
Abstract

The question
One of the most pervasive questions in the COVID-19 pandemic is ‘differential susceptibility’: Why do some become so ill? We know who is at greatest risk – those with co-morbidities and advanced age – but as yet the ‘why’ is not clear.
The spectrum of disease severity with the COVID-19 infection ranges from the 80% who have a mild to moderate illness and barely notice the infection to the 20% who are quite ill with severe disease, of which one-fourth progress to critical respiratory failure, requiring intubation and ventilator support. Also, 60%–80% of ventilator patients eventually die. The public’s greatest fear is not just becoming ill with coronavirus, but that they may become deathly ill. According to the Centers for Disease Control (CDC), over three-quarters of people with severe disease have significant co-morbidities and/or age over 65 years. 1 Surprisingly, in the United States, about one-fourth of younger people under the age of 65 years with no apparent co-morbidities have life-threatening disease.
Pathophysiology
Although coronavirus victims may develop cardiac or kidney failure later in their clinical course, the hallmark of severe disease is respiratory insufficiency with confluent areas of pneumonia. Patients report they feel like they are drowning and rapidly progress to respiratory failure, acute respiratory distress syndrome (ARDS) and requisite ventilator support. This deadly clinical picture of ARDS apparently results from the virus triggering intense inflammation resulting in damage to the walls of the alveoli with capillary leakage of protein-containing fluid that fills up the alveoli. The result is severe respiratory failure, rapidly progressing to death in 60%–80%. 2 When the virus infects the lung cells in some patients, it elicits an intense, immune over-reaction sending in leukocytes that release pro-inflammatory cytokines, especially IL-6. The resultant runaway hyper-inflammation termed ‘cytokine storm’ unfortunately damages the normal lung cells more than the virus it targets. Cytokine storm causing ARDS is the common denominator for respiratory failure and death not only in COVID-192 but also in Middle East respiratory syndrome (MERS), severe acute respiratory syndrome (SARS) and H1N1 influenza.
Cytokines are a diverse, large group of proteins released by various immune system cells that regulate inflammation and immune function. Some cytokines cause inflammation and others calm it down. Chronic inflammation 3 is a common theme in a number of age-related disease states such as hypertension, coronary artery disease, chronic lung disease, liver and kidney disease, obesity, diabetes, autoimmune and immunocompromised disorders, cancer and advanced age – all of which are the common co-morbidities that increase the risk of severe COVID-19 respiratory disease. The newly created COVID-19-Associated Hospitalization Surveillance Network just reported that nearly 90% of the hospitalised patients (with severe disease) in March 2020 had some type of underlying condition. Obesity was the condition most often seen in the younger age groups: 49% of those aged 50–64 years and 59% in those aged 18–49 years. 4 The Office of National Statistics in the United Kingdom just reported that 90% of COVID-19 patients dying have an underlying co-morbidity. 5
Since hyperinflammation may be the key pathophysiologic pathway leading to severe COVID-19 pneumonia, then corticosteroids that vigorously suppress IL-6 and multiple other cytokines should provide great therapeutic benefit. Despite concerns that corticosteroids may delay viral clearance and be detrimental, 6 the recently completed randomised, multicentre RECOVERY Trial randomised study of 6425 patients demonstrated that the use of the common corticosteroid dexamethasone significantly reduced the 28-day mortality in hospitalised COVID-19 patients requiring respiratory support. 7 Theoretically, more targeted anti-cytokine IL-6 blocking agents may provide greater benefit in this hyperinflammatory state with cytokine storm pneumonia, but clinical trials of this therapeutic strategy are still ongoing. 8
Potential explanation
The term ‘inflammaging’ (inflammation with aging) was coined in 2006 3 to describe the chronic, sterile pro-inflammatory process occurring in age-related diseases associated with the decline in the effectiveness of the immune system termed immunosenescence. Along with the chronic inflammatory state in these degenerative diseases, pro-inflammatory cytokines are significantly elevated, especially the cytokine IL-6. Current smokers and obese individuals also have marked chronic inflammation and elevated cytokines. Even just a sedentary lifestyle in younger people results in a chronic pro-inflammatory state, which is aggravated further by a poor diet that is deficient in fruits, vegetables and whole grains, and is filled with refined sugars and high amounts of saturated fats, meat and processed foods (pro-inflammatory diet). 9
Recent statistics show that minorities, especially African Americans, have a disproportionate higher mortality from the virus, amounting to 42% of all deaths where the demographic data are known. 10 This disparity has been immediately attributed to inequality in healthcare, air pollution, poverty and/or depressed economic opportunity. Perhaps there is another factor at work? France’s chief epidemiologist Jean-François Delfraissy stated that he was worried about Americans ‘where they will have the most problems because of obesity’. 11 According to the CDC, 42% of Americans are obese but that number rises to 50% in African Americans. Diabetes, hypertension and kidney disease are complications that commonly accompany obesity: all of these problems cause chronic inflammation and elevated cytokine levels. The culturally preferred, pro-inflammatory high saturated fat/high salt//high refined sugar diet and pronounced physical inactivity may predispose urban African Americans living in areas of high population density to a more severe disease course with COVID-19.
Although many scientists are desperately searching for the genetic polymorphisms that predispose COVID-19 victims to a poor outcome, perhaps there is an alternative, plausible explanation for this so-called ‘differential susceptibility’ that causes some individuals to progress to severe respiratory disease. The common thread that runs through all of the co-morbidities (including obesity and advanced age
3
) that is associated with severe disease is the presence of a turned-on, overactive immune system with chronic inflammation and elevated cytokine levels. Therefore, it is logical that where there is ongoing chronic inflammation that adding an acute viral infection/inflammation such as COVID-19 (or MERS, SARS or H1N1 influenza) is essentially pouring gasoline on the already-burning fire, resulting in hyperinflammation and severe disease. Figure 1 is a graphic summary of the proposed pathway to severe COVID-19 disease.
Pathway to severe COVID-19 disease.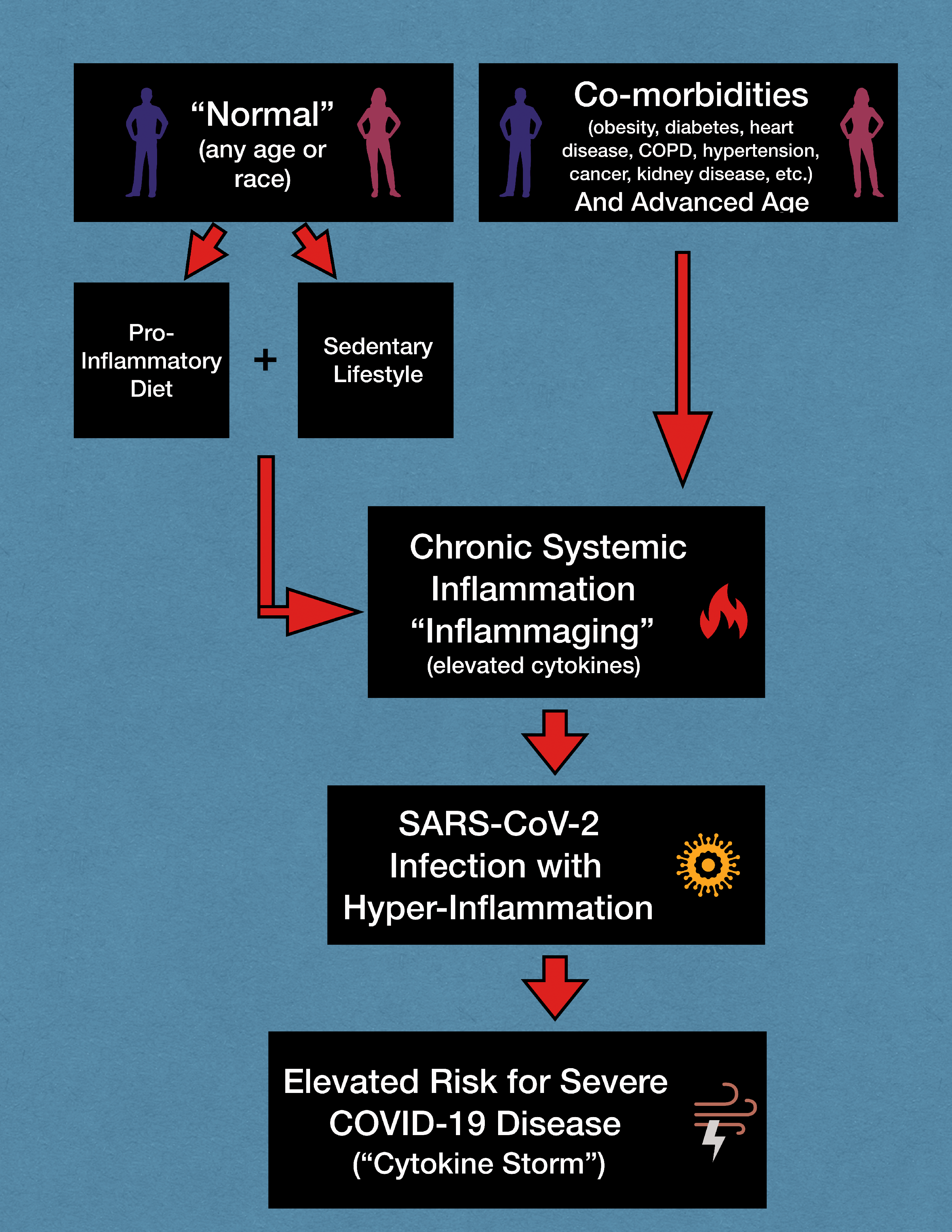
Short-term measures
If chronic inflammation from its various causes is the key to severe disease, are there any short-term measures that these high-risk individuals can do to lessen their possibility of adverse effects if infected with the virus? Fortunately, lifestyles changes can rapidly decrease chronic inflammation and high cytokine levels, independent of co-morbidities. Aerobic exercise provides the fastest results, but coupled with diet modifications inflammatory markers drop rapidly.12–14
In light of the current COVID-19 pandemic with the necessity of following shelter-at-home orders, many people worldwide are practising an unsustainable lifestyle including a poor diet of high fat, high sugar ‘comfort foods’ and minimal exercise that promotes even more whole-body inflammation as they sit working from home and/or watching television.
Even if certain genes or families of genes are eventually discovered that predispose to more severe COVID-19 disease in some people, this does not mean that individual is doomed if they develop the infection. Studies have demonstrated that ‘DNA is not your destiny’. 15 Genes are only functional if they are activated by their ‘off-on switches’, the epigenes. Lifestyle and environmental factors (such as diet, exercise, smoking, etc.) control the epigenes 16 which in turn control silencing or activation of genes, including the detrimental ones that might predispose to severe COVID-19 disease.
Limitations
Even though this hypothesis of systemic chronic inflammation predisposing to severe disease logically may fit the reported demographics, it still may not be an important feature of the pathophysiology of the disease since Nature does not always follow human logic. Hopefully in the future, careful epidemiological studies of the pre-illness lifestyle of victims of severe COVID-19 disease will help prove or disprove this hypothesis. However, in the meantime, would it not be prudent for people to dramatically change their lifestyle to a healthy diet, daily exercise and no tobacco? It definitely will result in less degenerative diseases in the long term, and in the short term it may save their life.