
Abstract
This study examined changes in child mealtime behavior, diet variety, and family mealtime environment after intensive interdisciplinary behavioral treatment (IIBT) for 52 children referred to a day treatment feeding program. Children fell into three developmental status groups including autism spectrum disorder (n = 16), other special needs (n = 19), and no special needs (n = 17), with some having no known medical problems (n = 22) and some having gastrointestinal, cardiopulmonary, and/or endocrine-metabolic problems (n = 28). At pre-intervention and post-intervention, caregivers completed the About Your Child’s Eating scale, the Brief Assessment of Mealtime Behavior in Children, and a food preference inventory of 70 common foods (20 fruits, 23 vegetables, 12 proteins, 8 grains, 7 dairy). Mixed-factor 2 × 3 ANOVAs compared each of the 11 feeding outcomes across the two study phases (pre-, post-intervention) for the three developmental status groups. All feeding outcomes except fruit acceptance showed significant improvements from pre- to post-intervention, with no main effects for developmental status, and no interaction effects. Additionally, mixed-factor 2 × 2 ANOVAs compared each of the 11 feeding outcomes across the two study phases (pre-, post-intervention) for children with and without medical problems. All feeding outcomes except fruit acceptance showed significant improvements from pre- to post-intervention, with no main effects for medical status, and no interaction effects. Present results suggest that IIBT is effective for improving a number of children’s feeding problems, regardless of their developmental or medical status.
Keywords
Introduction
Although definitions for conceptualizing and classifying pediatric feeding disorders vary (Estrem, Pados, Park, Knafl, & Thoyre, 2017), it is estimated that over 20% of typically developing children and 70% of children with developmental disabilities exhibit some type of feeding problem during development (Benjasuwantep, Chaithirayanon, & Eiamudomkan, 2013; Sullivan et al., 2000). Pediatric feeding problems are often comprised of medical, behavioral, and oral motor components (Piazza, 2008) and may result in limited diet variety, chewing and or drinking difficulties, and reliance on supplemental tube feedings.
A growing number of studies demonstrate positive outcomes for children receiving behavioral intervention to treat various pediatric feeding disorders (Lukens & Silverman, 2014; Sharp, Jaquess, Morton, & Herzinger, 2010). Behavioral intervention has been found effective for reducing children’s dependency on supplemental tube feedings, increasing calories or grams of foods they consumed orally, expanding diet variety, and improving children’s mealtime disruptive behavior and its associated caregiver stress as well as aversion to mealtimes. Furthermore, research has supported the cost-effectiveness of intensive interdisciplinary behavioral treatment (IIBT) approaches for treating severe feeding problems (Dempster, Burdo-Hartman, Halpin, & Williams, 2016; Williams, Riegel, Gibbons, & Field, 2007).
Despite studies demonstrating the effectiveness of IIBT as well as the cost saving associated with such interventions, insurance companies are often reluctant to pay for services, such as day treatment programs which generally involve providing behavioral intervention across the day for a span of several weeks in a hospital setting with oversight by an interdisciplinary team of medical professionals, speech or occupational therapists, a dietitian, and a psychologist (Dempster et al., 2016), so it is important to continue reporting the benefits of IIBT programs. Further, although previous studies have compared the diets of those with and without autism spectrum disorder (ASD; Schreck, Williams, & Smith, 2004; Williams, Gibbons, & Schreck, 2005), to the best of our knowledge researchers have not yet examined children’s demographics associated with improvements seen in feeding problems after IIBT. For example, children may vary in how readily they respond to IIBT based on their developmental status (e.g., ASD, those with other special needs, and those without special needs), or based on the presence of medical problems (such as gastrointestinal, cardiopulmonary, endocrine-metabolic issues).
Purpose of the Present Study
The purpose of the present study was to conduct a retrospective chart review to examine the effects of IIBT on 11 feeding outcomes, including children’s mealtime behavior, diet variety, and family mealtime environment, in a sample of children with various developmental status and medical problems who completed intervention at a day treatment feeding program. Our hypothesis was that all feeding outcomes would show significant improvements after IIBT for children from each of three developmental status groups (ASD, other special needs, no special needs), and for children from two medical status groups (no gastrointestinal, cardiopulmonary, endocrine-metabolic problems; one or more of these medical problems).
Method
Participants
Study participants included 52 caregivers of children who completed IIBT at a hospital-based day treatment feeding program in a large metropolitan city (76.9% male; mean age = 52.56 months, SD = 31.20; mean body mass index z-score, BMIz = −.20, SD = 1.39; mean days of treatment = 22.76, SD = 7.83) during a span of 2 years (2015–2017). During this time period, an additional 13 patients received day treatment at the feeding program; however, eight families did not return post-intervention measures at the completion of treatment, five families withdrew from treatment, and three children were placed on a “medical hold” as they exhibited signs and symptoms of gastrointestinal (GI) discomfort during admission and required additional medical evaluation before continuing treatment. Caregivers completed a pre-intervention intake packet to report the children’s demographic information such as their child’s age, gender, medical diagnoses, developmental status, and endorsed treatment goals for their children’s admission. Possible treatment goals included increased food variety, increased food volume, improved mealtime behavior, improved food acceptance, improved chewing, and weaning from tube feeding.
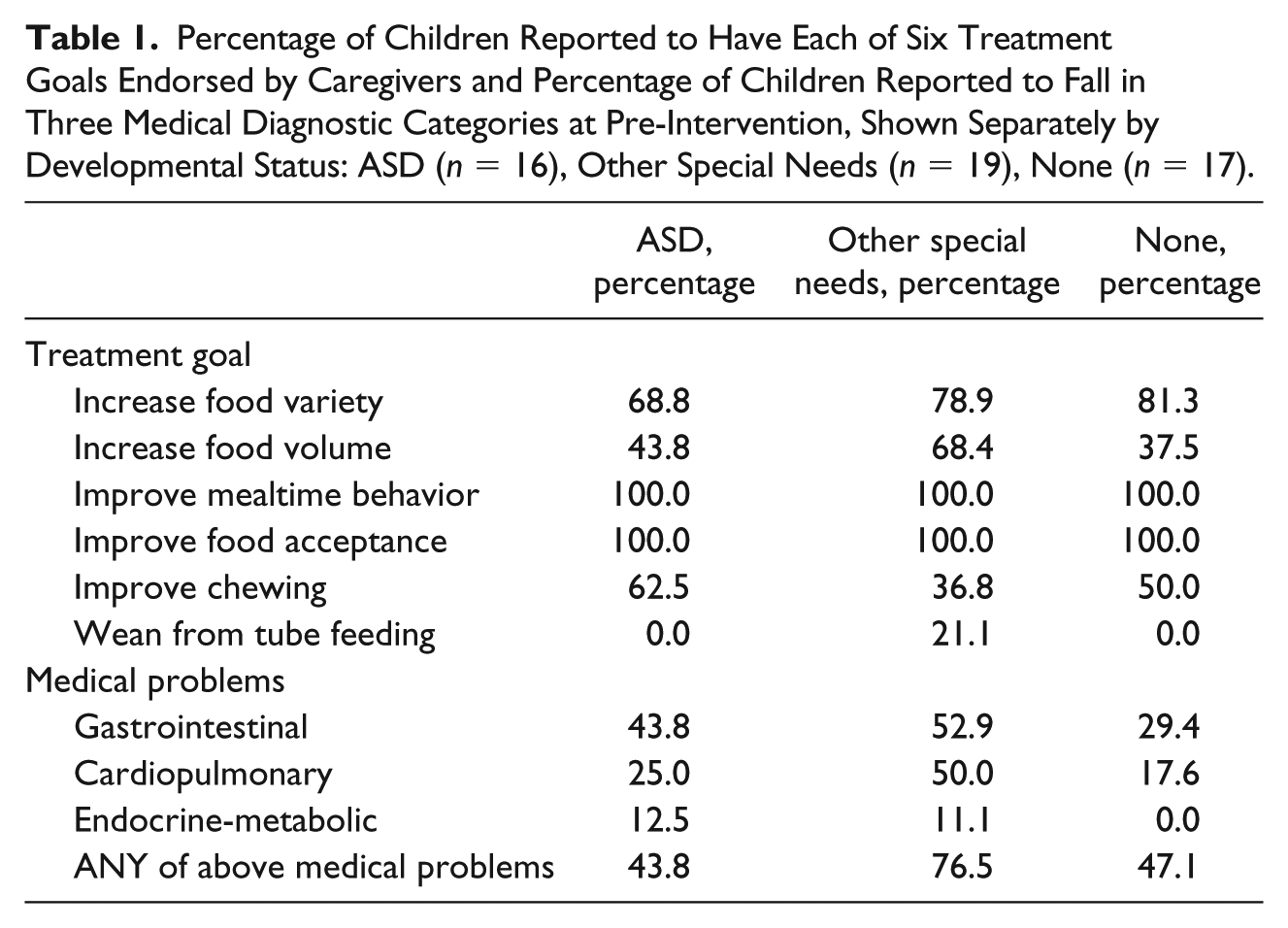
Caregivers reported whether or not (yes, no) their children had current or previously diagnosed gastrointestinal problems (i.e., gastroesophageal reflux, constipation, diarrhea, delayed gastric emptying, food allergies, lactose intolerance, and eosinophilic esophagitis), cardiopulmonary problems (i.e., heart abnormality, asthma, pneumonia, lung abnormality), or endocrine-metabolic problems (i.e., diabetes, kidney disease, liver disease, metabolic syndrome, growth abnormality). Additionally, the three above clusters of medical problems were summarized in a measure of whether or not (yes, no) children had any of the above medical problems (with missing data for 2 of the 52 children). Children’s weight status was determined by hospital staff, who measured the child’s weight in kg and height in cm, then calculated the child’s body mass index (BMI = kg2/m) z-scores in comparison to children of their age and gender, using data files from the Centers for Disease Control or the Children’s Hospital of Philadelphia online software for children over 24 months of age ( http://stokes.chop.edu/web/zscore ), and PediTools for children under 24 months of age ( http://www.peditools.org/growthinfant/ ). Children’s developmental status was determined by review of patient records and initial caregiver interviews by an interdisciplinary team that included a speech-language pathologist, dietitian, psychologist, pediatric nurse practitioner, and pediatric gastroenterologist. Three developmental status groups were identified: ASD (n = 16), other special needs including intellectual disability, speech problems, learning disabilities, cerebral palsy, spina bifida, seizure disorders, obsessive compulsive disorder, traumatic brain injury, and neurological problems (n = 19), and no special needs other than the children’s feeding problems (n = 17). Table 1 shows descriptive statistics for initial treatment goals endorsed by caregivers, and reported medical problems at pre-intervention, separately by children’s special needs status (ASD, other, none).
Percentage of Children Reported to Have Each of Six Treatment Goals Endorsed by Caregivers and Percentage of Children Reported to Fall in Three Medical Diagnostic Categories at Pre-Intervention, Shown Separately by Developmental Status: ASD (n = 16), Other Special Needs (n = 19), None (n = 17).
Prior to intervention, all children were reported to exhibit problem behaviors during mealtimes which prevented advancement in diet variety and/or consumption of age-appropriate textures thus, making a good fit for a behavioral model of care. Further, after undergoing an initial interdisciplinary evaluation, all patients were given medical clearance by the medical providers on the interdisciplinary team to receive IIBT as there were no suspected ongoing organic medical conditions (e.g., gastroesophageal reflux, slow gastric emptying, malabsorption, eosinophilic esophagitis, food allergies or intolerances) or feeding safety concerns that needed to be ruled out or treated prior to intervention.
Description of IIBT
Participants attended a day treatment feeding program between the hours of 8:15 am and 3:00 pm, Monday through Friday. Each child received four 45-min intervention sessions per day to address their individual treatment goals. All target foods and liquids were selected based on discussion with the feeding program’s dietitian and caregivers, who were asked to select foods eaten by others in the household but not yet eaten by their child. Intervention entailed the implementation of individualized behavioral protocols with manipulation of antecedent conditions and consequences throughout the meal (Laud, Girolami, Boscoe, & Gulotta, 2009; Seiverling, Hendy, & Yusupova, 2017; Sharp, Jaquess, Morton, & Miles, 2009; Williams, Field, & Seiverling, 2010). More specifically, intervention components included the use of positive reinforcement for acceptance of target foods, stimulus fading to increase bite sizes of new foods and introduce more advanced textures, and escape extinction which involved the non-removal of feeding demands contingent upon inappropriate mealtime behavior. Intervention length varied from 2 to 8 weeks (mean days of treatment = 22.76, SD = 7.83) and was determined by progress made towards achieving the child’s long-term goals (e.g., child accepts at least 85% of bites and drinks presented during meals within 10 s of presentation; child exhibits inappropriate mealtime behavior during less than 15% of bite and drink presentations during meals) that were developed by the feeding team and family at the outset of treatment. Behavioral therapists and speech-language pathologists initially implemented the behavioral feeding protocols, then caregivers were trained to implement the protocol. After caregivers successfully implemented the protocol in the clinic setting, they were instructed to apply it during all home meals for the remainder of the child’s admission and upon discharge.
Across each child’s admission, a dietitian, pediatric nurse practitioner, and gastroenterologist provided nutritional and medical monitoring. Nutritional and medical monitoring involved weekly case review meetings with therapists to review patient data, and weekly meetings with each patient family. The dietitian weighed each patient during family meetings, discussed volume and variety of foods eaten, provided recommendations regarding daily caloric intake and food choices, the patient’s daily menu, and tube weaning (if applicable). The nurse practitioner closely monitored signs and symptoms of GI discomfort across intervention and considered and prescribed medications such as H2 blockers, Proton Pump Inhibitors, prokinetics and/or appetite stimulants if a patient demonstrated GI signs and symptoms of discomfort. The nurse practitioner also reviewed any medications being taken by the patient, consulted with the patient’s other medical providers (e.g., primary care provider, allergist, or gastroenterologist) and made recommendations regarding supplemental formulas to be trialed during intervention, and medical testing (e.g., endoscopy, modified barium swallow study, allergy testing) to be performed based on patient signs and symptoms of GI discomfort or swallow safety concerns observed during intervention. The nurse practitioner also inquired about bowel movements and provided recommendations if the patient was experiencing any constipation or diarrhea during intervention. For instance, constipation could be addressed with dietary changes such as increased fiber content or formulas that may be more tolerable, or medication to improve bowel maintenance (e.g., Miralax).
Measurement of Feeding Outcomes
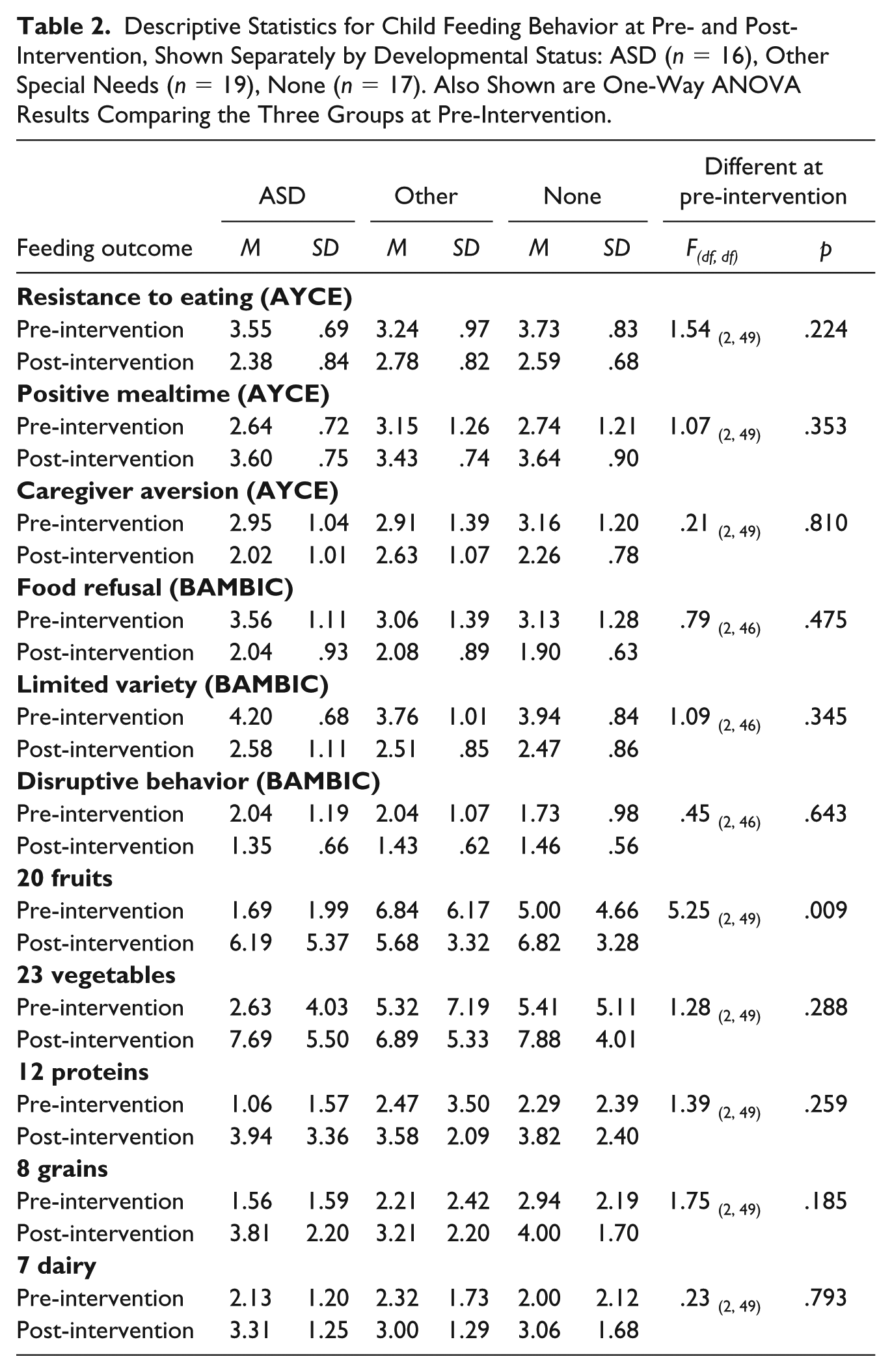
From parent surveys pre-intervention and post-intervention, children’s mealtime behavior and caregiver distress were measured with three subscales from the About Your Child’s Eating scale (AYCE; Davies, Ackerman, Davies, Vannatta, & Noll, 2007), and three subscales from the Brief Assessment of Mealtime Behavior in Children (BAMBIC; Hendy, Seiverling, Lukens, & Williams, 2013). Additionally, children’s food group-specific acceptance was measured with a 70-item food inventory comprising 20 fruits, 23 vegetables, 12 proteins, 8 grains, and 7 dairy foods. Table 2 shows descriptive statistics for each feeding outcome, shown separately by developmental status (ASD, other special needs, none).
Descriptive Statistics for Child Feeding Behavior at Pre- and Post-Intervention, Shown Separately by Developmental Status: ASD (n = 16), Other Special Needs (n = 19), None (n = 17). Also Shown are One-Way ANOVA Results Comparing the Three Groups at Pre-Intervention.
AYCE
Caregivers were asked to use five-point ratings to report how often each mealtime behavior usually occurred (1 = never, 2 = once in a while, 3 = sometimes, 4 = often, 5 = nearly always) for the 20-item AYCE (Davies et al., 2007). The AYCE includes three subscales of mealtime events. The 11-item Child Resistance to Eating subscale includes items such as “my child hates eating” and “I feel that it is a struggle or fight to get my child to eat” (Cronbach’s α = .81 at pre-intervention, .88 at post-intervention). The five-item Positive Mealtime Environment subscale includes items such as “mealtimes are among the most pleasant in the day” and “the family looks forward to meals together” (Cronbach’s α = .83 at pre-intervention, .73 at post-intervention). The four-item Caregiver Aversion to Mealtime subscale includes items such as “I dread mealtimes” and “it is hard for me to eat dinner with my child because of how he/she behaves” (Cronbach’s α = .79 at pre-intervention, .81 at post-intervention). The score for each AYCE subscale was determined by first revising ratings for any reversed items (1 = 5, 2 = 4, 3 = 3, 4 = 2, 5 = 1), then calculating the mean five-point rating for items in the subscale. Higher scores indicated more of the behavior represented by that AYCE subscale.
BAMBIC
Caregivers were asked to use five-point ratings to report how often each mealtime behavior usually occurred (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always) for the 10-item BAMBIC (Hendy et al., 2013). The BAMBIC includes three subscales of mealtime events. The three-item Food Refusal subscale includes the items “my child turns his/her face or body away from food” and “my child cries or screams during mealtimes” (Cronbach’s α = .82 at pre-intervention, .70 at post-intervention). The four-item Limited Variety subscale includes “my child dislikes certain foods and won’t eat them,” and “my child prefers the same foods at each meal” (Cronbach’s α = .43 at pre-intervention, .63 at post-intervention). The three-item Disruptive Behavior subscale includes the items “my child is aggressive during mealtimes – hitting, kicking, scratching others” and “my child is disruptive during mealtimes – pushing or throwing utensils, food” (Cronbach’s α = .80 at pre-intervention, .71 at post-intervention). The score for each BAMBIC subscale was determined by first revising ratings for any reversed items (1 = 5, 2 = 4, 3 = 3, 4 = 2, 5 = 1), then calculating the mean five-point rating for items in the subscale. Higher scores indicated more of the behavior represented by that BAMBIC subscale.
Food group acceptance
Caregivers were given a food preference inventory of 70 common foods and asked to report how often their child consumed the food (0 = never, 1 = daily, 2 = weekly, 3 = monthly). The foods included 20 fruits, 23 vegetables, 12 proteins, 8 grain products, and 7 dairy products. The child’s score for food group-specific acceptance was calculated as the total number of foods from that group that the child ate at least monthly.
Data Analysis
Pre-intervention comparisons
One preliminary data analysis was to compare children from three developmental status groups (ASD, other special needs, no special needs) for their pre-intervention reports of the 11 feeding outcomes, and for their report of medical problems. Therefore, we used SPSS 24 software to conduct one-way ANOVAs that compared the three developmental status groups for each feeding outcome. Also, we used SPSS 24 software to conduct 3 × 2 chi-square analyses that compared the three developmental status groups for their report (no/yes) of each cluster of medical problems (gastrointestinal, cardiopulmonary, endocrine-metabolic), as well as whether or not (no, yes) they had ANY of these medical problems (see Table 1).
Changes after IIBT according to developmental status
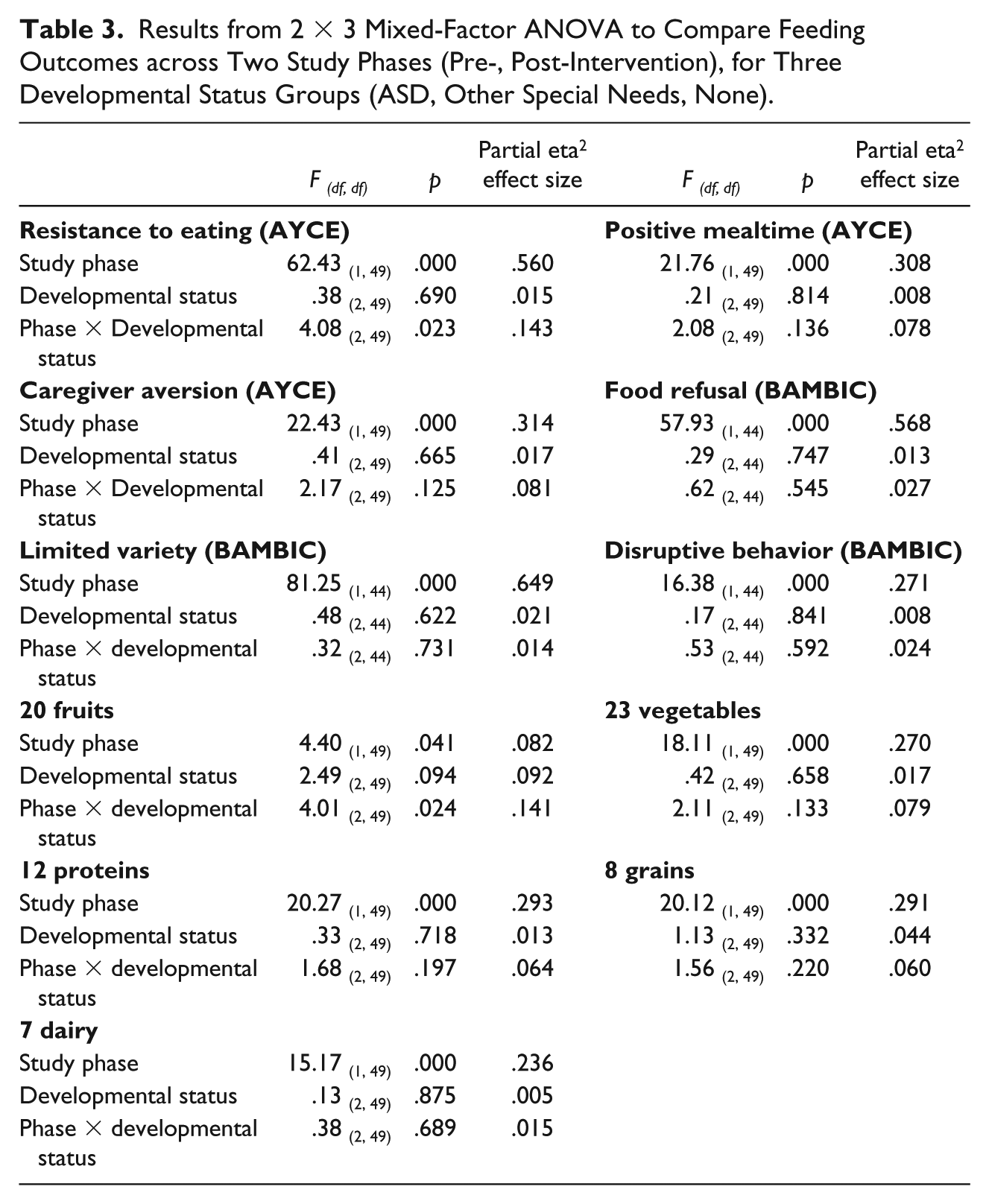
One primary goal for data analysis was to examine changes in the 11 feeding measures across two study phases (pre-intervention, post-intervention with IIBT), and for children from the three developmental status groups. We used SPSS 24 software to conduct 2 × 3 mixed-factor ANOVAs to compare each feeding measure across two study phases as the within-subjects factor, and three developmental status groups as the between-subjects factor. Because 11 analyses of feeding outcomes were conducted on the same small sample of 52 children, a conservative p < .01 was chosen as the criterion for significance to reduce the chance of Type I errors (see Table 3).
Results from 2 × 3 Mixed-Factor ANOVA to Compare Feeding Outcomes across Two Study Phases (Pre-, Post-Intervention), for Three Developmental Status Groups (ASD, Other Special Needs, None).
Changes after IIBT according to medical problems
Another primary goal for data analysis was to examine changes in the 11 feeding measures across two study phases (pre-intervention, post-intervention), and for children from two medical problems groups (no, yes). We used SPSS 24 software to conduct 2 × 2 mixed-factor ANOVAS to compare each feeding measure across two study phases as the within-subjects factor, and two medical problem groups as the between-subjects factor. Again, because 11 analyses of feeding outcomes were conducted on the same small sample of 52 children, a conservative p < .01 was chosen as the criterion for significance to reduce the chance of Type I errors (see Table 4).
Results from 2 × 2 Mixed-Factor ANOVA to Compare Feeding Outcomes Across Two Study Phases (Pre-, Post-Intervention), for Two Medical Problems Groups (No, Yes).

Changes in length of treatment according to developmental and medical status
Additionally, a one-way ANOVA was used to compare the days in treatment for children in the three developmental status groups (ASD, other, none). Also, a t test was used to compare the days in treatment for children with no or some medical problems.
Results
Pre-intervention comparisons
Results from the one-way ANOVAs revealed that the three developmental status groups were similar at pre-intervention for 10 of the 11 feeding measures considered in the present study (see Table 2). Only fruit acceptance showed significant differences for the three developmental status groups at pre-intervention, with post hoc comparisons indicating that children with ASD had less fruit acceptance at pre-intervention than either children with other special needs or children with no special needs (t(33) = 3.20, p = .003; t(31) = 2.62, p = .013), with no differences between the latter two groups (t(34) = 1.00, p = .324). Results from the 3 × 2 chi-square analyses revealed that the three developmental status groups did not differ significantly in their experience of gastrointestinal problems (chi-square = 1.96, p = .375), cardiopulmonary problems (chi-square = 4.69, p = .096), endocrine-metabolic problems (chi-square = 2.19, p = .334), or the summary measure of ANY of the above medial problems (chi-square = 4.42, p = .110) (see Table 1).
Changes after IIBT according to developmental status
Results from the 2 × 3 mixed-factor ANOVAs revealed significant improvements from pre- to post-intervention with IIBT for all 11 feeding outcomes except fruit acceptance. No significant main effects were found for developmental status, and no study phase × developmental status interaction effects, were found for any of the 11 feeding outcomes (see Table 3).
Changes after IIBT according to medical problems
Results from the 2 × 2 mixed-factor ANOVAs also revealed significant improvements from pre- to post-intervention with IIBT for all 11 feeding outcomes except fruit acceptance. No significant main effects for medical problems, or study phase × medical problems interaction effects were found for any of the 11 feeding outcomes (see Table 4).
Changes in length of treatment according to developmental and medical status
To compare the days in treatment for children in the three developmental status groups (ASD, other, none), a one-way ANOVA found no significant differences (F(2, 48) = 3.05, p = .057). The mean number of days in treatment was 26.3 (SD = 8.1) for ASD, 20.0 (SD = 5.5) for other special needs, and 22.6 (SD = 8.9) for no special needs. To compare the days in treatment for children with no or some medical problems, a t test found no significant differences (t(47) = 1.53, p = .133). The mean number of days in treatment was 24.9 (SD = 8.4) for children with no medical problems and 21.4 (SD = 7.3) for children with one or more medical problems.
Discussion
Results from the present study replicate findings from previous research showing significant improvements in pediatric feeding problems after IIBT (Benoit, Wang, & Zlotkin, 2000; Byars et al., 2003; Laud et al., 2009; Marshall, Hill, Wallace, & Dodrill, 2018; Seiverling et al., 2017; Sharp et al., 2009; Silverman et al., 2013). The finding that children with ASD had less fruit acceptance at pre-intervention than either children with other special needs or children with no special needs also supports previous studies comparing diet variety in those with and without ASD (Schreck et al., 2004). One new feature was the present study’s evaluation of changes in children’s feeding behavior after IIBT separately for children from three developmental status categories (ASD, other special needs, none), and for children from two medical problem status groups (no, yes).
Present results found significant improvement after IIBT for all 11 feeding outcomes considered except fruit acceptance, with these patterns similar for children from three developmental status groups (ASD, other special needs, no special needs), and for children from two medical status groups (no gastrointestinal, cardiopulmonary, endocrine-metabolic problems; one of more of these medical problems). The finding that fruit acceptance showed no improvements from IIBT warrants further investigation. As food choices for intervention were not standardized across participants and instead were selected based on consultation with the dietitian and the household diet, fruits may have been targeted less heavily than other food groups that were more calorie- and protein-rich.
Study Limitations and Directions for Future Research
The present study has several limitations. First, the study had a relatively small sample size. It is possible that additional differences with respect to feeding outcomes by developmental and medical status may be found with a larger sample and also if developmental and medical status categories are further broken down. For the purpose of this study, children included within the “other special needs” and “medical problems” categories had a range of diagnoses. Future researchers should continue to examine how children’s demographics are associated with improvements seen in feeding problems after IIBT. Children with various developmental disabilities and medical conditions (e.g., gastrointestinal, cardiopulmonary, endocrine-metabolic) may differ in their responsiveness to IIBT; however, such an examination of medical conditions may be challenging as it is common for a child to have more than one current or previous medical problem that could affect his or her feeding. While we were able to compare the outcomes of those with and without any identified gastrointestinal, cardiopulmonary, or endocrine-metabolic medical condition, future research with larger samples may allow examination of how specific medical problems may influence effectiveness of IIBT to improve pediatric feeding problems. Additionally, future research could also examine which feeding problems (e.g., chewing deficits, food selectivity, dependence on supplementary tube feedings) are associated with most improvement in mealtime behavior and diet variety after IIBT.
Another important limitation to mention is that the IIBT intervention length varied in the present study depending on progress made towards achieving the child’s long-term goals. While the average intervention length was just over four weeks and did not differ significantly across developmental and medical status, it was not consistent across all participants and could have impacted the results. Future research should examine how feeding outcomes vary according to the frequency and duration of IIBT, which could guide clinician recommendations for IIBT admission length and help determine whether IIBT could be successful in a less intensive outpatient model (e.g., for 1 hr per week instead of a full-day program, Monday through Friday).
It is also important to note that an additional 13 children received day treatment during this span of time for which post-intervention measures were not completed. While five families withdrew from treatment due to various reasons and three children were placed on “medical hold,” eight families of children who completed treatment did not return the post-intervention measures. It is possible that families did not complete the post-intervention measures due to dissatisfaction with the intervention; however, seven of these eight families did not speak English as their primary language and the post-intervention measures, which were given to families during the last several days of treatment, were not translated for each family unless the family requested translation services. Thus, the post-intervention measures may not have been completed for at least some of these families due to a language barrier.
Another limitation of the present study was found in some of the feeding measures themselves. First, only caregiver-reported measures were included in this study and not direct observation of mealtime behaviors before and after intervention. It is possible that there is poor correspondence between the caregiver-reported measures and actual child and caregiver mealtime behavior measured through direct observation of pre- and post-intervention meals. Further, although caregivers endorsed specific intervention treatment goals when filling out the initial intake packet prior to intervention, their ratings of each treatment goal following intervention were not included in the post-intervention outcome survey measures for this study. Although our food inventory examined acceptance of foods from various food groups, it is not a standardized measure and does not capture how often the foods were actually consumed or how much of the food was consumed. Standardized diet variety measures are limited, so future research should develop psychometrically sound measures of diet variety with easy-to-understand food amounts and frequency of consumption for use by caregivers in order to more accurately assess consumption. Additionally, future research should examine how IIBT changes food group-specific diet variety several months and even years after intervention. For instance, are children more likely to keep newly introduced grains and dairy foods in their diets compared to fruits and vegetables?
The present study’s measurement of one BAMBIC subscale (Limited Variety) was also problematic because its internal reliability values were below the traditionally expected .70, with Cronbach’s α = .43 at pre-intervention and .63 at post-intervention. This finding is not consistent with previous studies examining the psychometrics of the BAMBIC measure, which found internal reliability values well above .70 (Hendy et al., 2013; Seiverling et al., 2016) and warrants future research. The present study, as far as we are aware, is the first to use the BAMBIC subscales as outcome measures in evaluating IIBT effectiveness. Future research should continue to include the BAMBIC as well as other psychometrically tested feeding measures to determine which ones are best for capturing improvements following IIBT.
Lastly, it is important to note that the present study examined children’s feeding problems at pre- and post-intervention with IIBT, but no untreated control group was included. Therefore, it remains possible that the significant improvements seen in feeding problems were due to some other factor besides the IIBT intervention, such as expectation effects by caregivers. Future research should also consider implementing randomized controlled studies to examine improvement in feeding problems following IIBT.
Implications for Practice
Present results continue to support the use of IIBT for improving a wide range of children’s feeding problems (mealtime behavior, diet variety, family mealtime environment), with new documentation that such improvements are seen regardless of children’s developmental (ASD, other special needs, none) and medical problem status (no/yes). Currently, a limited number of locations exist where patients can receive IIBT (Silverman, 2010), with families often required to travel great distances and be on long waitlists prior to receiving intervention. Thus, there is a growing need for more facilities and programs to offer IIBT in inpatient, outpatient, and even telehealth services to provide easier access for families seeking IIBT for pediatric feeding problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.