fertile ground for deferential vulnerability. 130 In fact, scholarly literature acknowledges “that vulnerability is a relational feature, borne of power asymmetries between participants and research staff, investigators and institutions.” 131
Another conception of vulnerability asserts that all research subjects are vulnerable; this conception should be challenged, then dismissed. 132 The notion of universal vulnerability in clinical research—which can be described as a “categorical claim” of vulnerability—is “both clearly right and fundamentally problematic.” 133 While all human beings are susceptible to harm, ascribing vulnerability to all human subjects serves to “undermine rather than promote” protections for clinical research subjects. 134 Such a generalized definition supports the need for research regulation in general, 135 but if we insist on employing “special protections” for all subjects, then we are “providing special protections for no one.” 136 It is argued, however, that attempts to formulate specific lists of vulnerable populations can lead to stigmatization and the harmful suggestion that persons on these lists are “everywhere and always” incapable of taking care of themselves and their interests. 137 The Canadian Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (“TCPS2”) states that “individuals should not automatically be considered vulnerable simply because of assumptions made about the vulnerability of the group to which they belong.” 138
Lists and categories may strip individuals of autonomy not only in the research setting, but in other areas of life as well. 139 While categories may be problematic, so too is the current “IRB free-for-all” in interpreting U.S. federal regulations 140 as they relate to people who suffer from mental illness. 141 Without lists, firm definitions, or guidance, a category of subjects may be deemed “vulnerable to coercion or undue influence” at one institution on a given day and “not vulnerable to coercion or undue influence” at another institution, or even the same institution, the very next. Erring on the side of more protections may be better than insufficient and inconsistent protections. 142 Requiring consideration of heightened protections should not stymie research with mentally ill participants, but should aim to add structure and consistency to the research endeavor so those who might need extra protections are afforded them.
To counter the risk for “over-inclusiveness” in describing people who require additional protections in research, some scholars rely on comparative and contextual analyses. 143 A comparative approach to defining vulnerability highlights that protections needed for a particular subclass may be more than are necessary for the class as a whole. 144 A contextual analysis additionally contemplates under what circumstances this particular subclass requires additional protections. 145 Another relevant consideration is “situational” vulnerability, which involves temporary vulnerability. 146
C. Voluntarism must be Considered in Assessing Mentally ill Participants ’ Vulnerabilities to “Coercion or Undue Influence ”
Bioethicists have conjured numerous interpretations and conceptions of what it means to be vulnerable, which makes it all the more remarkable that most interpretations of the Common Rule and rCR employ impaired decision-making capacity 147 as the sole criterion for determining mentally ill participants’ vulnerability to coercion or undue influence. 148 Again, while specifically naming persons who are vulnerable—prisoners, children, educationally or economically disadvantaged individuals, as well as individuals with impaired decision-making capacity—the introductory language “such as” clearly leaves the field open. 149 Impaired decision-making capacity is but one example of vulnerability to coercion or undue influence: 150 whether or not this was the intent of those who drafted the rCR, the words “such as” are akin to the legalese “including but not limited to.”
Asserted earlier in the Article, the need for additional protections for participants suffering from mental illness may not necessarily arise from an impairment in decision-making ability, but rather from a sometimes undetectable susceptibility to coercion or undue influence from a variety of sources. 151 For these individuals, the effects of mental illness, psychotropic medications, power dynamics, and “structural coercion” 152 may not alter their ability to make a decision, but can change the decision they make. 153 The rCR ignores this possibility, not necessarily as written but as interpreted and applied in practice.
This type of susceptibility—the risk of altered decision-making—is the very type of situation where the concept of “voluntarism” is implicated. 154 Professor Laura Weiss Roberts asserts that informed consent has three components: information, decisional capacity, and voluntarism. 155 Voluntarism is “the individual’s ability to act in accordance with one’s authentic sense of what is good, right, and best in light of one’s situation, values, and prior history,” and “involves the capacity to make [choices] freely and in the absence of coercion.” 156 Unfortunately, voluntarism is often overlooked, if considered at all. 157 Instances may arise where, for example, mental illness or psychotropic medications unduly influence thought processes, preferences, and judgments and may, in fact, alter the patient’s decision to participate in clinical research. 158 Under these circumstances, choices may not be truly voluntary because they do not reflect the participant’s true self. 159 Due to these concerns, the concept of voluntarism should be a key factor in determining a mentally ill participant’s vulnerability to coercion or undue influence.
IV. CONSULTING THE EXPERTS
One scholar suggests that appropriate protections for research participants need not focus on the “concept of vulnerability” or involve attempts to create lists or categories of vulnerable populations. 160 Instead, this scholar argues that experts must develop guidelines to determine group and individual vulnerabilities based on the contexts of particular studies and certain circumstances, and then formulate context-specific protections. 161 This approach relies on “expertise regarding the specific individuals and contexts in question.” 162 But, it raises obvious questions: How much representation of individual participants is feasible? What is meant by expertise? Who is an expert? Might expertise differ based on context? And finally, is the expert the psychiatrist or the psychiatric patient? To answer this last question, perhaps both individuals possess expertise that is complementary but not necessarily overlapping. Another source of expertise might be leaders at HHS, the National Institutes of Mental Health, and mental health advocacy groups.
A. The Experienced Research Participant
One novel proposal suggests that experienced research participants have expertise, and directly engaging them in conversation will better inform research ethics and oversight. 163 This approach recommends appointment of experienced research subjects to research ethics and policy development committees and IRBs. 164 Alternatively, institutions could establish advisory groups of research participants with varied experiences who could be called upon for specific issues by their human subjects protection programs. 165 More generally, it is asserted that engaging research participants with first-hand experiences is necessary to develop research ethics and policy and to strengthen the factual and moral bases of guidelines and regulations. 166
Some challenges of this proposal are readily apparent. The recommendation of including research subjects as IRB members may be unrealistic for certain populations, such as those in studies on terminal diseases. 167 For these groups, an unfortunate but inevitable attrition rate would deplete the pool of individuals available to serve as IRB members. Participants in studies implicating stigmatized diseases—e.g., clinical trials for antidepressant drugs—could experience repercussions in their personal, social, and professional lives if it is somehow disclosed that they serve as a representative of those suffering from mental illness. 168 For someone carrying the burden of mental illness and trying to get well or maintain wellness, this may be too much to ask.
B. Representation Through Empirical Research
Another approach suggests accessing the expertise of veteran research participants less directly, relying on empirical research as the preferred method of including participants’ views. 169 Built into this empirical research, however, is a power imbalance between researchers and participants. 170 With empirical studies that “express” the affected population’s perspectives, the “research community remains in control of the research and continues to determine its appropriateness, and research participants remain outside of the room except for their indirect voices in the data.” 171 This point warrants repeating: ethics research on clinical research subjects is framed and interpreted by researchers. 172 And inherent in research design are the “‘value judgments’ that necessarily reflect the background beliefs, the vested interests and the ideology of the investigator.” 173 Nonetheless, a recent qualitative study, hereafter “the Lawrence study,” is a fine example of indirect representation through examining depressed patients’ attitudes about DBS, an experimental intervention for treatment-resistant depression. 174 Psychiatry has a tempered hopefulness about the effectiveness of DBS, but optimism is based on inconsistent results seen in case reports and small open-label trials with no control groups. 175 The limited data on efficacy raises “ethical questions about vulnerability” in potential DBS patients. 176 Recognizing concern within the research community about unrealistic hopes, feelings of desperation, or inability to adequately weigh risks and benefits, the Lawrence study interviewed treatment-resistant depressed patients to assess “interest level, hopes, fears, and decision-making processes.” 177 Study participants appeared to understand the risks of DBS, were aware of their own limitations in processing information, and expressed cautious approaches to considering engagement in clinical research trials. 178
While qualitative studies often allow research participants opportunities for elaboration and originality of thought, the researcher devises the initial prompts. 179 Criticisms of the Lawrence study point out that the authors summarily and prematurely dismissed relational vulnerabilities, both “power-relational vulnerability” 180 and “identity-relational vulnerability.” 181 It is also suggested that participants in the Lawrence study should have been asked additional questions to fully analyze relational vulnerabilities and avoid misleading conclusions. 182 Even so, first-person accounts of prospective research participants who suffer from mental illness, and evidence-based research focused on their experiences, undoubtedly are valuable sources of information for mental health research. 183
C. Expertise on Institutional Review Boards
As shown in Part II, the rCR still requires consideration of including on IRBs those with knowledge about and experience working with subjects from potentially vulnerable categories. 184 IRB community members, however, can be quite seasoned by life experience or education, without having worked with a particular population. The rule’s “working with” requirement is an unnecessary limitation. Further, while the rCR requires that every IRB have at least one community member, 185 providing the opportunity to recruit community members experienced with particular populations, little evidence demonstrates that IRB community members are assigned to reviews based on their specific knowledge or interests. 186
It is possible to recruit and assemble a pool of IRB community members who have acquired expertise or highly relevant knowledge through various avenues, supplementary to or by means other than employment. 187 The discretionary mandate—effectively no mandate at all—that “consideration shall be given to the inclusion of one or more individuals who are knowledgeable about and experienced in working with these categories of subjects” is a missed opportunity to actually mandate or strongly encourage inclusion of the rich knowledge base accessible through targeted IRB community member recruitment and assignment. 188
V. POSSIBLE SOLUTIONS
A. What HHS Could /Should Do
HHS must either further revise the rCR or issue binding guidance on biomedical research with people who suffer from mental illness. Three points should be kept in mind: (1) some who live with mental illness or conduct research with this community assert that “it is stigmatizing to equate a mental illness with incapacity,” 189 that “no one-to-one relationship between a psychiatric disorder and decisional incapacity” exists, 190 and that it is inappropriate to label all people with mental illness as vulnerable; 191 (2) as interpreted and applied in practice, decisional capacity is the exclusive mechanism under the rCR for viewing the vulnerabilities to coercion and undue influence in people with mental illness; 192 and (3) individuals with mental illness can be deemed to have traditional decision-making capacity based on widely accepted assessments, but still be vulnerable to coercion or undue influence for other reasons. 193 HHS does not need to amend rCR language to designate all people who suffer from mental illness as vulnerable. This approach would likely be met with substantial pushback from researchers, 194 community advocacy groups, and perhaps many individuals who live with mental illness. But, the current use of “such as … individuals with impaired decision-making capacity” creates a catch-all category for vulnerabilities to coercion or undue influence arising from mental illness that is simply too narrow.
A rather straightforward proposal would be to amend the rCR by adding a reference to “subjects who are potentially vulnerable to coercion or undue influence, such as individuals who suffer from mental illness” in both “Criteria for IRB Approval of Research” at 45 C.F.R. §§ 46.111(a)(3), (b) and “IRB Membership” at 45 C.F.R. § 46.107. The use of “potentially vulnerable” would likely satisfy legitimate objections to labeling all people with mental illness as vulnerable to coercion or undue influence. Saying people with mental illness are potentially vulnerable to coercion or undue influence is less essentialist and judgmental than saying they are vulnerable, always.
Alternatively, HHS could bypass any need for additional formal rulemaking, instead issuing binding guidance to clearly address and fill the enduring gaps in protections for mentally ill people in biomedical research. 195 First, HHS should provide definitions or guidance on the rCR’s vague concepts, e.g., the parameters of being “vulnerable to coercion or undue influence.” HHS should also answer whether it intended for IRBs to exclude all factors beyond traditional notions of decision-making capacity when considering how to properly protect mentally ill participants against vulnerabilities to coercion or undue influence: if that was the department’s intent, this stance must be revisited. Without officially revising the regulation’s language, binding guidance could offer clarifications. Additionally, effective guidance related to operationalizing the charge to IRBs under 45 C.F.R. § 46.111(b), that would facilitate needed protections for mentally ill participants, might look something like the proposed guidance set forth in Figure 1 :
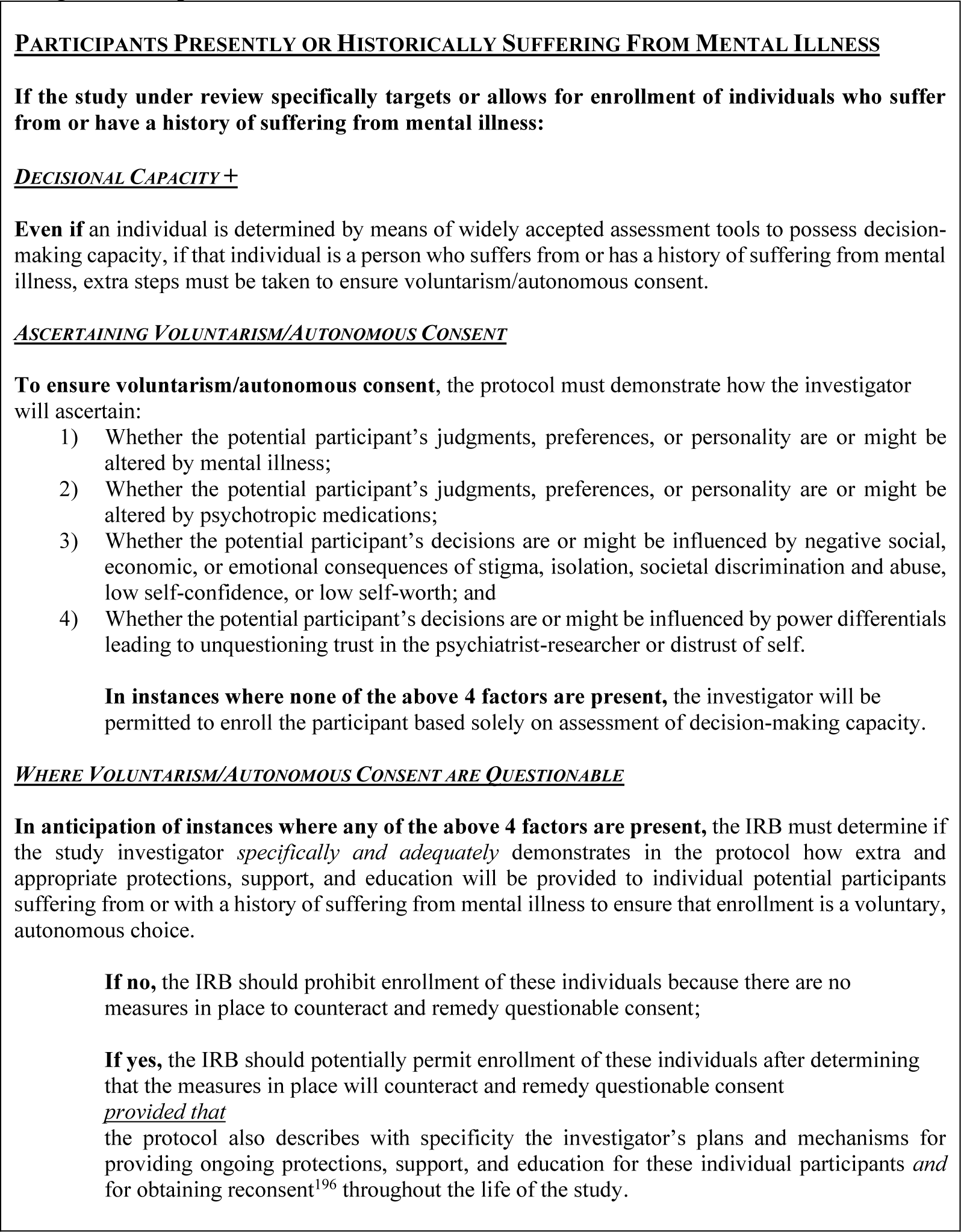
Proposed Guidance
To consistently and comprehensively implement this proposed guidance, IRBs and investigators would benefit from consensus on assessment of voluntarism/autonomous consent, and standardized tools such as template language for protocols and consents.
To realize additional well-informed and meaningful policy changes, HHS should assemble and seek advice from a panel of lay experts—people who live with, or have a close connection to another who lives with, mental illness. HHS should ask what members of this population want researchers to consider. Involving those who have experienced or witnessed psychiatric crises would be especially useful, as these individuals have meaningful perspective on living through decompensation and coming out the other side, and the effects of various interventions and circumstances along the way. While mental health advocacy organizations could also be consulted, any ties to large pharmaceutical corporations should disqualify such groups from providing input, as the sponsorship and influence of these corporations may lead to bias and conflicts of interest. 197 No solution will be perfect: the goal should be to craft policy approaches that first listen to those who have personal experience with mental illnesses, and then use information gathered to better protect this community in biomedical research. 198
B. People with Mental -Illness Experience are Integral to Research Review Process
People who have experienced a mental illness crisis and now manage their illness reasonably well truly know the vulnerability both of being in crisis and carrying the sometimes constant worry of relapse. 199 Recovery is a balancing act, and who would know better the competing forces and challenges of slogging through life with mental illness than those who live that experience each day? 200 The idea of involving affected populations in research related to their communities is not new. In fact, academic researchers in the United Kingdom are required, and private industry researchers strongly encouraged, to involve mentally ill people in research affecting their community. 201 Such approaches for involvement from the very early stages of research—even research idea generation—are admirable, but requiring such involvement in the United States would entail a major restructuring of how we conduct publicly funded research. While worthy of serious contemplation in the United States, extensive revamping of research regulations is beyond the scope of this Article and not a feasible option for promptly addressing the issues presented here. 202
In the absence of HHS revising the rCR, clarifying definitions or providing guidance on enrollment of mentally ill people in research, or in addition to such actions, this Article proposes a modification to how IRBs are assembled in order to enhance representation of potentially vulnerable mentally ill participants. The proposal could be implemented as a policy measure not subject to public comment and the official rulemaking process. A template exists in the National Institutes of Health’s (“NIH”) restructuring of its former institute-specific IRB system into a centralized Intramural IRB. 203 In eliminating institute-specific protocol reviews, the NIH implemented a mechanism to ensure scientific expertise is represented at each IRB table: physicians and scientists from the various institutes may be called upon for more technical, disease-specific reviews. 204 These specialists are considered “subject matter experts,” and whenever necessary, subject matter experts will be appointed to IRB panels. 205 A similar arrangement could be implemented in recruiting IRB community members.
NBAC’s 1998 recommendations to include people suffering from mental disorders or their advocates as IRB members were in line with historical international initiatives aimed at improving “the quality of research review by carefully attending to the concerns of particular communities of individuals” that may be vulnerable. 206 NBAC’s recommendations 207 reflected an awareness that family members of those who may not be available or able to serve on IRBs are in a unique position to share perspectives and represent certain otherwise voiceless segments of the population in research ethics determinations. 208 Likewise in 2008 to 2009, the Secretary’s Advisory Committee on Human Research Protections (“SACHRP”) approved similar recommendations by the Subcommittee on Inclusion of Individuals with Impaired Decision-making in Research (“SIIIDR”): “IRBs should give special consideration, as appropriate, to the involvement of the following types of individuals in the review process: i. Patients, former patients, patient advocates or family members or others who can represent the views and perspectives of the research participants.” 209 Interestingly, in the Lawrence study, when asked whom they would consult regarding decisions about undergoing a DBS procedure, participants ranked close family members, romantic partners, and friends higher than psychiatrists, doctors, therapists, or experts in DBS. 210
If former mental illness research participants are available and able, their voices at the IRB table surely would be invaluable. But, one need not have served as a research participant to have pertinent information on the unique concerns mentally ill research participants may have. A family member who has spent a dozen years securing medical treatment and medication for a patient suffering from bipolar disorder or schizophrenia will surely possess knowledge of participants’ specific needs. Further, a person who lives with mental illness themselves and is in remission—though never a research participant—would bring highly pertinent perspective to the research review process. Official guidance and clear definitions would be of substantial value; however, institutions and their IRBs could move immediately to work on and implement positive changes. Simply changing who is at the IRB table interpreting regulations and guidance is a feasible way to more appropriately represent mentally ill people in research. 211
As noted above, under its new IRB structure, the NIH matches physician and scientist subject matter experts to specific protocols in panel reviews. 212 Likewise, a similar “subject matter expert” or “subject matter area of interest” pairing of community members to protocols could be both appropriate and effective. Where a research institution maintains IRB community member pools, community members could be asked to specify areas of experience or interest, without being required to reveal their own protected health information or that of family members; these members could then be assigned to review protocols relating to their indicated experience and interest. Such targeted representation on clinical research protocol reviews would allow the institution to capitalize on the vast and varied knowledge bases of community members, increasing the likelihood that potentially vulnerable populations’ unique needs are properly articulated, understood, and addressed. While taking some effort to set up, this modification would satisfy concerns about community representation without placing extra burdens on former research participants 213 who may not be well, able, or available to serve on IRBs.
VI. CONCLUSION
As clinical research with people who suffer from mental illness moves forward in new and exciting directions, eager anticipation of resulting benefits must be balanced by mindfulness of this community’s history of stigmatization and abuse. Beyond common concerns about research with vulnerable populations, the prospects of using new technologies in research efforts aimed at curing psychiatric illness—e.g., gene editing—potentially will bring with them extreme risks and major ethics considerations; serious thought about special regulations for these new biotechnologies must begin in the near term. 214 Here and now, however, gaps in protections endure for mentally ill people in “ordinary” biomedical research, such as research using combinations of psychotropic medications that are not considered novel biotechnologies.
As recognized by many—including NBAC—during the past several decades, awareness and acknowledgment of the gaps in protections is required 215 : an earnest effort to resolve still unanswered questions about how adequately to protect mentally ill people in biomedical research is needed to finally close that gap. Unyielding adherence to traditional notions of decision-making capacity is a doorstop to closing the gaps in protections because other potential vulnerabilities to coercion or undue influence for mentally ill participants will remain unaddressed and ignored.
Standing alone, the rCR is not problematic; rather, it is the misguided application of the rule in the context of mental illness. Perhaps those in positions to interpret the rule, e.g., busy professionals at research institutions, are taking the most direct path to save time and simplify approaches to protect against vulnerabilities to coercion or undue influence. It is doubtful these approaches stem from lack of care about people who live with mental illness, and more likely that decisions are influenced by lack of time. Choices on implementation of protective policy that lean toward expediency, however, may leave unfulfilled the duty to protect people with mental illness in biomedical research.
Forty years after the Belmont Report, even with the 2018 revisions in the rCR, “we remain without sufficiently thorough policy guidelines for working with persons [who suffer from] mental illness.” 216 Perhaps in the next round of rulemaking, if ever that happens, the rCR will be further revised to address these deficiencies. Some scholars have encouraged an alternative approach of more frequent modifications to the Common Rule, facilitated by mechanisms such as framework rulemaking and strategic consultation. 217 Rather immediately, new guidance and policies could interpret the regulations in ways allowing novel approaches to safeguard potentially vulnerable participants. 218
In any event, it is important to recognize that most of the literature on the acceptability of research with mentally ill people is produced by researchers who conduct research on psychiatric interventions, some of which is sponsored by major pharmaceutical corporations. 219 Further, strong support regarding the acceptability of such research comes from community advocacy groups that largely are sponsored by big pharmaceutical corporations. 220 Without imputing ill intent to these parties, their perspectives may be biased toward the argument that mentally ill people are unfairly and improperly excluded from research. Limiting considerations to traditional decision-making capacity may be appealing to drug manufacturers and the researchers they sponsor, but this approach is simply not enough. The challenge of finding the right balance is difficult, but that should not dissuade an attempt to do so.
While confusion persists about the meaning of vulnerability to coercion or undue influence in clinical research with mentally ill people, creativity is needed in formulating new approaches to facilitate important research on mental illness while protecting potentially vulnerable participants. No solution can or will be perfect. The most straightforward remedy would be for HHS to further revise the rCR or provide clarity on the parameters of “vulnerability due to coercion or undue influence” and what this concept might include in real-life circumstances. Additionally, HHS should clarify its stance on “impaired decision-making capacity” and its relation to mentally ill participants. Also needed is binding guidance, like that suggested in Part V, on how to expand our thinking about mentally ill research participants’ vulnerabilities to coercion or undue influence, beyond traditional consent-based decision-making capacity. HHS should speak to the practical application of these concepts so as to afford appropriate and consistent protections for mentally ill research subjects. In the absence of specific HHS leadership, or in addition to such guidance, changes in federal agency policies could require that any IRB reviewing protocols for research with this community must include affected people in remission or family members of severely mentally ill people.
Looking to community members who possess experience-based knowledge about mental illness and who, thus, may appropriately represent the interests of future participants would be a major step toward progress. These stakeholders should be invited to participate in the process of brainstorming, planning, and drafting binding guidance, beyond the traditional public comment for regulatory changes. Asking stakeholders—including community members in remission or family members of those struggling—to assist HHS in determining necessary changes, and bringing these same groups to the IRB table to review research, will enhance protections for potential research participants who are suffering from mental illness and unable themselves to pull up a chair.
Footnotes
1
New research in the field of psychiatric genetics and neuroscience may yield valuable discoveries that potentially could lead to better treatments or cures. There is substantial interest in controversial experimentation, such as gene editing and deep brain stimulation, to explore possible treatments and/or cures for mental illness. See, e.g., Alexandra L. Foulkes et al., Legal and Ethical Implications of CRISPR Applications in Psychiatry, 97 N.C. L. R
2
Decisively defining “mental illness” is no easy task. “Identifying what counts as a mental illness seems to require some understanding of what counts as mental health, and this may in turn depend on some conception of normal or acceptable behavior, moods, and thought patterns. Thus, an understanding of mental illness is not merely descriptive of actual behavior; it is also prescriptive of what healthy behavior actually is.” G![]() ] (The Mayo Clinic describes mental illness as “a wide range of mental health conditions—disorders that affect your mood, thinking and behavior. Examples of mental illness include depression, anxiety disorders, schizophrenia, eating disorders and addictive behaviors.”). Note, too, that there is now a small sector of the community moving to embrace “mental illness” as a part of one’s identity, critical of the extent to which psychiatry has pathologized “madness” and challenging “the tendency to adopt, too readily, the (medical) view that madness is inherently disabling.” See., e.g., Mohammed Abouelleil Rashed, In Defense of Madness: The Problem of Disability, 44 J. M
] (The Mayo Clinic describes mental illness as “a wide range of mental health conditions—disorders that affect your mood, thinking and behavior. Examples of mental illness include depression, anxiety disorders, schizophrenia, eating disorders and addictive behaviors.”). Note, too, that there is now a small sector of the community moving to embrace “mental illness” as a part of one’s identity, critical of the extent to which psychiatry has pathologized “madness” and challenging “the tendency to adopt, too readily, the (medical) view that madness is inherently disabling.” See., e.g., Mohammed Abouelleil Rashed, In Defense of Madness: The Problem of Disability, 44 J. M
3
For example, see Buck v. Bell, 274 U.S. 200, 207 (1927), an antiquated U.S. Supreme Court decision (never overturned and still “good law” in the United States) that wholeheartedly embraced systemic disregard of the human rights and dignity of people allegedly afflicted with mental illness. The Court gave its stamp of approval to the medical establishment’s abuse of “imbeciles” or “mental defectives.” Id. Specifically, in this case Justice Holmes upheld a Virginia eugenic sterilization statute and stated that “three generations of imbeciles” are enough, allowing sterilization of an allegedly mentally ill woman whose mother and daughter also had been designated mentally defective. Id. For a detailed overview and analysis of the case, the widely accepted historical abuse of persons with mental illness, and the machinations of the eugenics movement, see P
4
For a critical report and overview of this research study, see S
5
Id. at 7.
6
Id. at 9-10, 17, 19.
7
As early as 1997, Carl Elliott sounded the alarm that we must consider that “depression often leaves a patient’s cognitive abilities intact,” but frequently changes their values, thoughts and behaviors, and also may make them less concerned about potential risks of harm to themselves from research. Carl Elliott, Caring About Risks: Are Severely Depressed Patients Competent to Consent to Research?, 54 A
8
James DuBois et al., Restoring Balance: A Consensus Statement on the Protection of Vulnerable Research Participants, 102 A
9
See Revised Common Rule, 45 C.F.R. § 46 (2019).
10
See Corinne Lajoie et al., The Concept of Vulnerability in Mental Health Research: A Mixed Methods Study on Researcher Perspectives, 15 J. E
11
P
12
Bruce G. Link et al., Stigma as a Barrier to Recovery: The Consequences of Stigma for the Self-Esteem of People with Mental Illnesses, 52 P
13
Jo C. Phelan & Bruce G. Link, Fear of People with Mental Illnesses: The Role of Personal and Impersonal Contact and Exposure to Threat or Harm, 45 J. H
14
Evelien P. M. Brouwers, Social Stigma Is an Underestimated Contributing Factor to Unemployment in People with Mental Illness or Mental Health Issues: Position Paper and Future Directions, 8 BMC P
15
Karen L. Fortuna et al., Unmet Needs of People with Serious Mental Illness: Perspectives from Certified Peer Specialists, 90 P
16
Debra Lerner et al., Unemployment, Job Retention, and Productivity Loss Among Employees with Depression, 55 P
17
John Sylvestre et al., Poverty and Serious Mental Illness: Toward Action on a Seemingly Intractable Problem, 61 A
18
Allison C. Nugent et al., The Ethics of Clinical Trials Research in Severe Mood Disorders, 31 B
19
See Elliot, supra note 7, at 115; Lisa E. Smilan, The Off-Label Loophole in the Psychopharmacologic Setting: Prescription of Antipsychotic Drugs in the Nonpsychotic Patient Population, 30 H
20
David Wendler, A Pragmatic Analysis of Vulnerability in Clinical Research, 31 B
21
See Marion Boulicault & Timothy Emmanuel Brown, How Relationships Matter: The Need for Closer Attention to Relationality in Neuroethical Studies, 9 AM. J. B![]() ] (discussing clinical research conducted in physicians’ offices).
] (discussing clinical research conducted in physicians’ offices).
22
See, e.g., Patrick Robinson et al., Measuring Attitudes Towards Mental Health Using Social Media: Investigating Stigma and Trivialisation, 54 SOC. PSYCHIATRY & PSYCHIATRIC EPIDEMIOLOGY 51, 51 (2019) (finding stigma in regards to mental health is a significant barrier for early diagnosis and treatment); Shoji Yokoya et al., A Brief Survey of Public Knowledge and Stigma Towards Depression, 10 J. CLINICAL MED. RES. 202, 202 (2018) (finding that thirty percent of participants in the survey had the stigmatizing belief that a weak personality causes depression).
23
See, e.g., John H. Noble Jr. & Vera Hassner Sharav, Protecting People with Decisional Impairments and Legal Incapacity Against Biomedical Research Abuse, 18 J. D
24
Many scholars and researchers alike seem to find it repugnant to even consider saying that all mentally ill people are likely to be vulnerable to coercion or undue influence due to their mental illness. See Nugent et al., supra note 18, at 447 (“Indeed, we would argue that formally classifying those with mood disorders as a vulnerable population could potentially contribute to stigma and devalue the societal contributions made by these individuals.”); see also, Lajoie et al., Concept of Vulnerability, supra note 10, at 140. Why this is so offensive to these professionals, most of whom presumably are not members of this community, is unclear. While some in this patient population may argue that their mental differences are not an illness, it is fair to say that people who are mentally ill generally are considered to be ill, and mental illnesses specifically target the mind—where emotion, thought and information processing are regulated (or not). (Interestingly, for decades few in biomedical ethics, health policy or law balked at the notion that all pregnant women are vulnerable in research. See Anna C. Mastroianni et al., The Pathway Forward: Insights on Factors that Facilitate Research with Pregnant Women, 42 E
25
As applied in practice, “decision-making-capacity” as the catch-all category for vulnerability to coercion or undue influence in the context of mental illness precludes a broader understanding of mental illness vulnerabilities (even if this was not the intent of those who drafted the Revised Common Rule).
26
People with severe intellectual disabilities are also excluded here, as the assumption is that these individuals at no point possessed decision-making capacity required to consent to research. If abided by, the Common Rule and rCR should provide adequate protections for these individuals, as well as those who are experiencing active psychosis. See Common Rule, 45 C.F.R. § 46 (1991); Revised Common Rule, 45 C.F.R. § 46 (2019). Involuntarily institutionalized people also should be protected under the existing rules, because of the inherently coercive nature of that environment and the relationship between institutionalized patient and mental health provider. Extant literature addresses involuntarily institutionalized individuals in clinical research. See, e.g., N
27
For a detailed overview of concerns and debates, see Richard J. Bonnie, Research with Cognitively Impaired Subjects: Unfinished Business in the Regulation of Human Research, 54 A
28
45 C.F.R. § 46 (1991).
29
Common notions of “mental disability” bring to mind persons with lower IQs, congenital brain abnormalities or traumatic brain injuries. However, there could be near-genius individuals who suffer from bipolar disorder or major depressive disorder, for example, who may be vulnerable at certain times and under certain circumstances, not due to an inability to think but due to effects the mental illness (and, perhaps, medications used to treat the illness) has on their brains and true selves.
30
E
31
N
32
See id. at 5.
33
Id. at iii, 53.
34
Id. (emphasis added). Where the IRB ordinarily does not address protocols involving potential subjects who suffer from a “mental disorder,” NBAC recommended that the IRB’s discussion should include “two ad hoc consultants who are familiar with the nature of these disorders and with the concerns of the population being studied; at least one of these consultants should be a member of the population being studied, a family member of such a person, or a representative of an advocacy organization for this population.” Id. (emphasis added).
35
D
36
Resnik points to the diversity within populations living with mental disability or mental illness that makes it not necessarily appropriate to put them in categories: “[S]ome mentally ill or disabled adults may have good decision-making abilities, while others may not. Also, some may be able to make decisions under certain conditions … but not [under] others.” Id. at 227.
37
Revised Common Rule, 45 C.F.R. § 46 (2019).
38
Id. §§ 46.107, 46.111.
39
See infra Part IV.
40
See Protection of Human Subjects, 38 Fed. Reg. 31,738, 31,738 (proposed Nov. 16, 1973). For a full discussion, see Diane E. Hoffmann et al., Regulating Research with Decisionally Impaired Individuals: Are We Making Progress?, 3 D
41
Common Rule, 45 C.F.R. §§ 46.107, 46.111 (1991).
42
See 45 C.F.R. § 46 (1991).
43
Americans with Disabilities Act, Pub. L. 101-336, § 3, 104 Stat. 327, 330 (1990) (codified as amended at 42 U.S.C. § 12102(1)(A) (2012)).
44
See, e.g., John Petrila & Thomas Brink, Mental Illness and Changing Definitions of Disability Under the Americans with Disabilities Act, 52 P
45
Revised Common Rule, 45 CFR §§ 46.107(a), 46.107(e) (2018), WL 45 CFR § 46.107 (showing Westlaw comparison of version effective until July 18, 2018 and current version effective July 19, 2018). Other relevant changes in the Revised Common Rule, regarding criteria for IRB approval of research with potentially vulnerable subjects are:
§ 46.111 Criteria for IRB approval of research. In order to approve research covered by this policy the IRB shall determine that all of the following requirements are satisfied: …. (3) Selection of subjects is equitable. In making this assessment the IRB should take into account the purposes of the research and the setting in which the research will be conducted …. When some or all of the subjects are likely to be vulnerable to coercion or undue influence, such as children, prisoners,
and. involving populations pregnant women, mentally disabled personspregnant women, mentally disabled persons
45 C.F.R. §§ 46.111(a)(3), 46.111(b) (2018), WL 45 CFR § 46.111 (italics added) (showing Westlaw comparison of version effective until July 18, 2018 and current version effective July 19, 2018).
46
Compare 45 C.F.R. §§ 46.107, 46.111 (1991) (omitting those with “impaired decision-making capacity” as an example of individuals vulnerable to coercion or undue influence), with 45 C.F.R. §§ 46.107, 46.111 (2019) (including those with “impaired decision-making capacity as an example of individuals vulnerable to coercion or undue influence).
47
See 45 C.F.R. § 46 (2019).
48
In the Preamble to the final revised rule, HHS stated that it was using “‘individuals with impaired decisionmaking ability’ to replace the term ‘mentally disabled persons.’” Federal Policy for the Protection of Human Subjects, 82 Fed. Reg. 7,149, 7,204 (Jan. 19, 2017) (to be codified at 45 C.F.R. pt. 46). HHS stated that some public comments had argued that the term “mentally disabled” was “potentially patronizing.” Id. One comment had suggested the use of the term “populations with impaired decision making ability” to replace the term “mentally disabled,” and HHS adopted this new language and incorporated it in the revised rule. Id. Note, too, that HHS stated that the Secretary’s Advisory Committee on Human Research Protections (SACHRP) suggested in 2009 the use of the phrase “impaired decisionmaking capacity,” but it is not stated what it was to replace or what categories of subjects it should include. See id. (citing SACHRP, Recommendations Regarding Research Involving Individuals with Impaired Decision-Making, U.S. D![]() ]. IRBs are tasked with delineating the concept of “impaired decisionmaking capacity” on a protocol-by-protocol basis.
]. IRBs are tasked with delineating the concept of “impaired decisionmaking capacity” on a protocol-by-protocol basis.
49
45 C.F.R. § 46.111(b) (2019).
50
See, e.g., Paul S. Appelbaum et al., Competence of Depressed Patients for Consent to Research, 156 A
51
45 C.F.R. §§ 46.107(a), 46.111 (1991); 45 C.F.R. §§ 46.107(a), 46.111 (2019).
52
Yes, some people with mental illness have impaired decision-making capacity. Many more, especially those with major depressive disorder, may score well in capacity assessments, see Fisher, supra note 11, at 74, but be vulnerable to coercion or undue influence for other reasons related to their mental illnesses and treatments. While many scholars and researchers argue that it is harmful to put all people with mental illness in one bucket (assuming that they all are vulnerable to coercion or undue influence), surely it is just as harmful to exclude many mentally ill people from the bucket because they happen to be able to provide reasonable and rational answers to questions, even if those answers do not reflect their true values, opinions and judgments.
53
See RESNIK, supra note 35, at 219-220; Yanos et al., supra note 50, at 377.
54
45 C.F.R. §§ 46.107(a), 46.111 (2019).
55
Id.; RESNICK, supra note 35, at 217-20.
56
45 C.F.R. §§ 46.107(a), 46.111 (2019).
57
See, e.g., Yanos et al., supra note 50, at 376 (recognizing the concept of vulnerability as broad despite focusing on only two interpretations during research).
58
See, e.g., Fisher et al., supra note 11, at 74.
59
Elliott, supra note 7, at 115.
60
Roberts, supra note 21, at 706.
61
Nugent et al., supra note 18, at 443.
62
Lawrence et al., supra note 1, at 215-16 (citing A
63
Elliott, supra note 7, at 115.
64
Lawrence et al., supra note 1, at 216. Clouded judgment should qualify as impaired decision-making, but as the regulation is applied, most likely it would not because such nuances would not be picked up in the traditional capacity assessment. As long as the subject was agreeing to participate in the research, this likely would be assumed by the researcher to be a reasonable and rational decision, even if it differed from the subject’s prior beliefs (unknown to the researcher), e.g., that participating in research is a very bad idea. Some scholars have advocated in the clinical care setting that current assessments of capacity miss many aspects of how mental illness potentially changes one’s choices. See Aryeh L. Goldberg, How Bioethics and Case Law Diverge in Assessments of Mental Capacity: An Argument for a Narrative Coherence Standard, 11 A
65
See Smilan, The Off-Label Loophole, supra note 19, at 267 n.181, 268. The Author recognizes that there is great variability in mental illnesses and their treatment. While one medication, e.g., an antipsychotic, might alter the true self of the non-psychotic patient, that same medication may restore the true self of someone experiencing a “psychotic break” associated with bipolar disorder. See id. at 294.
66
See Fortuna, supra note 15, at 579.
67
See Corinne Lajoie et al., Lived Experiences of Participation in Mental Health Research in Canada: Breaking the Glass Wall, D![]() ] (describing how mental health research participants expressed that their participation fostered a sense of involvement and belonging in society, making them feel “important, valued, and listened to,” believed, recognized, and helpful). Such recognition and validation “is especially meaningful for individuals who have historically been ignored and silenced.” Id. at 14.
] (describing how mental health research participants expressed that their participation fostered a sense of involvement and belonging in society, making them feel “important, valued, and listened to,” believed, recognized, and helpful). Such recognition and validation “is especially meaningful for individuals who have historically been ignored and silenced.” Id. at 14.
68
Roberts, supra note 21, at 709.
69
RESNIK, supra note 35, at 228 (citing N
70
Michelle Biros, Capacity, Vulnerability, and Informed Consent for Research, 46 J.L. M
71
See, e.g., Melissa D. McCradden & Michael D. Cusimano, Questioning Assumptions About Vulnerability in Psychiatric Patients, 9 A
72
See Laura Weiss Roberts et al., Perspectives of Patients with Schizophrenia and Psychiatrists Regarding Ethically Important Aspects of Research Participation, 157 A
73
See, e.g., A
74
See supra notes 45-47 and accompanying text.
75
See, e.g., Fisher, supra note 11, at 74; supra note 52 and accompanying text.
76
See N
77
See Coercion, B
78
The words “vulnerable” and “vulnerability” are not found in the widely accepted authority on legal definitions, Black’s Law Dictionary. See B
79
See Common Rule, 45 C.F.R. § 46.102 (1991); Revised Common Rule, 45 C.F.R., § 46.102 (2019).
80
Robert Klitzman, How IRBs View and Make Decisions About Coercion and Undue Influence, 39 J. M
81
Fisher, supra note 80, at 369.
82
See Informed Consent FAQs, O![]() ].
].
83
Id. This is consistent with the legal definition: Coercion “may be actual, direct, or positive, as where physical force is used to compel act against one’s will, or implied, legal or constructive, as where one party is constrained by subjugation to other to do what his free will would refuse” and in the context of criminal law, coercion “can be mental as well as physical.” Coercion, B
84
See Fisher, supra note 80, at 363-64.
85
Id. at 360.
86
Id. at 359.
87
Id. at 360.
88
Id. at 363-64.
89
See id. at 365 (noting how Phase I investigational drug studies often pay thousands of dollars to participants, who view the money as a way to support themselves and their families)..
90
See Fisher, supra note 80, at 364 (“What is often characterized by researchers and ethics scholars as participants’ ‘desperation’ can influence people’s perspectives that a clinical study is their only chance for an effective therapy or needed income.”); see also Lajoie et al., Lived Experiences, supra note 67, at 6, 8 (describing testimony of one mental health research participant who explained that “participating in research studies helped her financially and made her feel helpful to society,” and another who expressed that the financial compensation contributed to her decision to participate in research, along with the belief that participation would help her by getting her “mind off other things,” in addition to making her feel valued and important).
91
This brings to mind the friendship and sense of community at Miss Rivers’ Lodge, where the nurse who played a central role in the Tuskegee syphilis study continued friendships with study subjects for decades. See Susan M. Reverby, Rethinking the Tuskegee Syphilis Study: Nurse Rivers, Silence and the Meaning of Treatment, 7 N
92
O
93
O
94
See Fisher, supra note 80, at 357.
95
Dearbhail Bracken-Roche et al., The Concept of ‘Vulnerability’ in Research Ethics: An In-Depth Analysis of Policies and Guidelines, 15 H
96
See Nugent et al., supra note 18, at 444.
97
Lawrence et al., supra note 1, at 214.
98
See supra note 71 and accompanying text (discussing voluntarism); infra note 157 and accompanying text (discussing “autonomous consent”); see also Roberts, supra note 21, at 706.
99
Hannah Skye Martens & Timothy Emmanuel Brown, Trusting Oneself and Others: Relational Vulnerability and DBS for Depression, 9 A
100
Id. (quoting Carolyn McLeod & Susan Sherwin, Relational Autonomy, Self-Trust, and Health Care for Patients Who are Oppressed, in R
101
Id.
102
See Smilan, supra note 19, at 303-04 (noting that psychotropic medications sedate and control patient behaviors, often with “life-altering chronic and irreversible side effects”). Nugent et al. note that “[i]nformed consent requires that decisional autonomy not be compromised by either external and potentially coercive forces, or by internal forces resulting from the illness or impairment.” Nugent et al., supra note 18, at 444 (emphasis added).
103
See Elliott, supra note 7, at 114 (noting that an actor’s emotional state may impair his decision-making and render him incompetent to consent to treatment).
104
Revised Common Rule, 45 C.F.R. § 46.107 (2019) (recommending inclusion of persons who are knowledgeable about and experienced in working with vulnerable subjects); Common Rule, 45 C.F.R. § 46.107 (1991).
105
45 C.F.R. § 46.111(a)(3) (2019) (advising researchers to account for the purpose and setting of the research when selecting subjects); 45 C.F.R. § 46.111(a)(3) (1991).
106
45 C.F.R. § 46.111(b) (2019) (requiring additional safeguards for vulnerable subjects); 45 C.F.R. § 46.111(b); see Hurley, supra note 48 (noting that beyond the circumstances of enrollment, also important is how subjects are treated throughout the research process).
107
Bracken-Roche et al., supra note 95, at 15.
108
See Hurley, supra note 48 (noting that exploitation, excessive risks, and exclusion are types of vulnerability in research beyond coercion and undue influence). If anything, language in the rCR seems to yield even more discretion to IRB members than did the original rule by requiring judgments on the scope and parameters of “impaired decision-making capacity,” with no direction on implementation. See 45 C.F.R. § 46 (2019) (requiring special protections for persons with “impaired decision-making capacity” without defining this term).
109
See, e.g., Eric Racine & Dearbhail Bracken-Roche, Enriching the Concept of Vulnerability in Research Ethics: An Integrative and Functional Account, 33 BIOETHICS 19, 20 (2018) (noting that scholars struggle to agree on consistent use and understanding of vulnerability in research ethics); Wendler, supra note 20, at 520 (defining “vulnerable” according to Merriam Webster’s Dictionary, research literature, and standard English).
110
Wendler, supra note 20, at 520 (citing Kenneth Kipnis, The Limitations of “Limitations”, 4 AM. J. BIOETHICS 70, 70 (2004)); see also Racine & Bracken-Roche, supra note 109, at 20 (“[S]cholars have been advancing competing accounts of vulnerability and struggling to reach consensus about the conceptualization and operationalization of vulnerability in research ethics.”).
111
Vulnerable, MERRIAM WEBSTER DICTIONARY, https://www.merriam-webster.com/dictionary/vulnerable [![]() ]. The words “vulnerable” and “vulnerability” do not appear in Black’s Law Dictionary. BLACK’S LAW DICTIONARY (11th ed. 2019) (defining only “vulnerable adult,” “vulnerable-adult abuse,” and “vulnerable zone”).
]. The words “vulnerable” and “vulnerability” do not appear in Black’s Law Dictionary. BLACK’S LAW DICTIONARY (11th ed. 2019) (defining only “vulnerable adult,” “vulnerable-adult abuse,” and “vulnerable zone”).
112
Bracken-Roche et al., supra note 95, at 16.
113
Lawrence et al., supra note 1, at 216 (citing Andrew Coulter, Deep Brain Stimulation Research Protocols and Depressive Patients with Previous Suicidality: We Can’t Afford to Lose Focus, 4 AM. J. BIOETHICS NEUROSCIENCE 41, 41 (2013)).
114
See Lajoie et al., Concept of Vulnerability, supra note 10, at 140 (citing the need for further qualitative research on mental health research participants’ perspectives regarding vulnerability in mental health and views relating to possible overuse and stigmatization).
115
Bracken-Roche et al., supra note 95, at 1; see also Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research, 44 Fed. Reg. 23,192, 23,195 (Apr. 18, 1979).
116
Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research, 44 Fed. Reg. at 23,195.
117
Id. at 23,196 (“Injustice may appear in the selection of subjects, [because] even if individual subjects are selected fairly … unjust social patterns may nevertheless appear in the overall distribution of the burdens and benefits of research.”).
118
Id. at 23,197 (emphasis added).
119
Wendler, supra note 20, at 517; see also Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research, 44 Fed. Reg. at 23,196.
120
Wendler, supra note 20, at 517 (citations omitted); see also Proposed Regulations on Research Involving Those Institutionalized as Mentally Disabled, 43 Fed. Reg. 53,950, 53,950 (proposed Nov. 17, 1978) (to be codified at 45 C.F.R. pt. 46) (“[Institutionalized mentally infirm] persons by the very nature of their disabilities may not be competent to provide informed consent …. At the same time, the nature of their disabilities requires extensive research efforts to study the etiology, pathogenesis, prevention, therapy, and management of their conditions.”). This “justification” for excluding mentally ill people from heightened protections while imposing unnecessary restrictions on pregnant women is illogical if it was done in good faith, and makes perfect sense if done to perpetuate stereotypes and inequitable gender roles in the case of pregnant women and make research with mentally ill patients who lacked the wherewithal to protect themselves that much easier for researchers.
121
Wendler, supra note 20, at 517. Similarly, FDA regulations regarding criteria for IRB approval of research in the context of clinical research, state: “When some or all of the subjects, such as children, prisoners, pregnant women, handicapped, or mentally disabled persons, or economically or educationally disadvantaged persons, are likely to be vulnerable to coercion or undue influence additional safeguards have been included in the study to protect the rights and welfare of these subjects.” 21 C.F.R. § 56.111(b) (2001); see also 21 C.F.R. § 56.111(a)(3) (2001) (stating that the IRB should be cognizant of the special research problems encountered by vulnerable populations); 21 C.F.R. § 56.107(a) (1991) (requiring at least one IRB member be “primarily concerned” with the welfare of vulnerable subjects if the IRB regularly reviews research involving these populations). FDA’s regulations have not been modified by the rCR.
122
Left to the interpretations of IRB members, “mentally disabled” persons could be those suffering from brain damage, or those with congenital brain abnormalities, or those with physical ailments that affect brain functioning. See Hoffman et al., supra note 40, at 550 (“Federal regulations merely call on [IRBs] to be attentive to the need for ‘additional safeguards’ ….”). Likewise, the term could be interpreted to include those with medically diagnosed mood disorders. See N
123
Bracken-Roche et al., supra note 95, at 1.
124
Biros, supra note 70, at 75 (citing Jo Aldridge, Working with Vulnerable Groups in Social Research: Dilemmas by Default and Design, 14 Q
125
Bracken-Roche et al., supra note 95, at 2 (citing Florence Luna & Sheryl Vanderpoel, Not the Usual Suspects: Addressing Layers of Vulnerability, 27 BIOETHICS 325, 326 (2013)).
126
Wendler, supra note 20, at 517.
127
C
128
Fields & Calvert, supra note 50, at 463-64; see also MacFarlane et al., supra note 50, at 64 (explaining temporary impairments and listing examples of such transient impairments).
129
Wendler, supra note 20, at 517. Interestingly, in a recent qualitative study, one participant living with mental illness stated that “you lose your capacity to make decisions in a sense. No, not your capacity, but it makes it harder […]. [You’re] quite vulnerable to whatever doctors will tell you you should do or your parents or your family or husband, whatever.” Lajoie et al., Enriching our Understanding, supra note 24, at 451.
130
See Bracken-Roche et al., supra note 95, at 16 (noting the capability of research environments to disempower research participants and subjects).
131
Id. at 16.
132
Wendler, supra note 20, at 519 (citing Frederick Grinnell, Subject Vulnerability: The Precautionary Principle of Human Research, 4 A
133
Id. at 519, 522.
134
Id. at 519.
135
Id. at 524.
136
Id. at 516.
137
Id.; see also Morian-Sanchez, Luna & Perez-Carceles, supra note 50, at 102.
138
Bracken-Roche et al., supra note 95, at 10 (quoting C
139
DuBois et al., supra note 8, at 2222, 2224. “Labeling particular groups as at risk for lacking decisional capacity or as incapable of making a voluntary choice reinforces stigma or stereotypes, when in fact members of such groups are frequently diverse and function as well as so-called healthy volunteers.” Id. at 2222 (citations omitted).
140
Leaving some discretion to ethics oversight committees or IRBs is often a good thing; however, inconsistent practices among various research institutions receiving federal funding is indeed problematic.
141
MacFarlane et al., supra note 50, at 64; see also Racine & Bracken-Roche, supra note 109, at 20 (discussing research ethics boards in Canada, a similar challenge there “of assessing and appropriately responding to vulnerability,” and implications for potentially vulnerable research subjects that may flow from boards’ actions or inaction); Yanos et al., supra note 50, at 374 (recognizing the lack of consensus among IRBs “on how to evaluate studies in which considerations of both degree of risk and vulnerability need to be made”).
142
Though, some scholars complain that “IRB members overestimate the risk of incapacity” present in the psychiatric patient population while underestimating levels of risk for patients with medical diagnoses that are unrelated to mental illness but nonetheless may impair decisional capacity. DuBois et al., supra note 8, at 2222 (citing Luebbert et al., IRB Member Judgments of Decisional Capacity, Coercion, and Risk in Medical and Psychiatric Studies, 3 J. E
143
Wendler, supra note 20, at 516.
144
Id. at 522.
145
Id. at 524 (recognizing how a contextual analysis may determine “that only some subjects are vulnerable” and “whether there are individuals for whom the general protections are not sufficient”).
146
Biros, supra note 70, at 75.
147
There are many instances that might give rise to impaired decision-making capacity: One might include a person in a comatose state after an automobile accident, another a person experiencing catatonia due to disease or infection. The category “impaired decision-making capacity” includes many potential research subjects, diluting the specific needs of and attention given those who are suffering from mental illness. See, e.g., R
148
See generally id. at 217-19 (summarizing different bioethicist’s definitions of vulnerable populations).
149
See supra Section II.C.
150
See R
151
See supra Section II.D.
152
Fisher, supra note 80, at 360.
153
See Elliott, supra note 7, at 114.
154
See Roberts, supra note 21, at 705.
155
Id.
156
Id. at 707.
157
See Smilan & Conklin, supra note 64, at 33-34 (using the term “autonomous consent” to highlight how true autonomy may be lacking in consent where the effects and implications of mental illness make voluntarism—a necessary component of autonomous consent—unlikely or impossible).
158
See Elliot, supra note 7, at 114-15.
159
Earlier scholarship discussed the authenticity of a mentally ill person’s actions and behaviors: “The authenticity argument supposes a person with a stable character and entrenched dispositions, who, while depressed, makes decisions so uncharacteristic that we feel bound to question whether those decisions were truly hers.” Id. at 115. The Author acknowledges that for certain severe mental illnesses, e.g., schizophrenia, it is the psychotropic medication that may elicit the true self of the psychiatric patient. See Smilan, supra note 19, at 302; Thompson et al., supra note 19, at 161.
160
Wendler, supra note 20, at 524.
161
Id.
162
Id. (emphasis added).
163
Rebecca Dresser, Experimentation Without Representation, 40 IRB. 3, 5 (2018). Bracken-Roche and colleagues similarly suggest that research participants, who “seem to have been largely left out of the development of research ethics guidelines” might also be important to the process of framing vulnerability. Bracken-Roche et al., supra note 95, at 17.
164
Dresser, supra note 163, at 5. Dresser acknowledges the inherent challenges in tasking research institutions and organizations with locating and recruiting research subjects as advisors or board members who also have “the necessary contacts and background to represent” the diversity and diverse experiences of other research participants. Id. at 6. In arguing for her proposed initiative, Dresser notes that “the complex perspectives of researchers, ethicists, and members of the public are weighed and balanced in research ethics and policy deliberations. Subjects’ complex perspectives could simply be added to the mix.” Id.
165
Id. at 5.
166
Id.
167
See Stephanie Solomon Cargill, Moving from the “Why” to the “How”: Two Approaches to Including Research Participants’ Voices, 40 IRB 8, 9 (2018).
168
See, e.g., Yokoya et al., supra note 22, at 203.
169
Cargill, supra note 167, at 9. Cargill concedes that the indirect approach of research subject input via empirical research may be compromised by “the current dearth of empirical research on research ethics, and research with research participants in particular.” Id. at 10. Also problematic is the difficulty in locating ethics research studies and translating mixed-methods or qualitative work into generalizable information. Id.
170
Id.
171
Id. Cargill states that this could result in strategic use of participant perspectives only “where it would promote the efficacy or expediency of research, and its dismissal in realms where it may hinder or challenge it.” Id.
172
See id.
173
Abby Lippman, Led (Astray) by Genetic Maps: The Cartography of the Human Genome and Health Care, 35 S
174
Lawrence et al., supra note 1, at 210. “Deep brain stimulation is a neurosurgical procedure in which electrodes are placed inside the brain and an electrical current is delivered to specific brain regions.” Id. While conducted with 24 adult psychiatric in-patients, excluded were patients “experiencing psychosis, delirium, dementia, intoxication, or catatonia, or [those with an] intellectual disability (mental retardation), … under court-ordered treatment, or [who] were non-English speaking.” Id. at 212.
175
Id. at 210.
176
Id. at 211.
177
Id. The cohort was not drawn from patients who had self-selected DBS as a potential treatment, but instead patients who were not necessarily seeking this treatment. Id.
178
Id. at 217.
179
See Loraine Busetto et al., How to Use and Assess Qualitative Research Methods, 2 N
180
Boulicault & Brown, supra note 21, at 235 (citing Bell et al., supra note 62, at 364) (describing “power-relational vulnerability” as “the vulnerability a research participant experiences as a result of asymmetrical power relations existing between investigators and participants”).
181
Id. at 236 (describing “identity-relational vulnerability” as “vulnerability that arises from how a person’s (evolving) self-identity both shapes and is shaped by their relationships with others”).
182
Id.
183
Şerife Tekin, supra note 71, at 240.
184
Revised Common Rule, 45 C.F.R. § 46.107 (2019).
185
Id.
186
See Robert Klitzman, Institutional Review Board Community Members: Who Are They, What Do They Do, and Whom Do They Represent?, 87 ACAD. MED. 975, 978-79 (2012) (finding that IRBs vary widely in the roles and functions assigned to community members).
187
The “working with” requirement may exclude perspectives of community members who are disabled or not members of the traditional workforce. See 45 C.F.R. § 46.107 (2019).
188
Id. (emphasis added). This proposition is discussed more fully in Part IV. See supra Part IV.
189
Jeste & Saks, supra note 19, at 623.
190
Id. at 609.
191
See Nugent et al., supra note 18, at 447; Lajoie et al., Concept of Vulnerability, supra note 10, at 129.
192
See supra Sections II.C, II.D.
193
See supra text accompanying note 52 and Section II.D.
194
Nugent et al. state that it is potentially harmful to declare all adults with mood disorders to be a vulnerable population, potentially contributing to stigma and devaluing of the societal contributions made by people with mood disorders. Nugent et al., supra note 18, at 447. These scholars draw comparisons between the dying cancer patient who consents to risky research and the patient suffering from depression because “severely ill patients rate the state of severe depression as equivalent to or worse than death.” Id. It is understandable why those who conduct research with mentally ill people want to show how their work is justifiable and should not be interfered with, however, there is no comparison between a dying cancer patient who literally has no alternative treatment and elects—with mental functioning fully intact—to take a huge risk to possibly avoid death and the severely depressed patient whose mental functioning is likely greatly compromised to take a huge risk in agreeing to take investigational psychotropic drugs or undergo other experimental psychiatric interventions. See Smilan, supra note 19, at 296-97.
195
Nugent et al. argue that our current system of informed consent is adequate, and that characteristics such as “extreme hopelessness and/or willingness to assume risk inappropriately should be relatively obvious in any properly conducted informed consent discussion, and could be deemed to invalidate consent.” Nugent et al., supra note 18, at 446. Underlying studies, such as those examined by Nugent et al. (to support their conclusions), that consider the benefits of research with mentally ill people are problematic in that research that asks mentally ill people about their experiences with research must be eyed with some skepticism: Structural coercion (or regular coercion) and undue influence may have been factors affecting their choices and preferences for the original research in which they participated, and then similarly in the research about that research. See, e.g., id. at 445-47; Monika Edlinger et al., Attitudes of Patients with Schizophrenia and Depression Towards Psychiatric Research, 177 P
196
Given the changes to one’s mind in many mental illnesses, reconsent would provide an opportunity for participants to express a change of choice if they changed their mind about participation.
197
Martha Rosenberg, Pharma Funding Advocacy Groups, U. S![]() ]. Large pharmaceuticals corporations have had their share of representation and influence already.
]. Large pharmaceuticals corporations have had their share of representation and influence already.
198
Suggestions have been offered in the context of consent in clinical care and in the treatment of mentally ill patients, where the traditional MacArthur criteria for decision-making capacity have been perceived as insufficient. See Goldberg, supra note 64, at 11 (“The ability to govern along one’s own self-narrative can, and therefore should, be clinically assessed and qualified. Although palpably absent from the current MacArthuer criteria, it is crucial to an assessment of self-governing capacity.”).
199
One participant in a recent study interviewing people who live with mental illness conveyed that “mental illness never completely disappears from one’s life and can always potentially reemerge.” Lajoie et al., Enriching our Understanding, supra note 24, at 448. Another participant in this same study offered that “[s]he has ‘accepted herself as a vulnerable person’ and knows that she needs to be vigilant and develop strategies to protect herself.” Id. at 447.
200
A current movement in the United States involves the use of Mental Health Peer Specialists in the treatment and recovery process of people with severe mental illness. See Matthew Chinman et al., Establishing a Research Agenda for Understanding the Role and Impact of Mental Health Peer Specialists, 68 P
201
See Sapfo Lignou et al., Ethical Challenges in Research, Industry and People Partnerships in Mental Health 1-2 (OSF Preprints, 2020) (quoting Make a Strong Application, N![]() ].
].
202
However, the Author advocates elsewhere that for genetics and genomics research relating to vulnerable or historically stigmatized populations (which would include people with mental illness) new governance approaches that include affected community members in decisions about research topics, design, recruitment, implementation, translation and dissemination are needed, especially when research results may lead to downstream harms to that community domestically and/or abroad. See Lisa E. Smilan, Balancing Benefits and Harms of Sexual Orientation and Gender Identity Genomics Research: Legal and Life Implications, 50 U. B
203
Michael Gottesman & Richard Wyatt, IRBs at NIH Revisited: Serving the Interests of Patients and Clinical Investigators, 25 NIH C
204
Id.
205
Id.
206
Françoise Baylis, IRBs: Protecting the Well-Being of Subject-Participants with Mental Disorders That May Affect Decisionmaking Capacity, 7 A
207
There is no need to “reinvent the wheel.” The work of NBAC, leading to the 1998 Research Involving Persons with Mental Disorders That May Affect Decision-making Capacity report, is still quite relevant and could be built upon in any current efforts to better protect in the biomedical research arena those subjects who suffer from mental illness. N
208
The Subcommittee on Inclusion of Individuals with Impaired Decision-making in Research (SIIIDR) was convened to develop recommendations regarding whether guidance and/or additional regulations were needed for research involving individuals with impaired decision-making capacity. SACHRP, supra note 48.
209
Id.
210
Lawrence et al., supra note 1, at 214.
211
See H
212
See Gottesman & Wyatt, supra note 203.
213
This is not to say that all people who live with mental illness would find participation burdensome.
214
The Author’s current work-in-progress focuses on this prospective concern. See Lisa Smilan, Rethinking Regulation in the Context of New Biologic Drugs: Psychiatric Polygenic Risk Scores, Somatic Genome Editing & Legal Off-Label Uses (forthcoming).
215
N
216
Williams, supra note 71, at 222.
217
Benjamin E. Berkman et al., A Proposed Process for Reliably Updating the Common Rule, 17 A
218
The National Institute of Mental Health (NIMH) has created the Human Subjects Protection Unit with Clinical Research Advocates (CRAs). N
219
“Journals have devolved into information laundering operations for the pharmaceutical industry.” Richard Smith, Medical Journals Are an Extension of the Marketing Arm of Pharmaceutical Companies, 2 PL
220
See Rosenberg, supra note 197.