
Abstract
Worry is associated with inflexibility in cognitive, emotional, and physiological functioning. In addition, worry’s negative valence and abstract level of construal are rigid characteristics that contribute to its nonadaptive consequences. Relaxation and cognitive therapy aim to increase flexibility in chronic worriers, and may have greater efficacy when administered in combination. We examined the extent to which relaxation enhances and/or worry inhibits cognitive flexibility during a cognitive restructuring exercise in which participants generated alternative predictions for their worries. Participants (n = 189) were randomly assigned to engage in relaxation, worry, or neutral thinking prior to cognitive restructuring. We measured the number and perceived likelihood of alternative predictions generated by participants, and coded those alternative predictions for their degree of positive valence, negative valence, and level of construal (abstractness to concreteness). Worry and relaxation did not lead to different numbers or perceived likelihood of alternative predictions. However, compared with participants with minimal symptoms of generalized anxiety disorder (GAD), those with elevated symptoms of GAD who engaged in prior worry generated alternative predictions characterized by greater negative valence and more abstractness (i.e., less concreteness). We also found that greater negative valence of alternative predictions was associated with more abstractness, whereas greater positive valence of alternative predictions was associated with more concreteness. These findings suggest that after engaging in worry, individuals with GAD may be less able to flexibly shift from the use of nonadaptive characteristics (negative valence, abstractness) associated with feared outcomes to the use of more adaptive characteristics (positive valence, concreteness) when considering alternative predictions.
Generalized anxiety disorder (GAD) is characterized by frequent, uncontrollable worry about a variety of topics (Diagnostic and Statistical Manual of Mental Disorders [5th ed., DSM-5]; American Psychiatric Association [APA], 2013). GAD is also characterized by high rates of comorbidity. In particular, major depressive disorder (MDD) is highly comorbid with GAD, with 64% of individuals with a lifetime diagnosis of GAD also meeting lifetime criteria for MDD, and 67% of individuals with lifetime MDD also meeting lifetime criteria for GAD (Brown, Campbell, Lehman, Grisham, & Mancill, 2001). One feature common to both GAD and MDD is the experience of repetitive negative thinking (RNT), with GAD entailing excessive worry and MDD entailing high levels of depressive rumination.
Watkins (2008) proposed that several features of repetitive thinking determine whether it will have adaptive or nonadaptive consequences. One hallmark of nonadaptive repetitive thought is that it is negatively valenced (Watkins, 2008). In particular, engaging in worry increases and maintains negative affect (NA) and decreases positive affect (PA; for example, Borkovec, Alcaine, & Behar, 2004; McLaughlin, Borkovec, & Sibrava, 2007). A second hallmark of nonadaptive repetitive thinking is that it is abstract in nature (Watkins, 2008). Stöber’s (1998) reduced concreteness theory of worry argues that the abstractness of worry leads to avoidance of fear-relevant imagery and its associated physiological and affective experience. Both worrisome problem elaborations (Stöber & Borkovec, 2002; Stöber, Tepperwien, & Staak, 2000) and the worry process itself (Goldwin & Behar, 2012) are predominantly abstract in nature, and worry is a predominantly verbal-linguistic (as opposed to imagery-based) process (Behar, Zuellig, & Borkovec, 2005; Borkovec & Inz, 1990; Hirsch, Hayes, Mathews, Perman, & Borkovec, 2012). Furthermore, during worry, concreteness is positively associated with degree of imagery-based activity and negatively associated with degree of verbal-linguistic activity (McGowan et al., 2017). Abstract mentation is also associated with maintenance of negative affective states (Ehring, Szeimies, & Schaffrick, 2009), increased anxiety (Feldman & Hayes, 2005), and increased risk for developing MDD (Watkins, Moberly, & Moulds, 2008). Moreover, Hirsch, Perman, Hayes, Eagleson, and Mathews (2015) found that mentation that is both negatively valenced and verbal-linguistic (which tends to be more abstract; McGowan et al., 2017) is particularly detrimental for worriers in that it results in more frequent negative thought intrusions than does engaging in negatively valenced imagery-based, positively valenced imagery-based, or positively valenced verbal-linguistic mentation.
Nonadaptive RNT is associated with inflexibility in cognitive, emotional, and physiological functioning. Psychological flexibility can be defined as the ability to adaptively respond on cognitive, emotional, and behavioral levels according to changing features of a situation, or to think about situations or problems in multiple, flexible ways. Cognitive models of worry (e.g., Hirsch & Mathews, 2012) conceptualize cognitive inflexibility in worry as being due in part to information processing biases and in part to difficulty shifting attention away from worry content. Individuals high in trait worry exhibit selective attention to potential threat and/or difficulty disengaging from threat, as well as a tendency to interpret benign information as threatening (Hayes & Hirsch, 2007). For example, worry is experienced as perseverative (e.g., involving infrequent topical shifts) and contains a higher frequency of words indicating rigid (threat) interpretations of potentially threatening situations (Molina, Borkovec, Peasley, & Person, 1998). Worry depletes working memory, which leads to difficulty inhibiting worrisome thought and shifting attention to more benign topics (Hayes & Hirsch, 2007; Stefanopoulou, Hirsch, Hayes, Adlam, & Coker, 2014), particularly when worry is verbal-linguistic (Leigh & Hirsch, 2011). Together, this weakening of attentional control and biased information processing may lead to the inflexible, intrusive, and uncontrollable qualities characteristic of worry.
Worry is also associated with inflexible patterns of emotional and physiological responding. For example, state-level worry is deployed to a similar extent during various emotional contexts that should theoretically lead to different levels of worry (i.e., neutral, happy, sad, or fearful film clips; Aldao, Mennin, & McLaughlin, 2013). Compared with prior relaxation and neutral thinking, prior worry is also associated with attenuated increases in negative emotion in response to subsequent fear-inducing film clips (Llera & Newman, 2010), suggesting that worry may lead to a restricted range of emotional responding. In addition, using spectral analysis, Fisher and Newman (2016) found that worry is associated with the degree of variability in daily diary reports of anxiety among individuals with GAD; specifically, higher worry was associated with less between-days variation in cyclic anxiety reported throughout the day. Several investigations have also demonstrated that engaging in worry leads to reductions in deployment of adaptive parasympathetic control over cardiac activity in response to stressors, as indexed by reduced heart rate variability (Hofmann et al., 2005; Llera & Newman, 2010). Together, these findings suggest that worry is associated with rigidity instead of flexible adaptation in response to shifting internal and external circumstances.
Treatments for GAD encompass an array of cognitive and behavioral techniques aimed at increasing cognitive, physiological, emotional, and behavioral flexibility. Cognitive therapy (CT) entails challenging and restructuring negative thoughts to generate more adaptive alternative responses. For example, cognitive therapists help GAD clients generate more realistic estimates of the likelihood of the feared outcomes of their worries and generate alternative predictions that have equal or higher likelihood of occurring (Behar & Borkovec, 2005). This process attempts to increase cognitive flexibility in that the generation of various alternatives to the feared outcome and/or the recognition that these alternatives are more likely to occur indicates increased ability to think about the situation in multiple, flexible ways. A second important component in the treatment of GAD is relaxation, which promotes adaptive physiological regulation and emotional functioning by increasing the relative proportion of parasympathetic to sympathetic nervous system activity (Sakakibara, Takeuchi, & Hayano, 1994; Yang, Yang, & Zhang, 2002), reducing salivary cortisol (Pawlow & Jones, 2002), and reducing state (Hazlett-Stevens & Borkovec, 2001) and trait (Manzoni, Pagnini, Castelnuovo, & Molinari, 2008) anxiety. It is efficacious as a stand-alone treatment for GAD (Arntz, 2003; Öst & Breitholtz, 2000), and has also been found to have a facilitative effect on various components of treatment for anxiety. For example, engaging in prior relaxation leads to enhanced fear reactivity, within- and between-session habituation, and vividness of fear-related imagery during subsequent exposure (Borkovec & Sides, 1979), which may facilitate reductions in somatic anxiety and symptoms of GAD (Donegan & Dugas, 2012).
CT and relaxation are both efficacious in the treatment of GAD (Hanrahan, Field, Jones, & Davey, 2013; Öst & Breitholtz, 2000; Siev & Chambless, 2007), and relaxation can augment the efficacy of CT for GAD (Borkovec & Costello, 1993). However, GAD remains difficult to treat, with rates of clinically significant improvement following relaxation-based treatment or CT reaching only 50% to 57% (Hanrahan et al., 2013; Siev & Chambless, 2007). Furthermore, some research suggests that RNT (e.g., worry, rumination) is associated with symptom chronicity and poorer treatment outcome (e.g., Schmaling, Dimidjian, Katon, & Sullivan, 2002). One approach to enhancing the efficacy of treatment for chronic worry is to utilize relaxation to augment the efficacy of specific CT interventions such as the generation of alternative outcomes. Although research indicates that the combination of relaxation and CT leads to greater efficacy than either component in isolation as measured by GAD symptom reduction (Borkovec & Costello, 1993), it remains unclear whether relaxation might enhance cognitive flexibility regarding specific worries. In addition, given evidence that relaxation enhances characteristics of key processes of various behavioral treatment approaches (e.g., vividness of imagery, fear activation; Borkovec & Sides, 1979), it is possible that relaxation might also ameliorate key nonadaptive processes during attempts to enhance flexibility. For example, relaxation might enhance the degree of positive valence and/or concrete processing of alternative predictions identified during cognitive restructuring procedures, both of which would theoretically be associated with more adaptive outcomes (Watkins, 2008). If so, this would indicate that being in a relaxed state leads to greater flexibility vis-à-vis characteristics of worry that otherwise lead to nonadaptive consequences.
In addition, although research indicates that GAD and trait worry are associated with cognitive inflexibility, no studies to date have examined whether RNT (i.e., state worry) leads to greater cognitive rigidity during attempts to enhance flexibility (e.g., during cognitive restructuring). Furthermore, it remains unclear whether worry exacerbates key nonadaptive processes during attempts to enhance flexibility. Engaging in worry might increase or maintain the degree of negative valence and/or the degree of abstract processing of alternative outcomes identified during cognitive restructuring. If so, this would indicate that being in a worrisome state leads to rigidity vis-à-vis the characteristics of worry that lead to nonadaptive consequences.
Finally, comorbidity is one factor that might affect nonadaptive characteristics of RNT. GAD and MDD are characterized by similar processes (Watkins, 2008), and key cognitive features of GAD and MDD (e.g., intolerance of uncertainty, poor problem orientation) are pronounced among individuals suffering from both of these conditions simultaneously (DuPuy & Ladouceur, 2008). In addition, engaging in RNT affects these individuals to a greater extent relative to those with either condition in isolation (A. M. Ruscio et al., 2015), perhaps due to greater nonadaptive characteristics of their RNT. Importantly, no studies to date have addressed the impact of comorbid MDD on the content or level of construal of worry.
The present study sought to examine whether (a) worry leads to reduced cognitive flexibility and/or (b) relaxation leads to enhanced cognitive flexibility. First, we examined the effects of worry and relaxation on the number and perceived likelihood of alternative predictions generated during a cognitive restructuring exercise. We hypothesized that participants who engaged in worry would generate fewer alternative predictions and would perceive those alternative predictions as less likely to occur; in contrast, we predicted that those who engaged in relaxation would generate a greater number of alternative predictions and would perceive those alternative predictions to be more likely to occur. Second, we investigated the effects of worry and relaxation on key characteristics (valence, level of construal) of alternative predictions. We hypothesized that participants who engaged in worry would generate alternative predictions characterized by less positive valence, more negative valence, and reduced concreteness; in contrast, we predicted that participants who engaged in relaxation would generate alternative predictions characterized by more positive valence, less negative valence, and greater concreteness. Third, we examined whether individuals with elevated symptoms of GAD and/or MDD differed from control participants on the above variables, as well as the degree to which relaxation and worry affected these variables. We expected that individuals with elevated symptoms of GAD and/or MDD would perceive initial feared outcomes as more likely to occur and that they would generate alternative predictions characterized by less positive valence, more negative valence, and less concreteness. We also expected that these characteristics would be pronounced among symptomatic individuals who engaged in prior worry, particularly those who also endorsed elevated symptoms of MDD (although our examination of the impact of comorbid MDD symptoms was exploratory in nature).
Method
Design
Four groups of participants were created by crossing minimal and elevated levels of GAD and MDD symptoms. Participants were randomly assigned to one of three inductions (relaxation, worry, and neutral thinking).
Participants
Participants were drawn from the undergraduate psychology subject pool at a large public institution. Potential participants were administered the Generalized Anxiety Disorder Questionnaire–IV (GAD-Q-IV; Newman et al., 2002) and the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) and were invited to take part in the study if their scores on the GAD-Q-IV were either less than or equal to 1.9 or greater than or equal to 5.7 and if their scores on the BDI-II were either less than or equal to 13 or greater than or equal to 20. 1 This procedure created four analog groups comprised of individuals with either (a) minimal symptoms of GAD and MDD (n = 58), (b) elevated symptoms of GAD and minimal symptoms of MDD (n = 59), (c) minimal symptoms of GAD and elevated symptoms of MDD (n = 21), or (d) elevated symptoms of both GAD and MDD (n = 51). The final sample (n = 189) had an average age of 19.23 (SD = 1.56), was predominantly female (71.5%), and was ethnically diverse (see Table 1 for demographic and clinical characteristics).
Sample Demographic and Clinical Characteristics.
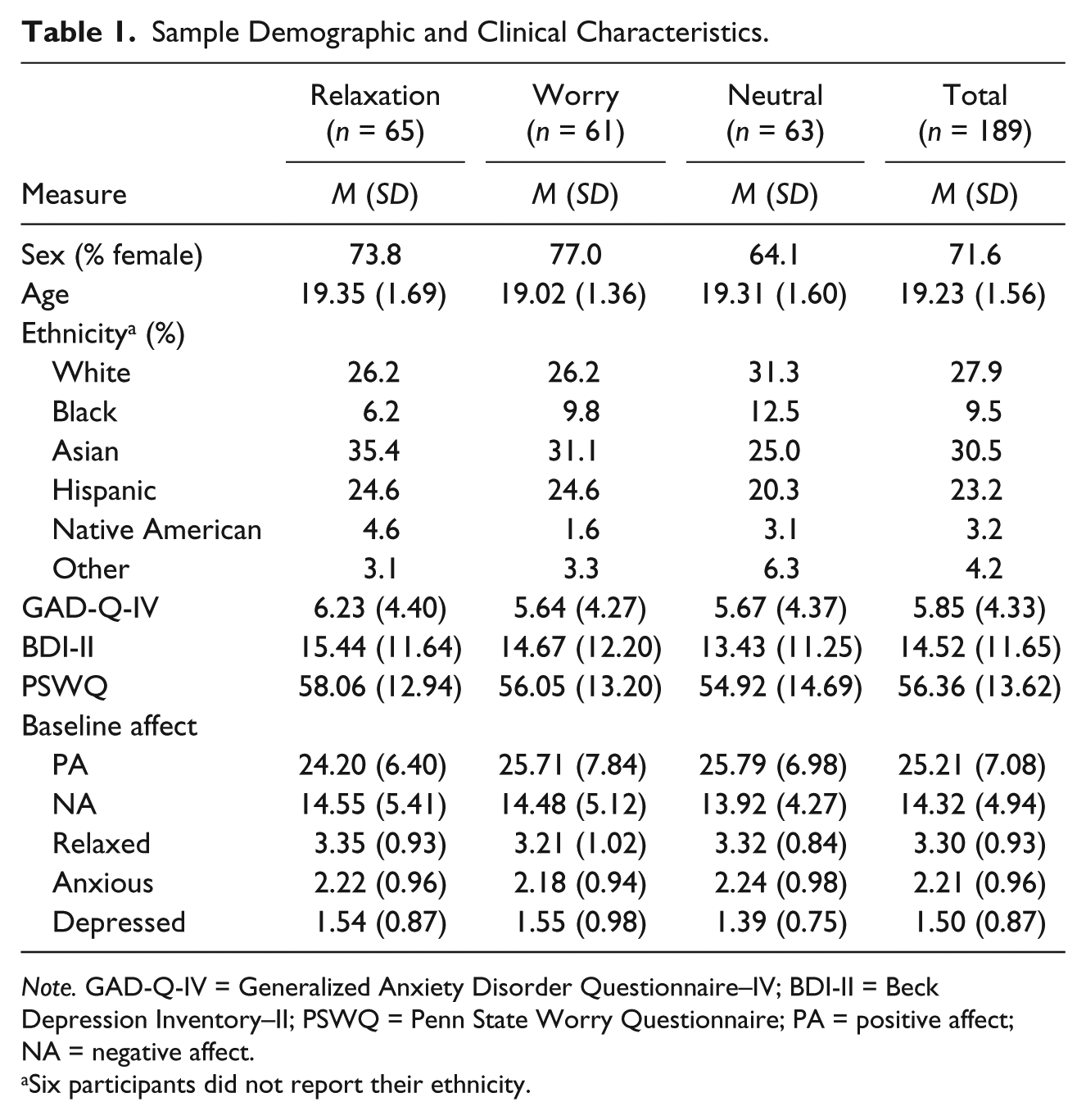
Note. GAD-Q-IV = Generalized Anxiety Disorder Questionnaire–IV; BDI-II = Beck Depression Inventory–II; PSWQ = Penn State Worry Questionnaire; PA = positive affect; NA = negative affect.
Six participants did not report their ethnicity.
Measures
GAD-Q-IV
The GAD-Q-IV (Newman et al., 2002) is a nine-item self-report measure of the diagnostic criteria for GAD. It has demonstrated good test-retest reliability, convergent validity, and discriminant validity. Compared with a gold standard diagnosis by the Anxiety Disorders Interview Schedule (ADIS), a cutoff score of 5.7 on the GAD-Q-IV identifies individuals diagnosed with GAD with 89% sensitivity and 83% specificity. In addition, a cutoff score of 1.9 (which evidences a 98.63% likelihood of correctly identifying an individual without GAD as determined by the ADIS) was used to identify individuals with minimal symptoms of GAD. Internal consistency of the GAD-Q-IV in this sample was good (α = .87).
BDI-II
The BDI-II (Beck et al., 1996) is a 21-item self-report measure of symptoms of depression over the past 2 weeks. In undergraduate samples, the BDI-II has high internal consistency and excellent test-retest reliability (Sprinkle et al., 2002). Scores below 13 are considered not clinically significant, scores greater than 13 are considered “mild,” scores over 20 are “moderate,” and scores over 29 are “severe.” We used a cutoff score of 13 to identify individuals with minimal symptoms of MDD, and a cutoff score of 20 to identify individuals with elevated symptoms of MDD. Internal consistency of the BDI-II was excellent in this sample (α = .94).
Penn State Worry Questionnaire (PSWQ)
The PSWQ (Meyer, Miller, Metzger, & Borkovec, 1990) is a 16-item self-report measure of frequency, intensity, and uncontrollability of worry. It evidences excellent internal consistency and test-retest reliability. The PSWQ is elevated among individuals with GAD and other anxiety disorders relative to healthy controls. A score of 62 is used to identify cases of GAD in undergraduate samples with 75% sensitivity and 86% specificity, and its utility in screening for other disorders is lower (Behar, Alcaine, Zuellig, & Borkovec, 2003). Internal consistency of the PSWQ in this sample was good (α = .89).
Positive and Negative Affect Schedule (PANAS)
The PANAS (Watson, Clark, & Tellegen, 1988) is a 20-item self-report measure comprised of 10 positive and 10 negative adjectives that assess PA and NA, respectively. The PANAS has good internal consistency and moderate test-retest reliability for momentary assessment of affect, and demonstrates good convergent and discriminant validity. Internal consistency was good to excellent for both subscales in the current sample (PA αs = .86-.91; NA αs = .83-.92).
Relaxed, anxious, and depressed affect
Participants rated the degree to which they felt “relaxed,” “anxious,” or “depressed” on a 1 (not at all) to 5 (extremely) Likert-type scale. These single-item ratings provided an additional assessment of affect that also served as a postinduction manipulation check.
Coding of Feared Outcomes and Alternative Predictions
Initial feared outcomes and alternative predictions were listed in random order (using a random number generator) across participants and conditions. Three trained coders blind to condition and study hypotheses independently rated each feared outcome or alternative prediction on three scales, then jointly came to consensus on each rating. 2 Only consensus ratings were used in analyses. Cronbach’s alpha was used to assess degree of agreement between raters.
Positive content and negative content
These two scales assessed the degree to which the content of alternatives was positively and negatively valenced on a 1 (not at all) to 5 (extremely) scale. Coders considered the valence of individual words as well as the implications of feared outcomes and alternative predictions. Positive and negative valence were treated as orthogonal constructs (Clark & Watson, 1988). Interrater reliability was excellent for the positive valence scale (α = .94) and good for the negative valence scale (α = .88).
Level of construal
This coding system by Stöber (1998) assesses the degree of abstractness or concreteness of thought samples, and has been used to assess level of construal of worry problem elaborations (Stöber & Borkovec, 2002; Stöber et al., 2000). Abstractness is defined as “vague/indistinct, cross-situational, or aggregated” including trait descriptors, whereas concreteness is defined as “distinct, situationally specific, clear, or singular,” including details that specify person, time, place, or means. The scale ranges from 1 (very abstract) to 5 (very concrete), and a rating of 3 indicates that the thought could be equally interpreted as abstract or concrete. As in other investigations of worry (e.g., Goldwin & Behar, 2012; McGowan et al., 2017), interrater reliability was adequate in this sample (α = .78).
Procedure
Participants were first asked to complete a baseline PANAS and baseline single-item affect ratings (relaxed, anxious, and depressed affect). Next, they were asked to write down their topic of greatest current worry. Worry was defined as “mental activity about some future event that causes you to feel anxious when you think about it.” After the experimenter checked participants’ topics to ensure that all provided topics complied with this definition, participants were asked to write down a potential outcome of their topic of worry and to provide a 0% to 100% rating of the likelihood of the feared outcome occurring. Participants then completed a posttopic (also referred to as a preinduction) PANAS and affect ratings.
Next, participants underwent a 5-min induction (relaxation, worry, or neutral thinking), depending on the condition to which they had been randomly assigned. Participants in the relaxation condition were asked to close their eyes and “relax as deeply and slowly as you can. Just let go of all tension, focusing your attention on your breathing, breathing from your diaphragm at a slow, comfortable rate.” These instructions mirrored those typically provided by clinicians during diaphragmatic breathing. Participants in the worry condition were asked to close their eyes and think about their worry topic as they usually did, but as intensely as possible, and to continue doing so until asked to stop. These instructions mirrored worry inductions used in other studies (Goldwin & Behar, 2012; McGowan et al., 2017). Participants in the neutral condition were asked to close their eyes and count backward by 3s beginning at 900, and to be as accurate as possible. They were told that they would be asked to write down the number they ended on, and that they could go at their own pace. Following this, they were asked to complete a postinduction PANAS and single-item affect ratings, which served as manipulation checks.
Participants were then asked to generate as many alternative predictions for their worry topic as they could that were different from the original feared outcome they provided, and then to rate these alternatives on the likelihood (0%-100%) of each prediction coming true. This procedure was intended to simulate cognitive restructuring methods typically used in CT for GAD (Behar & Borkovec, 2005), and was adapted for purposes of the experiment to enable participants to complete the exercise independently (i.e., without the aid of a therapist). Finally, participants completed a final PANAS and the single-item affect ratings.
Data Analysis
First, to ensure that the three conditions produced expected changes in affect, we conducted a 3 (Condition: relaxation, worry, neutral) × 2 (Time: preinduction, postinduction) repeated-measures MANOVA on affect ratings (PA, NA, relaxed affect, anxious affect, depressed affect). Second, to examine the unique and interactive effects of condition and symptom group on both the number of alternatives generated and the characteristics of those alternatives, we conducted a series of 3 (Condition) × 2 (GAD status: GAD, non-GAD) × 2 (MDD status: MDD, non-MDD) between-subjects ANOVAs on (a) the total number of alternative predictions generated, (b) the perceived likelihood of those alternative predictions, (c) consensus ratings from each of the three coded dimensions for the initial feared outcome of the worry, and (d) consensus ratings from each of the coded dimensions for generated alternative predictions. All variables were normally distributed, with the exception of positive valence for the initial feared worry outcome (skew = 9.87; kurtosis = 96.46). Given that only two participants’ initial feared outcomes were coded as having positive valence greater than a rating of 1, transforming this variable would not be appropriate, and it was therefore omitted from analyses. Bonferroni corrections were utilized to adjust for multiple comparisons.
Results
Demographic, Baseline, and Clinical Characteristics
We first sought to ensure that random assignment was successful in producing similar demographic and clinical characteristics across the three conditions. Two chi-square tests on proportions of gender and ethnicity indicated no between-groups differences on either variable (ps > .31). In addition, one-way (Condition) ANOVAs indicated no between-groups differences on age or PSWQ score (ps > .30). Thus, random assignment was successful in producing groups that were equivalent in demographic characteristics and trait worry (see Table 1).
Next, we conducted a 3 (Condition) × 2 (GAD Status) × 2 (MDD Status) MANOVA on baseline affect measures (PA, NA, relaxed affect, anxious affect, depressed affect). There was a multivariate Condition × GAD Status × MDD Status interaction, F(10, 338) = 2.22, p = .016,
Manipulation Checks
First, we conducted a 3 (Condition) × 2 (Time: baseline, post-topic-listing) repeated-measures MANOVA on the five affect ratings to ensure that participants across the three experimental conditions were affected equally by listing their worry topic prior to engaging in the inductions. There was a multivariate main effect of Time, F(5, 174) = 119.36, p < .001,
Next, the 3 (Condition) × 2 (Time: preinduction, postinduction) repeated-measures MANOVA on affect ratings indicated multivariate main effects of Condition, F(10, 352) = 1.90, p = .046,
Characteristics of Initial Feared Worry Outcomes
To examine the characteristics of initial feared outcomes of participants’ worries, we conducted a series of 3 (Condition) × 2 (GAD Status) × 2 (MDD Status) ANOVAs on the likelihood rating ascribed to the initial feared worry outcome as well as coded dimensions (negative valence, level of construal). As previously mentioned, positive valence was omitted from these analyses due to limited variance. We did not expect to find effects of Condition based on the fact that participants did not engage in the inductions until after having listed their feared outcomes. For perceived likelihood ratings, results indicated a main effect of MDD status, F(1, 177) = 11.63, p = .001,
For level of construal, there was a marginal Condition × GAD Status interaction, F(2, 177) = 2.93, p = .056,
Number and Perceived Likelihood of Alternative Predictions
We ran two separate 3 (Condition) × 2 (GAD Status) × 2 (MDD Status) between-subjects ANOVAs on the number of alternative outcomes participants generated, as well as the perceived likelihood of those alternative predictions coming true. Results indicated no main or interactive effects of Condition for the number of alternative predictions generated (ps > .34) or the perceived likelihood of those alternative predictions coming true (ps > .15).
Characteristics of Alternative Predictions
We conducted three separate 3 (Condition) × 2 (GAD status) × 2 (MDD status) ANOVAs on coded dimensions (positive valence, negative valence, level of construal) to examine the effect of symptoms and condition on key characteristics of alternative predictions generated during the simulated cognitive restructuring exercise.
4
For positive valence, there were no main or interactive effects of Condition (ps > .54). Results indicated a marginal GAD Status × MDD Status interaction, F(2, 177) = 3.52, p = .062,
For negative valence, there was a Condition × GAD Status interaction, F(2, 177) = 3.01, p = .05,

Negative valence (top) and level of construal (bottom) of alternative worry predictions during simulated cognitive restructuring.
For level of construal, there was a Condition × GAD Status interaction, F(2, 177) = 3.05, p = .05,
Relationship Between Valence and Level of Construal
Level of construal of alternative predictions was significantly correlated with valence of those predictions. Specifically, greater positive valence was associated with more concrete (i.e., less abstract) predictions (r = .46, p < .001), whereas greater negative valence was associated with less concrete (i.e., more abstract) predictions (r = −.49, p < .001). Given assertions by Watkins (2008) and Hirsch et al. (2015) that negative valence and verbal-linguistic processing (which is related to abstractness; McGowan et al., 2017) interactively contribute to worry’s nonadaptive consequences, we examined whether the observed Condition × GAD Status interaction for level of construal of alternative predictions could be partially accounted for by the valence of those predictions. We conducted two separate 3 (Condition) × 2 (GAD Status) ANOVAs on level of construal of alternative predictions with (a) positive valence and (b) negative valence of alternative predictions included as covariates. The GAD Status × Condition interaction was no longer significant controlling for positive, F(2, 176) = 2.06, p = .130,
Discussion
We compared the effects of relaxation, worry, and neutral thinking on aspects of cognitive flexibility among individuals with elevated and/or minimal symptoms of GAD and/or MDD. When participants listed the initial feared outcomes of their worries, those with elevated symptoms of MDD perceived the feared outcomes as more likely to occur than did those with minimal symptoms of MDD. This finding is consistent with literature indicating that individuals with MDD tend to think more negatively about the future, including about the likelihood and cost of potential outcomes (for a review, see Roepke & Seligman, 2016). However, our prediction that participants with elevated symptoms of GAD would perceive their feared outcomes as more likely to occur was not supported. Although this was surprising, research on positive beliefs about worry indicates that individuals with GAD superstitiously believe that worry lessens the likelihood of events (Borkovec, Hazlett-Stevens, & Diaz, 1999). Given that 85% of worries ultimately have a benign outcome, this belief may be negatively reinforced over time (Borkovec et al., 2004). It may be that our participants with elevated GAD symptoms espoused this belief, and thus did not perceive their worries as being more likely to occur. On the contrary, multiple investigations have found that individuals with GAD perceive feared outcomes as being more probable and costly (e.g., Hirsch et al., 2015; Riskind & Williams, 2005). Future research should examine the conditions under which chronic worriers are more or less likely to believe that their worries will come true. For example, using nonanxious samples, Levi and Pryor (1987) found that providing an explanation for why a particular outcome might occur increases the subjective likelihood of the event occurring. Perhaps by asking participants to list their feared outcomes without considering the context surrounding those worries, we did not provide the conditions under which worriers perceive their worries as more likely to occur.
We were primarily interested in examining the effects of relaxation and worry on cognitive flexibility during a subsequent cognitive restructuring task. Contrary to our predictions, worry did not lead to reduced cognitive flexibility and relaxation did not lead to enhanced cognitive flexibility as measured by the number or perceived likelihood of alternative predictions. Importantly, we had limited power to detect these differences (maximum observed power = .496). In addition, our worry manipulation may not have been ideal; although it was the only induction that led to the maintenance of anxious affect, it did not lead to increases in anxious affect. Although it is certainly possible that participants engaged in worry as a cognitive process but simply did not experience an increase in anxious affect, had our worry manipulation yielded an increase in anxious affect, we might have found significant effects of condition vis-à-vis the number of alternative predictions and their likelihood of occurring.
Although we cannot state that worry led to reduced cognitive flexibility or that relaxation led to enhanced cognitive flexibility as measured by these outcomes, we did find that for participants with elevated symptoms of GAD, worry was associated with the generation of alternative predictions that contained more nonadaptive characteristics. Only participants who had elevated symptoms of GAD and who engaged in worry generated alternative predictions that were characterized by a greater degree of negative valence and a greater degree of abstractness. Moreover, these effects remained after controlling for potential confounds such as participants’ ratings of the likelihood of the alternative predictions, as well as the negative valence and level of construal of the initial feared outcome. These findings are important given Watkins’s (2008) assertion that negative valence and level of construal are key factors in the nonadaptive characteristics and concomitants of RNT.
That negative valence and abstract construal were more pronounced among individuals with elevated GAD symptoms who engaged in prior worry is also in line with work by Hirsch (e.g., Hirsch et al., 2015; Leigh & Hirsch, 2011) indicating that negative valence and verbal mode of processing (which in turn is associated with abstractness; McGowan et al., 2017) are associated with more frequent negative thought intrusions, and that these effects are specific to individuals high in trait worry. If worry depletes attentional resources that otherwise enable individuals with GAD to flexibly shift between topics or away from negatively valenced content, various nonadaptive characteristics of initial worry predictions will likely be maintained and exacerbated during attempts at cognitive restructuring. Our results indicate that the negative valence and abstractness that are characteristic of worry persisted during these attempts at cognitive restructuring. Research indicates that engagement in a (verbal) worry episode is likely to activate abstract representations of worry-related material (Hirsch & Mathews, 2012); thus, engaging in worry might have led to more negative and abstract subsequent alternative predictions. In addition, diminished cognitive resources resulting from worry likely exacerbates information processing biases (e.g., Holmes, Mogg, de Fockert, Nielsen, & Bradley, 2014), potentially also leading to alternative predictions that persisted in their threatening meaning. Instead of our cognitive restructuring exercise leading to a loosening of rigid and nonadaptive styles of thinking about worries (i.e., incorporating negative valence and abstractness), state worry led to the persistent use (i.e., maintained rigidity) of these styles.
We also found that positive valence of alternative predictions was associated with greater concreteness, and that negative valence of alternative predictions was associated with reduced concreteness (i.e., abstractness). When we controlled for either negative or positive valence of alternative predictions, the interactive effect of worry and elevated GAD symptoms was mitigated. This indicates that among individuals with GAD, the effects of worry on level of construal of alternative predictions is partially due to the valence of those predictions. This is consistent with Watkins’s (2008) suggestion that negative valence alone does not lead to nonadaptive consequences of RNT, but rather that it interacts with other important variables such as diagnostic status and affective state to lead to those nonadaptive consequences. It is likely that negative valence interacts in complex and nuanced ways with GAD symptoms, worrisome states, verbal-linguistic thinking, and abstract thinking to produce a host of negative consequences.
If engaging in brief relaxation does not facilitate the generation of alternative worry predictions that are less negatively valenced and/or more concrete, what other approaches might be effective? If worry maintains inflexible patterns of thinking about worry outcomes vis-à-vis negative valence and abstractness, perhaps directly modifying these characteristics might be beneficial. For example, Hirsch and colleagues have trained worriers to use imagery-based thought, which results in fewer negative thought intrusions (Hirsch et al., 2015; Stokes & Hirsch, 2010). They also found that regardless of whether training was verbal or imaginal, positive (vs. negative) thought content led to reduced perceived cost of the worry outcome (Hirsch et al., 2015). Similarly, Watkins and colleagues (2012) have demonstrated that training depressed individuals to think concretely reduces rumination, as well as symptoms of MDD. Training individuals to worry concretely and using vivid imagery might have beneficial results, including greater flexibility in generating alternative predictions that are less negative and less abstract.
Contrary to our predictions, relaxation did not lead to beneficial outcomes. Research indicates that relaxation techniques are effective in treating GAD over the course of several sessions (Siev & Chambless, 2007); thus, perhaps a longer induction or multiple sessions of relaxation might lead to enhanced cognitive flexibility. Alternatively, it is possible that although relaxation affects affective and physiological response systems, it has weaker or more distal effects on cognitive systems including cognitive flexibility. Although Borkovec and Costello (1993) found additive effects of relaxation and CT for individuals with GAD, they postulated that these therapies operate via distinct mechanisms. Similarly, relaxation in conjunction with cognitive bias modification does not lead to enhanced reduction of biases, but does lead to enhanced PA (Stevens, Behar, & Jendrusina, under review). Further research is needed to understand mechanisms through which relaxation exerts effects to optimize its use in therapy both in isolation and in conjunction with other therapy techniques.
This study had several notable limitations. First, our recruitment methods might have limited the generalizability of our findings in at least two ways. In one respect, we may have decreased the generalizability of our findings to individuals formally diagnosed with GAD and/or MDD. Although we used clinically significant cutoff scores on validated measures of GAD and MDD to identify individuals who closely resemble clinical populations in various respects, our results might not generalize to formally diagnosed patients. In another respect, we may have decreased the generalizability of our findings to a broader population of high worriers. Research by A. M. Ruscio (2002) indicates that high worriers with analog GAD perceive their worry as more distressing and impairing than do high worriers without GAD. Similarly, Wells (e.g., Wells & Carter, 1999) suggests that meta-worry (i.e., worry about one’s worrying) is an important discriminating feature of diagnostic GAD. Thus, among high worriers, those with GAD (and not merely all high worriers) are more likely to perceive their worry as problematic, and it is precisely these individuals who are arguably most likely to seek therapy (including CT) for their worry. However, restricting our sample to individuals with analog GAD excluded many high worriers, which might reduce the generalizability of our results to a broader population of high worriers. This is especially important given evidence that GAD and MDD are likely dimensional, rather than categorical, in nature (A. M. Ruscio, Borkovec, & Ruscio, 2001; J. Ruscio & Ruscio, 2000). Future investigators might wish to examine GAD and MDD dimensionally as moderators of the relationship between the manipulations of interest and cognitive flexibility.
Second, our induction procedure was brief and consisted of a single session, potentially limiting our ability to detect the effects of relaxation, which is generally administered for longer periods of time and over multiple sessions. It is possible that relaxation does enhance cognitive flexibility and/or that worry reduces cognitive flexibility, and that these differences would have emerged had our inductions been longer in duration. Third, we used a self-guided cognitive restructuring exercise to provide a standardized laboratory simulation of this technique. However, in therapeutic settings, therapists actively guide clients in the generation of flexible alternatives. Our results may not generalize to such clinical situations in which trained clinicians promote more flexible patterns of thinking. Finally, our group of participants with elevated symptoms of MDD and minimal symptoms of GAD consisted of only 21 individuals, whereas our other symptom groups each consisted of 51 to 59 participants. Because unequal sample sizes increase the risk of Type II error, we may have failed to detect some group differences. Although we likely had adequate power to detect effects involving MDD status (which evidenced medium to large effect sizes), smaller effects may have been obscured. Although future investigators should avoid the problem of unequal sample sizes to mitigate this risk, it is worth noting that recruiting individuals with this symptom profile is difficult given elevated rates of comorbid GAD among individuals with primary MDD (67%; Brown et al., 2001).
In summary, this study demonstrates that for individuals with elevated symptoms of GAD, worrisome thinking is associated with persistence of nonadaptive characteristics (i.e., negatively valenced content and abstract level of construal) of alternative worry predictions during a cognitive restructuring exercise intended to increase cognitive flexibility. Negative valence was associated with reduced concreteness, and positive valence was associated with greater concreteness, and valence of alternative predictions at least partially accounted for the effects of worry on level of construal. This suggests that after engaging in worry, individuals with elevated symptoms of GAD may be less able to flexibly shift away from the nonadaptive characteristics of feared worry outcomes and toward the use of more adaptive characteristics when considering alternative outcomes of their worries. These findings add to a growing literature showing that worry is associated with nonadaptive consequences, including reduced flexibility on cognitive and emotional levels.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.