
Abstract
Anxious children report a more negative perception of their social performance and increased nervous behaviors. The video-feedback with cognitive preparation allows children to contrast and modify their negative social self-image, increasing their self-confidence and decreasing anxiety behaviors. This study aimed to examine the effectiveness of the Super Skills for Life (SSL) program in improving social performance in a sample of children with emotional symptoms. Results indicated that both objective and subjective evaluation showed positive effects of the SSL program on the children’s social performance, enhancing their social skills and reducing anxiety behaviors in social situations, both during the program and in the last session. Girls felt more comfortable and showed better speech and social performance than boys. Our findings increase the evidence about the short-term effects of the video-feedback with cognitive preparation of the SSL program and provide a useful transdiagnostic protocol for application in the clinical setting.
Introduction
Emotional problems at an early age are highly prevalent and have negative consequences in different areas of children’s lives (Aebi et al., 2014; Cullins & Mian, 2015; Kovess-Masfety et al., 2016; Polanczyk et al., 2015). Although fears are widespread during childhood and have an adaptive function, the anticipation of potential threats triggers negative thoughts that contribute to the emergence of emotional symptoms and distress (Canals et al., 2019; Muris et al., 2000). When these symptoms are frequent, they are known as anxiety disorders, which are the most common psychological problems in children and adolescents (Ghandour et al., 2019; Polanczyk et al., 2015). The prevalence of anxiety problems in children ranges from 6.6% to 47% worldwide, however, the subtypes of anxiety differ according to age (Canals et al., 2019; Ghandour et al., 2019). Preschoolers and young children tend to fear separation from their significant caregivers, animals, noises, darkness, and other specific phobias, while as they grow older, social fears become more important (Franz et al., 2013; Merikangas et al., 2010; Vicente et al., 2012). Early detection and intervention in these emotional problems are recommended to avoid their chronification, greater severity and the appearance of other psychological difficulties, such as other anxiety and depression disorders, behavioral problems, negative self-concept, and social skills deficits (Broeren et al., 2013; Jaureguizar et al., 2018; Willner et al., 2016).
The association between emotional problems in children (especially social anxiety) and lack of social skills has been reported in numerous studies (Albano & Hayward, 2004; Miers et al., 2013; Segrin & Flora, 2000; Spence et al., 1999; Wichstrøm et al., 2013). However, most of these studies have used children’s self-reports to assess their own social skills and social performance, which can produce biased results (Cartwright-Hatton et al., 2005). In contrast, other studies have found that when social performance is objectively assessed, anxious children did not necessarily have poorer social skills or social interaction than non-anxious children (Cartwright-Hatton et al., 2003, 2005). The main difference is that anxious children report a more negative perception of their social performance and increased nervous behaviors (Cartwright-Hatton et al., 2003; Ramos et al., 2008). Negative self-image causes anxious children to lack confidence during social interactions, anticipate worse outcomes, and report inadequate social performance (Cartwright-Hatton et al., 2003; Orgilés et al., 2020; Spence et al., 1999). Since social competence is related to internalizing symptoms and social rejection in childhood, interventions must not aim only at enhancing social skills, but also at improving children’s negative thoughts and social self-image (Huber et al., 2019; Milligan et al., 2017; Orgilés et al., 2020).
An example of this kind of intervention is the Super Skills for Life program, created by professors Essau and Ollendick (2013), a transdiagnostic prevention protocol aimed at children with emotional problems (i.e., anxiety and/or depression). The SSL program consists of eight sessions in which different effective cognitive-behavioral techniques are used to teach children how to improve their mood and cope with anxiety-provoking situations. These include psychoeducation, cognitive restructuring, behavioral activation, relaxation, problem-solving, social skills training, and video-feedback with cognitive preparation. The last component has been shown to be effective in improving children’s social performance, since video-feedback allows children to contrast and modify their negative self-image in social situations, increasing their self-confidence and decreasing their anxiety in future interactions (Clark & Wells, 1995; Harvey et al., 2000; Parr & Cartwright-Hatton, 2009; Ramos et al., 2008; Rodebaugh, 2004). The SSL program includes videotaped activities in which children must act in front of a camera and their peers (in the group version), conducting a 2-minute speech task or interacting with another person, and then evaluate their social performance. Before watching their videos, cognitive preparation allows children to imagine how their performance has been and helps them to objectively assess their behaviors during the speech (Essau et al., 2014; Morgan & Banerjee, 2006).
The original version of the SSL program proved to be effective in significantly reducing anxiety and improving the social performance behaviors of children aged 8 to 12 with emotional problems (Essau et al., 2014). Likewise, the Spanish version of the program obtained even more positive results, since the enhancement in social skills and the decrease in signs of nervousness and discomfort were evident from the posttest (Orgilés et al., 2020). In these studies of SSL, girls showed better social skills and social performance than boys, as well as in previous research on the treatment of social anxiety (Essau et al., 2014; Orgilés et al., 2020; Ramos et al., 2008; Rodríguez et al., 2003). These promising results were obtained in group modalities of the program, however, the effects of the individual format of SSL on improving children’s social performance have not yet been examined. Besides, the program has been delivered in school settings until now, and in the one-to-one version children received the SSL protocol in a clinical setting with more personalized attention (Melero et al., n.d.).
Therefore, the current study aimed to examine the effectiveness of the SSL program in improving the social performance of children with emotional problems through two objectives: (1) to analyze the impact of the video-feedback with cognitive preparation component on the improvement of children’s social performance through an objective and subjective evaluation, and (2) to explore gender differences in the objective and subjective change of children’s social performance behaviors (gaze, vocal quality, length, discomfort, conversation flow, micro-behaviors, nervous behaviors, and global impression). Based on previous studies of the SSL program, improvements in children’s social performance are expected to be observed after receiving the intervention, through an increase in social skills and a decrease in nervous behaviors (Essau et al., 2014; Orgilés et al., 2020). Furthermore, we hypothesize that SSL’s impact on social performance will be different according to gender, with girls showing better social skills and less nervous behavior than boys after treatment (Essau et al., 2014; Orgilés et al., 2020).
Methods
Participants
A total of 70 children aged between 8 and 11 years old (M = 9.34; SD = 1.15) participated in the study. Of these, 41 were boys (58.6%) and 29 were girls (41.4%). The participants were recruited from 28 public, charter, and private schools in central and southeastern Spain. All the children were Spanish speaking, although 94.3% were born in Spain and the rest in the United Kingdom (n = 3; 4.3%) and Brazil (n = 1; 1.4%). The children were mostly from upper-middle- and middle-class families. The mean number of siblings was 0.93 (SD = 0.62).
The children were selected to participate in the study through a screening instrument for emotional problems completed by the parents. This instrument was the Strengths and Difficulties Questionnaire (SDQ-P; Goodman, 2001), and a score equal to or greater than 4 on the emotional symptoms subscale was considered an inclusion criterion. The exclusion criterion was that children were currently receiving psychological or pharmacological treatment for emotional or behavioral problems. Selected children were evaluated at the baseline (Session 1), during the program (Session 7) and immediately after receiving the intervention (Session 8) (97.1% retention). All the children who answered the three time points were included in the analyses.
Measures
Sociodemographic variables
Sociodemographic variables were obtained by a set of items that evaluated gender, age, gender, school year, number of siblings, and the birthplace of the participants.
Rater-reported measures
The Social Performance Rating Scale (SPRS; Fydrich et al., 1998) evaluates behavioral indicators of anxiety in a videotaped social performance. The scale is composed of five dimensions: Gaze, Voice Quality, Length, Discomfort, and Conversation Flow. Each dimension is evaluated with a five-point Likert scale. The sum of these dimensions provides the total score. Observers were trained according to the guidelines provided by Fydrich et al. (1998). The internal consistency was adequate (α = 0.71) in the current sample.
The Objective Performance Questionnaire (OPQ-C; Cartwright-Hatton et al., 2003) requires an observer to rate the child’s performance during the 2-minute speech task. This scale contains eight items grouped into three dimensions: Micro-Behaviors (displayed during the social situation), Nervous Behaviors (how comfortably the child performs in front of the camera) and Global Impression (overall opinion of the performance). Each item is scored on a four-point Likert scale ranging from 1 (not very much) to 4 (very much). The scale had adequate reliability (α = 0.80) in this study.
Self-reported measures
The Performance Questionnaire (PQ-C; Cartwright-Hatton et al., 2003) is a self-report instrument completed by children to rate their social performance during a speech task. This scale contained the same eight items and the three dimensions as the OPQ-C (micro-behaviors, nervous behaviors and global impression), but the words “the child” in the items were replaced by “you.” The children should score each item on a range from 1 (not very much) to 4 (very much). The reliability of this scale was .74 in this sample.
Parent-reported measures
The Strengths and Difficulties Questionnaire—Parent version (SDQ-P; Goodman, 2001) is a brief screening questionnaire for assessing children’s and adolescents’ psychological adjustment. Its 25 items comprise five subscales: Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention, Peer Problems, and Prosocial Behavior. In this study, only the Emotional Symptoms score was used to select the participants. Following the original three-band categorization, cut-off scores of 4 or above were established, corresponding to the borderline and abnormal categories. These bands represent the presence of anxious and depressive symptoms in children, which increase the risk of developing more severe disorders (Goodman, 2001). Thus, children included in these bands were selected to receive the program. The Spanish parent version showed a Cronbach alpha coefficient of .71 for the Emotional Symptoms subscale (Rodríguez-Hernández et al., 2012). The ordinal alpha of the emotional symptoms scale was .36 in this study.
Procedure
This study was approved by the Institutional Review Board (IRB) of Miguel Hernández University, Spain (DPS.MO.01.17). Five primary schools in the provinces of Alicante and Madrid were randomly selected, were contacted to request their collaboration in the study. The headmasters who agree to participate distributed a letter to the families of students in grades 2nd to 6th informing about the research aims. The study was also advertised on social networks through an institutional account. Then, interested parents voluntarily completed an online form about their children’s emotional state that served as a screening tool. Children who met the inclusion and exclusion criteria above were included in the study. Parents provided informed consent for their children to participate and were informed about the SSL intervention, the objectives of the research and the confidentiality of their data.
The SSL program was delivered in its one-to-one version at the authors’ institution. Facilitators were psychologists (both genders) specialized in child and adolescent psychology and with more than 2 years of experience. All of them received an intensive training to explain the ethical issues, contents, objectives, and methodology of the sessions comprising the SSL program before its implementation. In addition, they were provided with the implementation manual, a video camera and school supplies. The researcher in charge held weekly meetings with the facilitators to supervise the proper protocol application, provide material, and collect data. Only the therapist and child were involved during the program, and the parents received brief oral feedback at the end of each session.
The SSL intervention consisted of eight weekly 45-minute sessions in which children learn skills to identify and manage their own and others’ emotions, improve mood and self-concept, relax, interact with others, cope with anxiety-provoking situations, and solve problems. The different techniques used include social skills training and video-feedback with cognitive preparation. These strategies were applied in the first, sixth, and last session, in which the children gave a 2-minute speech facing a video camera. In the first session, the child had to imitate a TV presenter introducing him/herself and sharing personal information (favorite dish, animal, and hobby). The same activity was repeated in the eighth session, also including information on which SSL activities they liked the most and which skills they considered most useful for their life, as an exercise of the generalization. In the sixth session, the videotaped activity consisted of performing a social situation between the child and therapist, in whom the child had to start a conversation with an unknown person and say goodbye properly.
Before the children watched their videos, they completed the PQ-C (Cartwright-Hatton et al., 2003) instrument by thinking about how they had performed during the speech task. They were then cognitively prepared to attend to their verbal and non-verbal language and overall social performance during their speech. After watching their videos, the children again completed the PQ-C scale by analyzing their social performance more objectively and subsequently the two assessments were contrasted. Recordings of each child were also independently rated by two psychologists with a master’s degree in child psychology, trained as observers. Both raters were blind to other children’s scores in other measures and did not participate in the SSL program implementation. Observers individually scored the children’s social performance using the previously indicated scales (see measurement section) and discrepancies between them were discussed in order to reach an agreement and obtain a final score. The final rating scores were used to evaluate the effectiveness of the intervention to change social performance outcomes in the speech task.
Statistical Analysis
SPSS Statistics 25.0 was used for data analysis. Results were analyzed using an intent-to-treat analysis (n = 70) such that information from all participants was included in the analyses. The equivalence between participants who enrolled in the study and those who dropped out was analyzed using cross-tables (categorical variables) and Mann–Whitney U test (continuous variables). The variables analyzed on social performance were evaluated through the viewing of videos by two raters (objective evaluations) and by the children (self-reported or subjective evaluation). The equivalence of the two raters was tested using Spearman-Brown. Discrepancies were resolved by agreement between the two raters. The repeated-measures data for the outcomes (SPRS, OPQ-C, and PQ-C) were analyzed using generalized estimating equations (GEE) (Liang & Zeger, 1986). The intervention effects were adjusted for covariates, including children’s age and gender, and baseline values for each outcome. A new variable “time” was created and included as categorical measure and group (children’s gender) by time interaction, to analyze differences in the time of the total sample, boys and girls. Gender differences in the outcomes were also explored. The level of statistical significance was set at a p-value of less than .05.
Results
Attrition
Attrition analysis revealed that children who were recorded and enrolled in the analysis of the efficacy of SSL regarding social performance (n = 68) and those who were not (n = 2) were equivalent in sociodemographic variables, including gender (p = .08), age (p = .15) and school level (p = .50) and number of siblings (p = .28).
Interjudge Reliability
The correlation coefficients of the two independent observers’ ratings for the SPRS and OPQ-C measures are shown in Table 1. The concordance index for these calculations was above 0.96 at the pretest, 0.87 during the intervention, and 0.93 at the posttest, indicating excellent inter-rater reliability on all subscales. Thus, a high agreement was obtained among the raters in the recording assessments.
Spearman Correlations for Interjudge Reliability.
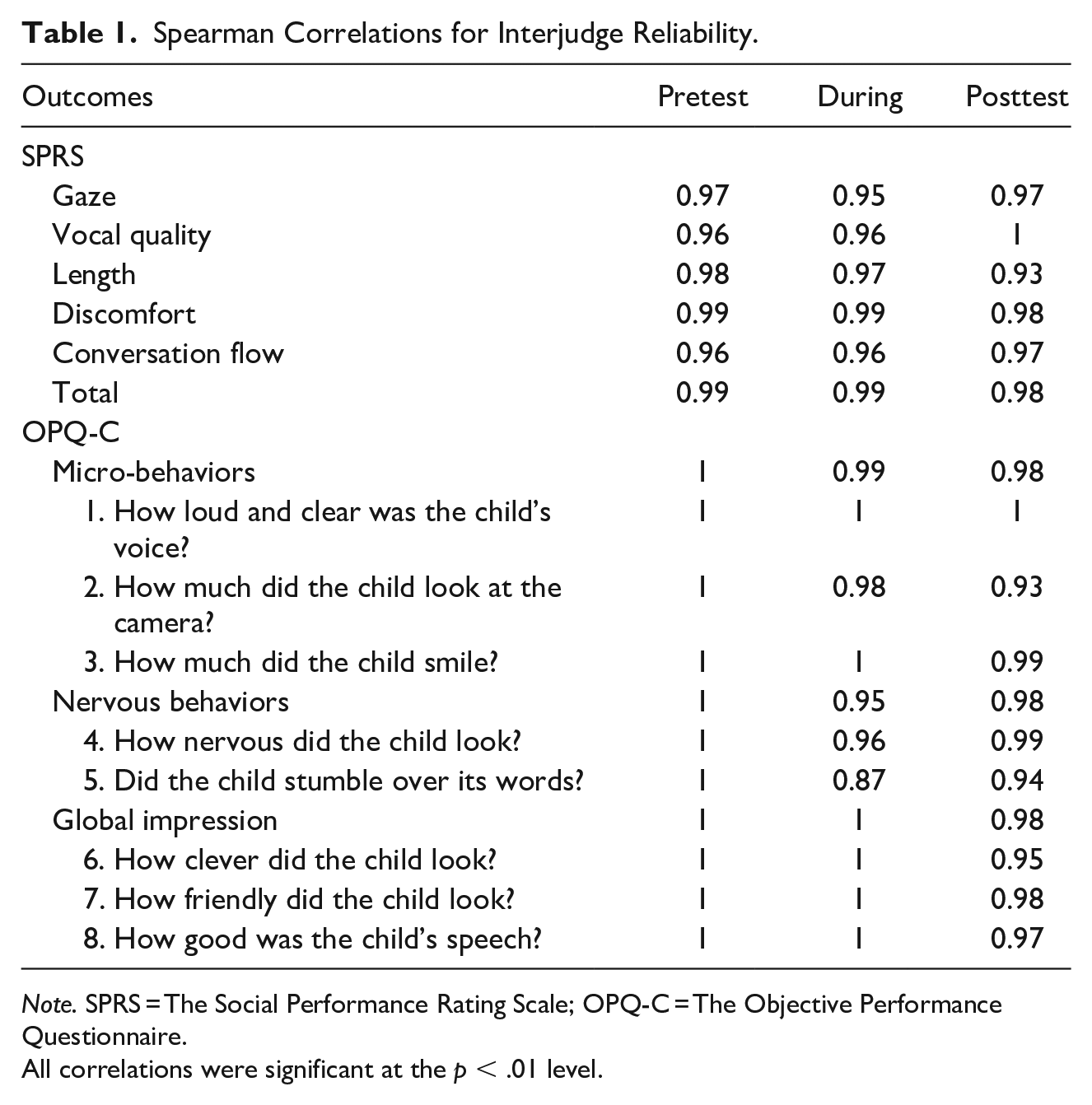
Note. SPRS = The Social Performance Rating Scale; OPQ-C = The Objective Performance Questionnaire.
All correlations were significant at the p < .01 level.
Objective Ratings of Social Performance Changes
Two objective observers analyzed the children’s recordings at all three time points. Table 2 shows the estimated marginal means of the children’s social performance in the speech task at the baseline, during the treatment and at the last session, by gender and for the total sample. Table 3 illustrates the effect of the program on the children’s social performance in the recordings for session 6 and session 8, compared to session 1.
Estimated Marginal Means (Confident Interval) of the Outcomes Between Pretest and During Treatment, Between Pretest and Posttest, and by Gender.

Note. Higher scores denote greater social skills except for “nervous behaviors” which higher scores indicate greater anxiety behaviors. CI = confidence interval; SPRS = The Social Performance Rating Scale; OPQ-C = The Objective Performance Questionnaire.
Generalized Linear Models and Effect Size Estimates for the Intervention Effect on the Speech-Task Outcomes During the Treatment and in the Posttest (Both Compared to the Baseline) and by Gender.
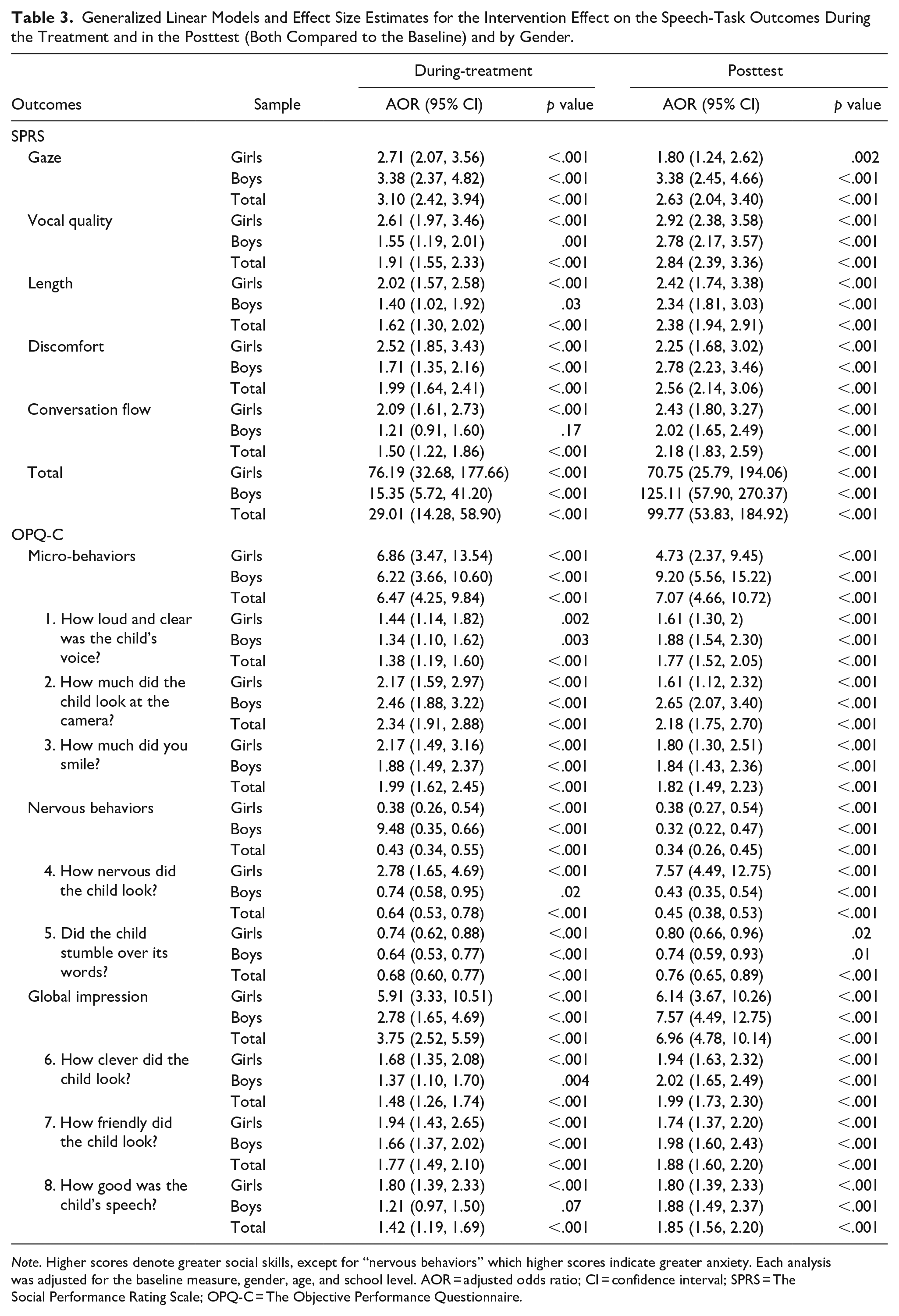
Note. Higher scores denote greater social skills, except for “nervous behaviors” which higher scores indicate greater anxiety. Each analysis was adjusted for the baseline measure, gender, age, and school level. AOR = adjusted odds ratio; CI = confidence interval; SPRS = The Social Performance Rating Scale; OPQ-C = The Objective Performance Questionnaire.
The social behavior in the activity of interacting with an unknown person (Session 6) improved significantly in all subscales compared to the first speaking task for the overall sample. When these results were analyzed by gender, significant changes were observed for all social performance measures for both boys and girls, except for males in the Conversation flow variable of the SPRS (p = .17) and the “How good was the child’s speech?” item of the OPQ-C (p = .07). Comparing the results between males and females, the improvement in Discomfort (p = .05), Total social performance (Total SPRP; p = .01) and speech adequacy (item 8; p = .02) were found to be greater for girls.
Regarding the change between pretest and posttest, significant within-subject improvements were found for all the outcomes of the SPRS (Gaze, Vocal quality, Length, Discomfort, Conversation flow, and Total) and OPQ-C (Micro-behaviors, Nervous behaviors, and Global impression) for the general sample and for both genders (p-values ranging from .02 to < .001). Although both boys and girls improved significantly at posttest, the impact of the program was greater for boys on gaze-related variables, that is, Gaze of SPRS (p = .01) and item 2 “How much did the child look at the camera?” of OPQ-C (p = .02). Therefore, children reduced their nervous behaviors and increased their overall social and communication skills during the program sessions and after the end of the SSL intervention.
Subjective Ratings of Social Performance Changes
The children evaluated their social performance before and after watching their three recordings. Table 4 shows the estimated marginal means for both assessments at each time point (pretest, during-treatment, and posttest) for the overall sample and by gender. For the total sample, the scores of the Micro-behaviors and Global impression subscales and their items increased or remained stable after the children’s cognitive preparation score of the scale (except items 1 and 2 at the pretest). The scores of the Nervous behaviors subscale and its items decreased after cognitive preparation at pretest, at during-treatment (except item 5), and posttest.
Estimated Marginal Means (Confident Interval) of the PQ-C at Before and After the Speech Task in the Three-Time Points (Pretest, During, and Posttest), and by Gender.
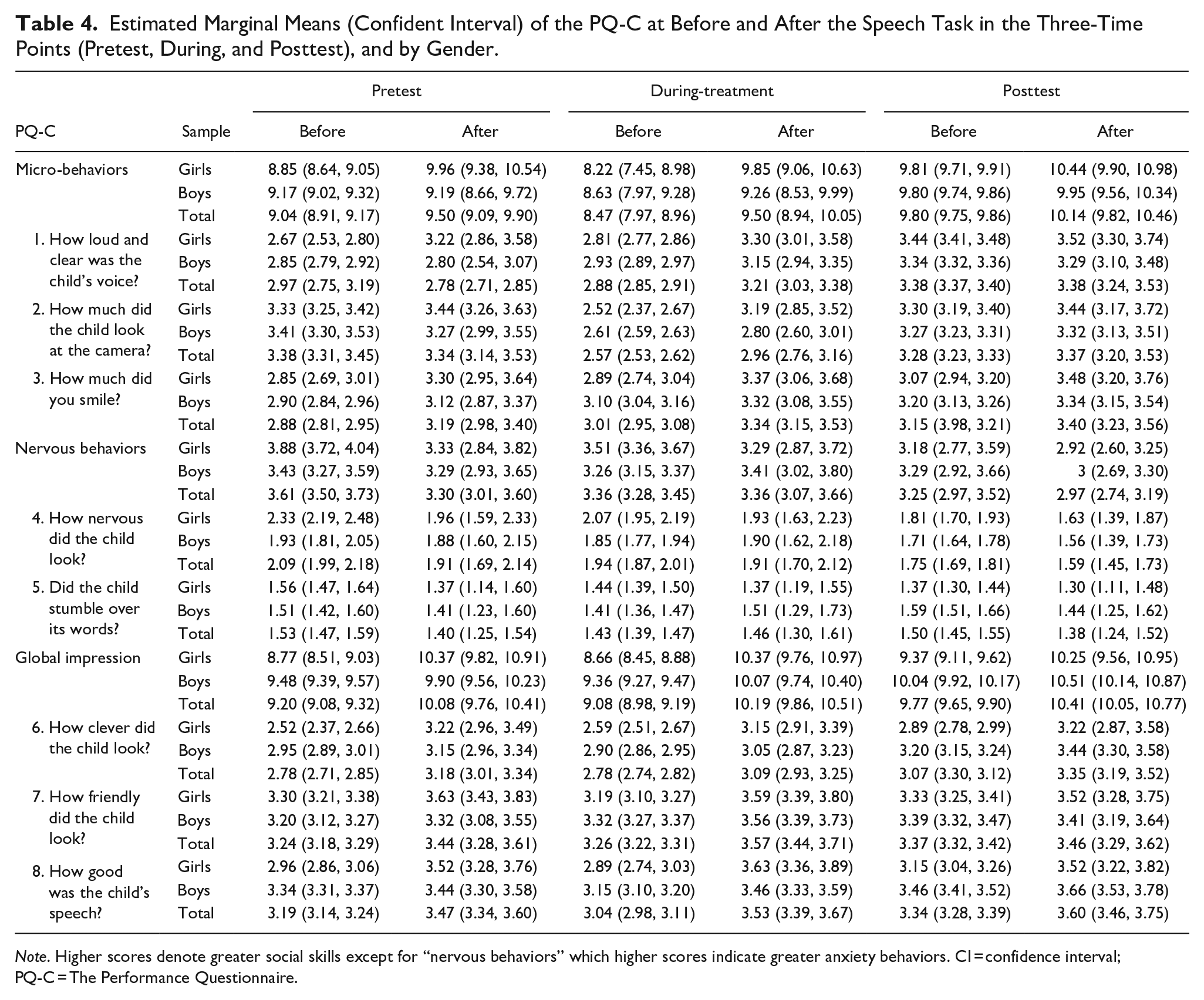
Note. Higher scores denote greater social skills except for “nervous behaviors” which higher scores indicate greater anxiety behaviors. CI = confidence interval; PQ-C = The Performance Questionnaire.
These changes were statistically significant at all three time points for Micro-behaviors, Global impression, and the items “How much did you smile?” (item 3), “How clever did the child look?” (item 6) and “How good was the child’s speech?” (item 8). Item 7 “How friendly did the child look?” obtained significant differences in the pretest and during-treatment but not in the posttest. The items “How loud and clear was the child’s voice?” (item 1) and “How much did the child look at the camera?” (item 2) only showed a significant difference between the before and after evaluation of the recordings in session 6 (during-treatment). Finally, the Nervous behaviors subscale decreased significantly only in the posttest (Table 5). Therefore, the children’s scores before and after watching their videos were more equal in the last session.
Generalized Linear Models and Effect Size Estimates for the Intervention Effect on the Speech-Task Outcomes (PQ-C) at Before and After the Task in the Three-Time Points (Pretest, During, and Posttest), and by Gender.
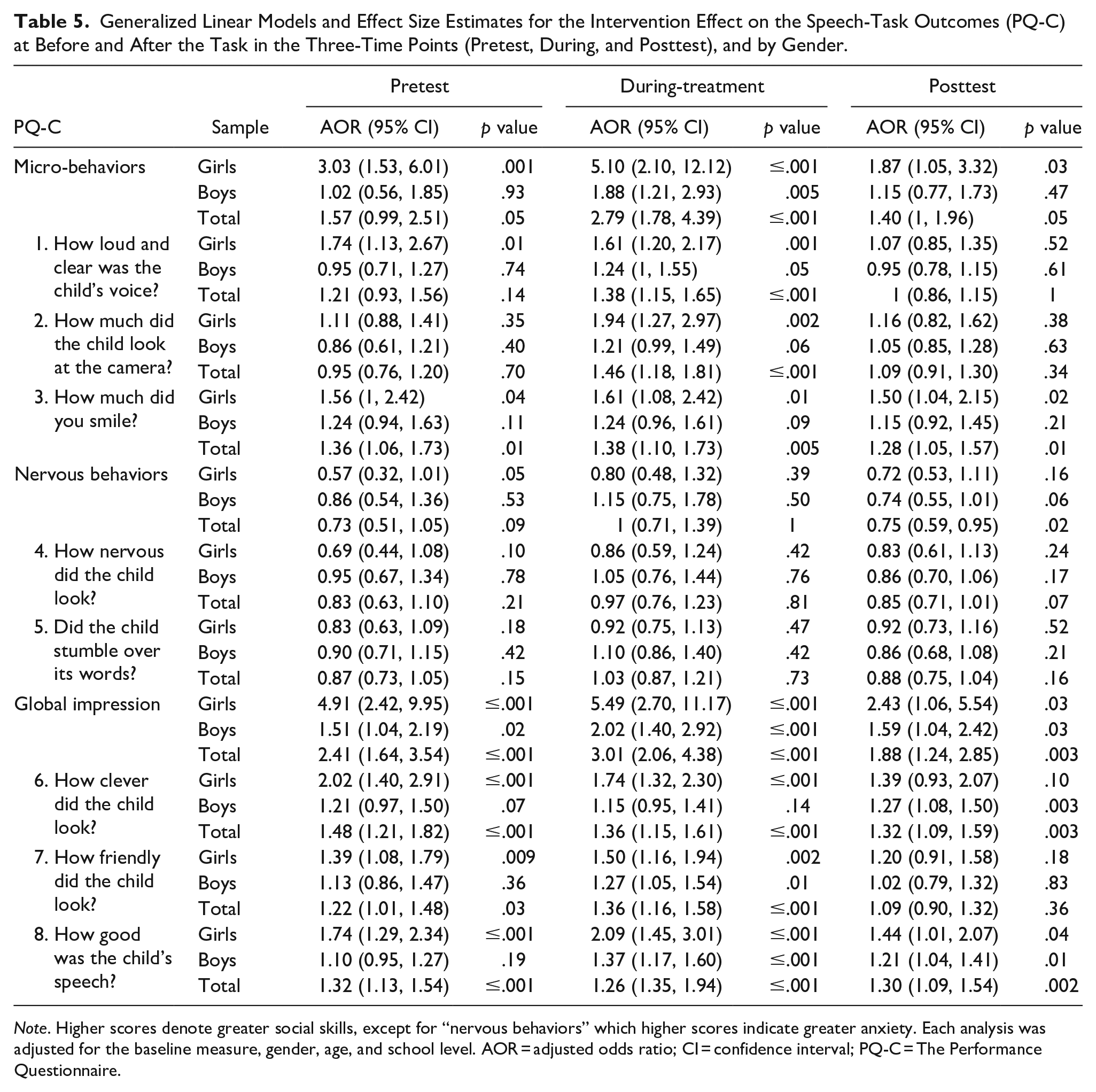
Note. Higher scores denote greater social skills, except for “nervous behaviors” which higher scores indicate greater anxiety. Each analysis was adjusted for the baseline measure, gender, age, and school level. AOR = adjusted odds ratio; CI = confidence interval; PQ-C = The Performance Questionnaire.
Regarding gender differences in the children’s rating, Table 4 shows that girls scored higher in the Micro-behaviors and Global impression subscales and all their items, and lower in the Nervous behaviors subscale and its items after cognitive preparation at all three time points. These improvements were especially significant for the variables Micro-behaviors, Nervous behaviors and Global impression, as well as for the smile (item 3), clever (item 6), friendly (item 7), and speech adequacy (item 8) at pretest. In session 6, significant differences were identified for the variables Micro-behaviors and Global impression, as well as for their items. Finally, the differences were reduced in the posttest, being only found in Micro-behaviors, Global impression and speech adequacy (item 8) (Table 5). Boys obtained similar improvements, especially significant in Global impression in the three measurement times, Micro-behaviors and voice (item 1), friendly (item 7), and speech adequacy (item 8) in the activity of interaction with an unknown person, and clever (item 6), and speech adequacy (item 8) in the final session (Table 5).
Significant between-subject effect of gender was obtained at pre-treatment, with the girls obtaining better scores in Micro-behaviors (p ≤ .001), voice (item 1; p = .01), smile (item 3; p = .04), Nervous behaviors (p = .054), Global impression (p ≤ .001), clever (item 6; p ≤ .001), friendly (item 7; p = .009), and speech adequacy (item 8; p ≤ .001) compared to boys. The girls also showed greater improvements than the boys in Micro-behaviors (p ≤ .001), voice (item 1; p = .001), gaze (item 2; p = .002), smile (item 3; p = .01), Global impression (p ≤ .001), clever (item 6; p ≤ .001), friendly (item 7; p = .002), and speech adequacy (item 8; p ≤ .001) in the activity of Session 6. These gender differences decreased in the posttest, as girls scored higher only on Micro-behaviors (p = .03), smile (item 3; p = .02), Global impression (p = .03), and speech adequacy (item 8; p = .04) than boys. In conclusion, the children’s self-report suggested that the impact of the program was greater on girls than on boys.
Discussion
The main objective of this study was to examine for the first time the impact of the individual modality of the Super Skills for Life program in improving the social performance of children with emotional problems. Different from previous research on SSL, this study included both objective and subjective evaluation of the social performance of children intervened in a clinical context on an individual basis. Additionally, as a novelty, the evaluation of the “meeting people” activity of Session 6, in which the child performs a role-playing game interacting with his/her therapist, was also included. The effects of the video-feedback with cognitive preparation component on the improvement of social performance behaviors (i.e., gaze, vocal quality, length, discomfort, conversation flow, micro-behaviors, nervous behaviors, and global impression) during videotaped activities were analyzed for the whole sample and according to gender for both perspectives. As hypothesized, the SSL program in one-to-one format showed positive short-term effects on the children’s social performance, with an improvement in their social skills and reduction of nervous behaviors (Essau et al., 2014; Orgilés et al., 2020).
The video-feedback technique is considered a useful CBT-based component for individuals who evaluate their performance during social tasks negatively, even though their social skills are adequate (Rodebaugh & Rapee, 2005). Moreover, the addition of cognitive preparation to this technique increases its beneficial effects, since it allows a more realistic assessment of behaviors in the speech task and a better performance in the subsequent speech (Harvey et al., 2000; Kim et al., 2002; Morgan & Banerjee, 2006). According to the previous studies, our results showed that the use of video-feedback with cognitive preparation had a positive effect on the children’s social performance, enhancing their social skills and reducing anxiety behaviors in social situations (Essau et al., 2014; Orgilés et al., 2020; Ramos et al., 2008). The objective observers and the children reported these improvements both during the program and in the speech task of the last session.
At the baseline, children significantly improved their scores on the variables micro-behaviors, global impression, smile, cleverness, friendliness, and speech adequacy after watching their videos. The objective raters observed significant positive changes in all of the children’s social behaviors (gaze, vocal quality, length, conversation flow, micro-behaviors, and global impression) and signs of nervousness (discomfort and nervous behaviors) during the intervention and in the posttest compared to the pretest. These results are consistent with previous studies that have examined the effectiveness of the SSL program in improving children’s social performance (Essau et al., 2014; Orgilés et al., 2020). In the “meeting people” activity in Session 6 the children reported significant improvements in variables related to micro-behaviors and global impression, although these were lower than those reported by the objective observers. The scores between the assessments before and after the video-feedback with cognitive preparation were more similar in the posttest, which indicates that the children assessed their social performance more objectively at the end of the program. Likewise, these subjective scores were more in line with those assigned by the objective raters at the posttest. These results confirm that children with emotional problems tend to underestimate their social skills and report greater signs of nervousness when compared to the objective evaluation of their social performance (Cartwright-Hatton et al., 2003, 2005; Ramos et al., 2008). However, cognitive preparation has favored the improvement of the children’s social self-image throughout the intervention (Harvey et al., 2000; Morgan & Banerjee, 2006; Parr & Cartwright-Hatton, 2009; Spence et al., 1999).
Analysis of the videotaped tasks showed some gender differences in both reports. According to the children’s report, the girls scored higher on social skills related to micro-behaviors (e.g., gaze, smile) and global impression (e.g., looking friendly, making a good speech) at all three time points. Moreover, objective observers indicated that girls felt more comfortable and showed better speech and social performance than boys in the activity of interacting with an unknown person (Session 6). However, in the posttest, the boys presented a more appropriate gaze to the camera compared to the girls. These findings provide further support for the existing literature, which indicates that girls tend to score higher on social skills and social performance than boys (Essau et al., 2014; Orgilés et al., 2020; Rodríguez et al., 2003). In contrast, the individual version contradicts previous studies in which girls showed greater signs of social anxiety and discomfort compared to boys when the format was group-based (Canals et al., 2019; Orgilés et al., 2020).
This study has shown beneficial short-term changes in the social performance of children who received the SSL program in individual modality. These results have been more positive than in the original version, in which changes were evident in the long-term from both perspectives (Essau et al., 2014). The Spanish group version of the program obtained similar outcomes in the objective evaluation of social behaviors, although there was no significant change in the length of the speech after the intervention (Orgilés et al., 2020). Therefore, in line with studies that have examined the use of video-feedback in individual and group interventions, the individual format showed greater improvements in social performance and less attrition compared to the group versions of SSL (Aderka, 2009; Stangier et al., 2003). This may be due to the advantages that one-to-one intervention offers, as each child receives unique attention tailored to his/her needs, there is more opportunity for in-session exposure and better feedback from the clinician (Aderka, 2009; Ehrenreich-May et al., 2018; Melero et al., n.d.).
In order to correctly interpret the results of this study, some limitations must be noted. Firstly, the sample size was small, because the implementation of the individual version of SSL required a longer time and greater material and human resources (Ehrenreich-May et al., 2018; Melero et al., n.d.). Secondly, as in the original study by Essau et al. (2014), no control group was included for ethical reasons. Thus, future randomized controlled studies with larger samples are needed to confirm the effects obtained from the one-to-one format of the program. Despite these limitations, this is a comprehensive study of the effectiveness of the video-feedback with cognitive preparation component of the SSL program, as it includes both self-reports and objective reports of social performance.
Conclusion
In conclusion, our findings contribute to increasing the evidence about the effects of the SSL program in improving children’s social performance and reducing their anxious behaviors through learned strategies, which are protective factors against the development of more severe disorders (Huber et al., 2019; Milligan et al., 2017; Wichstrøm et al., 2013). In addition, this study provides a useful transdiagnostic prevention protocol for application in the clinical setting in individual modality, which is more feasible in the daily practice of clinicians.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Culture and Sport of Spain (FPU16/02157), and the Ministry of Economy and Competitiveness (MINECO) of Spain (PSI2017-85493-P).