
Abstract
The aim of this research was to examine the efficacy of two cognitive-behavioral treatment modalities for panic disorder (PD) with nocturnal panic (NP). The first study was conducted to determine whether conventional CBT for PD was effective for PD with NP in three participants. A second study sought to explore whether a CBT adapted to NP would lead to different clinical outcomes in three other participants. A multiple-baseline single-case design across individuals was used in both studies. Treatment outcome was assessed with standardized clinician ratings, self-report questionnaires, and daily self-monitoring. Results revealed that both the conventional and the adapted treatments showed a faster decrease in NPs versus daytime panics and significant clinical changes in all measures for up to a year after therapy. Hence, the changes brought about by the adapted treatment seemed to be similar to those obtained using conventional treatment. In light of these results, it can be presumed that conventional strategies may be sufficient for the treatment of NP. These observations raise questions regarding the real need to adapt treatments specifically to NP.
Treatment of nocturnal panic (NP) has received little attention, yet it constitutes a relatively widespread phenomenon. Clinical studies indicate that between 44% and 71% of patients with panic disorder (PD) have experienced at least one NP (Freire et al., 2007; Sarisoy, Böke, Arik, & Sahin, 2008; Singareddy & Uhde, 2009). Moreover, 18% to 45% reported regular and frequent NP (Stein, Chartier, & Walker, 1993; Uhde, 1994) and 2% had mainly NPs (Krystal, Woods, Hill, & Charney, 1991; Uhde, 1994). Most patients with NP also experience daytime panic (DP) attacks.
NP refers to a sudden waking from sleep in a state of intense fear or discomfort accompanied by physical symptoms (e.g., heart palpitations, shortness of breath, heavy sweating, etc.) and cognitive symptoms (e.g., fear of dying, going crazy, or losing control, etc.) similar to those associated with DP. NP does not refer to a panic attack appearing after a lapse of waking time. Nor does it refer to arousal from sleep induced by nightmares or environmental stimuli, such as an unexpected noise (Craske & Rowe, 1997). NPs occur spontaneously and unpredictably. Sleep laboratory studies confirm that these attacks take place mainly during non–rapid eye movement (non-REM) sleep, in late Stage 2 or early Stage 3 (Landry, Marchand, Mainguy, Marchand, & Montplaisir, 2002) and more rarely, during Stage 4 (Dantendorfer et al., 1996).
Comparisons between NP and DP reveal some differences in terms of symptomatology (Krystal et al., 1991; Uhde, 1994). Among differences, patients suffering from NP seem to experience more autonomic nervous system dysregulation during sleep than patients suffering from DP alone, particularly in terms of cardiac variability (Aikins & Craske, 2008; Sloan et al., 1999).
They tend to react more strongly to interoceptive stimuli during sleep (Craske, Lang, Tsao, Mystkowski, & Rowe, 2001) and they are more prone to waking in a state of panic in response to physiological changes during sleep (Roy-Byrne, Mellman, & Hude, 1988). These changes are related to an already acquired fearfulness of interoceptive cues (particularly salient between Stages 2 and 3 of sleep (i.e., when NPs are most likely to occur). The interoceptively conditioned fear of sensations upon waking can in turn intensify the sensations (Craske & Rowe, 1997). Hence, patients with NP frequently become fearful of sleep and attempt to delay sleep onset. Avoidance of sleep may result in chronic sleep deprivation, which in turn can precipitate more NPs (Singareddy & Uhde, 2009; Uhde, 1994) and insomnia (Singareddy & Uhde, 2009). They are also more physiologically and subjectively sensitive to certain conditions similar to sleep, such as a state of relaxation (Aikins & Craske, 2008; Craske et al., 2001) and hypnotic imagery (Tsao & Craske, 2003).
This could support the hypothesis regarding greater fear of loss of vigilance in this population. Nevertheless, recent studies do not allow for the conclusion that NP represents a more severe form of PD (Craske et al., 2001; Craske et al., 2002; Freire et al., 2007; Levitan & Nardi, 2009). Instead, NP appears to be a more specific version of the disorder, one that is characterized by fearful associations with sleep and sleeplike states (Craske et al., 2002).
More than 20 comparative studies conducted with control groups have already shown the efficacy of cognitive-behavioral therapy (CBT) in treating PD (Gould, Otto, & Pollack, 1995). Given that NPs appear similar to DPs in terms of symptoms and explanatory factors, it is conceivable that the CBT conventionally used to treat PD could also be beneficial for NPs. However, no study to date has verified this hypothesis. On the other hand, NP appears to have several specific characteristics as exposed previously. A CBT that does not take these particularities into account may have limited efficacy (i.e., in terms of rapidity, specificity, and magnitude of change). In other words, a treatment that is adapted to NP’s characteristics may yield better results than a conventional CBT. One study has tested the efficacy of an adaptation of CBT for NP (Craske, Lang, Aikins, & Mystkowski, 2005). Results showed that the adapted treatment program was more effective than the passage of time alone and gains were maintained over a 9-month follow-up period. However, this study did not provide any answer regarding the relative efficacy of conventional strategies for NPs. It is not clear that the adapted treatment had a specific effect on NPs.
The aim of the current research was to examine the efficacy of two CBT modalities for PD with NP. The first study sought to determine whether conventional CBT alone (i.e., without interventions aimed at specifically modifying NP) is effective in treating PD with NP. The second study tried to determine whether a treatment adapted for NP produced a distinct treatment outcome. Since conventional treatment does not target the clinical characteristics specific to NP, we presumed that it would be ineffective in bringing clinically significant changes at post-test. Given that the adapted treatment targets NPs directly, we presumed that participants would attain significant clinical changes at post-test and maintain them for up to 12 months after therapy.
Study 1
Method
Participants
Three participants suffering from PD (with or without agoraphobia) and NP (with or without DP) took part in this study. They were recruited from a waiting list at the Louis-H. Lafontaine Hospital cognitive-behavioral therapy unit and through newspaper advertisements. The inclusion criteria were as follows: (a) aged between 18 and 55; (b) must have had a diagnosis of PD (scoring 4 or more on the 0-to-8-point scale of the Anxiety Disorders Interview Schedule [ADIS-IV]; DiNardo, Brown, & Barlow, 1994), with at least one NP per week or four per month, combined with at least moderate (scoring 4, on a 0-to-8-point scale) apprehension over their recurrence; (c) NPs must have been present for at least 6 months; and (d) any other diagnosis, if present, had to be lower in severity than PD. As suggested by Craske and Rowe (1997), NP was defined as waking abruptly from sleep with symptoms of arousal and fear felt immediately upon waking that were not attributable to frightening dreams, external interruptions, or other sleep disorders. Participants were excluded if they had (a) a sleep disorder, with the exception of insomnia; (b) a physical condition that might pose a risk for the patient or hinder treatment; (c) a substance abuse problem; (d) a psychotic disorder; (e) an organic mental disorder; and (f) participated in a CBT over the past year. Moreover, the participants had to agree to continue taking a consistent dose of their medication from the time of the psychiatric assessment until the 6-month follow-up; refrain from beginning the use of psychotropic drugs for the duration of the study; and not participate in any other therapy or support group until the end of the study.
Participant 1 was a woman recruited from the hospital wait list. She was 37 years of age, living in a common-law marriage, had two children, and had a CEGEP diploma (a preuniversity program in Québec). At the time of the assessment, she was unemployed, and was receiving welfare benefits. She reported having stopped working 6 years earlier when she began suffering from PD with agoraphobia (PDA). She was diagnosed with PDA (i.e., severity rating of 6/8 on the ADIS-IV; severe) and reported eight NPs and two DPs in the previous month. She also presented symptoms of generalized anxiety disorder (GAD; 3/8, mild/moderate), and of depression (2/8, mild). She was taking fluoxetine (40 mg) and lorazepam (1 mg, on average 3 times a day).
Participant 2 was a man recruited through newspaper advertisements. He was 27 years of age, living in a common-law marriage, had no children, had a vocational studies certificate and was working as a firefighter. Since adolescence, he had clinical symptoms compatible with NPs. A diagnosis of PDA was confirmed (4/8, moderate) at the initial assessment. NPs were predominant. He had experienced six NPs and no DP in the previous month. He also presented some symptoms of a specific phobia of vomiting (2/8, mild), a GAD (2/8, mild), and an obsessive–compulsive disorder (1/8, mild). He was not taking any psychotropic drugs.
Participant 3 was a woman who was recruited through newspaper advertisements. She was 37 years of age, divorced, and a mother of two children. She had a CEGEP diploma and worked as a secretary. She reported suffering from PDA symptoms for 10 years. At the initial assessment, she presented with a PDA (5/8, moderate/severe) and had experienced four NPs and four DPs during the previous month. Moreover, she had symptoms of depression (3/8, mild/moderate) and those for a specific phobia of spiders (2/8, mild). She had a prescription for bromazepam (3 mg), but had recently stopped taking it.
Instruments
ADIS-IV
The ADIS-IV (DiNardo et al., 1994) is a structured interview used to evaluate the presence or absence of anxiety disorders, mood disorders, somatoform disorders, substance use disorder, psychotic disorders, and medical problems. The severity is provided on a 9-point Likert-type scale (0-8). The ADIS-IV was used to establish the participants’ diagnosis (clinical level at 4 or more on the 0-to-8-point scale) to assess the impact of the treatment.
The Agoraphobia Mobility Inventory (AMI)
The AMI (Chambless, Caputo, Jasin, Gracely, & Williams, 1985) is a questionnaire that measures the severity of phobic avoidance. It consists of two subscales: alone and accompanied. In this study, only the first subscale (14 items) was used because it usually provides a better reflection of the agoraphobic person’s level of functioning.
The Body Sensations Questionnaire (BSQ)
The BSQ (Chambless, Caputo, Bright, & Gallagher, 1984) measures fear of 17 physical sensations associated with anxiety.
Agoraphobic Cognitions Questionnaire (ACQ)
The ACQ (Chambless et al., 1984) measures the frequency of 14 catastrophic thoughts related to panic attacks.
Anxiety Sensitivity Index (ASI)
The ASI (Reiss, Peterson, Gursky, & McNally, 1986) is a 16-item questionnaire that evaluates the beliefs related to the social and physical consequences of anxiety symptoms.
Beck Anxiety Inventory (BAI)
The BAI (Beck, Espstein, Brown, & Steer, 1988) is a 21-item questionnaire that measures the severity of cognitive, affective, and somatic symptoms related to anxiety.
Beck Depression Inventory (BDI)
The BDI (Beck, Rush, Shaw, & Emery, 1979) evaluates the presence and intensity of 21 symptoms of depression in the past 2 weeks.
Pittsburg Sleep Quality Index (PSQI)
The PSQI (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989) is a 19-item questionnaire that assesses sleep quality and disturbances over a 1-month time interval. The items are grouped into seven “components”: (a) the subjective quality of sleep, (b) sleep latency, (c) sleep duration, (d) sleep efficiency, (e) sleep disturbances, (f) use of sleeping medication, and (g) daytime dysfunction.
Sleep Impairment Rating Scale (SIRS)
The SIRS (Morin, 1993) contains seven items that provide a subjective index of sleep deterioration. The respondents estimate (a) the severity of their difficulties in falling asleep, nocturnal and premature wakings; (b) their level of satisfaction with the sleep obtained; (c) the degree of its interference in their daily functioning; (d) the appearance of the deterioration pertaining to their sleep problem; and (e) the level of concern that their sleeping problem causes.
Daily self-monitoring booklets
A daily self-monitoring booklet was used to evaluate the daily level of the different parameters associated with PDA and to track NP and DP attacks. The participants had to respond to a number of questions using a scale of 0 (not at all) to 10 (extremely), for example, “How afraid were you of your unusual bodily sensations today?” This booklet provided a baseline level and also a means of recording the changes observed during treatment and at the follow-ups.
Experimental design
A multiple-baseline design across individuals was used. This design provides control over maturational effects and life events by showing that participants improve when treatment is introduced (Barlow & Hersen, 1984; Ladouceur & Bégin, 1986).
Treatment
The treatment consisted of conventional cognitive and behavioral strategies for PDA and was derived from the book titled La peur d’avoir peur (Marchand & Letarte, 1993), similar to the protocol described by Craske and Barlow (1993). The treatment involved 15 one-hr sessions spread over a 16-week period (i.e., the last session was held 2 weeks after the 14th one) and consisted of the interventions presented in Table 1. It is important to mention that only DP attacks were targeted by the conventional treatment. The therapist was instructed to guide the subject to manage NP in the same ways as DP.
Therapeutic Strategies Presented by Session.
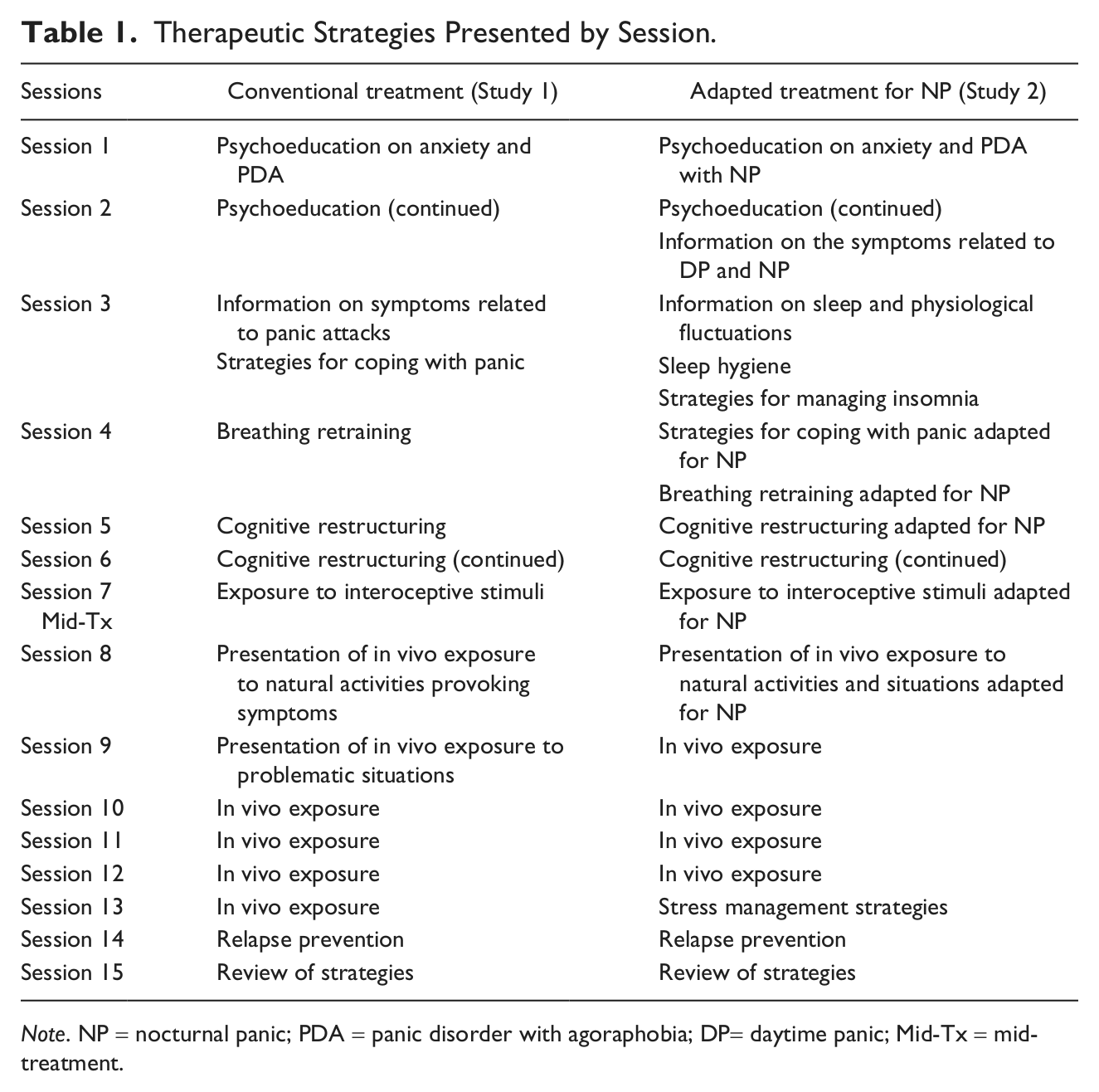
Note. NP = nocturnal panic; PDA = panic disorder with agoraphobia; DP= daytime panic; Mid-Tx = mid-treatment.
Procedure
The participants were first evaluated by a psychiatrist and then by the first author, a psychologist, using the ADIS-IV. To establish interrater agreement, the structured interviews were audiotaped and listened to by a research assistant blind to the research questions. Following the clinical assessment, the participants who met the inclusion criteria received information on the questionnaires and the self-monitoring booklets to be completed and brought back to the first meeting with the therapist 2 weeks after the initial assessment.
Therapy did not begin until the participant met the stability criteria on daily self-monitoring of level of fear of unusual bodily sensations for 14 days (Barlow & Hersen, 1984; Ladouceur & Bégin, 1986). The participants met with the therapist on an individual basis every 2 weeks to verify their fear levels. The participant who first attained the stability criteria began the therapy. The other participants then had a 30-min session involving no therapeutic interventions and saw the therapist again 2 weeks later, where the same procedure was repeated. When another participant met the stability criteria, he or she began treatment.
A psychologist with 15 years of clinical experience with CBT for anxiety disorders administered the treatment to all the participants. Each of the therapy sessions was recorded, and 25% of the audiotapes were listened to and rated by a trained graduate student. A therapeutic integrity of 98% was obtained.
The participants were reassessed midway through treatment, at the end of the treatment, and then at the 3-, 6-, and 12-month follow-ups using the measurement instruments. For the follow-ups, participants also had to complete the self-monitoring booklets during a 14-day interval. The interrater agreement for the diagnosis of PD for all three participants at all six measurement times was the same or within 1 point in 100% of the cases.
Results
Daily Self-Monitoring
Figure 1 shows the results of the daily self-monitoring of fear of unusual bodily sensations. The raw data were smoothed out by calculating a 3-day mean for each day: the day itself, the preceding day, and the following day. Data smoothing was applied so as to facilitate visual analysis by reducing the extent of day-to-day variability. A regression line was also added to better illustrate the general trend in the data.
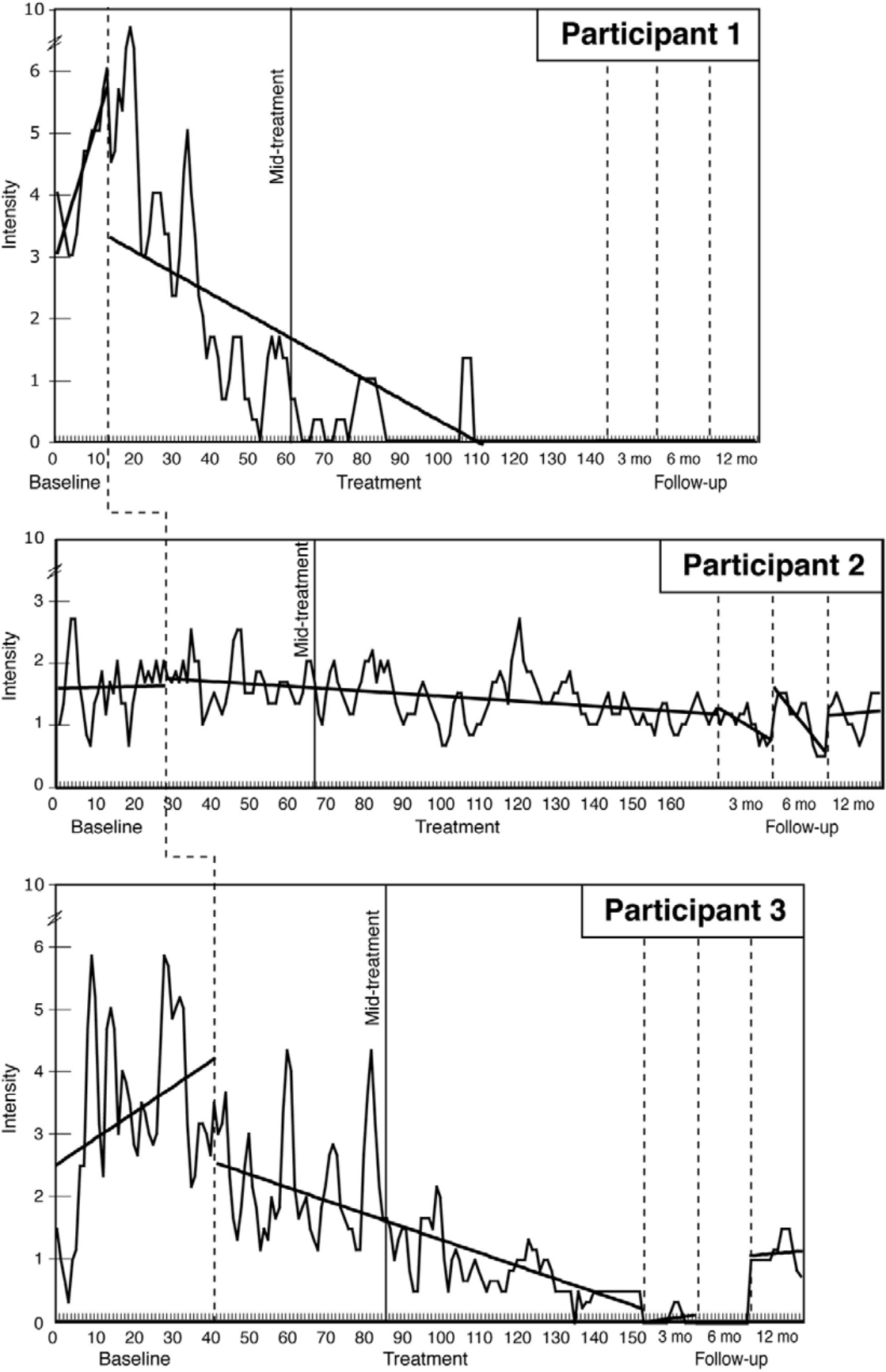
Level of fear of unusual bodily sensations as a function of duration and intensity, as reported by participants in their daily self-monitoring at baseline, during treatment, and at follow-ups in Study 1.
Taking a 50% decrease in the intensity of the fear of bodily sensations to indicate a clinical improvement, only Participant 2 did not improve sufficiently at any of the measurement times. However, the mean level of fear for Participants 1 and 3 dropped by more than 50% as of mid-treatment and was maintained at post-test, as well as at all follow-ups.
Standardized Clinician Ratings
At mid-treatment, all the participants still met the diagnostic criteria for PDA. However, at post-test and follow-ups, none presented PDA or any other comorbid diagnosis.
Self-Report Questionnaires
For the treatment outcome on self-report data, two indicators of clinically significant changes were calculated. First, a cutoff score corresponding to the C Index (Jacobson & Truax, 1992) was calculated for each questionnaire to determine whether the score obtained at the different measurement times had decreased in a clinically significant manner. As proposed by Jacobson and Truax (1992), clinical change should occur when the level of functioning subsequent to therapy places the client closer to the mean of the functional population compared with the dysfunctional population. The C Index was selected because data from normal samples were available (Turgeon, O’Connor, Marchand, & Freeston, 2002), and also, these data overlapped with scores from clinical samples.
The second method consisted of verifying the extent of the change or improvement induced by the treatment. Jacobson and Truax (1992) proposed a reliable change index (RCI). The cutoff point used here was 1.65, which corresponds to a one-tailed 95% confidence interval. Table 2 shows the scores obtained by each participant at the different testing times, their attainment or not of a score in the nonclinical range and of a significant level of change.
Questionnaire Cutoff Points and Scores Obtained by Participants at Pretest, Mid-Treatment, Post-test, and Follow-Ups in Study 1.
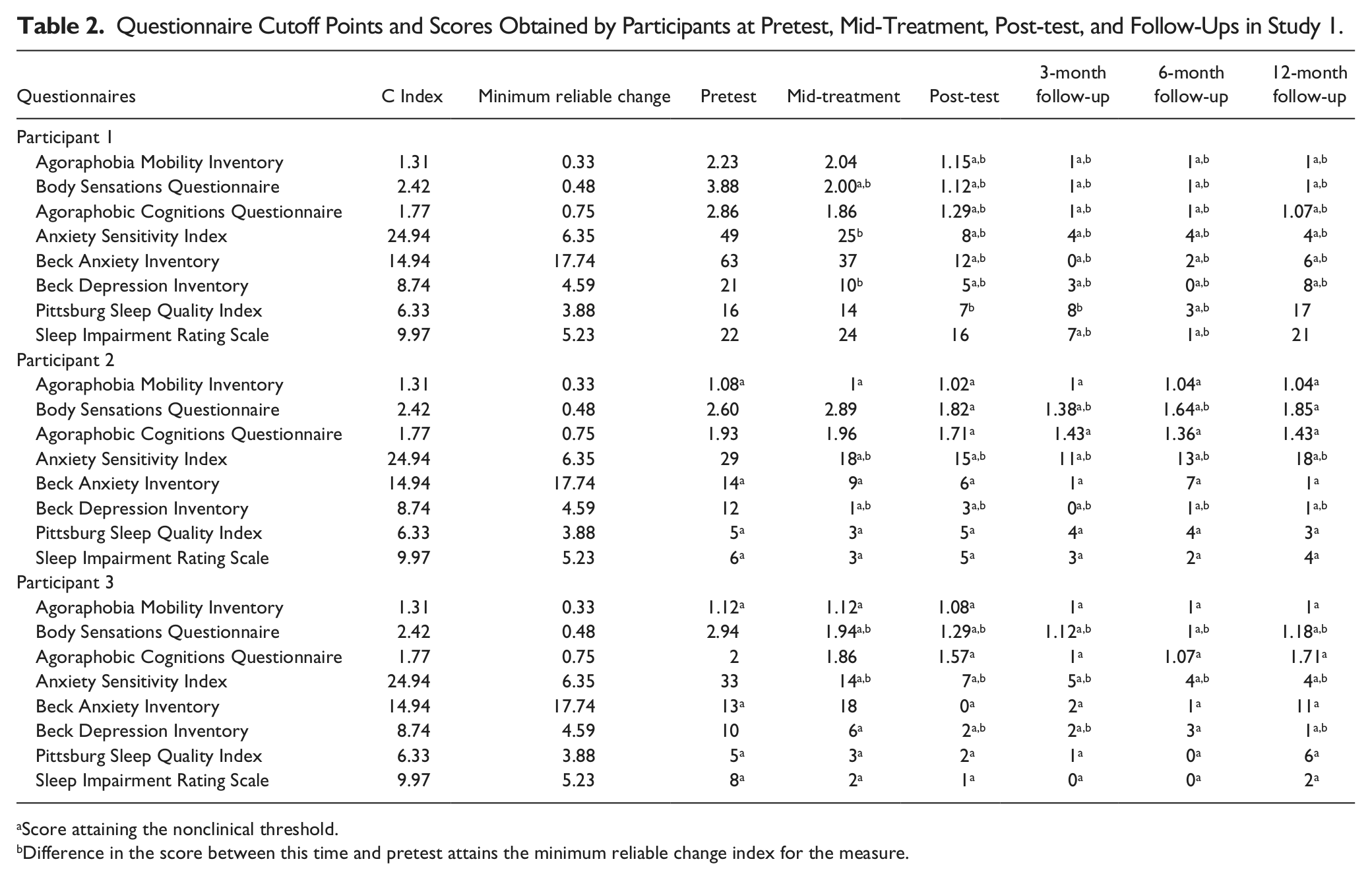
Score attaining the nonclinical threshold.
Difference in the score between this time and pretest attains the minimum reliable change index for the measure.
C Index
Participant 1 reached a nonclinical level only on the BSQ at mid-treatment, and a nonclinical range on all questionnaires at post-test and follow-ups, with the exception of sleep measures. Participant 2 presented nonclinical levels at mid-treatment for several measures, except the BSQ and the ACQ. However, he achieved scores in the nonclinical range for all measures at post-test and follow-ups. Participant 3 obtained the nonclinical threshold at mid-treatment for the majority of the measures, except the ACQ and the BAI, but then managed to attain it on all the questionnaires at post-test and follow-ups.
RCI
For Participant 1, a significant change was noted mainly at post-test and all the follow-ups for all the measures except in regard to sleep, where there appeared to be a resurfacing of problems 12 months after treatment. In Participant 2, there was a significant change noted at all testing times solely on the ASI and the BDI. A significant change was also noted on the BSQ at 3- and 6-month follow-ups. Participant 3 attained the RCI at mid-treatment on the BSQ and the ASI, and then on the BDI at post-test. These improvements were maintained at the follow-ups, except for a slight drop in gains on the BDI at the 6-month follow-up.
Frequency of DP and NP Attacks
Figure 2 shows the mean number of DP and NP attacks per week experienced by each participant during the pretest, treatment, post-test, and follow-up periods. The results indicate a marked decrease in the number of panic attacks for all participants following treatment. In fact, there was a total absence of panic at the end of treatment for two of the three participants. Gains were maintained over time.
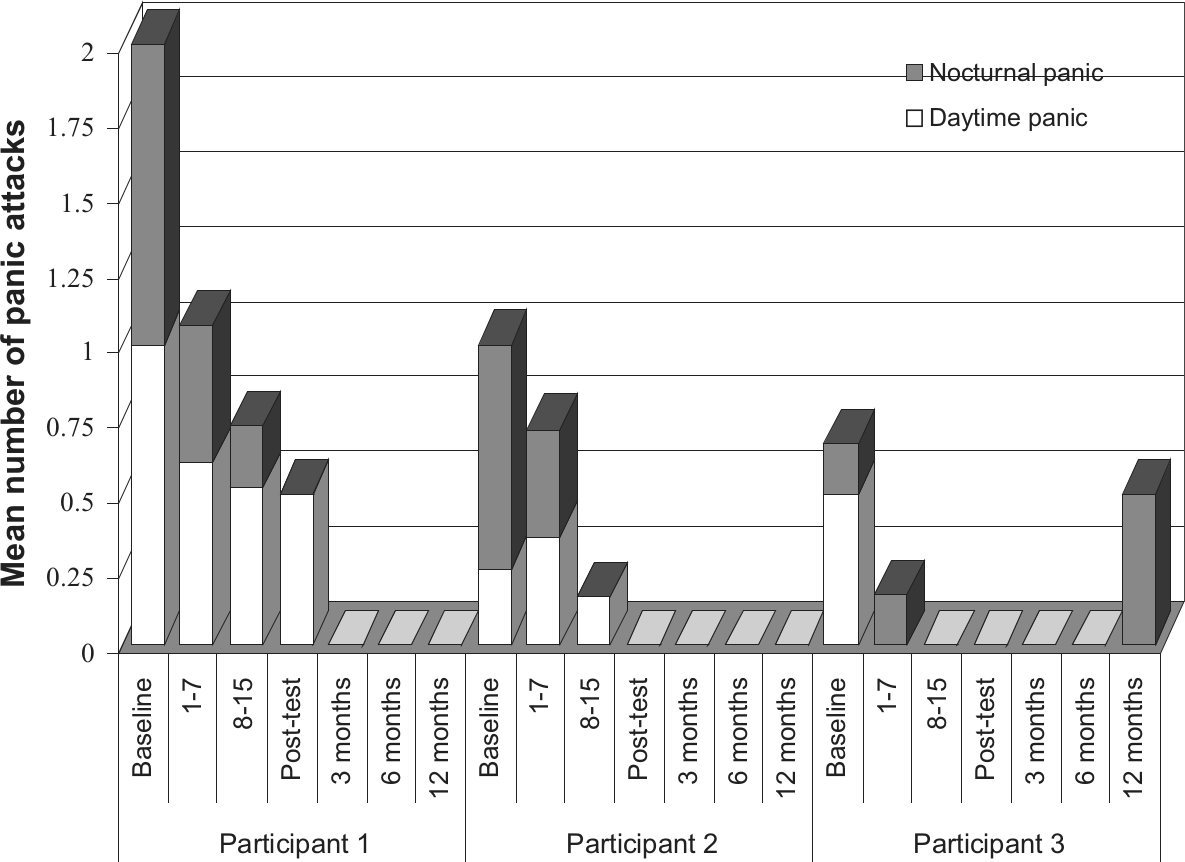
Mean number of daytime and nocturnal panic attacks per week as reported by participants in their daily self-monitoring during baseline, start-of-treatment to mid-treatment, mid-treatment to end-of-treatment, post-test, and follow-up periods in Study 1.
End-State Functioning
To determine the end-state functioning at the different testing times, a composite score was derived from the principal measures specific to PD with NPs. Criteria for the different assessment modalities were as follows: (a) a decrease of at least 50% in the scores obtained through self-monitoring of fear of unusual bodily sensations; (b) a decrease of at least 50% in the scores obtained through self-monitoring of worry over recurrence of DPs and NPs; (c) the absence of DP and NP; (d) the attainment of the C Index and of the RCI on the BSQ, as well as on the ACQ, (e) the ASI, (f) the BDI, and (g) the BAI; and finally, (h) the absence of PD diagnosis. The number of modalities on which the specific criterion was met determined the level of end-state functioning: low (0-2 modality), moderate (3-5), and high (6-8). Taking these criteria into account, Participants 1 and 3 attained moderate and low levels of functioning, respectively, at mid-treatment, but presented a high end-state functioning starting at post-test and at all the follow-ups. Participant 2 went from a low level at mid-treatment to a moderate level at post-test and the follow-ups.
Sleep Questionnaires
Results obtained from the sleep questionnaires indicated the presence of problems mainly in Participant 1. These problems appear to have diminished following treatment, as observed in the attainment of RCI on the PSQI at post-test and at 3- and 6-month follow-ups, as well as on the SIRS at the same follow-ups. However, her sleep disturbances resurfaced at the 12-month follow-up. Participant 2 did not suffer from any significant level of sleep impairment. Participant 3 had slight sleep difficulties initially, which then tended to diminish, but she did not attain the RCI due to a floor effect.
Discussion
Results show that two out of three participants attained and maintained a high end-state functioning for up to 12 months following treatment. Nonetheless, Participant 2 attained a moderate level of functioning at post-test and all follow-ups. In fact, he no longer met diagnostic criteria for PD, nor suffered from NP or DP at post-test and follow-ups. Generally speaking, all the participants benefited from this conventional treatment for their PD with NPs. These results do not therefore support our hypothesis to the effect that conventional treatment is ineffective in bringing significant clinical changes in patients with NPs.
A number of factors may explain the limited progress made by Participant 2, such as the use of cognitive avoidance of physical sensations, his beliefs regarding the importance of being in total control at all time, a specific phobia of vomiting, and more minor difficulties at pretest which limited the magnitude of progress.
Results also show a substantial decrease in NP and DP for all participants and even the absence of panic in two of the three participants at post-test and follow-ups. The appearance of a NP during the 12-month follow-up for Participant 3 may be explained by the presence of a new stressor in this person’s life (i.e., the beginning of a new intimate relationship). It therefore appears that conventional treatment strategies are sufficient to hinder the processes underlying the onset of NP. An even more noteworthy fact was the faster decrease in NPs versus the DPs in two of the three participants. This trend was not mentioned in any of the NP studies that we surveyed. One possible explanation may be that the strategies used in the first part of the treatment help reduce fear, hypervigilance, and the autonomic reaction to physical sensations relatively quickly. Then, as soon as this fear diminishes, participants become less aware of physiological changes during sleep and no longer awaken in a state of panic at night. However, they are still readily aware of such changes occurring during the daytime according to the state of wakefulness.
The impact of conventional treatment on the quality of sleep appears less significant. Participant 2 had few problems in this regard. For Participant 3, there was some improvement in her sleep, but as her difficulties were minor at the outset, this change did not prove significant. However, the quality of sleep of Participant 1 was more severely impaired prior to treatment. Her sleep improved significantly as of post-test, but deteriorated again 12 months after treatment, despite her improvement in terms of PD and NPs. Other factors appear to have intervened and impacted on her sleep, such as worries in regard to financial and interpersonal problems.
In summary, results suggest that conventional treatment for PD is effective for NPs and treatment gains remain for up to 1 year after therapy. These results suggest that clinicians may use the customary strategies for PD, without additions or adaptations, to treat their patients who suffer from NP.
Study 2
Method
This study used the same method as Study 1, except that the treatment protocol was adapted for NPs.
Participants
Participant A was a 25-year-old woman recruited through newspaper advertisements. She was living in a common-law relationship and had one child. She was studying toward her bachelor’s degree and did not have a paying job. She reported suffering from PDA for the past 3 years. At the initial assessment, she presented a diagnosis of PDA (i.e., severity rating of 5/8, moderate/severe), with four NPs and one DP during the previous month. She was not taking any psychotropic drug.
Participant B was a 43-year-old woman also recruited through newspaper advertisements. She was married and had two children. She had a CEGEP diploma and held a job as a dental hygienist. She reported having a problem with PDA for the past 11 years. At the initial assessment, a severe PDA was diagnosed (6/8), with five NPs and eight DPs during the previous month. She also had a diagnosis of GAD (4/8, moderate). She was not taking any medication on a regular basis, but had taken lorazepam (0.5 mg) twice in the past few months.
Participant C was a 24-year-old single woman, without children. She was recruited through newspaper advertisements. She was a student in a bachelor’s degree program and had a part-time job. She reported suffering from PDA for approximately 4 years. The initial assessment confirmed the presence of a PDA diagnosis (5/8, moderate/severe), with four NPs and one DP during the previous month. She also met the diagnostic criteria of a social phobia (4/8, moderate). She was not taking any psychotropic drug.
Treatment
The treatment used in this study included the same conventional strategies as in Study 1, but with adaptations made for NPs (see Table 1). The changes were derived from the modified treatment protocol for NPs developed by Craske (1993) as well as from the books La peur d’avoir peur (Marchand & Letarte, 1993) and Vaincre les ennemis du sommeil (Morin, 1997). Unlike the first study, the treatment addressed NPs as well as DPs.
Procedure
The interrater agreement for the diagnosis of PD was the same or within 1 point in 94% of the cases, and a therapeutic integrity of 96% was obtained.
Results
Daily Self-Monitoring
Figure 3 presents the results of the participants daily self-monitoring of their fear of unusual bodily sensations. All the participants improved following treatment, and gains were maintained for 12 months (i.e., 50% decreased). In addition, Participants A and B attained a 50% improvement as of mid-treatment.
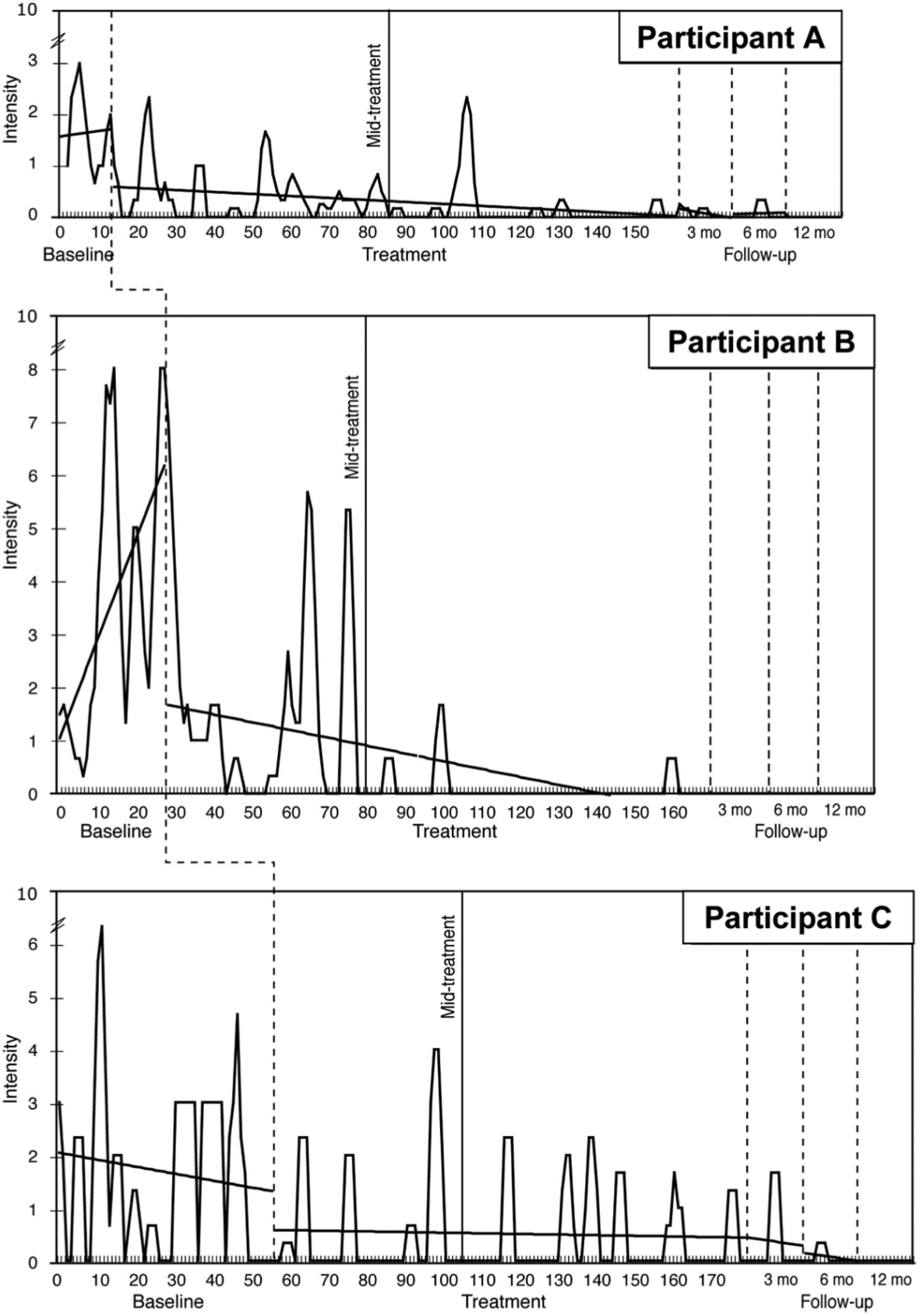
Level of fear of unusual bodily sensations as a function of duration and intensity, as reported by participants in their daily self-monitoring at baseline, during treatment, and at follow-ups in Study 2.
Standardized Clinician Ratings
Starting at mid-treatment, Participants A and C no longer met the diagnostic criteria for PDA, and this was maintained up to the 12-month follow-up. Participant B still met the diagnostic criteria for PDA at post-test but no longer at follow-ups.
Self-Report Questionnaires
Table 3 shows the scores obtained by each of the participants at the different testing times, the attainment of a nonclinical level, and the significant level of change.
Questionnaire Cutoff Points and Scores Obtained by Participants at Pretest, Mid-Treatment, Post-test, and Follow-Ups in Study 2.
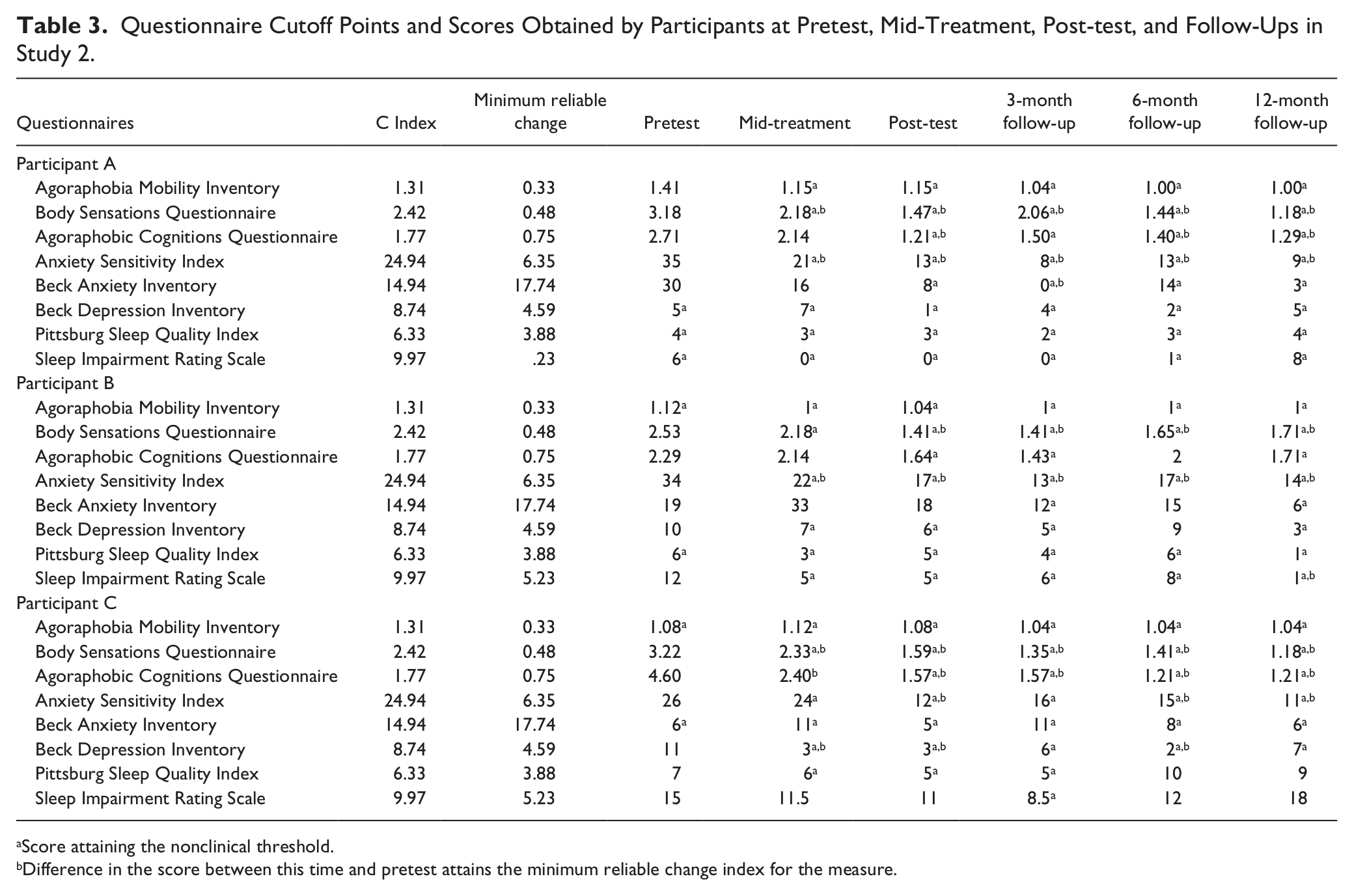
Score attaining the nonclinical threshold.
Difference in the score between this time and pretest attains the minimum reliable change index for the measure.
C Index
Participants A and B reached the nonclinical threshold as of mid-treatment on nearly all the questionnaires except for the ACQ and the BAI. Participant A attained it for all measures at post-test and the follow-ups. Participant B achieved the nonclinical level on all measures except for the BAI at post-test, but attained it on all questionnaires 3 months after treatment. There was a slight decrease in the gains at the 6-month follow-up on the ACQ, the BAI, and the BDI. However, 12 months after therapy, she again succeeded in attaining the nonclinical threshold on all measures. Participant C reached the nonclinical level on all questionnaires at all testing times, except for the ACQ at mid-treatment and sleep measures at mid-treatment, post-test, and 6- and 12-month follow-ups.
RCI
There was a significant change for Participant A, mainly at post-test and follow-ups, for the measures related specifically to PD, except for the ACQ at the 3-month follow-up and the AMI at all testing times. Participant B improved significantly only on the BSQ starting at post-test, and on the ASI starting at mid-treatment. Participant C attained the RCI for the PD-specific measures, except on the AMI and the ASI at mid-treatment and the 3-month follow-up. She also achieved the RCI on the BDI, but only at mid-treatment, post-test, and the 6-month follow-up.
Frequency of DP and NP Attacks
Figure 4 shows the mean number of DP and NP per week experienced by each participant at each time of measurement. Results revealed a quick decrease in the number of panic attacks. In fact, no panic was reported at mid-treatment by Participant A, and by Participant C at the end of treatment. Moreover, this absence of panic was maintained in the long term. Participant B reported no NP at the end of treatment, but the DPs continued to occur until 6 months after therapy, although less frequently. As in Study 1, NPs appear to have decreased faster than DPs for Participants A and B.

Mean number of daytime and nocturnal panic attacks per week as reported by participants in their daily self-monitoring during baseline, start-of-treatment to mid-treatment, mid-treatment to end-of-treatment, post-test, and follow-up periods in Study 2.
End-State Functioning
Participants A and C attained a moderate level of functioning as of mid-treatment, and a high end-state functioning at post-test and all the follow-ups. Participant B reached a low level of functioning at mid-treatment, and a moderate level at post-test and 3- and 6-month follow-ups. However, she managed to attain a high end-state functioning 12 months after the therapy.
Sleep Questionnaires
Participant A had no sleep problems at any testing times. Participant B experienced some improvement in her sleep problems beginning at mid-treatment and 12 months after therapy, but did not reach the RCI since her problems were relatively minor to begin with. Participant C had more substantial sleep problems, but the adapted treatment did not appear to bring about any significant change, and gains were not maintained at the 6- and 12-month follow-ups.
Discussion
Results showed that two of the three participants attained a moderate level of functioning at mid-treatment and high end-state functioning at post-test, which they maintained until 12 months after treatment. Although Participant B did not reach a moderate level of functioning until the 3- and 6-month follow-ups, she continued to progress and finally attained high end-state functioning 12 months after treatment. All participants showed significant clinical improvement and benefited from the adapted treatment. These results support our hypothesis that addressing NP in therapy will help improve the symptoms and are in concordance with those obtained by Craske et al. (2005).
A number of factors can explain the more limited and gradual progress made by Participant B. First, the slower decrease in DPs may be attributable to her cigarette and alcohol consumption which she used as a means for coping with stress, and could predispose to panic attacks. A review supported the role of polysubstance (i.e., daily cigarette smoking and alcohol) in relation to panic attack and PD vulnerability and maintenance (Zvolensky, Feldner, Leen-Feldner, & McLeish, 2005). She reduced her consumption at follow-up, and this factor may explain the absence of panic attacks at the 12-month follow-up. Moreover, she reported the presence of personal difficulties such as family conflicts and comorbid GAD that might have impacted her improvement.
Results also support the efficacy of the adapted treatment to decrease both DP and NP. In fact, no panic was reported by two out of three participants at the end of therapy and this lasted until 12 months after treatment. As observed in the previous study, NPs decreased more quickly than the DPs in two of the three participants. The other participant suffered almost exclusively from NPs from the beginning and her main fear was that of suffocating in her sleep.
Regarding the impact of the adapted treatment on sleep quality, it was difficult to reach any clear conclusions, largely owing to the few difficulties experienced at this level in this sample. Participant C, who had substantial sleep problems, saw her sleep quality barely improved and even worsened at the 6- and 12-month follow-ups. Possible factors other than NPs may have contributed to her sleep worsening and include the following two explanations: first, at the 1-year follow-up, the participant was trying to stop smoking and second, her apprehensions, worries, and physical activation related to social anxiety reached high levels. Participant B, who suffered from a comorbid GAD had only minor sleep problems, and these tended to improve. At the 3- and 6-month follow-ups, she reported a mild deterioration in her quality of sleep and this coincided with stressing factors present in her life.
Conclusion
Conventional and adapted CBT both appear to be effective in treating PD with NPs. Both treatments show reduction in the frequency of DP and NP. Moreover, changes brought by the adapted treatment on sleep quality measures were similar to those obtained using the conventional treatment. Hence, the addition or adaptation of certain strategies to target NPs does not seem to improve significantly the conventional treatment for NP.
Nonetheless, Study 2 does raise the possibility that an adapted treatment may bring clinical changes more quickly. In fact, two of the three participants attained a moderate level of functioning at mid-treatment, compared with only one in the first study. Since the level of end-state functioning is a composite score derived using different measures specific to PD with NP, it may serve as a good indicator, revealing the possibility of achieving faster change through adapted treatment. However, at the end of the treatment, the changes observed were relatively comparable in both studies: two out of three participants attained high end-state functioning. The faster changes noted in Study 2 appear to have occurred during the first part of the treatment. This could be explained by a number of factors like the adaptation of the information in the treatment to target NP.
While both studies generated interesting results, it is important to take into account their exploratory and descriptive nature, as well as the presence of certain limitations. First, the design used and the small samples which comprised mainly women make results difficult to generalize. Second, self-monitoring as a method of data collection sometimes lacks precision. However, the general decrease in scores concurs with results obtained through the self-report questionnaires and the standardized clinician ratings. Finally, the severity of PD in the samples was moderate which has limited the scope of symptom modifications that could be measured and resulted at times in a floor effect.
To the best of our knowledge, this is the first study that has sought to verify the efficacy of conventional CBT for PD in a sample of individuals suffering from NP. Future studies in this area could be done with a larger sample with the inclusion of a control group to verify whether time to clinical improvement is different between the two treatment approaches. A series of dismantling studies would help to evaluate the relative efficacy of the different therapeutic components (e.g., exposure compared with cognitive restructuring for NP). At last, evaluation of the impact of treatment on quality of sleep in people suffering from NP is needed by using more specific instrument, such as the sleep diary (Morin, 1993).
In light of our clinical observations, conventional strategies for DP appear to be generalized to NP and emerge as useful for targeting NPs. It is likely that a slight decrease in fear regarding bodily sensations is enough to eliminate the triggering of NPs. We can therefore assume that strategies such as information on bodily sensations, cognitive restructuring, and exposure to interoceptive stimuli may be very useful in helping decrease apprehension of the symptoms and in reducing the autonomic reaction caused by changes in bodily state experienced during sleep, which could in turn limit the arousals from sleep in a state of panic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.