
Abstract
Although science’s understanding (e.g., etiology, maintaining factors, etc.) of pediatric anxiety and related problems has grown substantially over recent years, several aspects to anxiety in youths remain elusive, particularly with relation to executive functioning. To this end, the current study sought to examine several facets to executive functioning (i.e., cognitive flexibility, inhibition, planning, working memory) within a transdiagnostic sample of youths exhibiting varying degrees of anxiety symptoms. One hundred six youths completed a comprehensive battery, including several self-report measures (e.g., Multidimensional Anxiety Scale for Children [MASC] or MASC-2) and an automated neurocognitive battery of several executive functioning tasks (Intradimensional/Extradimensional [IDED], Stop Signal [SST], Spatial Span [SSP], Stockings of Cambridge [SOC] tasks). Regression analyses indicated that youths exhibiting marked anxiety symptoms demonstrated increased planning time and probability of inhibition compared with youths with minimal or no anxiety symptoms. Youths with marked anxiety symptoms similarly demonstrated better cognitive flexibility (i.e., set shifting) compared with youths with minimal anxiety. In addition, analyses indicated a trend such that youths exhibiting marked anxiety symptoms demonstrated poorer working memory compared with youths with no anxiety symptoms. Group classification did not predict remaining outcomes. Limitations and future areas of research are discussed.
Collectively, anxiety disorders (e.g., generalized anxiety disorder, specific phobias, social anxiety disorder, separation anxiety disorder, etc.) are one of the most common clusters of pathologies found within youth populations (Merikangas, He, Brody, et al., 2010; Merikangas, He, Burstein, et al., 2010), with correlated impairment in several domains, including family, social, and academic functioning (Grover, Ginsburg, & Ialongo, 2007; Langley, Bergman, McCracken, & Piacentini, 2004; Mychailyszyn, Mendez, & Kendall, 2010). Although science’s understanding of pediatric anxiety has grown substantially (e.g., burgeoning comprehension of related risks factors and impairment, efficacious interventions, etc.), several aspects to anxiety in youths remain elusive, particularly with relation to underlying etiologies. Such limitation necessitates attention as future advancement within this domain (e.g., advancing etiological models of child anxiety, improving therapeutic interventions, etc.) depends upon a broader understanding and underlying pathogenesis of anxiety. Pertinent to this end, the National Institute of Mental Health’s (NIMH) Research Domain Criteria (RDoC) initiative suggests that further understanding of current psychopathology (e.g., anxiety-based disorders) may best be achieved through identification of brain–behavior relationships existing across disorders rather than relationships limited to discrete diagnoses (NIMH, 2011). In concordance with this initiative, research seeking to further understand the pathophysiology of anxiety in youths may benefit from this sort of transdiagnostic approach (i.e., examining anxiety symptoms rather than discrete anxiety diagnoses).
One domain that holds particular promise for advancing science’s understanding regarding the etiology and maintenance of child anxiety is cognitive functioning. Prior research has demonstrated a link between pediatric anxiety and several domains of cognitive functioning, including attention (i.e., ability to attend to specific stimuli, inhibit proponent responses, and focus attention for a prolonged period of time; P. Anderson, 2002), information processing (i.e., fluency, efficiency, and speed of processing), and working memory (i.e., ability to hold and simultaneously process/manipulate information within one’s short-term memory; Visu-Petra, Cheie, & Miu, 2013). With regard to attention, past research suggests that anxious youths (e.g., youths with generalized anxiety disorder, social phobia, and/or separation anxiety disorders, as well as subclinical low-level and high-level anxiety symptoms) demonstrate increased attention to threatening stimuli (e.g., threatening faces), with subsequent difficulty disengaging (Eysenck, Derakshan, Santos, & Calvo, 2007; Rebega & Benga, 2013; Roy et al., 2008). Similarly, research addressing information processing among this population indicates processing biases toward threatening stimuli, including words and pictures (Hadwin, Garner, & Perez-Olivas, 2006, Hoffman, Ellard, & Siegle, 2011). Furthermore, research demonstrating memory biases among anxious youths indicate impairments in working memory storage (Visu-Petra, Cheie, Benga, & Alloway, 2010; Visu-Petra, Tincas, Cheie, & Benga, 2010). Collectively, though research demonstrates cognitive biases (i.e., attention, information processing, and working memory biases) among anxious youths, explicit neuropsychological mechanisms (e.g., potential higher level brain processes) which may foster these biases are uncertain.
Presumably, clarification of the mechanisms underlying the biases mentioned above may be achieved through examination of executive functioning (i.e., higher order neurocognitive processes underlying goal directed behaviors; Suchy, 2009). Although debate persists regarding explicit factors of executive functioning, research often posits several components to this domain, including cognitive flexibility/set shifting (i.e., ability to switch between tasks as necessary for a particular goal; Ionescu, 2012), inhibitory control (i.e., ability to stop a prepotent response; B. R. Williams, Ponesse, Schachar, Logan, & Tannock, 1999), planning (i.e., ability to organize and follow a sequence of steps for a particular goal; Owen, 1997), and working memory (defined within the previous paragraph). Given the complexity of these facets to executive functioning (i.e., research demonstrating these components as both distinct and unifying processes; Miyake et al., 2000) and implications with respect to overlapping neurology (e.g., frontal cortical activation indicated in noted cognitive processes and executive functioning domains, frontal lobe impairment indicated among anxious individuals; Martin, Ressler, Binder, & Nemeroff, 2009), it is plausible that executive functioning may, collectively, contribute to the development and maintenance of the impairments in information processing, attention, and working memory noted previously. In fact, recent research hypothesizes that pathological anxiety may stem from the inability of executive functioning to inhibit limbic responses (Martin et al., 2009). For example, cognitive flexibility and inhibitory control may be key mechanisms in controlling attention and information processing, with deficits in executive functioning contributing to attentional and information processing biases noted in anxious youths. Similarly, considering the unifying nature of executive functioning (Visu-Petra, Stanciu, Benga, Miclea, & Cheie, 2014), though working memory biases inherently implicate an executive functioning impairment in itself (i.e., impairment in the working memory domain), additional mechanisms may also contribute to this bias. For example, impairment of inhibition and cognitive flexibility may lead to increased attention to excess stimuli (cognitive interference), which may in turn contribute to impairment in working memory processes/storage capacity (Visu-Petra, Cheie, et al., 2010). Given these hypotheses, youths with anxiety may show differential performance on tasks of executive functioning.
To date, executive functioning has received relatively little attention in the pediatric anxiety literature. Those studies that exist, however, do suggest impaired executive functioning among anxious youths (i.e., lowered performance on neutral and emotionally modified tasks of working memory, inhibition, and cognitive flexibility; Eschenbeck, Kohlmann, Heim-Dreger, Koller, & Leser, 2004; Ng & Lee, 2015; Richards, French, Nash, Hadwin, & Donnelly, 2007; Visu-Petra et al., 2014). For example, Ursache and Raver (2014) examined executive functioning in at-risk youths aged 9 to 12 years, with findings indicating that higher trait anxiety predicted lower performance on measures of working memory and inhibitory control (i.e., Hearts and Flowers Task and the Color-Word Stroop Task). Similarly, Toren and colleagues (2000) assessed youths with an anxiety disorder (i.e., separation anxiety disorder and/or overanxious disorder) aged 6 to 18 years, with results demonstrating lowered performance on a measure of cognitive flexibility (i.e., Wisconsin Card Sorting Test; Toren et al., 2000). Collectively, though findings largely support executive functioning deficits among anxious youths, conflictive findings exist as well. For example, (Günther et al., 2004) assessed working memory and attention (using the Rey Auditory-Verbal Learning Test and a simple reaction time task) among youths with an anxiety disorder (i.e., social phobia and generalized anxiety disorder), with results demonstrating no differences between anxious youths and controls. What is more, several important limitations exist to these prior studies, including (a) use of inconsistent measures of executive functioning (e.g., use of different measures of working memory in different studies, with rare overlap between measures), (b) often a focus on one domain of executive functioning rather than a comprehensive assessment (e.g., studies focused on working memory rather than a comprehensive assessment including additional executive functioning domains), and (c) often a focus on discrete anxiety diagnoses (e.g., requirement of clinical diagnoses to be included within samples) rather than viewing anxiety as a dimensional and transdiagnostic construct in accordance with the RDoC initiative and developmental psychopathology research. Notably, dimensional and transdiagnostic research may be particularly critical in the anxiety domain, given inclusivity of anxiety (i.e., symptoms experienced on a continuum to some degree by all individuals) as well as frequent comorbidity among the anxiety symptoms. As such, limitations in conjunction with the scant research within this domain (i.e., executive functioning in pediatric anxiety) strongly support the need for further research.
With both the RDoC initiative and limitation to prior research in mind, the current study aims to investigate the relationship between executive functioning and pediatric anxiety. Specifically, this study seeks to examine whether pediatric anxiety symptoms predict several facets to executive functioning (i.e., cognitive flexibility, inhibitory control, planning, and working memory), as measured by the Cambridge Automated Neuropsychological Test Assessment Battery (CANTAB). To examine this relationship, we utilized a transdiagnostic sample of youths exhibiting varying degrees of anxiety symptoms as assessed via a dimensional measure of youth anxiety (i.e., Multidimensional Anxiety Scale for Children [MASC]). Based on the majority of prior research in this area, we hypothesize that youths experiencing increased anxiety will exhibit differential performance, specifically poorer performance, on tasks of executive functioning (e.g., CANTAB tasks of cognitive flexibility, inhibitory control, working memory, planning).
Method
Participants
Participant data were collected as part of a larger, ongoing project examining biological and psychosocial risk factors for pediatric anxiety and related disorders. In total, 130 participants from Northeastern Ohio were recruited via newspaper advertisements, fliers, and letters to pediatricians and schools. Inclusion/exclusion were not based on the presence of anxiety-related symptoms in this study. Specific inclusion criteria required participants to be between 9 and 17 years of age, report English as their primary language, and provide complete data for all primary outcomes measures (see “Measures” section). Potential participants were excluded if there was any evidence of pervasive developmental disorder, due to its impact on participant ability to fully complete study procedure. Potential participants were also excluded if there was any evidence of psychotic disorder or current major depressive disorder, due to the seriousness of these mental health concerns. Disorder-specific exclusion criteria was assessed via structured diagnostic interview. Participants with incomplete data (n = 23) were excluded from analyses, resulting in 106 participants, including 39 youths demonstrating no anxiety symptoms (M age = 11.94), 40 youths demonstrating minimal anxiety symptoms (M age = 11.7), and 27 youths demonstrating marked anxiety symptoms (M age = 12.96). There were slightly more females in the youths with no anxiety sample (51.3%) and with minimal symptoms (51.2%). The sample with marked symptoms was predominately female (70.4%). Income for all groups was reported as being greater than US$60,000 (see Data Analytic Plan for a description of group formation and Table 1 for participant demographics). A priori group-based comparisons revealed no statistically significant difference between groups with respect to demographic characteristics.
Participant Demographics and Clinical Characteristics.
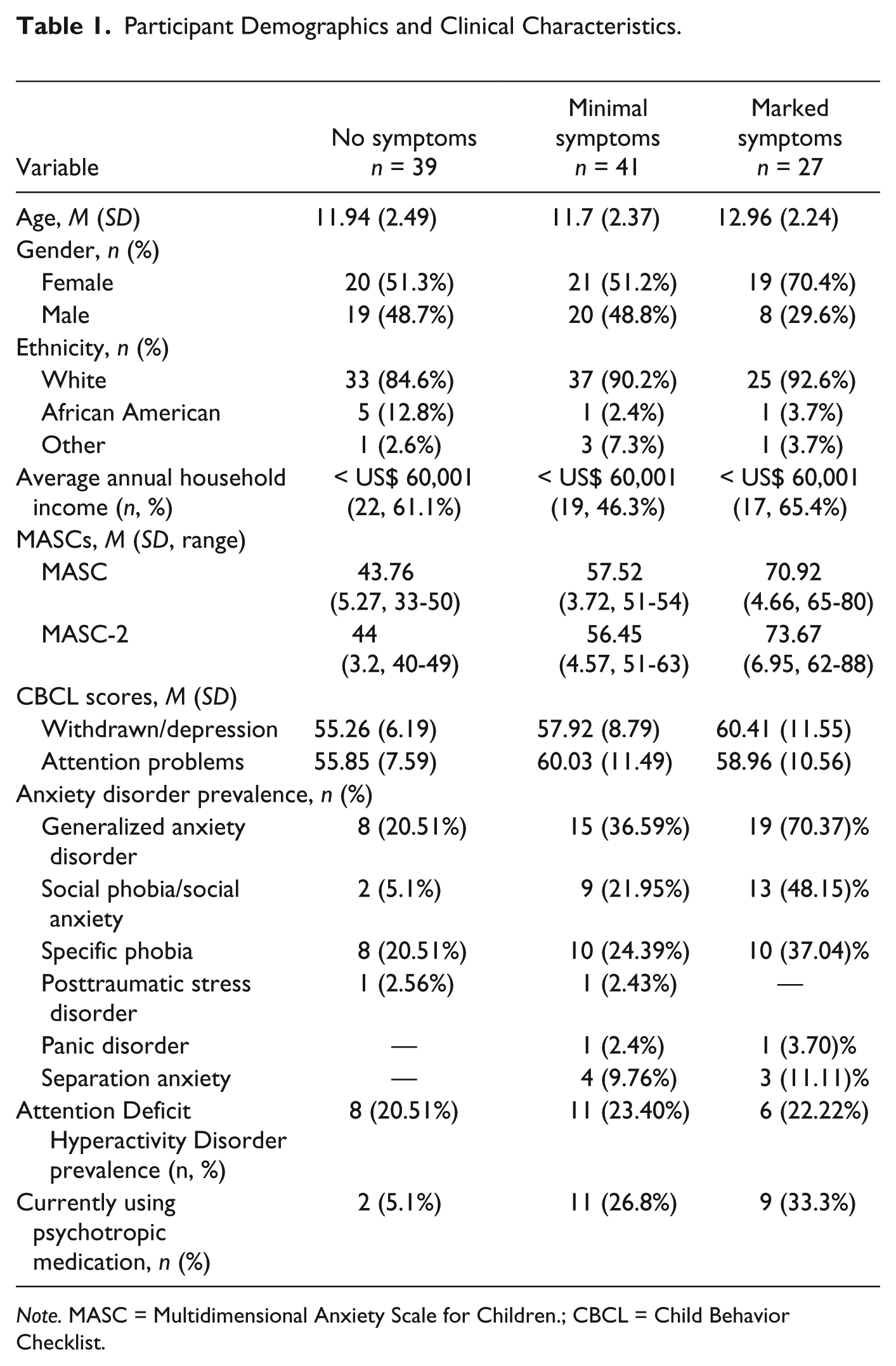
Note. MASC = Multidimensional Anxiety Scale for Children.; CBCL = Child Behavior Checklist.
Measures
Clinical symptoms
The Anxiety Disorders Interview Schedule for Children–Fourth Edition (ADIS-IV)
ADIS-IV (Silverman & Albano, 1996) is a semistructured interview that diagnoses anxiety disorders and comorbidities in children and adolescents. It is administered to parents and children jointly. The ADIS-IV has been shown to have excellent test–retest reliabilities throughout all age and disorder ranges (Langley et al., 2004).
The Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL)
K-SADS-PL (Kauffman et al., 1997) is a semistructured interview assessing both past and present diagnoses. It can be administered to children with or without input from their parents, and consists of a base screening portion and subsequent diagnostic supplements. The K-SADS-PL has been shown to have strong psychometric properties (Kaufman et al., 1997; Birmaher et al., 2009). The K-SADS-PL was used to assess for exclusion criteria of depression and psychotic disorders.
The Multidimensional Anxiety Scale for Children (MASC and revised MASC-2)
The MASC is a 39-item, 4-point Likert-type scale consisting of Physical Symptoms, Harm Avoidance, Social Anxiety, and Separation/Panic (March, 1999; March, 2012b; March, Parker, Sullivan, Stallings, & Conners, 1997). Past research assessing the MASC demonstrates strong psychometric properties (E. R. Anderson, Jordan, Smith, & Inderbitzen-Nolan, 2009). The revised MASC-2 was also used to obtain child anxiety-related symptoms, as the MASC became unavailable for purchase midway through the study. The MASC-2 is a 50-item self-report, with the addition of 11 items related to obsessive-compulsive disorder (OCD).
The MASC-2 demonstrates good discriminative validity (March, 2013). Both the MASC and MASC-2 are child self-report measures that produce subscale and total scores, with higher scores indicating increased anxiety symptoms. In the present study, 71 participants took the MASC and 37 took the MASC-2.
Child Behavior Checklist (CBCL)
The CBCL is a 112-item parent-report scale assessing child symptoms across several domains, including social skills, school functioning, and emotional and behavioral problems (Achenbach, 1991). Prior research utilizing the CBCL demonstrates strong reliability and validity among youth populations (Achenbach & Edelbrock, 1983; Dutra, Campbell, & Westen, 2004; Ivanova et al., 2007). Within the current study, the CBCL Withdrawn/Depression and Attention subscales were used to assess symptoms of depression and inattention, respectively. The CBCL syndrome scales have demonstrated adequate reliability and validity in discriminating between referred and nonreferred pediatric populations (Achenbach & Rescorla, 2001; Ebesutani et al., 2010).
Executive functioning
Cambridge Automated Neuropsychological Test Assessment Battery (CANTAB)
The CANTAB is an automated test battery of neurocognitive functioning used to measure cognitive flexibility, inhibition, working memory, and planning (Cambridge Cognition, 2011) among other neuropsychological domains. For purposes of the larger study from which these data were collected, participants completed a total of six subtests from the CANTAB. All participants were presented with these tests in identical order. What follows, however, is a brief description of the four CANTAB subtests employed from this larger battery most germane to the present study and designed specifically to assess executive functioning.
Intradimensional/Extradimensional (IDED) Task
The IDED is a frontal lobe sensitive computerized analogue of the Wisconsin Card Sorting test and is used to measure reversal learning and set shifting. In this task, the participant is presented with two images containing color-filled shapes and white lines. During the first trial, the participant is presented with two color-filled shapes and is instructed to use trial and error to select the correct image and learn an unknown rule. After touching each image, participants are given feedback indicating whether or not their selection was correct. Throughout this task, the shapes and lines arbitrarily and independently change positions on the screen. After demonstrating rule acquisition, the images and/or rules are changed, requiring a mental “switch” to the novel rule and an ability to respond according to feedback. In the initial trials, compound shapes are introduced (i.e., with lines); however, the color-filled shapes are the only relevant dimensions (i.e., shifts are intradimensional). After several trials, the rule shifts so that the lines become the relevant dimension (the extradimensional set shift) and participants must switch from the previously adhered shape dimension and irrelevant stimuli to apply a new line dimension rule. Prior research utilizing the IDED most typically utilizes total errors at Blocks 6, 7, 8, and 9 as the primary outcome measures of choice for assessing cognitive flexibility. In particular, total errors at Blocks 6 and 8 are summed for a measure of participant set shifting (Corbett, Constantine, Hendren, Rocke, & Ozonoff, 2009; Ozonoff et al., 2004) and total errors at Blocks 7 and 9 are summed for a measure of reversal learning (Gau & Shang, 2010; Ozonoff et al., 2004).
Stockings of Cambridge (SOC) Task
The SOC is a frontal lobe sensitive computerized spatial planning task, providing a measure of planning and organization. Within the SOC, participants are shown a split screen display containing three colored balls and are instructed to move the three identical balls in the lower display to match the pattern of balls in the top display. Each trial consists of a gradually increasing number of moves. The participant’s planning ability is measured via time taken and moves made to complete the pattern. In the second type of task, the participant is shown a similar split screen display of colored balls. He or she is instructed to move the balls in the bottom arrangement in a manner mirroring the pattern of moves made in the top arrangement. Primary outcome variables for the SOC include the number of problems solved in minimum number of moves as well as mean initial and subsequent thinking time for 2-, 3-, 4-, and 5-move problems (Corbett et al., 2009; Green et al., 2009).
Spatial Span Task (SST)
The SSP is a computerized task analogous to the Digit Span test. The SSP is a task of working memory capacity and is sensitive to frontal lobe functioning. During the SSP, participants are presented with a standard pattern of white boxes, some of which briefly change color. Upon hearing a tone, participants are instructed to touch the boxes in the same order in which they changed color—with the number of boxes changing color increasing from two to nine during the task. The primary outcome of the SSP is spatial span length, which represents the longest sequence successfully recalled by the participant (Gau & Shang, 2010).
Stop Signal Task (SST)
The SST is considered to be a validated classic stop signal response inhibition task (Cambridge Cognition, 2011). which has been used to measure motor response inhibition in children in multiple contexts (e.g. attention disorders, obesity, obsessive-compulsive disorder, etc.; Hybel, Mortensen, Lambek, Thastum, & Thomsen, 2017; Kulendran et al., 2014; Schneider, Lam, & Mahone, 2016). The SST begins with a sample trial in which participants are presented with a white ring in which a visual stimulus appears (i.e., an arrow pointing either to the right or left of the screen). Subjects are instructed to press buttons on a push-pad corresponding to the arrow’s direction (i.e., left button when a left arrow appears, right button when a right arrow appears). After 16 trials, a second phase begins in which participants are told to perform the same previous corresponding actions (“go” trials), but if they hear an auditory beeping signal, they should not push the button. The time span between the flashing arrow and the auditory signals are automatically adjusted depending on the participant’s performance. Primary outcomes measures of the SST include stop signal reaction time (i.e., estimated length of time taken to inhibit a response approximately 50% of the time), mean reaction time on go trials (i.e., average estimated time taken to execute a response on “go” trials), stop signal delay (i.e., estimated length of delay between stimulus and stop signal at which participant was able to stop 50% of the time), direction errors (i.e., number of times where participant presses the wrong button), and overall probability of successful inhibition (i.e., number of stop trials successfully inhibited divided by number of stop trials presented; Aron & Poldrack, 2006; Brennan, Francazio, Gunstad, & Flessner, 2015).
Procedures
The current study was approved by Kent State University’s (KSU) Institutional Review Board via the Pediatric Anxiety Research Clinic (PARC). Upon contact, graduate research assistants provided families with an overview of the study design, procedures, and aims, and conducted a brief phone screen to determine participant eligibility. If eligible, the child and one biological parent were mailed a comprehensive packet of several parent- and self-report forms (e.g., MASC/MASC-2, CBCL), to be completed before arriving for their scheduled session. All scheduled sessions took place at the PARC and lasted approximately 3 hr. After the informed consent process was completed, a trained graduate assistant administered structured and semistructured interviews jointly to the parent and child. Consented children were then asked to complete a neurocognitive test battery consisting of several CANTAB tasks, including the IDED, SOC, SSP, and SST. All participants were administered CANTAB-related tasks in identical order. While children completed CANTAB tasks, the parent completed several additional self-report forms, including a demographics questionnaire (e.g., gender, age, current medications). All participating families were compensated monetarily upon study completion.
Data analytic plan
Power analysis
Based on the range of effect sizes (i.e., small to large) gathered in previous research assessing executive functioning in anxious youths (Tincas, Dragos, Ionescu, & Benga, 2007; Ursache & Raver, 2014), a priori calculations indicated a total sample size of 85 to produce at least a medium effect size with four predictors (maximum number of predictors included in current analyses). As such, the present sample (n = 106) is deemed sufficient to detect medium effects.
Group classification
To employ a more dimensional and transdiagnostic approach, classification of anxiety symptoms/groups (i.e., no symptoms, minimal symptoms, and marked symptoms) within the current study was developed using participant scores from the MASC or MASC-2. Cutoff scores for this measure are based on previous research establishing clinical cutoffs of the MASC/MASC-2, thus further enhancing clinical utility of study findings (March, 1997; March, 2012a). Inclusion within the “no symptoms” group required an MASC/MASC-2 Total T-score less than or equal to 50. Inclusion within the “minimal symptoms” group required an MASC/MASC-2 Total T-score between 51 and 64. Inclusion within the “marked symptoms” group required an MASC/MASC-2 Total T-score greater than or equal to 65.
Executive functioning assessment
Two sets of regression analyses were used to examine whether group classification predicted performance on primary outcome variables from the IDED, SOC, SSP, and SST (see “Measures” section for all primary outcome variables). To allow for multiple comparisons, the first set of regression analyses was used to compare youths with minimal and marked anxiety symptoms with youths with no anxiety symptoms (i.e., youths with no anxiety symptoms used as the dummy coding reference group). The second set of regression analyses was used to compare youths with marked and no anxiety symptoms with youths with minimal anxiety symptoms (i.e., youths with minimal anxiety symptoms used as the dummy coding reference group). Based on prior literature, variables (i.e., age, gender, current medication use, symptoms of depression, symptoms of inattention/hyperactivity) potentially linked to executive functioning performance were examined via correlational analyses (see Tables 2 and 3). These analyses were particularly important to help isolate the effect of anxiety symptoms -above and beyond additional independent variables - on executive functioning performance, thus providing a more explicit answer to our research question. Those potential covariates demonstrating a statistically significant relationship (p < .01) with any of our outcome variables (i.e., primary outcomes variables of the IDED, SOC, SSP, and SST) were considered as covariates. As a result, only the following covariates were used within the analyses described below: symptoms of inattention (SOC Mean Initial Think Time 2 Moves, SST Stop Signal Reaction Time) and depression (SST Stop Signal Reaction Time) and child age (SSP Spatial Span Length, SST Stop Signal Reaction Time). Assumptions related to regression analyses were also examined. Violations to normality were detected for several SST (direction errors, stop signal reaction time, probability of inhibition) and SOC outcome variables (i.e., mean initial think time for 2 and 5 moves, mean subsequent think time for 2, 3, and 5 moves) and thus were transformed using the square root function. Additional assumptions of regression analyses were met. The focus of this study is centered upon child anxiety status predicting executive function performance. As such, although overall model significance is reported below (see Tables 5 -8), the alpha level of individual predictors was used to determine the particular relevance of the respective predictor.
Correlation Matrix for Potential Covariates Under Consideration for IDED, SSP, and SST Analyses.

Note. IDED = Intradimensional/Extradimensional Task; SSP = Spatial Span Task; SST = Stop Signal Task; Bold-faced values indicate signficant correlations.
Continued Correlation Matrix for Potential Covariates Under Consideration for SOC Analyses.
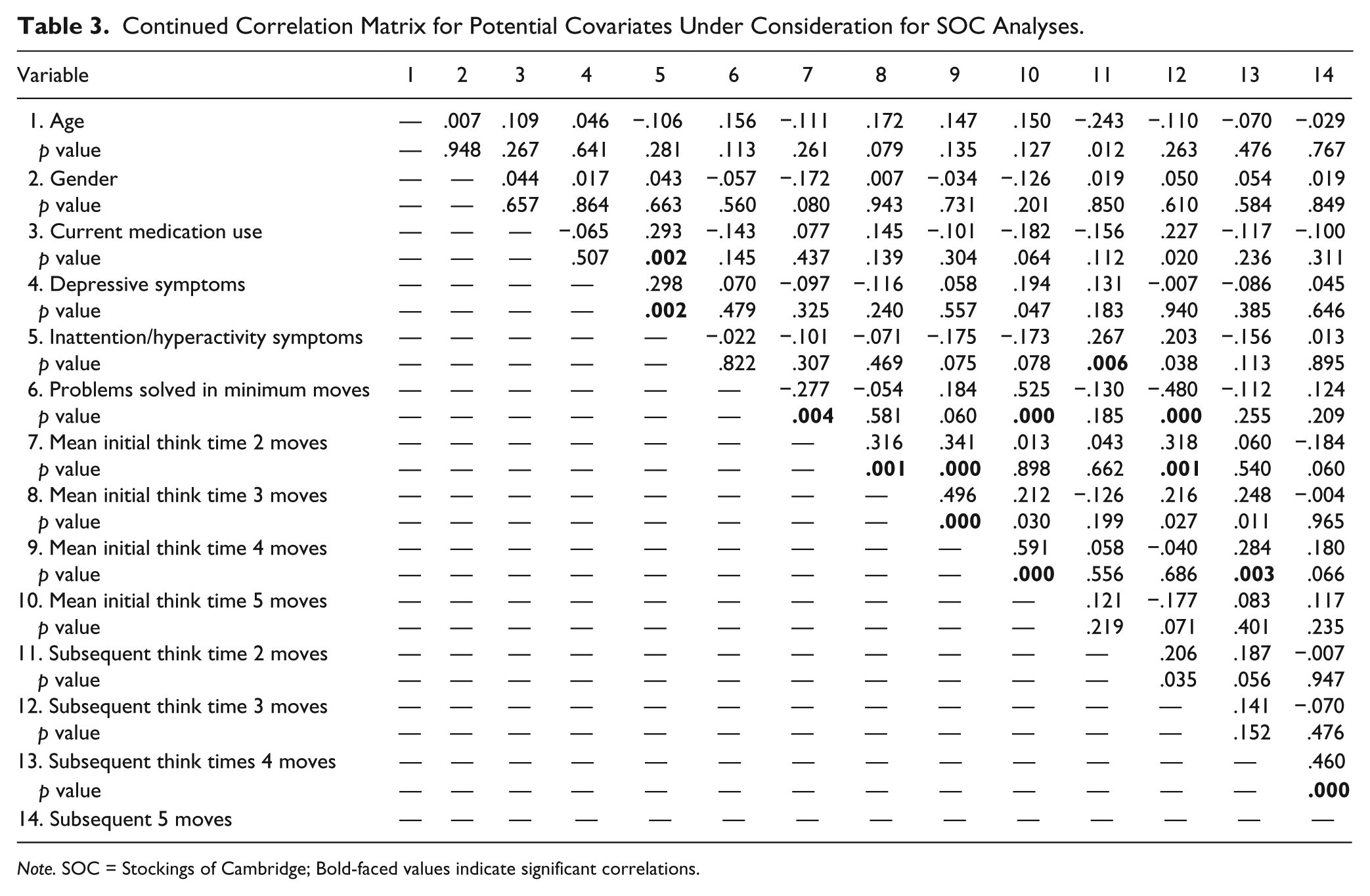
Note. SOC = Stockings of Cambridge; Bold-faced values indicate significant correlations.
Results
Raw means for noted outcome variables and results of regression analyses are presented in Tables 4 to 8. What follows is a brief overview of findings presented in Tables 5 to 8. Note that for repeated analyses (i.e., no anxiety symptoms compared with minimal anxiety symptoms; minimal anxiety symptoms compared with no anxiety symptoms), only first obtained coefficients are reported due to redundancy in the values obtained. Statistical significance was identified by a p value less than .05 and a trend was identified by a p value less than .10.
Participant Mean Scores for IDED, SOC, SSP, and SST Primary Outcome Variables.
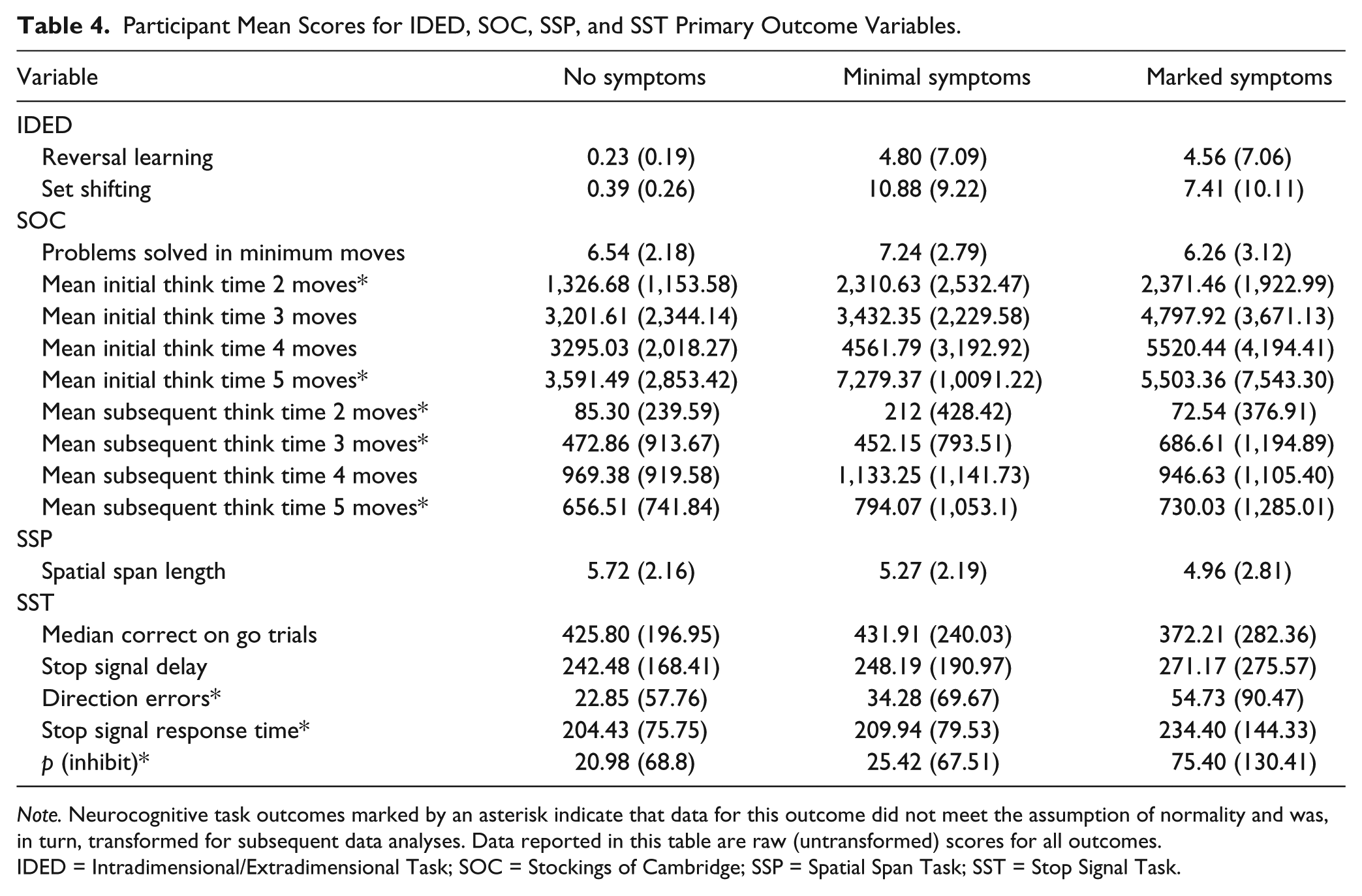
Note. Neurocognitive task outcomes marked by an asterisk indicate that data for this outcome did not meet the assumption of normality and was, in turn, transformed for subsequent data analyses. Data reported in this table are raw (untransformed) scores for all outcomes.IDED = Intradimensional/Extradimensional Task; SOC = Stockings of Cambridge; SSP = Spatial Span Task; SST = Stop Signal Task.
Summary of Regression Analyses for IDED.
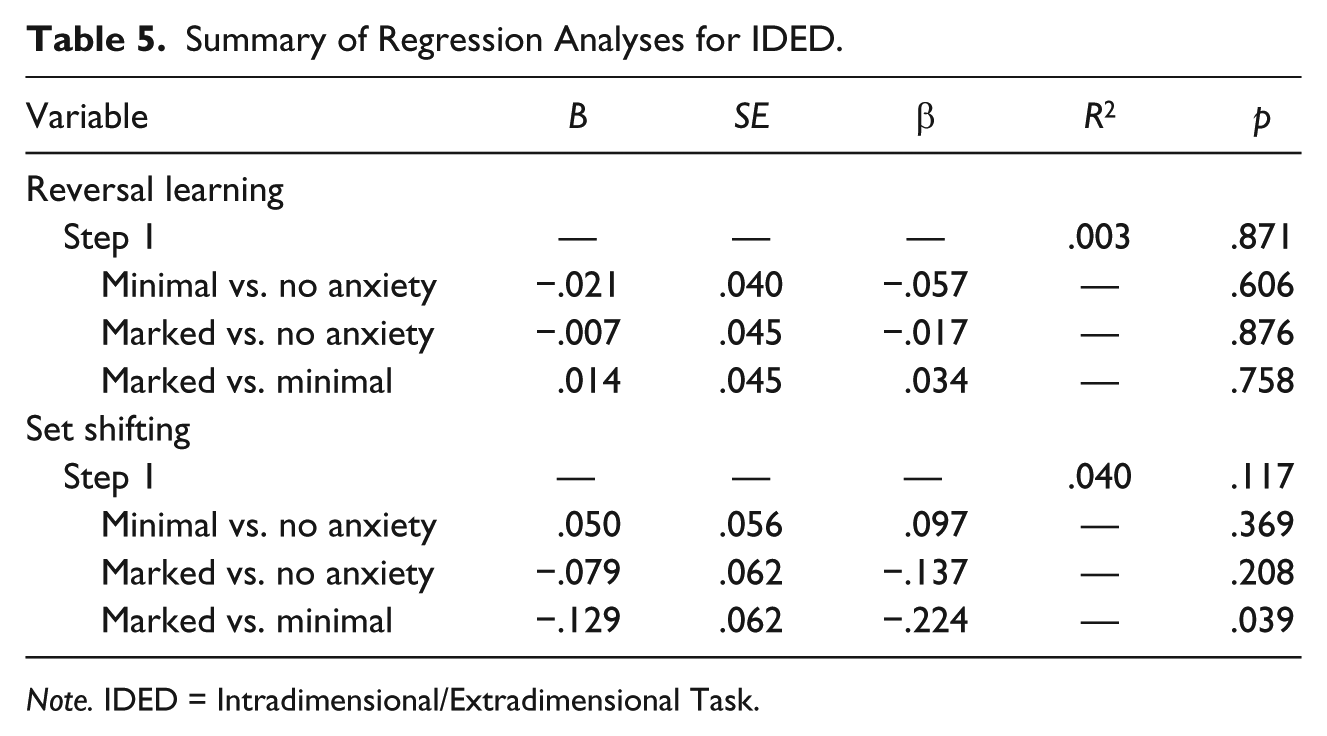
Note. IDED = Intradimensional/Extradimensional Task.
Summary of Regression Analyses for SOC.
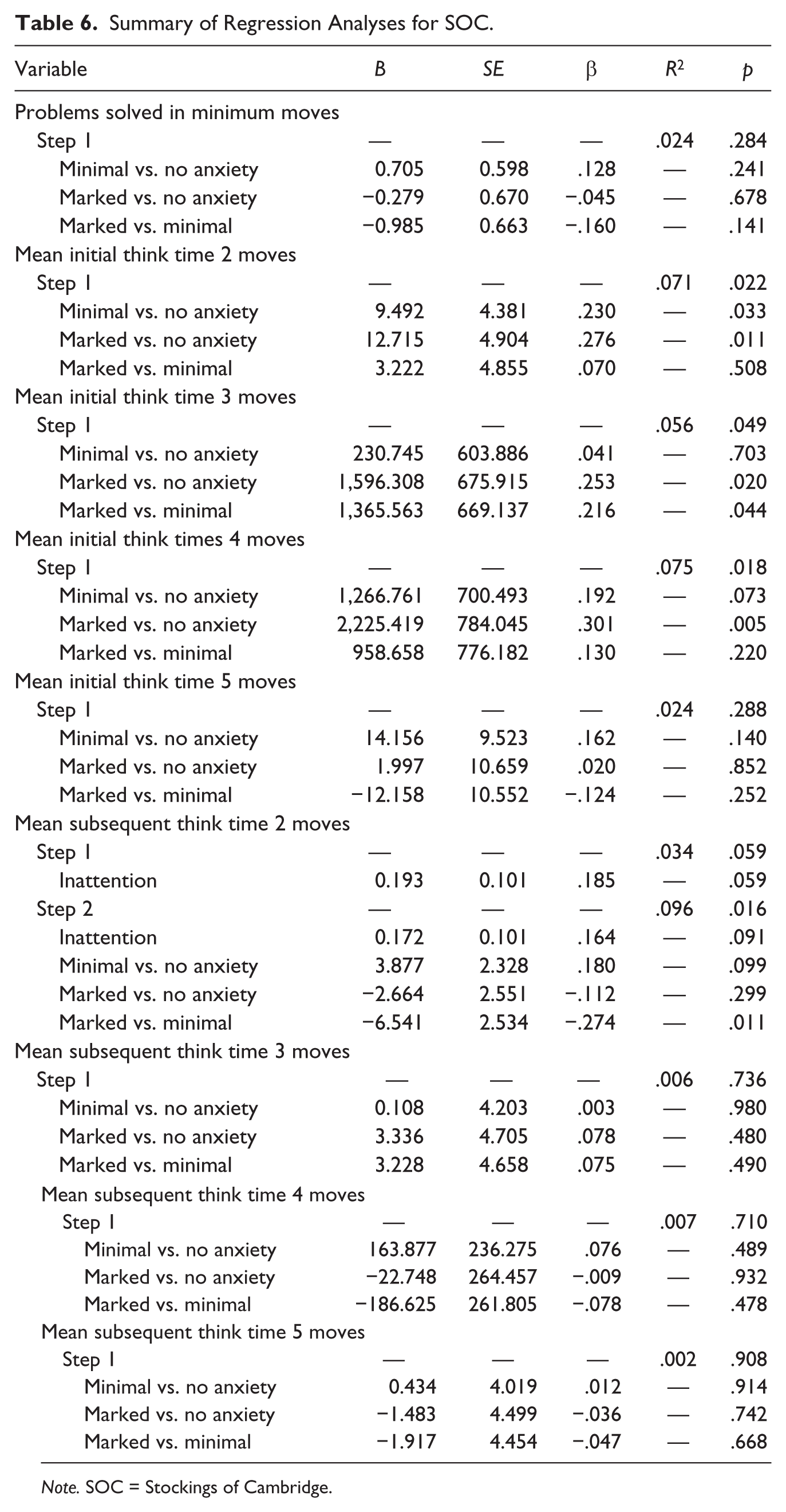
Note. SOC = Stockings of Cambridge.
Summary of Regression Analyses for SSP.
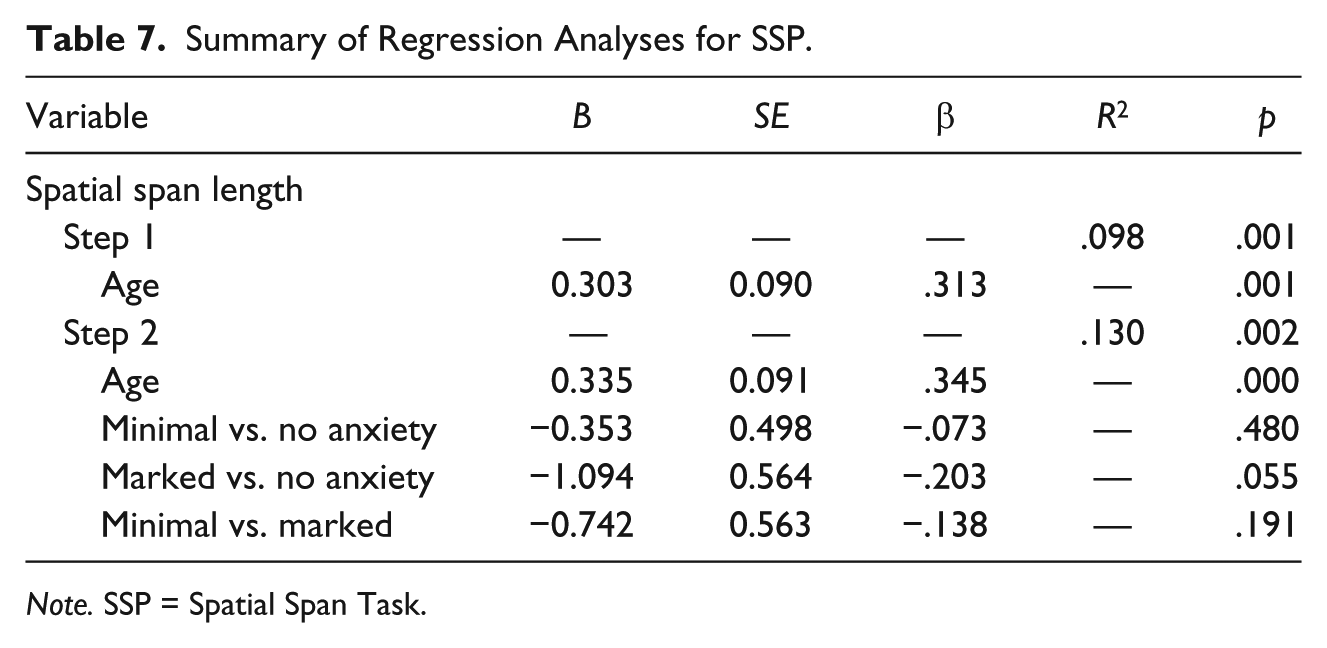
Note. SSP = Spatial Span Task.
Summary of Regression Analyses for SST.
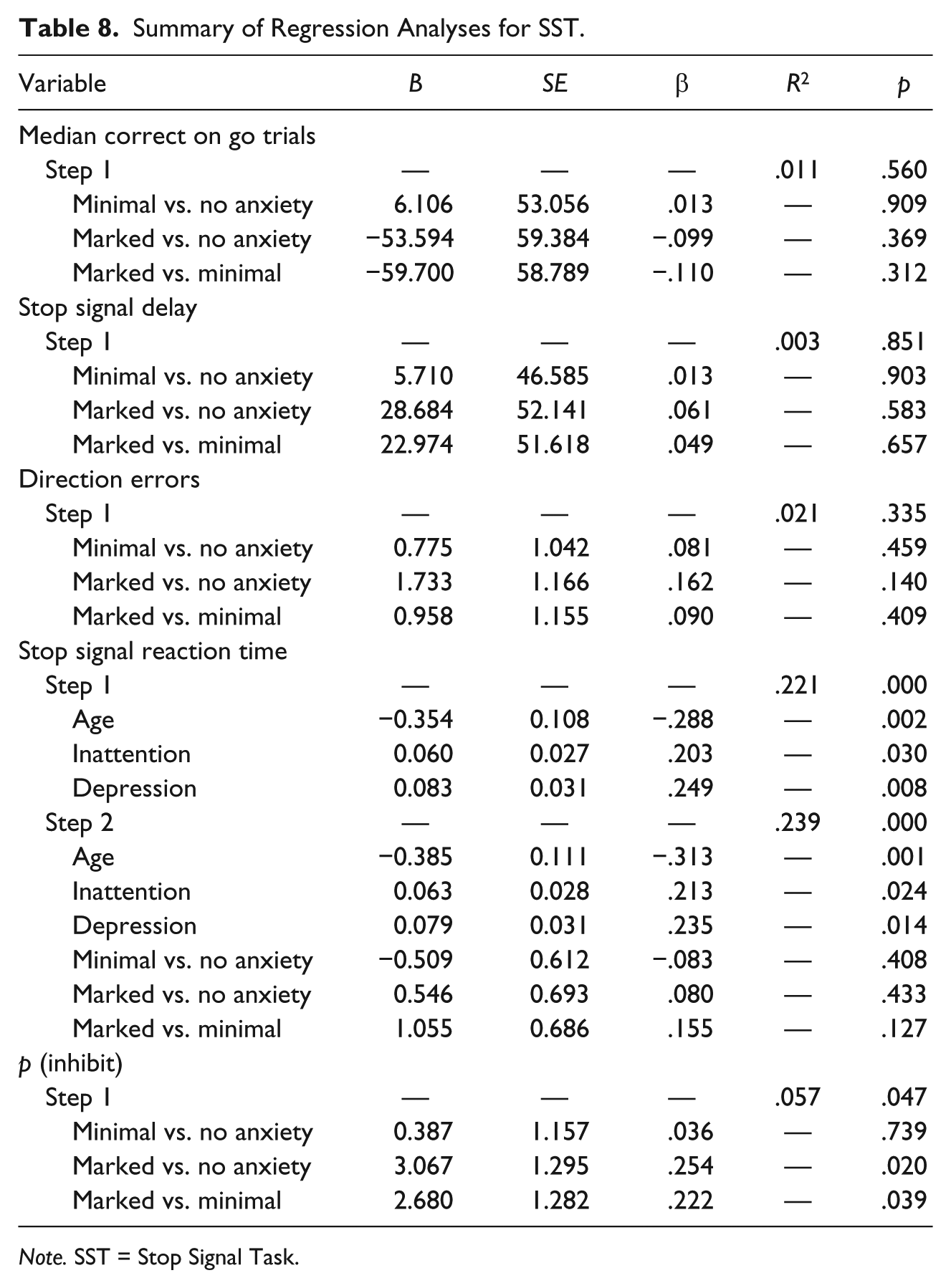
Note. SST = Stop Signal Task.
SST (Inhibition)
Finally, results demonstrated that group classification did significantly predict inhibition. Specifically, youths demonstrating marked anxiety symptoms exhibited increased overall probability of successful inhibition compared with both youths with minimal (β = .222, p = .039) and no anxiety symptoms (β = .254, p = .020). Group classification did not significantly predict remaining SST outcomes. See Table 8 for SST outcomes.
IDED (Cognitive Flexibility)
Although results demonstrated a weak trend for the overall model (R2 = .040, p = .117), group classification did significantly predict cognitive flexibility, such that youths demonstrating marked anxiety symptoms indicated better cognitive flexibility (i.e., set shifting) compared with youths with minimal anxiety symptoms (β = −.224, p = .039). Group classification did not significantly predict remaining IDED outcomes (i.e., reversal learning). See Table 5 for IDED outcomes.
SOC (Planning and Organization)
Results indicated that group classification did significantly predict planning, in that youths demonstrating minimal anxiety symptoms exhibited longer mean initial think time on two move problems (β = .230, p = .033) compared with youths demonstrating no anxiety symptoms. Similarly, youths demonstrating marked anxiety symptoms exhibited longer mean initial thinking time on two (β = .276, p = .011), 3 (β = .253, p = .020) and four move problems (β = .301, p = .005) compared with youths with no anxiety symptoms. In addition, youths with marked symptoms demonstrated shorter subsequent think time on two move problems compared with youths with minimal anxiety (β = −.274, p = .011; after controlling for attention). Although nonsignificant, results also indicated a trend such that youths with minimal anxiety symptoms demonstrated increased mean initial thinking time on four move problems (p = .073) and increased mean subsequent thinking time on two move problems (β = .180, p = .099; after controlling for attention) compared with youths with no anxiety symptoms. Group classification did not predict remaining SOC outcomes. See Table 6 for SOC outcomes.
SSP (Working Memory)
Although results demonstrated no significance in relation to SSP performance, analyses did indicate a trend (β = .203, p = .055; after controlling for age) such that youths demonstrating marked anxiety symptoms exhibited poorer working memory compared with youths with no anxiety symptoms. See Table 7 for SSP outcomes.
Discussion
The current study sought to address previous research limitations through the examination of executive functioning in a transdiagnostic sample of youths demonstrating varying degrees of anxiety symptoms. Anxiety symptoms did predict contrastive performance, or demonstrate a trend, in several domains of executive functioning, including cognitive flexibility, planning, working memory, and inhibition. What follows is a brief discussion of these findings and implications for the broader understanding of anxiety and future research.
Somewhat consistent with proposed hypotheses, youth report of anxiety predicted IDED performance (i.e., set shifting); however, contrary to hypotheses youths demonstrating marked anxiety symptoms indicated better cognitive flexibility compared with youths with minimal anxiety symptoms though the overall model demonstrated only a weak trend toward significance. Notably, however, differences were not indicated in comparison with youths with no anxiety symptoms and group classification did not predict reversal learning. These findings may suggest variability in set shifting among anxious youths, yet undistinguishable levels of set shifting compared with those with no anxiety symptoms (i.e., no critical distinguishing impairment). Given limitations (e.g., insignificance of overall model) of the current findings, however, additional replication research is warranted. Notably, collective findings are in contrast to prior research demonstrating lower cognitive flexibility among anxious youths compared with controls (Toren et al., 2000). Such discrepant findings may be attributable to differences in sample characteristics (e.g., current use of a transdiagnostic dimensional cluster rather than comparison of clinical or specific anxiety disorders with a healthy control sample), suggesting that cognitive inflexibility may be more relevant to a clinical anxiety sample. It is also plausible that disparities may be attributable to the emotional content of measures provided. Prior research using emotional (e.g., threatening) and nonemotional stimuli with anxious youths demonstrate intact cognitive flexibility to nonemotional stimuli, yet cognitive inflexibility to emotional stimuli (Mocan, Stanciu, & Visu-Petra, 2014; Tincas et al., 2007). For example, Mogg, Philippot, and Bradley (2004) compared attentional response with facial expressions (i.e., angry, happy, and neutral faces) in a sample of 15 individuals with social phobia and 15 matched controls. Compared with controls, results indicated that after 500 ms of exposure to the faces, individuals with social phobia demonstrated increased attention to angry faces relative to happy and neutral faces. The authors concluded that these findings supported initial vigilance for threatening stimuli among individuals with social anxiety. Additional research using tasks of varied emotion demonstrate similar results (Dresler, Mériau, Heekeren, & van der Meer, 2009; Richards et al., 2007; J. M. G. Williams, Mathews, & MacLeod, 1996). Findings such as these, and those demonstrated herein, may provide additional support to hypotheses suggesting that cognitive inflexibility is more confined to the context of emotional tasks (e.g., threatening faces, emotional Stroop Task, etc.) rather than nonemotional/neutral tasks (e.g., CANTAB tasks). Considering the conjectural nature of these hypotheses and paucity of research within this domain, particularly with youths, additional study of cognitive flexibility is necessary (perhaps further comparing performance on emotional and nonemotional tasks) among transdiagnostic samples of anxious youths.
With respect to SOC performance, youths indicating minimal and marked anxiety symptoms demonstrated longer think times (i.e., increased planning) on presented problems compared with youths indicating no anxiety symptoms. Interestingly however, despite increased planning time, presence of anxiety symptoms failed to predict overall planning accuracy (i.e., problems solved in minimum moves). Results suggest that deficits in planning and organization may be uncharacteristic of the transdiagnostic anxiety cluster. However, despite lack of effect on planning accuracy, one must still recognize the potential implications of increased planning indicated herein. Specifically, current results suggest that anxious youths spend additional time planning with little actual effect (neither positive or negative) on the final outcome. Although inconsequential to overall accuracy, increased planning (with no added benefit) may contribute to lowered efficiency in relation to usage of one’s time (either from spending longer time than necessary planning or needing longer time to come to the same conclusions) and may contribute to impairment outside of the planning and organization domain (e.g., limited time to devote to different activities due to increased time planning/thinking about one area). Such conjecture coincides with theory (e.g., processing efficiency theory, attentional control theory) and previous work using anxious samples in which results suggest that maladaptive worry impairs individuals’ task efficiency more than task accuracy (Derakshan, Ansari, Hansard, Shoker, & Eysenck, 2009; Elliman, Green, Rogers, & Finch, 1997; Eysenck & Calvo, 1992). In brief, such research and theory hypothesize that anxious individuals exert increased task effort to maintain effective performance. Given the lack of prior research assessing planning and organization in anxious youths, such findings warrant additional replication.
Although nonsignificant, SSP results indicated a trend such that youths with marked anxiety symptoms demonstrated poorer working memory compared with youths with no anxiety symptoms. Findings are somewhat consistent with previous research demonstrating lower working memory in anxious youths (Visu-Petra et al., 2014). Given trends herein, working memory deficits may represent a pathogenic marker specific to severe rather than mild anxiety. As such, lack of significant findings with relation to SSP performance may be attributable to the relatively small sample size—particularly with regard to the marked anxiety group. Given such hypotheses, future study in this domain may wish to examine working memory within a larger sample, perhaps comparing youths of increased severity (e.g., comparing clinical vs. nonclinical transdiagnostic samples). Nonetheless, considering proximity to significance (p = .055), current findings may further support working memory deficits as a facet underlying anxiety etiology and/or maintenance and may warrant further consideration in the development of transdiagnostic anxiety intervention (e.g., use of strategies within treatment aimed at increasing working memory capacity).
Finally, in relation to SST performance, youths indicating marked and minimal anxiety symptoms demonstrated greater inhibition. Specifically, youths indicating marked anxiety symptoms demonstrated significantly higher probability of inhibition compared with youths indicating minimal or no anxiety symptoms. This finding contradicts a small body of literature demonstrating poorer inhibition among anxious youths (Ursache & Raver, 2014), yet may complement existing research assessing attention deficit hyperactivity disorder (ADHD) and anxiety comorbidity in which researchers hypothesize that anxiety may, in part, contribute to decreased impulsivity and poorer working memory (Jarrett & Ollendick, 2008). Furthermore, findings herein may also complement previous research demonstrating no inhibition deficits among anxious samples (Günther et al., 2004). While this may suggest that inhibition deficits are uncharacteristic of transdiagnostic anxiety, it is worth noting that the majority of literature indicating impaired inhibition among anxious youths has done so within the presence of emotionally distracting stimuli (e.g., angry faces, angry related words, etc.; Ladouceur et al., 2006; Richards et al., 2007). Similar to IDED performance, this may suggest that inhibition deficits are more specific to emotionally salient stimuli rather than neutral stimuli. Taken together, this may indicate that among anxious youths, inhibition is decreased in the context of emotional distraction, yet increased in the context of neutral stimuli. Interestingly, SST performance within the current sample complements the findings found herein in reference to SOC performance. Specifically, youths with marked anxiety appear to demonstrate increased ability to inhibit prepotent responses, which may in turn contribute to increased time for planning. Such complementary performance perhaps further reflects the overlapping nature of executive functioning components.
Although findings of the present study contribute critical information to a paucity in literature, there are several limitations to consider. First, although findings generate several hypotheses regarding mechanisms underlying anxiety pathogenesis, the cross-sectional design of the current study hinders confirmation of such hypotheses. Future research may wish to consider use of longitudinal designs that may further elucidate the directionality of the relationships found herein. Second, though this study utilized a well-validated and comprehensive measure of executive functioning (i.e., CANTAB), tasks within the current study did not vary based on emotional content. Given finding from some prior research (i.e., impaired performance on some tasks potentially limited to emotional contexts), future research examining executive functioning among anxious youths may benefit from the modification of such tasks to include emotionally relevant stimuli, thus allowing for comparison in child performance across disparate tasks assessing the same broad construct (i.e., cognitive flexibility, inhibitory control). Third, though the current study provides a transdiagnostic sample of anxiety symptoms, the majority of youths within the sample were Caucasian females. Considering this potential limitation to the generalizability of this study’s findings, future studies should attempt to increase the heterogeneity (i.e., in ethnicity, gender, socioeconomic status, etc.) of the samples utilized to answer related questions. Fourth, related to sample makeup, the current study utilized a sample spanning a large age range. Although child age was controlled for when appropriate, it is plausible that findings may be differentially affected based on developmental differences. For example, given the natural development of executive functioning, differences between anxious and control participants may be more apparent in adolescence versus early childhood. Future research should consider examining the impact of transdiagnostic symptoms on executive functioning by age group (e.g., using longitudinal studies or larger groups of participants in specific age groups for cross-sectional comparisons). Finally, though the current sample was deemed sufficient for detecting medium effect sizes, it is plausible that findings of a smaller magnitude were not detected. Given the large range of effect sizes indicated in previous research (i.e., small to large), future studies may wish to consider larger sample sizes to identify potentially smaller meaningful effects.
In summation, youths indicating anxiety symptoms demonstrated increased cognitive flexibility (i.e., set shifting), planning and inhibition, and poorer working memory—with several of these relationships limited to marked anxiety symptoms. Such findings provide critical information for the understanding of anxiety pathogenesis—particularly from a transdiagnostic perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.