
Abstract
The purpose of this study was to summarize the evidence base for interventions targeting individuals with work-related posttraumatic stress disorder (PTSD), to make recommendations for clinicians and administrative decision makers involved in their rehabilitation, and to guide future research in this area. Particular attention was given to studies that were conducted in naturalistic clinical settings or in a workers’ compensation claim context. Electronic searches of Cochrane Central Register of Controlled Trials, MEDLINE, PubMed, PsycINFO, CINAHL, PILOTS, and EMBASE identified 11 articles. Study populations included railroad personnel, police officers, disaster workers, and individuals with industrial injuries. Interventions included trauma-focused cognitive-behavioral therapy and eye movement desensitization and reprocessing. Several studies specifically targeted workers who had failed to return to work (RTW) after standard PTSD treatment. The results suggest that psychotherapy interventions are beneficial for helping clients recover from PTSD symptoms and RTW. In studies that reported on work status, RTW rates increased over time and generally lay between 58% and 80% across follow-up time points. Narrative impressions were supplemented by calculation of Risk Differences for individuals working at pretreatment versus posttreatment. Clinical consideration, methodological issues limiting the current body of work, and recommendations for future research are discussed.
Introduction
Exposure to traumatic events is common in Western countries. Surveys among the general population suggest that 81.7% of U.S. Americans (Sledjeski, Speisman, & Dierker, 2008), 76.1% of Canadians (Van Ameringen, Mancini, Patterson, & Boyle, 2008), and 63.6% of Europeans (Darves-Bornoz et al., 2008) have experienced at least one traumatic event in their lives. About 5% to 10% of these individuals subsequently develop posttraumatic stress disorder (PTSD; Amstadter, Aggen, Knudsen, Reichborn-Kjennerud, & Kendler, 2013; Breslau et al., 1998; Roberts, Gilman, Breslau, Breslau, & Koenen, 2011), a mental health condition that is characterized by persistent symptoms of reexperiencing the traumatic event, hyperarousal, changes in feelings and beliefs, and avoiding trauma reminders. Epidemiological studies indicate that 3.5% of the U.S. (Kessler, Chiu, Demler, Merikangas, & Walters, 2005), 2.4% of the Canadian (Van Ameringen et al., 2008), and 0.6% to 2.3% of the European (Darves-Bornoz et al., 2008) general population have current PTSD.
PTSD poses a considerable burden to the individual and the society. Individuals diagnosed with PTSD are more likely to report physical illnesses, additional mental disorders, suicide attempts, poor quality of life, and short- and long-term disability than individuals without this diagnosis (Brady, Killeen, Brewerton, & Lucerini, 2000; Sareen et al., 2007). PTSD has also been linked to reduced work performance and productivity such as increased work loss and cutback days, reduced ability to manage job demands, and failure to return to work (RTW) after trauma exposure (Breslau, Lucia, & Davis, 2004; Lim, Sanderson, & Andrews, 2000; Matthews, 2005; Wald, 2009; Zatzick et al., 2008).
In numerous cases, posttraumatic stress is attributable to events that occurred at the workplace, and a significant number of workers have been exposed to injury, death, life-threatening situations, disasters, or assaults in the context of their professional duties (Hämäläinen, Takala, & Saarela, 2006; Skogstad et al., 2013). For example, studies have demonstrated that posttraumatic stress is prevalent among individuals with work-related physical injuries (Burgess, Hibler, Keegan, & Everly, 1996). In a study of 139 injured workers who participated in a physical rehabilitation program, 34.7% were diagnosed with PTSD and 18.2% reported symptoms suggesting partial PTSD (Asmundson, Norton, Allerdings, Norton, & Larsen, 1998). Certain professions such as police officers, emergency and rescue personnel, firefighters, bank officers, and train drivers carry a particularly high risk of exposure to traumatic events (McFarlane & Bryant, 2007). A recent meta-analysis examining the worldwide prevalence for current PTSD among rescue workers found rates of 14.6% for emergency personnel, 7.3% for firefighters, 4.7% for police officers, and 13.5% for other rescue teams (Berger et al., 2012).
Although natural recovery remains the most common trajectory after trauma, some individuals fail to do so and develop long-lasting disruptions and disabilities (McFarlane, 1997). Grunert, Devine, Matloub et al. (1992) observed that among persons with work-related hand injuries, symptoms of posttraumatic stress persisted 18 months after the injury. In a study of survivors of the Piper Alpha oil platform disaster, 36% of the participants reported survivor guilt and 21% met criteria for PTSD 10 years after the explosion (Hull, Alexander, & Klein, 2002). In another study, oil workers exposed to the Alexander L. Kielland platform capsize were significantly more likely to have current PTSD and a variety of other mental disorders than a matched group of nonexposed workers 27 years after the disaster (Boe, Holgersen, & Holen, 2011).
A number of interventions for the treatment of PTSD have been developed over the past decades and been tested in numerous studies, mainly with civilian and military samples. A variety of treatments have been shown to be effective for improving PTSD symptoms; recommended first-line psychotherapies include trauma-focused cognitive-behavioral therapy (TFCBT), such as exposure therapy and cognitive processing therapy, eye movement desensitization and reprocessing (EMDR), cognitive therapy (CT), and stress inoculation training (Forbes et al., 2010). A meta-analysis of 26 psychotherapy studies indicated that across interventions, 56% of the participants enrolled in the studies and 67% of those who completed the therapy no longer met criteria for PTSD at the end of treatment (Bradley, Greene, Russ, Dutra, & Westen, 2005). Recommended pharmacotherapies for PTSD treatment include serotonin reuptake inhibitors (SSRIs; Forbes et al., 2010); meta-analysis concluded that response rates approach 60% (Stein, Ipser, & Seedat, 2006) although more recent data suggest that SSRIs may be not as effective as previously thought (Bajor, Ticlea, & Osser, 2011). However, interventions specifically delivered to individuals with work-related PTSD have rarely been examined.
The conclusion that an individual’s posttraumatic stress is attributable to the workplace has significant implications for workers’ compensation and litigation. Early studies among the workforce have primarily focused on the existence of psychological distress in response to physical injuries; this mental health condition has also been most universally recognized as compensable throughout North American states and provinces (Lippel, 1989). Workers’ compensation boards (WCBs) today generally acknowledge the right to compensation for mental health problems attributable to psychological traumatic work stressors (Lippel & Sikka, 2010). However, except for military-related PTSD, research exploring psychological distress in response to traumatic work stressors has remained scant (McFarlane & Bryant, 2007).
If a claim of work-related PTSD was accepted by the WCB, the worker is entitled to receiving treatment for the PTSD. Typically, expectations pertaining to an intervention that is being funded by a workers’ compensation insurance agency are related to both reduction of PTSD symptoms and resumption of work. Although one could argue that clients will be ready to RTW once they have experienced significant improvements of their PTSD symptomatology, there is a fundamental difference between a decrease of symptoms and clinical improvements that enable individuals to function in their daily life and at their workplace, especially when the workplace is associated with the trauma. In fact, most studies examining the effects of PTSD interventions have focused on psychological outcome variables and did not provide any specific information regarding their participants’ working capacity. In a university-based treatment study, treatment-related reductions in symptoms were associated with improvements in occupational functioning (Taylor, Wald, & Asmundson, 2006); however, this study measured work functioning on a 11-point rating scale and did not provide any information as to how many of the participants actually returned to work. In a study examining the outcome of two CBT-based interventions for individuals who were on work-related stress leave, psychological complaints continuously decreased over the follow-up period but were unrelated to RTW (Blonk, Brenninkmeijer, Lagerveld, & Houtman, 2006). There is evidence to suggest that a substantial proportion of individuals with work-related PTSD struggle to RTW even when receiving treatment. MacDonald and colleagues conducted a retrospective file review of 44 workers whose claims were accepted for PTSD by a Canadian WCB. Although 93% of the workers had received some form of intervention by the time of the file review, only 43% have returned to their previous job with the accident employer (of whom 74% had some form of job modification), whereas 34% have not returned to work and two individual have received permanent disability awards due to their PTSD diagnosis (MacDonald, Colotla, Flamer, & Karlinsky, 2003). It is possible that RTW is an aspect of recovery that takes longer than symptom reduction, especially if the workplace is directly associated with the trauma. In view of additional studies that showed that unemployment following a traumatic event predicted persistence of PTSD symptoms (Nandi et al., 2004), and that reemployment was associated with subsequent mental health improvement (Hoare & Machin, 2010), it is therefore important to understand the current empirical status of treatments for individuals with work-related PTSD, to make best practice recommendations for clinicians, administrative decision makers (e.g., insurance case managers), and other professional involved in the workers’ rehabilitation, and to guide future research in this area.
Accordingly, the current study represents a systematic review of clinical studies evaluating the effects of interventions that specifically targeted individuals with work-related PTSD. Particular attention was given to studies that were conducted under representative conditions (e.g., in naturalistic clinical settings or in a WCB claim context). Our objective was to provide guidance as to how individuals with work-related PTSD can best be treated within a workers’ compensation claim system. We aimed to answer the following questions:
Materials and Method
Selection Criteria
We included all English-language studies that quantitatively evaluated the outcome of psychotherapeutic or pharmacological therapies addressing posttraumatic stress in individuals who have been exposed to a traumatic event during their work duties. At minimum, all study participants were required to both (a) have experienced a traumatic event in the context of their work duties and (b) report the presence of posttraumatic distress. We excluded studies with military samples, those that combined workers with civilian or military participants in their treatment sample (except when results were disaggregated), and those that included individuals who had experienced nontraumatic work stressors (e.g., working overtime). Because we aimed at identifying studies that had been conducted in naturalistic clinical settings, randomized, nonrandomized, and uncontrolled studies were accepted. Single case studies were excluded due to their limited generalizability. Treatments were not limited in terms of their approach but they were required to address existing trauma-related symptoms; interventions that aimed at preventing PTSD (e.g., critical incident stress debriefing) were excluded. Both psychotherapy and pharmacotherapy interventions were acceptable. Studies were required to report work-related (preferably RTW) outcomes; if this was not available, quantitative measures of traumatic stress symptomatology were acceptable. However, for all articles that did not provide work-related outcomes, we tried to obtain this information from the researchers via email (two attempts were made for each article). Studies that used nonpsychological/-RTW measures (e.g., cerebral blood flow or heart rate) as the only outcome variables were excluded. Studies were required to present the outcome variables for the sample as a whole using statistical analyses. Studies that reported treatment outcomes for each participant individually and those that did not use statistical analyses were excluded. After completing the risk of bias assessment for all articles, studies that received a “weak” rating for their methodological quality were also excluded due to the high risk of bias associated with this rating.
Search Strategy
Studies were identified by searching electronic databases in October 2016. Subsequently, the reference lists of included studies and other articles on work-related trauma were scanned. We also used the “search for related articles” function at scholar.google.com for all included studies. Electronic searches were conducted in PILOTS, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PubMed, PsycINFO, CINAHL, and EMBASE; the search was not restricted by publication date. We combined words related to posttraumatic stress with words related to work and words related to treatment. We searched for the following terms in titles, abstracts, and keywords: “trauma” or “ptsd” or “posttraumatic stress disorder” or “stress” and “work” or “job” or “duty” or “workers” or “employees” or “personnel” or “occupational” or “vocational” or “industrial” and “treatment” or “therapy” or “intervention” or “psychotherapy” or “exposure” or “EMDR” or “stress management” or “pharmacotherapy” or “psychotropic” or “drug” or “medication.” All articles meeting the broad inclusion criteria were reviewed and evaluated for eligibility. Uncertainty regarding study eligibility was resolved by consensus between the two authors.
Risk of Bias Assessment
To identify the risk of bias associated with individual studies, the two researchers independently assessed each selected article using the McMaster University Quality Assessment Tool for Quantitative Studies (QAT; Thomas, 1998). The QAT has been recommended for use in systematic reviews that include nonrandomized intervention studies (Deeks et al., 2003). Six individual study components (selection bias, study design, confounders, blinding, data collection methods, and withdrawals/dropouts) are rated as “strong,” “moderate,” or “weak” using standardized guidelines; these ratings are combined to provide a global rating of methodological quality. Strong ratings were associated with a randomized controlled design where participants were representative of the target population, which controlled for at least 80% of relevant confounders and used valid and reliable measures, where outcome assessment occurred in a blinded fashion, and which had acceptable drop-out rates. Quality assessment components were discussed for each study one by one; disagreements between the two authors were resolved by consensus. Studies that received a “weak” rating were excluded from further analysis.
Data Extraction and Analysis
For each study included in final analysis, both authors independently extracted information using a data extraction form. For each study, the following information was extracted: (a) publication details (i.e., first author, publication year, and country), (b) study population details (i.e., professions/occupations of participants, type of traumatic experiences, clinical diagnosis), (c) work-related issues (i.e., WCB involvement, the number of study participants working vs. not working at the beginning of the study, and the longest follow-up time point), (d) total number of participants enrolled in the study (N) and number of participants in each study arm, (e) intervention details, (f) comparison condition details (if applicable), and (g) follow-up time points.
Subsequently, the findings were reviewed in joint meetings. For each discrepancy or uncertainty identified, both authors re-reviewed the original article and resolved discrepancies by discussion and consensus. For each study that reported on participants’ work status, information was extracted regarding the total number of participants and the number of individuals who were working versus not working at two time points: the beginning of the study and the longest follow-up time point. These data were presented in a table and were used to calculate the Risk Difference (RD)—that is, the difference in the observed proportions of individuals who were working at follow-up compared with the beginning of the study—within each study group and across studies. For studies with a no-treatment comparison condition, only the active treatment arm was used for RD calculation. When two similar active interventions had been delivered in one study (e.g., imaginal vs. in vivo exposure, early vs. delayed exposure) with no significant differences in outcomes observed by the authors, the data of the two treatment arms were pooled for the table and calculation. When two different interventions had been delivered, or two similar interventions had resulted in significantly different outcomes, the data were presented separately. Heterogeneity between studies was tested using the I2 test. If the I2 value was greater than 50%, we used a random-effect model to calculate the RD. If the I2 value was lower than 50%, heterogeneity was considered low and we recalculated the RD using a fixed-effect model (Higgins, Thompson, Deeks, & Altman, 2003). Separate analyses were conducted for studies that included only workers who had failed to RTW after completing a standard PTSD program and studies that did not make this specification. Comprehensive Meta-Analysis Version 3.3.070 was used for all calculations.
Results
Study Identification
A flow chart describing the study selection and exclusion process is provided in Figure 1. The literature search identified a combined database of 3,822 potentially relevant abstracts. Of them, 3,701 were removed because they were clearly unrelated to our research question based on the title or abstract. The remaining papers were reviewed based on their full text. Fifteen of them—one dissertation (Salyards, 2005) and 14 journal articles—met our eligibility criteria and were included in a quality assessment. Of the 15 articles, seven did not provide information on work-related outcomes (Difede et al., 2007; Duckworth, 1986; Grunert, Weis, Smucker, & Christianson, 2007; Högberg et al., 2007; Lansing, Amen, Hanks, & Rudy, 2005; Rumyantseva & Stepanov, 2008; Solomon & Kaufman, 2002). Thus, the researchers were contacted to obtain these data, and work status could be acquired for two additional studies (Difede et al., 2007; Grunert et al., 2007). Because 100% of the participants were working in the study conducted by Difede and colleagues (2007), the study was included in the narrative part of this review but not in the RD analysis.

Flow chart of study inclusion and exclusion process.
Two articles were based on the same trial examining an intervention for transportation workers. One of them described short-term outcomes for the active treatment versus the waitlist condition (Högberg et al., 2007) and one reported long-term outcomes for the active treatment after the waitlist had also been provided with the intervention (Högberg et al., 2008); the latter study was selected to represent this data set in the RD analysis. Six reports stemmed from the same clinic (Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert, Matloub, Sanger, & Yousif, 1990; Grunert et al., 2007; Salyards, 2005; Weis, Grunert, & Christianson, 2012) delivering interventions to treat posttraumatic stress in individuals with industrial injuries. Their study participants were not identical but overlapped to some extent. While all of these studies are described in the narrative part of this review, Weis et al. (2012) was selected for the first RD analysis. Grunert and his colleagues were also the only study group examining interventions for workers who had previously failed to RTW with standard PTSD treatment; three of their articles (Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert et al., 2007; whose samples did not overlap) provided the data for the second RD analysis. One study (Bender et al., 2016) compared the outcome of workers who have received treatment as usual (TAU) with the outcome of workers who have been referred to “Best Practice Intervention” (BPI). Because BPI differed from active treatment conditions in all other studies in the sense that it involved a multidisciplinary assessment, education, and treatment program that was offered by several treatment providers using any of the evidence-based CBT and/or pharmacological interventions recommended in PTSD clinical practice guidelines (National Collaborating Centre for Mental Health, 2005), the study was included in the narrative part of this review but not in the RD analysis.
Quality Assessment
The quality of study designs, representativeness of participants, confounder control, blinding, data collection, and completeness of samples varied considerably across studies. Of the six controlled studies, two (Difede et al., 2007; Högberg et al., 2007) qualified as randomized controlled trials (RCTs) according to the QAT. Randomization was not described in sufficient detail to permit classification as an RCT for one trial (Gersons, Carlier, Lamberts, & van der Kolk, 2000), which was then categorized as a controlled clinical trial (CCT). All three obtained a strong QAT rating for study design. The remaining studies used a cohort analytic design where assignment to the intervention did not occur through randomization but depended on clinical considerations and external conditions (Bender et al., 2016; Salyards, 2005; Weis et al., 2012) or participants’ choices (Solomon & Kaufman, 2002). Two of them (Salyards, 2005; Weis et al., 2012) were retrospective analysis. The eight uncontrolled studies used a cohort design. The design quality of these 11 studies was rated as moderate.
Recruitment and selection of participants were not well described in most studies. If information was provided, it appeared that most studies relied on self-referral/self-selection as their main recruitment strategy and/or lost many eligible individuals before the intervention started. Thus, most study samples were likely not representative for their target population (particularly as additional exclusion criteria related to substance abuse, major depressive disorders, use of psychiatric medication, or trauma features further limited generalizability), resulting in a weak QAT rating for selection bias. Exceptions were studies conducted by Bender et al. (2016) where all participants appeared to be systematically referred by an Occupational Health and Claims Management Department (referral from a source in a systematic manner resulted in a moderate QAT rating). Furthermore, Grunert and colleagues received their referrals through a WCB. Weis et al.’s (2012) sample included “all of the patients treated in the clinic between January 1994 and July 1998” (p. 128). Salyards’s (2005) study participants consisted of all individuals who were treated with imaginal or in vivo exposure between 1985 and 2002; however, her focus on individuals with nonvisual flashbacks limited the generalizability of this sample (resulting in a weak rating for selection bias). Based on information in her dissertation, all other studies carried out by Grunert’s team exclusively comprised workers referred by a WCB; thus, they appeared to be “somewhat likely” to represent the target population (moderate QAT rating). These authors also did not apply (or report) any exclusion criteria.
Of the 13 studies that included individuals with PTSD or subthreshold PTSD, six used clinician-administered diagnostic interviews (Bender et al., 2016; Difede et al., 2007; Gersons et al., 2000; Högberg et al., 2007, 2008; Rumyantseva & Stepanov, 2008), whereas it remained unclear in the remaining studies how the diagnosis had been established. Most studies used data collection tools that were reliable and valid for assessing trauma-related distress; one study used a single measurement that was not PTSD-specific (Duckworth, 1986), and for three studies (Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert et al., 1990) RTW was the only outcome variable. Information on work status—denominated “return to work,” “work resumption,” or “full working capacity”—was available for 10 studies; only one (Bender et al., 2016) provided a more detailed definition of the term.
Few studies provided information on confounding variables. The two RCTs found no baseline differences between treatment groups (strong rating). In studies where significant baseline differences were reported, one study controlled for these variables in the analyses (Bender et al., 2016) and two did not (Gersons et al., 2000; Salyards, 2005). In terms of blinding, the outcome assessors of the two RCTs and the CCT were unaware of the participants’ intervention assignment. Blinding was not described in the remaining studies and it often remained unclear if study design, treatment, data collection, and analysis of results were conducted independently; thus, confirmation/detection bias could not be ruled out. When drop-out rates were reported, they were generally low except for two studies (Difede et al., 2007; Solomon & Kaufman, 2002). Of the seven studies that included a comparison condition, five received a moderate rating and two received a weak rating. Of the eight uncontrolled studies, six received a moderate and two received a weak rating. Because the risk of bias is considered high for studies with a weak rating, they were excluded from further analysis (i.e., Duckworth, 1986; Rumyantseva & Stepanov, 2008; Salyards, 2005; Solomon & Kaufman, 2002). Characteristics of the remaining 11 studies are presented in Tables 1 (for the five studies that included a comparison condition) and 2 (for the six uncontrolled studies).
Characteristics of Studies With a Comparison Condition.
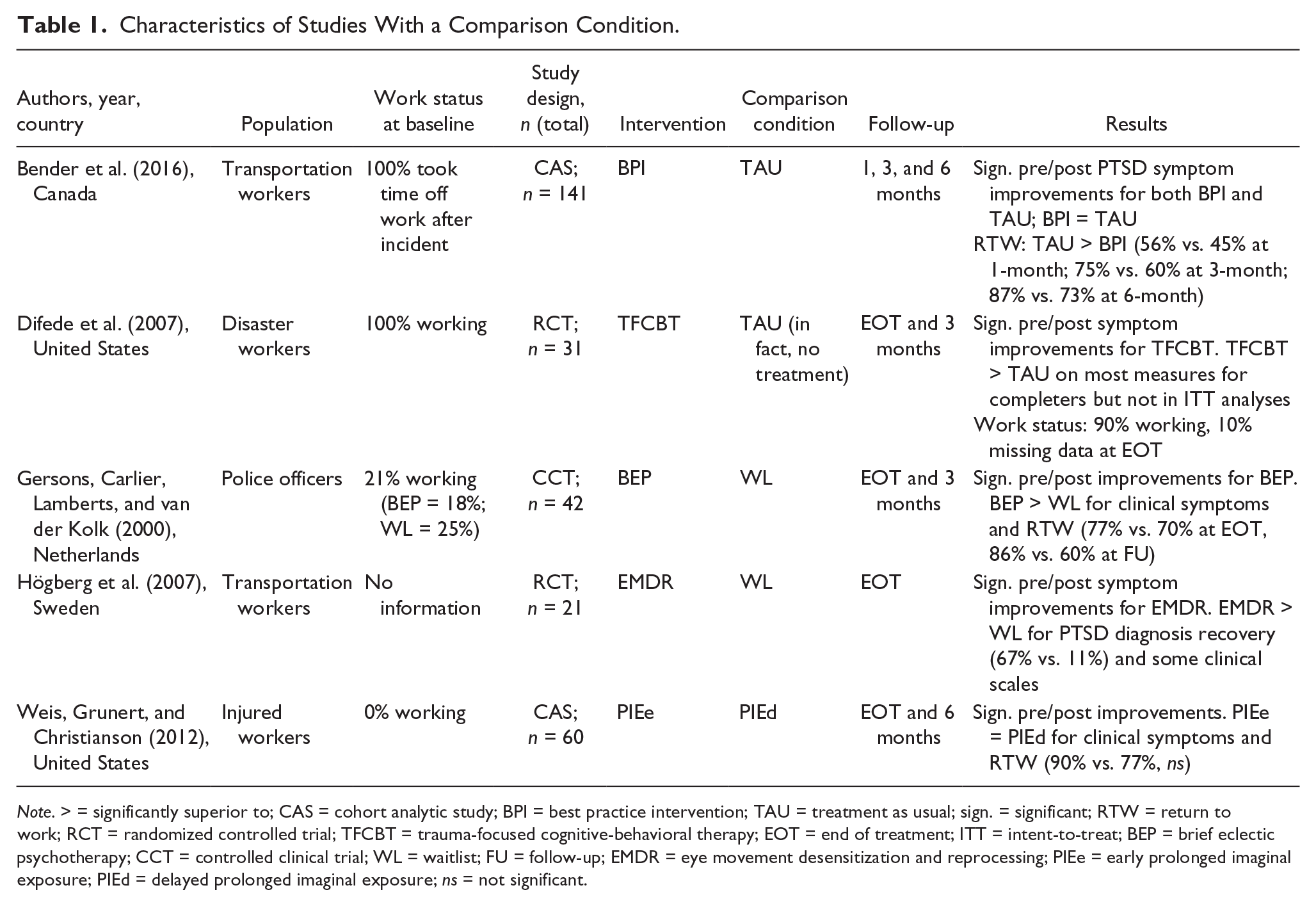
Note. > = significantly superior to; CAS = cohort analytic study; BPI = best practice intervention; TAU = treatment as usual; sign. = significant; RTW = return to work; RCT = randomized controlled trial; TFCBT = trauma-focused cognitive-behavioral therapy; EOT = end of treatment; ITT = intent-to-treat; BEP = brief eclectic psychotherapy; CCT = controlled clinical trial; WL = waitlist; FU = follow-up; EMDR = eye movement desensitization and reprocessing; PIEe = early prolonged imaginal exposure; PIEd = delayed prolonged imaginal exposure; ns = not significant.
Characteristics of Studies Without a Comparison Condition.
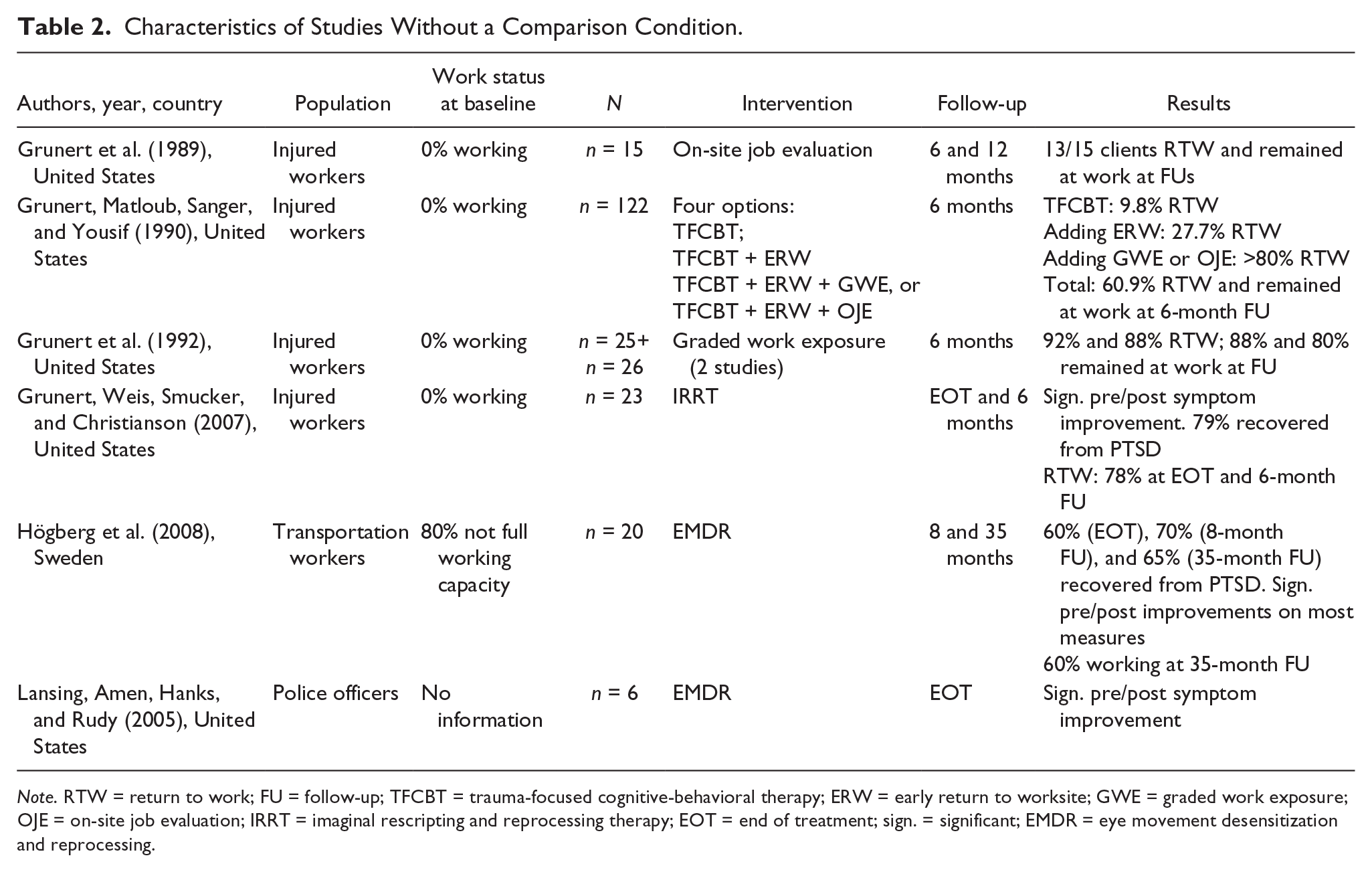
Note. RTW = return to work; FU = follow-up; TFCBT = trauma-focused cognitive-behavioral therapy; ERW = early return to worksite; GWE = graded work exposure; OJE = on-site job evaluation; IRRT = imaginal rescripting and reprocessing therapy; EOT = end of treatment; sign. = significant; EMDR = eye movement desensitization and reprocessing.
Participants
Study populations came from the United States, Canada, Sweden, and the Netherlands. Sample sizes ranged from 21 to 141 in studies that included a comparison condition, and from 6 to 122 in the cohort studies. Study populations included railroad personnel who had been involved in fatal accidents, assaults, or other traumatic events (three articles), police officers involved in shootings or other traumatic experiences (two articles), disaster workers exposed to the World Trade Center attack or its aftermath (one article), and individuals who had experienced severe upper extremity injuries at work (five articles, all from the same study group). For nine studies, the authors reported that their participants met criteria for a PTSD diagnosis or subthreshold PTSD, whereas two required the presence of posttraumatic distress (Bender et al., 2016; Grunert et al., 1989). Comorbidity was not extensively discussed: Six studies measured the presence of concurrent mental disorders (Bender et al., 2016; Gersons et al., 2000; Grunert et al., 2007; Högberg et al., 2007, 2008; Weis et al., 2012); major depressive disorder was an exclusion criterion for two studies (Högberg et al., 2007, 2008). In four studies, substance use disorder was an exclusion criterion for participation (Difede et al., 2007; Gersons et al., 2000; Högberg et al., 2007, 2008). About 80% to 100% of the participants were not working at baseline in most studies although work status was unknown for two articles. In one study, all participants were working at baseline (Difede et al., 2007).
Interventions
For most participants, the intervention included some form of exposure—either through revisiting trauma memories or through in vivo exposure to trauma reminders or both (Difede et al., 2007; Gersons et al., 2000; Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert et al., 1990; Grunert et al., 2007; Weis et al., 2012). While therapy protocols somewhat varied between studies, these interventions were categorized as TFCBT. EMDR was the treatment of choice in the remaining articles (Högberg et al., 2007, 2008; Lansing et al., 2005). One study (Bender et al., 2016) compared TAU with a “Best Practice Intervention” (BPI). For TAU, the workers underwent an assessment of their PTSD symptomatology; if clinically significant symptoms were detected, written information of these findings was sent to their family doctors who then proceeded with their usual care. The BPI involved (a) a standardized educational intervention (i.e., a Powerpoint presentation, a Response to Trauma booklet, and a PTSD fact sheet for family members), (b) referral to a multidisciplinary treatment program (including evidence-based PTSD treatment by a PhD-level psychologist, occupational therapy, physiotherapy, consulting psychiatric care, and return-to-work coordination), and (c) specialized return-to-work strategies in collaboration with the employer (i.e., in vivo exposure therapy, job site RTW coordination meetings, work accommodations, and regular contact during RTW and post-RTW). Psychology treatments could include any of the evidence-based interventions recommended in PTSD clinical practice guidelines (National Collaborating Centre for Mental Health, 2005), but were not described in greater detail.
Of note, four articles described interventions specifically targeting workers who had failed to RTW with the clinic’s standard TFCBT that involved coping skills training and imaginal exposure to their trauma memories (Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert et al., 1990; Grunert et al., 2007) In a series of three studies, Grunert and colleagues described specific interventions they developed after observing that, although their clients’ clinical symptoms had somewhat improved with TFCBT, they continued to struggle to return to the worksite where the injury had been sustained. Because the authors felt that this was due to ongoing symptoms of avoidance, they added worksite-specific exposure and coping skills training elements including (a) early return to the worksite by encouraging and coaching the clients to RTW during the first postinjury month; (b) graded work exposure by increasing working time and demands over several weeks, supported by weekly psychology sessions; and (c) on-site job evaluations that involved exposure to the workplace in the presence of the treatment team who coached the workers in using their coping skills during work activities and discussed work accommodations and limitations with the employer (Grunert et al., 1989; Grunert, Devine, Smith, et al., 1992; Grunert et al., 1990). In contrast, the fourth study was based on the assumption that a preceding prolonged exposure (PE) intervention was unsuccessful because PE primarily focuses on trauma-related fear but does not address other emotions such as anger, guilt, or shame. The authors believed that such emotions were predominant in the unresponsive clients, and that they would benefit from imaginal rescripting and reprocessing therapy (IRRT). IRRT has no worksite-specific elements but involves imaginal exposure plus development of a “mastery imagery” (a positive representation of the self as a competent survivor) to facilitate resolution of nonfear emotions.
In terms of the setting, three research projects were based at university medical centers (Difede et al., 2007; Gersons et al., 2000; Högberg et al., 2007, 2008) and in one case the employer facilitated the treatment that was conducted by therapists contracted with the employer (Lansing et al., 2005). Finally, for one study involving transit workers (Bender et al., 2016) and for all studies involving individuals with industrial injuries, the interventions were delivered within a regular WCB claim context. Follow-up periods varied; most of the follow-up assessments occurred between the end of treatment and 12 months posttreatment; one study (Högberg et al., 2008) had a 35-month follow-up.
Nine studies examined the effects of interventions on posttraumatic stress. All of them found that active psychotherapy effectively reduced symptoms from baseline through follow-up, with symptoms remaining stable or continuing to improve posttreatment. This was reported for samples of workers with and without physical injuries.
In addition, results from the three studies with no-treatment comparison conditions (Difede et al., 2007; Gersons et al., 2000; Högberg et al., 2007) suggested that active psychotherapy produced better outcomes than no treatment (although Difede et al., 2007, confirmed this in completers only but not in intent-to-treat analyses), with no-treatment groups showing little improvement over the (short) study periods. One nonrandomized retrospective study that compared two active exposure-based interventions (Weis et al., 2012) found that both groups significantly improved over time; PTSD symptoms decreased to a similar degree among clients receiving early imaginal exposure versus delayed imaginal exposure (with the timing depending on WCB referral patterns), but individuals who received early exposure required fewer sessions than individuals who received delayed exposure. In the nonrandomized study that compared a TAU approach with a BPI approach, both groups experienced significant decrease of PTSD symptoms throughout the 6-month study period with no statistical differences between groups at any time point.
Information on work status before and after the intervention is presented in Table 3. This information was available for nine articles; however, Grunert et al. (1990) was omitted from the table because the data overlapped with those from other studies, and Difede et al. (2007) was omitted because all participants were working at baseline. Four of the studies targeted workers who did not RTW with TFCBT; these studies are presented in the next section.
Work Status of Participants in Active Treatment Conditions Before Intervention and at Longest Follow-Up Time Point.
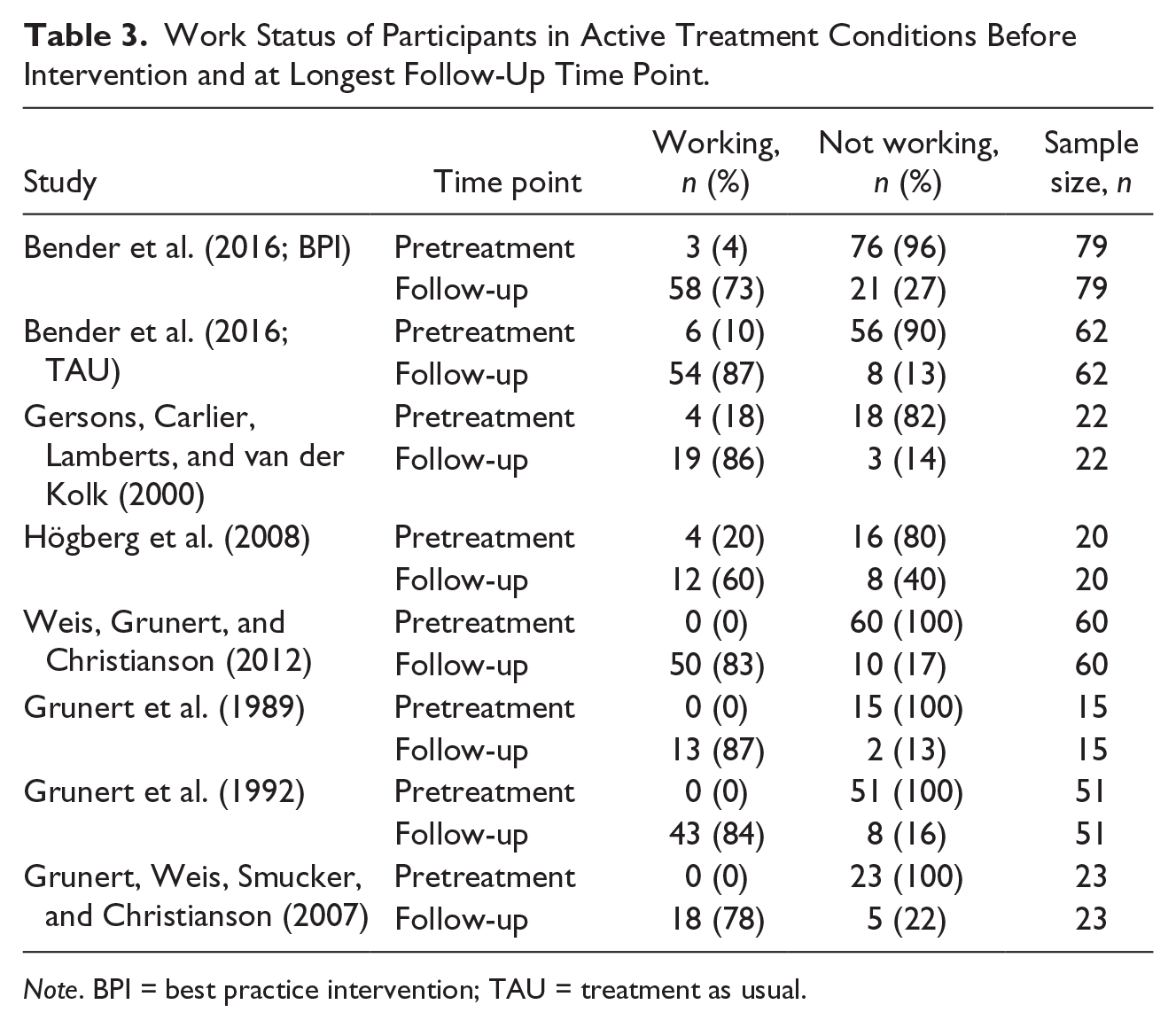
Note. BPI = best practice intervention; TAU = treatment as usual.
Högberg et al. (2008) reported that 60% of the transportation workers who participated in EMDR treatment were working about 35 months after the intervention. Gersons et al. (2000) reported that significantly more police officers were working 3 months after receiving brief eclectic psychotherapy compared with no intervention (86% vs. 60%). Weis et al. (2012) found no significant differences in RTW rates for two active exposure-based treatment conditions at 6- (and 12-) month follow-up. In contrast, Bender et al. (2016) reported that participants who received TAU had significantly higher RTW rates immediately after the trauma as well as at the 1-, 3-, and 6-month follow-up than participants who received BPI (10%, 56%, 75%, and 87% for TAU vs. 4%, 45%, 60%, and 73% for BPI).
Results of the binary random-effects model including RDs with confidence interval (CI) and heterogeneity test results are presented in Figure 2. RD calculations indicated that the proportion of participants who were working was 66.3% higher at the longest follow-up time point compared with the beginning of the study across the three studies (estimates = 0.663, 95% CI = [0.437, 0.890], p < .001). Overall, the findings suggested that psychotherapy interventions are beneficial for helping clients recover from PTSD symptoms and RTW.

Forest plot of risk differences for pretreatment versus posttreatment comparisons of proportions of individuals who were working at the time of the assessment.
The association of psychological distress and work status was examined in statistical analyses in only one study: Bender and colleagues found that participants who had not returned to work by the end of the 6 months follow-up period reported a significantly greater number of posttraumatic stress symptoms at all measurement time points (Bender et al., 2016). Furthermore, two authors noted that RTW was linked to reduction of PTSD symptoms (Högberg et al., 2008; Weis et al., 2012).
A total of four studies were conducted with workers who had failed to RTW after receiving TFCBT (Grunert et al., 1989; Grunert et al., 1990; Grunert et al., 2007; Grunert, Devine, Smith, et al., 1992), all of whom stemmed from the same clinic and had no control group. Three of the studies used worksite-specific interventions including early return to the workplace, graded work exposure, and on-site job evaluations (see interventions above). In an early study, Grunert et al. (1989) reported that 87% of their patients returned to their previous employment following an on-site job evaluation and have remained at work at the 6- and 12-month follow-up. In another study, 90% of the participants RTW with graded work exposure and 84% were still working 6 months later (Grunert, Devine, Smith, et al., 1992). In the third article, Grunert et al. (1990) described a decision tree developed to individualize interventions and optimize RTW outcomes: All workers who experienced posttraumatic stress after hand surgery were immediately referred to the psychologist. The standard psychology intervention involved coping skills training and imaginal exposure and reprocessing. For clients who did not RTW thereafter, early return to the worksite was initiated. If this remained unsuccessful, the clients received either graded work exposure (for those who were able to enter their worksite alone) or on-site job evaluation (for those who felt unable to enter their worksite). In a study using this strategy with 122 patients, the standard intervention yielded a low RTW rate (9.8%) but 27.7% RTW after adding early return to the worksite. Adding one of the two more structured workplace exposures resulted in 88.9% (for graded work exposure) and 83.3% (for on-site job evaluation) RTW rates. Overall, 60.9% of the patients RTW and remained at work 6 months later. The authors noted that graded work exposure and on-site job evaluation resulted in a temporary increase of PTSD symptoms, which required intervention before the patients were able to RTW full-time. In the fourth study where IRRT was used to treat workers who had failed to RTW, IRRT prompted improvements on all measures and 79% recovered from PTSD; 78% of the participants RTW at the end of the treatment and remained at work at the 6-month follow-up. The binary random-effects model to calculate the RD indicated that heterogeneity was low (τ2 = 0.0), Q(df = 2) = 0.539, p = .764, I2 = 0. Therefore, a binary fixed-effect model was calculated; the results (including RDs with CI and heterogeneity test results) are presented in Figure 3. RD calculations indicated that the proportion of participants who were working was 83.1% higher at the longest follow-up time point compared with the beginning of the study across the three studies (estimates = 0.831, 95% CI = [0.754, 0.909], p < .001).

Forest plot of risk differences for pretreatment versus posttreatment comparisons of proportions of individuals who were working at the time of the assessment.
Discussion
Discussion of Results and Limitations
The purpose of this study was to summarize the evidence base for interventions targeting individuals with work-related PTSD to make best practice recommendations for professionals involved in their rehabilitation, help workers to recover and RTW, and guide future research in this area to advance treatment development. A number of relevant and specific conclusions for future research can be drawn from the available evidence base. However, a number of limitations need to be considered when discussing clinical recommendations. First, the scientific literature base reporting on interventions for work-related PTSD is generally very limited. Although we included a search of gray literature, we may have missed studies. Given the already limited number of studies, we also did not examine potential for publication bias (e.g., using funnel plots). Second, few large and well-designed studies with representative samples are available that evaluate the effects of such programs in this particular population. This is surprising in view of the abundance of studies conducted with other PTSD populations, which form the basis for clinical practice guidelines in many countries. Because we aimed at illustrating the current state of the literature, we opted for inclusion rather than exclusion of studies; however, this resulted in inclusion of studies with a moderate risk of bias. Conducting an appropriate quality assessment was somewhat challenging. We selected the McMaster University QAT for Quantitative Studies because it has been recommended for use in systematic reviews that include nonrandomized intervention studies and studies without a comparison group (Deeks et al., 2003); however, we found that its criteria were somewhat more arbitrary than, for example, those of the Cochrane Collaboration. While information on settings often lacked details, most of the identified studies appeared to be conducted under natural clinical conditions and five occurred in a WCB claim context. Still, many study samples were not fully representative of the target population.
Despite these limitations, the following clinical recommendations can be made, although they may be refined with further research: Of those psychotherapy interventions that have been recommended for the treatment of PTSD in evidence-based clinical practice guidelines, TFCBT and EMDR have been used thus far to treat individuals with work-related PTSD. RTW rates in all studies increased over time with TFCBT and EMDR, and generally lay between 58% and 80% across follow-up time points. Brief eclectic psychotherapy (which was categorized as a TFCBT) resulted in higher RTW rates than the waitlist condition (Gersons et al., 2000), suggesting that TFCBT may be superior to no treatment in helping clients RTW. Different exposure-based interventions produced similar RTW outcomes when compared with each other (Weis et al., 2012). Contrary to expectation, a study comparing TAU with a multidisciplinary assessment and treatment program that followed best practice recommendations (BPI) found that TAU produced much higher RTW rates and similar declines in PTSD symptoms throughout the study period compared with BPI (Bender et al., 2016). While the authors of this study cited a number of challenges (e.g., randomization of participants was not acceptable by the employer, difficulties recruiting participants, lack of union support) and withheld important information, particularly related to details of both interventions (e.g., content, frequency, duration, intensity, etc.), the study underlines the need to include an active and relevant control group when researching treatment approaches for workers with PTSD.
Overall, our findings provide preliminary evidence that TFCBT and EMDR are effective for helping individuals with work-related PTSD RTW, although studies are needed that replicate these results in larger and more representative samples of clients. Research evaluating understudied programs and protocols would be valuable toward clarifying the extent to which the findings can be generalized to other evidence-based interventions for PTSD. For example, some key TFCBT protocols (e.g., cognitive processing therapy, PE, and CT for PTSD) and other non-TFCBT programs (e.g., stress inoculation training) have not yet been tested in individuals with work-related PTSD. Furthermore, the content and effectiveness of current TAU approaches should be investigated.
Meta-analytic research suggests that the majority of PTSD treatment study participants continue to experience substantial posttreatment symptomatology across trials, with only 44% of participants who entered treatment and 54% of those who completed treatment demonstrating “clinically meaningfully improvements” of their symptoms (Bradley et al., 2005). Consistent with this, several articles included in our review had found that workers did not RTW after receiving an intervention that appeared to be delivered in line with best practice recommendations. Open questions remain as to how these individuals should be treated. The evidence compiled in our review suggests that they can benefit from worksite-specific in vivo exposure interventions such as an early return to the workplace, graded work exposure, and on-site job evaluations. Unfortunately, all of the associated studies were conducted with the same population (injured workers), which limits the generalizability of their results. However, the rationale for this treatment approach is strong. Individuals who were traumatized at work report avoiding their workplace to prevent triggering recollections of the trauma and reoccurrence of similar traumatic events (MacDonald et al., 2003). Although many PTSD therapies include recommendations for clients to engage in in vivo exposure to situations that are being avoided, they often provide little instructions as to how to proceed with clients who do not comply with this homework. The treatment of individuals with work-related PTSD may require special adaptations of standard PTSD interventions. For example, worksite exposure programs for individuals with hand injuries have been conducted by a team consisting of a psychologist and a hand therapist (Grunert et al., 1989), and multidisciplinary teams are generally recommended for complex RTW processes (Rose, 2006; Strauser, 2008). For individuals without physical injuries, the team may include a psychologist and an occupational therapist (OT) who has been trained in delivering in vivo exposure interventions. The OT could supervise the clients’ in vivo exposure homework and accompany them to the workplace if necessary. In addition, the psychologist could use imaginal techniques by guiding clients to visualize successful RTW or real-life situations at the workplace, or cognitive restructuring to address workplace-related threat appraisals. In other cases, the OT may need to discuss modifications of the workplace with the employer (e.g., installation of surveillance cameras) to improve factually unsafe conditions. However, the differential effects of imaginal exposure versus in vivo exposure among individuals with work-related PTSD has not yet been explored.
Implications for Research
More well-designed clinical trials are sorely needed to move the field forward and develop guidelines and algorithms for the treatment of individuals with work-related PTSD. This will require the inclusion of large representative samples from a variety of practice settings (e.g., multiple community and/or WCB clinics) and studies using a pragmatic design. Research examining the association of clinical symptoms and work status would also be valuable to promote better understanding of this issue. Furthermore, it is important that exclusion criteria are limited to factors that contraindicate the use of a particular treatment in a conventional setting. For example, exclusion of individuals with substance use disorders or major depression (as reported in several studies included in this review) appears inadequate in view of the inherent comorbidity of PTSD with other mental disorders (Spinazzola, Blaustein, & van der Kolk, 2005), recent research suggesting that exposure treatment can be safely applied in individuals with a variety of comorbidities (van Minnen, Harned, Zoellner, & Mills, 2012), and the fact that effective integrated treatment programs exist for individuals with PTSD-related comorbidities (e.g., Torchalla, Nosen, Rostam, & Allen, 2012). Indeed, in a Canadian study among workers referred to a WCB-based psychological trauma program, the presence of comorbid psychiatric diagnoses was strongly associated with not working at the time of assessment (Hensel, Bender, Bacchiochi, & Dewa, 2011).
Particular attention needs to be paid to individuals who fail to RTW after receiving standard PTSD interventions. Although three of the four articles examining this population recommended workplace exposure interventions, it remains unclear to date if such an intervention is necessary and optimal. Indeed, the fourth article proposed that these individuals benefit from interventions that address non-fear emotions. Identifying the factors that predict failure to RTW following treatment and testing different treatment approaches will be essential for future work.
Furthermore, studies examining the effects of medication for individuals with work-related PTSD as a stand-alone treatment and in combination with psychotherapy would add much-needed knowledge to the field. Of the Canadian workers involved in a WCB claim, 55% received anxiolytic/hypnotic–sedative medication for their PTSD (MacDonald et al., 2003) despite lack of evidence for the effectiveness of these agents (Ipser & Stein, 2012). On the contrary, workers with depression and anxiety expressed concerns that the side effects of psychotropic drugs affected their ability to function at work and made them liable to accidents and reported frequent noncompliance with the medication due to side effects (Haslam, Atkinson, Brown, & Haslam, 2005; Haslam, Brown, Atkinson, & Haslam, 2004). Thus, although some antidepressants have been shown to be efficacious in treating PTSD (Stein et al., 2006), research examining their side effects on work performance (e.g., operating machinery, driving vehicles, working from heights etc.) would be valuable.
When studying treatment programs for work-related PTSD, comparison conditions should be clinically relevant alternative (e.g., briefer, less expensive, or usual) treatments rather than no interventions because this does more accurately reflect the situation faced by administrative decision makers. Although RCTs provide the highest level of evidence, randomization may not be feasible or acceptable in community settings. Alternative designs have been suggested such as interrupted time series and delayed treatment design (Glasgow, Magid, Beck, Ritzwoller, & Estabrooks, 2005), although delay of treatment may not be feasible if such a study is conducted in a WCB context. In addition to established PTSD symptom scales, outcome measures should include information on work functioning (e.g., work status, working capacity, reasons for not working). Economic considerations are also critical for WCBs and administrative decision makers; therefore, studies should provide some information related to the cost of delivering the intervention, cost-benefit analyses, or other economic outcomes. Finally, long-term follow-up periods are important to establish if individuals who RTW stay at work.
Recommendations and Conclusions
At this point, the following recommendations can be made to administrative decision makers and health professionals involved in the rehabilitation of individuals with work-related PTSD: In the first step, workers should be referred to a treatment provider in the community who is trained in delivering interventions that have been identified as first-line interventions for PTSD. At this point, preference should be given to exposure-based and EMDR protocols. If such an intervention failed to result in RTW, case managers should refer the worker to a more intensive and multidisciplinary treatment program that includes work-specific exposure elements. That said, it is critical not to discount the rather limited state of the existing body of literature because these recommendations may be refined with further research. There is no research available from which to infer recommendations for the treatment of individuals who were not able to RTW after completing such an intensive program. It is possible that the best solution for them is vocational rehabilitation given that the value of work for mental health and recovery has been documented (Waddell, Burton, & Kendall, 2008). Treatment can help identify clients’ strengths and ongoing barriers to be considered when searching for appropriate work and can support them in leading a productive life even if they do not RTW.
Generally, case managers also need to be aware that workers with PTSD may present with complex conditions as traumatic experiences may result in subsequent substance abuse, chronic pain, suicidality, or exacerbation of an existing mental disorder. Conversely, preexisting factors such as prior trauma, psychiatric comorbidities, and childhood abuse have been shown to increase the risk for developing PTSD following trauma exposure (Brewin, Andrews, & Valentine, 2000), make PTSD treatment difficult, and be associated with poorer treatment outcome (Hembree, Marshall, Fitzgibbons, & Foa, 2001; Schottenbauer, Glass, Arnkoff, Tendick, & Gray, 2008). Case managers need to be prepared that comprehensive treatment of these concurrent (non-claim-related) conditions may be necessary to achieve optimal outcome for the claim-related PTSD, which may require more intensive and interdisciplinary interventions compared with the treatment of a single workplace incident. In addition, other factors may complicate RTW including conflicts with employers/coworkers, lack of appropriate and acceptable modified work conditions, lack of appropriate response to the workplace incident (e.g., increasing workplace safety), legal factors, and so forth.
Given the high prevalence of trauma at the workplace, the chronicity of PTSD, and its disruption of many areas of functioning, additional research is clearly required to determine what can help individuals with PTSD to recover and RTW. Particular attention should be devoted to recruiting large representative samples, using pragmatic study designs and clinically relevant comparison conditions, evaluating understudied psychotherapies and medications, measuring work-related and cost-related outcomes, using long-term follow-up periods, and identifying factors that predict failure to RTW following treatment.
Footnotes
Acknowledgements
The authors thank Rebecca Lam, BKin, MOT for her feedback on the first version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.