
Abstract
In spite of the existence of good empirically supported treatments for posttraumatic stress disorder (PTSD), consumers and providers continue to ask for more options for managing this common and often chronic condition. Meditation-based approaches are being widely implemented, but there is minimal research rigorously assessing their effectiveness. This article reviews meditation as an intervention for PTSD, considering three major types of meditative practices: mindfulness, mantra, and compassion meditation. The mechanisms by which these approaches may effectively reduce PTSD symptoms and improve quality of life are presented. Empirical evidence of the efficacy of meditation for PTSD is very limited but holds some promise. Additional evaluation of meditation-based treatment appears to be warranted.
Keywords
Each year, millions of people worldwide are exposed to traumatic events, such as natural disasters, war, motor vehicle accidents, and assaults. Following such events, a significant minority develop posttraumatic stress disorder (PTSD; American Psychiatric Association [APA], 2000). Without treatment, the disorder is typically chronic and associated with impairment across multiple functional domains (e.g., Hidalgo & Davidson, 2000; Jaycox & Foa, 1999; Stein, McQuaid, Pedrelli, Lenox, & McCahill, 2000). Treatments such as exposure-based therapy can be highly effective at reducing PTSD symptoms (e.g., Powers, Halpern, Ferenschak, Gillihan, & Foa, 2010), but they do not meet the needs of every PTSD patient. Estimates suggest that between a third and a half of patients receiving empirically supported treatments for PTSD do not fully respond to treatment, at least on some measures (Bradley, Greene, Russ, Dutra, & Westen, 2005; Schottenbauer, Glass, Arnkoff, Tendick, & Gray, 2008). The average drop-out rate in trials of exposure-based and cognitive interventions for PTSD is in the range of 20% to 25% (Hembree et al., 2003). In addition, many therapists in clinical settings report that they feel uncomfortable using these treatments or infrequently use them (e.g., Becker, Zayfert, & Anderson, 2004). Thus, there is a need for additional therapeutic options.
Meditation has generated considerable interest as a way of reducing PTSD symptoms and associated functional impairments as many individuals have a preference for using such techniques to manage their symptoms. Mental health problems are among the most frequently cited reasons for seeking help from a complementary and alternative medicine provider (Strauss, Coeytaux, McDuffie, Nagi, & Williams, 2011). In addition, there are major efforts within the United States to make meditation available to individuals with PTSD or to those at risk for the disorder. For example, filmmaker David Lynch has launched “Operation Warrior Wellness” to provide transcendental meditation (TM) to veterans, with the aim of treating PTSD in 10,000 at-risk veterans (David Lynch Foundation for Consciousness-based Education and World Peace, 2011). Similarly, “Warrior Mind Training” is a course offered in several branches of the military that combines “ancient Samurai techniques” with “modern mind training techniques . . . to exceed the demands of their missions; to enable them to actively assist in self-regulating the effects of combat operational stress and PTSD during deployment; and to aid in decompression and reintegration upon returning home” (Warrior Mind Training, Inc., 2012). That these efforts currently are not supported by empirical evidence is a call to the research community to study the effectiveness of meditation for PTSD.
In the most general terms, meditation involves developing a different relationship with or greater awareness of the mind, but within meditation there are a variety of techniques with distinct aims (Ospina et al., 2007). Many of the techniques have been adapted from religious traditions but recently have been increasingly practiced in secular settings. Fundamental to all meditation techniques is cultivating mental focus. The way in which the focus is directed, however, differentiates the approaches. In mindfulness meditation, the object of focus is the arising, maintenance, and decay of various mental experiences. By observing such change, it is suggested that the meditation may bring insight into the nature of the mind and relief of suffering through that insight. We will discuss three possible mechanisms by which mindfulness may affect the practitioner; it cultivates the ability to intentionally shift attention, modifies maladaptive cognitive styles, and encourages a nonjudgmental stance. In mantra meditations (e.g., TM, Mantram Repetition Program, relaxation response), mental focus is sustained on an object with the intent of bringing about a sense of peace and relaxation. As we will describe, this type of practice is primarily associated with reduction of physiological arousal. Finally, in compassion meditation, the focus is on the wish to remove suffering or bring happiness to others. The techniques of compassion meditation have been adapted from the Southern Buddhist Tradition (referred to by their Pali name, metta) or from a Tibetan Buddhist tradition (referred to as lo jong). We will present evidence that compassion meditation elicits positive emotion and social connectedness, thus increasing resilience. The purpose of this article is to review the theoretical and empirical basis of each of these types of meditation as ways of mitigating trauma-related distress. Although meditation, particularly mindfulness, is a component of the third wave psychotherapies (e.g., dialectical behavioral therapy, acceptance and commitment therapy), a review of those approaches is beyond the scope of this review because they incorporate a number of components beyond meditation. To the extent meditation techniques are applied, the mechanisms discussed herein are likely among the active components of those approaches.
Mindfulness Meditation
The most common definition of mindfulness is attributable to Kabat-Zinn (1994): “paying attention in a particular way: on purpose, in the present moment, and non-judgmentally.” Mindfulness has also been described as a process of “reperceiving” (Shapiro, Carlson, Astin, & Freedman, 2006) or “decentering” (Safran & Segal, 1990) in that it creates an important shift toward an objective observer’s perspective of the mind and personal experience. We suggest that this shift in perspective may have important implications for mental health in general and for PTSD in particular.
Mechanism
The three parts of the Kabat-Zinn definition provide a framework for understanding the mechanisms by which mindfulness may be impactful.
Attention
The first part of Kabat-Zinn’s definition states that mindfulness occurs on purpose. That is, there is an intentional shifting of attention. More specifically, mindfulness is thought to influence two types of attention: “concentrative attention,” or voluntary orienting to a stimulus, and “receptive attention,” or alerting to sudden changes in stimuli or salient targets (Jha, Krompinger, & Baime, 2007). At this point, there is no good neuropsychological evidence for changes in cognitive processes related to mindfulness training, but high quality studies are lacking (Chiesa, Calati, & Serretti, 2011). Imaging studies, however, demonstrate enhanced performance on tasks that require sustained attention (Kozasa et al., 2011; MacLean et al., 2010) as well as orienting and allocation of attentional resources (van den Hurk, Janssen, Giommi, Barendregt, & Gielen, 2010; van den Hurk, Giommi, Gielen, Speckens, & Barendregt, 2010), and these improvements in attention extend across contexts (Hodgins & Adair, 2010). Such findings are typically observed in experienced meditators, that is, those with a long practice history or who have taken part in long training and/or retreats. It is yet to be established to what extent changes occur with shorter practice (Treanor, 2011), but there do appear to be different patterns of brain activation in novices as compared with more practiced meditators (Farb et al., 2007).
By practicing directing and sustaining attention purposefully (through concentrative attention), mindful individuals and those who have been trained in mindfulness may develop a greater capacity to control their allocation of attention. Rather than reacting automatically to stimuli, mindfulness may facilitate directing attention more productively, for example, to coping activities or problem solving (Baer, 2003; Frewen, Evans, Maraj, Dozois, & Partridge, 2008; Shapiro et al., 2006). Consistent with this, mindfulness was associated with less negative reaction to ruminative thoughts among undergraduates who received 15 min of training in these techniques, even though such thoughts were detected more frequently by those who received mindfulness training than those who trained in relaxation or loving kindness meditation (Feldman, Greeson, & Senville, 2010).
Cognitive style
The second part of the Kabat-Zinn (1994) definition limits mindfulness to attention in the present moment. This is in contrast to attention paid to the past or future, which can become pathological rumination or worry. Mindfulness meditation may reduce these maladaptive cognitive styles. Feldman, Hayes, Kumar, Greeson, and Laurenceau (2007) demonstrated that worry frequency was significantly negatively correlated with measures of trait mindfulness. Mindfulness-based stress reduction (MBSR; a specific approach that cultivates the state of mindfulness through mindfulness meditation and other techniques and includes 30 hr of instruction via weekly meetings and a day-long retreat; http://www.umassmed.edu/cfm/stress/index.aspx, accessed September 2, 2011) has been shown to reduce rumination in an uncontrolled trial (Deyo, Wilso, Ong, & Koopman, 2009) and as compared with relaxation in a controlled trial (Jain et al., 2007).
Nonjudgment
Finally, Kabat-Zinn highlights adopting a nonjudgmental stance as a critical component of mindfulness. During meditation, thoughts and sensations are simply noticed and then attention is turned back to the focus of the meditation (e.g., the breath).
Applicability to PTSD
Each of the mechanisms by which mindfulness may create change can be applied to PTSD. Attention is linked to PTSD in two ways. First, individuals with PTSD demonstrate attentional bias toward trauma-related stimuli (Buckley, Blanchard, & Neill, 2000), meaning that an individual with PTSD is more likely to detect such stimuli. Second, cognitive theories of PTSD suggest that deficits in cognitive control, that is, the ability to inhibiting irrelevant or unwanted information while attending to other information (Miyake, Friedman, Emerson, Witzki, & Howerter, 2000). Such deficits may partially explain reexperiencing symptoms (e.g., Anderson & Levy, 2009; Aupperle, Melrose, Stein, & Paulus, 2011; Joormann, Yoon, & Siemer, 2010; Verwoerd, de Jong, & Wessel, 2008). Researchers have demonstrated that attention training programs successfully reduce anxiety symptoms and alter cognitive processing in disorders such as social phobia and generalized anxiety disorder (Amir, Beard, Burns, & Bomyea, 2009; Beard & Amir, 2008; Schmidt, Richey, Buckner, & Timpano, 2009). Decreases in anxiety are purported to operate via changes in attentional allocation away from threat (Heeren, Lievens, & Philipott, 2011), although the possibility of a more general change in ability to flexibly utilize attention control has also been proposed (Klumpp & Amir, 2010). Although further research is needed, these findings suggest that interventions designed to moderate attention, including mindfulness, hold promise for PTSD.
The cognitive styles of worry and rumination have been shown to contribute to negative effect (McLaughlin, Borkovec, & Sibrava, 2007) and to the development and maintenance of anxiety disorders in general (e.g., Clark, 1986), and PTSD in particular (Ehlers & Clark, 2000; Wells & Sembi, 2004). Both worry and rumination are associated with increased PTSD symptomatology (Ehring, Szeimies, & Schaffrick, 2009). Furthermore, it appears that changing these cognitive styles reduces psychological distress. In an analogue study, students who were exposed to a set of slides that generate negative affective reactions reported less negative emotion if they had been trained in focused breathing (a brief mindfulness based exercise) as compared with being asked to engage in worry (Arch & Craske, 2006). Change in rumination partially mediated changes in distress in a study of MBSR (Jain et al., 2007). Bernstein, Tanay, and Vujanovic (2011) found that greater attention/awareness to the present was associated with lower PTSD symptom severity and comorbidity, anxious arousal, and anhedonic depression symptoms in a sample of trauma-exposed adults.
Finally, learning to observe without judgment may counteract the tendency among PTSD patients to negatively interpret internal and external experiences. For example, anxiety sensitivity, which is fear of anxiety and anxiety-related sensations, is a risk factor for the development of panic disorder (Schmidt, 1999) and has been shown to be elevated in individuals with PTSD (Lang, Kennedy, & Stein, 2002). There is a significant negative correlation between anxiety sensitivity and mindfulness, and high anxiety sensitivity is associated with heightened anxious arousal in the context of low mindfulness (Vujanovic, Zvolensky, Bernstein, Feldner, & McLeish, 2007) but less negative effect when paired with high mindfulness (Arch & Craske, 2010). Additional evidence that negative attributions are reduced by mindfulness comes from a study in which college students were trained in meditation or placed in a control condition. The meditative practice was associated with reduced anxiety and negative affect and increased hope, and these changes were mediated by changes in cognitive distortions (Sears & Kraus, 2009). Similarly, mindfulness was associated with less anxious responding to anxiety stressors (i.e., hyperventilation and relaxation) in the laboratory setting (Arch & Craske, 2010).
In addition to being less distressed by observed experience, those who adopt a nonjudgmental stance may be more willing to approach fear-provoking or otherwise emotionally laden stimuli, which counteract avoidance. Evidence for this comes from the previously described Arch and Craske (2006) study in which students viewed negative slides; those who engaged in focused breathing demonstrated more willingness to view the negative images. As a result, mindfulness could be helpful when engaging in therapies, such as exposure therapy and cognitive processing therapy, which require reflection on the traumatic event and related thoughts and feelings (Vujanovic, Niles, Pietrefesa, Schmertz, & Potter, 2011).
Three separate studies have shown that this third mechanism, observing without judgment, may be particularly important in relation to PTSD symptoms, particularly avoidance. After controlling for negative effect and number of traumatic exposures in a nonclinical population, the Accepting Without Judgment Scale of the Kentucky Inventory of Mindfulness Skills was negatively associated with PTSD symptoms, whereas the Observing, Describing and Acting with Awareness Scales were not (Vujanovic, Youngwirth, Johnson, & Zvolensky, 2009). Similarly, after controlling for emotional avoidance, the Nonjudgment Scale of the Five Facets of Mindfulness Questionnaire (but not Observe, Describe, Act with Awareness or Nonreactivity Scales) was negatively associated with PTSD avoidance symptoms (Thompson & Waltz, 2010). Data from a small clinical trial showed that improvements in observing and describing internal experiences were related to improvement in PTSD symptoms (Niles, Klunk-Gillis, Silberbogen, & Paysnick, 2009).
Empirical Support
There have been several reviews or meta-analyses of mindfulness, all concluding that mindfulness has a medium effect size for addressing mental health concerns. Hofmann, Sawyer, Witt, and Oh’s (2010) recent meta-analysis found a pre-post effect size of .63 for reducing anxiety and .59 for reducing depression; within samples with elevated anxiety or depression, the effect sizes were .67 for anxiety and .53 for depression. Similarly, in Grossman, Niemann, Schmidt, and Walach’s (2004) meta-analysis, the effect size for mindfulness as compared with control conditions was d = .54 for mental health variables. Approximately the same effect size was estimated based on change from pre- to post- in uncontrolled studies. The Baer (2003) review found an overall mean effect size of .59 at posttreatment and follow-up. Importantly, it should be noted that these reviews include studies using mindfulness-based cognitive therapy, so it is not clear what effect can be attributed to mindfulness alone.
To our knowledge, five studies have evaluated the effect of mindfulness on anxiety disorders. Two small, uncontrolled studies found significant reductions in anxiety associated with mindfulness practice (Bögels, Sijbers, & Voncken, 2006; Kabat-Zinn et al., 1992). Meditation-based stress management was shown to outperform psychoeducation for patients with generalized anxiety disorder or panic who were incomplete responders to pharmacotherapy (Lee et al., 2007). MBSR did not, however, do as well as group cognitive-behavioral therapy for social anxiety, but it was associated with a large pre-post within-group effect size (Koszycki, Benger, Shlik, & Bradwejn, 2007). In the largest randomized trial to date, Vøllestad, Sivertsen, and Nielsen (2011) found that MBSR, as compared with waitlist, led to significant reductions in anxiety, worry, insomnia, and general distress in a heterogeneous group of anxiety disorders patients (PTSD was not included); the effects were mediated by mindfulness.
Three studies have evaluated mindfulness for patients with trauma histories or PTSD. Kimbrough, Magyari, Langenberg, Chesney, and Berman (2010) executed an uncontrolled study of MBSR in a heterogeneous group of distressed survivors of childhood sexual abuse (n = 27), 15 of whom had presumptive PTSD. The investigators showed statistically significant reductions in PTSD symptoms (effect size (ES) at the end of the 8-week intervention was 1.2 and was 0.8 at 24 weeks). They observed the largest observed change in avoidance/numbing symptoms, consistent with the prediction that the nonjudgmental stance of mindfulness reduces the need for avoidance. There were also statistically significant changes in anxiety and depression. Niles et al. (2009) have presented data on mindfulness as compared with psychoeducation. Both interventions were delivered in eight sessions, with six of the sessions occurring via telephone. They found no group differences in completion; 82% overall completed and on average reported good satisfaction. Mindfulness was associated with greater reduction in clinician-rated and self-report PTSD symptoms, with a significant dose-response effect suggesting more improvement with more practice. Finally, Kearney et al. (2012) conducted an uncontrolled study of MBSR as an adjunct to usual care in 92 veterans with PTSD. On average, veterans attended approximately six of the nine classes. They observed a medium effect size change in PTSD symptoms, depression and functioning. Although it is hard to know what to attribute these changes with no control and with other interventions occurring concurrently, the changes were mediated by changes in mindfulness.
In summary, mindfulness has been studied as an intervention for several anxiety disorders, but only three studies have evaluated mindfulness-based interventions in PTSD. The existing trials suggest that mindfulness is associated with a medium-large effect size in anxiety disordered patients, but the studies are limited by small size and lack of control groups. A study of social phobics showed that mindfulness was not as good as group CBT, which is the best supported treatment for social anxiety (Koszycki et al., 2007). It is reasonable to believe that the same would be found if mindfulness were compared with evidence-based PTSD therapies, such as prolonged exposure or cognitive processing therapy. Even if mindfulness does not merit being a first-line intervention, it appears to make a meaningful impact on symptoms and may be a good alternative for patients who prefer meditation to other approaches. There are generally high rates of treatment completion (76%-85%) for mindfulness interventions (Baer, 2003; Kabat-Zinn & Chapman-Waldrop, 1988), although this estimate includes clinical and nonclinical samples and may overestimate compliance in mental health patients. Mindfulness may have a particularly important role in reducing avoidance and, thus, should also be evaluated as an adjunct to other PTSD treatments. Finally, the question of whether mindfulness has an impact that is unique from relaxation should be evaluated. Mindfulness practice is often reported to lead to a sense of relaxation (Baer, 2003), although relaxation is not a goal of the practice. Although it is hypothesized here that mindfulness leads to change by several other mechanisms, Jain et al. (2007) failed to find a difference in a student sample between mindfulness meditation and relaxation, with both conditions reducing distress and increasing positive affect.
Mantra Meditation
Mantra meditation involves focusing on an object to bring about a sense of peace and relaxation. For example, TM is a type of mantra meditative practice that “allows your mind to settle inward beyond thought to experience the source of thought, the most silent and peaceful level of consciousness” (The Transcendental Meditation Program, 2011). TM involves directing one’s attention to a mantra (a word or phrase), which is silently repeated until the repetition no longer needs to be consciously directed and the mind is free of thought (Ospina et al., 2007). There are other variations of mantra-based approaches, such as the relaxation response, in which the practitioner is instructed to progressively relax his or her muscles and then silently say “one” with each exhalation so the mantra is linked to the breath (Ospina et al., 2007), and the Acem meditation, in which the mantra is a nonword sound (Nesvold et al., 2011).
Another related practice is called the Mantram Repetition Program, which teaches repetition of a sacred word or phrase (i.e., a Mantram) that is repeated intermittently, at any time or place. The term Mantram, rather than mantra, is used to differentiate this program from TM and to acknowledge its originator, Easwaran (2008). Repeating a Mantram is intended to heighten awareness of the thought process rather than transcend it as is intended in TM. Slowing down and practicing one-pointed attention are associated skills taught to support Mantram Repetition. With repeated practice, the silent, refocusing of attention on a chosen spiritual phrase of comfort or inspiration may come to be an alternative reaction to the stress response.
Mechanism
The TM approach is thought to bring on a state of no thought in which physiological arousal is reduced while maintaining a high state of alertness (often referred to as “restful alertness”); this state is thus thought to be distinct from relaxation and sleep (Ospina et al., 2007). A number of different types of evidence are consistent with the idea that mantra meditation reduces physiological arousal, but whether this reduction is greater than that produced by relaxation or rest has not been definitively shown. Nesvold et al. (2011) found that Acem meditation was associated with increased parasympathetic and decreased sympathetic activity. In a recent meta-analysis, however, Ospina and colleagues (2007) reported that the relaxation response was no better than biofeedback in terms of reducing muscle tension and led to less reduction in heart rate than did rest. Engaging in TM does not appear to reduce blood pressure in the short term (Nidich et al., 2009; Ospina et al., 2007) but has been associated with changes in catecholamines and cortisol that suggest more adaptive long-term responding to stress (Infante et al., 2001; MacLean et al., 1997). An older meta-analysis of physiological differences between TM and rest concluded that TM had a larger effect size in basal skin resistance and respiration rate but not for heart rate and spontaneous skin resistance (Dillbeck & Orme-Johnson, 1987). Evidence for the heightened state of alertness that accompanies the reduction in physiological arousal comes largely from EEG studies (Dillbeck & Orme-Johnson, 1987).
Unlike TM, the Mantram Repetition Program is thought to heighten awareness of one’s thoughts (not transcend them) and may facilitate emotional self-regulation. It is taught as an intentional distraction that can be used to interrupt disturbing thoughts and behaviors to allow some “pause time” in which to make better choices, a process that has been described as “mindful distraction” (Vujanovic, Niles, Pietrefesa, Schmertz, & Potter, 2011). It is also possible that Mantram Repetition elicits a feeling of well-being or self-confidence, in part, perhaps, because of the personal spiritual meaning of the chosen word or phrase.
Applicability to PTSD
PTSD, like all anxiety disorders, is characterized by inappropriate triggering of the fight-flight response, the body’s automatic response to danger or fear-provoking stimuli that is controlled by the autonomic nervous system. Mantra meditation, by reducing autonomic responding (i.e., fight-flight response) in particular and emotional responding more generally, should counteract this aspect of PTSD. It would further be predicted that TM and related approaches are likely to lead to baseline reduction in arousal, whereas Mantram Repetition aims to reduce arousal in the moment.
Empirical Support
Few studies have evaluated mantra meditation for PTSD. An early meta-analysis of the effects of various types of relaxation on trait anxiety suggested that TM had a larger effect size (.70) than relaxation techniques (.39) and other types of meditation (.28) (Eppley, Abrams, & Shear, 1989). College students who were trained in TM showed reduced overall psychological distress, anxiety, and depression and increased coping ability (Nidich et al., 2009). Brooks and Scarano (1985) compared TM (n = 9) to eclectic individual psychotherapy (n = 9) in Vietnam veterans. They observed clinically significant reductions in PTSD symptoms and anxiety, but significant methodological issues with the study limit the conclusions that should be drawn (Strauss et al., 2011). Rosenthal, Grosswald, Ross, and Rosenthal (2011) conducted a very small (n = 5) uncontrolled trial of TM in veterans of the wars in Iraq and Afghanistan. The participants showed clinically meaningful improvement on clinician-rated and self-report measures of PTSD and in quality of life.
Finally, Bormann, Thorp, Wetherell, Golshan, and Lang (2011) conducted an initial randomized trial of Mantram Repetition plus usual care (medication and case management) as compared with usual care alone for PTSD in combat veterans. Those who participated in the Mantram Repetition Program (n = 71) as compared with controls (n = 75) demonstrated significantly greater reductions self-report (ηp2 = .03 1 ) and clinician rated (ηp2 = .03) PTSD symptoms, depression (ηp2 = .05), and improvement in mental health related quality of life (ηp2 = .03) after six group sessions. Change in PTSD symptoms was mediated by levels of spiritual well-being (Bormann, Liu, Thorp, & Lang, 2011), supporting the hypothesis that the spiritual aspect of the practice is important. There were very few dropouts, only 5 (7%). In spite of the promising findings, the lack of an active comparison group limits the interpretability of the results; it is not clear whether the findings can be attributed to Mantram Repetition Program specifically or may be due to nonspecific factors related to participating in a group in addition to usual care.
In summary, evidence for mantra meditation is also quite limited. The studies of TM are small and methodologically limited. Mantram Repetition has been associated with a small to medium effect size in a larger study, but additional work is needed to establish the efficacy of the approach.
Loving Kindness and Compassion Meditation
Practitioners of this type of meditation are guided to appreciate others and to wish them happiness (loving kindness meditation) and freedom from suffering (compassion meditation), potentially leading to a heightened sense of warmth toward and closeness to others (Negi, 2009).
Mechanism
Positive emotion
Several studies show that compassion meditation enhances positive affect. Hutcherson, Seppala, and Gross (2008) compared a 7-min loving kindness meditation exercise with an imagery exercise and found that even this very brief intervention, as compared with imagery, led to increased positive mood and decreased negative mood. Using a longer intervention, Fredrickson, Cohn, Coffey, Pek, and Finkel (2008) showed that six 60-min sessions of loving kindness meditation training over 7 weeks administered to workers (n = 102), as compared with waitlist control (n = 100), resulted in increasing positive emotion during the study. A pilot study (n = 18) of loving kindness meditation for negative symptoms of schizophrenia, which we believe is the first published application of this technique in a clinical sample, showed that the practice increased positive emotion and decreased negative emotion (Garland et al. 2010). Consistent with these findings, evidence from functional MRI shows activation in areas typically associated with positive affect (left medial prefrontal cortex and anterior cingulate gyrus) in an expert meditator engaged in compassion meditation (Engström & Söderfeldt, 2010).
Social connectedness
The brief meditation exercise used by Hutcherson and colleagues (2008) was associated with more positive explicit and implicit reactions about others. This increase in social connectedness may be direct, or the effect may be indirect. Positive emotions are associated with interpersonal closeness and enjoyment and lead to increased sociability and prosocial behavior; this effect may be self-perpetuating because social interaction leads to further positive emotions (Waugh & Fredrickson, 2006). Sharing of positive events, rather than providing support during negative events, is predictive of relationship health (Gable, Gonzaga, & Strachman, 2006). Positive emotions also lead to more flexible thinking, which, in turn, enhances one’s ability to take the other’s perspective and to feel close to and appreciate the other (Waugh & Fredrickson, 2006).
Broaden and Build Theory
The mechanism by which compassion meditation may effect change can be summarized using Fredrickson’s (1998, 2001) Broaden and Build Theory. The theory suggests that compassion meditation increases positive emotion and social connectedness, both of which increase personal resources, such as a sense of mastery, resilience, and social support. These increased resources, in turn, have been associated with improved life satisfaction. Positive emotion also appears to directly affect symptomatology (for description and tests of the model, refer to Fredrickson, 2001, 2008; Tugade & Fredrickson, 2004).
Applicability to PTSD
Positive emotions are commonly viewed as a brief respite or distraction from stress or negative emotion. In contrast to this view, however, it is argued that positive emotions actually counteract the cognitive and physiological effects of negative emotion. This may be in part due to neurobiologically based homeostatic processes that coordinate the autonomic system (Craig, 2009). Specifically, a model where the anterior insular cortex regulates sympathetic and parasympathetic nervous system input and activity can account for the apparent balance between types of affect. These systems are associated with unique affective and behavioral tendencies (parasympathetic—approach, affiliation-related affect; sympathetic–withdrawal, survival emotions such as fear). By this model, “coordinated opponency” (i.e., reciprocal regulation) between these two systems can account for findings that emotional and behavioral correlates of the parasympathetic system, including positive emotion, down-regulate negative emotion.
Induction of positive emotion may affect PTSD in three ways. First, PTSD in particular is characterized by strong negative affect—fear/anxiety, depression and anger/irritability—accompanied by a dampening of positive affect (Litz & Gray, 2002). If compassion meditation increased positive affect and decreased negative affect, it could have a profound impact on outcomes, as dysphoria appears to be the best predictor of problems in psychosocial functioning (Pietrzak, Goldstein, Malley, Rivers, & Southwick, 2010). Second, PTSD is associated with autonomic hyperarousal (APA, 2000; Barlow, 2002). Positive emotions, as opposed to neutral distractors or other negative emotions, reduce anxiety-related cardiovascular reactivity (Fredrickson, Mancuso, Branigan, & Tugade, 2000). Finally, positive emotions have been linked to resilience, that is, the ability to recover from negative experiences and to change based on situational demands (Tugade & Fredrickson, 2004). Positive emotions have been explicitly tied to the process of coping with highly stressful events. For example, Fredrickson, Tugade, Waugh, and Larkin (2003) found that positive emotions were a critical component in resilience among college students after the September 11 terrorist attacks. Similarly, bereaved caregivers who experienced positive emotion during their grief found more positive meaning in their loss and demonstrated more long-term goal setting and planning, which corresponded to greater well-being 12 months later (Moskowitz, 2001). It appears, however, that resilience is not only a trait characteristic but can be enhanced by induction of positive emotion (Tugade & Fredrickson, 2004). For these reasons, finding ways of generating and sustaining positive emotion is described as an important clinical need (Folkman, 2008).
Social connectedness plays an important role in mental health in general and PTSD in particular (see, for example Cacioppo, Hughes, Waite, Hawkley, & Thisted, 2006; Cacioppo & Patrick, 2008). Individuals with PTSD frequently report feelings of detachment or estrangement from others (APA, 2000). PTSD is associated with poorer marital and family functioning and more impairment in interpersonal relationships and social activities (Schnurr, Lunney, Bovin, & Marx, 2009). PTSD patients have been shown to have a diminished ability to empathically connect with others (Nietlisbach, Maercker, Rössler, & Haker, 2010), and deficits in empathy appear to be positively correlated with verbal aggression in veterans with PTSD (Teten, Miller, Bailey, Dunn, & Kent, 2008). Social impairment is a predictor of chronicity of the disorder (Marshall et al., 2006) and predicts return for additional care after initial treatment (Fontana & Rosenheck, 2010). Social isolation may be the strongest and the most reliable predictor of suicidal thoughts and behavior (Van Orden et al., 2010) and has been linked to increased risk of suicide in PTSD patients (Panagioti, Gooding, Dunn, & Tarrier, 2011). A sense of connection, or belongingness, on the other hand, is associated with better psychological and social functioning (Hagerty, Williams, Coyne, & Early, 1996), including reduced anxiety and greater self-esteem (Lee & Robbins, 1998). Finally, among veterans with PTSD, higher levels of altruism have been associated with lower levels of symptomatology (Kishon-Barash & Johnson, 1999).
Empirical Support
Compassion meditation has not been specifically evaluated for any anxiety disorder. Pace et al. (2009) recruited 61 college students into a study comparing compassion meditation and health education discussion. Participants were assessed using a standardized stress test (public speaking followed by mental arithmetic) and physiological measures. The more students had practiced meditation at home, the less distress they reported after the stress test. Johnson et al. (2011) conducted a pilot study of loving kindness meditation with individuals diagnosed with schizophrenia-spectrum disorders (n = 18). Of them, 88% completed the treatment, and the practice was perceived to be easy, enjoyable, and useful. Participants actively engaged in the meditation, practicing an average of 3.7 days per week with an average of 19.1 min of practice per day. In this study, loving kindness meditation was associated with a large effect size increase in positive emotion and life satisfaction, a large effect size reduction in negative symptoms and anhedonia, and a medium effect size reduction in asociality. These gains generally were maintained over a 3-month follow-up period (Johnson et al., 2011). Finally, Carson et al. (2005) applied loving kindness meditation for low back pain. They found that, as compared with standard care, loving kindness meditation led to reduced general psychological distress, anxiety and hostility after the intervention and 3 months later.
Discussion
Three different types of meditative interventions have been considered as ways to reduce symptomatology and improve quality of life for individuals with PTSD. As outlined in Table 1, the primary hypothesized mechanisms behind these interventions differ, but all are connected to the psychopathological processes that contribute to PTSD. Given the different ways in which these approaches may impact symptomatology, it is important that future researchers clearly describe the nature of the meditative intervention that they use and include measures to test whether the proposed mechanisms are mediating change.
Mechanisms for Meditation-Based Change in PTSD Symptoms
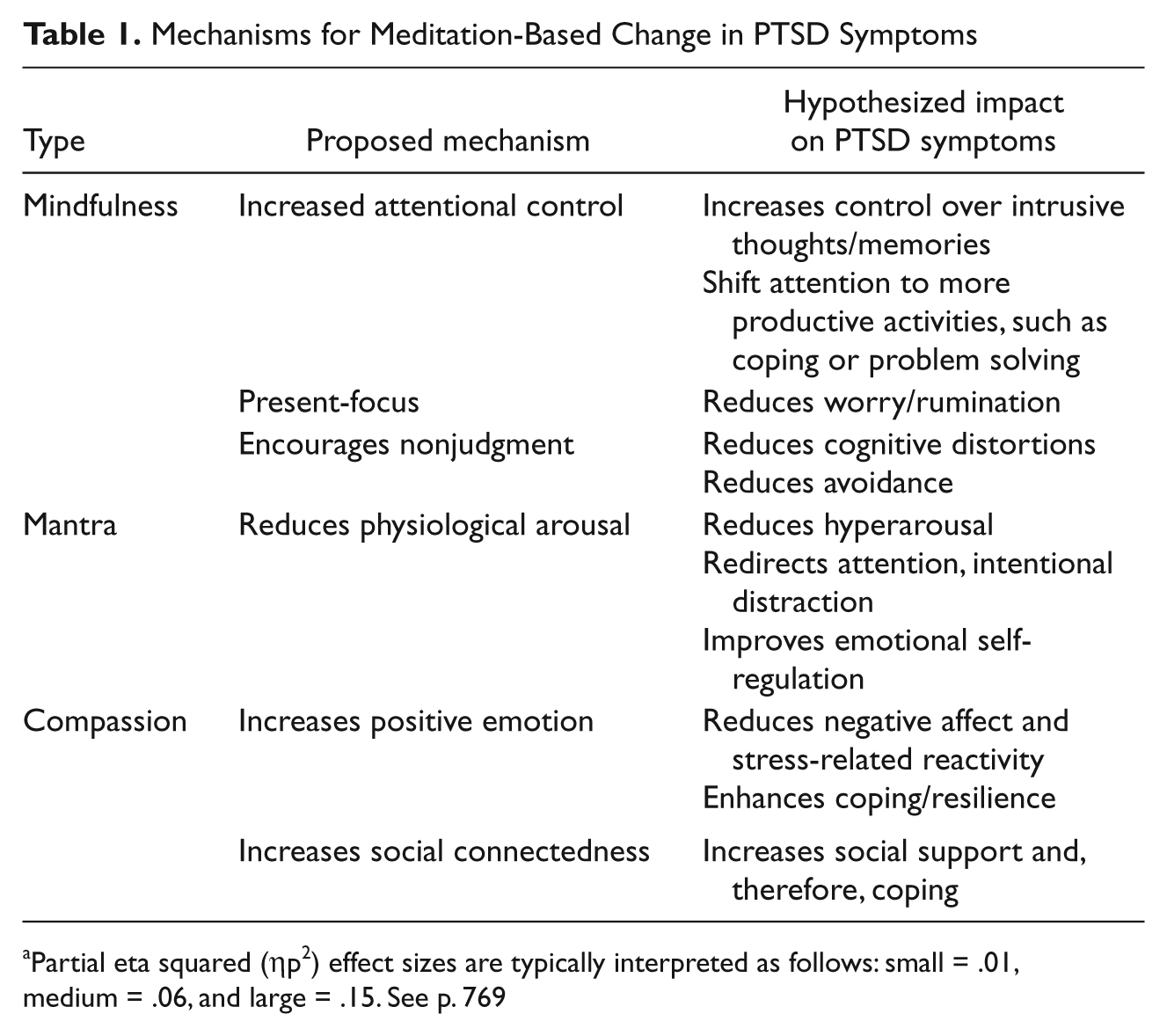
Partial eta squared (ηp2) effect sizes are typically interpreted as follows: small = .01, medium = .06, and large = .15. See p. 769
Mindfulness meditation has the best empirical support for treatment of PTSD, but the evidence is largely based on generalization from other anxiety disorders. Thus, an initial randomized clinical trial of mindfulness meditation is warranted. Mindfulness should also be evaluated as an adjunct to cognitive-behavioral therapies for PTSD. For example, by increasing willingness to approach feared stimuli, mindfulness may enhance the efficacy of exposure-based therapies. It also may increase awareness and malleability of automatic thoughts. Existing psychotherapies, such as mindfulness-based cognitive therapy, acceptance and commitment therapy, and dialectical behavior therapy, have utilized mindfulness in combination with other therapeutic strategies, but this strategy has not been applied specifically to PTSD treatment. The few studies of mantra meditations show promise, but there are significant methodological limitations to the studies to date. At this point, therefore, additional pilot work to estimate the feasibility and effect size of the mantra meditation interventions and to differentiate the effect of such practices from other approaches that target physiological arousal, such as rest and relaxation, is warranted. Compassion meditation has not been evaluated for any anxiety disorder but also merits additional evaluation. Empirically supported PTSD treatments (i.e., exposure-based therapy and cognitive therapy) focus primarily on the reduction of negative emotions. Hence, compassion meditation, which induces positive emotion, would complement these approaches. In addition, there has been recent recognition of the importance of building social support in those with PTSD. For example, a trial is underway evaluating the impact of involving the spouse in cognitive-behavioral therapy for PTSD (Billette, Guay, & Marchand, 2008). Compassion may be an alternative approach for targeting social support.
It is our hope that this work will inspire additional scientific interest in the study of meditation as a clinical tool. In addition to general questions about potential treatment efficacy within this population, questions about the mechanism of these meditation interventions (compared with one another and compared with other treatment types) remain. For example, all aspects of meditation-based approaches maintain a central focus on processes requiring sustained, concentrated attention (i.e., attention toward the present moment in mindfulness, attention to a word or phrase in the Mantram Repetition Program, attention toward wishing others well in compassion meditation). The distinct benefit or differences between the types of stimuli that are of focus is unknown, despite of the fact that these approaches vary in how much they emphasize the importance of the attentional component of meditation. A comparison of meditation approaches relative to processes implicated in cognitive-behavioral treatments (e.g., change in distorted cognitions or cognitive decentering, behavioral avoidance) would also further our understanding of mechanisms of action. It may be that these interventions represent distinct means to similar, functional ends (e.g., top-down control of affective responding). Alternatively, disparate mechanisms altogether may be at work.
Moreover, an understanding of the type and trajectory of behavioral change that occurs as a result of these interventions is not well understood. The effect of increased mindful control, social affiliative emotion, or decreased tension on PTSD presumably operates in part by changes in the individual’s behavioral repertoire. For example, in compassion meditation, one hypothesized mechanism is an increase in resources derived from improved positive affect. These changes (e.g., increased social support) are likely influenced by changes such as increased social approach behavior and displays of positive affect. Although studies have noted that loving kindness meditation increases perceived social support toward others (e.g., Fredrickson et al., 2008), how this may translate into increased social resources for individuals with psychopathology who may have damaged or lost their social relationships is currently unclear. As noted previously, increased ability to be mindful of the present moment or decreased judgment of internal experiences in mindfulness meditation may operate by increasing willingness to engage in activities that may activate negative emotions or cognitions. This decrease in behavioral avoidance may lead to symptom change over time. Thus, one future direction for this work would be to explore how changes in purported mechanisms change behavioral aspects related to psychopathology or functioning over time.
Integration of meditation-based approaches has a number of potential benefits. Delivering meditation is low cost as most practices are taught in a group format or can be taught relatively quickly. The approach has no significant side effects and has been shown to be well tolerated by individuals with PTSD (Bowen et al., 2006). There is no reason to believe that meditation would interfere with psychotherapy or pharmacotherapy but rather may facilitate other approaches. Although data are limited on effectiveness of interventions on, some clusters may be relatively less changed than others as a result of treatment (e.g., reexperiencing, numbing; Bryant et al., 2008; Lovell, Marks, Noshirvani, Thrasher, & Livanou, 2001). If meditation interventions specifically target these symptom clusters, they may be a beneficial adjunct for individuals struggling with residual symptoms. Meditation may not appeal to every individual with PTSD, but for those who are interested in complementary and alternative approaches, it would be a welcome addition to our repertoire of empirically supported treatment approaches.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr. Lang received salary support for the completion of this manuscript through the VASDHS Center of Excellence for Stress and Mental Health. Ms. Bomyea is supported by a grant from the National Institutes of Health (1F31MH088170-01). Ms. Good is supported by a MARC U-STAR Award (Award Number T34GM087193) from the National Institutes of Health, National Institute of General Medical Sciences. The content is solely the responsibility of the author(s) and does not necessarily represent the official views of the National Institute of General Medical Sciences or the National Institutes of Health.