
Abstract
It has been suggested that reinforcing problem behavior during functional analyses (FAs) may raise ethical questions, such as resulting in an increase in problem behavior outside of FA sessions. The current translational study assessed whether conducting an FA resulted in increases in problem behavior outside of the FA setting for six participants using a nonconcurrent multiple baseline across participants design. The rate of problem behavior was measured outside the FA setting prior to and during an FA. Idiosyncratic results suggest that problem behavior outside of the FA setting may increase, decrease, or be unaffected by conducting an FA.
Studies have shown that basing treatments for problem behaviors upon the results of a prior functional analysis (FA; Iwata, Dorsey, Slifer, Bauman, & Richman, 1982/1994) produces better outcomes (Didden, Korzilius, van Oorsouw, & Sturmey, 2006; Herzinger & Campbell, 2007). Thus, as a tool that guides subsequent interventions for problem behaviors, few assessments have exceeded the impact of FA. Within a typical FA, the reinforcers responsible for maintaining problem behaviors are identified by manipulating antecedent variables and delivering associated consequences contingent upon problem behavior within test conditions. The schedule of reinforcement for problem behavior in these test conditions is generally dense (e.g., fixed ratio 1 [FR1]). Betz and Fisher (2011) suggested that such dense schedules of reinforcement have the advantages of (a) establishing a strong and salient contingency between problem behavior and reinforcement, which may lead to a clearer demonstration of the function of the problem behavior and (b) the possibility of producing lower, and therefore potentially safer, levels of problem behavior than intermittent schedules.
The positive impact of FA methodology upon the quality of the interventions experienced by those who exhibit problem behavior has been widely recognized (Mace, 1994). For example, school systems are required to conduct functional assessments prior to developing behavior intervention plans (Individuals With Disabilities Education Act, 2004). There is also some evidence that with the rise in use of FA methodology, there has been a concomitant reduction in the reliance upon punishment-based strategies for the treatment of problem behavior (Pelios, Morren, Tesch, & Axelrod, 1999). However, despite its standing as one of the most well-supported guides to treatment, FA methodology has not been without some criticism. In his seminal paper that explored the etiology for self-injurious behavior (SIB), Carr (1977) described the possibility of assessing the function of SIB through a reinforcer assessment, not unlike an FA, but raised ethical concerns with reinforcing such destructive behavior. Similarly, while expressing general support for FA methodology, others have raised related concerns (e.g., Hastings & Noone, 2005). In these critiques, the misgiving with conducting FAs is generally not in regard to the safety of allowing problem behavior such as SIB to occur. Rather, these authors have expressed unease with the ethical dilemma of reinforcing problem behavior. That is, they are raising the question of whether it is acceptable to reinforce problem behavior and therefore potentially increase dangerous or destructive behaviors.
Aside from the fact that FAs are typically accompanied by subsequent treatments that should theoretically reduce any increases produced by reinforcement during an FA, the concern over reinforcement of problem behavior can potentially be addressed by carefully selecting the setting in which an FA is conducted. Although it has been shown that FAs can be successfully conducted in natural settings such as homes (e.g., Harding et al., 2001), and in the community (Tarbox, Wallace, & Williams, 2003), a review study found that in most of the published accounts of FAs, they were conducted in hospital facilities, schools, or institutions (Hanley, Iwata, & McCord, 2003). In such settings, FAs can be conducted in spaces specifically selected or designed for that purpose. Similarly, when FAs are conducted in schools, it is frequently possible to run the sessions in a space other than the student’s typical classroom. The setting of the FA is relevant to the concern about reinforcement of problem behavior because novel personnel and features of the environment may exert sufficient stimulus control over problem behavior during FA sessions such that generalization to other settings is minimized (Conners et al., 2000). However, there are some documented accounts of parents and teachers expressing concerns regarding the impact of reinforcing their child’s or student’s problem behavior in an FA conducted in a clinical setting upon the rates of problem behavior in the natural environment (Call, Zangrillo, Delfs, & Findley, 2013; Shabani et al., 2013). In other words, these caregivers have expressed misgivings with conducting an FA because they fear reinforcement of problem behavior in the FA will produce increases in problem behavior in the natural environment where they must then contend with it.
When an FA is conducted in a setting other than the natural environment, the contingencies for problem behavior experienced in the FA setting and natural environment may best be described as a multiple schedule. That is, different schedules of reinforcement alternate (i.e., FR1 in the FA setting; some other, presumably intermittent schedule in the natural environment), with discriminative stimuli associated with each schedule in the FA setting and natural environment. Reynolds (1961) described changes in behavior in one component of a multiple schedule that result from a change in the schedule of reinforcement in the other as an interaction effect. Induction is one type of interaction effect in which responding in both components increases. Thus, increases in problem behavior in the natural environment as a result of introducing a dense schedule of reinforcement in the FA setting could be described as induction. The question of whether induction can occur in the natural environment when an FA is conducted in another setting affects the social validity of FA methodology.
Two recent studies have examined the possibility of induction of problem behavior as a result of conducting an FA (Call, Findley, & Reavis, 2012; Shabani et al., 2013). Shabani et al. compared the rates of problem behavior in students’ regular classrooms immediately before and after FA sessions that were conducted in a separate room. Results from that study found that for three of the four participants the FA, and accompanying dense schedule of reinforcement, had little impact on the rates of problem behavior outside of FA sessions. However, for the fourth participant, slightly elevated rates of problem behavior were observed in the brief period immediately following some FA sessions. This result raises the possibility that FA sessions have the potential to influence rates of problem behavior outside of the setting in which the FA is conducted. However, the study was limited by the fact that there was no control over the contingencies of reinforcement for problem behavior in the non-FA setting. In addition, only brief periods (i.e., 10 or 15 min) immediately prior to and after FA sessions were examined for interaction effects.
Another study by Call, Findley, and Reavis (2012) addressed some of these issues within a day-treatment program in which participants regularly spent portions of their day in session rooms where FAs were conducted, as well as on the unit of the facility. The schedule of reinforcement whenever participants were on this unit was kept at a variable ratio 3 (VR3) in an attempt to replicate the intermittent schedule of reinforcement likely in place in a home. Data on problem behavior were collected during five daily probes outside of the FA setting (i.e., unit): arrival, bathroom, lunch, free time, and departure. By comparing the rates of problem behavior during these probes prior to the FA to those once the FA had begun it was possible to detect whether there was any induction of problem behavior on the unit as a result of conducting an FA in session rooms. Results of the study were mixed, in that two participants’ problem behavior in the non-FA setting increased when the FA was conducted, it remained stable for another, and decreased for a fourth participant. These findings again suggested the possibility for interaction effects, but also suggested that not only increases (i.e., induction) but also decreases (i.e., contrast) in problem behavior outside of the FA setting were possible. However, this study was limited by the absence of data on exposure to specific motivating operations (MOs; Laraway, Snycerski, Michael, & Poling, 2003) on the unit. Ensuring that participants contacted the relevant antecedents during the probes would be necessary to ensure that the MOs responsible for evoking problem behavior were present in both the FA setting and on the unit. If there was no contact with such MOs, changes in the rate of problem behavior on the unit could have been attributed to fluctuations in the motivation to engage in problem behavior. The purpose of the current translational study is to replicate and extend the work of Call, Findley, and Reavis (2012) by addressing some of the limitations of that prior work. Specifically, it examined the influence of conducting an FA on problem behavior outside the FA setting while ensuring that the MO found to maintain problem behavior during the FA were contacted during the probes on the unit.
Method
Participants and Settings
Four male and two female children participated while receiving services in a day-treatment clinic that specialized in the assessment and treatment of problem behavior. The participants ranged from 5 to 13 years old. Topographies of problem behavior included aggression (AGG), disruptive behavior (DIS), SIB, dropping, hair pulling, pica, and spitting. Table 1 depicts specific topographies of problem behavior for each participant. For each participant, it was hypothesized that all the topographies exhibited were members of a single response class.
Participant Characteristics.

Note. Participant age, topography of problem behavior, and function of problem behavior are described. AGG = aggression; DIS = disruptive behavior; SIB = self-injurious behavior; TANG = tangible; ESC = escape; ATTN = attention.
Participants attended the clinic for 6 hr each day, 5 days a week, with the average length of participation lasting 10 days (range = 6-14 days). For the purposes of data collection, all participants’ time was divided into time spent in the FA setting or on the unit. The FA setting consisted of session rooms ranging between 5 m × 4.3 m and 4.3 m × 3 m. Some session rooms were equipped with padded walls, and all had one-way mirrors. Throughout each day, participants took several scheduled and unscheduled breaks on the unit, defined as all spaces outside of the FA setting (e.g., lunchroom, bathrooms, playroom, hallways). A therapist always remained within arm’s reach of the participant while on the unit. Although staffing changes did occur, for the most part, the same team of clinical personnel (i.e., 2-3 therapists) was assigned to each participant for the duration of their admission. In addition, the clinical team assigned to a participant on a given day was with them for the entire day, including time spent in both the FA and unit settings. Unit probe and FA sessions were conducted by these team members; thus, more than one staff member may have conducted various sessions throughout the day.
Data Collection and Experimental Design
The rate of problem behavior per minute that occurred on the unit served as the primary dependent variable. The frequency of problem behavior was collected using hand-held tally counters. A different tally counter was used to record the occurrence of each topography of problem behavior. Problem behaviors were summed to represent a total frequency. Therefore, it was hypothesized that each problem behavior was part of the same response class. Problem behaviors were individually identified and operationally defined for each participant (see Table 1). Therapists collected data during the FA conducted in the session rooms on desktop computers located in the adjoining observation room. Data were collected within a nonconcurrent multiple baseline across participants.
A second observer simultaneously but independently recorded the target behaviors for a mean of 68.46% of probes on the unit across participants (range = 39.3%-93.8%) and a mean of 39.18% of FA sessions (range = 28.57%-56.25%). Interobserver Agreement (IOA) was calculated by dividing the number of agreements by the total number of agreements and disagreements and converting the ratio to a percentage. IOA across participants averaged 95.67% (range = 82.73%-100%) during unit probes and 98.98% (range = 87.59%-100%) during FA sessions.
Procedure
Three probes were conducted each day on the unit throughout all conditions. Probes took place during the same 10 min (participants: Walt, Sally, and Matt) or 5 min (Alan, Aidan, Hannah, and Sam) of regularly scheduled activities that were common for all participants: arrival, break after lunch, and departure. Thus, probes could occur before, between, or after FA sessions that were conducted during that day. We chose to include probes at various times of the day because we were interested in the molar effects of conducting an FA on problem behavior rather than the molecular (i.e., temporally proximal) effects as evaluated in Shabani et al. (2013). Probes were never conducted in a session room (where the FA was being conducted). Probes included procedures identical to the test conditions of the FA (i.e., escape, attention, and tangible conditions; see below). The purpose of the probes was to ensure that participants exposed to an MO found to maintain problem behavior in the FA during data collection on the unit at least once per day. However, there was no additional control for other MOs that could arise naturally during the course of the probe. Thus, it was possible that some MOs could have been present during multiple probes each day. For example, participants were not given continuous attention during all probes, so it was likely that they were exposed to several instances of restricted access to attention, including during tangible and escape probes. All probes were conducted throughout each phase of the study using identical procedures in each phase; however, only probes using procedures matching those conditions found to maintain problem behavior in the FA were included for analysis. The order of the probes (i.e., which MO was ensured to be present) was randomized each day along with the location of where the probes were conducted on the unit.
Throughout the experiment, problem behavior on the unit produced reinforcement on a VR3 schedule. This schedule was utilized because it was thought to approximate the intermittent schedule of reinforcement likely to occur in the participants’ natural environments. Therapists working with each participant utilized a printed sheet of numbers as a prompt for the number of responses required before a putative reinforcer would be delivered according to the VR3 schedule. Prior to the FA and the identification of the function(s) of problem behavior, the consequences that were delivered contingent on problem behavior when the participant was on the unit were based on the antecedents present prior to that instance of problem behavior. That is, if the VR3 schedule requirement was met and problem behavior occurred during a demand situation, escape from that demand was provided; if it occurred when a preferred item was restricted, the item was delivered; or, if it occurred when attention was not being provided, attention was delivered from the therapist in the form of a brief reprimand. If the antecedent to problem behavior was unclear, the therapist delivered a brief reprimand. Again, during probes, it was possible for more than one MO to occur. Thus, if during a tangible probe an item was restricted and no problem behavior occurred, but later, during the same probe, the therapist placed a demand and the participant engaged in problem behavior, all relevant consequences would be delivered. That is, the participant would receive escape from the demand and the tangible item. If the schedule requirement was not met, no differential consequences were delivered and the MO remained until the schedule requirement was met.
Tangible probe
Immediately prior to the initiation of the tangible probe, the participant was allowed free access to any item present at the location where the probe was taking place for 2 min. Following the 2 min of access, the therapist restricted whichever item or activity the participant was engaged with at that moment, and the probe began. The same item was restricted throughout the probe. That is, if an item was restricted and the participant then engaged with a different item, that second item was not restricted.
Attention probe
Immediately prior to the initiation of the probe, the therapist delivered social attention for two min. The therapist then told the participant that attention was no longer available (e.g., “I can’t talk to you anymore, I have to do some work”) and then diverted their attention.
Demand probe
During the demand probe, a demand was placed every minute (during 10-min probes) or every 30 s (during 5-min probes). Demands included tasks that naturally occurred during daily routines on the unit (e.g., open the door, sit here, stand up, throw an item away). A three step, least-to-most (i.e., independent, model, and physical), prompting procedure with a 5-s interprompt interval was used to ensure compliance with demands.
Baseline occurred during the time between the beginning of the participants’ admission and the initiation of the FA. During this time, several activities were completed while participants were present in the FA setting that did not involve reinforcing problem behavior. These activities included completing intake paperwork, interviews with caregiver(s), and conducting one or more preference assessments. Problem behavior that occurred in the FA setting during these activities was blocked and ignored. Problem behavior that occurred on the unit was reinforced on a VR3 schedule of reinforcement as described above.
During the Functional Analysis condition, a multielement FA (Iwata et al., 1982/1994; participants Matt, Sam, and Aidan) or combination of multielement and pairwise FA (Iwata, Duncan, Zarcone, Lerman, & Shore, 1994; participants Sally, Walt, and Hannah) was used. Each participant’s FA included the semirandom presentation of tangible, attention, demand, and toy play conditions conducted within a multielement design or the sequential comparison of test and control conditions in the pairwise analyses (see Iwata et al., 1994). The total number of FA sessions (M = 56.17 sessions; range = 16-104) and number of sessions conducted per day varied for each participant. Problem behavior that occurred in the FA setting was reinforced on a FR1 schedule in all test conditions. The contingencies on the unit remained unchanged from the baseline condition. Probes were discontinued once the FA was completed.
Results
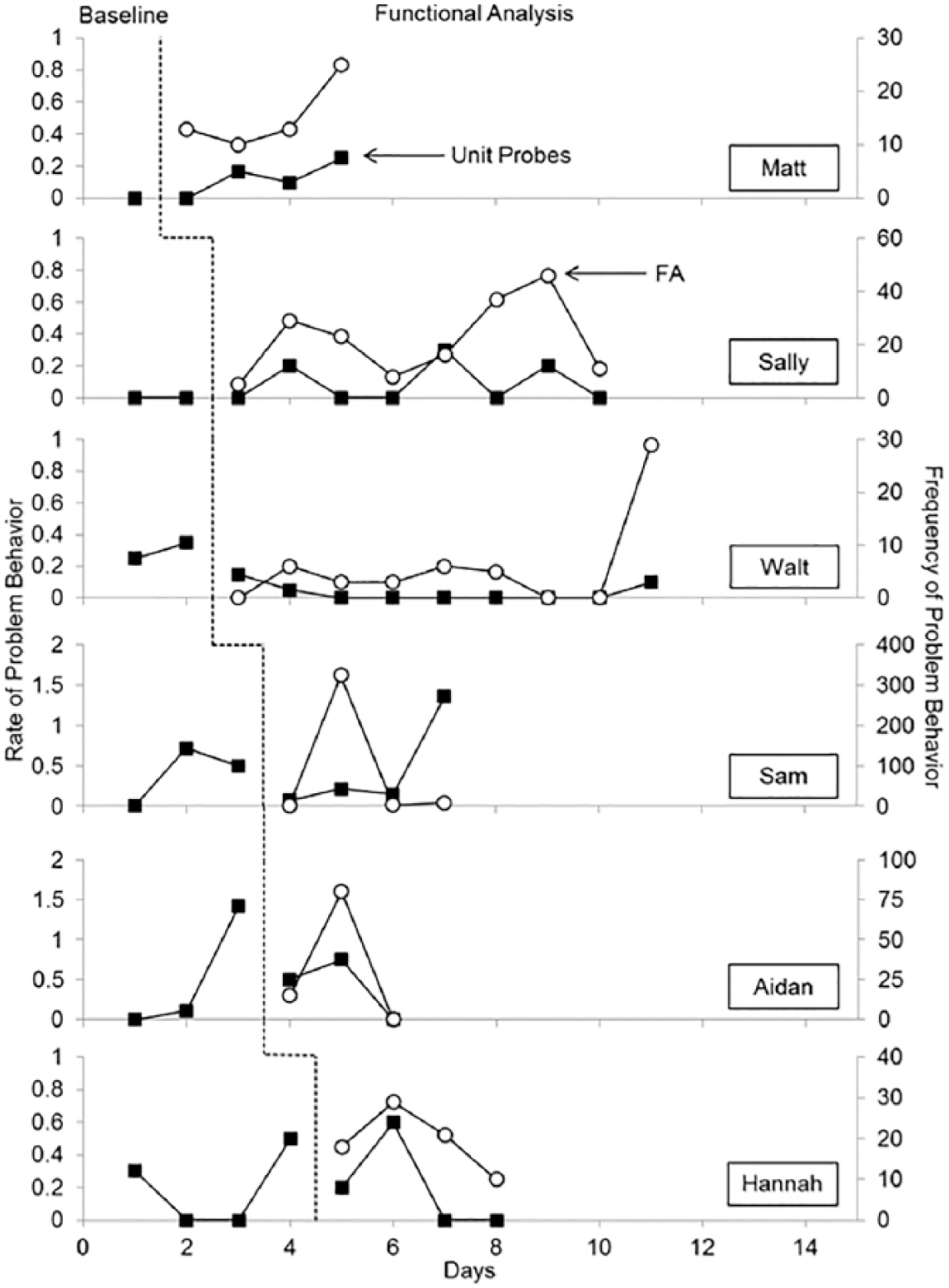
The findings of the current study are shown in Figure 1 for all participants. Each panel depicts the rate of a participant’s problem behavior on the unit during the probes (primary y axis) in the baseline condition (i.e., pre-FA) and once the FA began in the session room. The frequency of problem behavior during FA sessions (secondary y axis) is shown during the FA phase for all participants. The inclusion of the data from FA sessions provide a comparison for the rates of problem behavior observed on the unit and serve as an indication of the frequency of the reinforcement of problem behavior in the FA setting. All unit probe and FA data include problem behavior that occurred during probes or FA sessions that match the reinforcer identified as maintaining each participant’s problem behavior during the FA. That is, if problem behavior was determined to be maintained by positive reinforcement in the form of access to tangible items, only unit probes and FA data during tangible arrangements are presented. For example, the findings of the FA for Matt indicated that his problem behavior was maintained by access to tangible items and escape from demands. Thus, only data from these FA sessions and unit probes are shown in Figure 1. It is important to note that differing scales for the y axis are used for each participant’s graph to aid with visual inspection of the data.
Results of conducting an FA on problem behavior across participants.
Overall, the results were mixed. Rates of problem behavior during unit probes in the baseline phase were generally low, although variable rates were observed for Walt and Sam. For Matt and Sally, problem behavior collected on the unit, not including unit probes, was observed throughout the day; however, no problem behavior was observed in unit probes during the baseline phase for either participant. Once the FA was being conducted in the session room, the rate of problem behavior gradually increased for both participants. This increase was observed during unit probes, though there was no change in the schedule of reinforcement in that setting. To quantify the change in the rate of problem behavior on the unit, the percentage of change was calculated by taking the absolute value of the difference between the mean rates of problem behavior per minute in baseline and FA phases, dividing by the mean rate during baseline, and multiplying by 100. If the mean rate of problem behavior during baseline was 0.00, then the denominator was changed to 1.00, which may be a conservative calculation of the percent change. A modest increase in problem behavior on the unit was observed for both participants. Matt engaged in no problem behaviors during baseline, but averaged 0.20 responses per minute in the FA condition (i.e., a 20.00% increase). For Sally, the rate of problem behavior on the unit increased from no responses in the baseline condition to a mean of 0.09 responses per minute in the FA condition, a 9.00% increase in problem behavior during the unit probes. In addition, higher rates of problem behavior during unit probes appeared to be associated with a higher frequency of problem behavior during FA sessions for these participants.
In contrast to results for the two participants for whom problem behavior on the unit increased, Walt’s problem behavior decreased on the unit when the FA was introduced in the session room. That is, rates of problem behavior increased and remained stable and elevated in unit probes in the baseline condition (M = 0.30). However, when the FA began in the session room, problem behavior decreased during unit probes to an average of 0.04 instances of problem behavior per minute, an 86.67% decrease. Although less pronounced than Matt and Sally’s data, visual inspections suggests a similar relationship between the rate of problem behavior during unit probes and the frequency of problem behavior during FA sessions.
For the remaining three participants (Sam, Aidan, and Hannah), little change was apparent in the rate of problem behavior in the unit probes during baseline and when the FA began in the session room. The mean rate of Sam’s problem behavior in the FA condition (M = 0.49) was higher than rates observed in the baseline condition (M = 0.43; 13.95% increase). Visual analysis indicates that a single outlier in the FA phase may account for the calculated increase, with little difference between phases when this data point is excluded. The frequency of problem behavior during the FA did not appear to be related to the rate of problem behavior during unit probes for Sam. For Aidan, differences in the rate of problem behavior in baseline (M = 0.44) and the FA (M = 0.46) showed an increase of 4.55%. Similar to Matt, Sally, and Walt, higher frequencies of problem behavior during FA sessions were associated with a higher rate of problem behavior during unit probes for Aidan. Finally, Hannah’s results indicated no difference in the rate of problem behavior per minute in baseline (M = 0.20) and FA (M = 0.20) phases. The rate of problem behavior during unit probes appears to be positively related to the frequency of problem behavior during the FA sessions for Hannah.
Discussion
Overall, the impact of conducting an FA in session rooms had the expected idiosyncratic effect on the rate of participants’ problem behavior on the unit. For two participants, there was a gradual increase in problem behavior, whereas for another, there was a more immediate decrease. For the remaining three participants, conducting an FA seemed to have little impact on problem behavior on the unit. This result replicates those of previous studies on this issue (i.e., Call, Findley, & Reavis, 2012; Shabani et al., 2013) and contributes further evidence suggesting that interaction effects can be, but are not necessarily consistently, observed when an FA is conducted in another setting. That is, results of the present study also replicate those of Call, Findley, and Reavis in which a participants’ problem behavior decreased when an FA was introduced. Thus, both studies seem to demonstrate that the interaction effects produced by conducting an FA in one setting can be in the form of induction or contrast. Furthermore, this study addressed a major limitation of that study by ensuring that participants were exposed to the relevant antecedent events in the non-FA setting.
Results from this study may be useful to clinicians who conduct FAs. In particular, it may be important to monitor behavior in settings other than the one in which the FA is being conducted to protect against induction. In addition, caregivers who express apprehension about conducting an FA due to concerns of increases in problem behavior in other settings can be informed that induction can occur, but that in some cases, contrast effects may also result. The possibility that problem behavior may actually decrease in the non-FA setting would seem to be a positive result of conducting an FA and may help allay such fears. However, the modest number of participants included in this study and those that examined this topic previously still make it impossible to determine the probability of an interaction effect. The limited findings to date suggest that conducting an FA has idiosyncratic effects on problem behavior outside of FA sessions.
Despite idiosyncratic findings across participants during unit probes in baseline and FA phases, a potential relationship between problem behavior during FA sessions and unit probes was observed for three of six participants during the FA phase. This finding differs from those of Shabani et al. (2013), who reported little effect of FA sessions on problem behavior during subsequent observations, relative to those conducted prior to FA sessions. In the work by Shabani et al., it is unclear whether the relevant MO for problem behavior was present during pre- and post-FA observations as teachers were instructed to interact with the participants in a typical fashion. Although the findings of the current study provide some preliminary evidence of a potential relationship between problem behavior during FA sessions and unit probes, the mechanism for the observed relationship is unclear.
The unit setting included in this study was selected to serve as an analogue to the natural environment because it included discriminative stimuli and a schedule of reinforcement that differed from those present in the FA setting. However, it remains unclear whether interaction effects would be observed across settings that have less in common than the unit and session rooms did in this study, such as a client’s home and the clinic in which an FA is conducted. Such settings are likely to differ more in terms of the individuals present (e.g., parents vs. teachers/staff/other students), physical characteristics (e.g., furniture and decor), history of reinforcement, and the amount of variability in schedules of reinforcement in each setting. However, the basic research on generalization suggests such interaction effects may be less likely when schedule correlated stimuli are present (Reynolds, 1961; Schwartz, Hamilton, & Silberberg, 1975). Thus, such differences between the natural environments and analogue settings used in this study may mean that interaction effects are less likely in the real world.
Results of this study are limited by the fact that behavior changes on the unit were not immediate for those participants who showed an increase. Within a multiple baseline design, demonstrations of experimental control are strongest when changes in the dependent variable are observed when the independent variable is introduced while remaining unchanged in baselines without changes in the independent variable. However, such immediate effects may have been less likely due to the hypothesized operative mechanism being induction. That is, it could be expected to take some time for the effects of reinforcement in one stimulus condition to spread to another. For the remaining participant where an interaction effect was observed (Walt), problem behavior decreased on the unit shortly after the FA began in the session room. This result suggests the possibility that different mechanisms may be responsible for the induction and contrast effects observed, and may be an area for future research. For example, the dense schedule of reinforcement in the FA may have produced changes in problem behavior on the unit because of satiation.
The use of a multiple baseline design also presents challenges to interpreting these data because single subject methods are not ideally suited to demonstrate the lack of an experimental effect. For three participants (Sam, Aidan, and Hannah), minimal changes in problem behavior were detected when the FA was introduced. However, had reinforcement of problem behavior in the FA produced an eventual increase in problem behavior on the unit, a multiple baseline design would have been well equipped to detect such an effect. Furthermore, even though the multiple baseline design, like most research methods, is designed to detect changes in behavior rather than the lack of a change, in this case, the absence of an effect was as noteworthy as its presence. From a clinical perspective, the absence of increases in problem behavior in the non-FA setting in half of the cases evaluated may help to allay caregiver concern about having an FA conducted with their dependents.
The current study measured the rate of responding during unit probes, so it is not possible to describe potential changes in other dimensions of behavior (e.g., magnitude, latency). Future research should consider the possibility of the effects of conducting an FA on these dimensions that may also have implications for the social validity of FAs. In addition, this study attempted to approximate the schedule of reinforcement for problem behavior in the natural environment using a VR3 schedule. This schedule was selected based on the assumption that problem behavior is likely reinforced on an intermittent schedule, and so a VR3 seemed an appropriate analog. However, future studies could better control for this variable by assessing the schedule of reinforcement present in the natural environment and yoking the schedule used in the study to it. Finally, researchers may wish to continue this line of research by evaluating the potential for interaction effects in other, more naturalistic settings such as classrooms or participants’ homes. Another limitation of the current study was that the decision to begin conducting the FA was based on the clinical needs of the participants. Once the initial activities that were scheduled to be conducted in the session room were completed, the FA began, regardless of whether baseline rates of problem behavior on the unit were stable. For some participants, this meant that the FA began with rates of problem behavior on an increasing trend (e.g., Hannah), which is not ideal for a multiple baseline design.
Despite these limitations, the present study could be seen as contributing to what is otherwise a largely underrepresented question about the use of FAs in clinical settings. An understanding of the specific variables responsible for induction and contrast within the context of clinical activities such as an FA has the potential to alter what currently constitute best practices, such as when and how behavior analysts conduct FAs. Thus, the field could also benefit from additional research that examines the clinical impact of the factors shown in the basic literature to affect the probability or magnitude of interaction effects. For example, the basic literature suggests that whether an interaction effect is manifest as induction or contrast may be a result of the degree of stimulus control present in a setting (Pear & Wilkie, 1971), with strong stimulus control resulting in contrast and weak stimulus control resulting in induction. This could mean that the probability of induction of problem behavior in a home environment, as a result of an FA in clinical or school settings, may be even less likely than what occurred in the present study because discriminability between such settings is likely to be even greater than between the unit and session rooms used in this study. Future research could examine whether the effect of reinforcing problem behavior during an FA on problem behavior in the natural environment could potentially be mediated by, or even capitalized upon, the addition of discriminative stimuli to either setting. That is, establishing strong discriminative control in the setting in which the FA is conducted could decrease the probability of induction or even produce a contrast effect in the form of a decrease in problem behavior in the natural environment. Such an outcome would likely increase the social validity of conducting an FA.
Footnotes
Acknowledgements
The authors thank Richard Smith for his help with a previous version of this article.
Authors’ Note
Natalie A. Parks is now affiliated with Trending Up. Andrea R. Reavis is now affilitaed with Trumpet Behavioral Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.