
Abstract
Tourette syndrome (TS) is marked by the chronic presence of motor and vocal tics that are usually accompanied by aversive sensory experiences called “premonitory urges.” Phenomenological accounts suggest that these urges occur before tics and diminish following their occurrence. This has led some to suggest that tics are negatively reinforced by removal of premonitory urges. This hypothesis has proven difficult to test experimentally, however, due in part to challenges in measuring premonitory urge strength. We tested predictions of the negative reinforcement conceptualization of premonitory urges using novel experimental tactics within the context of the “tic detector” paradigm. We compared tic rates and ratings of premonitory urge strength exhibited by youth with TS or chronic tic disorder under free-to-tic baseline (BL), reinforced tic suppression (RTS), and reinforced tic suppression with escape (RTS + E) conditions. Results were consistent with previous research and hypotheses of the present study. Participants rated the strength of their premonitory urges as higher during RTS conditions than during BL conditions. Within RTS + E conditions, tic rates were higher during escape portions when the contingency supporting tic suppression was inactive than during components where the contingency was active, and ratings of urge strength were higher at the onset of break periods than at the offset. All participants engaged in some level of escape from reinforced suppression during the course of the experiment. Results of this study support the notion that tics may be negatively reinforced by removal of aversive premonitory urges. Future directions for basic and clinical research are discussed.
Chronic tic disorders (CTDs), including Tourette syndrome (TS), are childhood-onset neurobehavioral conditions marked by the presence of multiple motor and/or phonic tics that have been consistently present for one year or longer (American Psychiatric Association, 2013). In addition to the tics, a majority of individuals report the presence of “premonitory urges” immediately prior to ticcing. Patients describe these urges as aversive somatosensory experiences which occur prior to a tic and temporarily diminish as the tic occurs (Bliss, Cohen, & Freedman, 1980; Kane, 1994; Leckman, Walker, & Cohen, 1993; Shapiro, Shapiro, Young, & Feinberg, 1988; Woods, Piacentini, Himle, & Chang, 2005).
Such descriptions of the urge have led some (e.g., Bullen & Hemsley, 1983; Evers & van de Wetering, 1994) to hypothesize that relief from premonitory urges functions as a negative reinforcer central to tic maintenance. Research using patient-report data has been consistent with this negative reinforcement hypothesis. In a survey of adolescents and adults with TS (Leckman et al., 1993), 92% reported their tics were “in response to” premonitory urges. Likewise, in another study of youth with TS (Woods et al., 2005), a large majority of participants noted that after they performed a tic, premonitory urges were reduced, at least temporarily.
Researchers have also evaluated the negative reinforcement hypothesis using controlled laboratory evaluations. Himle, Woods, Conelea, Bauer, and Rice (2007) demonstrated that ratings of urge strength (made every 10 s on a Likert-type scale) were higher during periods of reinforced tic suppression (RTS) than during free-to-tic baseline (BL) conditions. This was interpreted as consistent with the negative reinforcement hypothesis, which would predict that (a) blocking the performance of tics would increase the salience of the urge and (b) urge ratings would be relatively low under BL conditions, in which many tics occur and could reduce urges. However, several laboratory studies (Capriotti, Brandt, Ricketts, Espil, & Woods, 2012; Conelea, Brandt, & Woods, 2011; Specht et al., 2013; Woods, Walther, Bauer, Kemp, & Conelea, 2009) have failed to replicate this finding. Reasons for these failures to replicate are unclear, but one possible reason is that different measures were used to assess urge strength. Himle and colleagues (2007) collected ratings of urge strength every 10 s during experimental conditions, whereas two of the three other studies relied on retrospective reports collected at the end of each 5 to 10 min experimental condition. In addition, the authors of two of these studies (Conelea et al., 2011; Woods et al., 2009) reported that their data were trending toward a replication of the Himle et al. (2007) study and suspected the failure to replicate may have been due to low statistical power. On the whole, experimental evidence may be regarded as partially consistent with the negative reinforcement hypothesis, with the need for further, well-powered replications to provide clarification.
Aside from statistical power, problems exist with respect to how urges are assessed. Currently, no techniques for directly assessing momentary urge strength exist, and no robust biomarker for the phenomenon has been established. Given these barriers, a plausible alternative approach may involve operationalizing urge strength as the rate of an observable response upon which removal of the urge is contingent. Indeed, at least one previous study (Hoogduin, Verdellen, & Cath, 1997) has evaluated premonitory urges within this framework by regarding tic frequency as a proxy for urge strength. Unfortunately, this particular approach does not allow for dissociation of urge phenomena from ticcing itself. In the present study, we aimed to solve this problem using a novel experimental paradigm. This approach involved (a) inducing increased urge strength via reinforcing tic suppression, (b) including an observable behavioral response distinct from ticcing itself that would produce the opportunity to escape from premonitory urges (i.e., it would produce a brief, free-to-tic period), and (c) utilizing a response that could be standardized across groups of patients with tics.
Using this novel measure along with existing measures of the urge, the present study aimed to replicate and extend previous research on the functional role of premonitory urges. We hypothesized that tic rates would be lower during periods in which reinforcement was provided contingent on the nonoccurrence of tics compared with conditions in which no programmed consequences for ticcing were in effect (Hypothesis 1). We also made a number of other predictions based on a negative reinforcement model. We predicted that average urge ratings would be higher during reinforced suppression conditions than during free-to-tic baseline conditions (Hypothesis 2). As an exploratory aim of the present study, we also sought to find patterns in the data that might explain inconsistency in previous findings regarding the negative reinforcement hypothesis. We predicted that tic rates would be higher during free-to-tic breaks in which the participant was allowed to temporarily terminate the reinforced suppression (also known as “escape periods”) than during preceding and subsequent periods in which suppression was reinforced (Hypothesis 3). We hypothesized that ratings of momentary urge strength would be higher at the initiation of the escape-producing response than at the end of the escape interval (Hypothesis 4), and that children who indicated the presence of premonitory urges on the Premonitory Urge for Tics Scale (PUTS; Woods et al., 2005) would engage in some level of the target escape-producing behavior (Hypothesis 5).
Method
Participants
Children were consecutively recruited for a separate treatment study conducted through the Tic Disorders Specialty Clinic at the University of Wisconsin–Milwaukee. The present study occurred as part of an initial visit to the clinic to determine eligibility for the larger treatment study. Inclusion criteria for participation in the present study included (a) age of 8 to 17 years, (b) positive diagnosis of TS or a CTD, (c) Yale Global Tic Severity Scale (YGTSS) total tic score ≥ 13 but ≤ 30 for youth with TS, or ≥ 9 but ≤ 20 for youth with CTD, and (d) IQ ≥ 75 on the Wechsler Abbreviated Scale of Intelligence (The Psychological Corporation, 1999). Exclusion criteria were (a) ≥ 3 sessions of previous behavioral treatment for tics, (b) positive diagnosis of a current or past substance use disorder, psychotic disorder, bipolar disorder, or schizophrenia, (c) report of significant suicidal ideation and/or attempts in the past 3 months, and (d) having begun, ended, or modified a psychiatric medication regimen in the past 4 weeks. In addition, children’s participation was terminated if they did not tic at least once per minute during the initial BL condition of the experiment. Children and their parents (n = 25 dyads) provided consent/assent and began participation. Seven youth did not meet study inclusion/exclusion criteria for the following reasons: one had previously undergone behavior therapy for TS, one did not tic once per minute during the initial BL condition, two did not meet the minimum tic severity requirement, one exceeded the maximum tic severity cutoff, and two did not meet diagnostic criteria for a tic disorder. Of the 18 qualifying participants, one withdrew assent during the preexperimental assessment, another’s participation was terminated due to problem behavior during the experiment, and another consistently failed manipulation checks designed to test for understanding of experimental instructions. These participants were excluded from analyses, resulting in the current sample of 15 participants, whose demographic and diagnostic information appear in Table 1. Of these 15 participants, 13 completed the experiment completely and accurately, one terminated his participation following the fourth of eight experimental conditions due to time constraints, and one’s tic data were lost due to equipment failure. Data from the latter two participants were included in present analyses when possible.
Demographic and Clinical Characteristics of Included Child Participants.
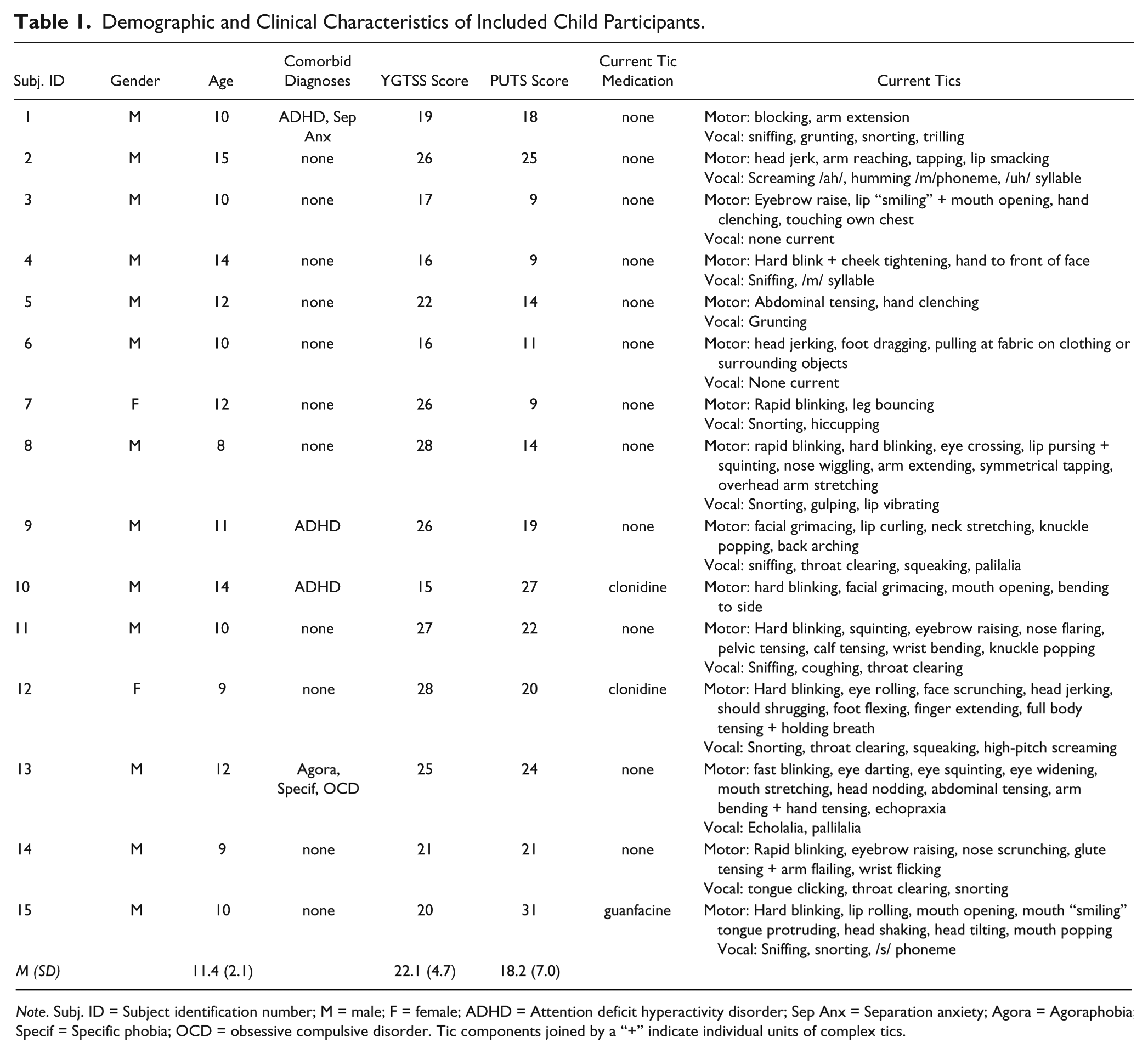
Note. Subj. ID = Subject identification number; M = male; F = female; ADHD = Attention deficit hyperactivity disorder; Sep Anx = Separation anxiety; Agora = Agoraphobia; Specif = Specific phobia; OCD = obsessive compulsive disorder. Tic components joined by a “+” indicate individual units of complex tics.
Measures
YGTSS
The YGTSS is a structured, clinician-rated scale used to assess tic severity. This measure has excellent internal consistency and interrater reliability (Leckman, Riddle, Hardin, & Ort, 1989). Severity is rated for motor and vocal tics along several dimensions (number, frequency, intensity, complexity, and interference; range = 0-5 each), which are summed to yield a total severity score (range = 0-50) and separate motor and vocal severity scores (range = 0-25, each).
Mini Neuropsychiatric Interview for Children (MINI-KID)
The MINI-KID is a brief, psychometrically sound (Sheehan et al., 2010), structured interview that yields full diagnostic information on current Axis I psychiatric disorders.
Wechsler Abbreviated Test of Intelligence (WASI)
The WASI is a brief, psychometrically sound test of intellectual functioning for persons ages 6 to 89 (The Psychological Corporation, 1999). The two-subtest version was used to estimate full-scale IQ.
PUTS
The PUTS is a nine-item, self-report measure in which respondents rate statements describing premonitory urges on a 4-point Likert-type scale anchored by not at all true and very true. Total PUTS scores range from a minimum of 9 to a maximum of 36. The PUTS has demonstrated good internal consistency (α = .81), temporal stability, and convergent and discriminant validity in treatment-seeking samples (Woods et al., 2005).
Urge and Stress Thermometers
The Urge Thermometer and Stress Thermometer are adaptations of the 9-point “feelings thermometer” rating scale designed for measuring self-reports of symptom severity during administration of the Anxiety Disorders Interview Schedule-IV (Silverman & Albano, 1996).
Manipulation checks
Before each condition, the experimenter (M.R.C.) provided the child instructions and described the contingencies programmed for the upcoming condition. The experimenter asked the child to repeat the instructions, identify whether he or she was supposed to stop tics, and, when relevant, state how points were earned, how breaks were taken, and whether it was possible to earn points during breaks. If the child correctly summarized the instructions and contingencies placed on tics for the upcoming condition, the experimenter acknowledged that the response was correct and left the room. If the child answered incorrectly, the experimenter provided the correct answer(s) and prompted the child to answer again. Immediately following the termination of each condition, the experimenter asked the child questions to assess the child’s understanding of and compliance with the instructions for the just-terminated condition. Answers to these questions were recorded, but no feedback was provided regarding their accuracy.
Procedure
Before the main experiment, a trained master’s-level clinician (J.E.T.) administered the YGTSS, WASI, and the MINI-KID and conducted a structured interview to determine if the child met inclusion/exclusion criteria. Qualifying participants were exposed to a series of eight experimental conditions in an ABACABAC modified alternating treatments design, with condition “A” corresponding to BL conditions, “B” to RTS conditions, and “C” to reinforced tic suppression with escape (RTS + E) conditions, during which tic suppression was reinforced, but participants could initiate free-to-tic breaks. Detailed descriptions of conditions are provided below. Participants completed all conditions in a single, continuous session. Prior to the start of the experiment, the experimenter oriented participants to the Urge and Stress thermometers using standardized instructions and anchored examples. After the participant completed this training to criterion, the initial BL condition began.
Immediately prior to each condition, the experimenter read instructions describing the upcoming condition, conducted a pre-session manipulation check, and exited the room. Conditions started shortly (<30 s) thereafter, as signaled by a brief tone. Throughout all conditions, the experimenter monitored the participant via a head-on video stream transmitted through a webcam on top of the monitor of the experimental apparatus. The experimenter recorded tics and urge ratings on a keyboard connected to a computer powering the experimental display. Immediately following the offset of each condition, the experimenter reentered the experimental room, requested global retrospective ratings of stress and urge intensity for the just-terminated condition, and conducted a postsession manipulation check.
BL conditions
Throughout BL conditions, no contingencies were programmed for ticcing. The monitor displayed a black background with the words “TIC DETECTOR ON” in the bottom right corner of the screen. Momentary urge ratings were solicited one s after condition onset and every 30 s thereafter. Participants were instructed to provide the ratings when the screen background turned red and the words “RATE YOUR URGE (0-8)” appeared. Immediately after the participant provided an urge rating, the screen background reverted to black and the rating-prompting text disappeared. At the offset of the condition, the words “TIC DETECTOR OFF” replaced “TIC DETECTOR ON” in the corner of the screen. Initial BL conditions were 10 min in duration and subsequent BL conditions lasted for five min.
RTS conditions
During RTS conditions, the monitor background was blue and text reading “Point Count:” followed by a number indicating the number of points earned in the present condition was displayed in the center of the monitor. Points were said to be exchangeable for money, at a rate of “a few cents each” upon completion of the larger treatment study, which lasted about two months. Points were delivered according to a resetting DRO 10-s schedule of reinforcement: Immediately following each 10-s interval during which no targeted tics occurred, the point total increased by one and a brief tone sounded. When a targeted tic occurred, the 10-s interval reset. Momentary urge ratings were elicited throughout RTS conditions in a manner identical to that of BL conditions, except that the monitor background color changed to green when the prompt to provide a rating appeared. RTS conditions were 10 min in duration.
RTS + E conditions
RTS + E conditions were similar to RTS conditions in terms of programmed reinforcement contingency and monitor display. However, during RTS + E conditions, participants could initiate 10-s “free to tic” time-out periods from the DRO contingency by pressing the spacebar on the keyboard in front of them. Upon pressing the spacebar, an urge rating was elicited, with a visual display identical to that in the RTS condition. Immediately after the participant provided an urge rating, a 10-s break began, during which time the screen was black, and a countdown with the number of seconds remaining in the break was displayed. When the break terminated, the programmed reinforcement contingency resumed, and an urge rating was prompted. RTS + E conditions were to be terminated after 10 min of active DRO time or 15 min of total condition time had elapsed, although the latter never occurred.
Data Collection
During administration of the YGTSS, the participant, his or her parent(s), and the interviewer collaboratively generated a comprehensive list of tics the child had displayed in the past week. These tics were operationally defined and “targeted” in the present study, in that they were recorded by the experimenter, and monetary rewards were contingent on their suppression during RTS and RTS + E conditions. Other apparent tics or repetitive behaviors were not entered into the dependent variable of tic occurrence, nor did they affect the reinforcement contingency.
The experimenter served as the primary rater of tic frequency and urge ratings, and the computer program used to run the experiment automatically produced a record of the observations. To assess interobserver agreement (IOA), trained research assistants, blind to study hypotheses, reviewed videorecordings of experimental conditions and recorded the occurrence of targeted tics. Coders rated all experimental conditions for each of the participants for which video footage was available (N = 10; [67% of all sessions]; five recordings were lost due to equipment failure). To quantify the degree of IOA between the experimenter and the blind coder, tic event records from the experimenter and coder’s observations were grouped into 10-s bins and scored according to a frequency-within-interval method for each bin (Himle et al., 2007). An average IOA score was calculated for each participant. The mean IOA score across participants was 82% (range = 69%-85%). Urge ratings were recorded by a blind coder, different from the coder who recorded tics. IOA for urge ratings was computed by calculating the percentage of ratings for which the experimenter and coder recorded the same number. Mean IOA for urges was 97% (range = 90%-100%).
Independent Variable Integrity
Programmed contingencies
Due to the use of an automated system to deliver reinforcers, programmed contingencies were implemented with perfect integrity. Review of experimental records indicated that 100% of reinforcers were delivered within 1 s of their scheduled time.
Rules describing contingencies
Participants’ understanding of the rules regarding the contingencies in effect was assessed during the manipulation check procedure described above. Fourteen of the 15 included participants answered all manipulation check questions for each condition correctly on the first attempt. During the post-condition manipulation checks for the second RTS and RTS + E conditions, one participant stated that the instructions were not to suppress tics but that he was not attempting to do so; data from these two conditions were excluded.
Results
To test Hypothesis 1, that tic rates would be lower during periods of reinforced suppression than during free-to-tic BLs, we compared participants’ mean tic rates (in tics per minute) during RTS conditions to those during BL conditions using a paired-samples t test. Tic rates were significantly lower (t13 = 4.9, p < .001, Cohen’s d = 1.5) during RTS conditions (M = 2.2, SD = 2.0) than during BL conditions (M = 5.5, SD = 2.3). In addition, tic rates were significantly lower (t13 = 6.9, p < .001, d = 1.5) during the active components (i.e., not during breaks) of RTS + E conditions (M = 1.5, SD = 1.0) than during BL conditions. Visual analysis of individual participant data (Figure 1) indicated that these patterns were also reflected on a within-subject level in a majority of participants

Tic rates and average urge ratings across conditions for individual participants. Bars depict tic rates, with filled bars corresponding to BL conditions and open bars representing periods of RTS (the entirety of RTS conditions and the portions of the RTS + E conditions when the reinforcement contingency was active). Data points depict average urge ratings, with filled circles reflecting BL conditions and open squares representing RTS conditions.
To test Hypothesis 2, that average urge ratings would be higher during RTS conditions than during BL conditions, we compared mean in-session urge ratings during RTS conditions to those during BL conditions using a paired-samples t test. Urge ratings were significantly higher (t14 = 2.1, p = .028, d = .44) during RTS conditions (M = 3.4, SD = 2.7) than during BL conditions (M = 2.4, SD = 1.8).
To test Hypothesis 3, that tic rates would be higher during escape components (i.e., breaks) of RTS + E conditions than during components of RTS + E conditions in which the programmed reinforcement contingency was active, we compared average tic rates from these two components of RTS + E conditions using a paired-samples t test. During RTS + E conditions, tic rates were significantly higher (t13 = 3.2, p = .004, d = 1.2) during breaks (M = 33.3, SD = 36.9) than during active components (M = 1.5, SD = 1.0).
We used a two-step approach to test Hypothesis 4, that ratings of momentary urge strength would be higher at the initiation of breaks during RTS + E condition than at the end of breaks. First, we first computed change scores for urge ratings at each break by subtracting the rating at break initiation from the rating at break termination, such that a negative score indicated a change in the hypothesized direction. Then, we submitted participants’ average change scores to a one-sample t test against a value of 0, reflecting a null hypothesis that ratings would remain constant across the two time points. The mean change score across all participants was −1.75 (SD = 1.69), which was significantly lower than the null mean of 0 (t14 = −3.86, p = .001, d = 2.1).
To test Hypothesis 5, that participants who indicated the presence of premonitory urges on the PUTS would initiate at least one break during RTS + E conditions, we examined count data describing the number of breaks each participant took in each RTS + E condition. During the first RTS + E condition, all participants took at least one break (M = 3.4, SD = 2.5, range = 1-8). During the second RTS + E condition, seven of 13 participants for which data were available (54%) initiated at least one break and the other six (46%) initiated no breaks. Excluding the two participants who had a PUTS score of 9, reflecting no report of any premonitory urge experience, 55% (6/11) initiated at least one break in the second RTS + E condition, and 45% (5/11) did not. No participant pressed the spacebar during BL or RTS conditions. A paired-samples t test revealed that, among participants who completed both RTS + E conditions, the number of breaks taken in the second RTS + E condition (M = 1.8, SD = 2.1) was significantly lower (t12 = −3.43, p = .003, d = .63) than the number initiated during the first RTS + E condition (M = 3.3, SD = 2.5).
Exploratory Analyses
We also conducted exploratory analyses to examine factors that may explain the mixed findings in previous research examining ratings of urge strength under RTS and BL conditions. We examined the implications of potential order effects by conducting “local” analyses, (in which urge ratings during each RTS condition were compared with those during the BL condition immediately preceding it) and comparing these to the more molar analyses used to test Hypothesis 2, in which data from each iteration of each condition type were averaged and submitted to analysis. A paired-samples t test revealed a significant increase (t13 = 2.00, p = .04, d = .35) in average urge ratings from the first BL condition (M = 2.9, SD = 1.8) to the first RTS condition (M = 3.7, SD = 2.7). In contrast, the increase from the third BL condition (M = 2.1, SD = 1.9) to the second RTS condition (M = 2.7, SD = 2.7) did not reach significance (t11 = 1.0, p = .17, d = .26).
We also explored correlations between the average number of breaks taken during RTS + E conditions and dimensions of tic severity, premonitory urge severity, estimated IQ scores, and age. Results of these analyses are displayed in Table 2. The average number of breaks taken correlated significantly with participants’ age (r14 = .54, p = .04). For analyses of correlations with the PUTS, we removed one apparent outlier, who had a PUTS score of 31, which was 2.1 standard deviations above the mean reported by Woods et al. (2005). Figure 2 shows a scatterplot of average number of breaks taken against PUTS scores. With the outlying participant removed from the analysis, PUTS scores were significantly correlated with average number of breaks taken (r13 = .63, p = .01) and the number of breaks taken in the second RTS + E condition (r11 = .69, p = .02); the correlation between the PUTS and the number of breaks taken in the first RTS + E condition was marginally significant (r13 = .48, p = .09). When the apparent outlier was included, the correlations between the PUTS and each index of break-taking weakened, such that they did not reach significance (see Table 2).
Pearson Product Moment Correlation Coefficients for Relationships Among Break Taking and Demographic and Clinical Variables.
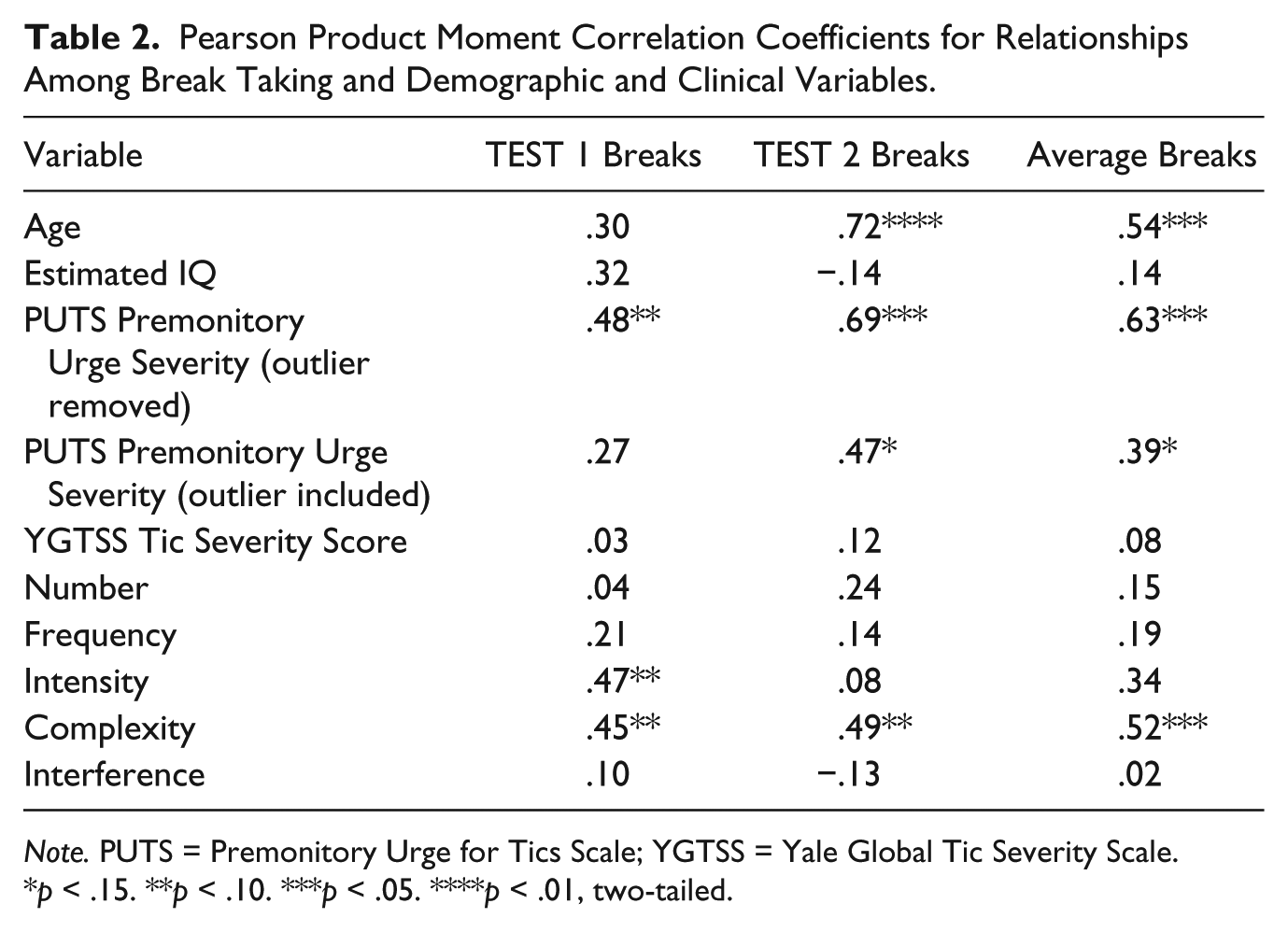
Note. PUTS = Premonitory Urge for Tics Scale; YGTSS = Yale Global Tic Severity Scale.
p < .15. **p < .10. ***p < .05. ****p < .01, two-tailed.
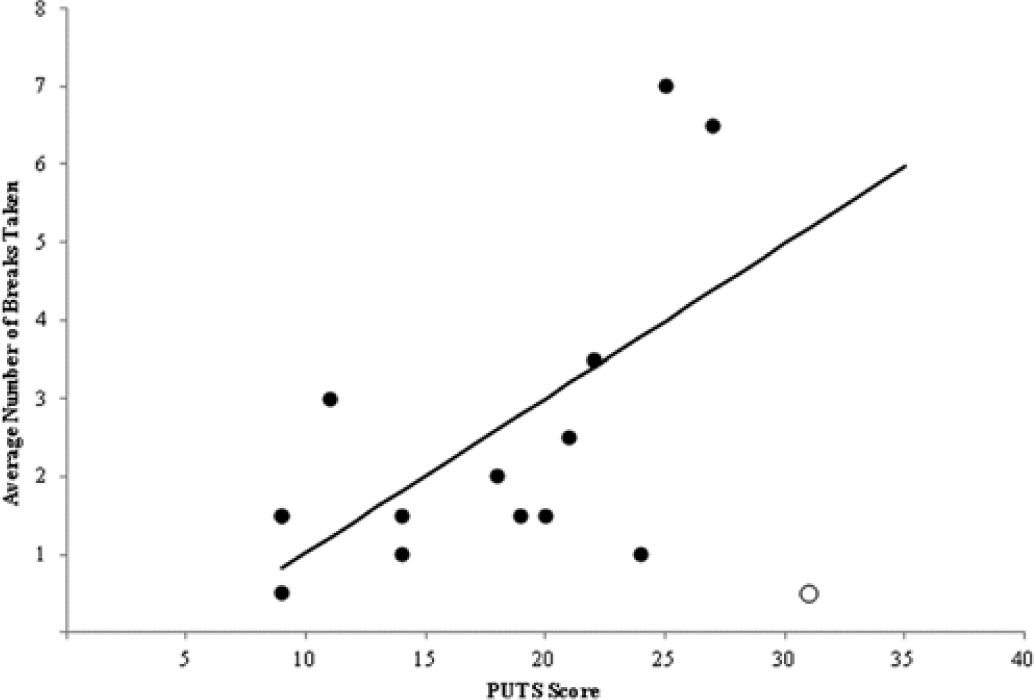
Scatterplot of average number of breaks taken in RTS + E conditions against PUTS scores.
Discussion
Previous research has suggested indirectly that tics may be negatively reinforced by removal of premonitory urges. This study sought to investigate this possibility more directly using a controlled experimental approach. Data were consistent with all five a priori hypotheses. Tic rates were lower during reinforced suppression conditions than during free-to-tic BLs (Hypothesis 1), while ratings of premonitory urge strength were higher during periods of RTS than free-to-tic baselines (Hypothesis 2). As proposed in Hypothesis 3, tic rates were found to be higher during the escape portions of RTS + E conditions compared with “active” portions of those conditions when a contingency supporting tic suppression was in place. In addition, within the RTS + E condition, urge ratings decreased from break onset to break offset, as predicted in Hypothesis 4. Finally, all participants who endorsed the presence of premonitory urges on the PUTS engaged in some level of break taking during RTS + E conditions, consistent with Hypothesis 5.
This pattern of results provides the strongest evidence to date in favor of the negative reinforcement hypothesis. Findings consistent with Hypotheses 2 to 4 suggest that tic rate covaried inversely with premonitory urge strength. Furthermore, the data suggest that the opportunity to experience such a reduction during an extended period of tic suppression functions as a reinforcer, in that it maintained a behavioral response (i.e., spacebar pressing; Hypothesis 5). Qualitative observations argued against alternative explanations for why access to breaks might have functioned as a reinforcer; during breaks, children remained seated in front of the experimental apparatus and did not access other potentially reinforcing materials (e.g., food, toys). Although further investigation could more directly rule out such alternative explanations, the present data are highly consistent with the negative reinforcement hypothesis.
This study clarified the functional role of premonitory urges in tic expression, and its findings were consistent with existing clinical conceptualizations of TS (e.g., Bullen & Hemsley, 1983; Evers & van de Wetering, 1994; Verdellen, Keijsers, Cath, & Hoogduin, 2004; Woods et al., 2008). These perspectives hold that producing decreases in the severity of premonitory urges and/or teaching patients a new way to respond to the occurrence of the urge is a key mechanism of change in behavioral interventions for TS. Future research could focus on the extent to which decreases in premonitory urge severity mediate treatment-induced symptom reduction in TS.
In addition to supporting this negative reinforcement hypothesis, the present study clarified possible methodological issues that may have led to contradictory findings in this area. Two possible reasons have been purported for these failures to replicate Himle and colleagues’ (2007) study: low statistical power (Woods et al., 2009) and lack of sensitivity of global, retrospective ratings of urge strength (Conelea et al., 2011). In the current study, the possible problem of low statistical power was addressed by using a larger sample size than had been used in previous studies. Although the current sample size was still relatively small, a post hoc power analysis showed that, for the main statistical tests used in the present study (one-tailed paired-samples t tests with α = .05), our study was powered to detect a large effect size (d = .8) with a power of .90 and a medium effect size (d = .5) with a power of .58.
This study contributes to the literature on tic expression and suppression in several other areas. First, these data replicate previous findings that providing monetary rewards for tic-free intervals reduces tics to sub-baseline rates; moreover, this study extends that finding to include arrangements where an escape contingency is in place. Beyond its basic significance as a systematic replication of earlier work, this finding may also have translational implications. This could inform development of function-based clinical interventions for tics, in that the results of the present study suggest that allowing individuals to self-initiate brief breaks from tic suppression does not necessarily disrupt suppression abilities.
Second, exploratory analyses suggested that the magnitude of suppression-induced increases in urge strength diminished with repeated exposure to the tic suppression paradigm. Previous studies failing to find a significant difference in this area may have been influenced by these effects, as they combined data from all baseline and suppression conditions before running analyses. We suggest that future research take these order effects into account when planning and interpreting analyses of data. This finding also may have clinical implications. Efficacious behavioral therapies, such as habit reversal training (Azrin & Nunn, 1973) and Comprehensive Behavioral Intervention for Tics (Woods et al., 2008), instruct patients to practice suppressing tics by performing a “competing response” that is physically incompatible with the target tic. Based on this study, patients may be assured that any premonitory urge-related discomfort associated with initial attempts to suppress tics would be expected to decrease with repeated practice over time. Providing this information to patients at the start of therapy may increase the acceptability of these interventions and/or increase motivation to practice using the competing response.
It is also interesting to note that, just as the magnitude of suppression-induced urge decreased throughout the experiment, the number of breaks taken also decreased from the first RTS + E condition to the second one. These parallel findings may suggest that, as the magnitude of suppression-induced increases in urge strength lessen, so does the motivation to escape from premonitory urges. In addition, results of this study show different patterns of correlation with tic and urge severity for the number of breaks taken in the first and second RTS + E conditions. This suggests that initial motivation to escape from premonitory urges (represented by breaks during the first RTS + E condition) and persistence of this motivation with repeated practice of tic suppression (represented by the number of breaks during the second RTS + E condition) exist as distinct behavioral processes. If viewed as a treatment analogue, this finding suggests that patients may require less frequent use of some tic-specific accommodations (e.g., the ability to self-initiate breaks) as they gain experiencing in suppressing their tics using competing responses. Conversely, if a patient shows increased capacity for tic suppression as treatment progresses, but continues to use break-based accommodations frequently, clinicians may then consider other factors that could be contributing to this (e.g., social anxiety about non-tic themes, skill deficits that establish the task from which the patient is taking a break aversive).
Fourth, the paradigm used in RTS + E conditions in the present study may also inform future research on the behavioral and neural mechanisms involved in tic suppression and expression. Neuroimaging research surrounding this topic has proven difficult, as tic expression involves neural activation patterns associated with both movement and the premonitory urge experience (Kompoliti, 2011). Researchers have attempted to overcome this problem using subtractive methods (i.e., comparing patterns of activation during simulated and naturally occurring tics, with the nonoverlapping activation being interpreted as subserving the premonitory urge; Peterson et al., 1998) or time-course analysis, in which signal changes in the interval immediately preceding a tic is interpreted as relating to the urge experience (Wang et al., 2011). These methods have shed some light on potential correlates of the urge but have not produced highly convergent results across studies. The paradigm employed in the present study may be helpful in future research, as it allows for isolation of relatively increased periods of urge strength (i.e., at break initiation) that are not necessarily time-locked with tics themselves.
In addition to its potential utility in experimental psychopathology research, this break-taking paradigm could generate novel indices of premonitory urge severity that would be useful in clinical research. Currently, the PUTS is the only empirically validated measure of premonitory urge severity. Despite its relatively strong psychometric properties (Woods et al., 2005), it is limited in that it is relatively insensitive to change and does not demonstrate strong construct validity in children 10 and younger (Woods et al., 2005). In the present study, the number of breaks taken in RTS + E conditions showed promising psychometric properties as a measure of urge severity; it demonstrated convergent validity in that it correlated positively with PUTS scores and tic complexity (as does the PUTS; Woods et al., 2005) and discriminant validity in that it did not correlate significantly with overall tic severity or IQ. If future research were to establish the validity of a behavioral measure of urge based on this paradigm, this measure could be quite useful in examining mechanisms of change in TS treatment.
In summary, this study provides evidence suggesting that temporary removal of premonitory urges functions as a negative reinforcer that maintains tics in youth with TS. Further investigation is needed to identify biological and environmental factors that contribute to the formation and maintenance of this negative reinforcement process. Ultimately, research in this area is likely to generate important information about factors involved in tic suppression and should inform the development of integrated models of tic disorders.
Footnotes
Acknowledgements
The authors would like to thank Christopher Bauer, Rachel Johnson, and Derek Spaeth for their assistance with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by a grant from the Tourette Syndrome Association awarded to Han-Joo Lee.