
Abstract

Introduction: why uncertainty matters
As if writing prophetically about the global COVID-19 pandemic, in 1984 Eddy suggested, ‘Uncertainty creeps into medical practice through every pore. Whether a physician is defining a disease, making a diagnosis, selecting a procedure, observing outcomes, assessing probabilities, assigning preferences, or putting it all together, he (or she) is walking on very slippery terrain’. 1 COVID-19 has rapidly become a disease associated with unbridled uncertainty with its aetiology and management, for the healthcare systems and health professionals who provide care, and among its ultimate victims, patients and their families.
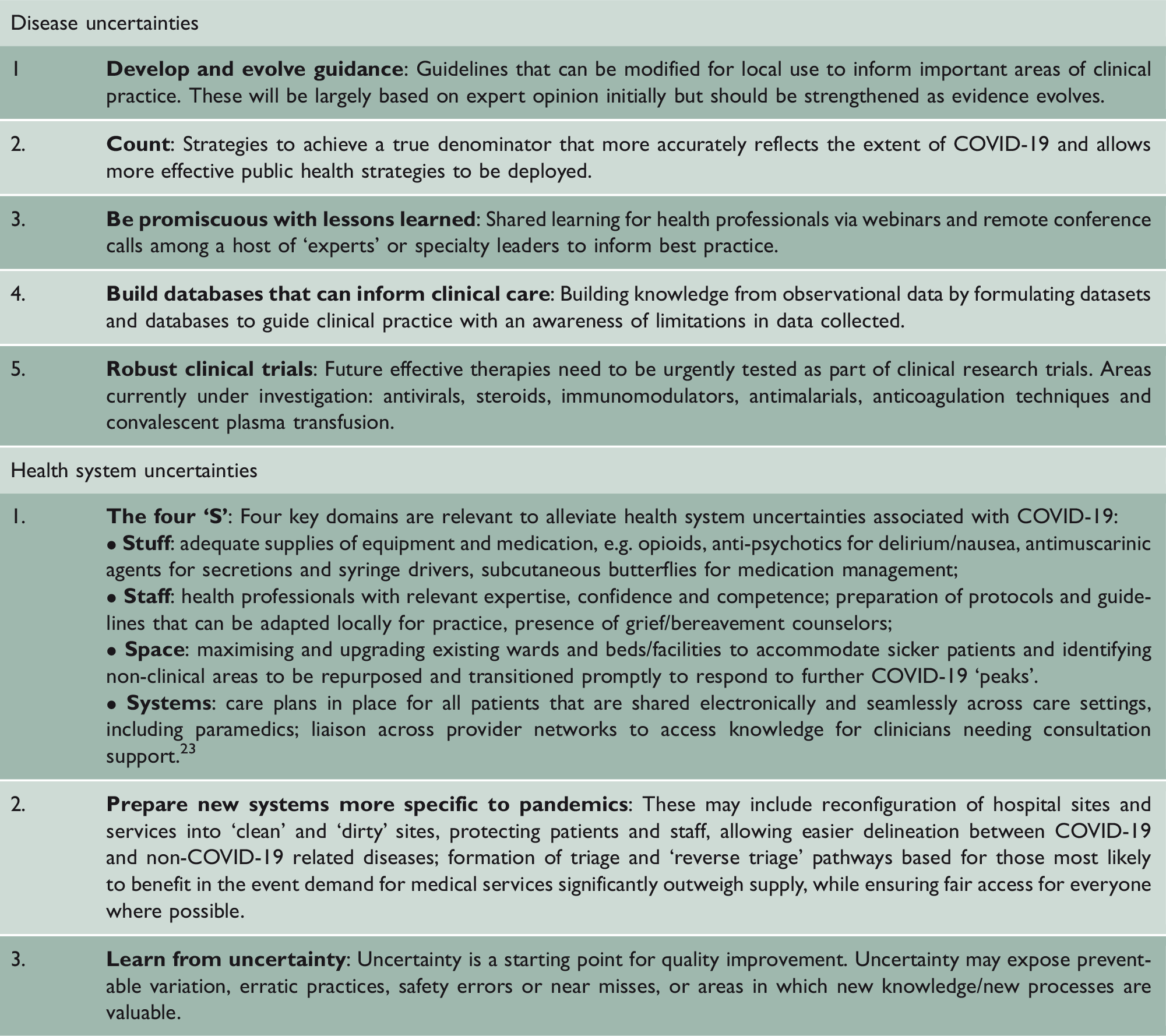
Recommendations to address disease and health system uncertainties.
Recommendations to address health professional, patient and family uncertainty.
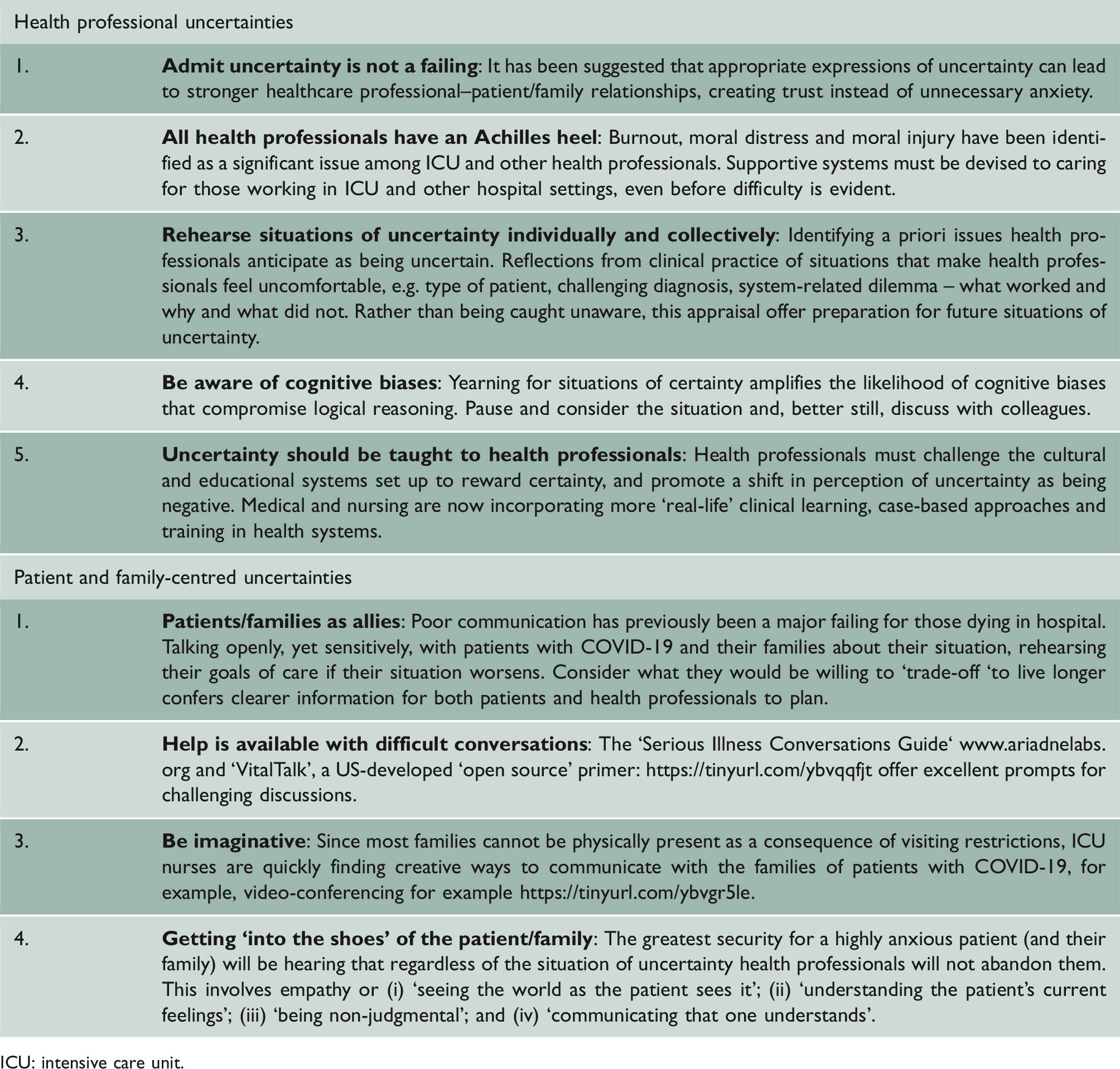
ICU: intensive care unit.
COVID-19: known unknowns and unknown unknowns
At the time of writing, there are over 3.6 million confirmed cases of COVID-19 across 187 countries/world regions, of whom more than 250,000 have now died. 6 Despite these figures, our understanding of the disease is still very much in its infancy. Confusion is present about the uncertain denominator making true mortality figures hard to quantify compounded by the unknown prevalence of asymptomatic infection. Moreover, in many countries accurate testing equipment is inadequate.
We currently lack a sophisticated understanding of the COVID-19 disease process and particularly why some individuals and groups are more affected than others. Those severely affected by the disease are typically over-represented by those who are elderly, those with multiple morbidities and are frail, and mysteriously those from certain ethnic groups. However, the uncertainty of COVID-19 has resulted in catastrophic consequences, regardless of these contributory factors.
As yet, there are no effective therapies for COVID-19 and those available are essentially supportive or palliative. Treatments currently being tested include antimalarial, antiviral, immunomodulator and steroid drugs, often adaptive in design with multiple intervention arms, reducing the chance of patients being randomised to just placebo. However, the trade-off is potential harms may be present associated with multiple-drug interactions. For example, the American College of Cardiology has issued a warning statement of the potential harm and higher risk of mortality when combining hydroxycholoquine with azithromycin. 7
Vagueness extends to an incomplete understanding of patient outcomes. Until recently, mortality figures typically included only hospital deaths but not community deaths, including care homes, confusing the true incidence of the disease. For those with severe enough symptoms to be admitted to hospital, their routes tend to take one of two roads, both of which may lead to a chasm. Those with the best prospects of survival may end up in the intensive care unit whereas those with more underlying problems may be sent to an acute medical unit where they may succumb or survive. Specifically, outcomes data for intensive care unit patients is biased towards those with shorter length of stay because they are still receiving care at the time of analysis, an unavoidable occurrence during a constantly changing pandemic. 8 At present, no information is available on longer-term survival or non-mortality-related outcomes, including quality of life influenced by physical disability, psychosocial morbidity and new dependency needs. 9
In turbulent COVID-19 waters, health systems are ships that require navigation
The COVID-19 pandemic is presenting unprecedented uncertainty in terms of how healthcare systems should respond 10 and exists at the level of structures and processes of care. Specifically, structural uncertainty relates to physical environments of care, medical equipment and consumables. Services are trying to extrapolate from emerging and incomplete data to guide levels of resources required by patients, confused by additional uncertainty as to whether subsequent peaks in COVID-19 may be expected. Hospital beds, intensive care units and their associated equipment, including ventilators and infusion pumps, are vital for the treatment of patients with a severe illness. However, previously untested models have been developed to identify that need.
At the most mundane level uncertainty includes basic hospital resources, medication and the highly publicised provision of personal protective equipment. Not knowing also extends to the location of care. For example, there is evidence that while the number of hospitals beds devoted to COVID-19 has been reducing, there have been unpredicted increases in the level of care provided by nursing homes to frail, elderly people with complex needs, against a backdrop of limited staff and resources.
Moving from structures to processes of care, there is considerable uncertainty concerning how to effectively process and manage patients who have tested positive for COVID-19 and those who have not, particularly if they present in emergency departments, a concern as the COVID-19 nasopharyngeal swab has a relatively high false-negative rate. 11 If patients are falsely screened-negative they may be sent to a ‘clean ward’ environment where they are potentially subjecting other patients and health professionals to risk. Conversely, if based on symptoms they are assumed positive and then located onto a ‘dirty ward’ but subsequently turn out negative, then these patients are in turn put at risk, particularly if they are already vulnerable.
The peak of this pandemic may stretch systems and the decisions required to identify which COVID-19 patients are most likely to benefit from escalating care (including admission to the intensive care unit). These judgements are beset with health process-related uncertainties. It is here that questions should be asked whether decision support aids in line with the best available evidence. The COVID-19: Rapid Guidance for Critical Care developed by NICE emphasises choices be based on the ‘likelihood that a person will recover … to an outcome that is acceptable to them’. 12 However, from what we do know, considerable prognostic uncertainty is present. 13 Where possible, clinicians should attempt to ascertain patients' wishes and values regarding the escalation of care, particularly those who exhibit signs of impending or established organ failure. This should be factored into whether or not an escalation of care to an intensive care unit is appropriate, is in their best interests and acceptable to them. 14 However, in a pandemic scenario, it may be practically difficult to engage in lengthy conversations with acutely unwell patients. In addition, under pandemic conditions, where the availability of resources remains in doubt, it may be much harder to argue ‘all patients be treated without discrimination because everyone is of equal value’ 15 with emphasis on their autonomy. Here, the concept of utilitarianism governing how health systems operate under stress may override this. Decisions to admit might also be influenced by health professionals' implicit cognitive biases 16 to compensate for health system uncertainties regarding intensive care unit bed availability.
People at the epicentre of uncertainty: health professionals, patients and their families
In the face of uncertainty, health professionals may react variably where their training has deliberately focused them towards specialism. However, the trade-off is that there is less personal adaptability for cross-specialty cover and confidence required in the current pandemic. As more health professionals deliver care outside their comfort zones, this has the potential for over-investigation, overtreatment, or its opposite, that may compromise patient safety. 5
Health professionals who believe they are uncertain about how a patient's condition may progress or respond to treatment might feel they have let patients and families down. Moreover, some might make clinical decisions they feel uncomfortable about or disagree with. As a consequence, they may become candidates for ‘moral injury’ resulting in stress, depression and post-traumatic stress disorder. 17 Many patients cared for with COVID-19 may be ‘ill enough to die’. In hospital settings and the absence of family members, health professionals may well be required to comfort these individuals but feel that they lack confidence and competence to do so to good effect, particularly when they are not normally exposed to ‘life and death’ situations in their usual practice. Doubt also extends beyond the patients health professionals care for. For example, they might be working in new ward environments where the stability and familiarity of a known clinical team are not present.
Pre-pandemic times, the existence of an information mountain might have provided a myth of certainty for the wider public. Paradoxically, given the current COVID-19 climate where we are exposed to an ‘infodemic’ of news from multiple sources with multiple, contradictory messages, certainty is now an illusion and anxiety is omnipresent. For those individuals with COVID-19 sick enough to be admitted to hospital, they may rapidly become isolated from families, especially where visiting restrictions are in force. Both parties may be anxious about this period of profound separation and when, or even if, they will be reunited, survive and, if so, what it might look like. This echoes closely with Florence Nightingale's concern for those in vulnerable positions, ‘Apprehension, uncertainty, waiting, expectation, fear of surprise, do a patient more harm than any exertion. Remember he is face to face with his enemy all the time’ (p53). 18 We know from qualitative studies of illnesses pre-dating COVID-19 uncertainty can negatively impact on patients’ experiences and outcomes of care. Where uncertainty about their situation is present, patients become preoccupied to such an extent that their sense of self is changed. 19 Patients and their families often want to discuss their situation of uncertainty; however, this rarely happens. 20
Patients may experience an environment of care alien to any previous hospital experience which may be profoundly disconcerting. The requirement of health professionals to wear personal protective equipment and the possible absence of continuity of health professionals caring for them has potential to amplify this and more so if they are already confused as a direct consequence of their illness or from other co-morbidities. 16
Before the COVID-19 pandemic, evidence suggests exploring patients’ wishes regarding admission to the intensive care unit were uncommon. This is despite evidence of older patients’ decreased willingness to want burdensome therapy or to risk severe disability to avoid death. 21 Patients therefore may need assistance to recognise possible ‘trade-offs’ among their values and to understand the relationship between what is important to them and their families and treatment preferences. 22
If they are not able to obtain timely and accessible information and updates about loved ones, families might be in a state of heightened anxiety. Evidence from an evaluation of a UK-developed intervention to serve patients whose situations were clinically uncertain and where there was a risk they may die during their hospital stay observed inconsistencies in information family members received with concomitant repercussions for satisfaction. 20 Additionally, families may challenge healthcare decisions if they do not understand what is happening.
Multiple barriers to a discussion of prognosis with patients with COVID-19 and their families may be present including lack of time, lack of expertise and a fear of taking away hope. It is also possible health professionals may have overriding concerns not to share their uncertainty about a patient's situation, believing patients and their families might question their competency or honesty, resulting in loss of professional confidence. Nevertheless, it has been shown appropriate expressions of uncertainty do indeed lead to stronger health professional--patient family relationships.
Conclusions
In the current global pandemic of COVID-19, we can not eliminate uncertainty or the multitude of questions and doubts it creates. We argue a paradigm focused purely on its removal is futile. However, it can be managed far better than is done now to minimise its damage. The main business in hand must be for health professionals to support those patients and their families that occupy the ‘grey Covid-19 zone’ and build trusting empathetic relationships with them where uncertainty can be communicated in such a way that enables shared decision-making to reduce distress. 5 We must then learn from this pandemic and develop strategies to change professional cultures that have thrived on developing antibodies to uncertainty and avoiding its presence.