
Abstract

Diagnostic errors present a major problem in health systems, with a recent study estimating that diagnostic error alone may account for 795,000 cases of permanent disability or death annually in the United States. 1 Consequently, there have been renewed calls to re-evaluate and strengthen clinical reasoning processes through various pedagogical and practice-based interventions. 2 Traditionally, clinical reasoning has been understood from the perspective that human cognition operates at two levels: either an automatic, intuitive process that is unconscious, rapid and highly reliant on pattern recognition, or a slow, deliberate, systematic, analytical thought process that is activated when faced with unfamiliar problems.2,3 Within such a framework, ‘biases’ (defined as structured, predictable, systematic errors in thinking) have been singled out as the major cause of cognitive errors, associated with over-reliance on intuitive judgements, such that an overwhelming proportion of clinical reasoning literature and quality improvement endeavours have focused on de-biasing interventions. Yet, it remains unclear if cognitive de-biasing strategies, especially those that require clinicians to actively slow down and systematically weigh individual options in decision-making, are truly effective and can be habituated into routine clinical practice. 2
Recently, it has been suggested that ‘noise’ (defined as an undesirable variability in human judgements) is a highly important, yet under-recognised source of error in human decision-making, which is potentially easier to tackle as compared with cognitive bias, through the implementation of noise audits and standardised decision-hygiene frameworks.4,5 Therefore, in this article, we sought to spotlight the problem of ‘noise’ in clinical decision-making, and discuss its contributors as well as practical pedagogical and practice-based interventions that may reduce undesired variability in clinical practice that compromises the quality of health services.
Defining ‘noise’ and identifying its contributors in clinical decision-making
In Nobel Laureate Daniel Kahneman et al.’s most recent work, 4 they identified ‘bias’ and ‘noise’ as the two major sources of errors in human decision-making – where bias refers to predictable, systematic errors skewed in the same direction, and noise is randomly scattered error due to judgement variability. 4 The distribution of errors in biased and/or noisy decision-making is perhaps best visualised with a shooting target illustration (Figure 1). While biases are a well-known phenomenon in decision-making, noise remains an under-recognised but highly prevalent issue (to the extent that ‘wherever there is judgment, there is noise’ 4 ) and reduction of either bias or noise will improve judgement accuracy 4 ).
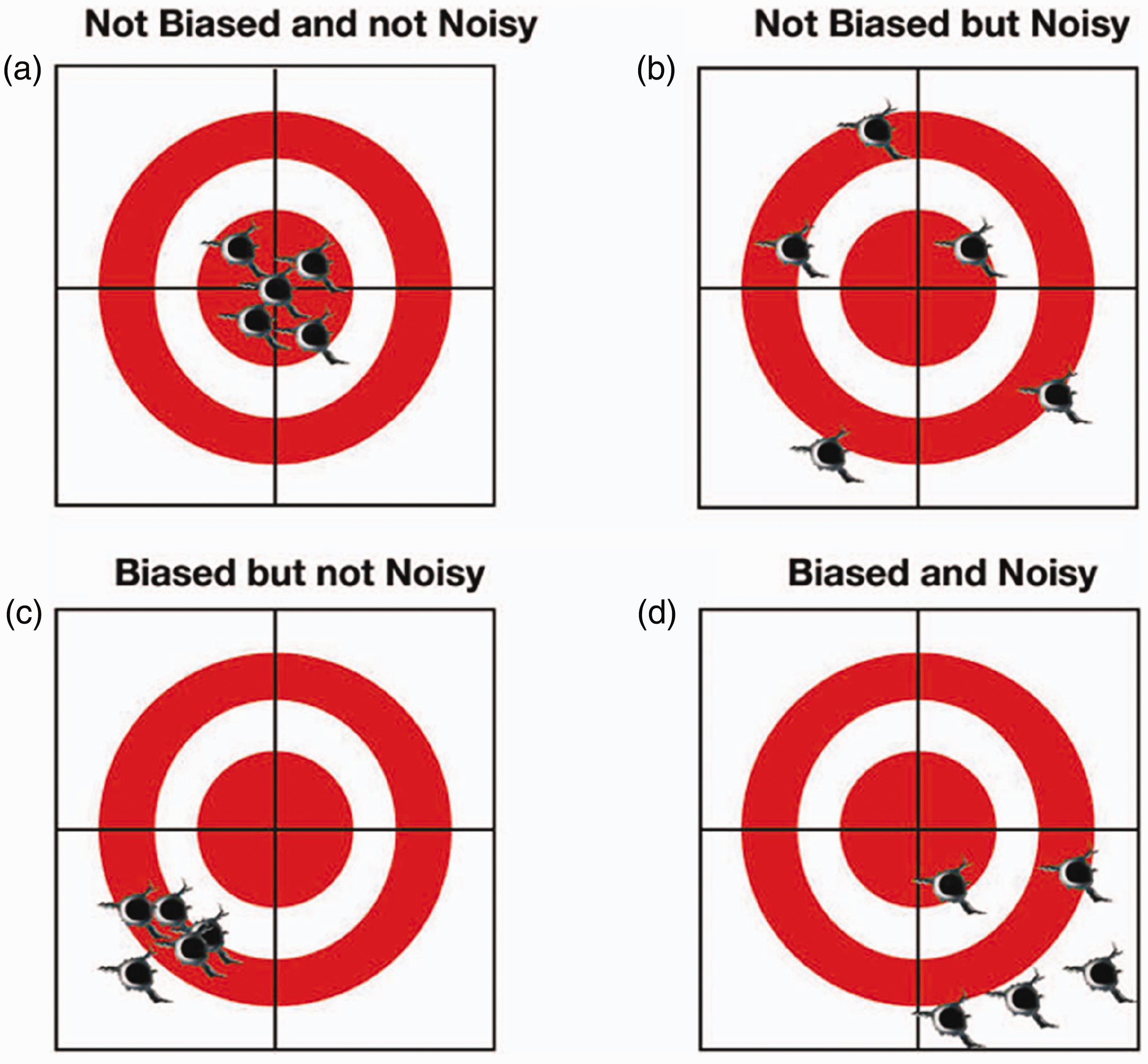
Depiction of ‘noise’ and ‘bias’ in decision-making using a shooting target illustration. The figure is reproduced from Mullins and Coughlan,5 with permission obtained from the article’s corresponding author Dr. JJ Coughlan and copyright holder Oxford University Press (license number: 5947530278516, license date 14 January 2025).
To be clear, ‘noise’ is not merely any form of heterogeneity in human thinking/behaviour, which could be desirable to allow for flexibility and creativity in decision-making, but instead strictly refers to a pre-defined unacceptable or undesirable level of practice variability that leads to inconsistent, unreliable and poor-quality decision-making. 4
In the clinical realm, significant practice variation may be observed either between different physicians (i.e. level noise 4 ) or within the same physician but under different circumstances (i.e. pattern noise, or occasion noise 4 ). In 2022, Song et al. performed a nationwide cohort study in the United States, which found sizeable physician-level practice variations in seven studied subspecialties by looking at clinical decision-making in 14 common clinical scenarios. 6 In fact, ‘noise’ could be observed in decisions made in all areas of clinical practice – from diagnostic testing, 7 health screening, 6 to treatment decision-making such as medication prescriptions or surgical/procedural interventions, 6 goals-of-care decision-making 8 and referrals to allied health services 6 or other subspecialties. 9 Among the variables that could influence clinical decision-making, Cutler et al.’s study in 2019 reported that physician beliefs about medical treatment were the most important predictor of heterogeneity noted in Medicare claimable clinical services utilised. 10 They posit that the physicians’ beliefs and actions were often guided by their knowledge/expertise (or lack thereof), experiences, personality/practice styles and individual responses to patient/referring colleagues’ requests and malpractice concerns. 10
At the broader level, there are also significant geographical/regional heterogeneity in terms of offered clinical interventions for common conditions, which are generally reflective of differences in local physician training and practices, patient profile/demand for interventions, availability of relevant specialists, technology and resources and locoregional regulatory frameworks. 11
Intriguingly, besides inter-physician practice differences, studies have also found intra-physician variability in prescription habits (e.g. opioids, antibiotics) attributed to environmental factors such as time of the day,12,13 where common patient-requested, but clinically less appropriate medications tend to be prescribed more liberally towards the end of the clinic session or work day when there is greater physical/decisional fatigue.
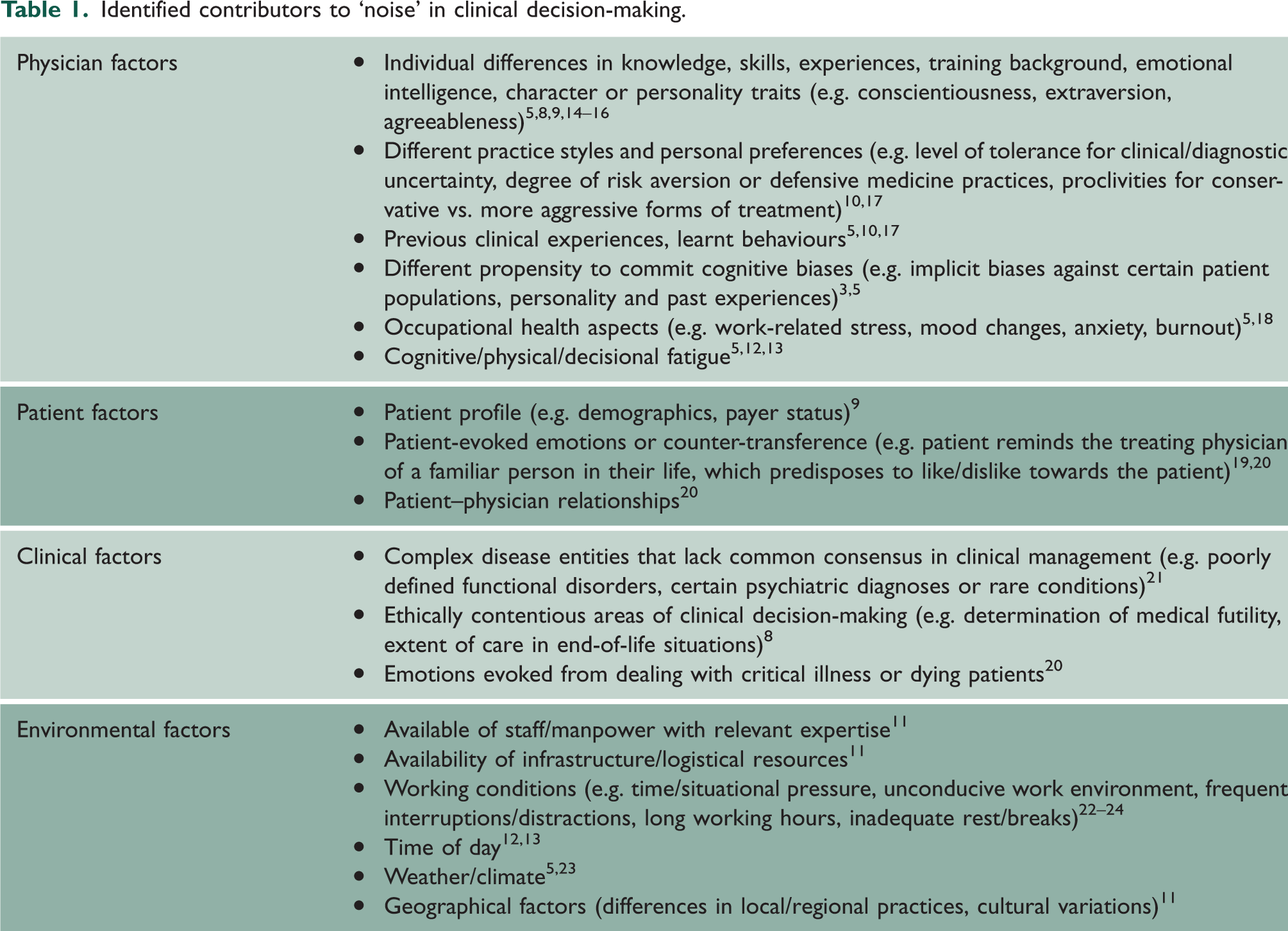
From literature review and our practice experiences, we herein summarised a comprehensive list of physician, patient, clinical and environmental-related factors that commonly contribute to ‘noise’ in clinical decision-making3–6,12 (Table 1).
Identified contributors to ‘noise’ in clinical decision-making.
Mitigating ‘noise’ in clinical practice and health systems
Before we can begin to address the problem of ‘noise’ in clinical practice, it is necessary to first recognise that it exists. 4 For the individual physician, metacognitive practice through reflection, mindfulness and consciously seeking out feedback on clinical decision-making helps to increase self-awareness of how personal practices and decision-making can be influenced by situational/environmental variables. 3 Interestingly, a recent study highlighted the potential of using a patient outcomes-driven feedback platform to cultivate closed-loop learning and enable self-regulation of one’s practice habits. 25 At the institutional level, routine ‘noise’ audits can be conducted to measure the extent and source of ‘noise’ in the health system. 4 This could be done through anonymous surveys on physicians to assess their clinical judgements/decision-making on common clinical scenarios, or retrospective case reviews to assess internal practice variations in the management of similar patients. The intention of such noise audits is to detect the level of noise and determine internally how far it exceeds what is considered an acceptable/healthy level of practice variability.
There are various pedagogical or practice-based strategies that may reduce ‘noise’ in clinical practice, which should be applied based on internal root-cause audits/analyses on predominant contributors to system noise.
First, maintaining high standards of clinical skills with regular workplace-based assessments remains important – as this reduces ‘noise’ introduced by wrong clinical judgements due to incompetency/knowledge deficits. Specifically, foundational teaching on clinical reasoning first principles (such as adopting a Bayesian-centric testing-and-treatment threshold model) would be useful in standardising physicians’ approaches to clinical decision-making. 2
Second, decisional fidelity may be further enhanced through the following methods: consensus/institutional guidelines, 3 artificial intelligence driven clinical decision support systems, 26 and use of choice architecture with appropriate behavioural nudges 27 (e.g. pre-orders/default options to optimise prescribing habits). In particular, there are specific ‘decision hygiene’ templates that have been proposed, including breaking down clinical problems into small, discrete assessment items, sequencing judgements to avoid arriving at premature conclusions4,28 and collating aggregate judgements of various ‘experts’ 4 (‘wisdom of the crowd’; e.g. medical grand rounds to discuss complex cases) or actively challenging one’s own assumption/generating differential explanations (‘the crowd within’; also known as Herzog and Hertwig’s ‘dialectical bootstrapping’ method 29 ). Heuristics-based decision hygiene templates have also been proposed, such as the ‘pivot-and-cluster’ strategy (identifying primary diagnosis, and clustering differentials with radius of cluster guided by degree of clinical uncertainty), 28 or practising a three-step clinical reasoning documentation of counter-diagnostic features, things that do not fit and red-flags. 30
Third, optimisation of physicians’ physical and mental condition during decision-making can be achieved through psychological strengthening and practical improvements to the immediate working environment. For instance, cognitive-behavioural techniques, self-care and stress management strategies, as well as workplace support groups could be helpful to regulate experienced emotions or psychological distress in clinical practice to avoid maladaptive coping and decision-making. 3 Moreover, systemic improvements in working environments such as regulation of duty hours, work intensity and frequency of interruptions, as well as provision of adequate administrative/information technology support would all contribute to reduction of cognitive overload and physical fatigue that could cloud clinical judgements. 12
Conclusion
In summary, we herein described ‘noise’ as a highly prevalent and hitherto under-recognised source of error in clinical decision-making. The appropriate strategies to reduce ‘noise’-induced errors in health systems require a nuanced approach guided by noise audits that measure degree of ‘noise’ and its contributing factors, in order to decrease unhealthy practice variation while preserving a necessary degree of physician autonomy to practise individualised, person-centred medicine.