
Abstract
Many adolescents with developmental disabilities do not learn the safety skills needed to maintain physical well-being in domestic and community environments. Literacy-based behavioral interventions (LBBIs) that combine print, pictures, and behavioral rehearsal are effective for promoting acquisition and maintenance of self-care skills, but have not been investigated as safety skill intervention. Also, LBBIs have primarily been implemented by teachers and other professionals. In this study, a peer partner was taught to deliver an LBBI story to students so they would learn to perform a basic first aid routine: cleaning and dressing a wound. Results showed that students’ accuracy with the first aid routine increased after a peer delivered the LBBI instructional package, and maintained after the peer stopped delivering it. This study demonstrates the effectiveness of the LBBI instructional package for teaching first aid safety skills, and extends previous research showing the efficacy of peers in delivering this intervention.
Students with developmental disabilities often require explicit training in the personal safety skills required to maintain physical well-being, but training these skills is frequently overlooked by educators and caregivers (Dixon, Bergstrom, Smith, & Tarbox, 2010). Agran and Krupp (2010) noted that “many teachers and parents have assumed that students with disabilities either have these skills or are incapable of learning them if they do not” (p. 304), even though other daily living and personal skills are frequently integrated into students’ curricula. The absence of safety skills training leaves students with developmental disabilities vulnerable to household injuries and accidents. In a meta-analysis and systematic review of the literature, Shi et al. (2015) sought to determine whether children with disabilities are at a greater risk of injury than children without disabilities. Shi et al. discovered that children with developmental disabilities are significantly more at risk of unintentional injuries than their typical peers. This risk also increases with age.
Safety skills refer to a wide variety of skills needed to maintain physical well-being, including routines such as crossing a street, responding to a house fire, and contacting emergency services (Collins, Wolery, & Gast, 1992; Dixon et al., 2010; Garcia, Dukes, Brady, Scott, & Wilson, 2016). One class of safety skills, basic first aid, has long been identified as an essential skill set required for people with disabilities to live independently (Collins et al., 1992). Knowing how to prevent accidents and how to respond if faced with an emergency, either at home or in the community, is necessary to function as independently as possible (Ozkan, 2013). Incorporating first aid skills into education and habilitation programs facilitates independent living during adulthood.
Researchers have demonstrated that students with developmental disabilities are capable of learning a wide range of complex first aid skills when these skills are explicitly taught by educators. Procedures for teaching first aid skills include individual training (Spooner, Stem, & Test, 1989), interactive storytelling (Marchand-Martella, Martella, & Marchand, 1991), backward chaining (Gast, Winterling, Wolery, & Farmer, 1992), peer teaching and tutoring formats (Marchand-Martella et al., 1992), small group instruction (Timko & Sainato, 1999), and peer and self-video modeling (Ergenekon, 2012; Ozkan, 2013). These teaching procedures incorporated explicit and didactic instruction, and the majority were delivered by adults.
Another teaching procedure that has shown promise for teaching self-care skills and routines to students with autism and intellectual disability (ID) involves the use of literacy-based behavioral interventions (LBBIs). LBBIs provide a literacy context with print or pictures, along with discrimination training and rehearsal, to guide instruction within a storytelling environment (Bucholz & Brady, 2008). LBBI is a term that describes an assortment of interventions that uses pictures, written scripts, and stories, along with behavioral rehearsal of the routines and stories in a step-by-step format, to teach novel tasks. As an “umbrella” term, LBBIs include social narratives (Collet-Klingenberg & Franzone, 2008), comic strips (Daly & Ranalli, 2003), social scripts (Krantz & McClannahan, 1998), picture activity schedule books (Spriggs, Gast, & Ayres, 2007), and Social Stories™ (Gray, 1998). All these interventions have multiple instructional components that incorporate some form of visual aid to supplement explicit written directions, and most rely on behavioral rehearsal to increase learners’ opportunity to practice and gain performance feedback. Teachers, parents, and other adults have used these LBBI storybook packages to teach novel skills to preschool students, elementary students, and secondary students with developmental disabilities. LBBI storybooks have been used to teach employment skills (Bucholz, Brady, Duffy, Scott, & Kontosh, 2008), independent living skills (Brady, Hall, & Bielskus-Barone, 2016), adaptive daily living skills and routines (Brady, Honsberger, Cadette, & Honsberger, 2016), and self-regulation skills (Hall, Brady, & Morris, 2017).
Although the majority of these and similar investigations have relied on teachers, job coaches, or parents to provide the intervention (Kokina & Kern, 2010; Styles, 2011), one recent iteration of the LBBIs has included delivery of the storybook and rehearsal activities, facilitated by a peer (Brady, Hall, & Bielskus-Barone, 2016; Brady, Honsberger, et al., 2016). Brady, Honsberger, et al. (2016) reported results from the first study that examined the effect of peer-mediated LBBIs on skill acquisition. The researchers investigated an LBBI delivered by peers to teach adolescents with autism the daily living skills involved in making a sandwich. Students and their peer partners jointly reviewed a storybook, where each page presented a single step of the task analysis accompanied by a picture of the step presented from a personal point of view. As students reviewed the storybook, the peer pointed to the words and pictures, paused while the students practiced the activities on the page, and then reinforced students for accurately playing out the activities on the page. The students’ sandwich-making accuracy significantly increased after reviewing the LBBI with the peer, and maintained after the LBBI was withdrawn. In a school-based follow-up study, Brady, Hall, and Bielskus-Barone (2016) investigated peer-mediated LBBIs to teach handwashing to elementary-aged children with severe disabilities. Each student was paired with a different peer who completed a read-along of the student’s storybook, and mediated the point, pause, rehearse, and reinforce routine. Accuracy of the self-care skill increased significantly after reviewing the handwashing storybook and participating in the support activities with a peer. As in the first study, the accuracy of the skills maintained after the LBBI was removed. In addition, the students’ newly acquired skills showed signs of generalization when the students began washing their hands at novel sinks that had never been part of the training routine.
The purpose of this study was to determine the effectiveness of a peer-mediated LBBI to teach a first aid safety routine, cleaning and dressing a wound. This study was designed to explore further the LBBI research by examining the impact of LBBI instructional packages on safety skill acquisition. The study also provided a further exploration of the role of peers in delivering the multiple components of an LBBI instructional package for skill acquisition and maintenance. Two research questions were asked:
Method
Participants
Three adolescents (aged 15-17) with developmental disabilities who attended a public charter school for students with autism spectrum disorder (ASD) participated. All students were diagnosed with ASD as their primary eligibility category, and this was noted on their Individual Education Programs (IEPs). All three students also scored below average on standardized IQ tests, and all had an additional diagnosis of a speech and/or language impairment indicated on their IEPs. Each student received daily language therapy; Tim also received weekly speech therapy, and Derek received weekly occupational therapy. Each of the students communicated verbally—Randy and Derek via two- to three-word utterances with frequent echolalia, and Tim via full sentences. Tim and Derek were in the 10th grade and attended the same classroom. Randy was in 11th grade in a different classroom. Each of the students participated in a high school diploma program via Access Points (i.e., in a “special diploma” curriculum track). Reading comprehension for all three students was at the first-grade level.
A fourth student, Miguel, served as the peer facilitator for all the target students. Miguel was enrolled in the same school and also had a primary eligibility of ASD designated on his IEP. Miguel was in 11th grade and working toward a standard high school diploma. Miguel was known to the target students and had interacted with them prior to the study during lunch and other activities at the school. Miguel was chosen as the peer facilitator due to his ability to read at or near grade level, his ability to follow adult directions, and his interest in participating.
All students provided verbal and written assent to participate in the study. Parents of all students provided written consent prior to the beginning to the study, and the study received formal approval from the university’s human subjects review board. A summary of participant characteristics is presented in Table 1.
Participant Characteristics.
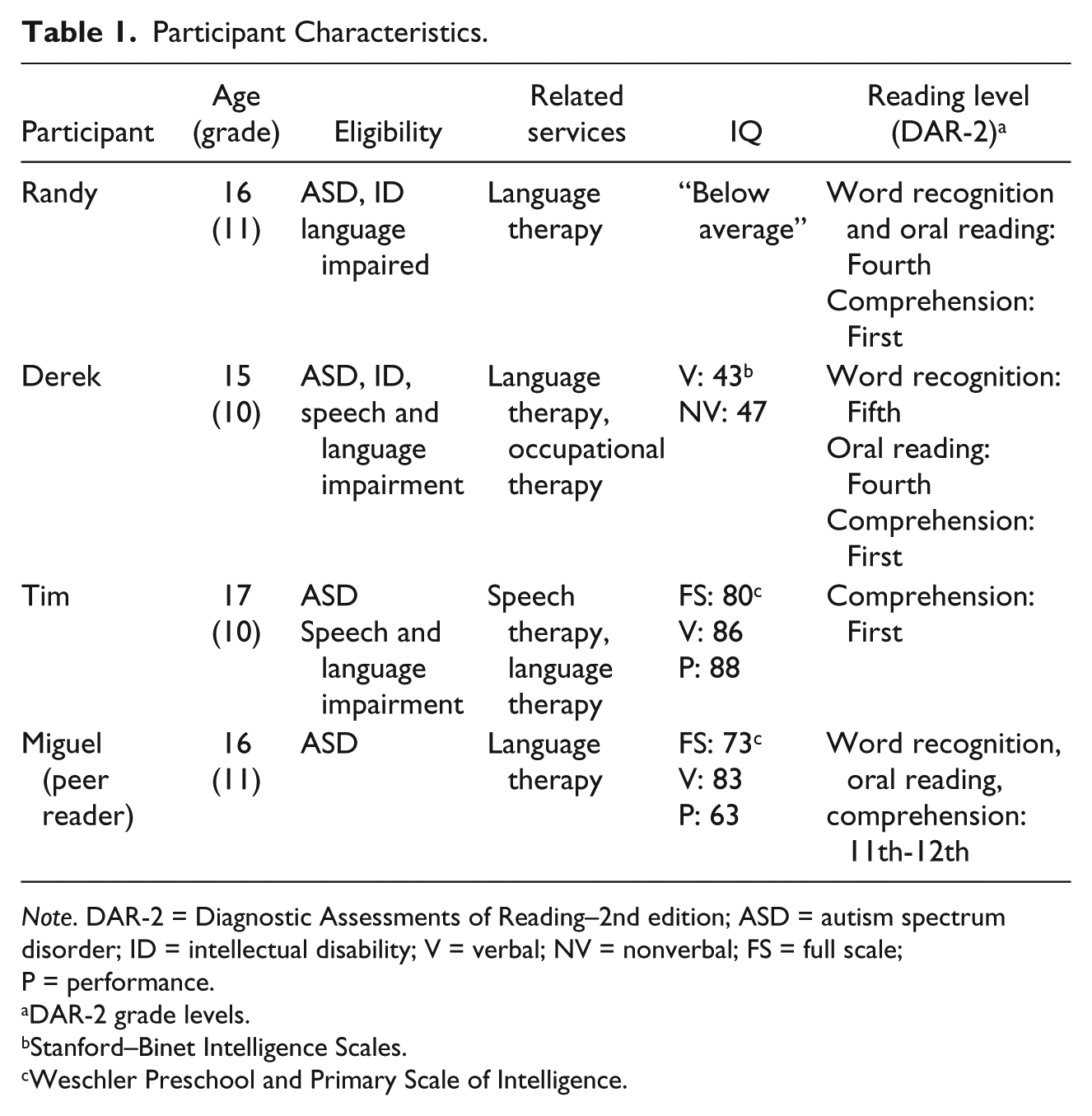
Note. DAR-2 = Diagnostic Assessments of Reading–2nd edition; ASD = autism spectrum disorder; ID = intellectual disability; V = verbal; NV = nonverbal; FS = full scale; P = performance.
DAR-2 grade levels.
Stanford–Binet Intelligence Scales.
Weschler Preschool and Primary Scale of Intelligence.
Task and Setting
First aid skills were identified as a needed area of instruction for all participants. An assessment of the first aid routine was conducted prior to initiating the study. During this assessment, students were asked to help an adult with a simulated wound by cleaning and dressing the wound. All bandaging materials were on a cafeteria table, and the request was initiated by the adult pointing to the wound and saying, “I’m hurt. Can you help me?” During this preexperiment assessment, none of the target students were able to complete the first aid routine independently. Based on these results, instruction on the first aid routine was deemed important. Cleaning and dressing a wound is commonly taught in first aid classes because most other first aid skills build upon this routine, and it is a skill required to live independently. No other first aid skill training was provided in these students’ curriculum. (Details of this task are provided in the “Behavioral Measure” section.)
All instruction took place in the school cafeteria based on the schedule and availability of the cafeteria, and the presence of a sink needed to complete the routine. The cafeteria was approximately 100 × 100 ft square with tables, attached benches, a sink, a washer and dryer, several microwaves, and a stove. Although the cafeteria was used for instruction and meals throughout the day, no other students or staff were present during the study. All materials needed to complete the first aid routine were stored in a first aid kit located on a counter in the cafeteria. All baseline, intervention, and maintenance observations took place in this setting.
Behavioral Measure
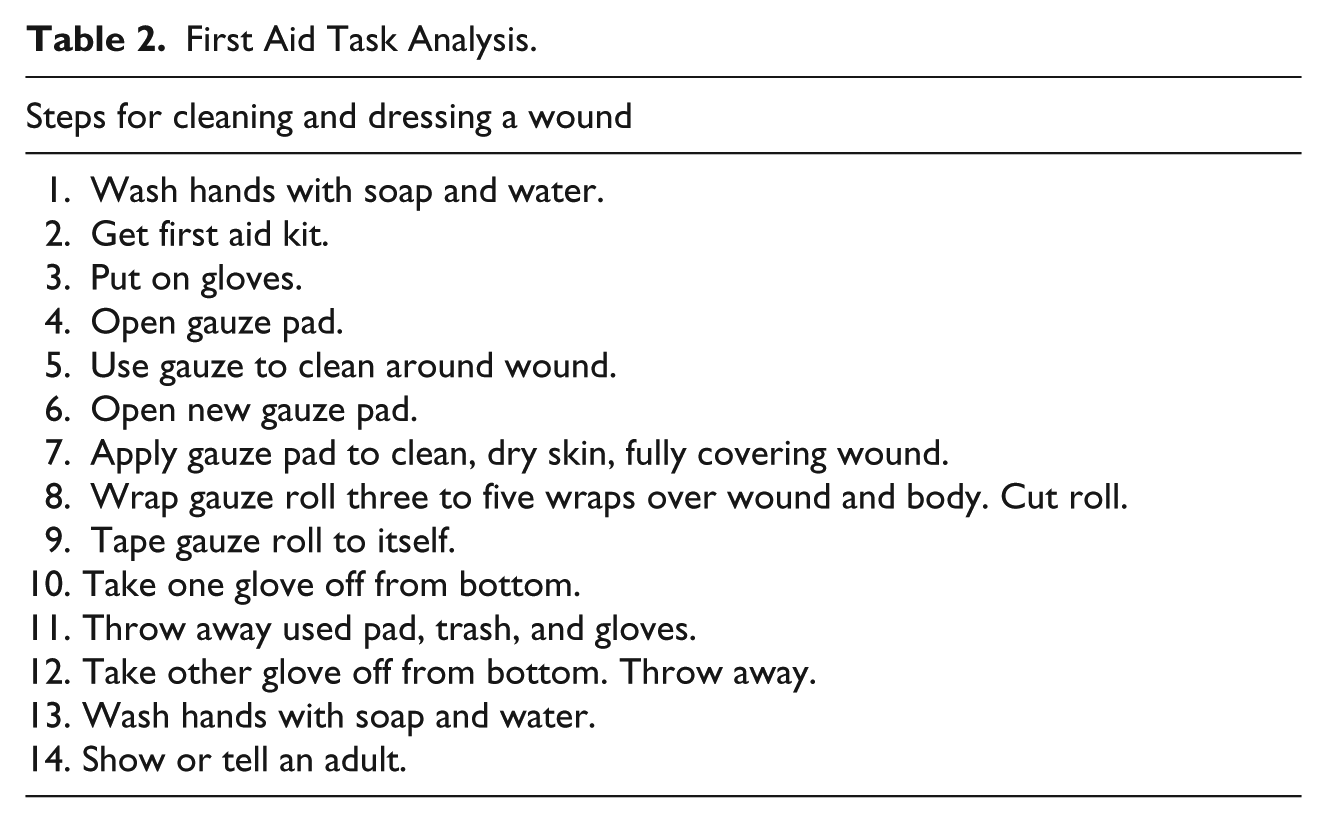
A task analysis was created for the first aid skills of cleaning and dressing a wound on another person. The task analysis was comprised of 14 steps (see Table 2), incorporating a consensus protocol based on the 2015 guidelines for basic first aid (American Safety & Health Institute, 2016; Singletary et al., 2015). Data were collected individually for each student while observing the student clean and apply gauze to a simulated wound on the peer facilitator. Each step was scored by a data collector as (a) correct and independent, (b) correct but required a prompt from the peer, or (c) no attempt made. A prompt was delivered to the student only in response to the student making an error, or not initiating a step within 30 s. A prompt was defined as the peer facilitator delivering feedback to the student to “remember what the story said” while turning to the page in the story, and then reading the page again. Steps of the task analysis did not necessarily have to be performed in order; however, some steps required completion in sequence. For example, students had to retrieve the first aid kit prior to putting on gloves or opening a gauze pad; however, handwashing could occur before or after getting the kit.
First Aid Task Analysis.
Data Collection and Interobserver Agreement (IOA)
Data were collected by one of two observers using paper data sheets created by the authors. The two observers were experienced teachers currently enrolled in a graduate program in special education. A third observer collected data for IOA purposes, and was a staff member at the school. All observers were trained to use the data sheets prior to beginning the study. To determine IOA, data were collected live and concurrently by two observers during 38% of all sessions. These agreement sessions were conducted in 33% of baseline, 43% of intervention, and 50% of follow-up sessions for Randy (42% overall); 33% of baseline, 33% of intervention, and 50% of follow-up sessions for Derek (39% overall); and 25% of baseline, 33% of intervention, and 50% of follow-up sessions for Tim (36% overall). Agreement was determined by counting the steps of the task analysis scored the same by both observers, and dividing that number by the total number of steps observed, then multiplying by 100. Agreement between the two observers across all students and sessions (combined) was 99%. For individual students across conditions, agreement was 99.6% for Randy, 97.6% for Derek, and 100% for Tim.
Experimental Design
A multiple baseline design across participants was used to determine the effects of the LBBI instructional package. The design used multiple probes during baseline to prevent exposure to extended inaccurate practice of the skills before the intervention (Kennedy, 2005). Follow-up observations were held after the intervention was removed to assess potential maintenance of the learning.
Data Analysis
Data were analyzed first using traditional visual inspection procedures. Next, data were summarized by calculating measures of central tendency and ranges for each student’s dependent measure during baseline, intervention, and follow-up. Additional attention was paid to direction, trend, and level of the data in each condition. These data are reported using a modified format recommended by Gast and Spriggs (2014). Condition changes were made based on the level and trends of individual data points. The decision to move from baseline to intervention was based on multiple data points showing low and stable performance. The decision to move from intervention to follow-up was more specific. Each student showed a minimum of four consecutive sessions with 86% or more of the steps correct and independent prior to ending the intervention.
Two post hoc analyses were conducted to supplement the visual inspection procedures for the graphed data. For a nonoverlap index, we calculated the percent of nonoverlapping data (PND) for each student. This established separate indices for baseline-to-intervention and baseline-to-follow-up conditions for each student. Although there is little consensus regarding effect size and nonoverlap procedures for single subject research (Ledford, Wolery, & Gast, 2014), PND is frequently advocated because it (a) honors the logic of single subject research designs, (b) shows consistency of effects across participants instead of as a cumulative effect, and (c) is appropriate for baselines that do not show data outliers. For a true effect size estimate, we also calculated a Tau-U coefficient (Parker, Vannest, Davis, & Sauber, 2011). Tau-U provides a single, omnibus effect size based on the weighted average of each participant’s baseline and intervention differences. For this analysis, we used the Tau-U web-based calculator (Vannest, Parker, Gonen, & Adiguzel, 2016). These calculations included only the baseline to intervention effect, and did not include the baseline to follow-up or intervention to follow-up contrasts.
Social Validity
The investigators developed a social validity measure to evaluate the perceptions of professionals and students on the LBBI as an instructional strategy (five items) and on students’ ability to perform first aid (three items). The survey contained eight items for teachers and three items for students. Teachers were provided with the survey, asked to circle the answer that best represented their perceptions, and then return the instrument to an investigator. For the students, an investigator read the items to each student individually, and asked them to respond by telling their response or circling the response on the survey. Response options for each item on the professionals’ instrument were based on a 4-choice scale (strongly agree, agree, disagree, strongly disagree with a not sure option). For the students’ survey, response options were based on a 4-point scale (absolutely, kind of, not really, no way), with an emoticon accompanying each choice. The social validity assessment was conducted 16 weeks after the last follow-up observation. Four professionals participated in the social validity evaluation including the two teachers who taught the students, and a paraprofessional and behavior analyst who worked with the students and teachers. All the four participating students (including the peer facilitator) responded to the student survey. Data analysis included calculating means for each item.
Development of the LBBI
After creating the task analysis of cleaning and dressing the wound of another person, an LBBI storybook was created. The storybook contained 15 pages, one page matching each step of the task analysis, plus one cover page. Each page contained one simple sentence written in first person, and one matching photograph. For example, on the first page was written “I wash my hands with soap and water” and had a matching photograph of hands under a sink faucet. The photographs were taken by the data collectors prior to baseline; all photographs were taken from the student’s point of view, within the school cafeteria. The words in the sentences on each page were printed in Franklin Gothic Book size 44 font, and the photographs were approximately 6 × 8 inches. The length of the sentences ranged from four to 15 words on each page. The pages were assembled into a one-inch, three-ring binder. See Figure 1 for a sample page from the LBBI storybook.

Sample page from LBBI storybook.
Experimental Procedures
Baseline
During baseline, the peer facilitator was present in the room, but did not interact with the participating students. The peer had a simulated cut on his forearm created by making a 2-inch mark with a red felt-tip marker. An investigator gestured to the cut and said to the student, “He’s hurt. Can you do first aid?” No additional assistance was provided to the student (or the peer) during baseline. A baseline session ended if students did not initiate any steps of the first aid routine after 30 s, or if they indicated verbally or physically that they were done helping.
Peer training
Before beginning the intervention with the students, an investigator taught the peer to use the LBBI with students to show them how to implement a first aid routine to clean and dress a wound. Peer training was conducted over 2 days, for approximately 20 min each day. The peer was taught to read the sentence on each page of the storybook, point to the picture, gesture to an item, and provide praise after the student completed each step correctly. Before implementing the LBBI procedure with any of the students, the peer performed these steps for each page of the storybook with the investigator, and demonstrated the ability to implement the intervention accurately. When the intervention was delivered with each student, the peer rehearsed the intervention steps with the investigator daily, prior to the participants entering the room. However, no formal data were collected on fidelity of the LBBI delivery by the peer reader.
Intervention
When the intervention was implemented, the peer sat next to each participating student, and held the book in front so they could both see each page. As a storybook-based intervention, the LBBI was designed to be delivered as a table-top activity, without the interruption that would ensue from students moving to various locations to obtain materials, use the sink, clean up, and so forth. It should be noted that the LBBI in this study was a multicomponent intervention. From previous LBBI research with people with ID (Brady, Hall, & Bielskus-Barone, 2016; Brady, Honsberger, et al., 2016; Bucholz et al., 2008), effective interventions included the written and pictorial presentations, combined with activities to draw attention to difficult steps (i.e., a precorrection procedure). These activities typically include pointing out materials or routines that are unfamiliar to the students who receive the LBBIs (e.g., gauze, cleaning the wound). Effective interventions also include behavioral rehearsal prior asking the students to perform the routine independently. In this study, these LBBI components were delivered in the following way. First, the peer read aloud the sentence on each page, pointed to the picture, and then gestured to designated items (e.g., gloves, gauze pad). When the peer finished reading the story, the investigator gestured to the simulated cut on the peer and said, “He’s hurt. Can you do first aid?” If the student did not initiate a step within 30 s, an investigator asked the peer to go to the corresponding page in the storybook and prompt the student with, “Remember what the story said.” The peer then reread the sentence, pointed to the picture, and requested the student to perform the step again. If the student responded but made an error on a step, the same correction was provided, but the correction was prompted by the peer without an investigator prompt.
Because the improvements with Randy were slow and variable, after six intervention sessions, the LBBI procedure was enriched by adding an error correction procedure delivered by the peer that included more explicit rehearsal. This error correction procedure consisted of (a) opening the LBBI to the corresponding page, (b) saying “Remember what the story said,” (c) reading the sentence, (d) pointing to the picture, and (e) asking the student to rehearse the step. To rehearse, the peer began to perform the step, and then stopped and asked the student to complete the remainder of the step. For example, if the error involved opening the wrapper of a gauze pad, the peer initiated the rehearsal by creating a small tear in the wrapper, and then asking the student to finish opening the gauze pad. For the step of handwashing, full rehearsal was not requested, but the peer prompted the students either to point to the sink or to verbalize, “Wash hands.” Full rehearsal did not enable students to go to the sink and wet their hands because they would perform the whole routine immediately after practicing.
To maintain consistency of the intervention across all the students, the correction procedure also was added to Derek’s LBBI on Session 11. Because Session 11 was Tim’s first day of intervention, all his intervention sessions included the correction procedure as part of his LBBI. Based on the results displayed by Randy and Derek, this minor modification was made to the LBBI for Tim (the third student). All other elements of the LBBI implemented with Randy and Derek remained the same for Tim.
Follow-up
During the follow-up condition, the LBBI was removed to determine whether any of the skill improvements would maintain in the absence of the intervention. The criterion for removing the LBBI was successful completion of 12 of the 14 steps (86%) for four consecutive sessions. The LBBI was removed after 14 intervention sessions for Randy, 12 sessions for Derek, and six sessions for Tim. Follow-up observations were conducted for Randy 10 and 19 days after intervention; follow-up observations for Derek were held seven and 16 days after the intervention was removed, and 12 and 21 days after Tim’s last intervention session.
Results
Intervention Effects
The effects of the peer-mediated LBBI on individual students are shown in Figure 2. A summary of performance changes within each condition is shown in Table 3.
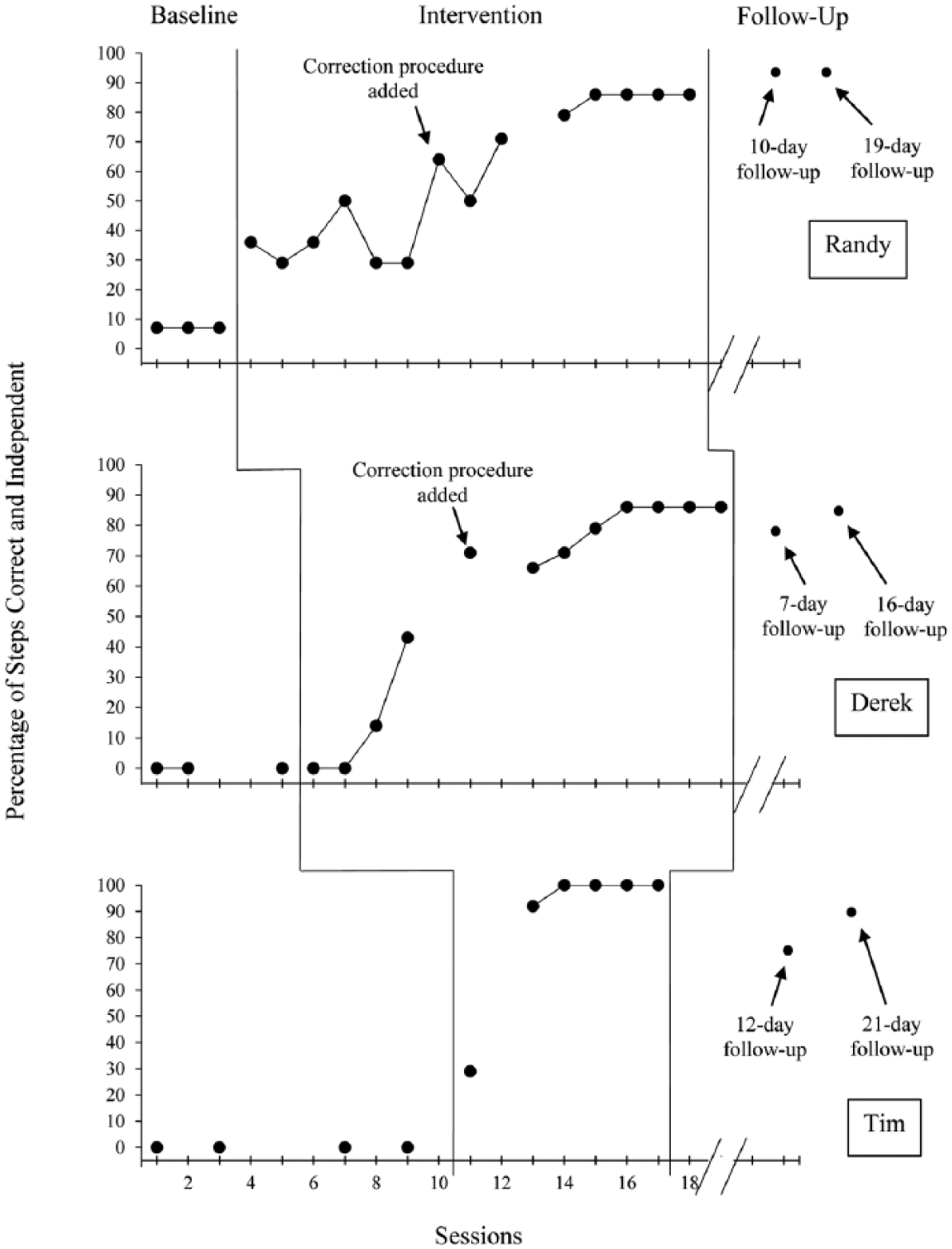
Percentage of correct independent steps of task analysis for cleaning and dressing a wound.
Performance Within Conditions.

Baseline
During baseline, data remained low and stable, with no student accurately completing more than 7% of the steps in the first aid routine. Randy was able to complete one step accurately, but Derek and Tim did not initiate any steps in the task analysis during baseline.
Intervention
When the peer-mediated LBBI instructional activities were introduced, all participants began completing the routine with more accuracy. However, due to Randy’s variability, the LBBI was enriched with the correction procedure described earlier during the seventh intervention session. While receiving the enriched LBBI, Randy steadily increased until he reached 86% accuracy for 4 days in a row. Prior to adding the correction procedure with Derek, his performance was low but accelerating. Derek produced a significant increase in accurate completion of steps after the correction procedure was added (during his fifth intervention session), reaching 86% accuracy for 4 days in a row. Tim received the LBBI package with the correction procedure immediately after baseline and had a significant increase in skill accuracy, reaching 100% on the third intervention session. He continued to perform 100% of the steps accurately and independently for four consecutive days.
Follow-up
Upon the removal of the peer-mediated LBBI, Randy’s skill accuracy continued to improve, increasing to 93%. His follow-up data remained stable during these two observations. Derek’s performance during the follow-up observations was slightly more variable, decreasing slightly during his first follow-up observation, before returning to his previous performance (86%). Tim showed a greater decrease once the intervention was removed. His accuracy decreased from 100% during his final intervention sessions to 79% during the first follow-up session, and then returned to 86% on the second follow-up session.
Post Hoc Analysis and Effect Size
The first post hoc analysis of the findings using PND indicated that the LBBI was effective to very effective based on standards described by Ledford et al. (2014) and Scruggs and Mastropieri (2013). Randy’s PND between baseline and intervention was 100%; between baseline and follow-up Randy’s PND also was 100%, indicating the intervention was very effective. Derek’s PND between baseline and intervention was 83%, indicating an effective intervention. Between baseline and follow-up, Derek’s PND was 100%, indicating the impact on maintenance was very effective. Finally, Tim’s PND between baseline and intervention was 100%; between baseline and follow-up, his PND also was 100%, indicating the intervention was very effective. The post hoc analysis using the Tau-U results showed an overall effect size of .945. Although this suggests a robust effect size across the students (Parker et al., 2011), it should be noted that this analysis did not include data reported during the follow-up observations.
Social Validity
The social validity assessment measured professionals’ perceptions on LBBIs as an instructional strategy, as well as their perceptions of students’ ability to perform the first aid routine. The strongest findings from the social validity assessment regarding LBBIs as an instructional strategy was the belief by professionals that using an LBBI will (a) help students learn skills and routines (3.75 of 4.0) and (b) increase student willingness to learn new skills (3.25). Professionals would also recommend using LBBI instructional packages to others (3.5). The weakest finding among the professionals was that having a student peer deliver the lessons would be an effective way to teach this population (1.5). The professionals held a moderate degree of confidence that students would (a) be willing to perform the first aid routine of cleaning and bandaging another person’s wound (2.5) and (b) want to learn other first aid skills (2.25). They had low confidence that the students would be able to perform the skill (1.5). Student beliefs about their first aid skills showed a marked contrast to the professionals. Students strongly reported that they (a) were willing to perform the first aid routine (3.25), (b) wanted to learn other first aid skills and routines (3.25), and (c) were confident in their knowledge of the skill (3.0).
Discussion
The purpose of this study was to determine whether a peer-mediated LBBI that includes multiple instructional activities would increase the acquisition of a first aid routine by adolescents with developmental disabilities, and to establish whether any acquired skills would maintain after the intervention was removed. All students who received the peer-mediated LBBI improved their ability to clean and dress a wound. All students maintained the skill after the intervention was removed during the follow-up sessions. Although the initial intervention produced some gains, the skill acquisition was rapid and robust when the LBBI was enriched by adding a correction procedure that included more explicit skill rehearsal to the story. For all three students, the learning gains maintained when the LBBI was removed. This acquisition pattern closely mirrors the learning gains in previous LBBI studies in which rehearsal has been a critical part of the intervention (Brady, Hall, & Bielskus-Barone, 2016; Bucholz et al., 2008; (Hall et al., 2017). Also, this study is only the third examination of LBBIs delivered by peers. To date, story-based interventions have been implemented primarily by teachers, parents, and other professionals. As a third investigation showing the effectiveness of peers in implementing LBBIs, these findings extend the literature base on LBBIs, and create future options for other extensions of this intervention.
When examining the individual students’ effects, it should be noted that neither Randy nor Derek ever reached 100% accuracy on the first aid routines. Interestingly, the two steps missed continuously by these students were the two handwashing steps in the task analysis, a skill on which each student had already shown proficiency outside the research sessions. When reading the storybook to the students, the peer simply pointed to the sink when they reached this step in the routine. That is, Miguel did not ask the students to rehearse this step (which occurred twice during the task analysis). This was the only step that was not actually rehearsed in real time, and it was the only step that did not reach mastery. This rehearsal protocol differs from previous research where all the steps were rehearsed through simulation (Brady, Hall, & Bielskus-Barone, 2016; Brady, Honsberger, et al., 2016). In this study, once the students read the LBBI and were asked to perform the routine, Derek and Randy either gestured to the sink or verbalized “wash hands” without actually completing the step. This lack of rehearsal for handwashing might explain why 100% mastery was not reached for two students and provides support for the need for rehearsal.
Like all research, this study has limitations. For example, this study did not have a generalization focus (other than maintenance). Because many students with ID and autism do not easily generalize newly learned skills, future research should include a generalization measure to assess whether the LBBI protocol might result in a spontaneous use of the first aid routine in novel settings, with other people, or with different types of bandaging materials. Another generalization question might include an investigation of whether students who learn this basic routine for wound care might spontaneously alter the procedure for different sizes, types, or locations of wounds. The wounds simulated in the current study were all less than 2 inches in size and on the peer’s arms, a location easy to find, clean, and apply dressings and tape. Although the basic care protocol is similar for wounds in other areas (e.g., the scalp or torso) and for wounds of different sizes, caring for these wounds requires additional problem solving when selecting dressings that match the size of the wound, and applying dressings securely. A second limitation of this study is the lack of fidelity data. To assure that the peer could deliver the intervention as designed, the researchers conducted a practice session with the peer reader prior to each intervention session with each student. In our previous research on peer-mediated interventions, this procedure was successful in assuring accurate delivery of the intervention by peers (Brady, Hall, & Bielskus-Barone, 2016; Brady, Honsberger, et al., 2016). However, no actual fidelity data were collected during these practice sessions or during the actual observations. This should be considered as a limitation in any attempt to extrapolate the findings as support for LBBIs as an evidence-based practice, and should be included as a standard in future studies to assess the viability of LBBIs as an evidence-based practice (Cook et al., 2015; Kratochwill et al., 2013). Finally, the researchers did not assess whether the students were successful in keeping the items used to clean and dress the simulated wounds sterile. Keeping dressings sterile after they are removed from packaging is an expectation for citizen responders who apply first aid; yet, little emphasis was paid to that during the training. It was not assessed whether the dressings remained sterile, as expected in first aid standards for actual wounds, and that expectation should be included and evaluated in future studies.
The effectiveness of most LBBI instructional packages may be due to the flexibility with which they are designed and delivered. For most LBBIs, there is no specific formula that must be followed regarding sentence structure, picture size, or form of rehearsal. Indeed, in most LBBI investigations, the stimulus materials are designed based on the principle that many people with developmental disabilities learn well with visuals and skill rehearsal (Quill, 1997; Van Laarhoven, Kraus, Karpman, Nizzi, & Valentino, 2010), and then customize the LBBI to accomplish that. There are other components of instructional packages that might increase the efficacy of these interventions. These components include different direct instruction protocols, more explicit discrimination training, precorrection procedures, self-assessment, graduated guidance, use of learning strategies, and different functions of language and literacy. For example, as this study was under way, a parallel program of research was investigating the comparative effects of using different forms of mobile technology for delivering LBBIs (Hall, Brady, Kearney, & Downey, in press); these delivery formats could easily be adapted for safety training interventions. It is possible that the most significant limitation of the present study was a delivery format, which limited the intervention to a single set of stimulus materials and intervention procedure, delivered by a single peer. To produce a more effective LBBI, interventions might be more individualized and include a range of different but effective instructional procedures solely contingent on a student’s performance in the moment. This might require a return to a type of intervention that encouraged professionals to “train loosely” so that students would experience a wider variety of training and environmental stimuli, thus preparing them to respond to a wider range of problems (Campbell & Stremel-Campbell, 1982). Although these instructional innovations would no doubt wreak havoc on investigators’ procedures to establish experimental control within a study, this type of flexibility and innovation might yield important clinical and applied lessons.
In the past decade, a number of different types of LBBIs have been investigated and shown to be effective for their positive impact on people with developmental disabilities. From a number of research reviews, it has become evident that the various forms of LBBIs have typically been used as a strategy to reduce problem behavior, and few have investigated this intervention as an instructional strategy designed to teach new skills (Bucholz, 2012; Kokina & Kern, 2010; Test, Richter, Knight, & Spooner, 2011). This study was conducted to extend the knowledge base on LBBIs (a) as a multicomponent instructional strategy, (b) as a peer-mediated intervention, and (c) as a means of teaching basic first aid skills and routines. The results of the study indicate that the peer-mediated LBBI instructional package was effective as a teaching procedure for safety skills, and holds promise for teaching other safety skills and routines to adolescents and adults with disabilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.