
Abstract
The immediate management of poisoned patients is a major activity in emergency departments and acute medical wards. This can mean the neglect of more detailed enquiry that would make clear the underlying cause of the poisoning and suggest ways to reduce the risk of repeated poisoning for the individual and more generally. The history and circumstances of poisoning may make the precipitants evident, but it is still important to consider what factors contributed. Here, we divide poisoning into unintentional and intentional, and suggest how these major groups may be subdivided. There is a need in unintentional poisoning to consider whether the patient has been poisoned because of their vulnerability, for example, resulting from dementia. Where a carer such as a parent or partner has committed an error, they too may be vulnerable. If the poisoning is a result of error by a clinical professional, then the question of clinical competence can arise. If the poisoning is deliberate, mental ill-health may have contributed, and the patient may not have capacity to make decisions. There may also be a conflict between what the patient wants and what the clinician deems to be in the patient’s best interest, in which case it may be necessary to consider mental capacity. A systematic approach to these important questions can offer the best prospect for prevention of further poisoning for the individual. Broader attempts to prevent poisoning require good data on the causes and circumstances in which it occurs, but these are often lacking.
Introduction
Clinical toxicology focusses on the immediate management of the poisoned patient: life-saving measures, clinical and laboratory investigations and appropriate general and specific treatments. Careful investigation of what led to poisoning, which is usually a less urgent concern, has received less attention. It is nonetheless important because understanding the factors that have led to poisoning, both for the individual and more widely, can help to prevent further episodes. This is true whether the patient has intentional self-poisoning, poisoning due to error or criminal poisoning. The treatment of the poisoned patient depends, to a large extent, on the poison or class of poison used and the clinical syndrome (the toxidrome) thus produced. That is beyond our scope here. Instead, in this commentary, we suggest an analytical scheme to make explicit the factors that led to an episode of poisoning, so that healthcare professionals can take appropriate actions to protect their poisoned patients and help prevent further episodes.
Methods
We based our review on the experience gained in a busy poisons unit, supplemented by a focussed literature search.
Discussion
Intentional and unintentional poisoning
The reasons for poisoning can broadly be divided according to the underlying intent. Intentional poisoning is the result of a conscious decision to cause harm or – for example, in the case of adulteration – to ignore possible harmful consequences. Unintentional poisoning is the result of an error or mischance.
Harm from toxic effects is very common. On average, in each of the 6 years 2017–2022 in England, there were 48,900 admissions to hospital for which a principal discharge diagnosis was ‘self-poisoning’. Of those, 23,600 cases were in people aged 20–39 and 4600 in people aged 60 years or older. 1 For many episodes, the question of intent is answered by the patient’s account of events or by the circumstances in which they are found. It is insufficient, however, simply to assume that a case of poisoning was intentional or unintentional, even in cases that appear straightforward. An individual who works in an electroplating workshop and who has slipped and fallen into a bath containing cyanide might have been poisoned unintentionally by mischance, but malevolence might also explain the facts; were they, for example, pushed? And in another case, a suicide note and several empty packets of tablets might lead to the assumption that the poisoning was intentional, but duress or subterfuge could not necessarily be excluded.
Vulnerability
An assessment of the factors underlying an episode of poisoning is especially important in vulnerable patients, who may be less able to make decisions in their own best interests. The NHS defines being vulnerable as ‘in need of special care, support, or protection because of age, disability, risk of abuse or neglect’. 2 This does not, it seems, include those who willingly indulge in dangerous activities such as hang-gliding or cigarette-smoking.
Vulnerability is most often encountered at the extremes of age. The United Nations Convention on the Rights of the Child defines a child as ‘every human being below the age of eighteen years unless under the law applicable to the child, majority is attained earlier’. 3 In England and Wales, children are those under compulsory school age and young persons are those above compulsory school age but below the age of 18 years. Children and young people are, by legal definition, considered to be vulnerable. Toddlers are especially vulnerable to poisoning. 4 Older adults can become vulnerable as they lose intellectual ability, acquire physical disabilities and are prescribed more medication. This is an increasing problem in clinical toxicology because both the number and proportion of older people who attend hospital with poisoning is increasing in developed countries. Contributory factors are the increasing rates of unintentional poisoning with age after middle life that result from medication errors related to polypharmacy or inadvertent exposure to household products, and the increasing rates of intentional self-poisoning.
For example, in the United States in 2021, rates of suicide by poisoning were reportedly 20 to 25 per million in men aged 55–84 years, and 35 per million in men aged 85 years and older. 5 Reported rates of suicide by all causes increased with age after middle-age in the European Union, from 147 per million between 50 and 54 years to 265 per million in those 85 years or older in 2022. 6 In Austria, the rate was 157 per million at the age of 50–54 years, and 521 per million at 85 years or older. The ‘5-D’ model, a recent description, lists the factors leading to suicide in older life as: Depression, Deadly means (of self-harm), Disease (multimorbidity), Disconnection (social isolation and loneliness) and Disability (and dependence). 7
Capacity
Capacity is the term used to describe the ability to make decisions. This ability has four components: to understand relevant information, to retain it, to weigh possible alternative courses of action, and to express the preferred course of action.
In England, it is assumed that all adults and young persons over the age of 16 years are able to decide how they want to be treated, unless they are shown to lack capacity, either temporarily – for example, as a result of acute delirium, or because of acute mental illness, or permanently – for example, as a result of brain damage or dementia. 8 In many cases, the patient and the doctor can agree that treatment is in the patient’s best interests, and as a result the patient accepts treatment. When a patient lacks capacity to make decisions, and cannot agree – for example, because they are unconscious – the doctor must act in the patient’s best interest, using formal procedures. In England and Wales, these are governed by the Mental Capacity Act 2005.
There will also be circumstances in which patients represent a danger to themselves or others by reason of psychiatric disease, in which case it may be appropriate to organise detention in a hospital for them to receive treatment under a section of the Mental Health Act 1983. 9
Care after recovery from poisoning will often include psychiatric or psychological support. One difficulty is that the patient may choose to curtail suffering at the end of life by taking poison. In some jurisdictions, and recently debated in England and Wales, the law allows ‘assisted dying’ in some circumstances. The patient can then enlist the active help of a doctor to take poison to end suffering at the end of life. By extension, a patient who experiences great suffering and is near to death may retain mental capacity and choose to end life by self-poisoning. However, it is currently an offence in England and Wales, under the Suicide Act 1961, for a person intentionally to do an act capable of assisting the suicide or attempted suicide of another person. 10
A scheme of analysis of the underlying cause of poisoning
A suggested analytical scheme is shown in Figure 1.
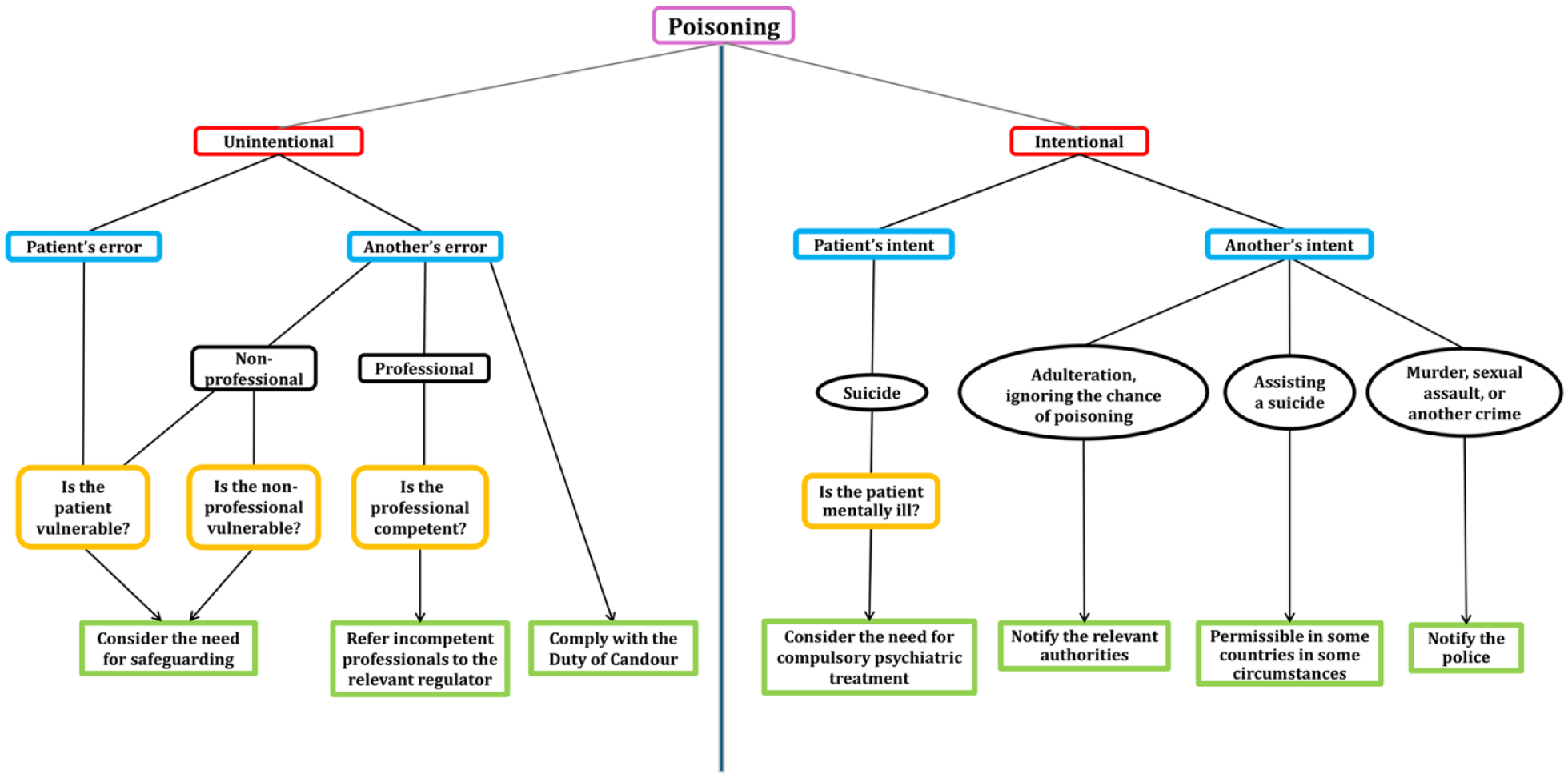
Factors to consider in analysing the events associated with poisoning.
In this scheme, the first step is to decide whether the event was unintentional. Unintentional events are in practice usually the result of an error. Generally, errors can be considered as mistakes, slips or lapses. 11 Mistakes are errors in the planning of an action. They can be knowledge based or rule based. Slips and lapses are errors in carrying out an action – a slip through an erroneous performance and a lapse through an erroneous memory. Errors that arise from an absence of elementary precautions, or from acts that any reasonable person would predict to cause harm, may be classified as negligence.
If an error has been made, then it is necessary to consider whether the error was made by the patient or by another. Examples of errors leading to poisoning include a person picking and eating a toxic mushroom misidentified as safely edible 12 ; a mother inadvertently leaving tablets within reach of a toddler 13 ; or a pharmacist negligently dispensing a medicine of the wrong strength. 14
If the error was made by the patient, consider whether vulnerability has led to error. 15 Older people, in particular, may be physically vulnerable because of infirmities, and they are also more likely to suffer from cognitive impairment that diminishes their capacity to make decisions on their own behalf. The incidence of dementia rises steeply with age, from 4 per thousand in those aged 60–69 to 65 per thousand in those aged 80–85. 16 For adults who have made errors and appear vulnerable, there is a system of ‘safeguarding’, which seeks to protect the individual from harm. Safeguarding may also be relevant if the error was made not by the patient but by another. Toddlers, keen to explore their environment, are clearly vulnerable, and parents are responsible for ensuring that children are kept safe. A parental error may put a child in danger. Healthcare professionals have a duty to establish whether there is a need for ‘safeguarding’ for any child, young person or adult at risk who has or may come to harm. The UK Department of Health issues guidance on this, 17 as do others. 18 The elements of safeguarding include providing help and support, protecting from maltreatment and ensuring safe and effective care.
If the error is made by a healthcare professional, it is necessary to consider the reasons for the error, which can include insufficient experience or training, fatigue, staff shortages, and illness. 19 Formal systems exist to report potential incompetence by healthcare personnel, including doctors and nurses, to regulatory bodies – in the United Kingdom, the General Medical Council and the Nursing and Midwifery Council. There is a statutory Duty of Candour in the UK that obliges a health service body to act in ‘an open and transparent way with relevant persons’ if a notifiable safety incident has occurred. 20 The most serious errors in clinical care can lead to a charge of gross negligence manslaughter, 21 but even lesser errors need actions to alert the professional concerned and to report the errors, in the hope of preventing future, and potentially more serious, errors. In other circumstances, it may be necessary to involve specialist agencies, for example the UK Health and Safety Executive for UK workplace-related incidents, or medicines regulatory agencies, such as the US Food and Drug Administration or the European Medicines Agency for medicinal or food safety errors. It may be necessary to involve health protection services when a potential public health risk exists or notify the police when a crime is suspected. 22
Negligent exposure to toxic substances can result in unintentional poisoning, sometimes affecting many people. Examples include poisoning episodes from illicitly distilled spirits contaminated with methanol 23 ; from medicines made up in diethylene glycol 24 ; and from shellfish containing poisonous amounts of organic mercury. 25
One rare category of unintentional poisoning is that which arises from natural events, as happened with the release of a gas cloud from Lake Nyos in Cameroon 26 and toxic gas emissions from the Whakaari volcanic eruption in New Zealand. 27
Most toxic events that result in admission to hospital are, however, intentional, and usually attributable to the patient. Rarely, another person intends to administer a toxic substance to someone to do them serious harm or to kill them. Doctors, even clinical toxicologists, rarely consider whether a patient has been deliberately harmed by another, and unless there is some suspicion, it is difficult to demonstrate that this has happened. A counsel of perfection is to consider in every case whether it was the patient or another who had the intent to cause harm. It may be that, even if the patient had intentionally taken a poison, the act was precipitated by coercion on the part of another. It also happens that the patient intends to take a drug, unaware that it has been adulterated – for example, levamisole added to cocaine, or fentanyl admixed with heroin – with unintended but serious consequences.
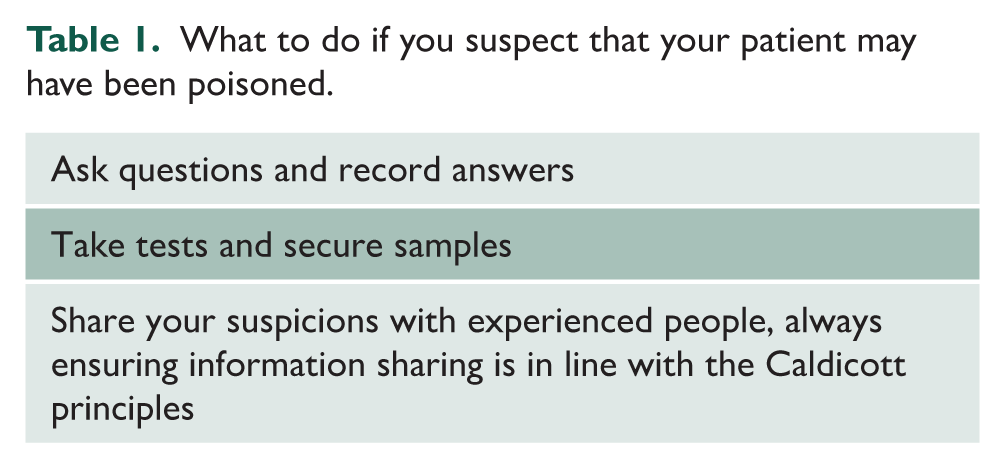
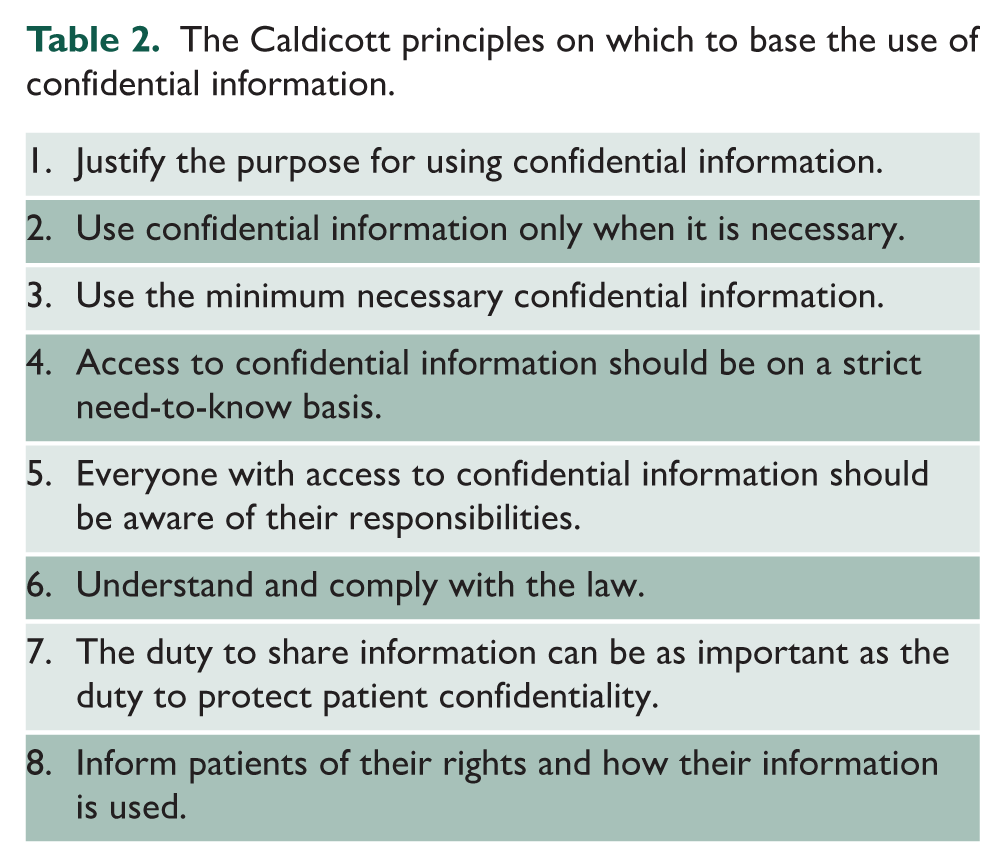
The duty to pursue a diagnosis of deliberate criminal poisoning falls not on the physician, but on the police, who should be contacted if there is any reasonable suspicion of a crime. Preliminary steps can help to increase or allay suspicion (Table 1). In all circumstances, it is the duty of healthcare professionals to maintain confidentiality as prescribed by law. In the United Kingdom, the rules are set out in the eight Caldicott principles (Table 2). 28
What to do if you suspect that your patient may have been poisoned.
The Caldicott principles on which to base the use of confidential information.
Prevention of future episodes
It is important after treating a poisoned patient to consider how to prevent episodes in others. In order to do this, detailed information about the clinical characteristics of individual cases, the poisons used and the circumstances in which the poisonings occurred would be helpful. However, the routine hospital episode statistics and information about deaths are related to the ICD codes, which are currently non-specific and therefore unhelpful. Some information, for example from the National Poisons Information Service, contains more details, but covers only a small proportion of cases of poisoning, and is often incomplete. Information from inquests, which might also be of help, is largely lost or ignored and lessons are not learnt. 29
When information is collected, effective action can be taken. For example, understanding of the factors leading to paracetamol overdoses led to restrictions of the purchase of over-the-counter paracetamol, which led to a reduction in the incidence of self-poisoning. 30
Conclusion
The protection of poisoned patients presents healthcare professionals with ethical and practical dilemmas. How they are resolved depends on an assessment of whether the event was unintentional or intentional, who was responsible and whether the patient lacks capacity or is vulnerable in another way. Most patients who are themselves responsible for the event will accept treatment, but when they do not and when they lack capacity, it may be necessary to invoke formal procedures to allow treatment to proceed.