
Abstract
Participation in social skills therapy (SST) facilitates cognitive functioning in children with developmental disabilities. The present pilot study examined whether participation in SST was associated with enhanced encoding and 1-month delayed recall in children with Down syndrome (DS). Children were presented with novel three-step event sequences in an elicited imitation procedure. Immediate imitation was permitted as an index of encoding; long-term memory was assessed 1 month later. Parents completed questionnaires inquiring about children’s participation in SST. Participation in SST was associated with enhanced encoding of temporal order information and 1-month delayed recall of individual target actions. In addition, encoding mediated the relation between group and 1-month delayed recall. The conducted research indicates that involvement in SST may be beneficial for children with DS despite their noted strengths in imitation and social learning. As such, additional experimental work is warranted to determine causality.
The ability to recall the past is at least in part socially constructed. When considering typically developing (TD) children, the manner in which parents discuss the past with their children has implications for the ways in which children discuss the past themselves. For example, Fivush and Fromhoff (1988) reported that children of mothers who were characterized as elaborative in their narrative style (i.e., those who talked more and asked more memory-related questions when conversing about past events with their children) recalled more detail about past experiences relative to children of mothers who had repetitive narrative styles (i.e., mothers who tended to repeat information). The social environment also contributes to cognitive functioning in children with developmental disabilities. As evidence of this, participation in social skills therapy (SST) has been associated with improved eye contact, joint attention, and imitation, among other abilities, in children with autism spectrum disorders (ASD; Cappadocia & Weiss, 2011; Hwang & Hughes, 2000); causality has also been confirmed in at least one report (Ozonoff & Miller, 1995). Despite these promising results, little research has been conducted to examine whether observed or parent-reported participation in SST is associated with improved cognitive outcomes in children with Down syndrome (DS). The paucity of relevant research may be explained by previous reports indicating that children with DS are relatively skilled at imitation and social interaction (Dykens & Hodapp, 2001; Libby, Powell, Messer, & Jordan, 1997; Rast & Meltzoff, 1995; Roberts & Richmond, 2015; Wright, Lewis, & Collis, 2006), thereby suggesting that such additional intervention in this domain will yield few returns. However, recent findings have demonstrated that children with DS experience impairments in long-term recall memory relative to TD children matched on developmental age (DA; Milojevich & Lukowski, 2016). Given the demonstrated effectiveness of SST for improving cognitive functioning in children with ASD, the present exploratory research was conducted to examine whether parent-reported participation in SST was associated with enhanced encoding and 1-month delayed recall by children with DS.
Understanding how cognitive development proceeds in children with DS is not only important due to the prevalence of this genetic disorder but also because of the long-term cognitive consequences associated with DS. DS is the most common autosomal chromosomal disorder worldwide, affecting approximately 1 in every 700 infants born in the United States (Centers for Disease Control and Prevention, 2014). Although other genotypes exist, DS is most commonly characterized by an extra chromosome on the 21st pair. Children with DS experience numerous functional challenges relative to TD children, including physical impairments, issues with receptive and expressive language, and cognitive deficits (Abbeduto et al., 2001; Laws & Bishop, 2003; Selikowitz, 1997). As such, understanding the effectiveness of early intervention efforts for maximizing functional outcomes early in life and beyond should be a primary goal in the research on children with developmental disabilities.
Part of the challenge in examining associations with cognitive functioning, however, is that infants and young children cannot report on the past using language. For this reason, researchers use a behavioral paradigm known as elicited or deferred imitation to assess the emergence and development of recall capabilities in the first years of life (Lukowski & Milojevich, 2016). In one version of this procedure, children interact with novel three-dimensional stimuli during a pre-demonstration baseline period. A researcher then demonstrates how to complete a sequence of actions with the materials. Children are allowed the opportunity to imitate the actions immediately after the demonstration as an index of encoding and/or after delays ranging from minutes to months as an index of long-term memory. The data are then coded to determine whether the participants perform the demonstrated target actions (TA) and whether the completed actions are reproduced in the correct temporal order (for additional information, see Bauer, DeBoer & Lukowski, 2007). In a modification of the standard procedure just described, generalization across cues are assessed by varying the perceptual features of stimuli presented at demonstration and at test (e.g., Lukowski & Milojevich, 2013; Phung, Milojevich, & Lukowski, 2014).
Although a significant literature has been established on the conditions that best support recall in TD infants and children, few studies have used the elicited imitation paradigm to examine recall memory in children with DS. The research that has been conducted indicates that children with DS successfully imitate demonstrated actions both immediately and after delays ranging from minutes to months (e.g., Milojevich & Lukowski, 2016; Rast & Meltzoff, 1995). In one study, for example, young children with DS imitated single- and multi-step pretend-play actions after watching an adult model (Libby et al., 1997). Other research indicates that children with DS encode TA and temporal order information at levels comparable with TD children; children with DS also recall individual TA after a 1-month delay. Although these findings have been taken to indicate that children with DS experience relative strengths in social interaction and imitation (Dykens & Hodapp, 2001; Libby et al., 1997; Rast & Meltzoff, 1995; Wright et al., 2006), children with DS also experience impairments in long-term memory. That is, whereas TD children recall the temporal order of three-step event sequences after a 1-month delay, children with DS do not (Milojevich & Lukowski, 2016).
One possible means of improving cognitive functioning in children with DS may be through the use of early interventions, particularly those that target the development of social skills. As a result of the Individuals with Disabilities Education Act (IDEA; 20 U.S.C. § 1400 et seq), a variety of federally mandated educational and intervention services are available to children with DS, with the overarching goal of enhancing functional outcomes across a variety of domains (National Down Syndrome Society, 2012). Although there is no research to our knowledge to indicate whether participation in SST is associated with enhanced cognition in children with DS, other forms of early intervention promote cognitive functioning (Connolly, Morgan, Russell, & Richardson, 1980; Connolly, Morgan, Russell, & Fulliton, 1993; Feeley, Jones, Blackburn, & Bauer, 2011). For example, longitudinal studies have demonstrated that children who participate in early intervention programs score significantly higher on tests of intelligence and general cognitive functioning relative to age-matched children with DS who have not received early intervention (Connolly et al., 1980). Importantly, these early intervention benefits are seen both immediately and over time, extending into adolescence (Connolly et al., 1993). Furthermore, research on children with other developmental delays has repeatedly demonstrated that SST is associated with (Cappadocia & Weiss, 2011; Hwang & Hughes, 2000)—and even directly enhances (Ozonoff & Miller, 1995)—cognitive functioning. In particular, Hwang and Hughes (2000) reviewed 16 empirical studies that examined the impact of SST on young children with ASD. Based on their review of the literature, they concluded that involvement in SST improves eye contact, joint attention, and imitation, among other cognitive and social skills, in children with ASD. Whether children with DS would experience any cognitive benefits associated with their involvement in SST is unknown.
The primary goal of the present study was to collect pilot data from a small sample of children with DS to examine whether participation in SST was associated with enhanced encoding and 1-month delayed recall memory and generalization across cues. In exploratory analyses, we examined the associations between participation in SST and cognitive functioning in particular because (a) previous work has documented the importance of the social context in shaping recall memory (e.g., Fivush & Fromhoff, 1988) and (b) SST interventions are not commonly experienced by children with DS. Because children with DS have demonstrated strengths in imitation and social learning (Dykens & Hodapp, 2001; Libby et al., 1997; Rast & Meltzoff, 1995; Roberts & Richmond, 2015; Wright et al., 2006), we predicted that children would show evidence of encoding the demonstrated actions relative to baseline regardless of their intervention history. However, given the social nature of the elicited imitation procedure (Heimann, Laberg, & Nordoen, 2006), we expected that children who had participated in SST would perform more TA and pairs of actions (PA) at immediate imitation relative to children who had not participated in SST. When considering long-term memory, we predicted that participation in SST would also be associated with recall performance, particularly when considering memory for TA relative to temporal order information, as previous research indicates that children with DS do not recall temporal order information after a 1-month delay (Milojevich & Lukowski, 2016). Finally, we used mediation models to examine the process by which participation in SST might impact encoding and 1-month delayed recall memory.
Method
Participants
Nineteen children diagnosed with DS (mean age = 33 months, 9 days; range from 18 months, 12 days to 53 months, 1 day; 11 girls) served as participants. Two additional children were tested but were later excluded from data analysis: One child experienced seizure activity shortly after birth, whereas the other child was not developing as expected based on parent report. These participants were recruited to participate in a study examining recall memory and related abilities in children with DS along with TD children matched to the children with DS on DA. Portions of the data collected in the larger study have been published (Lukowski & Milojevich, 2017; Milojevich & Lukowski, 2016) or are currently under review (Lukowski, Slonecker, & Milojevich, 2019; Milojevich, Slonecker, & Lukowski, 2019), but none of this work addresses the exploratory research questions presented herein.
Participants were recruited from local early intervention centers, organizations that provided educational and support services to children with DS and their families, and through snowball sampling. Interested families provided the researchers with their phone number and email addresses and were contacted with additional information about participating in the study.
Of the 19 participants, 53% were Caucasian, 21% were Asian, 5% were African American, and 16% were of mixed race; the race of 5% of the participants was unknown. Thirty-seven percent of the children were of Hispanic ethnicity. Eighty-four percent of the children were exclusively or primarily exposed to English at home, 5% were exposed to English less than half of the time at home, and 11% did not provide information sufficient to allow for categorization. Seventy-nine percent of mothers had obtained at least a 4-year college degree. Parents received US$30 in appreciation of their participation and children received either a small toy or a “junior scientist” t-shirt.
Materials and Measures
Questionnaires
Parents provided demographic information, including child race and ethnicity, parent education, and family income, among other things. They also completed an early intervention questionnaire (Ly, 2013) that was developed to examine participation in interventions by children with ASD. The questionnaire inquired as to whether the child was participating in various interventions at the time of the study, had previously participated in the listed interventions but was not participating in them at the time of the study, or had never participated in the listed interventions (e.g., occupational therapy, physical therapy, psychotherapy, and speech therapy). Additional space was provided for parents to write in other interventions experienced by the child. For those interventions with which the child had experience, parents also recorded the number of months the intervention was in place.
Bayley Scales of Infant Development-III (BSID-III; Bayley, 2006)
The mental dimension of the BSID-III was administered at the first session to determine each child’s DA.
Elicited imitation
Children were presented with six three-step event sequences across two study sessions; four of these sequences are featured in the present report (two presented at the first and second sessions and two presented at the second session only). Each event sequence was constrained by enabling relations, such that the three steps had to be completed in the correct temporal order for the sequence end-state to become apparent (although the actions could be physically completed in any order). We used sequences constrained by enabling relations to allow children with DS the best opportunity for immediate imitation and long-term delayed recall, as work with TD children has demonstrated that children younger than 20 months perform at chance on sequences that are arbitrarily ordered (Wenner & Bauer, 1999).
As shown in Figure 1, each event sequence was created in an analog form to allow an assessment of delayed generalization across cues (e.g., Lukowski, Wiebe, & Bauer, 2009; Phung et al., 2014). The analog sequences differed from the original in color and shape but not in size or texture. The sequences were blocked into groups of two and counterbalanced across event types (memory and generalization) and conditions (familiar or control); the sequence order within event types and conditions was randomized across sessions.
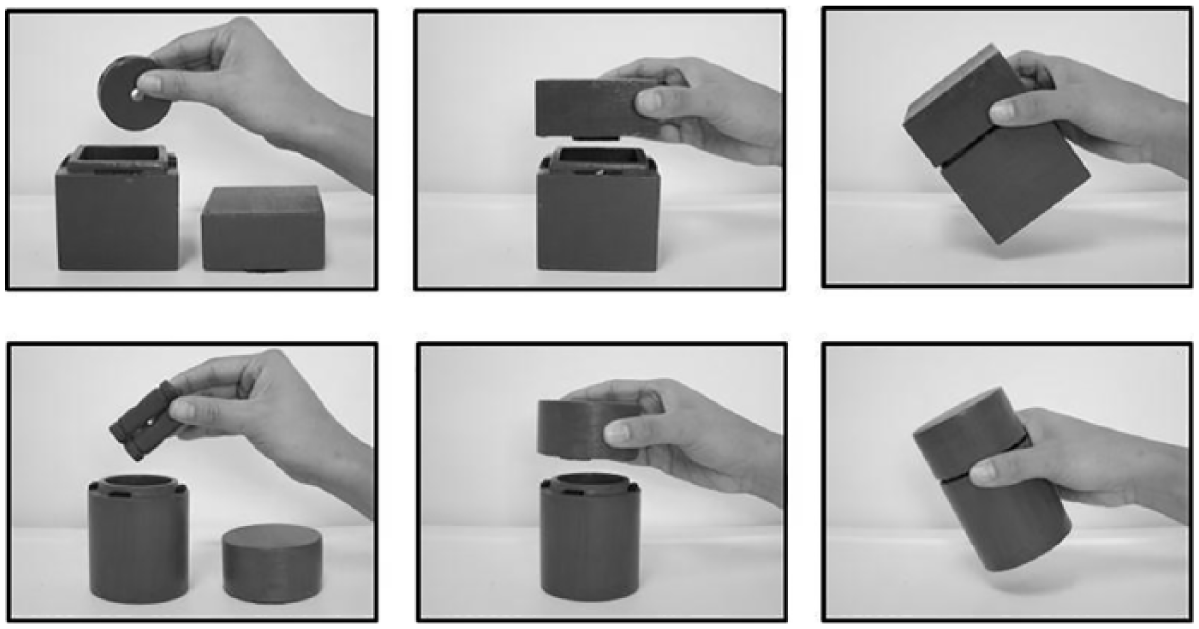
Example of the three-step event sequence Make a Shaker.
Procedure
The study was approved by the relevant Institutional Review Boards. For the questionnaire portion of the study, a waiver of written informed consent was granted; parents signed informed consent statements at the first session indicating their willingness to allow their child to participate in the behavioral portion of the study. All children were tested by the first author. Sessions were video recorded to allow for protocol checks and offline data coding.
Questionnaires
Parents received the questionnaires by mail, completed them at home, and returned them at the first session. Parents who did not have the questionnaires completed at that time returned them at the second session.
BSID-III (Bayley, 2006)
The child was seated across the researcher at an adult-sized table. After a brief warm-up procedure (e.g., Bauer & Lukowski, 2010; Bauer, Wenner, Dropik & Wewerka, 2000; Lukowski, Phung, & Milojevich, 2015; Phung et al., 2014), the researcher administered the mental portion of the BSID-III (Bayley, 2006). After the assessment was complete, parents were given a pamphlet describing chronological age-appropriate developmental milestones along with the recommendation to discuss any concerns with their child’s pediatrician.
Elicited imitation
Following administration of the BSID-III (Bayley, 2006), children were presented with four novel three-step event sequences in turn; two of these sequences are the focus of the present report. The researcher presented each sequence in turn along with a general verbal prompt (“What can you do with this stuff?”). This baseline period was child-controlled such that this phase of testing ended when children engaged in repetitive or off-task behaviors (e.g., repeatedly banging the props on the table or dropping them on the floor; Bauer et al., 2000; Bauer & Lukowski, 2010; Lukowski et al., 2015; Phung et al., 2014). After the baseline period, the researcher demonstrated each sequence of actions twice in succession with narration.
Immediate imitation was assessed for two of the sequences as an index of encoding (Bauer & Lukowski, 2010; Bauer et al., 2000; Lukowski & Milojevich, 2013; Lukowski et al., 2015; Lukowski et al., 2005; Phung et al., 2014). The researcher returned the sequence materials to the children along with the name of the event (“You can use this stuff to Make a Shaker. How do you Make a Shaker just like I did?”). The imitation period ended when children engaged in repetitive or off-task behaviors.
Approximately 1 month later (mean delay = 31 days; range from 27 to 41 days), children returned to the laboratory for an assessment of delayed recall memory or generalization across cues. Children tested in the memory condition (n = 10) were provided with the same event sequences that they had seen at the first session, whereas children in the generalization condition (n = 9) were presented with event sequences that were functionally identical to, but perceptually distinct from, those they had seen at the first session. Children were also presented with two novel control sequences that were not previously demonstrated by the researcher. These sequences were included because the participants were expected to have developed more mature problem-solving abilities over the 1-month delay (Bauer et al., 2000). As such, increased performance at delayed recall relative to baseline may result from increased spontaneous production of the TA rather than memory per se. For this reason, the most rigorous test of long-term memory occurs when performance on previously modeled familiar sequences are compared with performance on novel event sequences presented at the same session (Bauer et al., 2000; Lukowski et al., 2005).
The researcher presented the children with the familiar and novel control sequences in turn along with the name of each event. The event name was expected to serve as a retrieval cue for familiar events and as a suggestion of activities that could be completed with the novel sequence materials (“You can use this stuff to Make a Shaker. How do you Make a Shaker with this stuff?”) (Bauer et al., 2000). The delayed recall period ended when children engaged in the repetitive or off-task behaviors described earlier.
Data Reduction
Questionnaires
The data from the intervention questionnaire (Ly, 2013) were reduced to determine the percent of children involved in various interventions at the time of the study, previously but not at the time of the study, or never. We also recorded the number of months the intervention was in place for those children who had participated in each intervention.
BSID-III (Bayley, 2006)
The data obtained from the BSID-III were reduced as described in the administration manual so as to yield a DA for each child.
Elicited imitation
The average number of TA (maximum = 3) and PAs produced in the correct temporal order (maximum = 2) were coded and reduced separately by event type (memory or generalization), phase (baseline and immediate imitation at the first session), and condition (delayed recall and performance on novel control sequences at the second session). TA were coded when children performed any of the three actions demonstrated by the researcher; PAs were coded by recording the order in which the TA were produced. As the most conservative measure of recall, only the first occurrence of each TA was coded thus reducing the likelihood of providing credit for behaviors produced by chance or trial-and-error problem-solving (Bauer et al., 2000; Lukowski & Milojevich, 2013; Lukowski et al., 2015; Lukowski et al., 2005; Phung et al., 2014).
Data were coded by an undergraduate research assistant who was trained on data coding procedures using an existing corpus of data prior to participant testing and was unaware of the hypotheses of the study. The first author then independently recoded the data for 25% of the sample (n = 5). Mean percent agreement on the production of TA and their order was 97% (range from 90% to 100%).
Results
Twenty-one percent (n = 4) of the children were participating in SST at the time of their involvement in the study, 5% (n = 1) had previously participated in SST but were not involved at the time of the study, and 74% (n = 14) of the children had never participated in SST. Given the small percentages of children who ever experienced SST, we grouped children into those who had ever participated in SST (the SST+ group) and those who had not (the SST– group).
Demographic Information
One-way ANOVAs and Fisher’s exact tests (FET) were conducted to determine whether children differed by group on potentially relevant demographic characteristics. As shown in Table 1, group differences were not found when considering chronological age, DA, child sex, child ethnicity, child exposure to English in the home, maternal education, or the percent of children who had ever participated in occupational therapy, physical therapy, psychotherapy, or speech therapy.
Differences in Demographic Characteristics by Group.

Note. Group differences for categorical values were examined using Fisher’s exact tests due to the small sample sizes. The p-value associated with two-sided effects is reported. SST = social skills therapy.
Preliminary Analyses
As delayed recall memory and generalization across cues were assessed in a between-subjects design at the second session, we conducted preliminary analyses to examine whether performance differed by event type (delayed recall memory or generalization across cues) at each study session.
Encoding
We examined the impact of event type on encoding at the first session by conducting two 2 (event type) × 2 (phase: baseline and immediate imitation) mixed ANOVAs on the production of individual TA and PA completed in the correct temporal order. Main effects of phase were found on both dependent measures TA, F(1, 17) = 25.92, p < .0001, r = .78 and PA, F(1, 17) = 16.07, p < .001, r = .70, such that children performed more TA and PA at immediate imitation (TA: 1.71 ± .25; PA: .86 ± .19) relative to baseline (TA: .71 ± .15; PA: .11 ± .05). There were no main effects or interactions involving event type (null effects that were expected as the event type manipulation was not imposed until the second session).
Delayed recall
We then examined the impact of event type on mnemonic performance after the 1-month delay by conducting two 2 (event type) × 2 (condition: familiar and novel event sequences) on TA and PA. As at the first session, the analyses revealed only main effects of condition on TA, F(1, 17) = 11.50, p = .003, r = .64, and PA, F(1, 17) = 5.71, p = .03, r = .50, such that children performed more TA and PA on familiar events (TA: 1.37 ± .20; PA: .53 ± .12) relative to novel control sequences (TA: .87 ± .17; PA: .31 ± .11). There were no main effects or interactions involving event type.
These analyses indicate that, as a group, children with DS did not perform differently by event type at encoding or after the 1-month delay. Whereas a more stringent analytic approach would have included participation in SST as a between-subjects factor, such analyses could not be conducted due to the naturally occurring distribution of children in each group. Among children in the SST+ group, four children were tested on memory events and four children were tested on generalization events. Among children in the SST– group, six children were tested on memory events and one child was tested on generalization events. Because only one child in the SST– group was tested on generalization events, formal statistical analyses could not be conducted to determine whether involvement in SST was differentially associated with mnemonic performance by event type at each session. In addition, there is no existing literature to suggest whether participation in SST would be differentially associated with delayed recall memory and generalization across cues in children with DS. For these reasons, we collapsed across event type in the following analyses and adopted the conservative approach of including event type as a categorical covariate type (0 = delayed recall memory or 1 = generalization across cues) in all analyses concerning mnemonic performance at the second session (when the event type manipulation was imposed).
Mnemonic Performance and Participation in SST
Encoding
We examined whether participation in SST was associated with encoding by conducting two 2 (group) x 2 (phase) mixed ANOVAs on the production of TA and their order. A main effect of phase was found for TA, F(1, 17) = 34.45, p = .0001, r = .82, such that children performed more TA at immediate imitation (2.00 ± 0.25) relative to baseline (0.80 ± 0.16). A main effect of group was also apparent, F(1, 17) = 4.76, p = .04, r = .46, as children in the SST+ group performed more TA across phases (1.80 ± 0.32) relative to those in the SST– group (1.00 ± 0.19).
When considering memory for temporal order information, main effects of phase, F(1, 17) = 26.27, p = .0001, r = .78, and group, F(1, 17) = 8.65, p = .009, r = .58, were qualified by an interaction with one another: F(1, 17) = 5.24, p = .04, r = .49. These data are shown in Figure 2(a). Follow-up pairwise comparisons revealed that children performed more PA at immediate imitation relative to baseline regardless of their involvement in SST (ps < .01). Comparisons conducted by phase, however, indicated that children in the SST+ group performed more PA at immediate imitation relative to children in the SST– group (ps < .01); group differences were not found when considering performance at baseline.
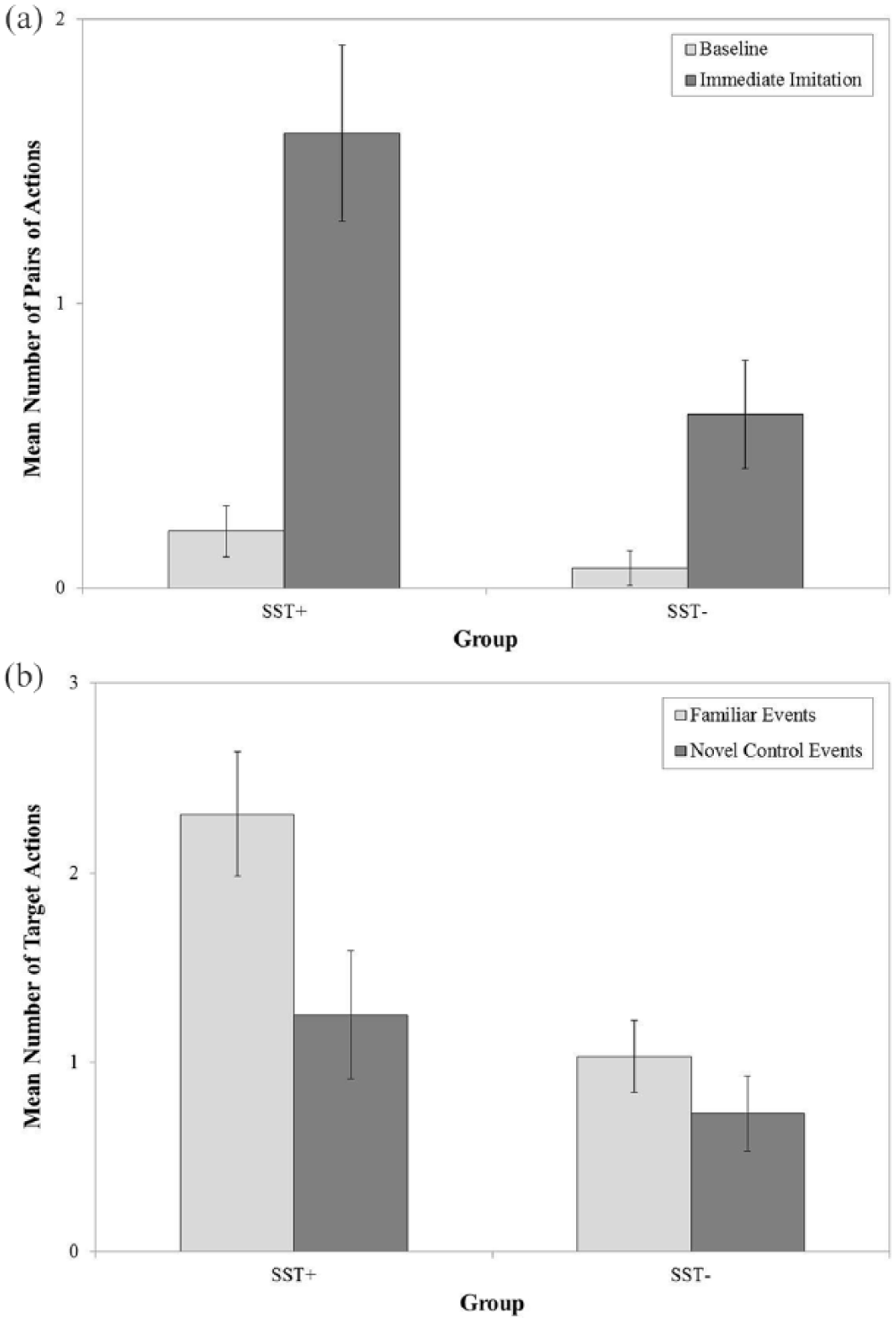
(a) Significant Group x Phase interaction for pairs of actions at the first session. Although children in both groups produced more pairs of actions at immediate imitation relative to baseline, children in the SST+ group produced more pairs of actions at immediate imitation relative to children in the SST– group. (b) Significant Group x Phase interaction for target actions at the second session. Delayed recall was found only for children in the SST+ group; in addition, children in the SST+ group produced more target actions on familiar events relative to children in the SST– group. SST = social skills therapy.
Delayed recall
We examined whether participation in SST was associated with mnemonic performance at the 1-month delay by conducting two 2 (group) × 2 (condition) mixed ANOVAs on the production of individual TA and their order controlling for event type. The analysis for TA yielded main effects of condition, F(1, 16) = 10.10, p = .006, r = .62, and group, F(1, 16) = 6.10, p = .03, r = .53 that were further qualified by an interaction with one another, F(1, 16) = 5.96, p = .03, r = .52. These data are shown in Figure 2(b). Follow-up pairwise comparisons conducted by group revealed that children in the SST+ group produced more TA on familiar sequences relative to novel control events (p < .001), whereas differences were not found by condition for children in the SST– group. Pairwise comparisons conducted by condition revealed that children in the SST+ group performed more TA on familiar events relative to children in the SST– group (p < .005); group differences were not found on novel control sequences. No significant effects were found when examining PA.
Encoding as a Potential Mediator
Because the ANOVAs revealed that participation in SST was associated with increased encoding of temporal order information and better memory for TA after a 1-month delay, we examined whether performance at immediate imitation mediated the relation between participation in SST and 1-month delayed recall of familiar events. Mediation models were examined using the regression-based approach outlined in Hayes (2013), in which evidence of mediation is obtained when a bias-corrected confidence interval (k = 10,000 resamples) does not include 0. Separate analyses were conducted for TA and PA. In both analyses, event type was included as a categorical covariate.
Comparable findings were obtained across the two tested models. Participation in SST (0 = SST– group or 1 = SST+ group) was positively associated with encoding (TA: a = 1.27, p = .03; PA: a = 1.04, p = .02). Encoding was also positively associated with 1-month delayed recall (TA: b = .39, p = .03; PA: b = .44, p = .004). The direct effect of participation in SST on 1-month delayed recall was not significant for either dependent measure (TA: c’ = .78, p = .07; PA: c’ = .14, p = .58), whereas the indirect effect of encoding on the association between participation in SST and 1-month delayed recall was significant for both TA and temporal order information (TA: ab = .50, confidence interval from .0074 to 1.2969; PA: ab = .4,542, confidence interval from .0351 to 1.1440).
Given these significant findings, we then examined the specificity of the effects by conducting comparable analyses on the number of TA and PA performed on novel control sequences at the second session. Neither the direct nor indirect effects were significant.
Discussion
Although participation in SST has been associated with improved cognitive outcomes in children with ASD (Cappadocia & Weiss, 2011; Hwang & Hughes, 2000; Ozonoff & Miller, 1995), there is a lack of research examining the potential benefits of this intervention on cognitive functioning in children with DS. The limited attention to the potential benefits of this therapeutic technique likely results from previous studies indicating that children with DS experience relative strengths in imitation and social interaction (Dykens & Hodapp, 2001; Libby et al., 1997; Rast & Meltzoff, 1995; Roberts & Richmond, 2015; Wright et al., 2006). Such competencies are also evident in research conducted using the elicited imitation paradigm, as children with DS encoded TA and temporal order at levels comparable with TD children matched on DA. Despite this strength in encoding, long-term memory for temporal order information was impaired in the children with DS. That is, whereas TD children recalled the temporal order of three-step event sequences after a 1-month delay, children with DS did not (Milojevich & Lukowski, 2016). The present study was conducted to collect pilot data from a small sample of children with DS to examine whether participation in SST was associated with enhanced encoding and 1-month delayed recall. We chose to examine the potential benefits of participating in SST in particular, as the social context shapes the manner in which TD infants recall the past (Lukowski et al., 2005; Phung et al., 2014) and children (e.g., Fivush & Fromhoff, 1988).
Consistent with previous research (Rast & Meltzoff, 1995; Roberts & Richmond, 2015), the results revealed that children with DS encoded the TA and their order relative to baseline independent of their involvement in SST. Similarly, children in the SST+ and SST– groups demonstrated encoding of temporal order information relative to baseline. However, participation in SST was associated with enhanced encoding of temporal order, such that children in the SST+ group performed more PA at immediate imitation relative to children in the SST– group. This finding indicates that although participation in SST was not necessary for children to encode the demonstrated TA and their order, participation was associated with more robust encoding of temporal order information in particular.
Contrary to what was observed at the first session, involvement in SST was necessary to support memory for individual TA after a 1-month delay (children did not show evidence of remembering temporal order information over the long term). In addition, examination of performance on familiar and novel events revealed findings that varied by group and condition. Participation in SST was only associated with performance on familiar events, as children in the SST+ group performed more TA on familiar events relative to children in the SST– group. The lack of group differences on novel events indicates that participation in SST was preferentially associated with memory and did not result in increased problem-solving abilities or general interaction with the sequence materials.
Given the demonstrated association between involvement in SST and mnemonic performance, mediation analyses were conducted to examine the process through which involvement in SST might facilitate recall. The results revealed that participation in SST was not directly associated with memory after the 1-month delay. Instead, encoding mediated the association between involvement in SST and 1-month delayed recall. This finding was observed when considering memory for individual TA and PA for previously modeled events but was not observed when considering performance on novel control events presented at the second session. The results pertaining to familiar events are reminiscent of other work conducted with TD infants in which encoding manipulations promoted evidence of long-term recall. For example, allowing infants additional exposures to to-be-remembered information (Bauer, Wiebe, Waters, & Bangston, 2001) or the opportunity to imitate the demonstrated TA before the imposition of an extended delay (e.g., Lukowski et al., 2005) has been associated with enhanced memory over lengthy delays.
Limitations and Future Directions
The present research represents proof of the concept that participation in SST is associated with enhanced encoding and 1-month delayed recall in children with DS and supports the notion that additional empirical attention should be devoted to understanding the potential benefits of participating in SST for children with DS. In addition to focusing on causal relations and additional description of the mechanism underlying the observed associations between involvement in SST and recall memory, subsequent research on this topic should account for some of the limitations of the present study. Given the preliminary nature of this research, we did not ask parents to report on the particular elements of SST experienced by children in the SST+ group. Future researchers should ask parents to report on the particular characteristics of the interventions experienced by their children so as to identify the specific elements of SST that are associated with encoding and delayed recall. In addition, although generally acceptable for pilot research and proof of concept studies, one of the primary limitations of this work is the rather small sample of children with DS who had participated in SST. However, this limitation reflects the natural state of participation in SST, as this intervention is not commonly experienced by children with DS. Despite this shortcoming, reported effect sizes for the conducted statistical analyses were quite large (most rs ≥ .50; Rosenthal & Rosnow, 1984), suggesting that future research with larger samples should yield similar findings.
Implications for Research and Practice
Although exploratory, the conducted research advances our understanding of the utility of SST for children with DS by revealing associations with encoding and 1-month delayed recall memory. These findings are meaningful in that they draw attention to the potential benefits of an intervention that is not commonly experienced by children with DS. Based on these preliminary results, future research should also determine whether SST facilitates performance on declarative memory tasks in older individuals and under test conditions that are less socially focused (such as the ability to recall previously presented word pairs; for a review of other hippocampus-dependent memory processes, see Eichenbaum, 2004). Experimental work is also needed to determine which elements of SST are causally associated with improvements in declarative memory. Better understanding of the impact of social skills interventions on children with DS through future empirical research may be instrumental in promoting cognitive competencies in these individuals. Specifically, such findings would have significant implications for promoting learning and retention in children with DS in educational and therapeutic contexts, thereby facilitating adaptive functioning in the short term as well as over extended delays.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by the Undergraduate Research Opportunities Program (UROP) at the University of California, Irvine.