
Abstract
Despite the efficacy of exposure for childhood anxiety disorders (CADs), dissemination has been unsuccessful. The current study examined community-therapist response to a brief (90-minutes) training in technology-assisted exposure therapy for CADs. The results indicated that therapists found the training in the therapy approach and technology acceptable, despite endorsing mainly non-exposure-based practice prior to the training. Training also increased positive beliefs about exposure, t (23) = 4.32, p < .000, that persisted 6 months later, t (23) = 4.56, p < .000. In addition, the number of therapists reporting an intention to implement exposure increased substantially from baseline (41.7%) to post-training (83.3%), with many therapists (70.8%) reporting use of exposure within the 6 months following training. However, automatically recorded data indicated little use of the technology. Results suggest that a dissemination message focusing on exposure is acceptable and has the potential to increase the use of this central treatment component.
A large empirical literature supports the efficacy of cognitive behavioral therapy (CBT) for childhood anxiety disorders (CADs) and OCD (hereafter jointly referred to as CADs; Skarphedinsson et al., 2015; Wang et al., 2017), marking these therapeutic approaches as evidence-based treatment (EBT). CBT for both conditions is similar (leading to their combination in this study), consisting of exposure-based exercises and other anxiety management strategies (AMS; e.g., relaxation and cognitive strategies) incorporated to varying extents (Ale et al., 2015). Because of its noted efficacy, there have been concerted efforts to disseminate CBT for CADs to community therapists. Unfortunately, these efforts have been generally unsuccessful (Beidas & Kendall, 2010; Whiteside, Deacon, et al., 2016), in part because of barriers in the clinical arena (e.g., clinician attitudes) that are largely outside the direct control of treatment developers in research settings (Becker-Haimes et al., 2017; Beidas et al., 2017). As a result, efforts have been made to improve dissemination by decreasing the complexity and increasing the accessibility of EBT (Weisz et al., 2012), two factors that are within the control of researchers. Consistent with this approach, the current feasibility pilot endeavors to improve community-based therapy for CADs by examining the self-reported response of community therapists who underwent training on a technology-enhanced protocol for CADs that focuses exclusively on exposure.
The success, or lack thereof, in disseminating EBT for CADs (i.e., CBT) is generally judged through the limited use of exposure by practicing clinicians (Higa-McMillan et al., 2017; Whiteside, Deacon, et al., 2016). Exposure has the most expert (Stewart et al., 2016) and empirical (Peris et al., 2017; Peris et al., 2015; Whiteside, et al., 2020) support as the active ingredient of CBT for CADs. However, surveys suggest that only approximately 5% of therapists provide exposure therapy and reviews of medical records indicate that only 15 to 25% of children receiving treatment outside of specialty clinics are introduced to exposure therapy (Higa-McMillan et al., 2017; Whiteside, Deacon, et al., 2016; Whiteside, Sattler, Hathaway, et al., 2016). Perhaps more concerning is that therapists who receive intensive training (day-long workshop plus weekly supervision) still do not deliver sufficient doses of exposure within controlled effectiveness trials (e.g., only 59% of youth received exposure; Southam-Gerow et al., 2010), or utilize exposure 3 to 5 years later (Chu et al., 2015). As such, the predominant approach to massed training in CBT for CADs with ongoing supervision has not been successful at increasing the use of exposure.
One avenue to improve dissemination of EBT for CADs may be to simplify the content of the treatment. While the absence of exposure use by community clinicians may be accurately seen as a failure of dissemination, it may be an overgeneralization to attribute this solely to clinician resistance to change. In fact, the research above decrying the poor use of exposure can also be interpreted to reflect the largely successful dissemination of other components of CBT for CADs. Therapists in the effectiveness trial were rated to be extremely adherent to the prescribed CBT protocol (98.8%; Southam-Gerow et al., 2010), and almost 80% of those therapists reported continued use of CBT 3 to 5 years later (e.g., primarily cognitive and problem solving strategies, as well as emotion education and relaxation; Chu et al., 2015). In addition, community-based therapists overwhelmingly endorse a cognitive-behavioral orientation (81.2%) and reliably report most frequently using components of CBT for CADs (e.g., problem solving, identifying emotions, relaxation training, and cognitive restructuring; Reid et al., 2018; Whiteside, Deacon, et al., 2016). Similar results are found when examining therapist documentation of clinical practice (Higa-McMillan et al., 2017; Whiteside, Sattler, Hathaway, et al., 2016). As such, community practice is actually fairly similar to the CBT for CADs used in research studies that typically begins with relaxation and cognitive strategies (AMS) followed by exposure later in treatment (Ale et al., 2015; Beidas et al., 2012; Southam-Gerow et al., 2010). In fact, treatment protocols used in research studies prescribe in-session exposure less frequently than one might expect, only in approximately one-third of sessions on average, with approximately one-quarter of protocols not requiring any in-session exposure (Whiteside, et al., 2020). As such, it appears that CBT for CADs is being successfully disseminated to community-based therapists, just not exposure.
Simplifying CBT for CADs could be achieved by focusing exclusively on exposure without other AMS components (Becker-Haimes et al., 2017; Whiteside, et al., 2020). The clinical appropriateness of such an approach is supported by the growing body of evidence suggesting that exposure without other AMS can be tolerable, effective, and efficient (Ale et al., 2015; Whiteside et al., 2015; Whiteside, et al., 2020). Clinicians might be more open to an approach to dissemination that encourages the flexible implementation of an evidence-based principle (e.g., exposure) than to one that prescribes adherence to a highly structured, sequential, multi-session manual (the literature regarding clinician attitudes not withstanding; Whiteside, Deacon, et al., 2016). In fact, a flexible and procedure-based modular approach to dissemination has been shown to more successfully improve community-based outcomes across anxiety, depression, and conduct problems in comparison to the standard structured manuals (Weisz et al., 2012).
The success of modular approaches supports continued efforts to redesign EBTs, rather than insisting that clinicians adopt treatment structures incompatible with clinical practice. However, it remains to be seen if a modular approach increases clinician delivery of the most effective and efficient treatment components (i.e., exposure), as it includes other AMS (self-calming, modifying negative cognitions). Moreover, like previous approaches to training in multi-component manuals, the modular approach begins with intensive training (6 days) followed by weekly supervision; a training model that may hinder adoption (Fritz et al., 2013; Whiteside, Sattler, Hathaway, et al., 2016). Promisingly, technology-based tools (e.g., online training) have been developed to connect clinicians with EBT tools to facilitate the implementation of modular protocols (Chorpita et al., 2008).
Accordingly, the current pilot study examines community-therapist response to a brief training in technology assisted exposure-focused therapy for CADs. The protocol and training differ from previous approaches in several ways: (1) by focusing exclusively on exposure as the active treatment component (Whiteside et al., 2015), (2) in its brevity (i.e., 90-minutes as compared to a full- or multiple-day training; Beidas et al., 2012; Weisz et al., 2017), and (3) in reliance on technology (i.e., Anxiety Coach, described in Methods section), rather than supervision, to support independence and change over time. The study has the following aims: (1) examine whether the brief technology-assisted training increased therapist openness to, and use of, exposure, (2) examine whether use of the technology could generate objective data regarding exposure use, and (3) explore therapist acceptance and satisfaction with the treatment protocol and technology. We hypothesized that community-based therapists would increase their self-reported acceptance and use of exposure following the training, with changes persisting over 6 months of practice.
Methodology
Sample
The sample consisted of 24 therapists (23 women, 95.8%) working in the community. The most frequently represented profession was social workers (15, 62.5%), followed by licensed marriage and family therapists (4, 16.7%), licensed professional counselors (3, 12.5%), and doctoral level psychologists (2, 8.3%). The most commonly endorsed theoretical orientation was cognitive behavioral (17, 70.8%), followed by cognitive (3, 12.5%) and eclectic (3, 12.5%), and then psychodynamic (1, 4.2%). The therapists had been practicing for an average of 16.46 years (SD = 11.22, range = 3 to 46). The majority of therapists (18, 75%) reported treating children with an anxiety disorder often or very often, while the remainder reported treating childhood anxiety disorders sometimes. At the beginning of the study, therapists most commonly reported treating generalized anxiety disorder (GAD) with 87.5% responding that they treated such patients sometimes, often, or very often, followed by OCD (75%), social anxiety disorder (62.5%), separation anxiety (58.3%), specific phobias (45.8%), panic (45.8%), and agoraphobia (8.7%).
Procedure
Potential therapists for the current study were recruited from participants in an earlier state-wide survey (Whiteside, Deacon, et al., 2016) and by word of mouth. A study coordinator contacted 149 therapists by email and invited them to participate in a study to pilot a new technology (Anxiety Coach) to facilitate treatment of CADs. The 25 therapists that expressed interest in the study were consented by the study coordinator via phone. One therapist discontinued before completing the consent process. The 24 therapists were then asked to complete an online survey regarding their approach to CADs (Time 1). Following the completion of the survey, 21 therapists completed a 90-minutes training in the therapy content and use of the technology with one of the study intervention specialists (three therapists declined training citing time conflicts and/or unrelated personal events). The therapists were then asked to familiarize themselves with the technology over the next 2 weeks before completing a second survey about their intentions for treating CADs in the coming 6 months, as well as their impressions of the technology (Time 2). Twenty therapists completed the Time 2 survey. During the next 6 months, the therapists were encouraged to use the Anxiety Coach application with their patients. The intervention specialist that provided the initial training was available for consultation via phone or email as needed. At the end of 6 months, 17 therapists completed a final survey about their treatment of CADs over the past 6 months as well as their experience with the technology (Time 3). Of the 17 therapists who completed all three timepoints of the current study, eight had also participated in a previous community survey (Whiteside, Deacon, et al., 2016), termed Time 0 herein, and thus data from an additional time point prior to the training associated with the current study. This pre-existing data was again included in the present study to examine whether symptom variables had improved with the passage of time between studies, rather than due to the training intervention. The therapists were remunerated for their participation with an iPodTouch and $50. The study was approved by the Institutional Review Board.
Materials
Surveys
Treatment techniques
Therapists were asked to describe their practice by rating the frequency with which they used 34 therapy techniques in their typical clinical practice. Details including a listing of each item have been published previously (Whiteside, Deacon, et al., 2016). Respondents endorsed the frequency with which they used treatment techniques when working with anxious children (0-never used, 1-rarely used, 2-moderately used, 3-often used, 4-always used). The directions at Time 1 and 3 were revised to focus on the last 6 months. The directions at Time 2 were reworded to reflect intent (changes indicated in all capital letters): “Please indicate how often you PLAN TO USE the following techniques OVER THE NEXT 6 MONTHS to treat
As in the earlier study, items were combined into the following treatment categories: (a) Exposure: therapist-assisted and client-directed exposure, as well as elimination of safety behaviors; (b) Anxiety Management Strategies (AMS): non-exposure techniques included in traditional CBT for CADs (i.e., problem solving, identifying emotions, breathing retraining, muscle or breathing relaxation, cognitive restructuring), (c) CBT-related strategies: other techniques that are not included in traditional CBT for anxiety but have some topographical relation to CBT through targeting thoughts, behavior, or mindfulness (i.e., mindfulness, meditation, biofeedback, motivational interviewing, replacing negative thoughts with positive thoughts, thought stopping, distraction, positive imagery); and (d) Non-CBT: techniques that are not part of CBT, are more experiential in nature, are not included in evidence-based treatment manuals for child anxiety, and do not topographically relate to CBT techniques (i.e., client centered, nondirective, family systems, music therapy, art therapy, sand tray therapy, play therapy, attachment, psychodynamic, hypnosis). To estimate the degree to which therapists used exposure versus other techniques, the categories were compared as proportions of total technique use (i.e., items within each of the four categories were averaged and divided by the total of scores from the four categories). Finally, after completing the list of techniques respondents were provided with a brief description of exposure and asked whether they provided this therapy to anxious children, during which session they began implementation, and the percentage of therapy spent with the child alone, the parent alone, and both together.
Therapist Beliefs about Exposure Scale
The Therapist Beliefs about Exposure Scale (TBES) is a 21-item questionnaire that assesses therapist beliefs about the safety, tolerability, and ethicality of exposure therapy (Deacon et al., 2013). Participants use a 5-point scale ranging from 0 (disagree strongly) to 4 (agree strongly) to indicate their agreement with statements illustrating potential therapist concerns about exposure (e.g., “Most clients perceive exposure therapy to be unacceptably aversive”). Higher scores indicate greater negative beliefs about using exposure therapy to treat anxious clients. The TBES has previously demonstrated excellent internal consistency (α = .95), 6 month test-retest reliability (r = .89), and good construct validity (Deacon et al., 2013). The instructions for the TBES were the same as previous usage at each time point.
Modified System Usability Scale
The Modified System Usability Scale (mSUS) is a 10-item scale developed to quickly assess the usability of a given product or service (Brooke, 2013). Respondents rate items from 0 (disagree strongly) to 4 (agree strongly). Items include ease of use, level of complexity, perceived need for support, and liking. The total score is the sum of the items multiplied by 2.5. The mSUS has shown good reliability and validity over the more than 30 years of its wide use, during which time the wording has been slightly modified to improve clarity (Bangor et al., 2008). In addition to the 10-items, the mSUS includes a single-item adjective rating scale ranging from worst imaginable to best imaginable. Therapists completed the mSUS after the initial training (Time 2) and again after having the opportunity to integrate the training and use of the Anxiety Coach application into their practice (Time 3).
In addition to the mSUS, therapists rated eight items regarding the content of the Anxiety Coach program and training from 0 (disagree strongly) to 4 (agree strongly). The items covered ease of use for each treatment component (psychoeducation, fear ladder building, recording exposures) and interface (mobile app, web-based), adequacy of the training in specific skills (conducting exposure therapy, using the technology), and likelihood of recommending Anxiety Coach to other therapists. The wording at Time 2 reflected anticipated use (e.g., “It will be easy to use. . .”) while wording at Time 3 reflected past experience (e.g., “It was easy to use. . .”). At both Time 2 and Time 3, therapists were asked to provide comments about what they liked most and least as well as what they would change. Finally, at Time 3, therapists reported on how many patients they used the program with and reasons why they did and did not use Anxiety Coach with patients.
Training
Phone training
Intervention specialists provided training in using an online- and mobile device-based application to conduct parent-coached exposure therapy. The training was delivered during a single 60- to 90-minutes phone call. Prior to the call, the study coordinator provided the therapist with an iPodTouch, instructions for accessing the application, and a written therapist manual. During the training, the intervention specialist reviewed common questions and concerns therapists have about exposure, helped the therapist create a training patient account that could be accessed through both the online- and mobile device-based application, and covered how to use the technology to implement parent-coached exposure therapy. The specialist also reviewed two quick-reference guides, one providing screen shots and explanations regarding how to use the technology and a second that provided a session-by-session timeline for therapy. Finally, the specialist encouraged the therapist to contact him or her whenever needed during the study with any questions about the technology, the treatment protocol, a specific patient, or any other topic.
Treatment Content
The treatment protocol consisted of parent-coached exposure therapy which has been described previously (Whiteside et al., 2015). The treatment is designed to maximize engagement in exposure by: (1) beginning in-session exposure as soon as possible, (2) not presenting other techniques (e.g., relaxation, cognitive restricting) that divert time and attention from exposure, and (3) conducting exposures in-session with children and parents together to train parents to be exposure coaches for out of session practice. The training manual provided a session-by-session guide recommending that psychoeducation about the cognitive behavioral model of anxiety be introduced and used to understand the child’s symptoms in session 1, followed by building a fear ladder in session 2, and beginning in-session and assigned parent-coached exposure in session 3. The content of all subsequent sessions involved the therapist helping the parent coach the child through in-session exposures and planning/reviewing home exposures of increasing difficulty.
Online- and Mobile Device-Based Application
The technology consisted of the Mayo Clinic Anxiety Coach application as described previously (Carper, 2017; Whiteside, 2016; Whiteside et al., 2019). Anxiety Coach contains four treatment sections: (1) progress and engagement tracking, (2) psychoeducation, (3) fear ladder creation, and (4) completion of exposures. The online computer-based interface provided tools to facilitate the therapists’ delivery of education, building fear ladders, and recording exposures with patients in the office, but did not provide a specific structure (i.e., it did not include a session-by-session format). To facilitate fear ladder building, Anxiety Coach provides a library of exposure exercises grouped by fear topic to assist in populating fear ladders, while also allowing items to be entered via free-text. To facilitate exposure, Anxiety Coach walks the user through selecting an item from the fear ladder, rating anxiety throughout the exposure, and reviewing the outcome of the exposure. Children and their parents can use the mobile device-based application to conduct and record exposures at home, as well as rate symptoms, and revise their fear ladder. Information entered in one medium is synchronized with the other, allowing therapists to track patient engagement and improvement remotely. Usage data from Anxiety Coach was also available to for analysis. The study staff could review the patient accounts for each therapist and record whether: (1) fear ladders were built; (2) the computer-based interface was synched with a mobile-device; (3) symptom severity ratings were entered; and (4) exposures were recorded.
Intervention Specialists
Three intervention specialists (one doctoral level psychologist, and two masters level therapists) provided training for the study therapists. Each of the intervention specialists were familiar with Anxiety Coach and had extensive experience providing parent-coached exposure therapy. The doctoral level psychologist designed the curriculum and trained the masters level therapists in its delivery.
Planned Analyses
Descriptive analyses were used to examine demographics, acceptability of the program at Time 2 and Time 3, as well as use at Time 3. Independent samples t-tests and a Goodness of Fit Chi-square test were used to compare the current sample to the community study sample (Whiteside, Deacon, et al., 2016). McNemar’s test was used to compare percentage of therapists endorsing use of exposure between Time 1 and Time 2 as well as between Time 1 and Time 3. Paired-samples t-tests were used to examine change in TBES and proportional technique use from Time 1 to Time 2 and from Time 1 to Time 3. When responses were missing at Time 2 and/or Time 3, the last observation was carried forward. To account for the eight analyses at each time point, a Bonferroni correction was applied resulting in a significance level of .006. To control for the effect of time, changes in TBES, as well as proportional use of exposure and AMS, were examined with repeated measures analyses of variance (RMANOVAs) using the Time 0 data from the previously described subsample (n = 8) (Whiteside, Deacon, et al., 2016). Correlational analyses were used to examine the association between acceptability at Time 2 and years of practice. Therapist comments about the program collected at Times 2 and 3 were combined and summarized.
Results
Representativeness (Time 1)
The current sample was similar to that from the previously reported state-wide study describing treatment of CADs in community settings (Whiteside, Deacon, et al., 2016). Therapists in the current sample reported practicing for an average of 16.46 years, SD = 11.22 (vs. 15.63 years, SD = 10.3 in previous sample) and most frequently endorsed CBT as a theoretical orientation (70.8% vs. 81.2%). The sample consisted of social workers (62.5% vs. 42.9%), marriage and family therapists (16.7% vs. 10.8%), psychologists (8.3% vs. 30.3%), and professional counselors (4.2% vs. 16.0%). Treatment variables are presented in Table 1. Fewer therapists in the current sample (41.7%) endorsed using exposure than the 61.4% in the previous study, X2 (1, N = 24) = 3.94, p = .047. The current therapists’ mean scores differed from the earlier sample on proportional use of exposure [t (23) = 2.89, p = .008] and proportional use of non-CBT techniques [t (23) = 3.03, p = .006]. The current therapists’ more negative views about exposure on the TBES were not statistically significant, t (23) = 1.90, p = .07.
Survey Results.
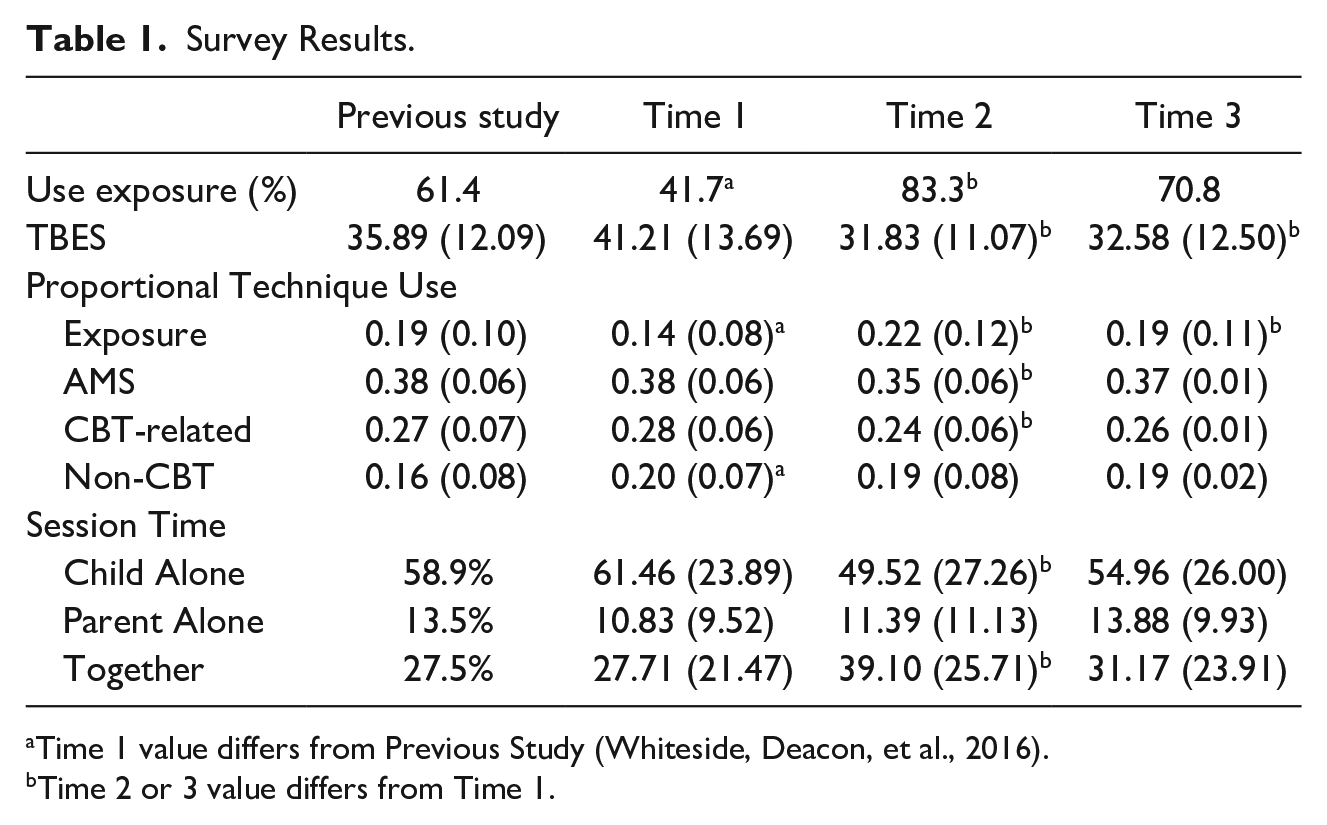
Time 1 value differs from Previous Study (Whiteside, Deacon, et al., 2016).
Time 2 or 3 value differs from Time 1.
Four of the participants did not complete the survey at Time 2. Although the small sample size precluded statistical analyses, when compared to study completers (provided data at Time 2, n = 20), the non-completers (n = 4) had been practicing for more years (21.75 vs. 15.40), were less likely to endorse a CBT or cognitive orientation (50% vs. 90%), spent more session time with the child alone (78.75% vs. 58.00%) and less with parent and child together (11.25 vs. 31.00), reported less proportional use of exposure (.10 vs. .15), more AMS (.40 vs. .37), more non-CBT (.22 vs. .20), and were less likely to endorse using exposure (50% vs. 60%). Similar differences were found when comparing therapists who completed Time 3 to those who dropped out at Time 3. Finally, comparison of the subsample of therapists who had both participated in the community study and provided data at all three time points for the present study (n = 8; Whiteside, Deacon, et al., 2016) to the remainder of the sample (n = 16) revealed that the subset had been practicing for more years (22.13 vs. 13.63), included at least 75% social workers/ marriage and family therapists, was similarly likely to endorse a CBT or cognitive orientation (87.5% vs. 81.3%), spent less session time with the child alone (51.25 vs. 66.56) and more with parent and child together (36.88 vs. 23.13), reported more proportional use of exposure (.19 vs. .12), less use of AMS (.36 vs. .39), less non-CBT treatment methods (.19 vs. .21), and were more likely to endorse using exposure (62.5% vs. 56.3%).
Response to Training (Time 2)
The results from the Time 2 survey are presented in Table 1. The percentage of therapists reporting an intent to use exposure was significantly greater than the percentage that had previously reported using exposure at Time 1, McNemar’s test df = 1, p = .002. Compared to their Time 1 description of their practice, at Time 2 therapists reported intent to use more exposure [t (23) = 5.90, p < .000], in contrast to less intent to use AMS [t (23) = 3.07, p = .005], and CBT-related techniques [t (23) = 4.63, p < .000], but no change in non-CBT techniques [t (23) = 2.62, p = .015]. At Time 2, therapists also reported fewer negative beliefs about exposure on the TBES, t (23) = 4.32, p < .000. Finally, compared to Time 1, therapists at Time 2 described intent to spend less session time with children alone [t (23) = 4.17, p < .000] and more time with parent and child together [t (23) = 3.11, p = .005].
Practice Change (Time 3)
The results from the Time 3 survey are presented in Table 1. The percentage of therapists reporting use of exposure over the previous 6 months was non-significantly greater than the percentage that had reported using exposure prior to Time 1, McNemar’s test df = 1, p = .016. Compared to their Time 1 description of their practice, at Time 3 therapists reported more proportional use of exposure [t (23) = 3.69, p = .001], but no change in use of AMS [t (23) = 2.28, p = .032], CBT-related techniques [t (23) = 2.41, p < .024], and non-CBT techniques [t (23) = 2.55, p = .018]. At Time 3, therapists also reported fewer negative beliefs about exposure on the TBES, t (23) = 4.56, p < .000. Finally, therapists’ description of the time spent with children and parents at Time 3 did not differ significantly from Time 1.
Controlling for Passage of Time (Times 0-3)
Eight of the therapists had completed the survey for the previous study of child anxiety treatment in the community (Time 0; Whiteside, Deacon, et al., 2016) and all three surveys in the current study. Results from the four time points for percentage endorsing exposure use, as well as mean score on TBES, proportional exposure use, and proportional AMS are presented in Figure 1. The change in TBES over time was significant, F (3, 21) = 12.45, p < .001. Simple planned contrasts indicated that Time 0 did not differ significantly from Time 1, F (1, 7) = 0.40, p = .55. However, Time 0 was significantly greater than Time 2 [F (1, 7) = 12.86, p = .009] and Time 3 [F (1, 7) = 19.44, p = .003], indicating increasing approval and positive attitudes toward exposure over the course of the current study. The change in proportion of exposure utilized in practice over time was significant, F (3, 21) = 18.81, p < .001. Simple planned contrasts indicated that Time 0 was significantly lower than Time 1 [F (1, 7) = 12.72, p = .009], Time 2 [F (1, 7) = 21.31, p = .002] and Time 3 [F (1, 7) = 38.26, p < .001]. Finally, the change in proportion of AMS over time was significant, F (3, 21) = 7.80, p = .001. Simple planned contrasts indicated that Time 0 did not differ significantly from Time 1, F (1, 7) = 3.60, p = .10. However, Time 0 was significantly greater than Time 2 [F (1, 7) = 10.75, p = .014] and Time 3 [F (1, 7) = 25.15, p = .002], indicating decreased use of AMS over the course of the current study.
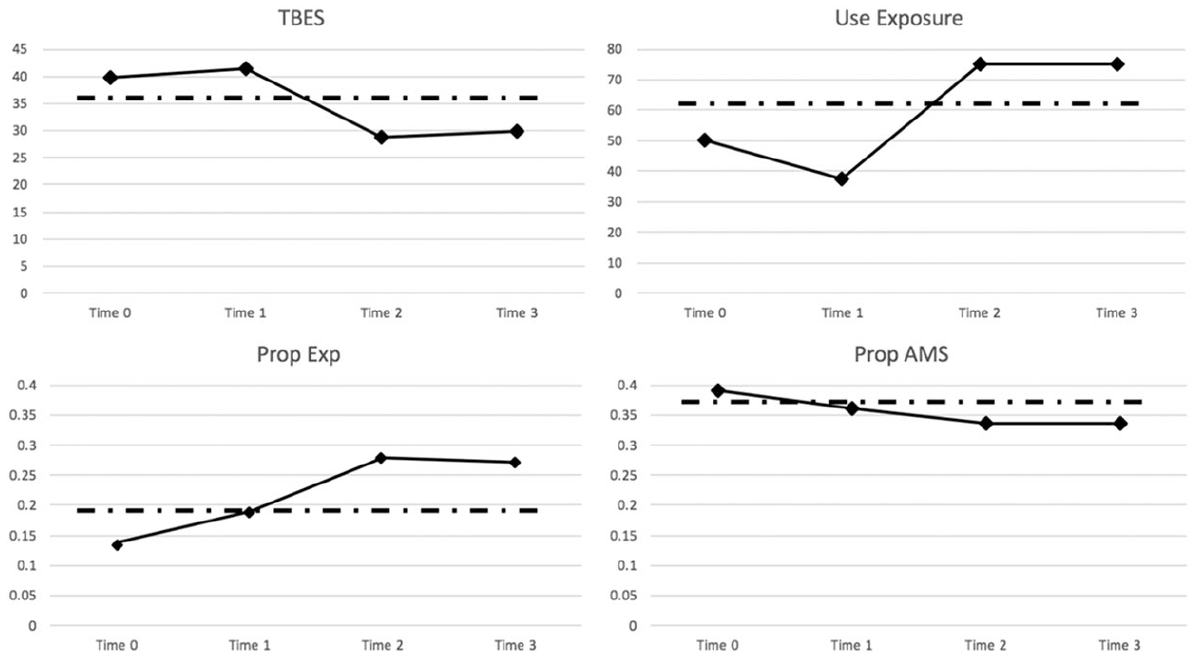
Change over time.
Acceptability
Therapist ratings regarding acceptability are presented in Table 2. At Time 2, on average, the therapist ratings indicated agreement that the training in the therapy content and technology use was adequate (mean of 2.80 and 2.75 respectively; response value of 3 = agree). Regarding the therapy content, 85% of the therapists agreed or strongly agreed that the training was adequate, while 15% were unsure or disagreed. Regarding technology training, 75% of the therapists agreed or strongly agreed that the training was adequate, while 25% were unsure or disagreed. Respondents generally agreed (means of 2.90 to 3.15; response value of 3 = agree) that each component would be easy to use, but were less sure (means of 2.45 to 2.55) that the interfaces would be easy to use or if they would recommend it to other therapists. The average mSUS ratings for the Anxiety Coach application at Time 2 fell in the marginal range (Brooke, 2013) and the mean adjective rating (ranging from worst imaginable to best imaginable) of 4.80 fell just below good (response value of 5). The majority of the sample (70%) rated Anxiety Coach as Good or Excellent, while 20% rated it as Okay, and 10% as Poor. Years of practice was negatively related to therapist ratings of adequacy of therapy training (−.48, p = .034), adequacy of technology training (−.58, p = .008), and mSUS (−.58, p = .007).
Acceptability Ratings.
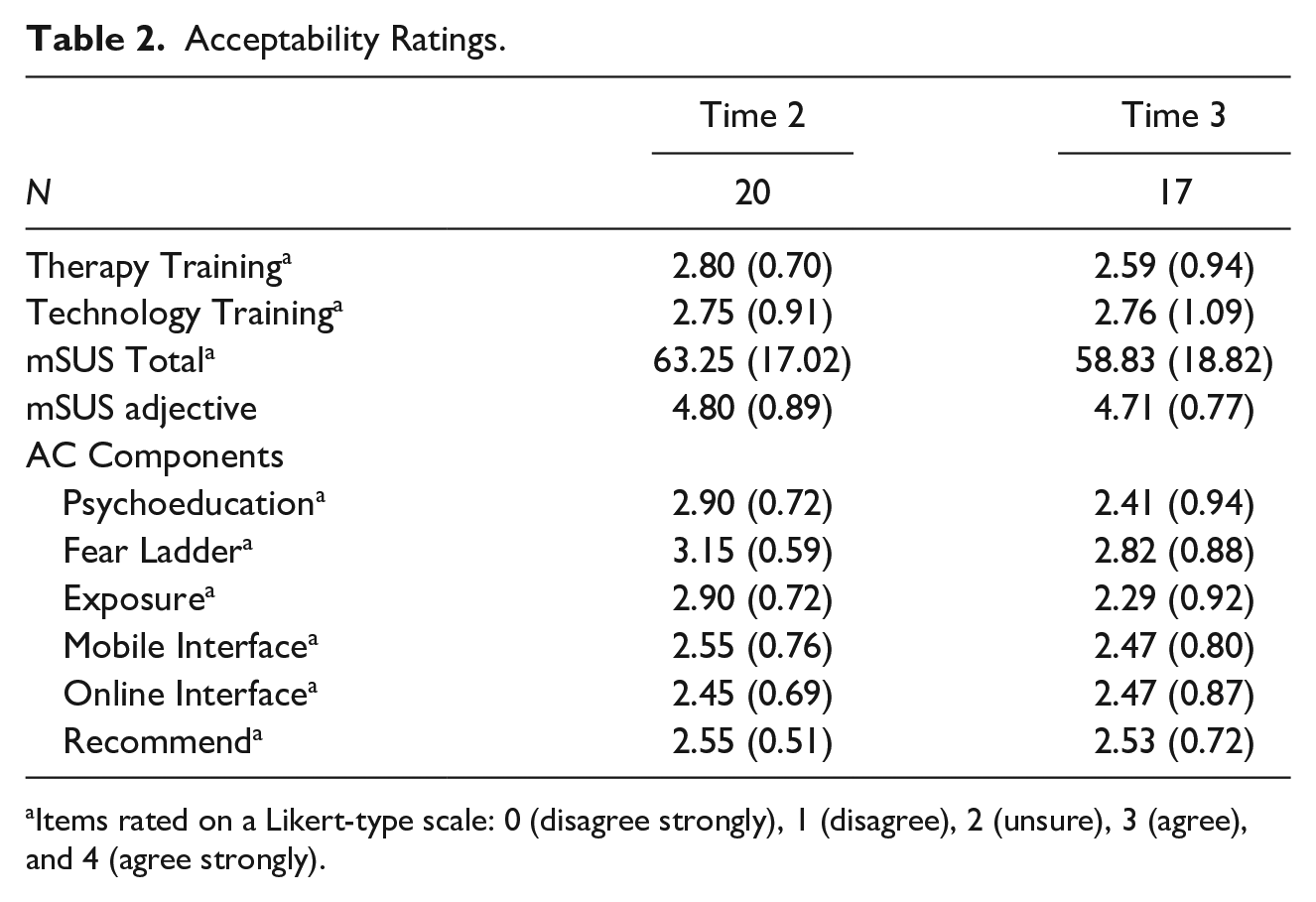
Items rated on a Likert-type scale: 0 (disagree strongly), 1 (disagree), 2 (unsure), 3 (agree), and 4 (agree strongly).
Therapist ratings at Time 3 were generally lower than those at Time 2. Only 64.7% of therapists agreed or strongly agreed that the therapy training was adequate after having the opportunity to implement it in their practice, while 35.3% were unsure or disagreed. Regarding the technology training, 76.4% continued to agree it was adequate, while 23.5% disagreed. At Time 3, 64.7% continued to rate the program as Good or Excellent, while 35.3% rated it as Okay or Poor.
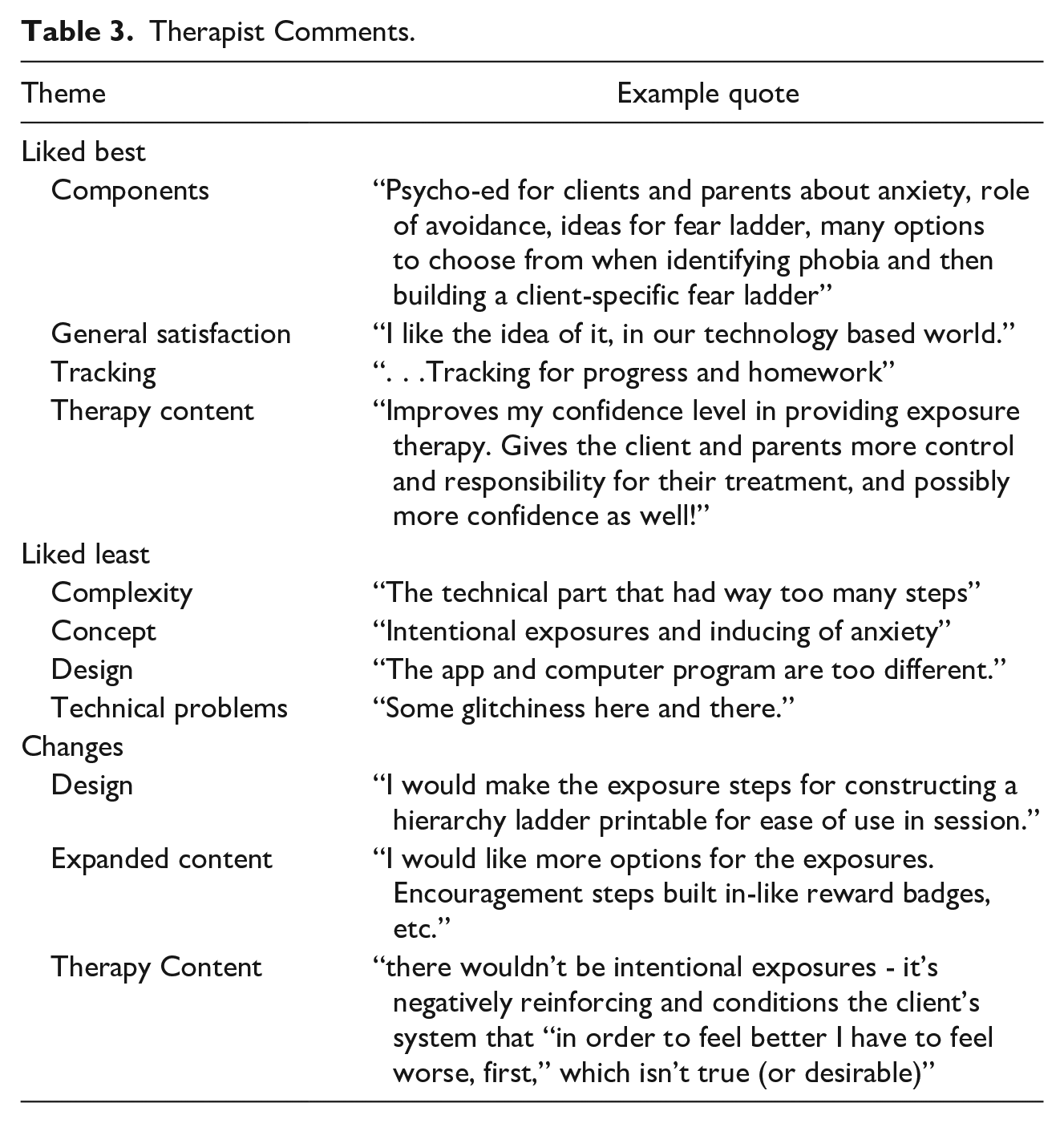
Fifteen therapists provided 26 comments about what they liked best about the program on the Time 2 and 3 surveys combined (total exceeds 26 as comments could address multiple themes; sample comments are in Table 3). Eleven of the comments expressed valuing the components for fear ladder building (9) and psychoeducation (4). Eleven comments expressed general positive impressions of the application. Five comments liked the ability to track patient progress and three comments liked the support for providing exposure therapy. Fourteen therapists provided 22 comments about what they liked least about the program. Eight comments referenced the complexity of the technology, six had difficulties with the approach in general (three disagreed with exposure therapy, two had difficulty engaging patients, one disliked the technology), five comments referenced weaknesses in the design, and five referred to technical problems. Nine therapists provided 15 comments regarding what changes they recommended to the application. Seven comments referred to improving the design or functioning of the application such as simplifying it or allowing the printing of material. Six comments referenced expanding the content, including adding more exposure categories (3). Two comments recommended changes to the therapy content (i.e., slower pace, no exposures).
Therapist Comments.
Use
At Time 3, 94.1% of the therapists reported treating children with an anxiety disorder at least sometimes over the past 6 months, the remaining 5.9% (n = 1) reported treating such patients rarely. The disorder most frequently reported treated during that time was GAD (94.1% sometimes or more frequently). Approximately half of the therapists (52.9%) reported using the application with a few of their patients with anxiety, while 23.5% reported using it with some, 5.9% with most, and 17.6% with none. The most frequently endorsed reason for using the application was that it might help engage patients in treatment (10), followed by it helped keep treatment focused on exposures (9), it provided more information about patient homework completion (5), and was more convenient than paper and pencil materials (3). The most frequently endorsed reasons for not using the application were patients not having the applicable mobile device (11), it required more work than paper and pencil materials (6), it didn’t seem appropriate for their patients (5), patient refusal (5), patients not wanting to pay for the mobile application (3), not thinking exposure was appropriate for their patients (3), not treating patients with anxiety (2), and didn’t think about it (1).
Data collected through the electronic application suggested that 6 therapists attempted to use the application with 11 patients. The data suggested that the application was used to begin a fear ladder (7), connect to the patient’s mobile device (4), provide at least one symptom rating (3), and record an exposure (2 recorded for 1 patient). Fear ladders were at times built 1 to 3 weeks after creating the patient’s account. Only one patient account included entries suggestive of a course of treatment (4-item fear ladder created 3 weeks after beginning treatment with six symptom-ratings over 7 weeks decreasing from 7 to 4, although no recorded exposures). Three therapists contacted the intervention specialist with procedural questions (i.e.., Can two patients use the same app? Do patients use the computer portal or mobile app? How do I find a patient after I save them?).
Discussion
The current study examined therapist response to a brief technology-assisted training in exposure therapy for CADs. The results suggest that exposure-focused training was acceptable to community therapists, based on their self-report, and has the potential to increase use of exposure in the treatment of CADs. Therapists were also accepting of the technology, despite limitations to the current functionality. However, data collected through the technology suggested that therapists did not incorporate use of the Anxiety Coach application with their patients. The successes and shortfalls of the current trial have implications for therapists’ attitudes toward disseminating evidence-based therapy for CADs, supporting therapist behavior change, and therapist adoption of technology in treatment.
The current study suggests that community therapists were generally open to increasing their use of exposure when treating CADs and to the idea of incorporating technology into their practice. The vast majority endorsed an intention to use exposure after the training and reported using exposure with their patients over the subsequent 6 months. This increase in reported use of exposure was accompanied by decreased negative beliefs about exposure and an initial decreased tendency to work with children individually, as opposed to jointly with the parents. Moreover, the increase in exposure endorsement was accompanied by a small initial decrease in use of AMS and non-CBT components. This is particularly noteworthy given that previous efforts to disseminate multi-component CBT have resulted in therapists primarily using non-exposure CBT strategies rather than exposure. Therapist comments and reasons for using the technology also frequently referenced appreciating having support in the delivery of exposure and its related procedures, e.g., fear ladder building. These positive responses are noteworthy given that the sample appeared to be initially as reluctant to use exposure-based therapy as community clinicians are in general and the improvements in beliefs about exposure and endorsement of using exposure, only began after the training. Finally, the changes were achieved with a brief, 90-minutes, single training session that covered two topics: teaching parent-coached exposure therapy and how to use a new technology.
Despite the success of increasing acceptance of exposure, the current study highlights the need to collect objective actionable data about behavior change and the potential role of technology in this collection. Consistent with the previous literature (Beidas & Kendall, 2010), the current study was not able to provide data documenting that the training and technology was able to change therapist behavior. Although all therapists reported treating anxious youth during the post-training trial period and the majority reported using exposure with them, the Anxiety Coach usage data did not capture implementation of exposure (as tracked by the application) during the study period. Specifically, in total two exposures were recorded with a single patient, although about a third of the therapists built a fear ladder presumably to guide exposure. Objective data regarding use has the potential to more accurately measure the effectiveness of dissemination efforts and to improve fidelity through data-driven supervision. Currently, such use data is only available through therapist’s report (Chu et al., 2015), review of clinical notes (Whiteside, Sattler, Hathaway, et al., 2016), recording and coding of sessions (Southam-Gerow et al., 2010), or observing and recording performance-based role-play (Beidas et al., 2012). Automatically collected use data, such as demonstrated here, likely provides more accurate data than the former approaches and is less resource intensive than all of the currently available approaches, making it potentially feasible in clinical settings. Although the current lack of exposure use data may underestimate actual exposure use (i.e., exposures recorded via paper and pencil or left unrecorded), a conservative interpretation of the current data, suggest change in therapist behavior was limited.
The current study suggests it will be difficult to deliver a technology-enhanced treatment platform that therapists will voluntarily adopt into their practice. Overall, the therapists appeared open to the application under study. The majority rated the technology as good or excellent, generally agreed that it would be easy to use and that the training was adequate. The majority also reported using the technology with their patients and many of the comments provided by the therapists were positive and included recommendations for expanding the content, suggesting that therapists saw the value the technology could bring to their practice. However, the use data suggested that less than one-third of the therapists attempted to use the application and their use was minimal in terms of number of patients and engagement with the full offering of the application (e.g., to plan and track exposures). The most frequently endorsed reason for not engaging with Anxiety Coach was that it required more effort than their status quo paper and pencil approach. Lack of fit with, or acceptance by, patients was the next most frequently endorsed barrier. The lack of use and associated reasons underscores the need to develop technologies that are integrated into a clinician’s daily workflow by being applicable to all patients, decreasing work burden, and being attractive to patients. Moreover, practicing clinicians may be more likely to use technology if it has been introduced early in training, embedded into electronic medical records, has minimal barriers to adoption, and provides financial incentives in terms of reimbursement.
The current study has a number of limitations. First, data collection was designed to examine therapist response to a training program to inform revisions in preparation for a randomized controlled trial. As such, the sample was small. In addition, we introduced therapists to three new items (exposure-focused therapy without AMS, integrating technology into therapy, and the characteristics of the specific digital application) and we cannot determine how they would have reacted to each in isolation. Each of these items likely influenced how therapists perceived the other items, as some therapists rejected the premise of exposure therapy, some indicated that it was more work to use technology than paper and pencil, and some commented on technical problems. Technical and design weaknesses of the current application likely interfered with therapist attempts to implement it in practice. However, it seems inaccurate to attribute the low uptake to design issues alone as the basic functioning of the application is supported by a previous pilot study (Whiteside et al., 2019), therapists were encouraged to contact the intervention-specialists with questions (which they did not), and the majority of the therapists appeared to not have engaged with the technology at all, as opposed to giving up after experiencing poor performance. As such, the generalizability of the findings to technology in general remains to be seen.
Another limitation was the lack of ongoing support for therapists during the study. While therapists were encouraged to use the technology in their practice and to contact the intervention specialist when needed, there were no requirements placed on the therapists, nor was any proactive support provided. As such, based on the previous dissemination literature identifying the importance of ongoing supervisory support (Beidas et al., 2012), the current design was unlikely to lead to significant changes in therapist behavior, which is reflected in the fact that the therapists’ description of their practice after 6 months continued to consist predominately of non-exposure CBT components and looked similar to the practice description in the normative study (Whiteside, Deacon, et al., 2016). However, initial training with no follow-up likely accurately reflects most real-world continuing education efforts, thus this study provides relevant information about current practices. Next, direct data regarding therapist use of exposure was only collected through the computer-based component of Anxiety Coach, thus data on the use of the mobile-based device by patient or therapist (without the computer-based component), and exposures conducted without the aid of the technology was not available. Finally, no additional information was available about the specific patients treated by each therapist during the study period, limiting our ability to verify the accuracy of the reported diagnoses. This limitation is notable given the high frequency of typically infrequent disorders (e.g., panic and OCD) reported by the community therapists. The predominance of GAD presentations could have discouraged use of exposure since the use of worry exposures is less intuitive than in vivo exposure or if the diagnoses were inaccurate, that is, included general distress or adjustment for which exposures might not be appropriate. Moreover, the absence of data collected from the patients prevents any conclusions about patient factors that may have influenced adoption and use.
Despite these limitations, we propose that the current data supports three conclusions with implications for future research. First, many therapists appear open and responsive to training that emphasizes exposure alone without other AMS. The reported increase in exposure at the expense of other anxiety management strategies suggest potential for improving upon dissemination of multi-modal CBT that has failed to lead to increased use of the most effective ingredient of CBT for CADs. Second, objective data regarding fidelity will be needed to provide accountability, and technology has the potential to collect data in a manner that is feasible outside of research studies. Finally, even a well-designed, easy to use technology will likely face high barriers to adoption by clinicians. To be adopted, technology will need to fit into the clinician’s’ daily workflow by meeting the needs expressed by clinicians. Only if these goals can be met, will technology have the potential to transform the way in which mental health care is provided.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was support by a grant from the National Institute for Mental Health, 1R34MH100468-01.