
Abstract
The current study investigated the effects of a Video Self-Modeling (VSM) intervention on the compliance and aggressive behavior of three children placed in a psychiatric hospital. Each participant viewed brief video clips of himself following simple adult instructions just prior to the school’s morning session and the unit’s afternoon free period. A multiple baseline design across settings was used to evaluate the effects of the VSM intervention on compliance with staff instructions and aggressive behavior on the hospital unit and in the hospital-based classroom. All three participants exhibited higher levels of compliance and fewer aggressive episodes during the intervention condition, and the effects were generally maintained when the intervention was withdrawn. Hospital staff reported at the conclusion of the study that the VSM intervention was easy to implement and beneficial for all participants. Taken altogether, the results suggest VSM is a promising, socially acceptable, and proactive intervention approach for improving the behavior of noncompliant children.
Improving compliance to adult instructions is a critical component of many behavior management programs in home, school, and clinical settings for children with emotional and behavioral disorders. This is particularly salient for children with Oppositional Defiant Disorder (ODD) who commonly defy or refuse to comply with adult instructions or rules (Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association, 2013). Lack of compliance to adult instructions and defiant behavior impedes positive interactions with adults and peers and may contribute to the presence of aggressive behavior, presenting a barrier to successful school and community integration for children with ODD. Interventions targeting compliance have traditionally consisted of antecedent (e.g., precision commands, increasing predictability) or consequent strategies (e.g., contingency contracts, differential reinforcement) with varying degrees of success. Though underutilized in school and clinical settings, video modeling presents a promising new intervention modality to address compliance in children with ODD and other emotional and behavioral disorders.
Video modeling is a technique that involves showing the child video footage of successful behavior. A video modeling intervention typically involves a child watching a video demonstration of a target behavior and then imitating the behavior of the model. Video modeling can be used with peers, adults, or self as a model (video self-modeling [VSM]). VSM is a specific application of video modeling that allows the child to observe herself or himself, rather than a peer, successfully performing a behavior (Dowrick, 2012). Research on video modeling indicates that watching predominantly positive and/or successful behaviors of oneself, as opposed to negative and/or unsuccessful behaviors, is an essential ingredient to effective modeling interventions (Bellini & Akullian, 2007; Dowrick, 2012).
Video modeling has been used across multiple disciplines and populations, including children with Attention Deficit Hyperactivity Disorder (ADHD), behavioral disorders, autism spectrum disorders, learning disabilities, cognitive disabilities, and various physical disabilities (Baker, Lang, & O’Reilly, 2009; Bellini, & Akullian, 2007; Dowrick, 2012; Woltersdorf, 1992). Numerous studies have demonstrated that VSM interventions produce substantial intervention, maintenance, and generalization effects across a myriad of dependent variables (Dowrick, 2012). As such, video modeling interventions have recently been identified as “evidence based” for youth with autism spectrum disorders (National Autism Center, 2009). Although not currently a widely adopted intervention for youth with emotional and behavioral disorders, research has indicated substantial promise for the use of video modeling with this population (Baker et al., 2009).
Baker et al. (2009) conducted a meta-analysis of 16 video modeling studies for youth with emotional and behavioral disorders published between the years 1976 and 2005. Results of the meta-analysis indicated that video modeling is an effective intervention modality for this population. The authors concluded that video modeling is highly suitable for children with emotional and behavioral disorders because it is positive and instructive, rather than punitive and reductive. Though the meta-analysis did not specifically measure the impact of video modeling on compliance to adult instructions, the studies included in the meta-analysis targeted a broad range of behaviors that encompass compliance, including positive peer interactions (Falk, Dunlap, & Kern, 1996; Kern-Dunlap et al., 1992; Kern et al., 1995), on-task behavior (Booth & Fairbank, 1983; Clare, Jenson, Kehle, & Bray, 2000; Walther & Beare, 1991; Woltersdorf, 1992), and inappropriate behavior (Davis, 1979; Embregts, 2000; Embregts, 2002; Esveldt, Dawson, & Forness, 1974; Kehle, Clark, Jenson, & Wampold, 1986; Lonnecker, Brady, McPherson, & Hawkins, 1994; O’Reilly et al., 2005; Osborne, 1986). Few of the participants included in the meta-analysis were identified as having ODD, and the results were not categorized by diagnosis. As such, the benefits of video modeling interventions for youth specifically diagnosed with ODD have not been empirically validated.
Dowrick (1999) separated VSM interventions into two categories, positive self-review (PSR) and video feedforward. PSR refers to individuals viewing themselves successfully engaging in a behavior or activity that is currently in their behavioral repertoire, but emitted at a low frequency. For instance, if a child complies with adult instructions, but at a very low frequency, then the intervention would consist of capturing the child’s behavior on video and then editing out all instances of noncompliance. The child would then be shown a brief video that depicts only instances of compliance to adult instructions. Video feedforward is another category of VSM interventions where individuals observe themselves successfully demonstrating behaviors that they never (or almost never) perform autonomously. A feedforward intervention may involve the use of “hidden” supports. For example, prompting and cueing might be provided to encourage the child to comply with adult instructions. The adult prompting is then edited out of the video prior to the child watching the compliance behavior. Another example of a feedforward intervention for compliance might involve “splicing” together disparate footage of adult instructions and child behavior. This type of intervention is best suited for children who refuse to comply with adult instructions in spite of prompting or cueing. For example, video footage of the child sitting down in a chair, or cleaning up toys, would be spliced together with footage (recorded at a separate time) of the adult instructing the child to “sit down” or to “clean up toys.” The child would then watch an edited video clip that depicts her or him ostensibly complying with her or his parents’ request to sit down or clean up.
Although research has found video modeling to be an effective intervention for youth with emotional and behavioral disorders, the literature is limited to studies examining video modeling as part of intervention packages (Baker et al., 2009). To our knowledge, there has not been an empirical study of video modeling or VSM as a single intervention modality for children with emotional and behavioral disorders. In addition, most of the existing research on video modeling as an intervention for youth with emotional and behavioral disorders has targeted peer interactions, on-task behavior, and aggression. Very few studies have investigated video modeling or VSM as an intervention for compliance with adult instructions. Lonnecker et al. (1994) targeted a broadly defined category of cooperative behavior that included following adult instructions. However, the reported dependent variable was cooperative behavior that also included other prosocial classroom behaviors such as active participation, completing classroom assignments, and speaking with an “indoor voice.” Finally, existing research has not fully addressed the social acceptability of video modeling or VSM with youth with emotional and behavioral disorders. Baker et al. noted the exclusion of social acceptability data in most of the studies examining video modeling or VSM as an intervention for youth with emotional and behavioral disorders. Assessing the social acceptability might be particularly important for video modeling, as the procedures are simple and require little time to implement, yet the technology involved in making the videos might limit the intervention’s practicability. The purpose of the current study was to address the aforementioned gaps in the literature by investigating the application of a VSM intervention for three noncompliant students. Specifically, we attempted to extend existing research examining the benefits of a VSM intervention in increasing compliance and decreasing aggressive episodes following noncompliance in a residential setting. The study also improved upon existing research by addressing the social acceptability of the VSM procedures by hospital staff (i.e., classroom teachers and paraprofessionals, nurses, direct care staff).
Method
Participants and Setting
Participants included three elementary aged children who engaged in high rates of noncompliant behavior. All participants were patients in an acute care psychiatric hospital, admitted at least 2 weeks prior to beginning the study. Each participant was referred to the psychiatric hospital because of a history of aggressive and defiant behavior at home and school. Dan was 8 years old at the time of the study and was diagnosed with ODD and ADHD. Bob was 8 years old at the time of the study and was diagnosed with ODD. Tom was 7 years old at the time of the study and was diagnosed with ODD and ADHD. Diagnostic information was obtained through a review of each participant’s most recent psychiatric and psychological evaluations. Each participant was Caucasian and spoke English as the primary language. Dan was prescribed 20 mg of Adderall XR and Tom was prescribed 36 mg of Concerta, each to be taken once daily in the morning. Bob was not prescribed medication at the time of the study. Clinical treatment team members (e.g., psychiatrists, therapists, educational staff) referred participants to the hospital’s psychological services team due to extreme levels of noncompliant behavior and physical aggression following defiant episodes.
The intervention was conducted in the hospital’s pediatric inpatient program during the months of March and April. Specifically, the study took place on the children’s psychiatric inpatient unit during the mid-afternoon free period (i.e., from 2:00 p.m. to 3:00 p.m.) and in a hospital-based classroom during the morning independent seatwork period (i.e., 9:30 a.m. to 10:30 a.m.). During the mid-afternoon free period, children were permitted to play games, watch television, or complete quiet activities (e.g., read, crafts). During the independent seatwork period, children were expected to complete simple academic assignments (e.g., reading passages and answer comprehension questions, math computation worksheets). The academic assignments were all at individual students’ instructional level. These periods were selected at the clinical treatment team’s request. The number of children on the unit during the study ranged from 8 to 15, whereas the number of children in the hospital-based classroom during the study ranged from 3 to 5. School staff consisted of a certified classroom teacher possessing a master’s degree in special education and two paraprofessionals who were trained to work with children with disruptive behavior disorders. Unit staff consisted of one or two psychiatric nurse practitioners, one registered nurse, and several direct care staff who were trained in working with children with psychiatric conditions. All patients of the hospital participated in daily individual and group therapy directed by licensed therapists. Patients also met daily with one of two unit psychiatrists. There were no concurrent behavioral interventions in place during the study.
Measures
Percentage of compliance with adult instructions was the primary dependent variable for analysis. Compliance was defined as initiating an adult instruction within 10 s of the instruction being verbally given and completing the instruction within an appropriate amount of time as determined by the adult giving the instruction. All instructions involved completing simple chores or tasks (e.g., put clothes away, wipe table, erase board, pick up pencil). Examples of noncompliance included arguing, complaining, exaggerated sighing, engaging in an unauthorized task, and ignoring the request. Percentage of compliance was calculated by dividing the number of instances of compliance by the number of instances of compliance plus the number of instances of noncompliance and multiplying by 100%. The first author trained direct care staff and paraprofessionals to collect behavioral observation data. The training involved a 1-hr formal presentation on behavioral observation followed by opportunities to practice collecting observational data. Before the intervention commenced, observers obtained agreement rates with the first author that exceeded 94%.
In addition, the percentage of instructions leading to an aggressive (i.e., physical, verbal) episode was obtained for each participant during baseline, intervention, and follow-up phases. All acts of physical and verbal aggression following an adult instruction were recorded by the hospital staff per regular hospital procedures and then stored in the participant’s electronic record. Data on physical and verbal aggression were gleaned from each participant’s electronic record at the conclusion of the study. As such, interobserver agreement data on the percentage of instructions leading to an aggressive episode were not collected. The hospital provided definitions of physical and verbal aggression as well as defined the parameters of an episode. Physical aggression was operationally defined as throwing objects, property damage, or assault (e.g., hitting a peer, kicking a staff member). Verbal aggression was operationally defined as swearing, making an insulting statement (e.g., name calling), or threats of physical aggression. An aggressive episode began with the observation by a staff member of an aggressive behavior and ended when the staff member observed the participant not engaging in an aggressive behavior for 1 min. All hospital staff members were trained to identify physically and verbally aggressive episodes. The percentage of instructions leading to an aggressive episode was calculated by dividing the number of episodes of aggression following an instruction by the number of instructions given and multiplying by 100%.
Finally, treatment acceptability data were collected using an informal seven-item questionnaire developed by the first author. Each teacher, paraprofessional, nurse, and direct care staff completed the questionnaire when the study was finished. Staff were told that the purpose of the questionnaire was to collect additional information about the intervention. The seven-item questionnaire addressed the following: teacher and staff satisfaction with the intervention, ease of implementation, and the nature of the outcomes of compliance, productivity (i.e., chore completion, academics), and overall behavior (i.e., cooperation with staff, physical and verbal aggression). Questionnaire items were rated on a 5-point Likert-type scale with the following response options: not at all (1), a little (2), somewhat (3), a lot (4), or very much (5).
Procedures
Before beginning the intervention, data were collected to identify specific adult instructions that frequently resulted in noncompliance. Psychiatric inpatient unit staff members and the certified classroom teacher independently developed a list of 30 common adult instructions given in each setting (e.g., “please put your clothes in the hamper,” “please pick up your pencil”). Staff members were told to select instructions that the participants would be able to independently complete within 1 min. Unit and classroom staff members then gave each participant each instruction 10 times randomly over an 8-day period during the unit’s mid-afternoon free period and classroom’s morning independent seatwork session. All instructions involved simple initiation commands (i.e., “do” or “start” something).
Percentage of compliance was calculated for each instruction. Instructions complied with 50% of the time or less were used in the study. Instructions complied with more than 50% of the time were not used in the study. Examples of instructions on the hospital unit included throwing away trash, bringing dishes to the housekeeping station, sitting down, putting clothing on, cleaning off desk, lining up, and turning off music or television. Examples of classroom instructions included taking out writing utensils, putting away items (e.g., schoolwork, writing utensils, toys), writing name on paper, putting feet on floor, and sitting in chair.
Video recording and editing
Raw video footage was collected over 2 days by direct care staff. Two weeks prior to beginning baseline data collection, approximately 1 hr of video was taken in each setting (i.e., hospital unit, school-based classroom). Hospital unit and educational staff members were instructed to interact with the participants and other children in a typical manner and maintain consistent patterns of responses to participant compliance or noncompliance. The VSM strategy of PSR was utilized for the intervention. Raw video footage was edited to include six instances of compliance with the previously identified instructions in each setting. Each video clip was approximately 1 min in length for a total of 6 min of footage in each setting. Video clips were saved on a DVD. Clips were accessible by using the menu feature on the DVD player (e.g., “School Clip 1,” “School Clip 2,” “Unit Clip 1,” “Unit Clip 2”). A DVD was produced for each participant. The hospital’s computing department conducted all video editing using Adobe Premiere Elements editing software.
Baseline
Baseline data collection began 3 days after the raw video footage was obtained. Each participant received between 10 and 15 identified instructions per setting per day given by either a hospital unit or classroom staff member. Staff members were instructed to select identified instructions that made sense given the context of the environment. The staff member stated the participant’s name followed by the instruction (e.g., “Dan, please put your feet on the floor”). The staff member giving the instruction provided brief verbal praise (e.g., “thank you,” “nice job”) following a participant’s compliance with the instruction. Staff members ignored noncompliance and waited at least 1 min before giving another instruction.
Intervention condition
The intervention condition occurred on 12 days across 3 weeks (i.e., 4 days per week). The intervention was conducted Monday through Thursday of each week. Due to significant changes in the hospital unit schedule (e.g., field trips, special programming), the intervention was not conducted on Fridays. The VSM intervention first began in the hospital setting, followed by the classroom setting for all three participants. On the first 2 days of the VSM intervention, participants viewed 4 video clips depicting compliance in the hospital setting only. Beginning on Day 3, participants also viewed an additional 4 video clips depicting compliance in the classroom setting. The eight video clips were shown each session until the VSM intervention was first withdrawn from the hospital setting only. Participants continued to view their video clips of the classroom setting for 2 additional days prior to beginning the follow-up phase in the classroom setting. Participants viewed classroom video clips in a spare classroom prior to starting the morning school session and inpatient unit video clips in a conference room on the inpatient unit after lunch and prior to beginning the unit’s afternoon free period. Participants were allowed to choose which video clips were viewed. Each participant was supervised by the same staff member when viewing the video clips and was alone with that staff member during the viewings. The staff member was instructed to only provide participants with brief verbal praise statements (i.e., “thank you for sitting appropriate,” “you’re doing a nice job”) contingent on appropriate viewing behavior defined as sitting quietly with head toward the television. The staff member was also instructed to redirect minor instances of inappropriate behavior. The intervention stopped when participant behavior became highly problematic or disruptive. The staff member told the participants prior to viewing the video clips that they would watch movies of themselves engaging in appropriate behavior. Similar to the baseline phase, during the intervention condition, participants were given between 10 and 15 identified instructions per setting per day and received brief praise for compliance. Staff members ignored noncompliance and waited at least 1 min before giving another instruction.
Follow-up condition
Following the intervention condition, all components of the treatment were removed. Participants were given between 10 and 15 identified instructions per setting per day. Staff members provided brief praise for compliance, ignored noncompliance, and waited at least 1 min before giving another instruction.
Data collection
Trained observers recorded participants’ instances of compliance and noncompliance during all conditions of the study. Data were collected during the hospital unit’s afternoon free period and the classroom’s morning independent seatwork session. Data were not collected on Fridays due to changes in the hospital unit schedule. The mean number of adult requests on the hospital unit for all participants was 11.63 (SD = 1.36). The mean number of adult requests in the classroom for all participants was 11.47 (SD = 1.10).
Experimental Design
A multiple baseline design across settings was used to assess the effects of the intervention on the percentage of compliance and number of aggressive episodes for each participant in each setting. Following baseline, the VSM intervention was presented to each participant. The intervention was removed at the end of the intervention phase and follow-up data were collected. Results were analyzed through visual and descriptive methods.
Interobserver Agreement and Treatment Integrity
Interobserver agreement (i.e., agreements divided by agreements plus disagreements and multiplied by 100%) was computed for 40% of baseline, 25% of intervention, and 25% of follow-up sessions for percentage compliance. The first author served as the second observer. The average observer agreement value was 99% (range = 97%-100%).
Treatment integrity was assessed via an intervention checklist completed by the hospital staff member assigned to sit with the participant during the viewing of video clips. According to the checklist, the appropriate number of videos was shown on all days. The first author or a research assistant conducted independent checks on 50% of the intervention days using the same intervention checklist. Integrity during the video viewings observed was 100%. Hospital staff noted that each participant was generally compliant during the viewings and rarely required redirection for inappropriate or disruptive behavior.
Results
Table 1 displays the percentage of compliance means and standard deviations for each condition, setting, and participant. Based on mean percentage of compliance, all three participants displayed higher levels of compliance during the VSM condition when compared with baseline levels. Two of the three participants (i.e., Dan, Bob) maintained high levels of compliance during the follow-up condition when compared with baseline levels. Tom displayed higher levels of compliance during the follow-up condition in the hospital unit setting but not in the classroom.
Means and Standard Deviations of Percentage of Compliance by Condition for Each Participant.
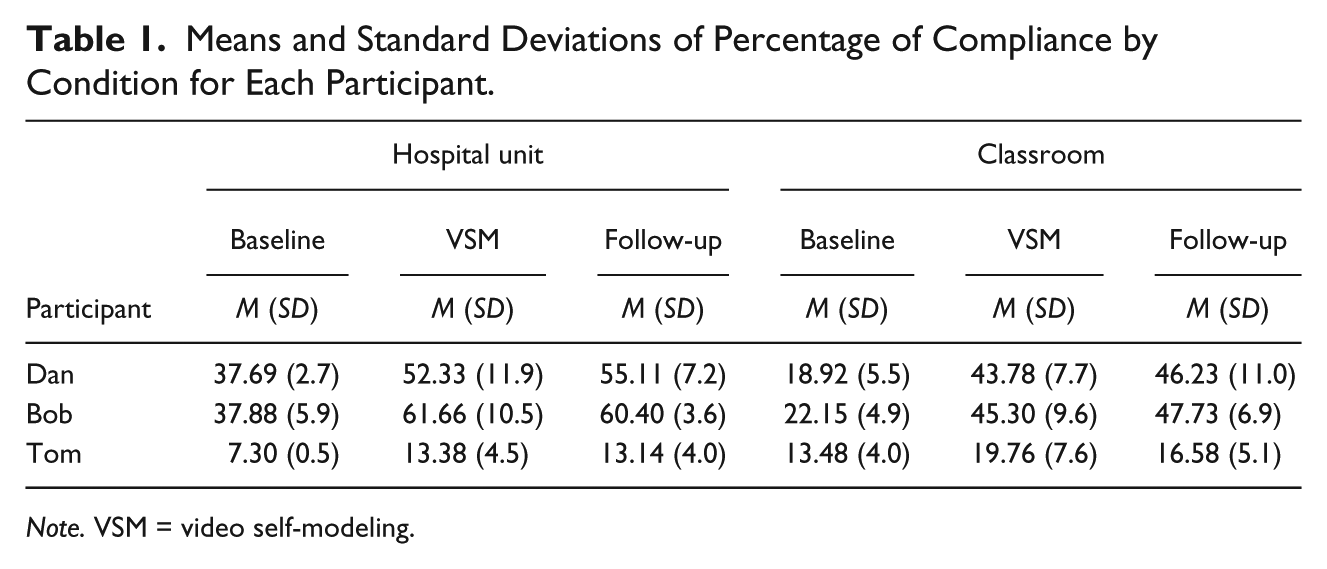
Note. VSM = video self-modeling.
Figures 1 to 3 display participants’ percentage of compliance during baseline, VSM, and follow-up conditions in both settings (i.e., hospital unit, classroom). Bob’s mean percentage of compliance during baseline for the hospital unit and classroom were 37.88% and 22.15%, respectively. During the VSM condition, his mean percentage of compliance increased to 61.66% on the hospital unit and 45.30% in the classroom indicating the intervention was effective at increasing Bob’s compliance in those settings. During the follow-up condition, Bob’s mean percentage of compliance were 60.40% on the hospital unit and 47.73% in the classroom suggesting Bob maintained his level of compliance in each setting after the removal of the VSM procedures.

Percentage of compliance for baseline, intervention, and follow-up conditions for Bob in the hospital unit and classroom settings.

Percentage of compliance for baseline, intervention, and follow-up conditions for Dan in the hospital unit and classroom settings.

Percentage of compliance for baseline, intervention, and follow-up conditions for Tom in the hospital unit and classroom settings.
Dan’s mean percentage of compliance during baseline was 37.69% on the hospital unit and 18.92% in the classroom. His mean percentage of compliance during the VSM condition was 52.33% on the hospital unit and 43.78% in the classroom suggesting the VSM intervention was effective in increasing Dan’s compliance in both settings. Follow-up mean percentage of compliance for the hospital unit and classroom were 55.11% and 46.23%, respectively, indicating Dan, like Bob, maintained his level of compliance in each setting following the removal of the VSM procedures.
Tom’s mean percentage of compliance during baseline for the hospital unit and classroom were 7.30% and 13.48%, respectively. During the VSM condition, his mean percentage of compliance for the hospital unit was 13.38%. For the classroom, Tom’s mean percentage of compliance was 19.76%. These data suggest the VSM intervention was effective in increasing Tom’s compliance when on the hospital unit but not as effective in the classroom. Tom’s mean percentage of compliance during the follow-up condition for the hospital unit and classroom were 13.14% and 16.58%, respectively. While the intervention’s effectiveness on the hospital unit was maintained after the removal of the VSM procedures, Tom’s percentage of compliance in the classroom decreased slightly when the VSM intervention was removed. However, Tom’s percentage of compliance in the classroom during the follow-up phase was higher than his percentage of compliance during the baseline phase.
Table 2 displays the percentage of instructions leading to an aggressive episode for each condition, setting, and participant. All three participants engaged in fewer incidents of aggression following an instruction during the VSM intervention condition when compared with baseline levels. In addition, all three participants engaged in fewer incidents of aggression in the follow-up condition compared with both baseline and intervention levels. For two participants (i.e., Dan, Bob), aggressive episodes following an instruction decreased to near zero levels in the follow-up condition.
Means and Standard Deviations of Percentage Instructions Leading to an Aggressive Episode by Condition for Each Participant.
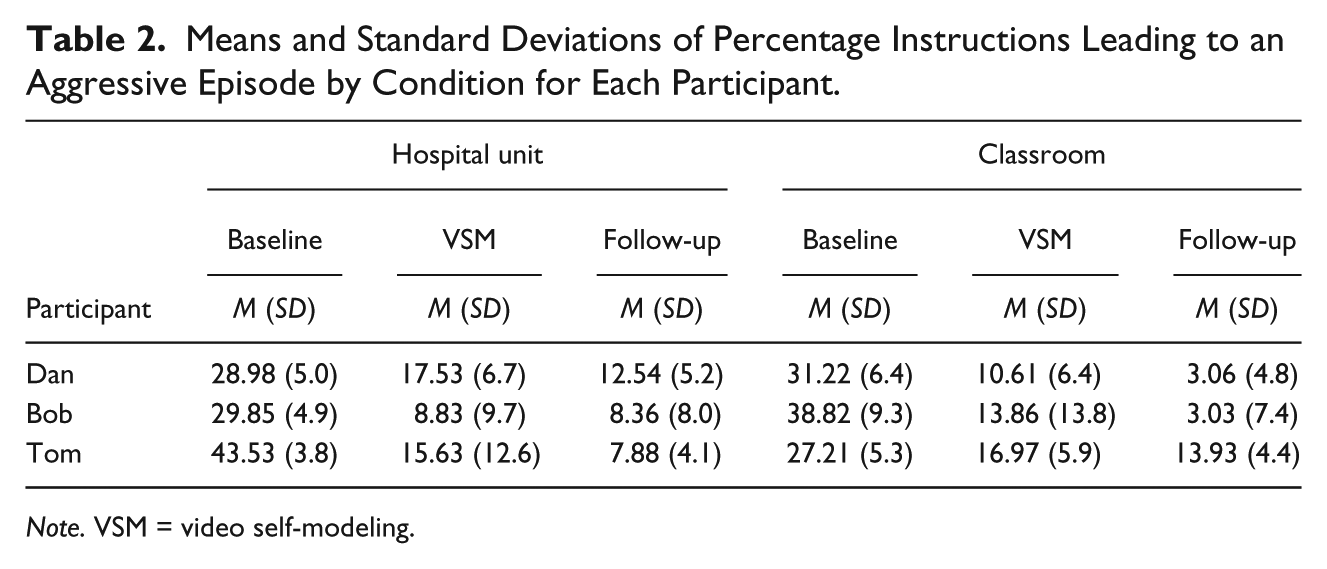
Note. VSM = video self-modeling.
Responses from hospital unit and classroom staff (e.g., classroom teacher, paraprofessionals, psychiatric nurse practitioners, registered nurse, unit direct care staff) on the treatment acceptability questionnaires indicated the VSM intervention was effective and easy to use. Mean scores, using the 5-point Likert-type scale that ranged from 1 (not at all) to 5 (very much), are provided. The intervention was generally successful (M = 4.23) and very easy to implement (M = 5). Staff members reported improved participants’ compliance (M = 4.31), productivity (e.g., chore completion, academics; M = 3.92), and overall behavior (e.g., cooperation, physical and verbal aggression; M = 3.85). Staff also noted a high likelihood of using VSM with other children (M = 4.85) and recommending VSM to other staff (M = 4.85).
Discussion
The primary purpose of the study was to investigate the application of a video modeling intervention for three noncompliant youth in a residential care setting. Specifically, the study incorporated PSR within a VSM intervention targeting compliance with adult instructions. VSM interventions rely on showing children a video of themselves engaging in appropriate behavior (e.g., compliance). Participants in this study displayed improvements in compliance with staff (i.e., classroom teachers and paraprofessionals, nurses, direct care staff) instructions during VSM and follow-up conditions when compared with baseline levels. In addition, participants displayed improvements in the frequency of aggressive incidents following an instruction during VSM and follow-up conditions when compared with baseline levels. Improvements were noted both on the hospital unit and in the classroom for all three participants. The results add to the growing body of research, suggesting VSM interventions can be effective for youth who exhibit problematic behavior. Perhaps most significant is this study’s finding that the percentage of compliance for two participants (i.e., Dan, Bob) did not change significantly after the removal of the intervention (i.e., follow-up condition) when compared with baseline levels. For the third participant (i.e., Tom), a slight decrease in the percentage of compliance was noted between the VSM and follow-up conditions in the classroom but not on the hospital unit. Furthermore, the percentage of instructions leading to an aggressive episode was lowest during the follow-up condition for all participants in both settings suggesting the intervention was not only effective at improving behavior following an adult instruction but may have contributed to continued improvements even after the intervention was removed.
Researchers have interpreted the success of VSM through a variety of conceptual lenses, including cognitive, social-cognitive, and behavioral perspectives (Dowrick, 1999; Kehle, Bray, Margiano, Theodore, & Zhou, 2002; Nikopoulos & Keenan, 2004). Kehle et al. (2002) speculated that watching edited self-modeling videos that depict positive and efficacious behavior may alter the viewer’s memories of their past behaviors. That is, their memories of past maladaptive behaviors may be replaced by memories of exemplary behaviors. Dowrick (1999) asserted that children not only acquire skills by observing behaviors depicted on the video but also increase self-efficacy through the viewing of their own efficacious behavior. Most salient to the present study, Nikopoulos and Keenan (2004) speculated that watching certain activities or behaviors on video serves as an establishing operation for young children, thereby increasing the reinforcing properties of the activities and behaviors featured on the video and making the behavior more likely to occur. After watching themselves comply with adult instructions, children in the present study may have viewed compliant behavior as more desirable or reinforcing. Watching behavior on video may also serve to “prime” the behavior, thereby preparing the child to think about the behavior, or to perform the behavior featured in the video.
The results are encouraging for several additional reasons. First, VSM interventions targeting noncompliance can have a positive effect on other problem behaviors such as aggression. In the current study, decreases in the frequency of aggressive incidents following an instruction were noted across all participants and settings despite the intervention’s primary target being compliance with adult instructions. Furthermore, staff reported improvements in compliance as well as chore completion, academics, and physical and verbal aggression. These findings are consistent with other empirical research suggesting improving a child’s compliance with adult instructions might simultaneously reduce problem behaviors in other domains. For example, Wells, Forehand, and Griest (1980) found that a parent training program targeting noncompliance not only effectively reduced noncompliance but also reduced problem behaviors that were not targeted for treatment (e.g., tantrums, physical and verbal aggression). Like parent training, the effects of VSM might generalize to untreated behaviors.
Second, the current study provides much-needed insight regarding the social acceptability of interventions based on VSM procedures. Both classroom and hospital staff found the intervention to be beneficial. Specifically, they believed that the intervention improved compliance, productivity (e.g., chore completion, academics), and overall behavior (e.g., cooperation, physical and verbal aggression). Staff also noted the ease of implementation and indicated a high likelihood of using the intervention with other children. Treatment approaches that have a high degree of social acceptability are needed, as interventions acceptable to practitioners have a higher probability of use compared with less acceptable interventions (Elliott, 1988). These findings are important in that professionals working with youth with emotional and behavioral disorders should implement interventions that are socially acceptable, have a high degree of perceived effectiveness, and are easy to implement.
Finally, the intervention procedure described in the current study is generally considered a proactive treatment. Unlike consequent strategies (e.g., response cost, time-out, and incentive system), proactive treatment approaches do not require the child to engage in the problem behavior before the corrective procedure is implemented. Proactive treatment approaches, such as VSM interventions, are thought to facilitate maintenance because the child is learning a skill or behavior via modeling that will remain with the child after the intervention is withdrawn (Bellini & Akullian, 2007; Dowrick, 1999). Results of the present study are consistent with this finding. Finally, VSM interventions are ideally suited as a skill acquisition strategy to teach the replacement behaviors targeted by the child’s behavior intervention plan.
Limitations and Directions for Future Research
Despite the promising results, this study had several limitations. First, although the percentage of compliance increased for all three participants during the intervention and follow-up conditions when compared with baseline levels, two of the three participants reached 50% compliance with instructions when on the hospital unit and none of the three participants reached 50% compliance when in the classroom. Criteria set for the current study indicated that instructions complied with less than 50% were targeted for intervention suggesting 50% compliance as a goal. On the hospital unit, Dan and Bob’s compliance with more than 50% of instructions during the intervention was sustained during the follow-up phase. However, Tom’s response to the intervention when on the hospital unit was much less pronounced. While Tom’s compliance with instructions increased almost 100% from baseline to intervention and follow-up, it remained rather low. In the classroom, the intervention was successful at increasing compliance with instructions but none of the participants ever reached 50%. While Bob and Dan approached 50% compliance with instructions during the intervention and follow-up conditions, Tom’s percentage of compliance remained low. It might be that all three participants required additional intervention components to increase their percentage of compliance above clinically acceptable levels. The effectiveness of the VSM intervention might have been more pronounced if a simple reward system was added to the VSM procedures. Future research should investigate the effects of including VSM procedures as part of a treatment package for those individuals who do not respond above clinically acceptable levels when exposed to the VSM intervention alone. Future research might also investigate using video clips depicting compliance collected during earlier parts of the interventions as a means of introducing novel material to participants.
Second, the study did not control for the frequency at which different staff delivered instructions across conditions and settings. While the classroom teacher was primarily responsible for issuing instructions in the classroom, the two paraprofessionals gave instructions as well. On the hospital unit, several different direct care staff as well as one or two psychiatric nurse practitioners and one registered nurse issued instructions. Data were not collected to determine whether the participants responded more appropriately to a particular staff member. Related, the study did not control for when instructions were issued during each 1-hr period (i.e., mid-morning independent seatwork period in the classroom, mid-afternoon free time on the hospital unit) across conditions. Because staff members were asked to issue instructions that made sense given the context of the setting, it is not likely they issued instructions randomly across the two 1-hr periods. Finally, there are no data presented indicating staff maintained their typical behavior in response to participants’ compliance or noncompliance during baseline, intervention, or follow-up conditions. Future research on using VSM procedures with noncompliant children should consider investigating the effects different personnel (e.g., teachers, paraprofessionals) or the manner in which instructions are issued (e.g., randomly distributed across sessions) might have on compliance.
Third, inter-rater reliability data were not collected on percentage of instructions leading to an aggressive episode. While all hospital staff members were trained to identify physically or verbally aggressive behavior and enter those data into a patient’s electronic record, nothing can be said of the reliability of those observations or the accuracy at which those data were recorded. Related, only the frequency of aggressive episodes was recorded. Data on the intensity and duration of the aggressive episodes following an instruction were not collected. While the percentage of aggressive episodes decreased for all participants during the intervention and follow-up conditions, conclusions regarding the intensity and duration of those episodes cannot be made.
Fourth, external validity is limited by the size of the sample and setting characteristics. Although this study adds to the growing body of research supporting the effectiveness of VSM, the relatively small sample size makes it difficult to establish the effectiveness of this intervention for a specific population and setting. Furthermore, it is unknown whether the increases in compliance and decreases in aggressive episodes following an instruction would generalize to other participants, settings, or task demands. Finally, data were not collected to assess the intervention’s long-term effectiveness during the follow-up phase. While the follow-up data were promising, future research should consider investigating maintenance of compliance rate and related aggressive episodes improvements beyond 1 or 2 weeks concluding the intervention.
Despite these limitations, empirical evidence reported in this study suggests that a VSM intervention holds promise for professionals looking for evidence-based interventions to implement with noncompliant children. These findings are important for professionals who could benefit from a proactive intervention that has shown to be effective at increasing compliance and has a high degree of social acceptability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.