
Abstract

Chronic overcrowding in emergency departments
Tolstoy opens his novel Anna Karenina with the line ‘All happy families are alike; each unhappy family is unhappy in its own way’. In this article, we discuss the extent to which this observation applies to emergency departments and, crucially, what this means for organisations trying to reduce overcrowding and delays in their unhappy emergency department. Based on the insights from operational research and ethnography, and on our work as an embedded research team within a UK hospital, we highlight how taking the time to understand why a particular emergency department is exhibiting crowding is essential for solving the problem.
Defined as ‘the situation where emergency department function is impeded primarily because the number of patients waiting to be seen, undergoing assessment and treatment, or waiting for departure exceeds either the physical bed and/or staffing capacity of the emergency department’, 1 overcrowding within emergency departments is a problem that affects health systems worldwide. Recent and ongoing problems in England have led to serious concerns about the safety of care within emergency departments 2 and measures such as the widespread cancellation of elective surgery and calls for medical students to volunteer their services to their local emergency department. 3
Silver bullets, Gatling guns and the fog of war
Those in charge of emergency departments, the hospitals in which they sit and the health economies they serve face a potentially bewildering array of interventions touted in the academic literature as having an evidence base for reducing emergency department crowding. Guidance and other initiatives aimed at making sense of this literature and promoting action by local decision makers can fall into the trap of oversimplifying the messages. Some focus on a single, silver bullet intervention, while others promote a whole raft of interventions with little guidance as to what changes or initiatives to prioritise (see for example references4–6), which can lead to a scatter gun approach.
As discussed by Morley et al., 7 the fundamental problem is that studies reporting success in reducing overcrowding rarely give sufficient context about the setting and operating conditions in which the intervention was implemented for the reader to understand whether it would work for their system. The same can be said of the edicts, guidance and other influences on local decision makers about what to try next, including anecdotes, folklore and personal experience of what worked well in a different setting five years previously.
In the hospital we worked with, numerous attempts had been made to change workflows within the emergency department, to the extent that staff on the ground felt that there was at times confusion about what protocols and operating procedures were current. Our interviews with staff indicated a widely held view that operational changes were not given sufficient time to bed in before an alternative was tried out. One explanation for this scatter gun approach is that those closest to where problems are manifest (essentially emergency department staff and managers) will often be expected to try changing all of the things that are under their direct control before convincing others in their organisation or beyond that action is required elsewhere. We note that the pattern of not giving ideas sufficient time to succeed (or even conclusively fail) can be repeated at different levels of organisational and political cycles, with each incoming departmental head, trust chief executive or minister keen to promote a solution different from the last.
The 2015 guidance from the Royal College of Emergency Medicine 8 stresses the importance of understanding the local causes of overcrowding before prioritising interventions. However, diagnosing problems in a complex healthcare system can be challenging and what constitutes a feasible intervention can differ between systems.
This is where the disciplines of operational research 9 and organisational ethnography 10 can add valuable insights. Operational research brings a focus on understanding complex systems and a rigour to what is meant by improvement, while organisational ethnography brings a focus on how work is organised and the capacity for organisations to adopt changes.
Differential diagnosis as to why an emergency department is symptomatic
One of the key insights of operational research is that a problem manifest at one point in a system may have its origins elsewhere. It is widely acknowledged that crowding and delays in the emergency department can stem from problems in other parts of the system, either through lack of access to primary care 11 or a lack of beds in the hospital to admit emergency patients to, 12 which in turn may be symptomatic of delays to hospital discharge associated with a lack of community or social care capacity. 2 Of course, sometimes problems in the emergency department can be down to how the emergency department is organised.
Different interventions are designed to reduce overcrowding by acting on different aspects of the system, whether through demand reduction and deflection, managing internal emergency department diagnosis, treatment and decision processes, speeding up admission processes or making space for hospital admissions (Figure 1).
Different interventions (shown in lower case) target different aspects of the system (shown in 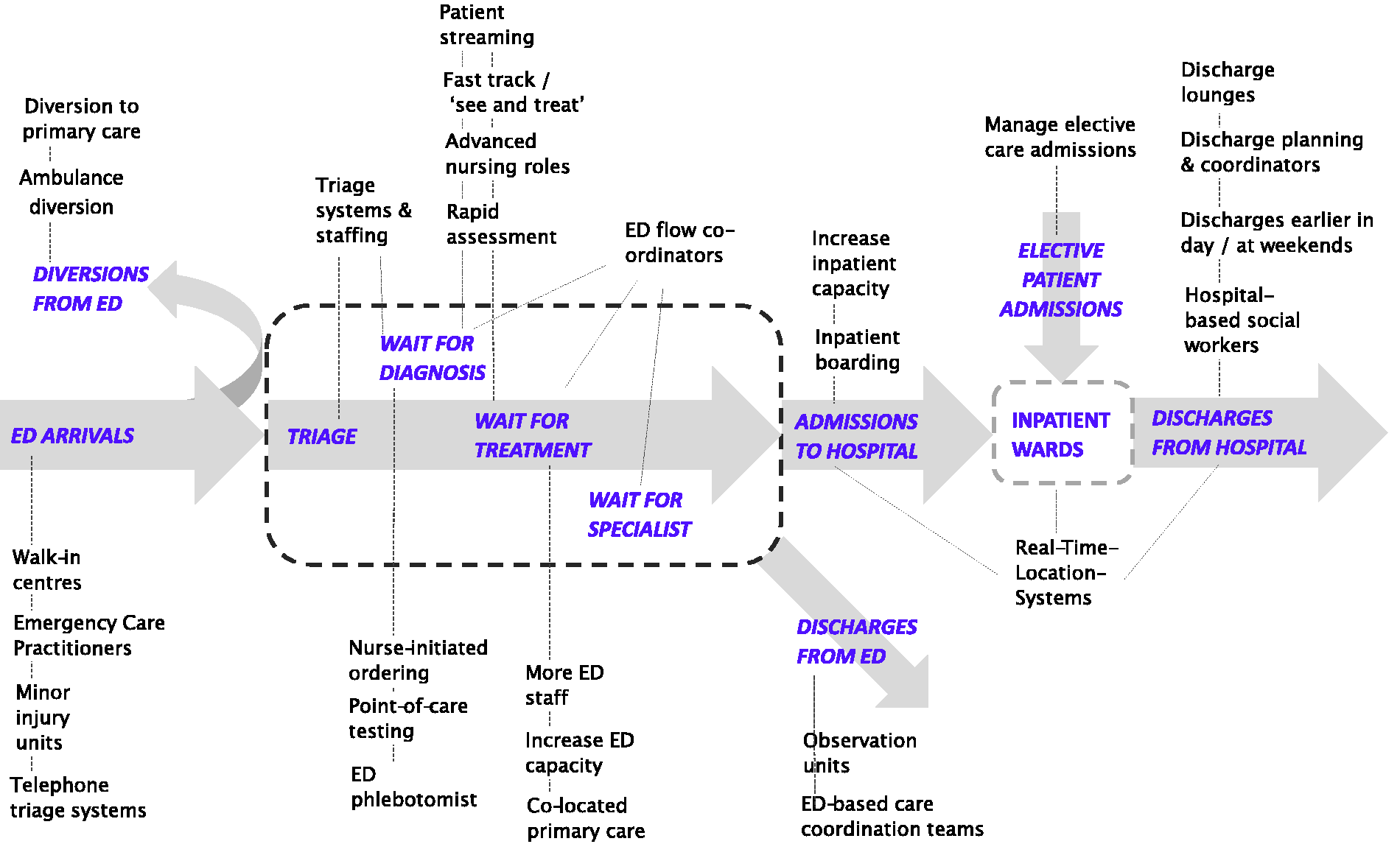
Building on an analogy made by the Nuffield Trust, 13 if physical congestion and delays in the emergency department are symptoms of an ailing system, care is needed to do the differential diagnosis as to why an individual emergency department is exhibiting these symptoms before deciding on what intervention or combination of interventions is indicated.
We recently conducted an ethnographic study for a UK hospital that documented staff perceptions of overcrowding, daily team dynamics in the emergency department, and the relationship between the emergency department and other departments and services. This informed the construction of a simple mathematical model of the system in which their emergency department operated to gauge the intrinsic limits on emergency department performance associated with factors outwith the emergency department’s immediate control. 14 The model, based on queueing theory, 15 was used to assess the nature and scale of improvements that would be associated with successful interventions acting at different points in the system. This allowed managers and staff to prioritise initiatives and have reasonable expectations about their impact.
Defining success and choosing how to fail
Overcrowding is often measured indirectly through the proportion of patients that are discharged from the emergency department within a certain time frame. For example, the target in the UK has been for at least 95% of all patients to be discharged or admitted within 4 h of arrival. In other settings, different time targets are applied to different priorities of patient (e.g. the Canadian Triage and Acuity Scale guidelines on time to clinical review 16 ). While they have proved valuable tools for measuring and motivating improvement in the emergency department operation, it is worth noting that such measures are not direct measures of crowding and, in some cases, can give a narrow view of performance, as discussed in papers from clinical 17 and operational perspectives. 18 This is important because an intervention may act to alleviate symptoms of overcrowding not captured in the metrics used to assess performance.
At the emergency department we worked with, breaches of the UK 4-h target were largely restricted to those patients eventually admitted to hospital, meaning that this performance metric would only be sensitive to changes that affect (directly or indirectly) this small group of patients. Among these patients, the biggest contributor to delay was waiting for a bed once the decision to admit had been made.
Our modelling study confirmed that, in this context, interventions aimed at reducing or deflecting arrivals of low-acuity patients to the emergency department would have little impact on performance against the 4-h target. For instance, reducing low-acuity arrivals by 25% within our queueing model increased the estimated proportion of cases in which the 4-h target would be met from 82% to 86%, as did halving the time between the request and reporting of diagnostic tests. The modelling also suggested that speeding up treatment and decision-making processes within the emergency department would have similarly modest impacts on 4-h performance unless combined with increased availability of hospital beds.
However, both types of interventions could have a beneficial impact on physical congestion in the emergency department and on the service provided to the large group of patients attending the emergency department that do not need to be admitted to hospital. For instance, the same 25% reduction in arrivals of low-acuity patients (which as a group accounted for around half of all arrivals) was modelled to have a disproportionately large effect of reducing the expected number of patients in the emergency department system (from all acuity groups) at peak times from 68 to 50. An organisation therefore needs to be clear what they mean by ‘reducing overcrowding’ since improvements in one aspect (e.g. physical congestion) may require a very different type of intervention from another (e.g. meeting time targets).
Influenced by our work, the hospital we worked with is prioritising action on speeding up admission processes and freeing up beds earlier in the discharge process as the most likely approach for them to improve 4-h performance.
As an aside, it is worth noting that interventions that reduce the arrival of low-acuity patients can, by reducing the size of a group that rarely breach time targets, have the unintended consequence of worsening the apparent performance of the emergency department without worsening the care or experience of any individual patient. This sort of effect can, understandably, motivate differences in which patients get included in the reporting of performance. 19
In pressured, incentivised systems, organisations can feel forced to choose between performing better and looking like they are performing better. Interventions that move patients from the emergency department to trolleys on ward areas can improve apparent performance without necessarily improving care or experience. This can lead to tensions between clinicians in different departments and between clinicians and managers. As operating conditions become such that achieving targets through delivering efficient and effective care aligned with professional standards is increasingly difficult, organisations can be faced with the unpalatable prospect of choosing how to fail.
Right solution, wrong organisation?
Our ethnographic study pointed to the importance of considering the local context when deciding which solution(s) to implement. By this we mean not just the local pressures, problems and demands but also the organisation’s capacity and willingness to address them. For instance, our interviews indicated that emergency department staff and staff in the rest of the hospital had differing understanding of the escalation processes in place for responding to overcrowding. Each group felt that other parties were responsible for emergency department escalation not being effective and highlighted a lack of alignment between emergency department escalation and hospital-wide policies.
The knowledge and engagement of frontline staff is crucial here as, after all, it is these staff that will need to adopt the changes. However, the literature and guidance does not reflect the fact that not all organisations will find it equally possible to implement all solutions. Some interventions need physical space that a hospital may not have, others need additional staff a hospital may not be able to recruit. Some of the solutions in the literature suit organisations adept at adopting new technology, others suit organisations with strengths in streamlining processes within a department through Quality Improvement. Other interventions depend on strong relationships, communication and a sense of shared ownership of the problem across an organisation, others still on open and collaborative relationships with commissioners and with other providers in the local system. Few organisations have strengths in all these areas, and organisations perhaps ought to focus on interventions that are likely to be achievable for them. Extending the clinical analogy, this equates to making an assessment of the treatments that the ailing system is likely to tolerate, adhere to and respond to.
Conclusions
The view of senior clinicians is that, for the current crises in England and many other countries, performance in terms of time to discharge or admission is dominated by problems associated with discharge from hospital and so energy should be focussed on this aspect of the system,2,12 with many of the solutions needing political action. While this is consistent with our study at a UK hospital, it is also important to recognise that some aspects of emergency department overcrowding not reflected in headline metrics can be alleviated through local action.
Hospitals first need to be clear what they want to achieve (reduced number of patients in system, reduced service times for all patients or reduced service times for high-acuity patients?) as this might lead to different choices of intervention. Before trying solutions, a hospital also needs to understand why their emergency department is clogged up. On this front, hospitals may benefit from the insights of operational research and ethnography, whether through strengthening their own analytical capability, collaborating with external academics, using specialised commercial consultants or employing embedded researchers in hospitals. 20
While there is a general awareness and a degree of lip-service is paid to problems in the emergency department being a ‘system problem’, as long as measures, incentives and punishments are focussed on the emergency department, the pressure to ‘do something’ may continue to outweigh the importance of doing the right thing.
Key points
Emergency department crowding and delays can be symptomatic of a range of system problems, so a solution that works in one setting may not work in another. Physical crowding and delays may respond differently to different interventions, so hospitals firstly need to decide what aspect(s) of overcrowding they are trying to improve. To identify the solution(s) most likely to work for them, organisations need an accurate diagnosis of the factors driving overcrowding in their emergency department and a realistic assessment of their scope for adopting new ways of working, informed by engagement with all relevant groups of staff.