
Abstract
Cognitive flexibility (CF), a subdomain of executive functioning (EF), involves abilities such as set shifting and reversal learning. Some variability in CF is normative across youth due to the gradual refinement of broader EF along with the prefrontal cortex. Prior research has suggested that a supportive parenting environment contributes to strong EF, whereas harsh/controlling parenting is associated with deficits. The current investigation explores whether certain parenting practices (e.g., parental accommodation, over-involvement, modeling) are associated with such deficits. Anxiogenic parenting and CF were assessed in 112 youth aged 9 to 17 years, with results demonstrating that parenting practices were not predictive of CF in these youth. Age accounted for the majority of differences in set shifting performance, potentially emphasizing the influence of parenting at different stages of development. Accordingly, future research is necessary to determine the potential impact of anxiogenic parenting at specific points in the development of CF.
Executive functioning (EF) refers to one’s ability to monitor and employ effortful control over cognitive processes (e.g., attentional control, working memory, planning), emotional responses, and behavioral impulses (Bradley, 1990; Lee, Bull, & Ho, 2013). Cognitive flexibility (CF; that is, set shifting), a subdomain of EF, refers to the ability to switch one’s attention from one task/stimulus to another and/or to adjust one’s behavior based on feedback. Both EF, in general, and CF, more specifically—as well as the functions they drive—have been closely associated with the development of the prefrontal cortex (PFC), as well as a wide network of neural structures (Bernier, Carlson, Deschênes, & Matte-Gagne, 2012; Stokes et al., 2013; Yuan & Raz, 2014). Development of the PFC, which continues throughout childhood into late adolescence/early adulthood, is thus supportive of advances in cognitive, emotional, and behavioral flexibility (Bradley, 1990; Lee et al., 2013; Yuan & Raz, 2014). The appropriate development of these processes in early childhood is vital to academic achievement, social competence, and emotion regulation throughout the life span (Blair & Razza, 2007; Raver et al., 2011), marking the importance of understanding factors that contribute to strong CF across childhood.
As CF is commonly measured by way of patterns in decision making and learning, several critical developmental periods have been observed during childhood. For example, using age-appropriate variations of the Wisconsin Card Sorting Task (WCST; Grant & Berg, 1948), children at age 3 reliably exhibit basic rule following and memory associated with CF. By age 5, children are able to inhibit their reaction to previously learned rules (i.e., shift cognitive set) in accordance with a new rule set (Zelazo, Carlson, & Kesek, 2008; Zelazo et al., 2003). Another period of rapid EF development occurs during puberty (Steinberg, 2005), a time characterized by considerable reorganization of the PFC, reprioritization of social influences, and increased risk taking behaviors (Blakemore & Choudhury, 2006; Selemon, 2013; Substance Abuse and Mental Health Services Administration, 2012). Unfortunately, such critical periods of growth and advancement also allow opportunity for vulnerability.
Dysfunction within the executive control system is accordingly neither uncommon nor homogeneous during childhood. For example, children of varying ages may exhibit poor impulse control, difficulties with planning and organization, poor critical thinking, and/or complications with memory. Although the impact of such difficulties can be both diffuse and diverse, severe presentations mirror and may be central to several forms of child psychopathology (e.g., attention-deficit hyperactivity disorder; Toplak, Bucciarelli, Jain, & Tannock, 2008). Children struggling with cognitive set shifting, in particular, may appear inflexible, rigid, and/or perseverative, with difficulty adapting to change and integrating new information into their repertoire (Anderson, 2002). This depiction parallels characteristics of the obsessive-compulsive and anxiety disorders (e.g., excessive question asking, strict routines, ritualized behaviors, stringent avoidance; Gross-Isseroff et al., 1996; Schultz & Searlman, 2002). The intricacies of the interaction between CF and anxiety are poorly understood, however. For example, whether cognitive inflexibility drives anxious tendencies or anxiety in itself encumbers flexible cognitive processing is yet debated (Ansari, Derakshan, & Richards, 2008; Bishop, 2009; Eysenck, Derakshan, Santos, & Calvo, 2007; Park & Moghaddam, 2017). Although this particular inquiry is beyond the scope of this article, there are yet several other gaps in this area of literature. In particular, how certain additional factors—such as parenting—may influence this interaction across the spectrum of adaptive to maladaptive functioning has received comparably little attention.
The healthy development of CF as well as abnormalities and dysfunction in this domain are certainly influenced by a myriad of factors. Biological processes such as genetics and physiological aspects of neural development are both implicated here. For example, the hormonal changes associated with puberty, as well as cortisol levels across childhood, are suggested to play a considerable role in the physiological changes to the PFC that affect CF (Berry et al., 2014; Selemon, 2013). The marked plasticity of the brain during early childhood in particular, when environmental influences such as parenting may be most relevant, has also been implicated in CF outcomes (Diamond, 2013; Diamond & Lee, 2011; Selemon, 2013).
The import of the parenting environment in itself has also been established across EF (Bernier, Carlson, & Whipple, 2014; Blair, Raver, & Berry, 2014; Fay-Stammbach, Hawes, & Meredith, 2014). Positive parenting behaviors, such as those which support child autonomy, for example, can promote the development of executive control (e.g., Bernier et al., 2014; Fay-Stammbach et al., 2014; Schore, 2001). Contrastingly, harsh parenting practices, such as those which exert excessive control or hostility toward the child, have been found to negatively affect EF (e.g., Cuevas et al., 2014; Rutter & O’Connor, 2004). For example, combative parenting is predictive of poor error processing in a similar fashion as is seen in clinical anxiety (Meyer et al., 2015). This overall relationship may even strengthen across the first few years of life, a time during which maternal EF—including CF—has also been linked directly with child EF (Cuevas et al., 2014). Unfortunately, much of the literature on parenting and CF has focused solely on younger children and has failed to include a range of parenting behaviors, which may, inadvertently, strengthen a child’s inflexibility. Within the current study, we aim to extend this line of inquiry utilizing an older cohort of youth (i.e., middle childhood to adolescence) and a more refined operationalization of maladaptive parenting practices, which may contribute to CF—anxiety-enhancing (anxiogenic) parenting practices.
Anxiogenic parenting practices (i.e., modeling, over-involvement, conflict, expressed emotion, parental accommodation, etc.) have long been implicated within developmental models of pediatric anxiety (e.g., Flessner, Murphy, Brennan, & D’Auria, 2017; Ginsburg & Schlossberg, 2002; McLeod, Wood, & Weisz, 2007). As such, a myriad of measurement tools have been designed to capture the relationship between parenting and anxiety, linking anxiogenic parenting practices with increased anxiety severity in youth (Creswell, Murray, Stacey, & Cooper, 2011; Flessner et al., 2017; Knappe, Sasagawa, & Creswell, 2015). Although anxiogenic parenting has primarily been studied within anxious populations (Kagan, Peterman, Carper, & Kendall, 2016; Lebowitz et al., 2013), anxiogenic parenting practices, such as those assessed by the recently developed Parenting Anxious Kids Rating Scale–Parent Report (PAKRS-PR; Flessner et al., 2017), are also likely present in other contexts (e.g., households without anxious children). In fact, Flessner et al. found positive correlations between parent report of child anxiety and parental behaviors such as accommodation and beliefs, over-involvement, modeling, and conflict. This relationship between anxiety and anxiogenic parenting was observed for both a nonclinical sample recruited through Amazon Mechanical Turk and the clinical sample utilized in the parent study to the present investigation. To date, however, research has failed to examine the potential role that these anxiogenic parenting behaviors may have in the maturation of CF. It is possible that conflict and parental warmth may be associated with EF considering the literature on the impact of negativity on EF (Cuevas et al., 2014; Rutter & O’Connor, 2004). For this article, however, three particular anxiogenic parenting practices, parental accommodation, over-involvement, and modeling, may be most conceptually and theoretically linked to difficulties with CF across youth such as by maintaining inflexible behavioral patterns (e.g., excessive question asking, rigid compulsions).
Parental accommodation refers to behaviors exhibited by a parent in response to their child’s anxiety-related symptoms. Accommodation may take the form of modifications to family routines to reduce a child’s distress, avoiding the experience of anxiety in the first place, or participating in a child’s symptoms (e.g., joining rituals, reassuring the child’s concerns; Lebowitz et al., 2013). These adjustments, though intended to reduce distress, may ultimately cause greater distress as children are less likely to learn how to respond to their environments in a flexible way. Importantly, accommodation is likely present across anxious and nonanxious youth’s households—though perhaps in differing amounts (Lebowitz, Scharfstein, & Jones, 2014), as parents may also accommodate child factors other than anxiety (e.g., behavioral difficulties; Flessner et al., 2017). Accommodation has even been linked with worse symptomatology across obsessive-compulsive disorder (OCD) and the anxiety disorders (Flessner et al., 2011; Lebowitz, Panza, Su, & Bloch, 2014; Lebowitz et al., 2013; Merlo, Lehmkuhl, Geffken, & Storch, 2009), though findings are mixed as to whether the degree of accommodation varies with symptom severity (Lebowitz, Panza, & Bloch, 2016; Lebowitz et al., 2013).
Over-involvement is conceptually comparable with accommodation in that it fosters dependence upon the parent and deters a child from developing flexible individualized approaches to environmental stimuli (e.g., decision making). It is important to note that, whereas family accommodation is in reaction to a child’s behaviors, over-involvement may precede symptoms. The presence of over-involvement suggests that parents are excessively controlling of their child’s daily functioning, likely interfering with the child’s sense of self-sufficiency (Flessner et al., 2017). Bowlby (1973) asserted that chronic over-control can lead to psychological dysfunction in children, including anxiety, aggression, and impulsivity. Unfortunately, cultural trends may promote this approach to parenting, whether children exhibit anxious tendencies or not, and may thus represent a factor in dysfunctional cognitive systems across families (Schiffrin, Godfrey, Liss, & Erchull, 2015).
Social modeling, including parental modeling of behaviors, has been discussed in the literature across normative and pathological development (e.g., Boerner, Chambers, McGrath, LoLordo, & Uher, 2017; Fisak & Grills-Taquechel, 2007; Magoon & Ingersoll, 2006; Muris, Steerneman, Merckelbach, & Meesters, 1996). For the purpose of this article, modeling is defined as a parent exhibiting specific behaviors (anxious behaviors in this context) in front of his or her child (Flessner et al., 2017). With regard to CF, it is again possible that parental modeling of certain behaviors might limit a child’s independent decision making and behavioral flexibility. Furthermore, a parent who models behaviors suggestive of cognitive inflexibility (e.g., anxious behaviors) may be more likely to have a child who exhibits the same behaviors—both due to the influence of modeling itself as well as genetic factors—and who may thus also show deficits in CF.
In consideration of the information provided throughout the above review, this article sought to explore the potential relationship between CF and anxiogenic parenting practices, particularly accommodation, over-involvement, and modeling (as assessed via the PAKRS-PR). As described above, we chose to focus upon these three parenting behaviors based on consideration of the operational definitions used to define these parenting constructs and their pursuant conceptual link to CF. A deeper understanding of the potential link between CF and other facets to EF has the potential to significantly advance the field and, ultimately, inform early interventions designed to promote the adaptive development of CF and EF more broadly, perhaps via the use of parent-based strategies. For the current exploratory investigation, our primary aim was to investigate whether parental report of greater anxiogenic parenting practices (e.g., accommodation, over-involvement, modeling, total scale) were predictive of diminished CF in youth. To further specify, we hypothesized that diminished performance will be observed in the two primary facets to CF: set shifting and reversal learning (described in the “Measures” section). Second, and in an exploratory aim, we sought to examine whether parents reporting greater (vs. lesser) engagement in these anxiogenic parenting practices differentiated youth in regard to their performance on a computerized task of CF. To our knowledge, no literature has addressed these domains of parenting in connection with either EF in general or CF more specifically.
Method
Participants
Participant data for the present study were collected as part of a larger, ongoing project examining biological (e.g., neurocognitive functioning) and psychosocial risk factors linked to the development of youth anxiety and obsessive-compulsive and related disorders, as compared with healthy controls. Following approval by the Kent State University Institutional Review Board, youth were recruited along with a parent/caregiver using newspaper advertisements, fliers, and letters to local pediatrician offices and schools from the Northeast Ohio area. A total of 130 participants were recruited for the larger project. One hundred twelve participants completed the measures requisite for the present study (described below) and were thus included in the present analyses. Additional inclusion criteria required participants to be between 9 and 17 years of age and report English as their primary language. Potential participants were excluded if there was any evidence of a pervasive developmental disorder, psychotic disorder, or significant depression, as assessed via structured diagnostic interview. Exclusion was not based on the presence of anxiety-related symptoms in the current study, as the presence of varying levels of anxiety is a very common, stable experience during childhood (Côté, Tremblay, Nagin, Zoccolillo, & Vitaro, 2002; Muris, Merckelbach, Gadet, & Moulaert, 2000). Demographic characteristics for the present sample can be found in Table 1.
Sample Characteristics and Descriptive Statistics for Measures of Interest—M (±SD) Unless Otherwise Noted.
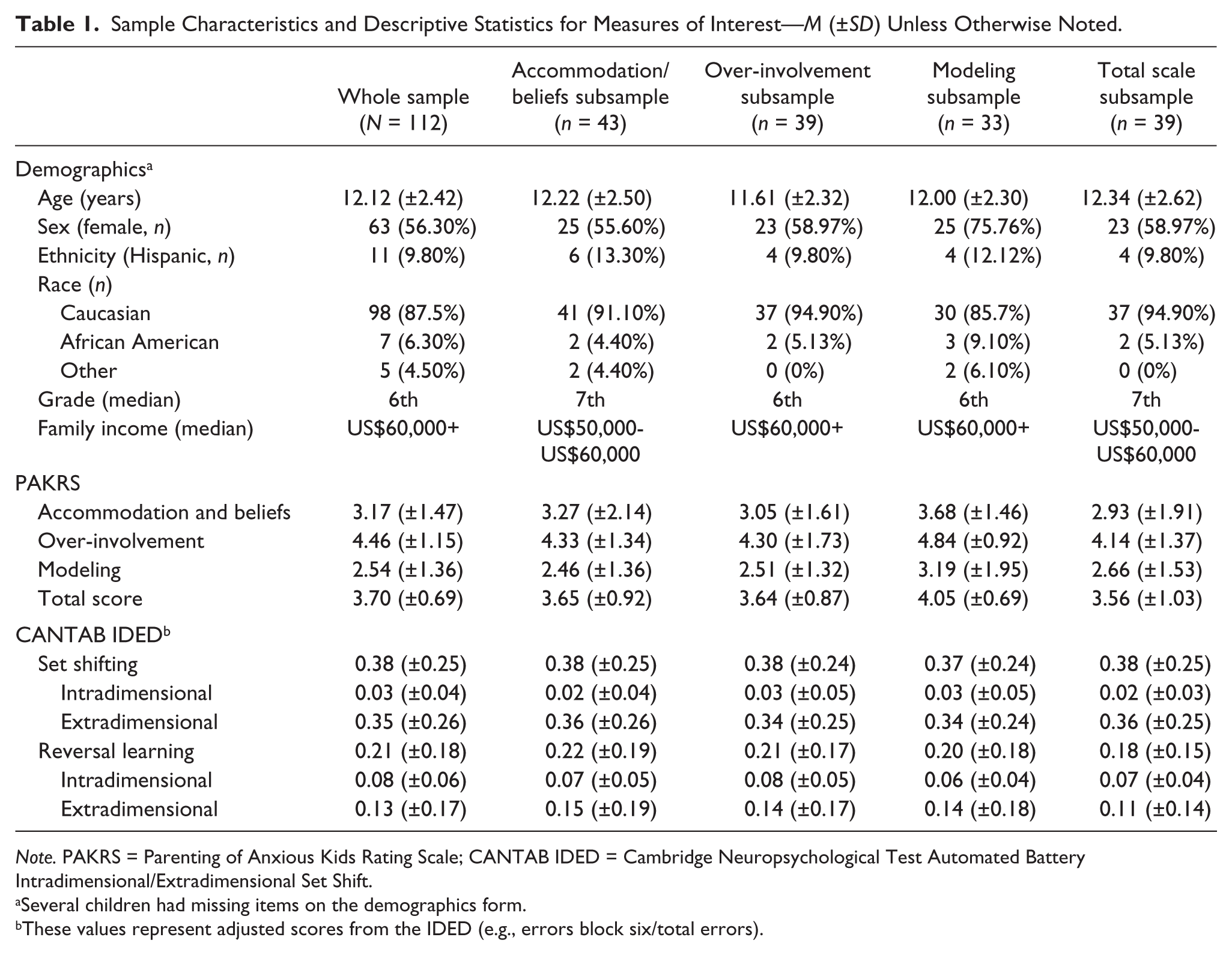
Note. PAKRS = Parenting of Anxious Kids Rating Scale; CANTAB IDED = Cambridge Neuropsychological Test Automated Battery Intradimensional/Extradimensional Set Shift.
Several children had missing items on the demographics form.
These values represent adjusted scores from the IDED (e.g., errors block six/total errors).
Measures
PAKRS-PR (Flessner et al., 2017) is 32-item measure designed to assess anxiogenic parenting behaviors among the families of children 7 to 17 years of age. The PAKRS follows a five-factor model resulting in subscales measuring Conflict (seven items), Over-Involvement (seven items), Accommodation and Beliefs (six items), Modeling (five items), and Emotional Warmth/Support (seven items), as well as a Total Scale score (i.e., summation of all PAKRS-PR items). Items are rated on a 7-point Likert-type scale ranging from 1 (strong disagree) to 7 (strong agree), and each subscale represents the sum of its items with higher scores indicating greater presence of said parenting behavior. The overall scale and each of its subscales have demonstrated strong reliability and validity across both Internet sample and community samples (Flessner et al., 2017). For the present study, only the Accommodation and Beliefs, Over-Involvement, Modeling, and Total Scale Scores were used (see rationale in the introduction). At present, a child-report version of the PAKRS has not yet been validated for use within anxious or nonanxious populations and thus is not reported upon herein.
Cambridge Neuropsychological Test Automated Battery (CANTAB; Cambridge Cognition Limited, 2006) is an automated test battery of neurocognitive functioning. Although the CANTAB consists of several individual subtests, the present study utilized only the below tasks to measure CF. This task was administered third in a series of six tasks (e.g., in order: pattern recognition memory, stop signal task, Intradimensional/Extradimensional Set Shift (IDED), stockings of Cambridge, rapid visual information processing, spatial span).
IDED is a computerized analogue of the WCST (Flessner, Francazio, Murphy, & Brennan, 2015) that tests frontal lobe functioning. CF is measured by way of shifting between rule sets (i.e., set shifting) and reversal learning. Participants must determine an ambiguous “rule” by selecting from two distinct visual stimuli, guided by feedback (e.g., “correct” or “wrong” appears on the screen). The computer periodically changes the rule, beginning a new block and requiring a mental “switch” to a novel rule according to the feedback. The first six blocks are all based on the “shape” rule. The intradimensional shift occurs in Block 6 when new stimuli are presented and the participant must continue to apply the old rule (e.g., shape). The rule is then reversed in Block 7 (e.g., shape A is no longer correct, one must now select shape B to follow the rule). The extradimensional shift occurs in Block 8 when new more complex stimuli are presented and the participant must figure out and follow the “line” rule to be correct. Which stimulus is correct is again reversed in Block 9. Primary outcome measures include total errors within and across these “shift” blocks (i.e., Blocks 6, 7, 8, and 9). For the current investigation, adjusted scores were calculated (as described below) to account for participants’ overall performance on this task.
Procedures
Information was provided over the phone to interested callers regarding the general overview of the methods, procedures, and aims of the overarching study, and a brief phone screen to determine eligibility was completed. Written informed consent, and assent if appropriate, was obtained in person during a scheduled assessment appointment. All participants (children and parents) completed self-report measures, structured and semistructured diagnostic interviews administered in person by a trained graduate research assistant (RA), and an automated neurocognitive test battery consisting of six computerized neurocognitive tasks. All tasks were administered in the same order across all participants.
Data Analysis
To account for overall performance across the IDED, total errors at Blocks 6 and 8 were summed and then divided by the total errors across all blocks for an adjusted score of participant set shifting (e.g., Errors on Block 6 + 8 / Total errors), and total errors at Blocks 7 and 9 were summed and then divided by the total errors for an adjusted measure of reversal learning (Gau & Shang, 2010; Ozonoff et al., 2004). Preliminary analyses suggested that the standard assumptions of normality (e.g., skewness, independent observations) were met within this sample.
Several covariates were considered for each subsequent analysis based on theoretical appropriateness (e.g., child anxiety, depression, age). For the analyses associated with Aim 1, which utilized the whole sample, age was found to be significantly correlated with the adjusted set shifting score (i.e., Blocks 6 + 8 / Total errors) as well as the individual set shifting components (e.g., Block 6 / Total errors) and was thus controlled for in those analyses. For Aim 2, four subsamples were created, one for each parenting practice subscale. Participants were divided into two groups within each based on the answers provided on the PAKRS-PR; each “high” group consisted of scores falling at least one standard deviation above that particular mean, and each “low” group of those falling at least one standard deviation below. Age was again checked for appropriateness as a covariate, and proved significantly correlated with set shifting performance for the subsample pertaining to the Over-Involvement subscale of the PAKRS-PR only. Regression analyses were then conducted to address our hypotheses, as are detailed below in the “Results” section. Hierarchical regression was utilized to best determine the unique predictive contribution made by parenting practices on CF when age was also a contributing factor.
Power analysis was utilized to determine whether our sample size was appropriate to fulfill the requirements of the statistical analyses employed to examine our primary aim (i.e., whether parenting practices are predictive of CF). With guidance from conceptually related studies, G*Power (Erdfelder, Faul, & Buchner, 1996) indicated the need for a minimum of 40 participants to detect a medium sized effect with a power of 0.80. As such, the current sample of 112 youth is sufficient to address our primary aim. Similar analyses in relation to our secondary (exploratory) aim were also conducted with results revealing that approximately 55 individuals would be necessary to detect an effect, should one exist. Although this power analysis suggests that we are slightly underpowered in relation to our secondary aim (ns between 33 and 43; see Table 2), the exploratory nature of this additional aim suggests that such analyses may still be fruitful as a means by which to inform future investigations and refine hypotheses to be tested henceforth.
Summary of Hierarchical Regression Analyses for Cognitive Flexibility in Subsamples Based on High Versus Low PAKRS Subscale Scores.
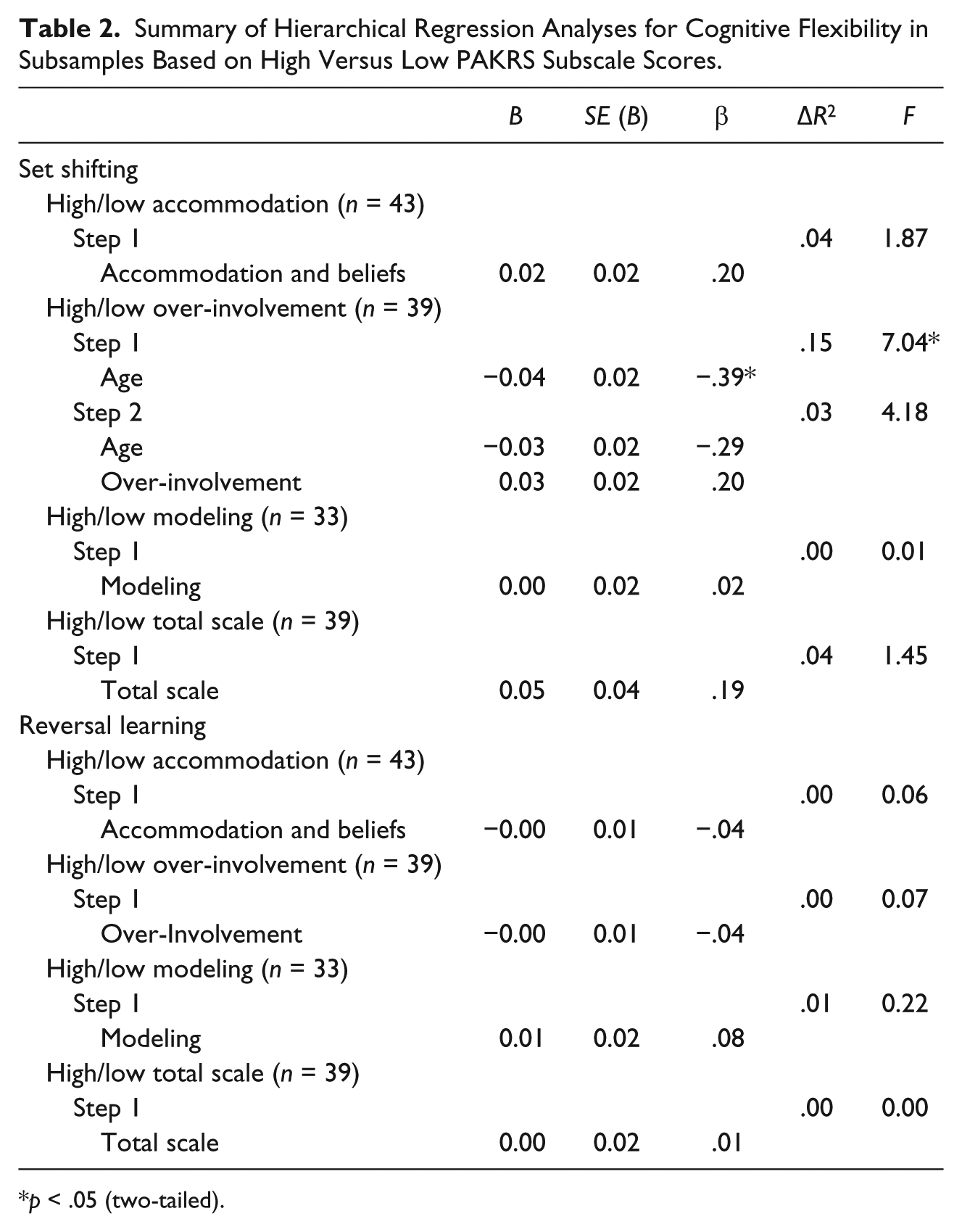
p < .05 (two-tailed).
Results
Descriptive statistics for the primary measures of interest, the PAKRS-PR and the IDED, are provided in Table 1.
Aim 1: Exploring Whether Anxiogenic Parenting Practices Predict CF
Set shifting
In brief, no significant parenting-related predictors were identified for set shifting in this sample of youth. Age (β = −.24, p = .01) was included in Step 1 of each subsequent analysis and accounted for 6% of the variability in set shifting in youth, R2 = .06, F(1, 109) = 6.92, p = .01. When the Accommodation and Beliefs subscale (β = .11, p = .27) was included in Step 2, analyses revealed that it accounted for only an additional 1.1% of the variance in set shifting, ΔR2 = .01, F(1, 108) = 4.09, p = .27. A second regression included Over-Involvement (β = .12, p = .20) as the predictor variable in Step 2, accounting for an additional 1.4% of the variability in set shifting, ΔR2 = .01, F(1, 108) = 4.30, p = .20. A third regression model analyzed whether parental modeling (β = −.02, p = .86) was predictive of set shifting performance above and beyond the effect of age, indicating no significant relationship, ΔR2 < .001, F(1, 108) = 3.45, p = .86. A fourth regression included the PAKRS-PR Total Scale score (β = .08, p = .44) to determine whether there is an overall relationship between anxiogenic parenting practices and set shifting performance on the IDED when age is controlled for yet accounted for only an additional 0.5% of variance, ΔR2 = .01, F(1, 108) = 3.75, p = .44. These results emphasize the importance of considering the dominant influence of age and thus neuropsychological development on set shifting performance but do not suggest a significant contribution for the anxiogenic parenting practices examined herein.
Reversal learning
A secondary grouping of linear regression models were conducted to determine the nature of the relationship between anxiogenic parenting practices and reversal learning, a secondary aspect of CF, similarly suggesting a lack of any statistically significant relationship. The inclusion of the Accommodation and Beliefs scale (β = −.03, p = .73) accounted for only an additional 0.1% of the model’s variability, R2 = .03, F(1, 110) = 0.12, p = .73. Over-involvement (β = −.01, p = .90) failed to account for any additional model variability, R2 < .001, F(1, 110) = 0.02, p = .90. The Modeling subscale (β = .03, p = .74) similarly accounted for a negligible amount of additional variability in reversal learning, R2 = .001, F(1, 110) = 0.11, p = .74. Finally, a fourth regression exploring the relationship between the PAKRS-PR Total Scale score (β = −.02, p = .87) and reversal learning revealed that PAKRS-PR Total Scale scores failed to account for any additional variability, R2 < .001, F(1, 110) = 0.03, p = .87, in reversal learning. Additional details for these models can also be found in Table 3.
Summary of Hierarchical Regression Analyses for PAKRS Subscales, Whole Sample.
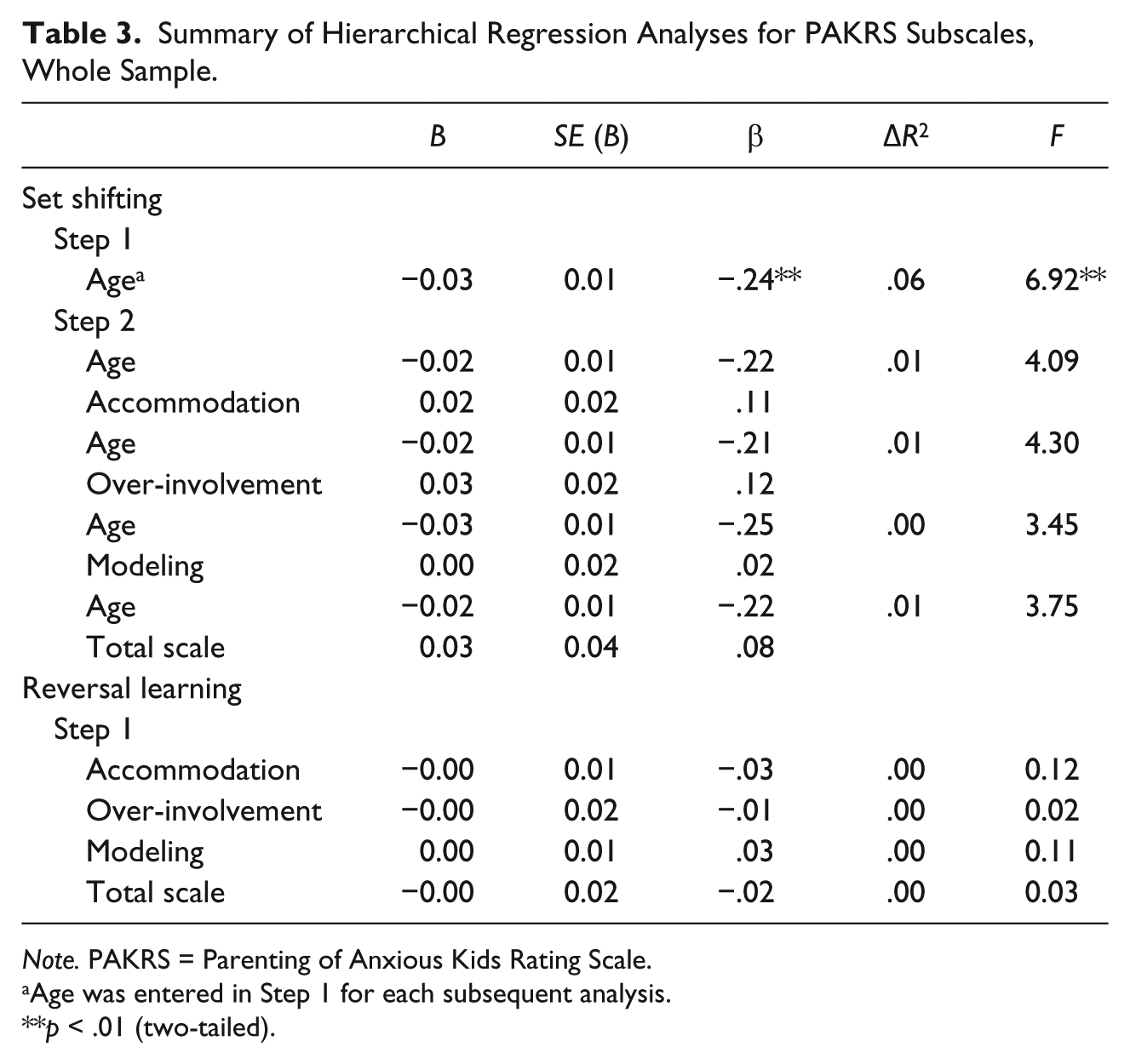
Note. PAKRS = Parenting of Anxious Kids Rating Scale.
Age was entered in Step 1 for each subsequent analysis.
**p < .01 (two-tailed).
Aim 2: Child Performance Based on High Versus Low Anxiogenic Parenting Practices
Set shifting
When the sample was split based on Accommodation and Beliefs subscale scores (e.g., high vs. low levels of accommodation; see Data Analysis section), the subscale (β = .20, p = .18) accounted for an additional 4.2% of the variance in the model as a predictor of set shifting, R2 = .04, F(1, 43) = 1.87, p = .18, but failed to reach statistical significance. Age (β = −.39, p = .01) was included in Step 1 for the split sample based on the Over-involvement subscale and accounted for 15% of the variability, R2 = .15, F(1, 39) = 7.04, p = .01, in set shifting. The Over-involvement subscale itself (β = .20, p = .27), added in Step 2, accounted for only an additional 2.7% of the variance in set shifting performance, ΔR2 = .03, F(1, 38) = 4.18, p = .27. For the split sample based on modeling scores, the Modeling subscale (β = .02,p = .92) again accounted for a negligible amount of the variance in set shifting, R2 < .001, F(1, 33) = 0.01, p = .92. Finally, the split Total Scale score (β = .19, p = .24) accounted for only 3.6% of the model variability, R2 = .04, F(1, 39) = 1.45, p = .24, and failed to reach statistical significance. Overall, none of the parenting practices appears to be predictive of differences in CF between youth whose parents engage in high levels of anxiogenic parenting versus those who reported low levels
Reversal learning
A final set of linear regression models were conducted to determine whether differences in reversal learning exist between youth whose parents engage in high versus low levels of the aforementioned parenting practices. For the split sample based on the Accommodation and Beliefs scores, high versus low levels of accommodation (β = −.04, p = .81) predicted only 0.1% of the variance in reversal learning, R2 = .001, F(1, 43) = 0.06, p = .81. For the high versus low over-involvement split sample, the subscale (β = −.04, p = .79) predicted only 0.2% of the variance in reversal learning within this context, R2 = .002, F(1, 39) = 0.07, p = .79. The Modeling subscale (β = .08, p = .64) accounted for only 0.7% of the variance in the model, R2 = .01, F(1, 33) = 0.22, p = .64. Finally, for the split Total Scale subsample, the Total Scale itself (β = −.01, p = .97) accounted for negligible variance in the model, R2 < .001, F(1, 39) = 0.001, p =.97, in reversal learning. Considering these results together, it appears that no differences in reversal learning exist between high versus low levels of the anxiogenic parenting practices measured herein.
Discussion
This study assessed whether certain anxiogenic parenting practices—specifically accommodation, over-involvement, and modeling—were predictive of poor CF in a sample of youth aged 9 to 17 years. We hypothesized that these practices might reduce autonomy and limit opportunities to exercise self-exploration and plasticity in decision making, thus potentially deterring CF. In contrast, when children are encouraged to take control of navigating their environments independently despite potential stressors, they may be enabled to challenge their previously understood rules (e.g., spiders are terrifying, crying gets me what I want), not unlike the paradigm presented within the IDED. As parental accommodation, over-involvement, and modeling suggest rigidity associated with cognitive inflexibility, and children whose parents are either excessively controlling or overly adaptive do not have as many opportunities to obtain practice in autonomy, we predicted that diminished CF would be associated with these parenting behaviors.
Based on the results of our initial set of analyses (Aim 1), we failed to find support for our hypothesis (i.e., anxiogenic parenting practices are predictive of CF) within this sample. When children were grouped based on high versus low exposure to these parenting practices in accordance with Aim 2, further evidence was provided to suggest that parenting practices did not appear to be significantly influential in regard to adding to the prediction of CF (set shifting or reversal learning) on their own. In alignment with expectations of normative EF development (e.g., Yuan & Raz, 2014), however, child age was a significant predictor of set shifting ability across both aims, though this was not the case in relation to reversal learning. Although these findings are cross-sectional in nature, results demonstrate support for the notion that set shifting, in particular, appears to improve across time as the brain develops. This corresponds with some prior research to note that the influence of parental intervention on child EF is partially explained by language acquisition, which also develops with age (Clark et al., 2013; Matte-Gagne & Bernier, 2011). This suggests the importance of considering additional child factors (e.g., influence of peers, communication styles) in conjunction with strategies, which reduce anxiogenic parenting (e.g., increasing awareness of accommodation; (Lebowitz, Panza, et al., 2014; Wu et al., 2016) in future research addressing CF development.
It is also important to recognize that the null findings with regard to parenting practices should not necessarily be interpreted as meaningless in themselves. Although the novelty of the current investigation is suggestive of strengths, there are several limitations that might have influenced these results. For example, as variability in neuropsychological performance is normative across childhood, the smaller samples may have hindered our ability to detect an effect from subtler influences on CF other than age in Aim 2 (i.e., splitting our sample between high vs. low scores on anxiogenic parenting practice subscales). With this, a small-to-medium effect size was demonstrated within our exploratory second aim, specifically with regard to predicting set shifting ability. Although this effect did not reach significance in the present sample, it again suggests the potential for this line of investigation and indicates a need for follow-up research utilizing larger sample sizes (e.g., N = 55). Of note, the current investigation was also limited by the lack of a validated child-report perspective on anxiogenic parenting. The cross-sectional nature of the current data comes with limitations in itself as no effects can be monitored across time. Future research projects would benefit from tracking the implementation of certain parenting practices and the development of CF (and other measures of EF) utilizing a prospective, longitudinal design.
Reflecting upon these limitations, the current findings serve to provide support for the pursuit of similar investigations in the future, building upon the current literature with hope of contributing to clinical understanding and improvement for youth with impairments in CF. To this, the potential interaction of parenting and developmental stage cannot be ignored, especially as prior research suggests that parental influence plays a particularly important role early in development (e.g., Diamond & Lee, 2011). Additional information could be obtained regarding specific age/developmental stages when certain parenting practices may be most commonly used and/or influential. The incorporation of additional parental traits (e.g., parent psychopathology) and relationship factors (e.g., time spent parenting the child), as well as child perception of parenting practices, could further enrich the literature.
Despite the absence of significant findings herein, this work represents an important bridge in what is currently a large gap in the literature on both CF and parenting practices. Accordingly, these findings, provide a springboard for tailoring future work within this subject area, particularly in light of the small-to-moderate effect sizes note in regard to Aim 2. For example, future work may also seek to more closely delineate the different aspects of CF (e.g., intradimensional vs. extradimensional set shifting and reversal learning) assessed via different modalities (i.e., paper-and-pencil, automated, ecologically valid models, etc.) and the influence anxiogenic parenting practices have on the facets to flexibility. Such investigations are likely to provide considerable insight into any truly causal relationships within these constructs, as well as more mechanistic approaches to their interactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.