
Abstract
The purpose of this study was to examine acceptance and commitment therapy (ACT) as a standalone treatment for trichotillomania in a randomized controlled trial of adults and adolescents. Participants consisted of a community sample of treatment seeking adults and adolescents with trichotillomania. Of the eligible 39 participants randomized into treatment and waitlist groups, 25 completed treatment and were included in the final analysis. Treatment consisted of a 10-session ACT protocol. Multiple mixed models repeated measures analyses were utilized to evaluate changes in trichotillomania symptom severity, daily number of hairs pulled and urges experienced, and experiential avoidance from pretreatment to posttreatment. Findings indicated significant changes in symptom severity and daily hairs pulled, but not daily urges experienced or psychological flexibility. However, psychological flexibility saw a 24.5% decrease in the treatment group and reduced from clinical to subclinical levels on average. This study suggests that ACT alone is an effective treatment for adults and adolescents with trichotillomania. Outcomes appear to be similar to trials that combined ACT and habit reversal training (HRT).
Trichotillomania (Hair Pulling Disorder) is characterized by repetitively pulling out hair that interferes with functioning. Hair can be pulled from various parts of the body, with the most common locations being the head, eyebrows, eyelashes, stomach/back, facial hair, arms, legs, and pubic area (Duke, Keeley, Geffken, & Storch, 2010). Hair pulling is often preceded by urges—physical sensations, cognition, and/or emotions that increase in intensity and motivate hair pulling. The urges to pull are often reduced or removed when hairs are pulled (American Psychiatric Association [APA], 2013).
Pulling has been conceptualized into two styles: automatic and focused (Flessner, Woods, Franklin, Cashin, & Keuthen, 2008). These pulling style categories have recently been updated and reconceptualized as awareness of pulling and internal-regulated pulling (Alexander et al., 2016). The terms automatic and focused are used in the current study as they are more well established and are here conceptualized in a manner consistent with the newer terms. Automatic pulling refers to hair pulling that is done without conscious effort. The puller does not realize pulling has occurred or only realizes it after it has happened. Automatic pulling often occurs during stationary tasks such as while reading, watching television, or driving. Conversely, focused pulling refers to hair pulling that is done with awareness and with the intention to reduce or remove an urge or unwanted internal experience (du Toit, van Kradenburg, Niehaus, & Stein, 2001). Focused pulling can be carried out using tools such as tweezers and mirrors. Pleasurable sensations and emotions can arise after the hair has been pulled as well (du Toit et al., 2001). Usually, both types of pulling occur to varying degrees across individuals with trichotillomania. It has been posited that automatic and focused pulling derive from two separate processes and might warrant different treatment strategies (Woods, Wetterneck, & Flessner, 2006). Traditionally, trichotillomania treatment has placed greater emphases on the automatic aspects of the disorder over the more deliberate and focused pulling behavior.
Habit Reversal Training (HRT; Azrin & Nunn, 1973) has been the leading nonpharmacological treatment for trichotillomania for multiple decades (Bate, Malouff, Thorsteinsson, & Bhullar, 2011). For example, a randomized controlled trial that included 34 participants demonstrated very good outcomes using HRT (Azrin, Nunn, & Frantz, 1980). At a 4-week follow-up 74% of the participants reported no hair pulling. HRT is well-designed to address automatic habits because of its strong awareness, blocking, and reinforcement components. However, HRT does not account for emotional and cognitive difficulties that usually occur within trichotillomania and are a major component of focused pulling (Flessner, Penzel, & Keuthen, 2010; Franklin, Zagrabbe, & Benavides, 2011; Lootens & Nelson-Gray, 2016). Furthermore, following through with a behavioral response (in automatic or focused pulling) is challenging when faced with intense bodily sensations and thoughts about needing to pull. In an attempt to increase compliance with HRT techniques and to address the thoughts, emotions, and urges that accompany focused pulling, additional treatments have been utilized in conjunction with HRT, such as acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 2011) and Dialectical Behavior Therapy (DBT; Linehan, 1993).
Trials combining DBT with HRT have demonstrated reduction in trichotillomania severity with adults and adolescents (Keuthen et al., 2011; Keuthen et al., 2012; Keuthen, Rothbaum et al., 2012; Welch & Kim, 2012). For example, Keuthen et al. (2012) reported a statistically significant 42.7% decrease in hair pulling severity scores in treatment completers at posttreatment. Another trial demonstrated a statistically significant 48.6% decrease in hair pulling severity in nine treatment completers at a 6-month follow-up (Keuthen et al., 2011). In addition, trials combining ACT with HRT have shown promising results, reducing trichotillomania severity with adults and adolescents (Crosby, Dehlin, Mitchell, & Twohig, 2012; Fine et al., 2012; Twohig & Woods, 2004; Woods et al., 2006). Specifically, ACT has been integrated with more traditional HRT procedures in a number of studies.
There is mounting evidence that ACT enhanced HRT (ACT/HRT) is able to effectively target automatic and focused pulling. The initial pilot study of ACT/HRT included six participants with trichotillomania and employed a multiple baseline across participants design (Twohig & Woods, 2004). Four of these participants reduced their hair pulling behavior significantly, and three maintained significant improvement at a 3-month follow-up. Additional studies have since replicated these findings. Crosby et al. (2012) reported significant reductions in hair pulling severity in four of five participants that were largely maintained at a 3-month follow-up. Flessner, Busch, Heideman, and Woods (2008) reported significant improvements across five participants and found that the order of receiving ACT or HRT treatment components did not affect outcomes. Woods et al. (2006) examined ACT/HRT in a larger sample of 25 participants and found significant, large improvements in trichotillomania compared to a waitlist control condition (η2 = .50) that were maintained at a 3-month follow-up. Finally, Fine et al. (2012) treated two adolescents and reported clinically significant trichotillomania severity outcomes. While there is limited support for the use of these combined treatments, no trial has examined a form of cognitive behavior therapy that specifically target emotion regulation processes (e.g., ACT, DBT) as a standalone treatment for trichotillomania. This reduces the ability to determine any potential additional benefits of these treatments beyond HRT alone.
Theoretically, ACT aims to increase psychological flexibility, which can be defined as the ability to engage in meaningful, values-directed behavior without any particular regard for inner experiences (i.e., thoughts, emotions, sensations). Psychological flexibility has been shown to be associated with lower levels of hair pulling severity, less frequent and intense urges to pull, and lower levels of distress related to pulling (Begotka, Woods, & Wetterneck, 2004; Bluett, Homan, Morrison, Levin, & Twohig, 2014; Twohig, Morrison, & Bluett, 2014). For example, in the treatment of trichotillomania, an ACT therapist would demonstrate the futility of attempting to change or control the client’s urge to pull, instead focusing on increasing the client’s willingness to experience the urge to pull as it is. This would allow the client to better experience urges as simply bodily sensations and internal thoughts that do not need to be removed before engaging in meaningful life actions.
While the role of psychological flexibility and the utility of ACT/HRT in the treatment of trichotillomania are promising, little is understood about what components of treatment are influencing the various attributes of trichotillomania. Specifically, it is difficult to tell what ACT alone is contributing to treatment. At this time, ACT alone has only been examined for problems similar to trichotillomania. The first was a multiple baseline across participants design that employed ACT with five participants with chronic skin-picking (Twohig, Hayes, & Masuda, 2006). Of the five participants, four reached near-zero levels of skin-picking at post-treatment, but only one maintained this progress at follow-up. ACT has been evaluated as a treatment for problematic Internet pornography viewing in two studies (Crosby & Twohig, 2016; Twohig & Crosby, 2010); which has been classified as a compulsive sexual behavior within the obsessive-compulsive spectrum by some (Kraus, Potenza, Martino, & Grant, 2015; Kraus, Voon, Kor, & Potenza, 2016; Potenza, 2017), but certainly not all. The multiple baseline study found an 85% reduction in viewing, and the RCT showed a 93% reduction for ACT versus a 21% reduction in the waitlist. Two of the three studies showed significant increases in psychological flexibility, providing further evidence of a potential mechanism of change within obsessive-compulsive spectrum disorders like trichotillomania. Until now, however, ACT alone has not been examined as a treatment for trichotillomania leaving many questions about the role ACT plays in the treatment of trichotillomania.
The purpose of the current study is to examine ACT alone as a treatment for trichotillomania in a randomized controlled trial of adults and adolescents. We chose to allow adolescents and adults into the study because the research question (“does ACT work without HRT?”) can be answered across age groups, and recruitment of participants with a diagnosis of trichotillomania is difficult. Moreover, the study will examine the role of psychological flexibility in treatment outcomes. We predict that ACT alone as a treatment for trichotillomania would demonstrate significant reductions in hair pulling symptoms and psychological inflexibility compared to a waitlist control condition. We hope to gain a better understanding the contributions that ACT provides to the treatment of trichotillomania.
Method
Participants
No formal recruitment for participants was performed for this study. All participants were treatment seeking individuals who agreed to participate in a research study as part of their treatment by a university research team. The research clinic receives referrals from community treatment providers and a listing on the TLC Foundation’s “Find a Therapist” webpage (bfrb.org). Totally, 39 participants met eligibility criteria for the current study. To be included in this study, participants were required to (a) meet Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) criteria for trichotillomania, (b) be seeking treatment primarily for concerns related to trichotillomania, (c) be at least 12 years old, (d) not be currently receiving psychotherapy, (e) not have started or changed psychotropic medication in the past 30 days, and (f) not be planning to start or change psychotropic medication during the course of the study. The eligible 39 participants were randomized into treatment (n = 22) and waitlist (n = 17) groups. Of these, 14 did not complete the posttreatment or postwaitlist (Time 2) assessment. Regarding the noncompleters, two completed treatment, but did not complete the posttreatment assessment, five dropped out before completing treatment (one following intake but after randomization, and following sessions 2, 3, 4, and 8), and seven did not complete the postwaitlist assessment (see Figure 1 for a participant flowchart). Thus, the actual dropout rate for the treatment condition was 22%. This rate is consistent with other similar trials. For example, an open trial of CBT for children and adolescents with trichotillomania had a dropout rate of 36% (Tolin, Franklin, Diefenbach, Anderson, & Meunier, 2007). Another CBT trial that included children, adolescents, and adults reported a dropout rate of 22% (Lerner, Franklin, Meadows, Hembree, & Foa, 1998). Demographic information for participants is displayed on Table 1.
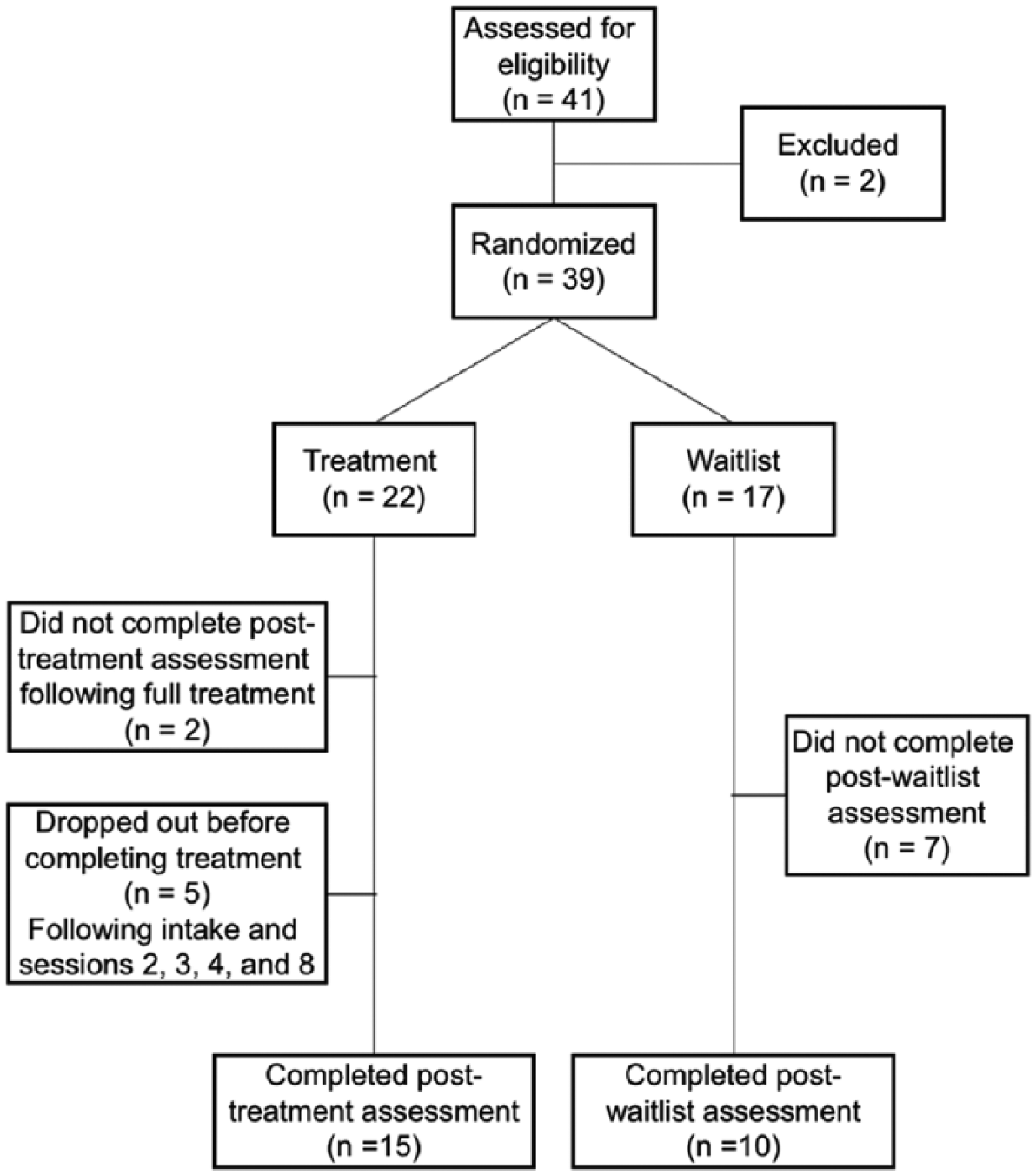
Participant flowchart.
Pretreatment Sample Characteristics.
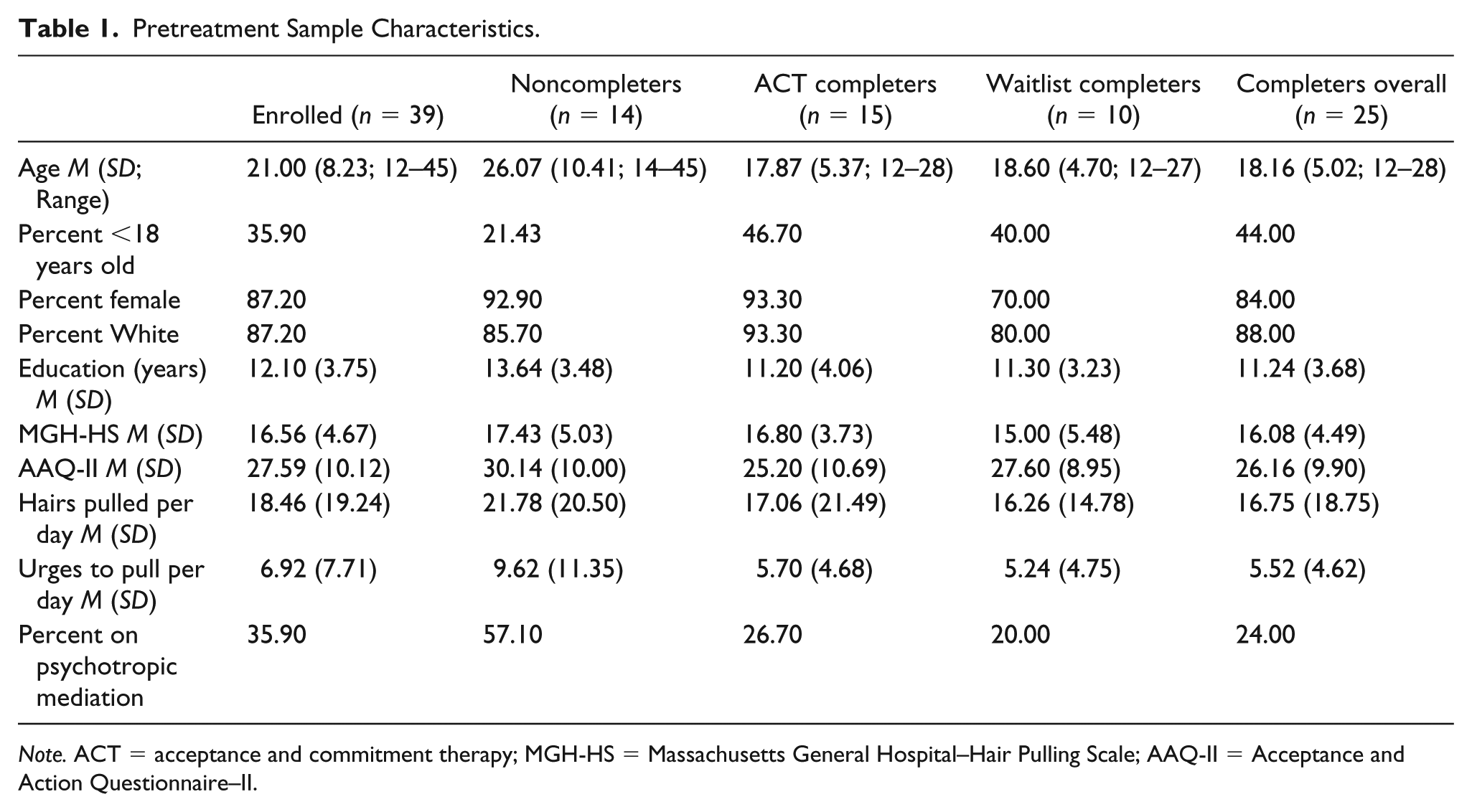
Note. ACT = acceptance and commitment therapy; MGH-HS = Massachusetts General Hospital–Hair Pulling Scale; AAQ-II = Acceptance and Action Questionnaire–II.
Procedure
The current study was approved by a university institutional review board. Eligible participants completed an intake session (Time 1), which consisted of gathering consent/assent and basic information about their hair pulling and completing a baseline assessment battery. Following the intake session, participants were randomized into either the treatment or waitlist control group based on odd or even numbers generated from a random number generator. This randomization method, led to uneven groups. Participants in the treatment group began therapy the following week, attended ten 50-min sessions of therapy and then completed a posttreatment assessment (Time 2). Participants in the waitlist control group waited 10 weeks, completed a postwaitlist assessment (Time 2) and then completed the same course of treatment as the treatment group.
ACT
The ACT intervention was conducted by master and doctoral level therapists who had been trained in ACT. The last author provided regular supervision and treatment integrity checks throughout the study. Treatment consisted of a 10-session ACT protocol developed by the last author. The following is a general outline of the protocol; however, because of the flexible nature of ACT and the tendency for participants to struggle with different ACT processes, session order and length of time spent on each topic varied slightly for each participant. Specifically, as determined by the therapist for each participant, some modifications were made for younger participants that included parental support and involvement and exercises and metaphors that were more developmentally appropriate. Similar exercises were used, but described more concretely and less metaphorically. When available, parents were encouraged to be involved in treatment. Parents would be invited to participate in approximately 10 min at the end of sessions. Here, participants would review what they had learned in the session and clarify goals with parents in an attempt to help parents to be able to better support their child between sessions. Overall, modifications to treatment were relatively minor and the treatment protocol was followed regardless of participant age. Similar modifications have been successfully demonstrated in an OCD trial for adolescents (Armstrong, Morrison, & Twohig, 2013). Sessions 1 and 2 included general assessment of trichotillomania symptoms and behaviors and an ACT technique known as creative hopelessness. Sessions 3, 4, and 5 introduced the problem of attempting to control thoughts, emotions, and urges and discussion of willingness or acceptance as an alternative to control. Sessions 6 and 7 introduced the ACT processes self as context and defusion. Session 8, 9, and 10 introduced values and values-directed behavior. Table 2 describes the session-by-session components and exercises used.
ACT for Trichotillomania: Abbreviated Treatment Manual.

Note. All exercise available in Hayes, Strosahl, and Wilson (1999). ACT = acceptance and commitment therapy; APA = American Psychology Association.
Measures
MGH-HS
The MGH-HS is a 7-item self-report measure of hair pulling severity. It includes questions related to urges to pull hair, pulling behavior, and consequences of pulling. Items are rated from 0 to 4 and are then summed into a 0 to 28-point total score, with higher scores reflecting greater hair pulling severity (MGH-HS; Keuthen et al., 1995). Changes of seven points or more are considered to be indicative of clinically significant treatment response and disorder remission (Houghton et al., 2015). The MGH-HS has demonstrated good internal consistency, test–retest reliability, and convergent and divergent validity (Keuthen et al., 2007). The MGH-HS was chosen to use a single scale for comparisons between adolescents and adults. While the measure’s psychometric properties are not well understood for adolescents, it has been successfully utilized in multiple child and adolescent studies (e.g., Bloch, Panza, Grant, Pittenger, & Leckman, 2013; Rahman, McGuire, Storch, & Lewin, 2017). The MGH-HS displayed good internal reliability in the current study (αs = .85).
Acceptance and Action Questionnaire-II (AAQ-II)
The AAQ-II is a 7-item self-report measure of psychological inflexibility or experiential avoidance (Bond et al., 2011). Items are rated on a 7-point Likert-type scale (1 = never true to 7 = always true). Items are summed into a 7- to 49-point total score, with higher scores reflecting greater levels of psychological flexibility. The AAQ-II has demonstrated satisfactory reliability and validity (Bond et al., 2011). The AAQ-II displayed good internal reliability in the current study (αs = .91).
Daily tracking form
Following each session, participants were given a form to record their daily behavior and experiences with trichotillomania symptoms each day between sessions. The form assessed the number of urges to pull experienced and number of hairs pulled daily. This simple form has not been validated and relies on the self-report of participants, and has been used in many studies. The weekly totals from the week prior to the intake session and the postassessment were averaged and used for Times 1 and 2.
Treatment Integrity
All sessions were video recorded, and 15% were scored for treatment integrity by the first and fourth author. Of note, the first author also treated participants, but did not score any of his own treatment sessions. Sessions for review were selected using a systematically random method that ensured that at least two sessions were reviewed for each participant and that each session number was reviewed approximately the same amount across participants. The sessions were scored for the quantity and quality of the overage of each ACT component using a system shown to be reliable and valid in previous research (Twohig & Crosby, 2010). For every session, each ACT process (i.e., acceptance, defusion, contact with the present moment, self as context, values, and committed action) was rated on a 5-point scale (1 = the variable was never explicitly covered to 5 = the variable occurred with high frequency and was covered in a very in-depth manner). The means for each process over the 10 sessions are as follows: acceptance M = 3.45 (SD = 1.22), defusion M = 2.47 (SD = 1.35), contact with the present moment M = 1.66 (SD = 0.99), self as context M = 1.47 (SD = 1.08), values M = 1.92 (SD = 1.24), committed action M = 2.55 (SD = 0.72). Each process was rated as a “5” for at least one session for all participants, indicating that all processes were thoroughly covered. Therapist adherence to the ACT model and therapist competency were also rated very highly on a 5-point scale, M = 4.42 (SD = 0.60) and M = 4.42 (SD = 0.68), respectively. Finally, therapeutic practices that were inconsistent with ACT were scored on a 5-point scale. These included cognitive challenging, offering experiential avoidant change strategies, and indicating that thoughts and feelings cause overt behavior. Each of these received a score of “1” indicating that they were not present in the sessions.
Data Analysis
Multiple mixed models repeated measures (MMRM) analyses were used to evaluate changes in MGH-HS and AAQ-II scores as well as self-reported number of hairs pulled and urges experienced from pretreatment to posttreatment between groups. This method utilizes all available data while allowing for the analysis of the full intent-to-treat sample. Thus, missing data are accounted for in a way that is less biased than methods such as listwise deletion or last observation carried forward (Salim, Mackinnon, Christensen, & Griffiths, 2008). Results were consistent with a completer analysis using ANOVAs, with the exception of the AAQ-II which moved from near significant to significant. In addition, results are similar with age entered as a covariate with regard to statistical significance and effect size.
Statistical assumptions were examined before analyzing the data. All data were normally distributed, as assessed by Shapiro–Wilk test (p >.05.) and Normal Q-Q Plots, except for number of urges experienced (ps < .01). In addition, no outliers were found, as assessed by examination of studentized residuals for values greater than ±3. There was homogeneity of variances between the treatment and waitlist groups at Time 1, as assessed by Levene’s test of homogeneity of variance (p > .05). However, there was heterogeneity of variance between the groups for MGH-HS scores and number of daily hairs pulled at Time 2 (p = .037 and p < .001, respectively). Because of the nonnormal urges data and the heterogeneous variance in the MGH-HS and hairs pulled data, these variables were transformed using a reflect and logarithmic transformation for the negatively skewed MGH-HS scores and a logarithmic transformation for the positively skewed urges experienced and hairs pulled data. Following, the transformations the variables met all required assumptions. Finally, homogeneity of covariance was found for MGH-HS and AAQ-II scores and self-reported number of hairs pulled and urges experienced, as assessed by Box’s test of equality of covariance matrices (ps = .782, .485, .197, and .765, respectively).
Independent sample t tests were performed using all available demographic and outcome variables between participants in the treatment and control conditions at intake to assess for proper randomization. Of the 13 variables examined, no statistically significant differences were demonstrated between the conditions for any variable (ps > .05). To assess for potential attrition bias, additional independent samples t tests were performed between treatment completers and noncompleters using the same demographic and outcome variables. Only age (p =.003) and years of education (p = .035) were significantly different between the groups. This indicates that older participants were more likely to dropout. Sample characteristics for participant groups are displayed in Table 1.
Results
Means and standard deviations for adolescents and adults for all outcome measures at Times 1 and 2 are displayed in Table 3.
Means and Standard Deviations for Adolescents and Adults on Outcome Measures at Time 1 and Time 2.
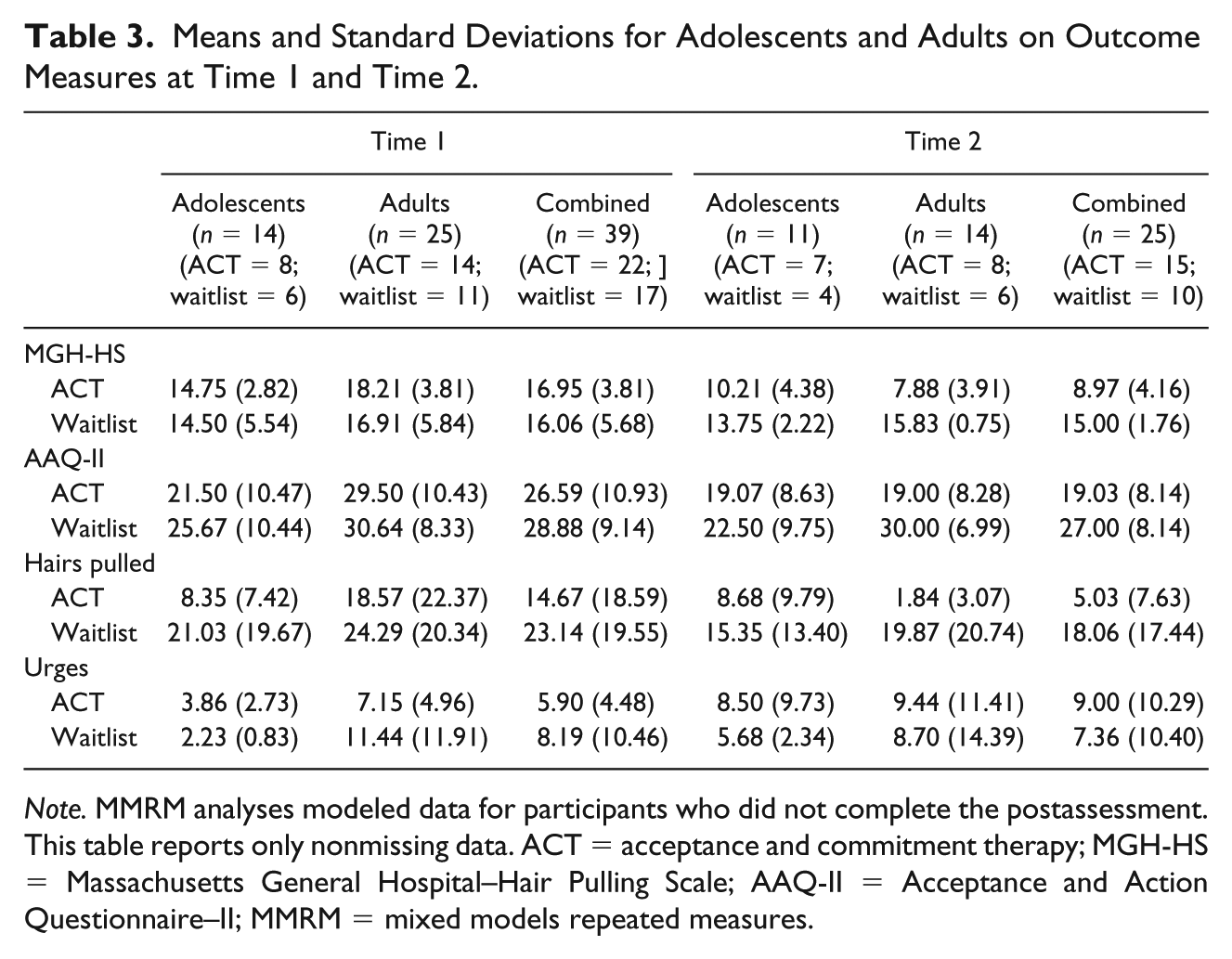
Note. MMRM analyses modeled data for participants who did not complete the postassessment. This table reports only nonmissing data. ACT = acceptance and commitment therapy; MGH-HS = Massachusetts General Hospital–Hair Pulling Scale; AAQ-II = Acceptance and Action Questionnaire–II; MMRM = mixed models repeated measures.
Effects on Hair Pulling Severity
MMRM analysis indicated a significant time × group interaction for MGH-HS scores, F(1, 30.73) = 12.59, p = .001, Cohen’s d = 1.28. Between-group comparisons indicated no significant difference between groups at Time 1, t(37.00) = −59, p = .560, d = .19, however, a significant difference was found at Time 2 t(23.11) = −4.37, p < .001, d = 1.78. A within-group comparison indicated a significant difference for the treatment group from pretreatment to posttreatment t(17.22) = -5.83, p < .001, d = .1.38. Moreover, the treatment group saw a 46.6% decrease in MGH-HS scores, while the waitlist group saw no change in scores from Time 1 to Time 2. Nine of the 15 (60%) treatment completers saw MGH-HS score reductions of seven points or greater, indicating clinically significant improvement. These findings indicate that on average, treatment had a significant, large effect on hair pulling severity.
Effects on Self-Reported Daily Hairs Pulled
The self-reported daily hairs pulled time × group interaction was nonsignficant, F(1, 32.79) = .45, p = .508, Cohen’s d = .23. In addition, there was no significant main effect for time, F(1, 32.79) = 3.52, p = .070, d = .66, but a significant main effect for group, F(1, 33.62) = 7.06, p = .012, d = .92. The treatment group saw a 77.4% decrease in self-reported daily hairs pulled, while the waitlist group saw a 10.0% increase from Times 1 to 2.
Effects of Self-Reported Daily Urges Experienced
Self-reported daily urges experience demonstrated a nonsignificant time × group interaction, F(1, 22.00) = .06, p = .803, Cohen’s d = .11. In addition, there was no significant main effect for time, F(1, 22.00) = 2.10, p = .162, d = .62, or group, F(1, 19.81) = .32, p = .576, d = .26. These findings indicate that participants in both the treatment and waitlist groups saw no significant changes in the number of daily urges to pull. In addition, treatment did not have a significant impact on the number of urges experienced.
Effects on Psychological Flexibility
AAQ-II scores demonstrated a nonsignificant time × group interaction, F(1, 28.16) = 2.57, p = .120, Cohen’s d = .60. In addition, there was a significant main effect for time, F(1, 28.16) = 5.63, p = .025, d = .89, but no significant main effect for group, F(1, 34.769) = 3.438, p = .072, d = .26. The treatment group saw a 24.5% decrease in AAQ-II scores, while the waitlist group saw only a 2.2% decrease from Times 1 to 2.
Session-by-Session Self-Reported Data
The daily tracking forms for each session were used to track the number of self-reported hairs pulled and urges experienced between each of the 10 sessions including all participants. These data were collected for clinical purposes throughout the study and were examined following the completion of the trial in an exploratory manner as they were potentially clinically useful. Totals were averaged for each session and are displayed in Figure 2. Visual inspection reveals that the number of hairs pulled generally reduces over the course of treatment while urges increase at sessions one and three and then remain relatively stable. Of note, the number of reported urges experienced at pretreatment was lower than any time throughout the course of treatment. This is likely due to the difficulty that many participants have in identifying urges and the lack of awareness of urges before beginning treatment. The spike in urges at sessions one and three might be, in part, explained by the awareness training and psychoeducation that occurs in early sessions.

Self-reported daily number of hairs pulled and urges experienced throughout treatment.
Differences in Adolescents and Adults
Although the study’s sample size precluded formal statistical analysis of the differences between adults and adolescents, the descriptive data are worth cautious consideration. Descriptive statistics broken down by age group and treatment group are displayed in Table 3. The full sample of 39 participants consisted of 14 adolescents (35.9%) that were evenly distributed between the treatment and waitlist conditions by percent (36.4% and 35.3%, respectively). Overall, adults appeared to be more responsive to treatment than adolescents. On average, MGH-HS scores were reduced by 56.7% in adults and 30.8% in adolescents. Moreover, seven of the eight adults who completed treatment saw a clinically significant reduction (seven points or more) in MGH-HS scores, while only two of the seven adolescents did. Furthermore, the adults saw meaningful reductions in the number of hairs pulled (90.1% on average), while adolescents saw a small increase in the number of hairs pulled (3.8% on average). This pattern continued for psychological flexibility. On average, adults saw a 35.6% improvement on AAQ-II scores, while adolescents saw an 11.3% improvement. These findings indicate that while overall, the treatment produced significant improvements, the majority of these improvements were made by the adult participants.
Discussion
ACT has been used as a treatment component in many successful trichotillomania trials (e.g., Crosby et al., 2012; Fine et al., 2012). However, until now, ACT has not been examined as an independent treatment, thus making it difficult to understand what it might contribute to the treatment of trichotillomania. The current study was an attempt to examine ACT alone as a treatment for trichotillomania in a trial that included adults and adolescents. In addition, the role of psychological flexibility in treatment outcomes was examined. The results indicate that some, but not all, adults and adolescents respond to ACT alone as a treatment for trichotillomania with adolescents demonstrating overall less improvement than adults. The measured outcomes appear to be similar to trials that combined ACT and HRT with hair pulling severity and the number of daily hairs pulled seeing significant reductions from pretreatment to posttreatment. For example, the largest randomized trial of ACT/HRT for trichotillomania to date demonstrated a 45% reduction in hair pulling severity (MGH-HS) scores from pretreatment to posttreatment, compared to 47% in the current study (Woods et al., 2006). Moreover, the self-reported number of hairs pulled fell 58% in the ACT/HRT trial compared to 77% in the current study.
As a field, we need to continue to investigate the processes of change that these interventions work through. For example, surface level comparisons of ACT and HRT might indicate process similarities, but only empirical work will really answer this question. Contacting the present moment in ACT emphasizes awareness and openness to experiences and often includes describing thoughts, urges, and sensations without attempts to change or control them while engaging in valued behavior. This process is similar to awareness training found in HRT that attempts to bring greater attention to urges to reduce automatic pulling. In addition, components of HRT, like stimulus control and competing responses functionally reflect the acceptance, values, and committed action processes in ACT that encourage commitments to engage in meaningful behavior while at the same time being willing to experience urges to pull.
ACT alone and ACT/HRT appear to be quality treatments for at least a significant portion of individuals with trichotillomania. It is likely that both share some processes of change and target the major components of trichotillomania. This may also be the case for other treatments, such as DBT, that have produced similar results. Therefore, it may not matter which treatment is used, so long as the automatic and focused elements of the pulling behavior are addressed. However, this small trial is the only examination of ACT alone for trichotillomania and these results should be interpreted with caution. It appears that ACT alone is potentially comparable to ACT/HRT; however, ACT/HRT has substantially more evidence for its efficacy at this time.
On average, psychological flexibility saw a nonsignificant improvement from pretreatment to posttreatment. However, on average, participants demonstrated improvement in psychological flexibility at what is considered clinically significant levels. While these data should be interpreted with caution, we feel that they are worth consideration. The 24.5% decrease in the treatment group reduced mean psychological inflexibility scores from clinical (25.2) to subclinical (19.0) levels over the course of treatment. These findings are in line with previous findings indicating that psychological flexibility may play a role in treatment (Houghton et al., 2014). Further research on this component of treatment is needed. The use of the trichotillomania-specific version of the AAQ (Houghton et al., 2014) would likely be more sensitive to change and should be used in future research to better examine the role of psychological flexibility in trichotillomania.
The findings indicate that the treatment was more effective for adults than adolescents, with adults seeing greater improvement in hair pulling severity and psychological flexibility than adolescents, on average. Although modifications were made to the treatment based on developmental needs, it appears that further modification to the protocol might be needed. Moreover, other treatment components might be needed when treating adolescents with trichotillomania. These components might include a greater emphasis on family involvement, support, and contingency management that might reinforce target behavior beyond the intrinsic reinforcement from treatment and self-improvement, more likely seen in adults. Unfortunately, research related to the role of developmental factors on trichotillomania and its treatment is severely lacking. Although, a recent trial of 12 children and adolescents (ages 7-17) demonstrated significant reductions in trichotillomania severity using HRT (Franklin, Edson, & Freeman, 2010). This provides further evidence that the more basic components of HRT might be more easily understood by children and adolescents than the more abstract components of ACT. Further study is needed to better understand the differential mechanisms of action in adult and adolescent treatment of trichotillomania
The current study has some limitations. The community, self-referred nature of the study led to higher than average dropout and incomplete posttreatment assessments. It does appear that those who dropped out and were not included in the study were similar to those who completed the study with regard to most demographic and all outcome variables; however, older participants were less likely to complete treatment. This provides some assurance that those who dropped out would have performed similarly to those who remained in the study. However, the relatively small sample size makes comparisons between groups difficult and it is impossible to conclude that dropout was entirely random. Also, while the sample size was sufficient for basic analysis between the two treatment groups, it did not allow for statistical analysis of potential differences between adolescents and adults. The descriptive data provide enough information to understand that age was an important differential factor in this study, however, a larger sample is needed to more systematically analyze and more fully understand what role age plays in ACT for trichotillomania. Moreover, while the waitlist control design of the study controls for changes due to the passage of time, it does not control for common therapeutic factors that could play a role in the treatment gains seen in the ACT condition. This study design is useful to answer whether ACT alone can effectively treat trichotillomania, but it does not answer whether this modality is better than other treatments or common factors. Future research in this area should consider comparisons to active treatments. Finally, the lack of follow-up data is a major limitation as it does not allow for the ability to assess for treatment gains over time and the limited process data makes mediational models impossible. This limitation is notable as relapse from treatment gains is a major concern for trichotillomania. Although the results of the current study were quite promising, we unfortunately cannot know if these results had a lasting effect. Further research that more fully examines long-term treatment gains and mechanisms of action are needed.
The findings provide additional evidence for the utility of ACT as a component of trichotillomania treatment, especially in adults. Moreover, the findings indicate that ACT alone is a potentially viable treatment, with or without explicit HRT components. For adults it appears that the specific methods of trichotillomania treatment are less important than the processes they target, so long as the automatic and focused components of hair pulling behavior are properly addressed. For adolescents, the evidence is less clear. Further research is needed to improve treatment and outcomes in youth. While a comparison of ACT, HRT, and ACT/HRT would perhaps clarify potential differences between the treatments, this may not be the most expedient course of action. Rather, it appears that focus should be placed more on specific processes of change and less on the overall treatment package.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.