
Abstract
Negative thoughts, experienced by 80% to 99% of the non-clinical population, have been linked to the development of psychopathology. The current study aimed to compare a cognitive restructuring and cognitive defusion technique for coping with a personally relevant negative thought. Over a 5-day period, participants used either a restructuring, defusion, or control strategy to manage a negative thought. Pre- and post-intervention participants reported (a) believability of the thought, (b) discomfort associated with the thought, (c) negativity associated with the thought, and (d) willingness to experience the thought. Daily online questionnaires assessing the total frequency of negative thought intrusions and their level of willingness to experience the negative thought were also used. Also, 10 positive and negative self-statements were rated on the same scales, and self-report measures of mood and psychological flexibility were completed. Findings indicated that defusion lowered believability, increased comfort and willingness to have the target thought, and increased positive affect significantly more than the control and cognitive restructuring. Within groups, cognitive restructuring also made significant gains in target thought discomfort, negativity, and “willingness to have” in the same direction as defusion but the no-instruction control did not. Negative thought frequency was reduced in the defusion group, maintained in the restructuring group, and increased in the no-instruction control group. Similar trends emerged from the secondary outcome measures, that is, the effects of the strategies on the positive and negative self-statements. The current findings support the efficacy of using defusion as a strategy for managing negative thoughts.
Keywords
Introduction
Intrusive negative thoughts are experienced by 80% to 99% of the non-clinical population (Belloch, Morillo, Lucero, Cabedo, & Carrió, 2004) and can be defined as “any distinct, identifiable cognitive event that is unwanted, unintended, and recurrent. It interrupts the flow of thought, interferes in task performance, is associated with negative affect, and is difficult to control” (Clark & Rhyno, 2005, p. 4). When intensified, it is likely that intrusive thoughts play a role in the development of psychopathology (Clark & Rhyno, 2005). The commonality of negative thoughts as well as the link to more serious mental health problems makes even subclinical negative thoughts interesting as targets for brief psychological interventions.
One therapeutic approach shown to be effective for a range of psychological difficulties is cognitive-behavior therapy (CBT; Butler, Chapman, Forman, & Beck, 2006). Within CBT, techniques designed to address negative or faulty thinking are referred to as cognitive restructuring (e.g., A. T. Beck, 1979; J. S. Beck & Beck, 2011). Such techniques are based on the premise that changing the way clients think will change their emotions and behavior (Clark & Beck, 2011). Besides the effect of changing the way they think, Beck suggested that “one of the central advantages of [cognitive restructuring] techniques is that the patient learns to ‘distance’ himself from the thoughts; that is, he begins to view his thoughts as psychological events” (1979, p. 157, content in brackets added). Common cognitive restructuring techniques include challenging the truthfulness of a thought by looking at evidence for and against the thought, identifying thinking errors the thought exemplifies, and developing alternative thoughts that more realistically reflect their experience (Arch & Craske, 2008).
An alternative to the cognitive restructuring model in CBT comes from acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999). ACT comes from the contextual wing of behavior analysis (e.g., Hayes, 2015) and is related to relational frame theory (RFT; Hayes, Barnes-Holmes, & Roche, 2001); a behavioral account of language and cognition. This gives ACT an approach to cognition as a behavior among other behaviors, albeit one that can only be observed by the individual doing the thinking. Behavior cannot be said to cause behavior, but it may have a controlling effect on behaviors in certain contexts (e.g., Hayes & Brownstein, 1986). Thus, ACT strives to create a context, wherein the person can become aware of his or her private verbal behavior (or cognition) itself. The process that makes one thus aware is called cognitive defusion or simply defusion. Defusion involves teaching individuals to view their thoughts as thoughts rather than considering them as having literal meaning (Healy et al., 2010). Therefore, while restructuring aims to challenge negative thoughts and find evidence against them (J. S. Beck & Beck, 2011), defusion does not attempt to control or change unwanted thoughts in form or frequency. Instead, it trains individuals to change their relationship to their thoughts, to view them without the need to dispute or challenge them to change overt behavior. The most common exercise used in defusion studies is the “word repetition technique,” first developed by Titchener (1916). This involves repeating a word until its semantic meaning is no longer dominant. When “defused,” the client will notice a lower attachment to the literal meaning of an unwanted thought, thereby making it less believable (e.g., Masuda, Hayes, Sackett, & Twohig, 2004).
More recently, a number of studies have demonstrated the efficacy of defusion with non-clinical populations (see De Young, Lavender, Washington, Looby, & Anderson, 2010; Hinton & Gaynor, 2010; Hooper & McHugh, 2013; Hooper, Sandoz, Ashton, Clarke, & McHugh, 2012; Masuda, Feinstein, Wendell, & Sheehan, 2010; Masuda, Twohig, et al., 2010), suggesting that it may be a plausible alternative technique to restructuring in the management of negative self-referential thoughts.
One such study by Healy et al. (2010) instructed three groups of participants that a defusion technique (to add a prefix of “I am having the thought that” in front of a negative thought) would either (a) decrease, (b) increase, or (c) do nothing about the emotional impact of self-statements. All three groups were then exposed to 10 positive (e.g., “I love life”) and 10 negative self-statements (e.g., “I am a bad person”) on a computer screen reformulated through (a) a defusion lens (e.g., “I am having the thought that I am a bad person”) and, to control for the novelty that the sentence might result in, they were also exposed to (b) an abnormal reformulation (e.g., “I have a wooden chair and I am a bad person”) of the self-statements. They also (c) were shown the self-statements without a prefix. Results indicated that the presentation format, and not the instruction, gave differences in believability, comfort, and willingness. The defused negative statements were rated as more comfortable, and participants were more willing to read and think about them than both the normal and abnormal negative statements. Interestingly, the defused negative statements were also rated as more believable. For the positive statements, it seemed that the abnormal presentation format resulted in lower believability, comfort, and willingness compared with normal but not compared with defusion.
One previous study has directly compared the effectiveness of defusion and restructuring. Deacon, Fawzy, Lickel, and Wolitzky-Taylor (2011) randomly assigned female high scorers on eating disorder and negative body image measures to either a defusion or restructuring exercise. The defusion group was exposed to the word-repetition exercise, whereas the restructuring exercise was adapted from a manual for eating disorders (Fairburn, Marcus, & Wilson, 1993). Each condition comprised of 90 min of technique rationale and training. Participants were required to repeat the strategy on a daily basis for a week. Both conditions showed significant improvements in subjective body image, which generalized from the targeted thought of being fat to self-generated synonyms of fat, such as “lazy.” The results indicated that defusion had an immediate alleviating effect on discomfort when having the thought of being “fat.”
Given the conceptual differences of cognitive restructuring and defusion, the aim of the current experiment was to compare the effectiveness of cognitive restructuring and cognitive defusion interventions in coping with a negative, unwanted thought. As previous research into defusion has focused on laboratory-based experiments (i.e., Healy et al., 2010) or utilized the word-repetition task (i.e., Masuda et al., 2004; Masuda, Price, Anderson, & Wendell, 2010), it was of interest to explore other defusion techniques, such as the one used by Healy et al. (2010), but as an intervention rather than just presenting the resulting statements and in a more naturalistic setting. Pre- and post-intervention measures included (a) the believability of the thought, (b) its associated discomfort, (c) negativity, and (d) participants’ willingness to have the thought. Believability and comfort are commonly used in defusion and cognitive restructuring research (e.g., Deacon et al., 2011) and willingness is synonymous with acceptance in the ACT model (e.g., Hayes, Strosahl, & Wilson, 2012). In the current study, a further dimension of negative-positive was added. This was based on three reasons. The first was that although the statements that were used for generalization came from Healy et al. (2010), the current sample had not rated the statements as positive or negative. Second, according to ACT a thought is only a thought. Any meaning can be related to a thought, so it is plausible that for some people a “positive” self-statement is not positive at all, and the relative positivity or negativity might be related to the other three dimensions as opposed to a mere categorical division. Third, although these four dimensions are potentially interrelated, they might be affected individually. That is, a negative thought is also an uncomfortable one initially and one that one is unwilling to have. This is also a common event in clinical practice where an evaluation is confused with the reaction “Of course I don’t want to think about negative things.” However, at the end of therapy it is possible that although the evaluation remains it is no longer uncomfortable to think of. Finally, the study also aimed to ensure that it reflected the aims of cognitive restructuring to reduce the negativity of faulty automatic thoughts.
Comparative effects on the same 20 positive and negative self-statements that Healy et al. (2010) used were used as a measure of whether the effect of the different techniques impact outside of a chosen target thought. Pre- to post-intervention effects on measures of depression, anxiety, and positive and negative affect were also assessed, while the ACT-specific measure of experiential avoidance (Bond et al., 2011) was included as a process measure. Finally, daily measures of the occurrence of an unwanted thought and participants’ willingness to experience that thought were made. Both restructuring and defusion were predicted to be more effective than a no-instruction control for reducing believability and negativity while also increasing the comfort and willingness to have the target thought. It was also predicted that the two strategies would affect the ratings of two lists of positive and negative self-statements.
Method
Participants and Design
The sample, aged 18 to 72 (M = 26, SD = 10.9), was recruited by opportunity sampling from Swansea University, including both student and community populations (n = 83; 16 males). No compensation, financial or otherwise, was given to participants. Participants were informed that the study explored ways of thinking about negative thoughts. No participants scored above 30, indicating severe depression, on the Beck Depression Inventory–2, (BDI-II; A. T. Beck, Steer, & Brown, 1996). Participants scoring 0 on the BDI-II were excluded from the analysis (n = 1) as this may suggest possible denial or faking of depression (Clark, Crewdson, & Purdon, 2000). Finally, non-comprehension exclusion (n = 11) was based on ratings of 4 or below on believability and willingness measures and 4 or above on comfort and negativity measures as that would have indicated that the selected thought was rated on the opposite end of the spectrum from instructions, for example, positive instead of negative. This left 24 participants in each of the restructuring and defusion groups, and 23 participants in no-instruction control group. The t tests identified no differences between participants or those who were excluded (all ps > .05) except on measures of target thought believability, comfort, and willingness.
The experiment, as illustrated in Figure 1, involved a mixed design with group (defusion, restructuring, and no-instruction control) as the between-subject factor and Time 1 (T1) and Time 4 (T4) measures as the within-subject factor.
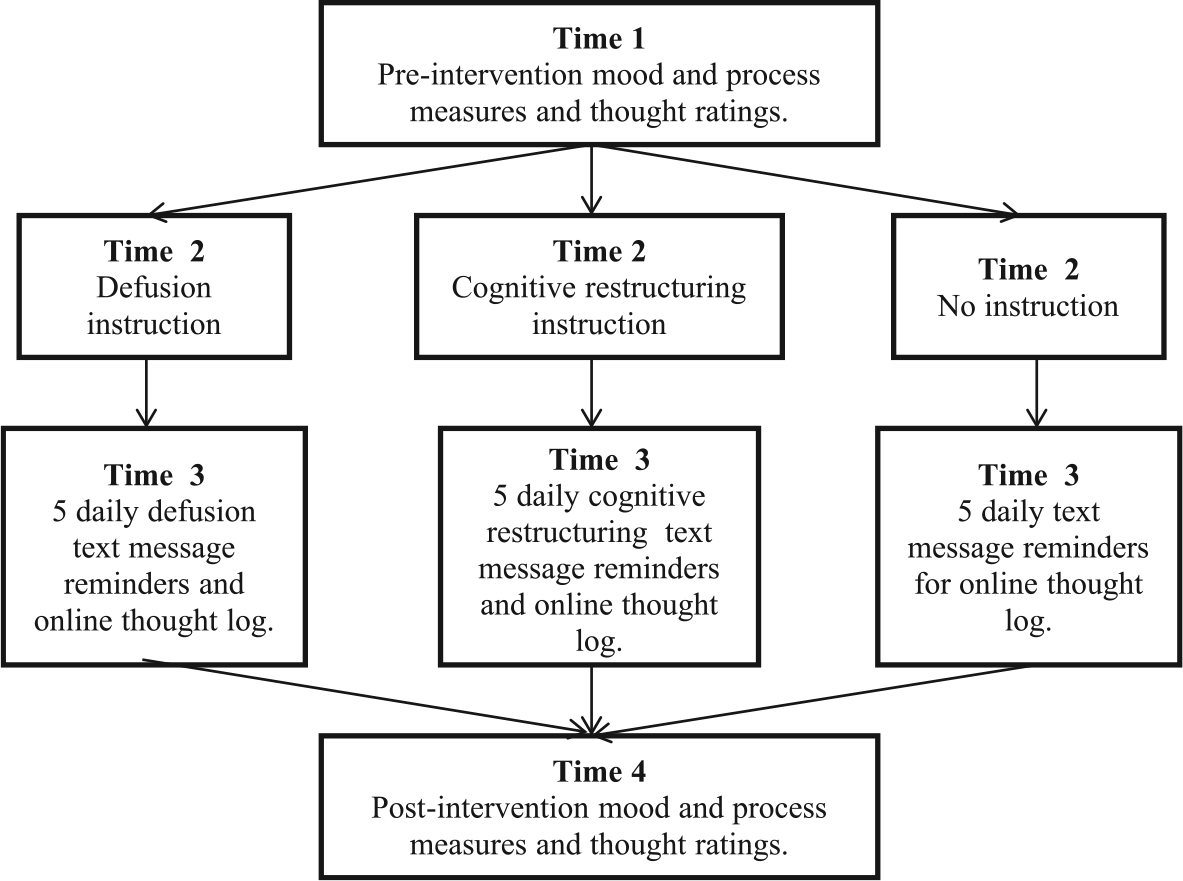
Flowchart of study design.
Measures
Mood
The BDI-II
BDI-II (A. T. Beck et al., 1996) is a 21-item self-report instrument assessing the existence and severity of symptoms of depression listed in the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994). The BDI-II was used as a T1 and T4 measure of subclinical depression. Each of the 21 items corresponds to a symptom of depression and comprises a 4-point scale. Higher scores indicate greater levels of depression. This unidimensional scoring method has been shown to have good construct validity with other common measures in non-clinical samples (Whisman, Perez, & Ramel, 2000). Internal consistency of participants’ BDI-II scores in the current study was high (Cronbach’s alpha = .89).
The State Trait Anxiety Inventory (STAI)
STAI (Spielberger, Gorsuch, Luschene, Vagg, & Jacobs, 1983), a 20-item scale, provides information about a person’s current level of anxiety. The STAI-s was employed as a between-group measure of state anxiety at T1 and T4. Items are scored on a 4-point scale, with higher scores being indicative of higher levels of anxiety. The STAI-s is widely used in research with clinical and student populations (Smith & Lay, 1974). Cronbach’s alpha on the STAI-s for all participants in the current study was .92, indicating a high internal consistency.
The Positive and Negative Affect Schedule (PANAS)
The PANAS (Watson, Clark, & Carey, 1988) has 10 items each measuring Positive Affect (PA) and Negative Affect (NA), each with a 5-point scale. It was implemented as a between-groups current mood measure T1 to T4. Construct validity has been found to be good, and confirmatory factor analysis has yielded two factors corresponding to the PA and NA scales (Crawford & Henry, 2004). Cronbach’s alpha in the current study of participants’ ratings was .89 for the PA scale and .91 for the NA scale.
The Acceptance and Action Questionnaire–II (AAQ-II)
This (Bond et al., 2011; Hayes et al., 2004) comprises seven items, each with a 7-point Likert-type scale. Higher scores indicate greater levels of psychological flexibility and lower levels of experiential avoidance (Hayes, Luoma, Bond, Masuda, & Lillis, 2006). The AAQ-II has been demonstrated to have good construct validity (Bond et al., 2011). The AAQ-II was used as a between-groups measure of psychological flexibility at T1 and T4, the target process of change in ACT that defusion is part of. Participants’ AAQ-II scores in the current study had high Cronbach’s alpha of .92.
Thought measures
Target thought
All participants were instructed to generate a target negative thought: Now pick a negative thought about yourself that would rate as EXTREMELY BELIEVABLE, EXTREMELY NEGATIVE, EXTREMELY UNCOMFORTABLE and that you are EXTREMELY UNWILLING to be thinking. Make sure that it isn’t to do with any physical properties about yourself.
The target negative thought was rated at T1 and T4 using four, 5-point, Likert-type scales adapted from Healy et al. (2010). A score of 1 indicated that the thought was “extremely” “unbelievable,” “uncomfortable,” “positive,” and “unwilling.” A score of 5 indicated “extremely” “believable,” “comfortable,” “negative,” and “willing.” The midpoint of the scale (3) was labeled “neither [ . . . ] or [ . . . ].”
Positive and negative self-statements
Participants rated 10 positive (e.g., “I am loved”) and 10 negative (e.g., “I can’t do anything right”) self-statements (Table 1) using the same scales as used in the target negative thought at T1 and T4. The list of statements was piloted by Healy et al. (2010) with 32 independent raters instructed to rate statements on a 20-point scale ranging from “extremely negative” to “extremely positive” and selecting the 10 most negatively and 10 most positively rated statements. Negative and positive self-statements in the current study displayed high Cronbach’s alphas of .89 and .95, respectively.
The 10 Positive and 10 Negative Self-Statements Used.
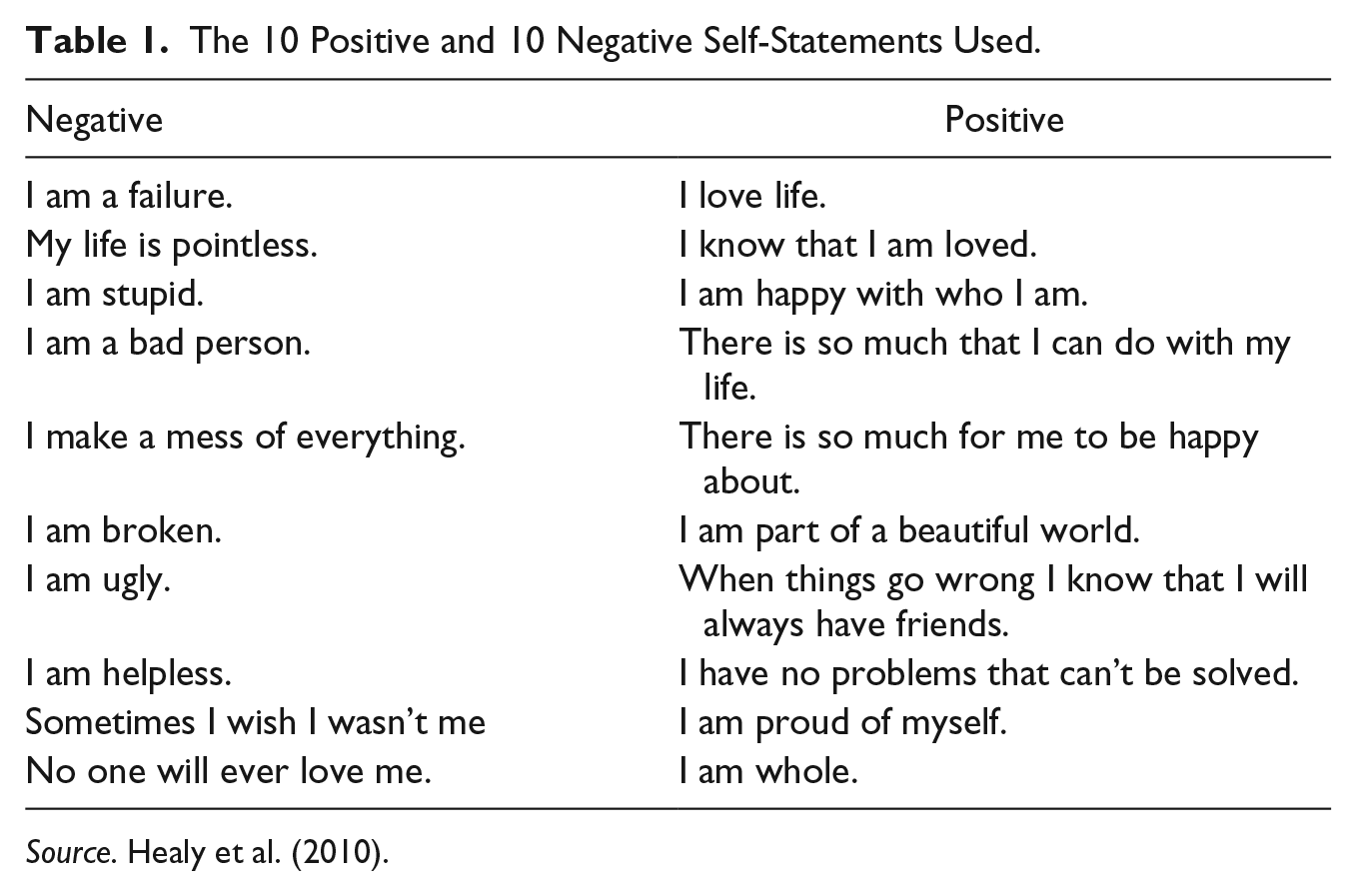
Source. Healy et al. (2010).
Thought log
Participants were provided with a thought log to carry with them to record (a) the occurrences of their self-generated thought in vivo and (b) how willing they were to have the thought. They were instructed to enter each daily tally of occurrence and willingness in an online form over a period of 5 days.
Procedure
Participants were randomly allocated to one of three groups (i.e., cognitive restructuring, defusion, and no-instruction control). At T1 (see Figure 1), participants completed the following questionnaires: BDI-II, STAI, PANAS, and AAQ-2. At this time, they also rated the positive and negative self-statements and generated a target thought which was also rated. Participants received their strategies at Time 2 (T2) when they had completed the questionnaires and rating scales. The researcher placed the instruction, printed on A4 paper, in front of the participant, and then read through the defusion or restructuring intervention out loud and later handed them the paper with the instruction. Participants were encouraged to try the intervention as it was read out to them.
The defusion strategy comprised of three exercises designed to reduce the literal meaning of the target thought. The full instruction was as follows: The way we think can affect our mood. We can often think in a negative way. We can have negative views of ourselves (e.g. “I’m no good”), the world (e.g. “Life has no meaning”) and the future (e.g. “I will always feel this way”). However, imagine we see thoughts in a way that is a little different from what is commonly the way. The ACT perspective is that the mind is a great storyteller. It tells stories of what we notice, who we are and aren’t, of who we’d wish to be and who we must not be. Sometimes they are true in the sense that someone else would agree or that the thought corresponds to some object or event we can see, we often call these thoughts “facts.” But most thoughts are hard to prove. They are evaluations, judgements, attitudes, morals, theories and dreams. What if we stop asking if the thought is “true” or “false” and start asking us if it’s helpful? To do this we need to learn how to take a step back from the thoughts. There are techniques used to enable us to take a step back from our thoughts and see them as what they are, a continuous story told by our mind. Thoughts are words and images strung together. We call the goal of these techniques defusion. This time, let’s try to listen to our experience. Try it out and see what happens!
This technique works like this. So now, pick a negative thought that usually upsets you. Perhaps the type that goes something like “I’m not good enough” or “I’m stupid” Now focus on that thought and really believe it. Now rewind the thought and this time put “I’m having the thought that . . .” in front of it. Notice what happens.
This technique is a little different. Pick a negative thought again. Hold it firmly and try to believe it as much as possible. Now replay the thought again but this time do it to the tune of “happy birthday.” Sing it to yourself and notice what happens.
This is similar to musical thoughts. As the previous methods, you pick a negative thought and once again believe it as firmly as possible. And now let the thought be said by your favorite funny cartoon character, Donald Duck, Bugs Bunny or anyone else you can think of. Let this character’s voice say your thought. Notice again what happens. Hopefully you sensed that the immediacy or the thought was reduced and it was a little easier to hang around with.
Every time you have the target thought in the following week, use the technique of putting “I am having the thought that . . .” before your thought.
The cognitive restructuring strategy presented to the participants can be found below: The way we think can affect our mood. We can often think in a negative way. We can have negative views of ourselves (e.g. “I’m no good”), the world (e.g. “Life has no meaning”) and the future (e.g. “I will always feel this way”). Negative thoughts like these have several characteristics. They are:
They just pop into your head without any effort on your part.
They do not fit all of the facts.
They keep you depressed, make it difficult to change, and stop you from getting what you want out of life.
You accept them as facts, and it does not occur to you to question them.
You do not choose to have them, and they can be very difficult to switch off. Thoughts like these can trap you in a vicious circle. The more down you become, the more negative thoughts you have, and the more you believe them. The more negative thoughts you have, and the more you believe them, the more depressed you become. According to psychologists one way to overcome negative thoughts (also called negative automatic thoughts) is to become aware of your thought errors. All negative thoughts can be categorized into the following thinking errors:
Jumping to the worst possible conclusion.
Thinking in extreme, all-or-nothing, terms.
Thinking things like “always” and “never” overgeneralizing from a isolated event.
Predicting the future instead of seeing what happens.
Jumping to conclusions of what other people are thinking.
Focusing on the negative and ignoring the positive.
Discounting positive information or twisting a positive into a negative.
Putting your whole person into a negative category. “I’m worthless/a failure.”
Listening too much to negative gut feelings instead of looking at objective facts.
Taking events or other peoples’ behavior personally or blaming yourself and overlooking other factors.
Using words like “should,” “ought” or “must” to make rigid rules about myself, the world or other people.
Thinking that something is too difficult or overwhelming, “I can’t stand it.” During the next week, when your target thought occurs, try your best to identify the thinking error behind it in that situation and then follow the steps below:
What evidence exists against this thought? Though we may believe something to be true, this does not necessarily mean that it is. It is often valuable to see if the facts of the situation back up what you are thinking, or whether they contradict what you are thinking. A good question to ask is: “Would other people accept my thoughts as true?”
What do I need to think in order to act and feel differently?
Every time you have the target thought in the following week, use the technique of identifying your thinking error and try to generate an alternative.
It should be noted that these instructions are adaptations of defusion and cognitive restructuring, made to be easily accessible as brief instructions. As such, they are not exhaustive examples of defusion (see Hayes et al., 2012, for more examples) and cognitive restructuring (see O’Donohue & Fisher, 2012, for more examples), or ACT and cognitive therapy as treatment packages. Both strategies were similar in word length (defusion 594 words; cognitive restructuring 560 words) but reading through the instructions was not timed.
After the 5-day period (Time 3; T3), participants returned to the lab (Time 4; T4) and completed all the rating scales completed at T1.
Text Message Reminders
To ensure that participants remembered to log their daily ratings, they were sent text message reminders once every evening that instructed them as follows: “Remember to go to < web page address > and submit your daily ratings.” Participants in the defusion and restructuring groups also received daily text messages reminding them to use the condition strategies. For the restructuring group, this comprised of “Remember to overcome your negative thought by identifying the thinking error and generating an alternative!” For the defusion group, the text message reminder was as follows: “Remember that a thought is just a thought.”
Data Analysis
All analyses were conducted using SPSS Statistics Version 19 for Mac. A MANOVA of all the measures at T1 was conducted to check for significant differences between the groups. Repeated-measures MANOVAs with Time (T1 and T4) being the within-subject variable and group (no-instruction control, cognitive restructuring, and defusion) being the between-subject variable were then conducted separately for the primary outcome variables, the secondary outcome variables, and the mood measures.
To determine if any differences between T1 and T4 scores on individual measures were significant, t tests were used. To reduce the risk of family-wise error, the alpha level was adjusted by Bonferroni correction to .0042 (0.05/12). Within group, effect sizes were calculated using Cohen’s d (Cohen, 1988).
The thought log results were analyzed for significant differences between the first (Day 1) and fifth (Day 5) day scores, using an ANOVA, and then subjected to two repeated-measures MANOVAs with the five daily frequency ratings and seven (T1 rating, five daily ratings, and T4 rating) ratings of willingness to have the target thought as a within-subject variable and group as the between-groups variable. Where there were significant differences at Day 1, a repeated-measures ANCOVA was used. All significant differences from the MANOVA were analyzed using Bonferroni post hoc tests.
Results
Pre-Intervention Analyses
Pre-intervention differences in primary and secondary outcome variables
Mean and standard deviation scores for each of the three conditions at T1 and T4 on the primary (the target thought ratings) and secondary (positive and negative self-statement ratings) outcome measures are presented in Table 2. No significant differences between the groups were found on any of the measures at T1 (all p > .05).
Summary of Pre (T1)- and Post (T4)-Scores on the Thought Ratings for Participants Who Rated x > 4 on Believability and Negativity, as Well as x < 2 on Discomfort and Willingness to Have Target Thought, n = 71.
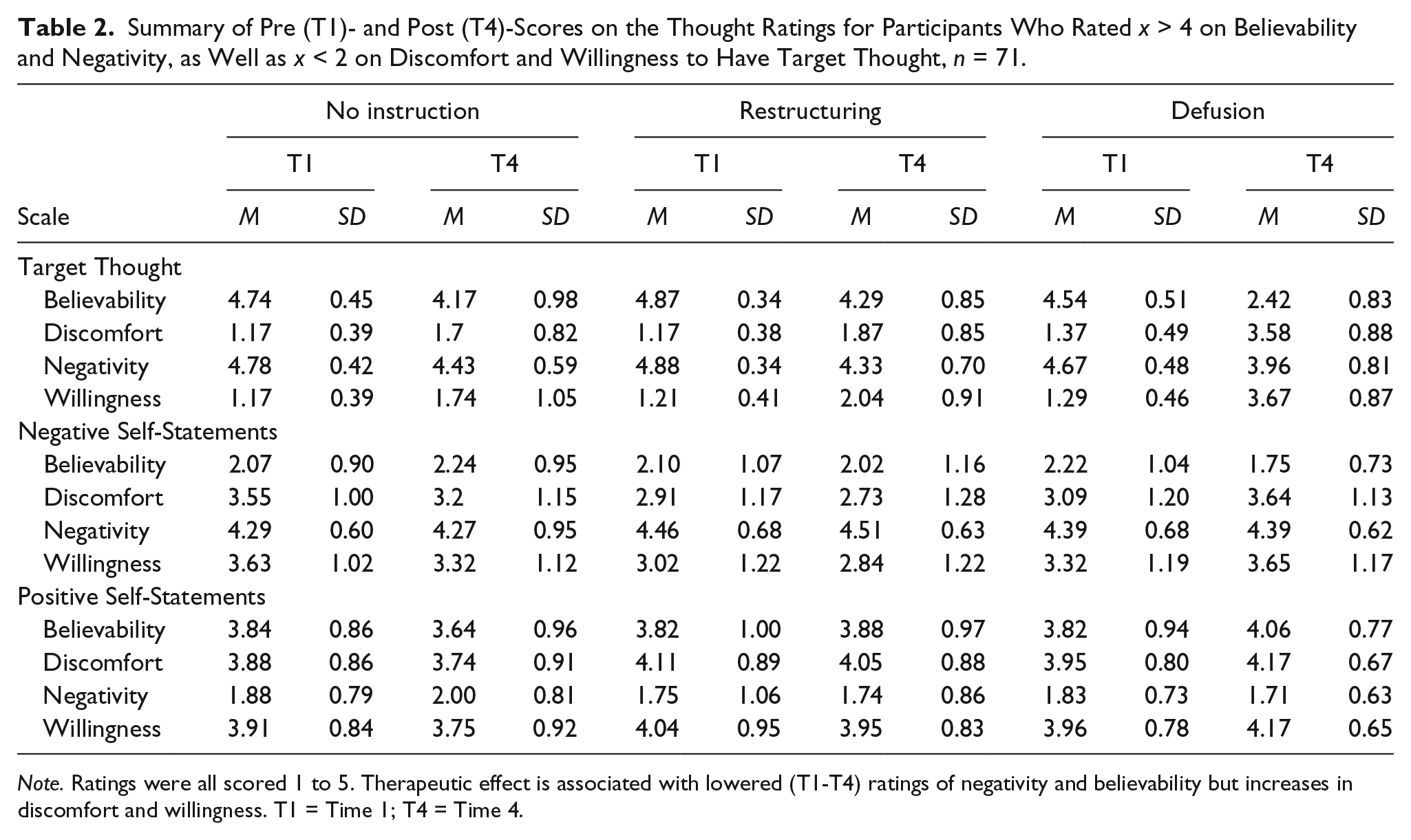
Note. Ratings were all scored 1 to 5. Therapeutic effect is associated with lowered (T1-T4) ratings of negativity and believability but increases in discomfort and willingness. T1 = Time 1; T4 = Time 4.
To assess whether participants evaluated the positive and negative self-statements on opposite ends of the Negative–Positive scale, a correlation analysis of the measures at T1 was conducted. This analysis identified a significant negative correlation (r = −.69, p < .001) between positive and negative self-statements.
Mood measures at T1
Mean and standard deviation scores for each of the three groups at T1 and T4 on the four measures, the BDI-2, STAI-s, and positive and negative PANAS, are presented in Table 3. The results of the T1 analysis indicated no significant differences between the groups on any measure at T1 (all p > .05).
Descriptive Statistics for the Three Groups at T1 and T4 on the Four Mood Measures.
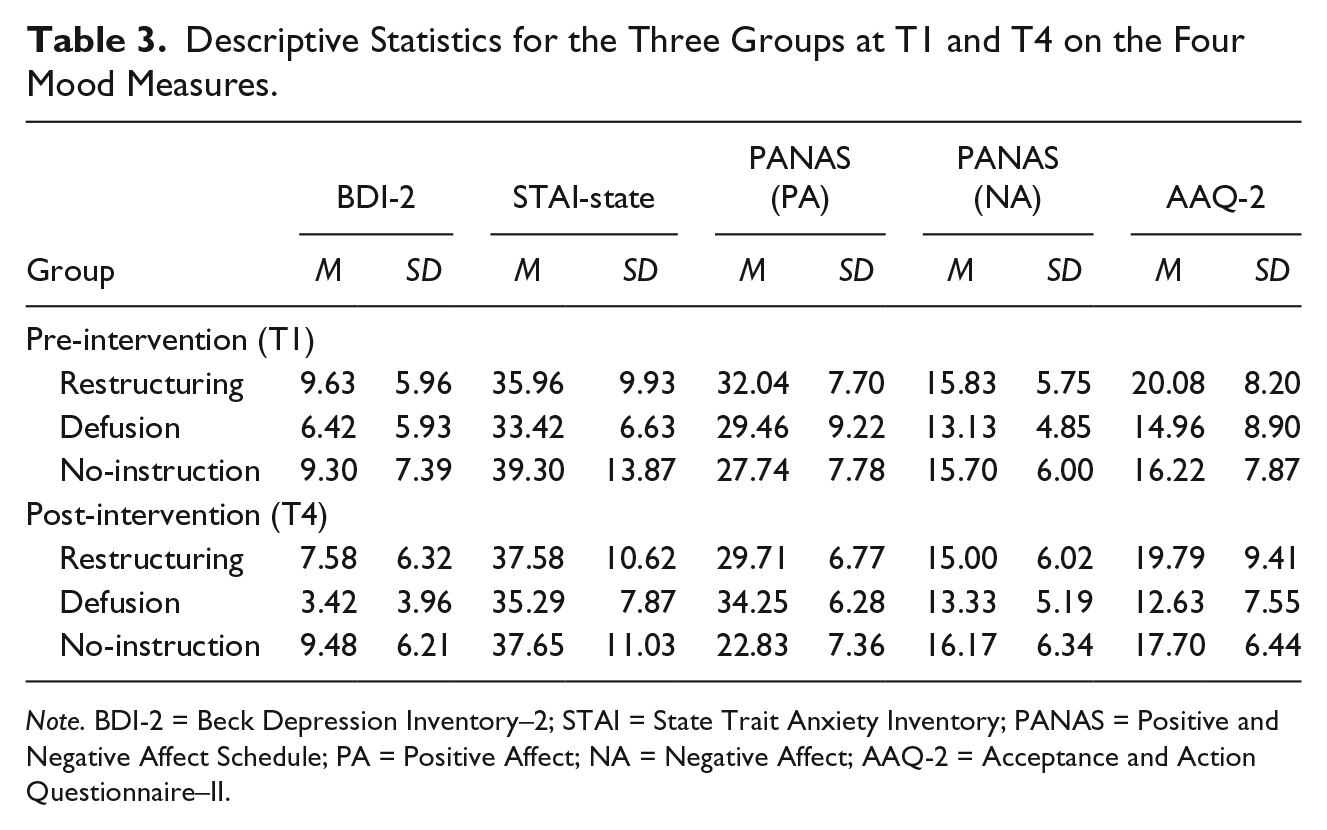
Note. BDI-2 = Beck Depression Inventory–2; STAI = State Trait Anxiety Inventory; PANAS = Positive and Negative Affect Schedule; PA = Positive Affect; NA = Negative Affect; AAQ-2 = Acceptance and Action Questionnaire–II.
Outcome Analysis
Primary outcome analysis
Repeated-measures MANOVA of the scales relating to the target thought showed a significant main effect of time (Wilks’ λ = .30), F(24, 114) = 37.22, p < .001, d = 3.06, as well as main interaction effect of group and time (Wilks’ λ = .48), F(24, 114) = 7.12, p < .001, d = 1.34. When looking specifically at the four scales of believability, discomfort, negativity, and willingness, they followed a similar pattern.
Believability of the target thought
For believability of the target thought, there was a significant effect of both time, F(1, 68) = 95.60, p < .001, d = 2.35, and Time × Group interaction, F(2, 68) = 29.68, p < .001, d = 1.60. Bonferroni-corrected post hoc analysis revealed that the defusion group achieved a significantly greater reduction in the believability of the target thought than both the restructuring and no-instruction groups (both p < .001); no significant difference was found between the restructuring and no-instruction control groups (p > .05).
Within-group analysis through within-subject t tests showed that the defusion group achieved a significant decrease in believability for the target thought, t(23) = −10.99, p < .0001, d = −4.58. The no-instruction control group, t(22) = −2.51, p = .02, d = −1.07, and cognitive restructuring group, t(23) = −3.69, p = .001, d = −1.57, did not show significant decreases in believability.
Discomfort of the target thought
There was a significant effect on discomfort ratings for the target thought of both time. F(1, 68) = 120.49, p < .001, d = 2.67, and Time × Group interaction, F(2, 68) = 26.24, p < .001, d = 1.67. Bonferroni-corrected post hoc analysis again showed that the defusion group lowered the discomfort of the target thought significantly more than both the restructuring and no-instruction groups (both p < .001), whereas no significant difference was found between the restructuring and no-instruction control groups on the measure of discomfort related to the target thought (p = 1.00).The within-group t tests showed that defusion, t(23) = −11.07, p < .0001, d = 4.61, and the cognitive restructuring group, t(23) = −4.30, p < .001, d = −1.83, decreased discomfort significantly, but that the no-instruction control group, t(22) = −2.96, p = .007, d = −1.26, failed to do so.
Negativity of the target thought
For the negativity ratings of the target thought, there was a significant effect of time, F(1, 68) = 29.68, p < .001, d = 1.31, but not for the Time × Group interaction, F(2, 68) = 1.13, p = .33, d = 0.35.
Within-group t tests showed that the defusion, t(23) = 3.33, p = .003, d = 1.39, and the cognitive restructuring group, t(23) = −3.68, p = .001, d = −1.57, both significantly decreased negativity. But the no-instruction control group, t(22) = −2.58, p = .017, d = −1.10, did not significantly reduce negativity of the target thought.
Willingness to have the target thought
The last primary outcome, willingness to have the target thought, again showed a significant effect of both time, F(1, 68) = 114.62, p < .001, d = 3.61, and Time × Group interaction, F(2, 68) = 23.13, p < .001, d = 1.67. Bonferroni-corrected post hoc analysis showed that the defusion group increased participants’ willingness to have the target thought significantly more than both the restructuring and no-instruction groups (both p < .001), whereas no significant difference was found between the restructuring and no-instruction control groups on willingness to have the target thought (p = .87).
Within-group t tests showed that both the defusion group, t(23) = 12.00, p < .0001, d = 5.00, and the cognitive restructuring group significantly increased willingness, t(23) = 4.70, p < .001, d = 2.00, whereas the change in the no-instruction control group, t(22) = 2.42, p = .024, d = 1.03, failed to reach significance.
As mentioned before, the means and standard deviations on target thought ratings are provided in Table 2; this also shows that for believability, discomfort, and willingness the mean in the defusion groups passed over the midpoint (3) on the Likert-type scales into the opposite end of the scales; that is, from believable to unbelievable, from uncomfortable to comfortable, and from unwilling to willing.
Thought log
Adherence to the use of the thought log was high. Only two participants, both in the cognitive restructuring group, failed to use the online report page and had lost their thought log. This might indicate a lower adherence for the cognitive restructuring group but as the participants stated that they had been using the log, this could be an overly strict interpretation.
Daily thought frequency ratings at T1 differed significantly, F(2, 68) = 6.32, p = .03. Due to the significant differences at Day 1, these scores were used as a covariate for a repeated-measures ANCOVA of target thought frequency across the three groups for Days 2 to 5. This analysis did not yield a significant main effect of time, F(1, 69) = 3.10, p = .08, d = 0.46. However, significant between-group, F(2, 68) = 19.44, p < .001, d = 1.60, as well as Time × Group interaction, F(2, 68) = 19.68, p < .001, d = 1.60, differences were found, with large effect sizes. These results are illustrated in Figures 2 and 3, which show that there was an increase in frequency in the no-instruction control, no change in a group level for the cognitive restructuring, and a decrease in frequency for defusion. Bonferroni-adjusted post hoc analysis showed that the no-instruction group increased in the frequency of the target thought significantly more than the brief cognitive restructuring self-help group (p = .01), and the brief defusion self-help group significantly decreased the frequency of the target thought significantly more than both the no-instruction control group (p < .01) and the brief cognitive restructuring self-help group (p = .04).
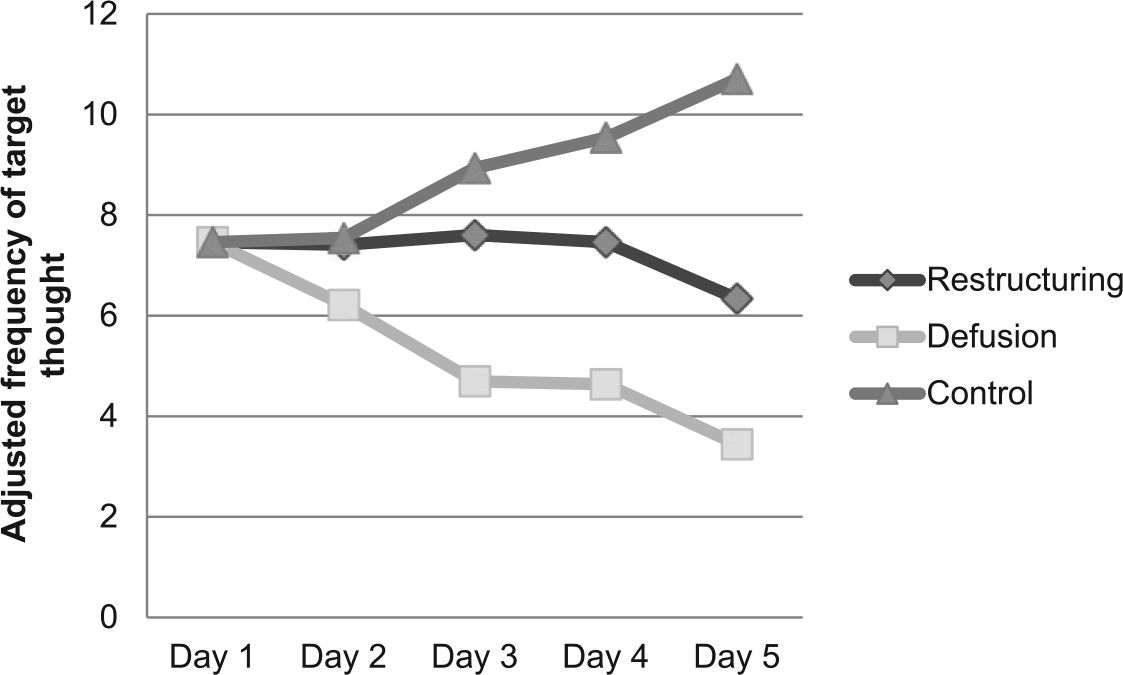
Adjusted frequency of the target thought for the three different groups across the 5 days (T3) between instruction (T2) and post-measure (T4).
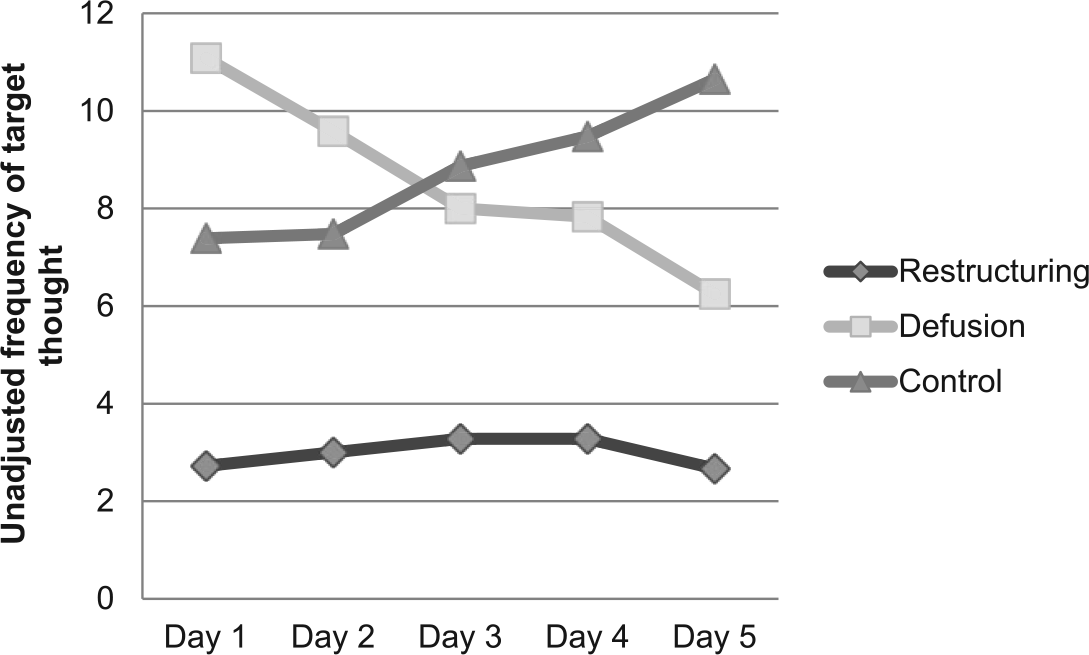
Frequency of the target thought for the three different groups across the 5 days (T3) between instruction (T2) and post-measure (T4)
Pre-experimental (T1) ratings for willingness to have the target thought did not vary significantly between conditions, F(2, 68) = 0.57, p = .57. The repeated-measures ANOVA of the 7 willingness rating time points resulted in a significant main effect of time and group (Wilks’ λ = .51), F(8, 73) = 6.52, p < .001. Bonferroni post-hoc tests show that both defusion (p = .002) and cognitive restructuring (p = .006) outperformed the no-instruction control group at increasing willingness to have the thought. The willingness data presented in Figure 4 show a marked but non-significant, F(2, 68) = 2.77, p = .07, increase in willingness. This increase continued for the active groups but the cognitive restructuring group observed a reduced willingness after Day 4. There is a slightly increasing curve for the no-instruction control, and for the defusion group, a continuous increase in willingness.
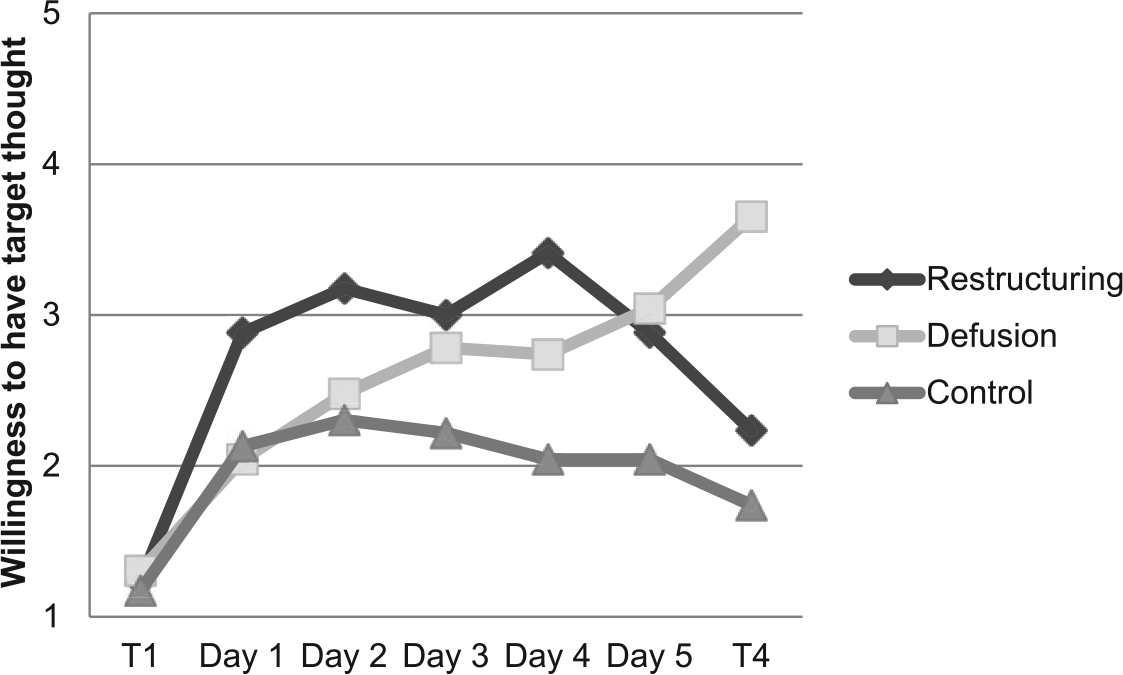
Willingness ratings over the seven measure points for each of the three groups.
Secondary outcome analysis
The repeated-measures MANOVA of scores for the negative and positive self-statements did not show a significant main effect of time (Wilks’ λ = .88), F(8, 61) = 0.99, p = .45, d = 0.74, but did show a significant interaction effect of group and time (Wilks’ λ = .49), F(16, 122) = 3.23, p < .001, d = 1.31. Detailed results follow below.
Believability of positive self-statements
When looking at believability ratings for the positive self-statements, there was no significant effect of time, F(2, 68) = 0.52, p = .47, but a significant Time × Group interaction was found, F(2, 68) = 7.19, p < .001. Bonferroni-corrected post hoc analysis showed no significant differences between the groups (both ps > .05). The within-group t test for the defusion group showed a significant increase in believability, t(23) = 3.00, p = .006, d = 1.25. No such within-group change was found for the no-instruction, t(22) = −2.33, p = .03, d = −0.99, or cognitive restructuring groups, t(23) = .71, p = .48., d = 0.30.
Discomfort of positive self-statements
There was no significant effect of time, F(2, 68) = 0.02, p = .89, but a significant Time × Group interaction, F(2, 68) = 6.31, p = .003, for discomfort ratings for positive self-statements was found. Again, the post hoc analysis showed no significant effects (ps > .05). The within-group t test for the defusion group showed a significant decrease in discomfort, t(23) = 4.27, p = .0003, d = 1.78. This was not found in the no-instruction, t(22) = 2.67, p = .11, d = 1.14, or cognitive restructuring groups, t(23) = −0.68, p = .50, d = 0.29.
Negativity of positive self-statements
Similarly, the negativity ratings for the positive self-statements showed no significant effect of time, F(2, 68) = 0.01, p = .94, or Time × Group interaction, F(2, 68) = 1.86, p = .16. The defusion group, according to the within-group t test, decreased negativity, t(23) = 2.07, p = .05, d = 0.83, which was not the case for the no-instruction, t(22) = 1.43, p = .17, d = .61, or cognitive restructuring groups, t(23) = 0.15, p = .88, d = 0.06.
Willingness of positive self-statements
Willingness ratings for the positive self-statements showed no significant effect of time, F(2, 68) = 0.06, p = .81, but a significant Time × Group interaction, F(2, 68) = 4.40, p = .02. Bonferroni-corrected post hoc analysis again showed that no significant difference could be found (both ps > .05). The within-group t test showed that the defusion group increased willingness significantly, t(23) = 3.92, p = .001, d = 1.63, the no-instruction control, t(22) = −1.99, p = .06., d = 0.85, and the cognitive restructuring groups, t(23) = −0.71, p = .49, d = 0.30.
Believability of negative self-statements
The ANOVA for believability ratings for the negative self-statements showed a significant effect of both time, F(2, 68) = 4.70, p = .03, and Time × Group interaction, F(2, 68) = 11.05, p < .001. Bonferroni-corrected post hoc analysis, however, showed no significant differences between the groups (both ps > .05).
The within-group t test showed that the defusion group decreased believability of negative self-statements significantly, t(23) = −4.28, p = .0003, d = −1.79. The no-instruction control group did not show a significant change in believability, t(22) = 1.91, p = .07, d = 0.81, nor did the cognitive restructuring group, t(23) = −0.91, p = .37, d = 0.38.
Discomfort of negative self-statements
There was no significant effect of time, F(2, 68) = 0.01, p = .93, but of Time × Group interaction, F(2, 68) = 16.93, p < .001, for discomfort ratings for the negative self-statements. However, again, Bonferroni-corrected post hoc analysis showed no significant differences between the groups (both ps > .05).
The within-group t test showed that the defusion group decreased discomfort related to the negative self-statements significantly, t(23) = 4.63, p = .0001, d = 1.93, but that this was not the case for the no-instruction, t(22) = −3.22, p = .007, d = −1.37, or cognitive restructuring groups, t(23) = 1.45, p = .16., d = 0.62.
Negativity of negative self-statements
The ANOVA for the negativity ratings for the negative self-statements showed no significant effect of time, F(2, 68) = 0.05, p = .983, or of Time × Group interaction, F(2, 68) = 0.20, p = .83.
The within-group t test showed that neither the defusion, t(23) = 0.83, p = .42, d = 0.35; the no-instruction control group, t(22) = 0.26, p = .79, d = 0.11; nor the cognitive restructuring, t(23) = −0.57, p = .58, d = 0.24, groups showed any significant change in negativity ratings of the negative self-statements.
Willingness of negative self-statements
Willingness ratings for the negative self-statements did not show a significant effect of time, F(2, 68) = .81, p = .37, but a significant Time × Group interaction, F(2, 68) = 9.20, p < .001. Bonferroni-corrected post hoc analysis again showed that no significant difference could be found (both ps > .05).
The within-group t test showed that the defusion group significantly increased willingness, t(23) = 3.19, p = .004, d = 1.33, but no such changes were found in the no-instruction, t(22) = −4.18, p = .02, d = −1.78, or cognitive restructuring groups, t(23) = −1.41, p = .17, d = 0.60.
Mood measures
Mean and standard deviation scores for each of the three groups (no-instruction control, defusion, and restructuring) at T1 on the four mood measures are presented in Table 2. The results of the T1 analysis indicated no significant differences between the groups on any of the measures (all p > .05).
A repeated-measures MANOVA for the mood measures over time showed a significant main effect of group (Wilks’ λ = .75), F(8, 130) = 2.49, p = .015, as well as Group × Time interaction (Wilks’ λ = .65), F(8, 130) = 3.84, p < .001, so there were both significant differences between the groups and as an effect of being in different groups over time.
PANAS
The ANOVA for the PA scale of the PANAS found no significant effect of time, F(1, 69) = 0.36, p = .36, but a significant Group x Time interaction, F(2, 68) = 10.69, p < .001. Bonferroni post hoc tests revealed a significant difference between no-instruction control and defusion groups (p = .003) and between no-instruction control and cognitive restructuring (p = .02), indicating that both active groups raised PA compared with the no-instruction control. The Negative Affect scale ANOVA found no significant effect of time, F(1, 69) = 0.01, p = .94, nor of Time × Group interaction, F(2, 68) = 0.38, p = .68.
For the within-group t tests for the PANAS, there was a significant increase on the Positive scale for the defusion group, t(23) = −3.17, p = .004, d = −1.32. There were no significant changes in any of the other groups nor on the Negative scale of PANAS (all ps > .0042).
BDI-2
Between-groups ANOVA results indicated a significant effect of time for the BDI-2, F(1, 69) = 8.06, p = .006, but no Time × Group interaction, F(2, 68) = 2.67, p = .08.
Results of the within-group t tests of the BDI-2 showed a significant decrease in the defusion group, t(23) = 3.86, p = .001, d = 1.61, but no significant change in any of the other groups (all ps > .0042).
STAI-s
The STAI-s ANOVA showed no significant effect of time, F(1, 69) = 0.26, p = .61, or of Time × Group interaction, F(2, 68) = 0.87, p = .42. No group changed significantly on the STAI-s according to the within-group t tests.
AAQ-2
Analysis of the AAQ-2 ANOVA showed that the interaction between group and time was close to, but failed to show, significance, F(2, 68) = 3.07, p = .053. No significant within-group changes were found for defusion, t(23) = 2.20, p = .04, d = 0.94; restructuring, t(22) = −0.37, p = .72, d = 0.16; or the no-instruction control groups, t(23) = −1.69, p = .10, d = 0.72.
Discussion
The present study tested the effectiveness of two psychological strategies, cognitive restructuring and defusion, against a no-instruction control for coping with negative thoughts. The study gauged the effect of these strategies on both a self-generated target thought and pre-selected negative and positive self-statements and on measures of mood and experiential avoidance. Of the two active strategies, defusion had significantly greater effects on lowering believability, increasing comfort, and increasing willingness to have the self-generated target thought than a no-instruction control and cognitive restructuring. Defusion was also found to increase PA significantly more than either of the other groups. Of particular interest is the result that the defusion group shifted from rating their thoughts as believable, uncomfortable, and unwilling to unbelievable, comfortable, and willing. The cognitive restructuring group also made significant gains in target thought discomfort and willingness in the same direction as defusion but not in the way that they were rated as comfortable or willing. However, even though the defusion and cognitive restructuring groups displayed a significant reduction in ratings of negativity, participants still rated their target thought as negative.
The initial difference in frequency of the target thought for the three groups means that direct comparison should be approached with caution. This is particularly the case given the fact that the cognitive restructuring group selected thoughts that were less frequently occurring. This could mean that their thought was less painful than the target thoughts of the other groups. Also, as the first frequency registration was taken after the instructions were given (T3 rather than T1), there is no baseline frequency measure. Despite this caution, it is important to note that analysis indicated the frequency of thinking the target thought was reduced in the defusion group, maintained in the restructuring group, and increased in the no-instruction control group.
The secondary outcomes, that is, the effects of the strategies on the positive and negative self-statements revealed similar trends. The between-groups analyses showed significant interaction effects for believability, discomfort, and willingness but not on negativity ratings. However, post-hoc analyses failed to show significant differences between the groups. This is probably due to the conservative nature of Bonferroni corrections. Within-group analyses showed that the defusion group had lower believability and discomfort and higher willingness to have the negative self-statements, and that they had higher believability and willingness and lower discomfort for the positive self-statements. No significant within-group changes were found in the other two groups. It is possible that the use of Bonferroni adjustment is too conservative, as noted by Perneger (1998), and we run the risk of overlooking interesting results.
The significant between- and within-group differences in effectiveness of the cognitive restructuring and defusion techniques as well as the significant within-group effects in the ratings of negative and positive self-statements in the defusion group, but not in the cognitive restructuring or the control group, suggest that defusion may provide a functionally different way of relating to thoughts than cognitive restructuring. Specifically, by viewing thoughts as a behavior, defusion undermines the negative effects of language by teaching clients to achieve some distance from their thoughts; this “de-literalization” (e.g., Masuda, Price, et al., 2010) alters the underlying function of those thoughts, so that their behavior controlling functions are reduced. With behavior analytic terms, we become aware of our own responding rather than just responding to our own responding. In contrast, cognitive restructuring involves disputing the thought by asking us to question how well it corresponds to external evidence. This might lead us to paradoxically hold on to the thought, if only to be able to dispute it. While cognitive restructuring is an effective way to deal with a negative thought, this could mean that it may have less capacity as a strategy to extend its effect to the whole behavioral class of “thinking” rather than just the one thought it targets. This difference may also be a reason why the positive self-statements became more believable in the defusion group.
The use of believability as an outcome has been challenged in defusion papers. Deacon et al. (2011), for example, use “accuracy” instead of believability when describing the scale but in the questionnaire given to participants, the VAS anchors were still variations on the term “believable”, similar to the current study. However, the challenge to the use of believability or level of belief, particularly when differentiating between effects of cognitive restructuring and defusion, is justified as belief may be construed both as literal belief and as lived experience. This means, for example, that while we would assume a cognitive restructuring intervention to reduce literal belief in a thought, (e.g., “I am a bad mother”), by looking at evidence for and against it, it could still be rated as believable because it is corresponding with the lived experience of someone (e.g., “I am in pain”). This is why it is important to also measure how much the thought is a hindrance to participants in pursuing a valued life according to ACT, which essentially is saying you may hold your thoughts as both believable and highly uncomfortable, and it is still counted as a success if defusion allows you to live a life you would value. This is the point to the “willingness” scale used in the present study and not used by Deacon et al. (2011).
Defusion involves creating a context where thoughts are seen as just thoughts, not to be reacted to as if literally true (Hayes et al., 2012). Therefore, it is interesting that the positive self-statements became more believable for the defusion group. Hayes et al. (2012) suggested that not reacting to thoughts as literally true could free people both of believing and disbelieving or struggling with thoughts. So it is possible that not struggling with the target thought allowed participants to see how the positive self-statements could correspond to their own lived experience. This is, of course, conjecture as there was no external measure of how well the positive self-statements described the participants, whether they had friends, were loved, and so on. It might also be that as the defusion group experienced a decrease in subclinical depression, the positive self-statements were easier to believe.
Previous research in defusion has used active controls such as various forms of distraction and suppression (e.g., Hooper & McHugh, 2013; Masuda et al., 2004; Masuda, Price et al., 2010) or cognitive restructuring (e.g., Deacon et al., 2011). The only similar control condition identified is the Hinton and Gaynor (2010) study using a wait-list control. That control condition did not result in significant effects on the outcome. One reason for the within-group effects in the present study might be that the no-instruction control was acting as a classic precursor to cognitive restructuring; using the technique of counting negative automatic thoughts (Beck, 1979) only without then moving on to do the actual cognitive restructuring. A second potential reason may have been that identifying a negative thought and rating positive and negative thoughts may have had a defusing quality in and of itself (Luoma & Hayes, 2009, in O’Donohue & Fisher, 2009). Third, the no-instruction group might have acted as an exposure condition for the thought in question. This can be explained according to either cognitive therapy as activating negative schemas that allow for reinterpretation of them (Clark & Beck, 2011 p. 40) or in ACT terms as acceptance (e.g., Hayes et al., 2012). In future studies, a passive control group that just completes pre- and post-measures without counting thought frequency or willingness on a daily basis would be of use.
As noted in the introduction, due to the short time span, no change in the mood measures was predicted. Despite this, the no-instruction control group scored lower on the PA scale of the PANAS, possibly caused by engaging with a negative thought across 5 days with no coping strategy. The defusion and cognitive restructuring groups demonstrated an increase in PA and a decrease in depression. Such an increase in positive mood reflects previous ACT findings (Ciarrochi, Robb, & Godsell, 2005). Although decreases in depressive symptoms (Ruiz, 2010) have been found previously in ACT studies, this is the first study that has found this effect, specifically using the component of defusion.
There are some limitations to the current study worthy of discussion. First, the techniques employed in this study were simplified and shortened analogues of cognitive restructuring or defusion as therapeutic phenomena. Of course, in treatment therapists use more techniques than the ones employed in the current study when teaching defusion (e.g., Hayes et al., 2012 and cognitive restructuring (O’Donohue & Fisher, 2012). One potential limitation of the current study is that the wording of the instructions was too brief, for example, singing out a thought (in defusion) that one has struggled with may feel invalidating, and saying that all negative thoughts fit into one of the thinking errors (in cognitive restructuring) could reduce the credibility of the instruction, future research should look into different types of cognitive restructuring and defusion to determine whether more extensive instructions produce different results in terms of participants’ responses to their negative thoughts. Second, instructing participants to rate their target thought as a minimum of 4 out of 5 at T1 may have provoked the no-instruction group to use some form of coping in response. As the most frequently used naturally occurring coping strategy for negative thoughts is thought suppression, which has been linked to increased occurrence of the suppressed thought (Hooper, Saunders, & McHugh, 2010; Wegner, Schneider, Carter, & White, 1987), this may have contributed to a rise in frequency and decreased willingness to have the target and other negative thoughts by such individuals. This relates to a second limitation, that is, the use of self-report questionnaires. One future avenue of research that would overcome the inherent difficulty with self-report measures (e.g., concealing responses, demand characteristics) might involve designing an implicit measure of thought believability.
Third, no follow-up test on negative thoughts and mood was included, limiting what can be said about the trajectory and stability of the effects demonstrated herein. Future research should include a follow-up test that monitors the stability of strategy-related changes over time. A fourth limitation was that, although treatment reminders were sent daily, no strategy adherence measure was included. Future research should include a treatment adherence measure. For example, a series of multiple-choice questions could be posed to participants after the strategy to determine whether the participants understand the relevant strategy (see Jeffcoat & Hayes, 2012, for an example of such a treatment adherence quiz). Finally, the credibility and expectancy of the strategies were not assessed, and thus, the between-group differences may have been influenced by differences in credibility or expectancy of one of the treatments.
Despite the limitations, this study is important in a number of ways. First, the results of the study suggest that both cognitive restructuring and defusion are effective techniques for managing unwanted thoughts in non-clinical populations. Second, the results indicate that participants who received the defusion strategy made greater gains than those who received the cognitive restructuring strategy, and that these gains generalize to non-target negative and positive self-statements. Taken together, the findings provide further empirical evidence that defusion is an effective strategy for large-scale dissemination in the management of unwanted negative thoughts. Introducing coping strategies for unwanted negative thoughts for the wider public could potentially have serendipitous effects of spreading more effective strategies to more distressed samples, and therefore benefitting the larger population of moderately distressed individuals (Kazdin & Blase, 2011). Although defusion studies on more distressed samples (Deacon et al., 2011) can be found, future research should compare the use of these even briefer strategies for clinical samples, as well as the potential effects of dissemination as a means to both reduce the risk of individuals with subclinical problems becoming clinical problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.